thyroid gland dr. faeza patho
TRANSCRIPT

Thyroid gland
April . 12. 2015

Thyroid gland
• Anatomy• Histology• Physiology• Pathology• Hyperthyroidism• Hypothyroidism• Tumors

15-25 grams

In adults •Two lateral lobes •Isthmus; level of 2nd – 3rd tracheal rings. •The highest rate of blood flow

Thyroid blood supply


High mag of thyroid follicles – note Parafollicular or C-Cells (arrows)
Many vegetables are goiterogens, fruits are NOT
Goitrogens; chemical agents inhibit function of the thyroid gland.Suppress T3 and T4 synthesis, so the level of TSH increases, &t hyperplastic enlargement of the gland (goiter) follows.

Thyrotoxicosis
• A hypermetabolic state caused by elevated circulating levels of free T3 and T4.
• hyperthyroidism

Disorders Associated with Thyrotoxicosis
Associated with HyperthyroidismPrimary• Diffuse hyperplasia (Graves disease)• Hyperfunctioning (“toxic”) multinodular goiter• Hyperfunctioning (“toxic”) adenoma• Iodine-induced hyperthyroidism• Neonatal thyrotoxicosis associated with maternal Graves diseaseSecondaryTSH-secreting pituitary adenoma (rare)Not Associated with HyperthyroidismGranulomatous (de Quervain) thyroiditis (painful)Subacute lymphocytic thyroiditis (painless)Struma ovarii (ovarian teratoma with ectopic thyroid)Factitious thyrotoxicosis (exogenous thyroxine intake)

Thyrotoxicosis
• The 3 most common causes of thyrotoxicosis:• Diffuse hyperplasia of the thyroid associated
with Graves disease (85% of cases)• Hyperfunctional multinodular goiter• Hyperfunctional thyroid adenoma

Hyperthyroidism
Clinical Course. Hypermetabolic state. Overactivity of the SNS
(increase in the β-adrenergic “tone”).

Hyperthyroidism
Increase BMR • The skin; soft, warm, and flushed because of
increased Bl. flow and peripheral vasodilation, adaptations that serve to increase heat loss.
• Sweating is increased because of higher levels of calorigenesis.
• Weight loss despite increased appetite.
Hyperthyroidism
• Cardiac manifestations• Elevated cardiac contractility and cardiac output, in
response to increased peripheral O2 requirements.• Tachycardia, palpitations. • Arrhythmias, particularly Atrial fibrillation.• Congestive HF.• Cardiomegaly
Hyperthyroidism
Over activity of Sympathetic Nervous System;• Tremor, hyperactivity, emotional labile, anxiety,
inability to concentrate, insomnia.• Thyroid myopathy; Muscle weakness and decreased
muscle mass. • GIT, hypermotility, diarrhea, & malabsorption

Hyperthyroidism
• Ocular changes;• Staring gaze• lid lag• Proptosis (only in Graves
Dis)


Hyperthyroidism
• The skeletal system. • Increased bone resorption & risk of
Osteoporosis & fractures• Atrophy of skeletal M.• Minimal liver enlargement due to fatty
changes in the hepatocytes; • generalized lymphoid hyperplasia &
lymphadenopathy in Graves disease.

Thyroid storm
• The abrupt onset of Severe hyperthyroidism.• Occurs in Graves disease, from an acute elevation in
catecholamine levels, (during infection, surgery, cessation of antithyroid medication, or any form of stress).
• Patients are often febrile and present with tachycardia out of proportion to the fever.
• Thyroid storm is a medical emergency. • Untreated patients die of cardiac arrhythmias.

Apathetic hyperthyroidism
• Thyrotoxicosis occurring in older adults, in whom advanced age and co-morbidities may blunt the typical features of hyperthyroidism.
• The diagnosis made during investigations for unexplained weight loss or worsening CV disease.

Diagnosis of hyperthyroidism
• Both Clinical and laboratory findings. • A low TSH value • High free T4. • Serum TSH is the most useful single screening test for
hyperthyroidism, because its levels are decreased even at the earliest stages, when the disease may still be subclinical.
• RAI uptake by the thyroid gland.


“T3 toxicosis”
• Occasionally, hyperthyroidism results from increased circulating T3 (“T3 toxicosis”)
• In these cases, free T4 may decreased,• And measurement of serum T3 may be useful

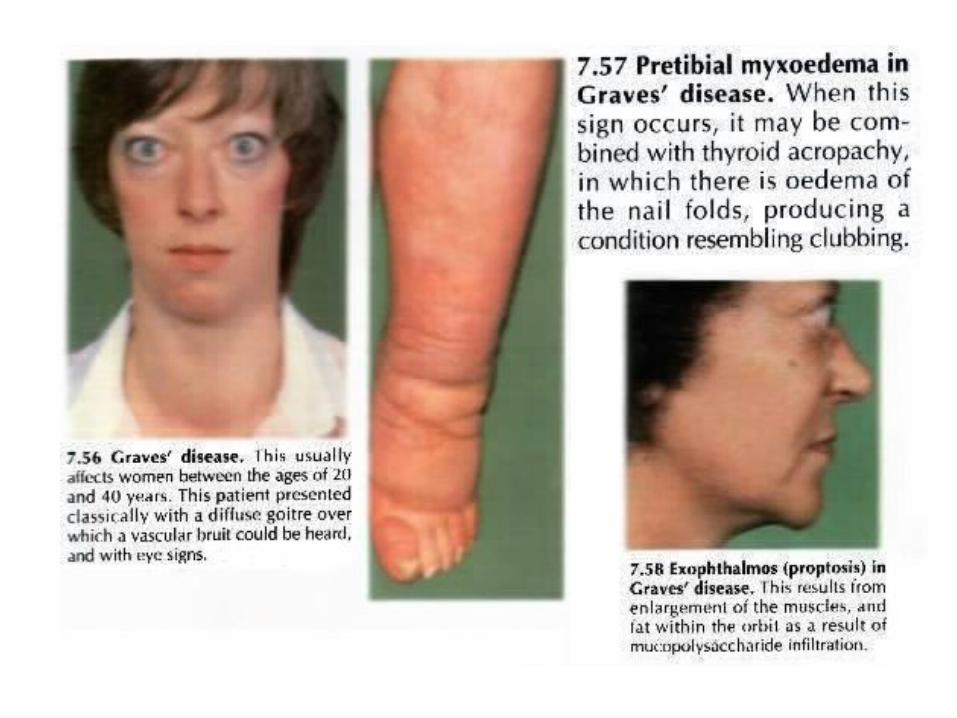
Graves disease
• The most common cause of endogenous hyperthyroidism. • Characterized by a triad of clinical findings:• • Hyperthyroidism associated with diffuse enlargement of the
gland• • Infiltrative ophthalmopathy with resultant exophthalmos• • Localized, infiltrative dermopathy, (pretibial myxedema,
which is present in a minority of patients

Graves disease
• peak incidence between 20 and 40 years of age. • Women are affected 10 times more than men. • affect 1.5% to 2% of women in USA

Pathogenesis of Graves disease
• Autoimmune disorder• Autoantibodies against multiple thyroid proteins,
most importantly the TSH receptor. • A variety of Abs that can either stimulate or block
TSH receptor• Thyroid stimulating immunoglobulin (TSI) Abs, in
90% of patients• TSI binds to the TSH receptor and mimics its actions,
stimulating adenyl cyclase and increasing the release of thyroid hormones.

Graves ophthalmopathy
• Exopthalmos, protrusion of the eyeball is associated with; increased Vo. Of retroorbital CT & extraocular M., for several
reasons;• (1) infiltration of retroorbital space by mononuclear cells; • (2) inflammation, edema and swelling of extraocular M;• (3) accumulation of ECM, glycosaminoglycans such as
hyaluronic acid and chondroitin sulfate; • (4) increased numbers of adipocytes (fatty infiltration). • These changes displace the eyeball forward and can interfere
with the function of the extraocular muscles.

The thyroid gland is symmetrically enlarged due to diffuse hypertrophy and hyperplasia of thyroid follicular epithelial cells
Graves disease

Graves disease

Graves Disease
• ■ Graves disease, the most common cause of endogenous hyperthyroidism,
• characterized by the triad of thyrotoxicosis, ophthalmopathy, and dermopathy.
• ■ It is an autoimmune disorder caused by activation of thyroid epithelial cells by autoantibodies to the TSH receptor that mimic TSH action (thyroid-stimulating immunoglobulins).
• ■ The thyroid in Graves disease is characterized by diffuse hypertrophy and hyperplasia of follicles and lymphoid infiltrates;
• glycosaminoglycan deposition and lymphoid infiltrates are responsible for the ophthalmopathy and dermopathy.
• ■ Laboratory features include elevations in serum free T3 and T4 and decreased serum TSH.


GOITER

Hyperfunctional thyroid adenoma

• The antithyroid agent propylthiouracil;
• inhibits the oxidation of iodide and thus blocks the production of thyroid hormones;
• & inhibits the peripheral deiodination of circulating T4 into T3, thus ameliorating symptoms of thyroid hormone excess

• Iodide, when given in large doses to individuals with thyroid hyperfunction, also blocks the release of thyroid hormones by inhibiting the proteolysis of thyroglobulin.
• Thus, thyroid hormone is synthesized and incorporated into colloid, but it is not released into the blood.

Hypothyroidism
• Primary and Secondary• caused by a structural or functional derangement
that interferes with the production of thyroid hormone
• common disorder• increases with age, • 10 fold more in women than men.• Myxedema (coma)
– Sluggishness– Cool skin
Causes of HypothyroidismPrimaryIodine deficiency*Autoimmune hypothyroidism Hashimoto thyroiditis*Postablative Surgery, radioiodine therapy, or external irradiationGenetic defects in thyroid development (PAX8, FOXE1, TSH receptor mutations) (rare)Thyroid hormone resistance syndrome (THRB mutations) (rare)Drugs (lithium, iodides, p-aminosalicylic acid)*Congenital biosynthetic defect (dyshormonogenetic goiter) (rare) *Secondary (Central)Pituitary failure (rare)Hypothalamic failure (rare)
Hypothyroidism
• Primary hypothyroidism • form majority of cases, • +/- (goiter).• Primary hypothyroidism can be • congenital, • autoimmune,• iatrogenic.

Congenital hypothyroidism
• Most often due to Endemic iodine deficiency in the diet.
• Rarely due to Inborn Errors of Metabolism, (dyshormonogenetic goiter), defect in synthesis of thyroid hormones.
• Complete absence of thyroid (rare)

Autoimmune hypothyroidism
• The most common cause of hypothyroidism in iodine-sufficient areas of the world.
• The majority are due to Hashimoto thyroiditis. • Circulating autoantibodies, are; • antimicrosomal, antithyroid peroxidase, and
antithyroglobulin antibodies, • Thyroid is enlarged (goitrous). • can occur in isolation or in conjunction with
autoimmune polyendocrine syndrome.

Iatrogenic hypothyroidism
• Surgery• Radiation-induced ablation. • Drugs (e.g., methimazole, & propylthiouracil) agents used to treat nonthyroid conditions
(lithium, p-aminosalicylic acid).

Secondary (central) hypothyroidism
• Deficiencies of TSH or, more uncommonly, TRH. • Any of the causes of hypopituitarism or of
hypothalamic damage from tumors, trauma, radiation therapy, or infiltrative diseases can cause central hypothyroidism.

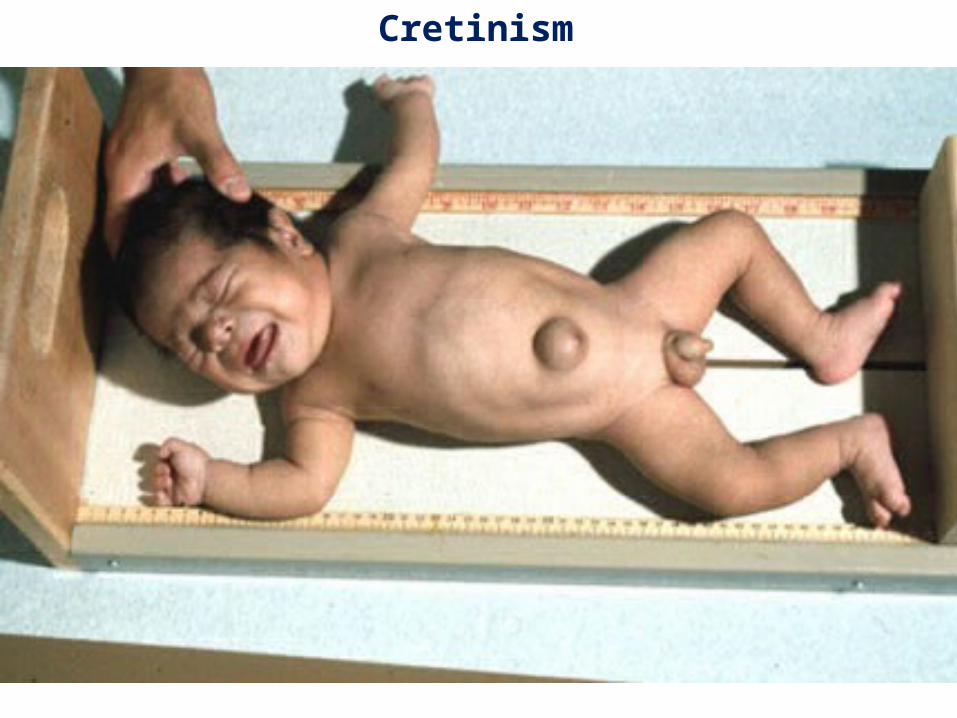
Cretinism
• Hypothyroidism in infancy or early childhood.• impaired development of the skeletal system and CNS,• severe mental retardation,• short stature,• coarse facial features, • protruding tongue• Umbilical hernia. • The severity of the mental impairment related to the time at
which thyroid deficiency occurs in utero.

Cretinism
Cretinism

Cretinism

• Myxedema is applied to hypothyroidism developing in the older child or adult.



Endocrine - Thyroid
•Embryology – Thyroglossal Duct Cyst (TGDC)

THYROGLOSSAL DUCT CYST