three easy pieces for maternal and child health policy: machs roundtable 2012
TRANSCRIPT

Three Easy Pieces for Maternal and Child Health Policy: MACHS Roundtable, Winnipeg, MB CANADA • December 11, 2012by Dennis D. Embry, PAXIS Institute
Mum & egg
Tuesday, December 11, 12

Maternal and Child Health Conference: Leadership to Action
• Name of Speaker: Dennis D. Embry, Ph.D.
• Title of Presentation: Three Easy Pieces for Maternal and Child Health Policy
• Date of Presentation: December 11, 2012
• Financial Disclosure
• Grants/Research Support: Yes, Co-Investigator, Towards Flourishing, PHAC
• Honoraria: I receive fees to speak at this conference and other Conference
• Consulting Fees: Yes, for multiple projects in Canada and the US
• Other: Training fees and royalties on multiple copyrights for publications
Disclosure of Poten/al for Conflict of Interest
Tuesday, December 11, 12

Foretelling my talk todayA new concept today of evolutionary mismatch that honors wisdom and scienceSolving linked multi-problems or syndemics instead of one-at-a-timeUsing low-cost proven strategies for all as public-health policy for Maternal and Child Health (MACH)
Tuesday, December 11, 12

My Three Easy Pieces for Today• Policy Goal 1: Reduce multiple sources of neuro-inflammation before pregnancy,
during pregnancy and during childhood—using low-cost, scientifically proven evidence-based kernels.
• Policy Goal 2: Recognize, reinforce and reward non-use of tobacco, alcohol & other drugs among women of childbearing age —using low-cost, scientifically proven evidence-based kernels.
• Policy Goal 3: Create public-private partnerships to promote specific nurturing environments actionable strategies for children and their caregivers.
Tuesday, December 11, 12

The first low-cost, proven, evidence-based kernel for maternal and child health
The Epidemiological Observation
Tuesday, December 11, 12

The first low-cost, proven, evidence-based kernel for maternal and child health
The Epidemiological Observation The Experimental Observation
ChlorineHandwash
Tuesday, December 11, 12

The first low-cost, proven, evidence-based kernel for maternal and child health
The Epidemiological Observation The Experimental Observation
ChlorineHandwash
Tuesday, December 11, 12

The first low-cost, proven, evidence-based kernel for maternal and child health
Tuesday, December 11, 12

Streptococcus pyogenesThe culprit of massive morbidity and mortality of mothers and children.
Image credit: CDC
Tuesday, December 11, 12
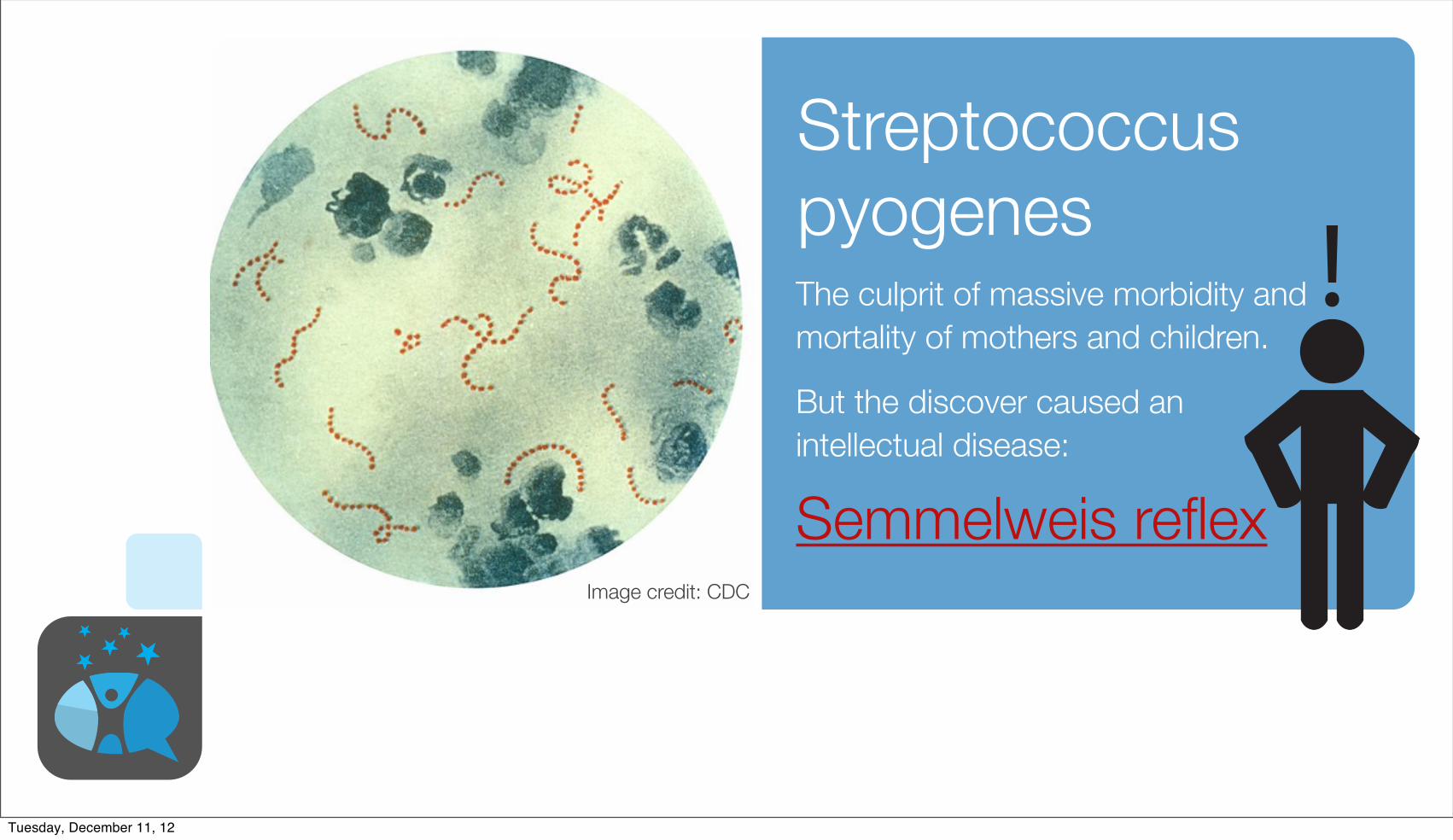
Streptococcus pyogenesThe culprit of massive morbidity and mortality of mothers and children.
Image credit: CDC
But the discover caused an intellectual disease:
Semmelweis reflex
Tuesday, December 11, 12

A policy…A course or principle of action adopted or proposed by a government, party, business, or individual.
Also, archaic, prudent or expedient conduct or action: a course of policy and wisdom.
ORIGIN late Middle English: from Old French policy ‘civil administration,’ via Latin from Greek politeia ‘citizenship,’ from politēs ‘citizen,’ from polis ‘city.’policy 2 |ˈpäləsē|noun ( pl. policies )
ORIGIN mid 16th cent.: from French police ‘bill of lading, contract of insurance,’ from Provençal poliss(i)a, probably from medieval Latin apodissa, apodixa, based on Greek apodeixis ‘evidence, proof,’ from apodeiknunai ‘demonstrate, show.’
Tuesday, December 11, 12

Let us begin with some wisdom and careful observations
Tuesday, December 11, 12

Elder wisdom about child-rearing selected by evolutionary mechanisms
Humans are everyday scientists of their
successes
Tuesday, December 11, 12

www.thisviewoflife.com “Look up Evolutionary Mismatch”Natural selection adapts organisms to their past environments and has no ability to foresee the future.
When the environment changes, adaptations to past environments can misfire in the current situation, producing a mismatch that can only be solved by evolving or by modifying the current environment.
Mismatches are an inevitable consequence of evolution in changing environments.
Tuesday, December 11, 12

This creates an evolutionary mismatch in the womb
Tuesday, December 11, 12

Early incubator experiences for premies
Tuesday, December 11, 12

Early incubator experiences for premies What did we learn?
Tuesday, December 11, 12
What did this nurse notice about this premie?
Tuesday, December 11, 12

What are we noticing with babies and mums more today?
Tuesday, December 11, 12

Some observable trends:• Increased postpartum depression
• More addictions
• More “inflammatory” diseases like asthma, diabetes and obesity
• More children with disabilities such as autism spectrum disorder
• Higher lifetime rates of mental, emotional, behavioral, and related physical disorders
Tuesday, December 11, 12
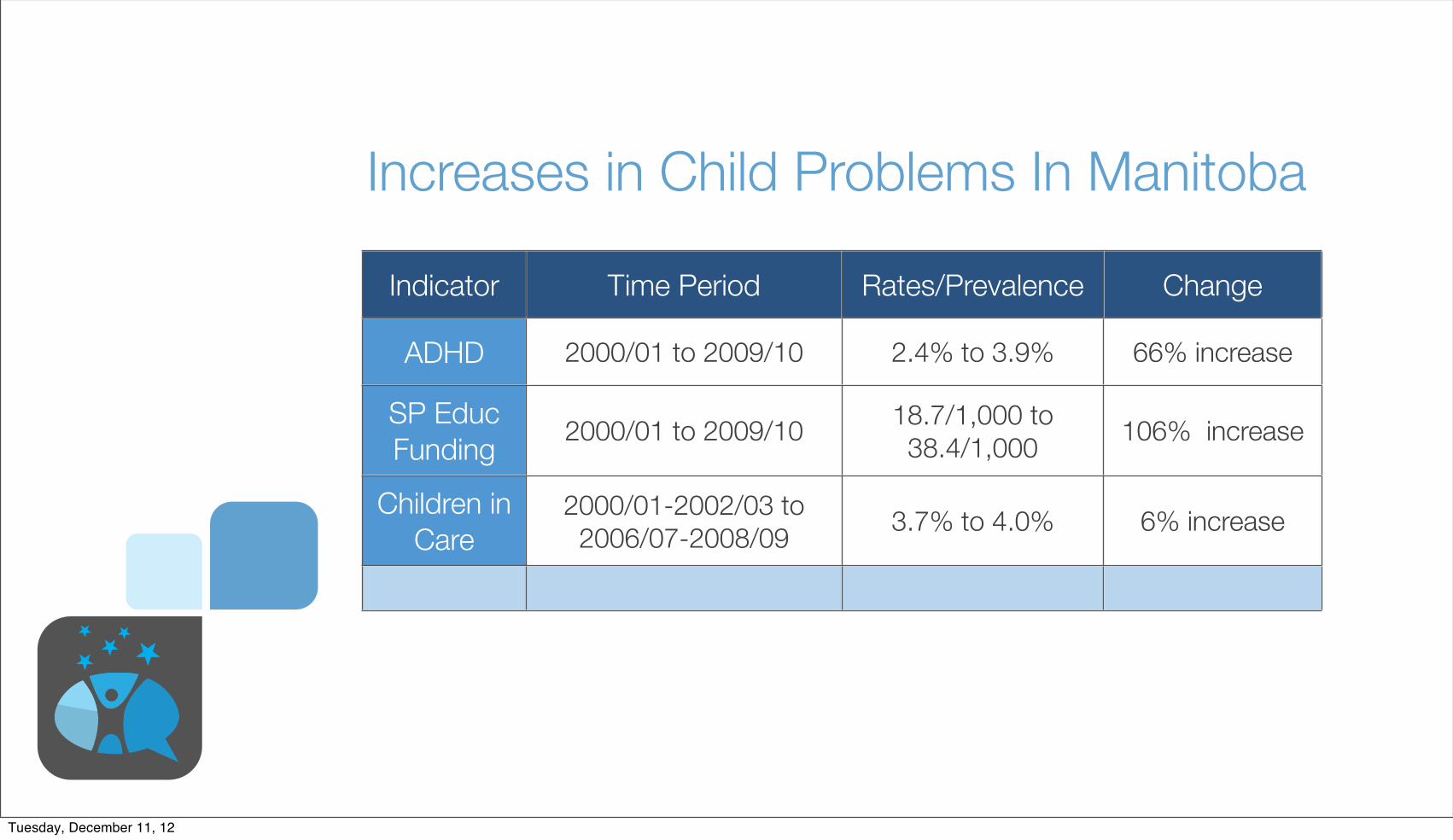
Increases in Child Problems In Manitoba
Indicator Time Period Rates/Prevalence Change
ADHD
SP EducFunding
Children in Care
2000/01 to 2009/10 2.4% to 3.9% 66% increase
2000/01 to 2009/10 18.7/1,000 to 38.4/1,000 106% increase
2000/01-2002/03 to 2006/07-2008/09 3.7% to 4.0% 6% increase
Tuesday, December 11, 12

2006 Statistics Canada report on the Participation and Activity Limitation Survey (PALS)
• According to Statistics Canada, more children in this country have a learning disability than all other types of disabilities combined.
• According to Statistics Canada, of all the children with disabilities in this country, more than half (59.8%) have a learning disability.
• According to Statistics Canada, more than half a million adults in this country live with a learning disability, making it more challenging for them to learn in universities and colleges, and on the job.
• According to Statistics Canada, learning disabilities increased considerably between 2001 and 2006 among Canadians aged 15 and over by almost 40 per cent to 631,000 people, making it one of the fastest growing types of disabilities in Canada that isn’t related to aging.
Tuesday, December 11, 12

With various early childhood disabilities increasing, how does that parents and families?
Tuesday, December 11, 12

With various early childhood disabilities increasing, how does that parents and families?
Impact of child's condition on parental employment for parents of children with disabilities aged 0 to 14, Canada, 2006
Tuesday, December 11, 12

Physiologicalinfluences triggeradverse biological
mechanisms
Reinforcementmore for anti-social
than prosocialbehaviors
Antecedentscue anti-social
acts and threats
Verbal Relationsoccasion perceivedthreats and related
reactions
Major Connected Causes of the Adverse Trends Predicting MEBs & Related Illnesses
Multi-Inflammatory Brain & Body Response
The Same Mismatches Predict Multiple MACH DisordersTuesday, December 11, 12
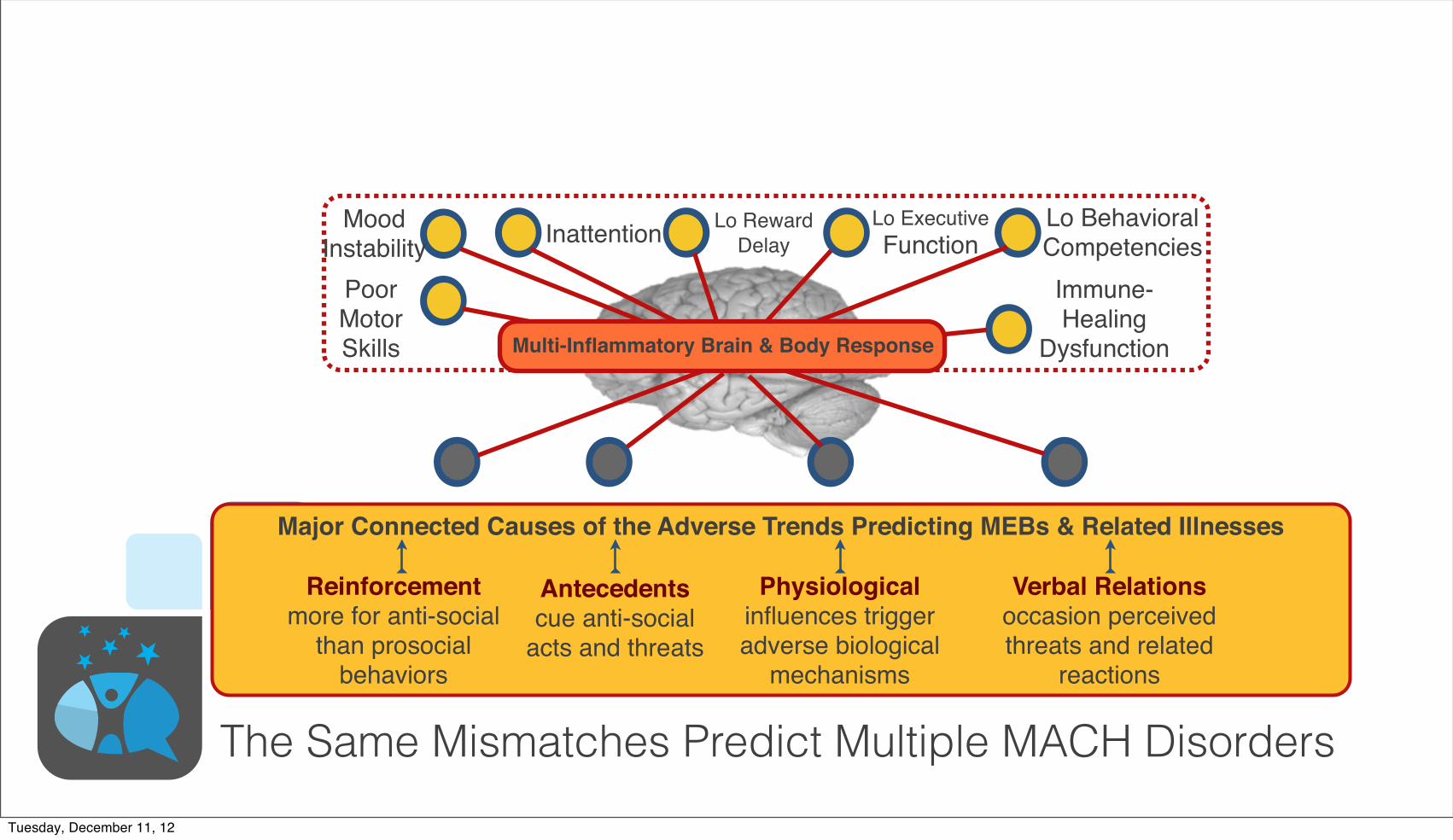
MoodInstability Inattention Lo Reward
DelayLo ExecutiveFunction
Lo BehavioralCompetencies
PoorMotorSkills
Immune-Healing
Dysfunction
Physiologicalinfluences triggeradverse biological
mechanisms
Reinforcementmore for anti-social
than prosocialbehaviors
Antecedentscue anti-social
acts and threats
Verbal Relationsoccasion perceivedthreats and related
reactions
Major Connected Causes of the Adverse Trends Predicting MEBs & Related Illnesses
Multi-Inflammatory Brain & Body Response
The Same Mismatches Predict Multiple MACH DisordersTuesday, December 11, 12

MoodInstability Inattention Lo Reward
DelayLo ExecutiveFunction
Lo BehavioralCompetencies
PoorMotorSkills
Immune-Healing
Dysfunction
Physiologicalinfluences triggeradverse biological
mechanisms
Reinforcementmore for anti-social
than prosocialbehaviors
Antecedentscue anti-social
acts and threats
Verbal Relationsoccasion perceivedthreats and related
reactions
Major Connected Causes of the Adverse Trends Predicting MEBs & Related Illnesses
Mental Illness SubstanceAbuse Violence Work
ProblemsObesity,
etc CancerEarlySex
School Failure
STD’s SpecialEdMulti-Inflammatory Brain & Body Response
The Same Mismatches Predict Multiple MACH DisordersTuesday, December 11, 12

Physiologicalinfluences trigger
protective biologicalmechanisms
Reinforcementmore for prosocial
behaviors
Antecedentscue prosocial
behaviors
Verbal Relationsoccasion perceived
safety andaffiliation
Multiple Behavioral Vaccines Protect the Futures of ALL Children, Youth and Adults
Multi Anti-Inflammatory Brain & Body Response
Changing Conditions Protect and Prevent MACHTuesday, December 11, 12

MoodStability
AttentionHi Reward
DelayHi Executive
FunctionHi BehavioralCompetencies
GoodMotorSkills
Immune-Healing
Efficiency
Physiologicalinfluences trigger
protective biologicalmechanisms
Reinforcementmore for prosocial
behaviors
Antecedentscue prosocial
behaviors
Verbal Relationsoccasion perceived
safety andaffiliation
Multiple Behavioral Vaccines Protect the Futures of ALL Children, Youth and Adults
Multi Anti-Inflammatory Brain & Body Response
Changing Conditions Protect and Prevent MACHTuesday, December 11, 12

MoodStability
AttentionHi Reward
DelayHi Executive
FunctionHi BehavioralCompetencies
GoodMotorSkills
Immune-Healing
Efficiency
Physiologicalinfluences trigger
protective biologicalmechanisms
Reinforcementmore for prosocial
behaviors
Antecedentscue prosocial
behaviors
Verbal Relationsoccasion perceived
safety andaffiliation
Multiple Behavioral Vaccines Protect the Futures of ALL Children, Youth and Adults
Mental health LowAddictions Prosociality Work
SuccessHeart Health
etc
LowCancerDelayed
SexHi Sch.Grad
LowInjuries
HigherEdMulti Anti-Inflammatory Brain & Body Response
Changing Conditions Protect and Prevent MACHTuesday, December 11, 12

Solving some current mismatches affecting MACH
Tuesday, December 11, 12

Richly Reinforce Pro-social Behaviors Reduce Toxic In!uences
Limit Problematic Behaviors Increase Psychological FlexibilityBiglan, A., B. R. Flay, et al. (2012). "The critical role of nurturing environments for promoting human well-being." American Psychologist.
Tuesday, December 11, 12

Mothers and children in Canada do not eat foods sufficient in Vitamin D
Mothers and children in Canada do not get sufficient Vitamin D via sunlight
This evolutionary mismatch harms MACH
Tuesday, December 11, 12

Mismatch, Latitude & Schizophrenia
both latitude and low temperature are highly significant(P< .001 in each case), the correlationwith infantmortalityis not significant at the .05 level. Moreover, the direction(sign) of the respective correlations of prevalence withlatitude and cold are consistent across all continents
and subgroups. In contrast, the direction of the correla-tion of prevalence with infant mortality is inconsistentacross different continents.The best-fit regression lines in figure 1 also suggest that
the increase in prevalence with increasing latitude occurs
Fig. 1. Schizophrenia Prevalence and Latitude by Continent and Infant Mortality.Note: SouthAsia siteswere from Indiaand Indonesia; those sites hadhigher infantmortality rates than all but one of theEastAsian sites. For theregressionlinesinNorthAmerica,thosewithinfantmortalityratesabove30per1000weregroupedashavingahigherrate, thosebelow30ashavinga lower rate.Theslopesof linear regression lineswere0.15 for theEastAsiansites, 0.22 for theAfricansites, 0.086 for theSouthAsiansites,0.14 fortheNorthAmericansiteswithlowerinfantmortality,0.51fortheNorthAmericansiteswithhigherinfantmortality,and0.48fortheEuropeansites.
Table 3. Correlations of Schizophrenia Prevalence with Predictor Variables
Geographic Group ofSamples N Absolute Latitudea Temperatureb Infant Mortalityc Fish Intaked
All study samples 49 .46** !.60*** !.26! !.10
Europe 18 .58* !.81*** !.22 !.21
North AmericaAll samples 10 .75* !.74* .92*** !.64!
High infant mortality 3 .94 !.99* .97 n/aLow infant mortality 7 .68! !.62 .58 !.85*
AsiaAll samples 15 .58* !.56* .05 !.05South Asia 9 .51! !.51! .49 !.49East Asia 6 .78* !.69 .46 !.20
Africa 4 .53 !.67 .25 !.81
Othere 2 n/a n/a n/a n/a
n/a = data available on only 2 samples.aAbsolute latitude in degrees north or south of the equator.bMean low temperature for the coldest month of the year in degrees Fahrenheit.cInfant mortality rate is the number of cases per 1000 adult population.dFish intake (in kg/person/year); n = 48 because data were not available for Oxford Bay.68eIncludes Christchurch, New Zealand, and Buenos Aires, Argentina.!0.05 < P " .10; *P < 0.05; **P < 0.001; ***P < 0.0005; all P values are two tailed, for Pearson product-moment correlations.
588
D. K. Kinney et al.
Relation of Schizophrenia Prevalence to Latitude, Climate, Fish Consumption, InfantMortality, and Skin Color: A Role for Prenatal Vitamin DDeficiency and Infections?
Dennis K. Kinney1–3, Pamela Teixeira2, Diane Hsu2, SienaC. Napoleon2,4, David J. Crowley2, Andrea Miller2,William Hyman2, and Emerald Huang2
2Genetics Laboratory, McLean Hospital, Belmont, MA; 3De-partment of Psychiatry, Harvard Medical School, Boston, MA;4Wellesley College, Wellesley, MA
Previous surveys found a large (>10-fold) variation inschizophrenia prevalence at different geographic sitesand a tendency for prevalence to increase with latitude.We conducted meta-analyses of prevalence studies to inves-tigate whether these findings pointed to underlying etiologicfactors in schizophrenia or were the result of methodolog-ical artifacts or the confounding of sites’ latitude with levelof healthcare at those sites. We found that these patternswere still present after controlling for an index of health-care—infant mortality—and focusing on 49 studies thatused similar diagnostic and ascertainment methods. Thetendencies for schizophrenia prevalence to increase withboth latitude and colder climate were still large and signif-icant and present on several continents. The increase inprevalence with latitude was greater for groups with lowfish consumption, darker skin, and higher infant mortali-ty—consistent with a role of prenatal vitamin D deficiencyin schizophrenia. Previous research indicates that poor pre-natal healthcare and nutrition increase risk for schizophre-nia within the same region. These adverse conditions aremore prevalent in developing countries concentrated nearthe equator, but schizophrenia prevalence is lowest atsites near the equator. This suggests that schizophrenia-producing environmental factors associated with higher lat-itude may be so powerful they overwhelm protective effectsof better healthcare in industrialized countries. The ob-served patterns of correlations of risk factors with preva-lence are consistent with an etiologic role for prenatalvitamin D deficiency and exposure to certain infectious dis-eases. Research to elucidate environmental factors that un-
derlie variations in schizophrenia prevalence deserves highpriority.
Key words: epidemiology/etiology/immune function/prenatal/geography/risk factor
Introduction
Schizophrenia is an unusually burdensome disorder be-cause of the great economic costs of extensive care andloss of economic productivity, as well as the personal suf-fering and stigma, which often affect a patient and his orher family for most of the patient’s life. Moreover, formost patients there is still no cure or even an effectiveway of treating many of the most disabling, ‘‘negative’’symptoms of the disorder. Therefore, a key goal of schizo-phrenia research is elucidation of etiologic factors, partic-ularly environmental ones that could be readily avoidedand used in effective, inexpensive, and ethically sound pri-mary prevention programs.In a comprehensive survey of schizophrenia prevalence
studies around the world that were published in Englishover a period of 4 decades, Torrey1 noted 2 importantpatterns. First, prevalence rates varied widely at differentgeographic sites, with the highest rate being more than 10times greater than the lowest. Second, there was a strongtendency for schizophrenia prevalence to increase withincreasing latitude; ie, prevalence rates tended to bevery low near the equator and to increase as one movedtoward the poles. Both of Torrey’s conclusions were alsoreached in a survey and meta-analysis by Saha et al,2
which included more recent studies as well as ones pub-lished in languages other than English. Several other sur-veys have also concluded that schizophrenia rates vary atleast 10-fold around the world, including studies usingmeasures of point prevalence, lifetime prevalence, andincidence.1,3–10
A number of explanations have been proposed for thisvariability inprevalence.Severalcomplementary linesofre-search suggest that the tendency for schizophrenia preva-lence to increase with latitude and cold climate may bedue, at least inpart, to someunderlyingpre-orperinatal en-vironmental influences. For example, several studies have
1To whom correspondence should be addressed; Genetics Lab-oratory, McLean Hospital, NB-G-28 115 Mill Street, Belmont,MA 02478; tel: 617-855-3439, fax: 617-855-2348, e-mail:[email protected].
Schizophrenia Bulletin vol. 35 no. 3 pp. 582–595, 2009doi:10.1093/schbul/sbp023Advance Access publication on April 8, 2009
! The Author 2009. Published by Oxford University Press on behalf of the Maryland Psychiatric Research Center. All rights reserved.For permissions, please email: [email protected].
582
Tuesday, December 11, 12

Mismatch, Latitude & Schizophrenia
both latitude and low temperature are highly significant(P< .001 in each case), the correlationwith infantmortalityis not significant at the .05 level. Moreover, the direction(sign) of the respective correlations of prevalence withlatitude and cold are consistent across all continents
and subgroups. In contrast, the direction of the correla-tion of prevalence with infant mortality is inconsistentacross different continents.The best-fit regression lines in figure 1 also suggest that
the increase in prevalence with increasing latitude occurs
Fig. 1. Schizophrenia Prevalence and Latitude by Continent and Infant Mortality.Note: SouthAsia siteswere from Indiaand Indonesia; those sites hadhigher infantmortality rates than all but one of theEastAsian sites. For theregressionlinesinNorthAmerica,thosewithinfantmortalityratesabove30per1000weregroupedashavingahigherrate, thosebelow30ashavinga lower rate.Theslopesof linear regression lineswere0.15 for theEastAsiansites, 0.22 for theAfricansites, 0.086 for theSouthAsiansites,0.14 fortheNorthAmericansiteswithlowerinfantmortality,0.51fortheNorthAmericansiteswithhigherinfantmortality,and0.48fortheEuropeansites.
Table 3. Correlations of Schizophrenia Prevalence with Predictor Variables
Geographic Group ofSamples N Absolute Latitudea Temperatureb Infant Mortalityc Fish Intaked
All study samples 49 .46** !.60*** !.26! !.10
Europe 18 .58* !.81*** !.22 !.21
North AmericaAll samples 10 .75* !.74* .92*** !.64!
High infant mortality 3 .94 !.99* .97 n/aLow infant mortality 7 .68! !.62 .58 !.85*
AsiaAll samples 15 .58* !.56* .05 !.05South Asia 9 .51! !.51! .49 !.49East Asia 6 .78* !.69 .46 !.20
Africa 4 .53 !.67 .25 !.81
Othere 2 n/a n/a n/a n/a
n/a = data available on only 2 samples.aAbsolute latitude in degrees north or south of the equator.bMean low temperature for the coldest month of the year in degrees Fahrenheit.cInfant mortality rate is the number of cases per 1000 adult population.dFish intake (in kg/person/year); n = 48 because data were not available for Oxford Bay.68eIncludes Christchurch, New Zealand, and Buenos Aires, Argentina.!0.05 < P " .10; *P < 0.05; **P < 0.001; ***P < 0.0005; all P values are two tailed, for Pearson product-moment correlations.
588
D. K. Kinney et al.
Semmelweis Reflex
Relation of Schizophrenia Prevalence to Latitude, Climate, Fish Consumption, InfantMortality, and Skin Color: A Role for Prenatal Vitamin DDeficiency and Infections?
Dennis K. Kinney1–3, Pamela Teixeira2, Diane Hsu2, SienaC. Napoleon2,4, David J. Crowley2, Andrea Miller2,William Hyman2, and Emerald Huang2
2Genetics Laboratory, McLean Hospital, Belmont, MA; 3De-partment of Psychiatry, Harvard Medical School, Boston, MA;4Wellesley College, Wellesley, MA
Previous surveys found a large (>10-fold) variation inschizophrenia prevalence at different geographic sitesand a tendency for prevalence to increase with latitude.We conducted meta-analyses of prevalence studies to inves-tigate whether these findings pointed to underlying etiologicfactors in schizophrenia or were the result of methodolog-ical artifacts or the confounding of sites’ latitude with levelof healthcare at those sites. We found that these patternswere still present after controlling for an index of health-care—infant mortality—and focusing on 49 studies thatused similar diagnostic and ascertainment methods. Thetendencies for schizophrenia prevalence to increase withboth latitude and colder climate were still large and signif-icant and present on several continents. The increase inprevalence with latitude was greater for groups with lowfish consumption, darker skin, and higher infant mortali-ty—consistent with a role of prenatal vitamin D deficiencyin schizophrenia. Previous research indicates that poor pre-natal healthcare and nutrition increase risk for schizophre-nia within the same region. These adverse conditions aremore prevalent in developing countries concentrated nearthe equator, but schizophrenia prevalence is lowest atsites near the equator. This suggests that schizophrenia-producing environmental factors associated with higher lat-itude may be so powerful they overwhelm protective effectsof better healthcare in industrialized countries. The ob-served patterns of correlations of risk factors with preva-lence are consistent with an etiologic role for prenatalvitamin D deficiency and exposure to certain infectious dis-eases. Research to elucidate environmental factors that un-
derlie variations in schizophrenia prevalence deserves highpriority.
Key words: epidemiology/etiology/immune function/prenatal/geography/risk factor
Introduction
Schizophrenia is an unusually burdensome disorder be-cause of the great economic costs of extensive care andloss of economic productivity, as well as the personal suf-fering and stigma, which often affect a patient and his orher family for most of the patient’s life. Moreover, formost patients there is still no cure or even an effectiveway of treating many of the most disabling, ‘‘negative’’symptoms of the disorder. Therefore, a key goal of schizo-phrenia research is elucidation of etiologic factors, partic-ularly environmental ones that could be readily avoidedand used in effective, inexpensive, and ethically sound pri-mary prevention programs.In a comprehensive survey of schizophrenia prevalence
studies around the world that were published in Englishover a period of 4 decades, Torrey1 noted 2 importantpatterns. First, prevalence rates varied widely at differentgeographic sites, with the highest rate being more than 10times greater than the lowest. Second, there was a strongtendency for schizophrenia prevalence to increase withincreasing latitude; ie, prevalence rates tended to bevery low near the equator and to increase as one movedtoward the poles. Both of Torrey’s conclusions were alsoreached in a survey and meta-analysis by Saha et al,2
which included more recent studies as well as ones pub-lished in languages other than English. Several other sur-veys have also concluded that schizophrenia rates vary atleast 10-fold around the world, including studies usingmeasures of point prevalence, lifetime prevalence, andincidence.1,3–10
A number of explanations have been proposed for thisvariability inprevalence.Severalcomplementary linesofre-search suggest that the tendency for schizophrenia preva-lence to increase with latitude and cold climate may bedue, at least inpart, to someunderlyingpre-orperinatal en-vironmental influences. For example, several studies have
1To whom correspondence should be addressed; Genetics Lab-oratory, McLean Hospital, NB-G-28 115 Mill Street, Belmont,MA 02478; tel: 617-855-3439, fax: 617-855-2348, e-mail:[email protected].
Schizophrenia Bulletin vol. 35 no. 3 pp. 582–595, 2009doi:10.1093/schbul/sbp023Advance Access publication on April 8, 2009
! The Author 2009. Published by Oxford University Press on behalf of the Maryland Psychiatric Research Center. All rights reserved.For permissions, please email: [email protected].
582
Tuesday, December 11, 12
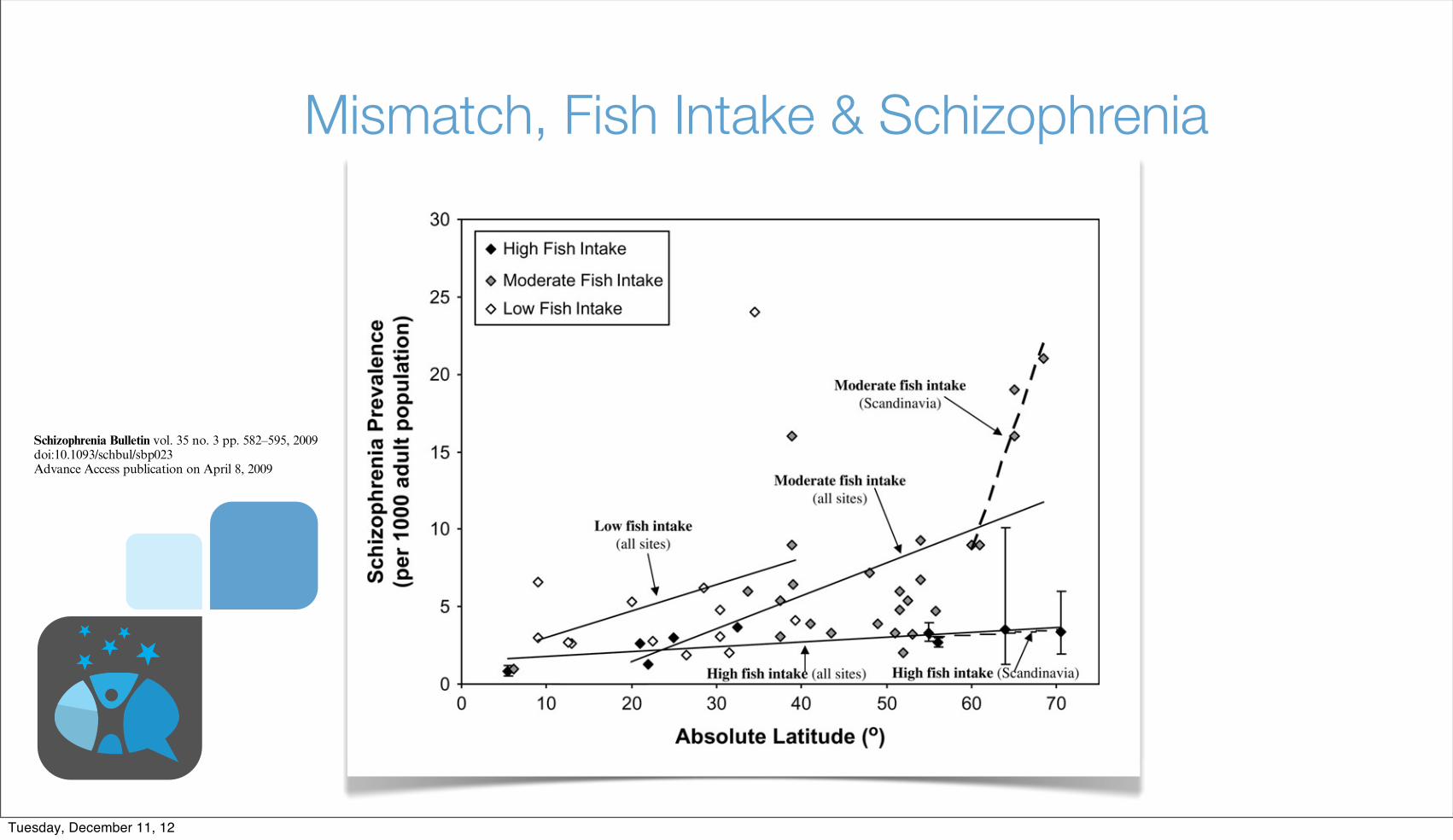
Mismatch, Fish Intake & Schizophrenia
different sites around the world1,2 were not simply arti-facts of differences in diagnostic and ascertainment meth-ods used by different studies. Even though our analysesrestricted prevalence studies to those that used more sim-ilar research methods for diagnosis and ascertainment ofschizophrenia cases, our analyses also found (a) thatprevalence rates varied more than 10-fold across geo-graphic sites and (b) that prevalence increased markedlywith increasing latitude.
That the correlation of schizophrenia prevalence withlatitude is both robust and large, and is not due simply tobetween-site differences in diagnostic and ascertainmentmethods, is further suggested by analysis of data collectedby Lehtinen et al.42 Their study is particularly informa-tive because it is the study that best controlled for possi-ble methodological sources of differences in prevalence atdifferent geographic sites; the same investigative person-nel, as well as the same methods, were used to obtainprevalence rates at several different sites within thesame country. Those investigators studied schizophreniaprevalence at 5 different Finnish sites in the same timeperiod, using a consistent set of diagnostic criteria andascertainment methods, and their data showed a veryhigh correlation of prevalence with both latitude(r = .97, P < .01) and mean low temperature (r =!.99, P < .001).
Athigher latitudes, there isanespeciallywidevariation inprevalence rates. By contrast, near the equator, prevalencefor all sites tends to be quite low. That is, for all groups andcontinental regions for which there are data frommultiplesites, thebest-fit (least squares) regression lines all havepos-
itiveslopes,andtheslopes tendtobesteeper forsitesathigh-er latitudes.This is evident by inspecting table 1, but ismostreadily visualized in figure 1.The results suggest that etiologic factors closely asso-
ciated with latitude and cold climate may be much morepowerful contributors to risk for schizophrenia than isgenerally recognized. The general level of a population’seconomic status and healthcare, as indexed in our anal-ysis by the infant mortality rate, appears to be a muchweaker predictor of risk for schizophrenia than are lati-tude and winter temperature. A high infant mortality rate
Fig. 2. Schizophrenia Prevalence and Latitude by Fish Intake.Note:Errorbars represent95%confidence limits.Theslopesof linear regression lineswere0.03 for siteswithhighfish intake, 0.21 for siteswithmoderate fish intake, and 0.17 for siteswith low fish intake. For the subset of Scandinavian sites, the slope of linear regression forwas 0.03 forsites with high fish intake and 1.57 for sites with moderate fish intake.
Fig. 3. Schizophrenia Prevalence and Latitude by Skin Color.Note: Error bars represent 95% confidence limits. The slopes of thelinear regression lines were 0.24 for those with lightest skin, 0.43 forthosewithintermediateskincolor,and0.31forthosewithdarkestskin.
590
D. K. Kinney et al.
Relation of Schizophrenia Prevalence to Latitude, Climate, Fish Consumption, InfantMortality, and Skin Color: A Role for Prenatal Vitamin DDeficiency and Infections?
Dennis K. Kinney1–3, Pamela Teixeira2, Diane Hsu2, SienaC. Napoleon2,4, David J. Crowley2, Andrea Miller2,William Hyman2, and Emerald Huang2
2Genetics Laboratory, McLean Hospital, Belmont, MA; 3De-partment of Psychiatry, Harvard Medical School, Boston, MA;4Wellesley College, Wellesley, MA
Previous surveys found a large (>10-fold) variation inschizophrenia prevalence at different geographic sitesand a tendency for prevalence to increase with latitude.We conducted meta-analyses of prevalence studies to inves-tigate whether these findings pointed to underlying etiologicfactors in schizophrenia or were the result of methodolog-ical artifacts or the confounding of sites’ latitude with levelof healthcare at those sites. We found that these patternswere still present after controlling for an index of health-care—infant mortality—and focusing on 49 studies thatused similar diagnostic and ascertainment methods. Thetendencies for schizophrenia prevalence to increase withboth latitude and colder climate were still large and signif-icant and present on several continents. The increase inprevalence with latitude was greater for groups with lowfish consumption, darker skin, and higher infant mortali-ty—consistent with a role of prenatal vitamin D deficiencyin schizophrenia. Previous research indicates that poor pre-natal healthcare and nutrition increase risk for schizophre-nia within the same region. These adverse conditions aremore prevalent in developing countries concentrated nearthe equator, but schizophrenia prevalence is lowest atsites near the equator. This suggests that schizophrenia-producing environmental factors associated with higher lat-itude may be so powerful they overwhelm protective effectsof better healthcare in industrialized countries. The ob-served patterns of correlations of risk factors with preva-lence are consistent with an etiologic role for prenatalvitamin D deficiency and exposure to certain infectious dis-eases. Research to elucidate environmental factors that un-
derlie variations in schizophrenia prevalence deserves highpriority.
Key words: epidemiology/etiology/immune function/prenatal/geography/risk factor
Introduction
Schizophrenia is an unusually burdensome disorder be-cause of the great economic costs of extensive care andloss of economic productivity, as well as the personal suf-fering and stigma, which often affect a patient and his orher family for most of the patient’s life. Moreover, formost patients there is still no cure or even an effectiveway of treating many of the most disabling, ‘‘negative’’symptoms of the disorder. Therefore, a key goal of schizo-phrenia research is elucidation of etiologic factors, partic-ularly environmental ones that could be readily avoidedand used in effective, inexpensive, and ethically sound pri-mary prevention programs.In a comprehensive survey of schizophrenia prevalence
studies around the world that were published in Englishover a period of 4 decades, Torrey1 noted 2 importantpatterns. First, prevalence rates varied widely at differentgeographic sites, with the highest rate being more than 10times greater than the lowest. Second, there was a strongtendency for schizophrenia prevalence to increase withincreasing latitude; ie, prevalence rates tended to bevery low near the equator and to increase as one movedtoward the poles. Both of Torrey’s conclusions were alsoreached in a survey and meta-analysis by Saha et al,2
which included more recent studies as well as ones pub-lished in languages other than English. Several other sur-veys have also concluded that schizophrenia rates vary atleast 10-fold around the world, including studies usingmeasures of point prevalence, lifetime prevalence, andincidence.1,3–10
A number of explanations have been proposed for thisvariability inprevalence.Severalcomplementary linesofre-search suggest that the tendency for schizophrenia preva-lence to increase with latitude and cold climate may bedue, at least inpart, to someunderlyingpre-orperinatal en-vironmental influences. For example, several studies have
1To whom correspondence should be addressed; Genetics Lab-oratory, McLean Hospital, NB-G-28 115 Mill Street, Belmont,MA 02478; tel: 617-855-3439, fax: 617-855-2348, e-mail:[email protected].
Schizophrenia Bulletin vol. 35 no. 3 pp. 582–595, 2009doi:10.1093/schbul/sbp023Advance Access publication on April 8, 2009
! The Author 2009. Published by Oxford University Press on behalf of the Maryland Psychiatric Research Center. All rights reserved.For permissions, please email: [email protected].
582
Tuesday, December 11, 12

Mismatch, Fish Intake & SchizophreniaSemmelweis
Reflex
different sites around the world1,2 were not simply arti-facts of differences in diagnostic and ascertainment meth-ods used by different studies. Even though our analysesrestricted prevalence studies to those that used more sim-ilar research methods for diagnosis and ascertainment ofschizophrenia cases, our analyses also found (a) thatprevalence rates varied more than 10-fold across geo-graphic sites and (b) that prevalence increased markedlywith increasing latitude.
That the correlation of schizophrenia prevalence withlatitude is both robust and large, and is not due simply tobetween-site differences in diagnostic and ascertainmentmethods, is further suggested by analysis of data collectedby Lehtinen et al.42 Their study is particularly informa-tive because it is the study that best controlled for possi-ble methodological sources of differences in prevalence atdifferent geographic sites; the same investigative person-nel, as well as the same methods, were used to obtainprevalence rates at several different sites within thesame country. Those investigators studied schizophreniaprevalence at 5 different Finnish sites in the same timeperiod, using a consistent set of diagnostic criteria andascertainment methods, and their data showed a veryhigh correlation of prevalence with both latitude(r = .97, P < .01) and mean low temperature (r =!.99, P < .001).
Athigher latitudes, there isanespeciallywidevariation inprevalence rates. By contrast, near the equator, prevalencefor all sites tends to be quite low. That is, for all groups andcontinental regions for which there are data frommultiplesites, thebest-fit (least squares) regression lines all havepos-
itiveslopes,andtheslopes tendtobesteeper forsitesathigh-er latitudes.This is evident by inspecting table 1, but ismostreadily visualized in figure 1.The results suggest that etiologic factors closely asso-
ciated with latitude and cold climate may be much morepowerful contributors to risk for schizophrenia than isgenerally recognized. The general level of a population’seconomic status and healthcare, as indexed in our anal-ysis by the infant mortality rate, appears to be a muchweaker predictor of risk for schizophrenia than are lati-tude and winter temperature. A high infant mortality rate
Fig. 2. Schizophrenia Prevalence and Latitude by Fish Intake.Note:Errorbars represent95%confidence limits.Theslopesof linear regression lineswere0.03 for siteswithhighfish intake, 0.21 for siteswithmoderate fish intake, and 0.17 for siteswith low fish intake. For the subset of Scandinavian sites, the slope of linear regression forwas 0.03 forsites with high fish intake and 1.57 for sites with moderate fish intake.
Fig. 3. Schizophrenia Prevalence and Latitude by Skin Color.Note: Error bars represent 95% confidence limits. The slopes of thelinear regression lines were 0.24 for those with lightest skin, 0.43 forthosewithintermediateskincolor,and0.31forthosewithdarkestskin.
590
D. K. Kinney et al.
Relation of Schizophrenia Prevalence to Latitude, Climate, Fish Consumption, InfantMortality, and Skin Color: A Role for Prenatal Vitamin DDeficiency and Infections?
Dennis K. Kinney1–3, Pamela Teixeira2, Diane Hsu2, SienaC. Napoleon2,4, David J. Crowley2, Andrea Miller2,William Hyman2, and Emerald Huang2
2Genetics Laboratory, McLean Hospital, Belmont, MA; 3De-partment of Psychiatry, Harvard Medical School, Boston, MA;4Wellesley College, Wellesley, MA
Previous surveys found a large (>10-fold) variation inschizophrenia prevalence at different geographic sitesand a tendency for prevalence to increase with latitude.We conducted meta-analyses of prevalence studies to inves-tigate whether these findings pointed to underlying etiologicfactors in schizophrenia or were the result of methodolog-ical artifacts or the confounding of sites’ latitude with levelof healthcare at those sites. We found that these patternswere still present after controlling for an index of health-care—infant mortality—and focusing on 49 studies thatused similar diagnostic and ascertainment methods. Thetendencies for schizophrenia prevalence to increase withboth latitude and colder climate were still large and signif-icant and present on several continents. The increase inprevalence with latitude was greater for groups with lowfish consumption, darker skin, and higher infant mortali-ty—consistent with a role of prenatal vitamin D deficiencyin schizophrenia. Previous research indicates that poor pre-natal healthcare and nutrition increase risk for schizophre-nia within the same region. These adverse conditions aremore prevalent in developing countries concentrated nearthe equator, but schizophrenia prevalence is lowest atsites near the equator. This suggests that schizophrenia-producing environmental factors associated with higher lat-itude may be so powerful they overwhelm protective effectsof better healthcare in industrialized countries. The ob-served patterns of correlations of risk factors with preva-lence are consistent with an etiologic role for prenatalvitamin D deficiency and exposure to certain infectious dis-eases. Research to elucidate environmental factors that un-
derlie variations in schizophrenia prevalence deserves highpriority.
Key words: epidemiology/etiology/immune function/prenatal/geography/risk factor
Introduction
Schizophrenia is an unusually burdensome disorder be-cause of the great economic costs of extensive care andloss of economic productivity, as well as the personal suf-fering and stigma, which often affect a patient and his orher family for most of the patient’s life. Moreover, formost patients there is still no cure or even an effectiveway of treating many of the most disabling, ‘‘negative’’symptoms of the disorder. Therefore, a key goal of schizo-phrenia research is elucidation of etiologic factors, partic-ularly environmental ones that could be readily avoidedand used in effective, inexpensive, and ethically sound pri-mary prevention programs.In a comprehensive survey of schizophrenia prevalence
studies around the world that were published in Englishover a period of 4 decades, Torrey1 noted 2 importantpatterns. First, prevalence rates varied widely at differentgeographic sites, with the highest rate being more than 10times greater than the lowest. Second, there was a strongtendency for schizophrenia prevalence to increase withincreasing latitude; ie, prevalence rates tended to bevery low near the equator and to increase as one movedtoward the poles. Both of Torrey’s conclusions were alsoreached in a survey and meta-analysis by Saha et al,2
which included more recent studies as well as ones pub-lished in languages other than English. Several other sur-veys have also concluded that schizophrenia rates vary atleast 10-fold around the world, including studies usingmeasures of point prevalence, lifetime prevalence, andincidence.1,3–10
A number of explanations have been proposed for thisvariability inprevalence.Severalcomplementary linesofre-search suggest that the tendency for schizophrenia preva-lence to increase with latitude and cold climate may bedue, at least inpart, to someunderlyingpre-orperinatal en-vironmental influences. For example, several studies have
1To whom correspondence should be addressed; Genetics Lab-oratory, McLean Hospital, NB-G-28 115 Mill Street, Belmont,MA 02478; tel: 617-855-3439, fax: 617-855-2348, e-mail:[email protected].
Schizophrenia Bulletin vol. 35 no. 3 pp. 582–595, 2009doi:10.1093/schbul/sbp023Advance Access publication on April 8, 2009
! The Author 2009. Published by Oxford University Press on behalf of the Maryland Psychiatric Research Center. All rights reserved.For permissions, please email: [email protected].
582
Tuesday, December 11, 12

Mismatch, Skin Color & Schizophrenia
different sites around the world1,2 were not simply arti-facts of differences in diagnostic and ascertainment meth-ods used by different studies. Even though our analysesrestricted prevalence studies to those that used more sim-ilar research methods for diagnosis and ascertainment ofschizophrenia cases, our analyses also found (a) thatprevalence rates varied more than 10-fold across geo-graphic sites and (b) that prevalence increased markedlywith increasing latitude.
That the correlation of schizophrenia prevalence withlatitude is both robust and large, and is not due simply tobetween-site differences in diagnostic and ascertainmentmethods, is further suggested by analysis of data collectedby Lehtinen et al.42 Their study is particularly informa-tive because it is the study that best controlled for possi-ble methodological sources of differences in prevalence atdifferent geographic sites; the same investigative person-nel, as well as the same methods, were used to obtainprevalence rates at several different sites within thesame country. Those investigators studied schizophreniaprevalence at 5 different Finnish sites in the same timeperiod, using a consistent set of diagnostic criteria andascertainment methods, and their data showed a veryhigh correlation of prevalence with both latitude(r = .97, P < .01) and mean low temperature (r =!.99, P < .001).
Athigher latitudes, there isanespeciallywidevariation inprevalence rates. By contrast, near the equator, prevalencefor all sites tends to be quite low. That is, for all groups andcontinental regions for which there are data frommultiplesites, thebest-fit (least squares) regression lines all havepos-
itiveslopes,andtheslopes tendtobesteeper forsitesathigh-er latitudes.This is evident by inspecting table 1, but ismostreadily visualized in figure 1.The results suggest that etiologic factors closely asso-
ciated with latitude and cold climate may be much morepowerful contributors to risk for schizophrenia than isgenerally recognized. The general level of a population’seconomic status and healthcare, as indexed in our anal-ysis by the infant mortality rate, appears to be a muchweaker predictor of risk for schizophrenia than are lati-tude and winter temperature. A high infant mortality rate
Fig. 2. Schizophrenia Prevalence and Latitude by Fish Intake.Note:Errorbars represent95%confidence limits.Theslopesof linear regression lineswere0.03 for siteswithhighfish intake, 0.21 for siteswithmoderate fish intake, and 0.17 for siteswith low fish intake. For the subset of Scandinavian sites, the slope of linear regression forwas 0.03 forsites with high fish intake and 1.57 for sites with moderate fish intake.
Fig. 3. Schizophrenia Prevalence and Latitude by Skin Color.Note: Error bars represent 95% confidence limits. The slopes of thelinear regression lines were 0.24 for those with lightest skin, 0.43 forthosewithintermediateskincolor,and0.31forthosewithdarkestskin.
590
D. K. Kinney et al.
Relation of Schizophrenia Prevalence to Latitude, Climate, Fish Consumption, InfantMortality, and Skin Color: A Role for Prenatal Vitamin DDeficiency and Infections?
Dennis K. Kinney1–3, Pamela Teixeira2, Diane Hsu2, SienaC. Napoleon2,4, David J. Crowley2, Andrea Miller2,William Hyman2, and Emerald Huang2
2Genetics Laboratory, McLean Hospital, Belmont, MA; 3De-partment of Psychiatry, Harvard Medical School, Boston, MA;4Wellesley College, Wellesley, MA
Previous surveys found a large (>10-fold) variation inschizophrenia prevalence at different geographic sitesand a tendency for prevalence to increase with latitude.We conducted meta-analyses of prevalence studies to inves-tigate whether these findings pointed to underlying etiologicfactors in schizophrenia or were the result of methodolog-ical artifacts or the confounding of sites’ latitude with levelof healthcare at those sites. We found that these patternswere still present after controlling for an index of health-care—infant mortality—and focusing on 49 studies thatused similar diagnostic and ascertainment methods. Thetendencies for schizophrenia prevalence to increase withboth latitude and colder climate were still large and signif-icant and present on several continents. The increase inprevalence with latitude was greater for groups with lowfish consumption, darker skin, and higher infant mortali-ty—consistent with a role of prenatal vitamin D deficiencyin schizophrenia. Previous research indicates that poor pre-natal healthcare and nutrition increase risk for schizophre-nia within the same region. These adverse conditions aremore prevalent in developing countries concentrated nearthe equator, but schizophrenia prevalence is lowest atsites near the equator. This suggests that schizophrenia-producing environmental factors associated with higher lat-itude may be so powerful they overwhelm protective effectsof better healthcare in industrialized countries. The ob-served patterns of correlations of risk factors with preva-lence are consistent with an etiologic role for prenatalvitamin D deficiency and exposure to certain infectious dis-eases. Research to elucidate environmental factors that un-
derlie variations in schizophrenia prevalence deserves highpriority.
Key words: epidemiology/etiology/immune function/prenatal/geography/risk factor
Introduction
Schizophrenia is an unusually burdensome disorder be-cause of the great economic costs of extensive care andloss of economic productivity, as well as the personal suf-fering and stigma, which often affect a patient and his orher family for most of the patient’s life. Moreover, formost patients there is still no cure or even an effectiveway of treating many of the most disabling, ‘‘negative’’symptoms of the disorder. Therefore, a key goal of schizo-phrenia research is elucidation of etiologic factors, partic-ularly environmental ones that could be readily avoidedand used in effective, inexpensive, and ethically sound pri-mary prevention programs.In a comprehensive survey of schizophrenia prevalence
studies around the world that were published in Englishover a period of 4 decades, Torrey1 noted 2 importantpatterns. First, prevalence rates varied widely at differentgeographic sites, with the highest rate being more than 10times greater than the lowest. Second, there was a strongtendency for schizophrenia prevalence to increase withincreasing latitude; ie, prevalence rates tended to bevery low near the equator and to increase as one movedtoward the poles. Both of Torrey’s conclusions were alsoreached in a survey and meta-analysis by Saha et al,2
which included more recent studies as well as ones pub-lished in languages other than English. Several other sur-veys have also concluded that schizophrenia rates vary atleast 10-fold around the world, including studies usingmeasures of point prevalence, lifetime prevalence, andincidence.1,3–10
A number of explanations have been proposed for thisvariability inprevalence.Severalcomplementary linesofre-search suggest that the tendency for schizophrenia preva-lence to increase with latitude and cold climate may bedue, at least inpart, to someunderlyingpre-orperinatal en-vironmental influences. For example, several studies have
1To whom correspondence should be addressed; Genetics Lab-oratory, McLean Hospital, NB-G-28 115 Mill Street, Belmont,MA 02478; tel: 617-855-3439, fax: 617-855-2348, e-mail:[email protected].
Schizophrenia Bulletin vol. 35 no. 3 pp. 582–595, 2009doi:10.1093/schbul/sbp023Advance Access publication on April 8, 2009
! The Author 2009. Published by Oxford University Press on behalf of the Maryland Psychiatric Research Center. All rights reserved.For permissions, please email: [email protected].
582
Tuesday, December 11, 12

Mismatch, Skin Color & SchizophreniaSemmelweis
Reflex
different sites around the world1,2 were not simply arti-facts of differences in diagnostic and ascertainment meth-ods used by different studies. Even though our analysesrestricted prevalence studies to those that used more sim-ilar research methods for diagnosis and ascertainment ofschizophrenia cases, our analyses also found (a) thatprevalence rates varied more than 10-fold across geo-graphic sites and (b) that prevalence increased markedlywith increasing latitude.
That the correlation of schizophrenia prevalence withlatitude is both robust and large, and is not due simply tobetween-site differences in diagnostic and ascertainmentmethods, is further suggested by analysis of data collectedby Lehtinen et al.42 Their study is particularly informa-tive because it is the study that best controlled for possi-ble methodological sources of differences in prevalence atdifferent geographic sites; the same investigative person-nel, as well as the same methods, were used to obtainprevalence rates at several different sites within thesame country. Those investigators studied schizophreniaprevalence at 5 different Finnish sites in the same timeperiod, using a consistent set of diagnostic criteria andascertainment methods, and their data showed a veryhigh correlation of prevalence with both latitude(r = .97, P < .01) and mean low temperature (r =!.99, P < .001).
Athigher latitudes, there isanespeciallywidevariation inprevalence rates. By contrast, near the equator, prevalencefor all sites tends to be quite low. That is, for all groups andcontinental regions for which there are data frommultiplesites, thebest-fit (least squares) regression lines all havepos-
itiveslopes,andtheslopes tendtobesteeper forsitesathigh-er latitudes.This is evident by inspecting table 1, but ismostreadily visualized in figure 1.The results suggest that etiologic factors closely asso-
ciated with latitude and cold climate may be much morepowerful contributors to risk for schizophrenia than isgenerally recognized. The general level of a population’seconomic status and healthcare, as indexed in our anal-ysis by the infant mortality rate, appears to be a muchweaker predictor of risk for schizophrenia than are lati-tude and winter temperature. A high infant mortality rate
Fig. 2. Schizophrenia Prevalence and Latitude by Fish Intake.Note:Errorbars represent95%confidence limits.Theslopesof linear regression lineswere0.03 for siteswithhighfish intake, 0.21 for siteswithmoderate fish intake, and 0.17 for siteswith low fish intake. For the subset of Scandinavian sites, the slope of linear regression forwas 0.03 forsites with high fish intake and 1.57 for sites with moderate fish intake.
Fig. 3. Schizophrenia Prevalence and Latitude by Skin Color.Note: Error bars represent 95% confidence limits. The slopes of thelinear regression lines were 0.24 for those with lightest skin, 0.43 forthosewithintermediateskincolor,and0.31forthosewithdarkestskin.
590
D. K. Kinney et al.
Relation of Schizophrenia Prevalence to Latitude, Climate, Fish Consumption, InfantMortality, and Skin Color: A Role for Prenatal Vitamin DDeficiency and Infections?
Dennis K. Kinney1–3, Pamela Teixeira2, Diane Hsu2, SienaC. Napoleon2,4, David J. Crowley2, Andrea Miller2,William Hyman2, and Emerald Huang2
2Genetics Laboratory, McLean Hospital, Belmont, MA; 3De-partment of Psychiatry, Harvard Medical School, Boston, MA;4Wellesley College, Wellesley, MA
Previous surveys found a large (>10-fold) variation inschizophrenia prevalence at different geographic sitesand a tendency for prevalence to increase with latitude.We conducted meta-analyses of prevalence studies to inves-tigate whether these findings pointed to underlying etiologicfactors in schizophrenia or were the result of methodolog-ical artifacts or the confounding of sites’ latitude with levelof healthcare at those sites. We found that these patternswere still present after controlling for an index of health-care—infant mortality—and focusing on 49 studies thatused similar diagnostic and ascertainment methods. Thetendencies for schizophrenia prevalence to increase withboth latitude and colder climate were still large and signif-icant and present on several continents. The increase inprevalence with latitude was greater for groups with lowfish consumption, darker skin, and higher infant mortali-ty—consistent with a role of prenatal vitamin D deficiencyin schizophrenia. Previous research indicates that poor pre-natal healthcare and nutrition increase risk for schizophre-nia within the same region. These adverse conditions aremore prevalent in developing countries concentrated nearthe equator, but schizophrenia prevalence is lowest atsites near the equator. This suggests that schizophrenia-producing environmental factors associated with higher lat-itude may be so powerful they overwhelm protective effectsof better healthcare in industrialized countries. The ob-served patterns of correlations of risk factors with preva-lence are consistent with an etiologic role for prenatalvitamin D deficiency and exposure to certain infectious dis-eases. Research to elucidate environmental factors that un-
derlie variations in schizophrenia prevalence deserves highpriority.
Key words: epidemiology/etiology/immune function/prenatal/geography/risk factor
Introduction
Schizophrenia is an unusually burdensome disorder be-cause of the great economic costs of extensive care andloss of economic productivity, as well as the personal suf-fering and stigma, which often affect a patient and his orher family for most of the patient’s life. Moreover, formost patients there is still no cure or even an effectiveway of treating many of the most disabling, ‘‘negative’’symptoms of the disorder. Therefore, a key goal of schizo-phrenia research is elucidation of etiologic factors, partic-ularly environmental ones that could be readily avoidedand used in effective, inexpensive, and ethically sound pri-mary prevention programs.In a comprehensive survey of schizophrenia prevalence
studies around the world that were published in Englishover a period of 4 decades, Torrey1 noted 2 importantpatterns. First, prevalence rates varied widely at differentgeographic sites, with the highest rate being more than 10times greater than the lowest. Second, there was a strongtendency for schizophrenia prevalence to increase withincreasing latitude; ie, prevalence rates tended to bevery low near the equator and to increase as one movedtoward the poles. Both of Torrey’s conclusions were alsoreached in a survey and meta-analysis by Saha et al,2
which included more recent studies as well as ones pub-lished in languages other than English. Several other sur-veys have also concluded that schizophrenia rates vary atleast 10-fold around the world, including studies usingmeasures of point prevalence, lifetime prevalence, andincidence.1,3–10
A number of explanations have been proposed for thisvariability inprevalence.Severalcomplementary linesofre-search suggest that the tendency for schizophrenia preva-lence to increase with latitude and cold climate may bedue, at least inpart, to someunderlyingpre-orperinatal en-vironmental influences. For example, several studies have
1To whom correspondence should be addressed; Genetics Lab-oratory, McLean Hospital, NB-G-28 115 Mill Street, Belmont,MA 02478; tel: 617-855-3439, fax: 617-855-2348, e-mail:[email protected].
Schizophrenia Bulletin vol. 35 no. 3 pp. 582–595, 2009doi:10.1093/schbul/sbp023Advance Access publication on April 8, 2009
! The Author 2009. Published by Oxford University Press on behalf of the Maryland Psychiatric Research Center. All rights reserved.For permissions, please email: [email protected].
582
Tuesday, December 11, 12

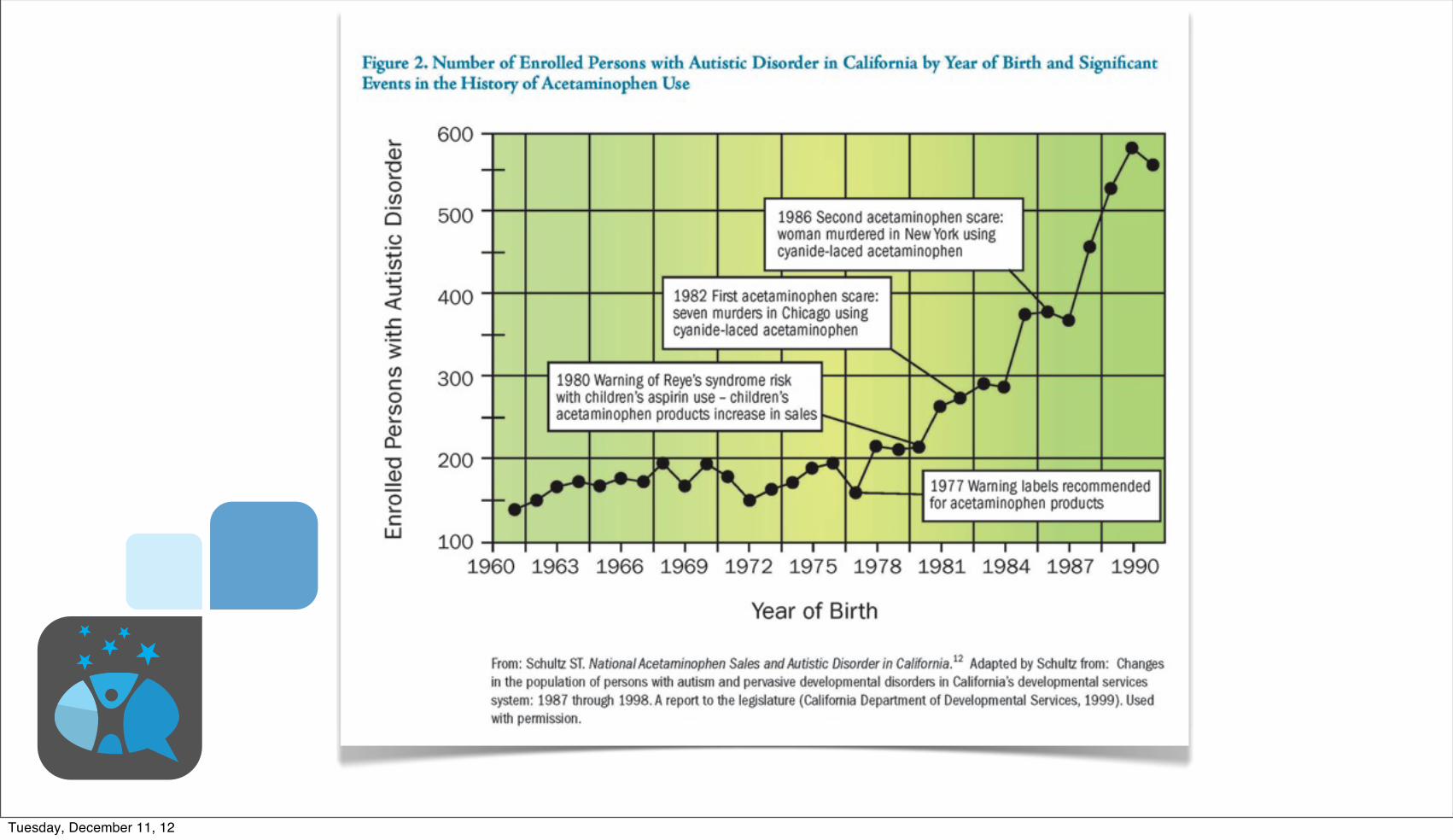
Latitude and Infantile Autism
Grant, W. B. and C. M. Soles (2009). "Epidemiologic evidence supporting the role of maternal vitamin D deficiency as a risk factor for the development of infantile autism." Dermatoendocrinol 1(4): 223-228.
Tuesday, December 11, 12

Latitude and Infantile AutismSemmelweis
ReflexGrant, W. B. and C. M. Soles (2009). "Epidemiologic evidence supporting the role of maternal vitamin D deficiency as a risk factor for the development of infantile autism." Dermatoendocrinol 1(4): 223-228.
Tuesday, December 11, 12

Estimated deaths per year would fallby 37,000 people, or about 16%-22% of annual mortality
in Canada.
And, $14 billion
Tuesday, December 11, 12

Semmelweis Reflex
Estimated deaths per year would fallby 37,000 people, or about 16%-22% of annual mortality
in Canada.
And, $14 billion
Tuesday, December 11, 12

Among pregnant women, lower Vitamin D is associated with:• Adverse fertility
parameters (n = 2),
• Preeclampsia (n = 5),
• Gestational diabetes or higher blood glucose (n = 6),
• Bacterial vaginosis (n = 4),
• Primary cesarean section (n = 1),
• Few days' (n = 2) shorter gestation,
• And, postpartum depression (n = 1)
Acta Obstet Gynecol Scand. 2012 Dec;91(12):1357-67. doi: 10.1111/aogs.12000. Epub 2012 Oct 17.The impact of vitamin D on pregnancy: a systematic review.Christesen HT, Falkenberg T, Lamont RF, Jørgensen JS.
Tuesday, December 11, 12

Among pregnant women, lower Vitamin D is associated with:• Adverse fertility
parameters (n = 2),
• Preeclampsia (n = 5),
• Gestational diabetes or higher blood glucose (n = 6),
• Bacterial vaginosis (n = 4),
• Primary cesarean section (n = 1),
• Few days' (n = 2) shorter gestation,
• And, postpartum depression (n = 1)
Acta Obstet Gynecol Scand. 2012 Dec;91(12):1357-67. doi: 10.1111/aogs.12000. Epub 2012 Oct 17.The impact of vitamin D on pregnancy: a systematic review.Christesen HT, Falkenberg T, Lamont RF, Jørgensen JS.
Semmelweis Reflex
Tuesday, December 11, 12

Vitamin D with Omega-3 (fish)
• Reduced postpartum depression
• Reduced lifetime depression, including bipolar disorder
• Increased child IQ
• Better academic success
• Reduced childhood mental, emotional, and behavioural disorders
Hibbeln, J., J. M. Davis, et al. (2007). "Maternal seafood consumption in pregnancy and neurodevelopmental outcomes in childhood (ALSPAC study): an observational cohort study." The Lancet 369(9561): 578-585.
Hibbeln, J. R., L. R. Nieminen, et al. (2006). "Healthy intakes of n-3 and n-6 fatty acids: estimations considering worldwide diversity." American Journal of Clinical Nutrition 83(6 Suppl): 1483S-1493S.
Tuesday, December 11, 12

Vitamin D with Omega-3 (fish)
• Reduced postpartum depression
• Reduced lifetime depression, including bipolar disorder
• Increased child IQ
• Better academic success
• Reduced childhood mental, emotional, and behavioural disorders
Hibbeln, J., J. M. Davis, et al. (2007). "Maternal seafood consumption in pregnancy and neurodevelopmental outcomes in childhood (ALSPAC study): an observational cohort study." The Lancet 369(9561): 578-585.
Hibbeln, J. R., L. R. Nieminen, et al. (2006). "Healthy intakes of n-3 and n-6 fatty acids: estimations considering worldwide diversity." American Journal of Clinical Nutrition 83(6 Suppl): 1483S-1493S.
Semmelweis Reflex
Tuesday, December 11, 12
Tuesday, December 11, 12

Semmelweis Reflex
Tuesday, December 11, 12

Semmelweis Reflex
Tuesday, December 11, 12

Semmelweis Reflex
Tuesday, December 11, 12

Semmelweis Reflex
Tuesday, December 11, 12

Semmelweis Reflex
Tuesday, December 11, 12

Tuesday, December 11, 12

Semmelweis Reflex
Tuesday, December 11, 12

Richly Reinforce Pro-social Behaviors Reduce Toxic In!uences
Limit Problematic Behaviors Increase Psychological FlexibilityBiglan, A., B. R. Flay, et al. (2012). "The critical role of nurturing environments for promoting human well-being." American Psychologist.
Tuesday, December 11, 12

How might we reduce alcohol, tobacco, and other drugs among women of child bearing age
Tuesday, December 11, 12

Which warning labels might work?
Tuesday, December 11, 12

Trendline for humorous warnings on binge drinking by women of child-rearing
No Warnings Humorous Warnings
Tuesday, December 11, 12

Trendline for humorous warnings on binge drinking by women of child-rearing
1995 1997 1999 2001 2002 2003 2004 2005 2006 20070
4
8
12
16
20Pe
rcen
tage
No Warnings Humorous Warnings
Tuesday, December 11, 12

Trendline for humorous warnings on binge drinking by women of child-rearing
1995 1997 1999 2001 2002 2003 2004 2005 2006 20070
4
8
12
16
20Pe
rcen
tage
No Warnings Humorous Warnings
Tuesday, December 11, 12

Trendline for humorous warnings on binge drinking by women of child-rearing
1995 1997 1999 2001 2002 2003 2004 2005 2006 20070
4
8
12
16
20Pe
rcen
tage
No Warnings Humorous Warnings
Tuesday, December 11, 12

Rewarding Clerks & Stores for Not Welling to MinorsYouth Who Smoked Every Day the Last 30 Days
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
1995 1997 1999 2001 2003 2005 2007
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
Baseline Reward and Reminder
Source: YRBS, US Centers for Disease Control
Wyoming
Wisconsin
United States
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
1995 1997 1999 2001 2003 2005 2007
Wyoming
Wisconsin
United States
Youth Who Smoked During the Last 30 DaysBaseline Reward and Reminder
Source: YRBS, US Centers for Disease Control
= Trend = Wyoming = Wisconsin =United States
Youth Who Smoked Every Day the Last 30 Days
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
1995 1997 1999 2001 2003 2005 2007
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
Baseline Reward and Reminder
Source: YRBS, US Centers for Disease Control
Wyoming
Wisconsin
United States
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
1995 1997 1999 2001 2003 2005 2007
Wyoming
Wisconsin
United States
Youth Who Smoked During the Last 30 DaysBaseline Reward and Reminder
Source: YRBS, US Centers for Disease Control
= Trend = Wyoming = Wisconsin =United States
Source: Youth Risk Behavior Survey
(YRBS), Centers for Disease Control
Tuesday, December 11, 12

Rewarding Clerks & Stores for Not Welling to MinorsYouth Who Smoked Every Day the Last 30 Days
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
1995 1997 1999 2001 2003 2005 2007
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
Baseline Reward and Reminder
Source: YRBS, US Centers for Disease Control
Wyoming
Wisconsin
United States
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
1995 1997 1999 2001 2003 2005 2007
Wyoming
Wisconsin
United States
Youth Who Smoked During the Last 30 DaysBaseline Reward and Reminder
Source: YRBS, US Centers for Disease Control
= Trend = Wyoming = Wisconsin =United States
Youth Who Smoked Every Day the Last 30 Days
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
1995 1997 1999 2001 2003 2005 2007
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
Baseline Reward and Reminder
Source: YRBS, US Centers for Disease Control
Wyoming
Wisconsin
United States
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
1995 1997 1999 2001 2003 2005 2007
Wyoming
Wisconsin
United States
Youth Who Smoked During the Last 30 DaysBaseline Reward and Reminder
Source: YRBS, US Centers for Disease Control
= Trend = Wyoming = Wisconsin =United States
Source: Youth Risk Behavior Survey
(YRBS), Centers for Disease Control
Tuesday, December 11, 12

Happens BEFORE the
behavior
Wait for the Timer for tobacco addictions with SMI/CMI
AntecedentKernel
Tuesday, December 11, 12
Writ
e a
thou
ght a
nd a
feelin
g on the leaf and put it on the thoughts and feelings “stream”
I am
hav
ing
the
thou
ght t
hat…
I am having a feeling of …
Copyright © 2007-2012, PAXIS Institute. All rights reserved. May be reproduced but not sold. www.paxtalk.com
I am having a sensation of …
Teaching Psychological flexibility by cognitive defusion
Tuesday, December 11, 12

Writ
e a
thou
ght a
nd a
feelin
g on the leaf and put it on the thoughts and feelings “stream”
I am
hav
ing
the
thou
ght t
hat…
I am having a feeling of …
Copyright © 2007-2012, PAXIS Institute. All rights reserved. May be reproduced but not sold. www.paxtalk.com
I am having a sensation of …
Teaching Psychological flexibility by cognitive defusion
Tuesday, December 11, 12

ReinforcementKernel
Lifespan example of one kernel for prevention, intervention and
treatment
Happens AFTER the behavior
Available from Amazon.com for $45
Tuesday, December 11, 12

Mobilizing for MACH
Tuesday, December 11, 12

Implementation & Logic Models
Recognize & Reward successes in/by��0HGLD��3ROLWLFDO�DUHQD��2WKHU�OHDGHUV��,PPLWDWDEOH�PRGHOV�IURP��DOO�DJHV�DQG�EDFNJURXQGV
Create CommunityPreventionScore/Dashboard
Multi-problem analyses
NurturingEnvironmentsLogic Model forpopulation-level
benefits
Identify%HKDYLRUVWR�,QFUHDVH�
Identify %HKDYLRUV�WR�'HFUHDVH
PredictBenefits:
(VWLPDWHORFDO��VWDWH���QDWLRQDOSUHYDOHQFH�FRVWV�VDYHG�E\SURSRVHGSUHYHQWLRQUHFLSHV��Update Research
Databases for ProvenPrevention Solutions3V\FKLQIR��SXEPHG�JRY�HWF��6HH�)OD\�HW�DO�������IRU�VWDQGDUGV�RI�HYLGHQFH�
Document 8VHU�([SHULHQFHV��/HVVRQV�/HDUQHG�DW�/RFDO��6WDWH�
�1DWLRQDO�/HYHOV
&LWH�SRZHUIXOVWXGLHV��OLQNVWR�FXOWXUDO�SUDFWLFHV�
&LWH�UHOHYDQW�HQGRUVHPHQWV�RU�VWDQGDUGV
Create�SROLF\�RUJDQL]DWLRQDO��DGYRFDF\�VXSSRUWVWR�QXUWXUH�HIIRUWV�
Cultivate VRPHFXUUHQW�RU�HDUO\�DGRSWHUV�IRU�ORFDOLPSDFW�GDWD�DQGORFDO�WHVWLPRQLDOV����
/R���+L
Launch Social Marketing: Advocacy & Media
Products KDYHFDWFK\��SRVLWLYHQDPH��D�PHPH�
PerformanceQDPHV�EHQHILWV��OLWWOH�SDLQ�
Place�IRU�JHWWLQJSURGXFW�LV�HDV\�QRQ�VWLJPDWL]LQJ
Promotion IRFXVHV�RQ�SRSXODULW\��MRLQLQJ��DOLJQHG�YDOXHV��EHQHILWV�IRU�DOO�&UHDWLYH�HSLGHPLRORJ\�DOLJQV�SHRSOH�RUJDQL]DWLRQV�IRU�FRPPRQ�DFWLRQ��
Create ZRUNIRUFH�WUDLQLQJV\VWHPV
�Report
RQ�PRQQLWRULQJ�HYDOXDWLRQ�RI�TXLFN��PHGLXP��ORQJHUWHUP�RXWFRPHV
Monitor & CoachLPSOHPHQWDWLRQ &SUR[LPDO�RXWFRPHV�
Plan Population-Level Change:5HDFK��(IÀFDF\�$GRSWLRQ��,PSOHPHQWDWLRQ�0DLQWHQDQFH
Price�LV�ORZ�IRUWR�XVH�LQ�PRQH\RU�WLPH�
Developmental stages
Multiple Settings
Families
SchoolsCommunities
Organiations
Birth Childhood Adolescence Adulthood
Inte
nsity
/reac
h le
vels
High IntensityLow reach
Low Intensity
A
B
C
Hi reach
Note: Workforce development e!ciency achieved by broad use of similar/same evidence-based strategies or evidence-based kernels.
&UHDWH�V\VWHPIRU�PRQLWRULQJ��HYDOXDWLRQ�UHVHDUFK��
Population-Level Targeting
Developed by PAXIS Institute © 2010-2012, all rights reserved. May be freely reporduced in total with attribution and notice
See:
Tuesday, December 11, 12

EpigenesisEpigenetics are heritable changes in gene expression caused by mechanisms other than changes in the underlying DNA sequence.
These changes can pass through multiple generations.
Genesis
Social Biological Environmental Inputs
Nurturing or Toxic Environments,
Disease, orThreats
Signali
ng
Morphogensis
PhosphorlyationAcetylation
Methylation
Histone RemodelingChromatin Stucture Changes
Development Immunity Stem Cell Changes Imprinting
ThreeGenerationE!ects
Parent, 1st Generation
Baby, 2nd Generation
Reproductive Cells,3rd Generation
These polygenes
can be “added”,
“subtracted”, “divided”, or “multiplied.”
Tuesday, December 11, 12
