the visual consequences of when a mild concussion becomes ... · the visual consequences of when a...
TRANSCRIPT

The Visual Consequences of when a Mild Concussion becomes a Severe Brain Injury…
Dan L. Fortenbacher, O.D., FCOVD
Lindsey Stull, O.D., FCOVD
Ryan Edwards, O.D. MVTSG 2014 – MCO
January 25, 2014
…an Advanced Model for Neuro-Optometric
Vision Rehabilitative Care
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
• Why? – Because too many patients who have a “mild concussion”
exacerbate into a more severe brain injury, resulting in severe visual problems, often weeks and months after the injury
• What? – We will attempt to remove some of the mystery surrounding
acquired brain injury (ABI) and show how even a “mild concussive event” can lead to serious vision problems
• How? – Show how you can apply the principals of this advanced model for
effective neuro-optometric vision rehabilitative treatment in your patient care
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

According to the US Centers for
Disease Control and Prevention
• Mild traumatic brain injury (mTBI) is:
…”the occurrence of injury to the head arising from blunt trauma or acceleration or deceleration forces with one or more of the following conditions attributable to the injury: any period of observed or self –reported transient confusion, disorientation or impaired consciousness, dysfunction of memory around the time of injury, or loss of consciousness lasting less than 30 minutes.”
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

mTBI continued
• …“In addition, observed signs of injury to
the head, irritability, lethargy, or vomiting
following head injury, especially among
infants and very young children;
headaches, dizziness, irritability fatigue or
poor concentration, especially among older
children and adults”
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
CDC 2003 Report to
Congress
• Of the more than 1.5 million people
experiencing TBI each year in the United
States, it has been estimated that 75%
experience mTBI
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Unified approach to managing
mTBIs
• Department of Defense and Department of Veterans Affairs
• Majority of TBIs in military and civilian population are considered mild
• “Mild” shouldn’t be used to define the severity of symptoms
• www.ncbi.nlm.nih.gov/pmc/articles/PMC3021720 Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Diagnosing with Imaging
• Common feature of mTBI is Diffuse Axonal Injury (DAI)
• Symptoms are primary tool for diagnosis of mTBI because:
• CT scans often normal
with mTBI patients
and poor at detecting DAI
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

MRI
• DAI is difficult to detect
using conventional MRI
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Advancements in Imaging
• Goal is create a unified approach to diagnose mTBI
• MRI technique called Diffusion Tensor Imaging (DTI)
• Detects microscopic brain matter tract lesions
• Measures Fractional Anisotropy (FA)- flow of water molecules along axons in brain
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Fractional anisotropy (FA) readings that were
detected using diffusion tensor imaging.
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Interpretation of Low FA
• Low FA represents disorganized movement of water molecules
• More disruption indicates more severe injury and more symptomatic
• High correlation between low FA and impaired executive function testing*
http://www.ncbi.nlm.nih.gov/pubmed/19567646
* Lipton, et al. Diffusion-Tensor Imaging Implicates Prefrontal Axonal Injury in Executive Function Impairment Following Very Mild Traumatic Brain Injury. Radiology 2009; 252: 816-824
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Interpretation of High FA
• High FA indicates more organization and
therefore may represent less injury or brain
is already trying to compensate for injury
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Conclusions
• An increase in the FA value may represent
a measurement of neuroplasticity and
improvement in brain organization
• FA values may give rehabilitation team a
marker to show progress and determine if
patient is responding well to treatment
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
“Post Trauma Vision Syndrome is the
most common visual sequel to mTBI.” 1998 Study guide: brain injury rehabilitation, pain rehabilitation, Supplement to
Archives of Physical Medicine and Rehabilitation, 79(3)(Supple.1), S10-S14
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Post Trauma Vision Syndrome
Characteristics
• Convergence insufficiency
• Exotropia or high exophoria
• Defective stereopsis
• Accommodative dysfunction
• Oculomotor dysfunction
• Low blink rate
• Spatial disorientation
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
Post Trauma Vision Syndrome
Symptoms
• Diplopia
• Dizziness
• Headaches especially with visually demanding tasks
• Light sensitivity
• Difficulty reading
• Skipping, repeating lines when reading
• Blurred vision especially at near
• Poor spatial judgment and depth perception
• Poor concentration and attention
• Poor balance, coordination, posture
• Poor visual memory
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

William Padula, O.D.
• Hypothesize that PTVS is due to shearing
injury particularly at the midbrain level
where the superior colliculi integrates and
organizes visual spatial information
• Disruption between focal and ambient
visual system
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Neural Substrates of Vision
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Four Anatomical
Components
• Cerebral Hemispheres
• Diencephalon
• Brainstem
• Cerebellum
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Cerebral Hemispheres (2)
• Four Lobes
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Frontal Lobe
• Most complex
• Last area of the brain to
mylenate
• Not a single functional unit
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
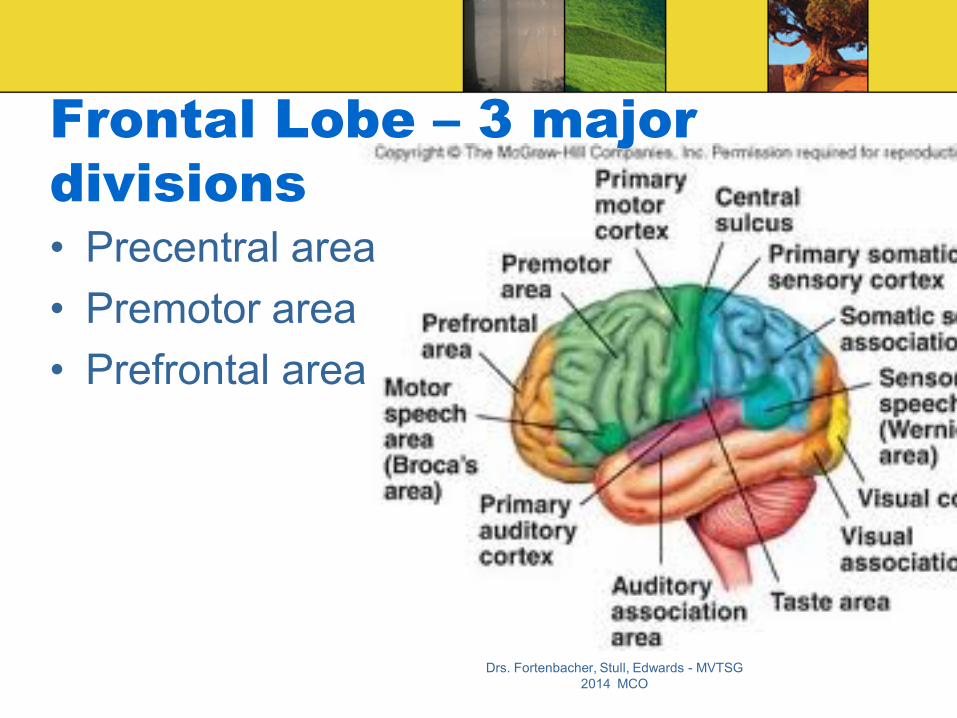
Frontal Lobe – 3 major
divisions
• Precentral area
• Premotor area
• Prefrontal area
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
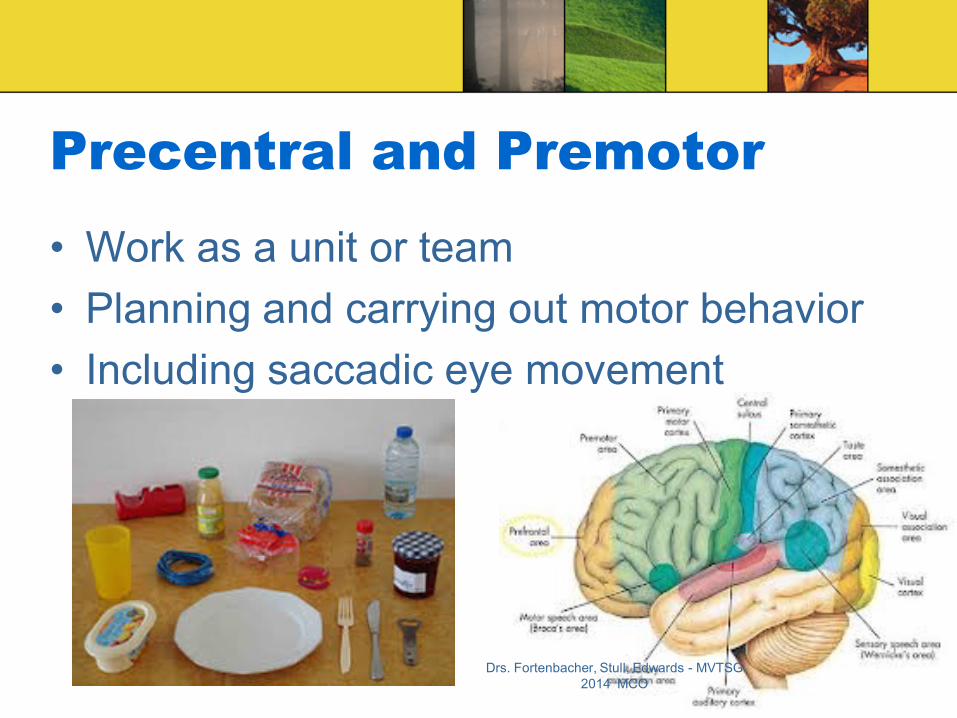
Precentral and Premotor
• Work as a unit or team
• Planning and carrying out motor behavior
• Including saccadic eye movement
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Prefrontal area
• Cognitive sophisticated integrative system
• Highest level of visual and other sensory modality
processing
• Results in higher action planning
• Incorporate meaning and intention
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

3 subdivisions of Prefrontal
• Dorsolateral
– Working memory
– Executive functioning
• Orbital frontal
– Personality
– Self Control
• Medial frontal
– Motivation for goal oriented activities Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Prefrontal Lobe
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
Books on the Frontal Lobe
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
Books on Frontal Lobe
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
Books on Frontal Lobe
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Books on Frontal Lobe
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Books on Frontal Lobe
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Temporal Lobe
• Object recognition
• Memory acquisition
• Emotional Variance
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Parietal Lobe
• Processing motion and location
• Multisensory integration
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Occipital
• Reception and early visual processing
• V1, V2 – Depth perception
• V3,V4,V5 – motion detection, size and
color
• V6- unknown
• V8 – Color analysis
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Diencephalon
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Pulivinar
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Diencephalon
• Thalamus – Pulvinar
• Integration of somatosensory and visual information
• Visual feature discrimination
• Analysis of vision
– Lateral Geniculate Nucleus – LGN • Part of afferent visual system
• Higher order visual processing at an early stage
• Hypothalamus – circadian rhythms and under control of the amygdala and prefrontal cortex
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Brainstem
• Diverse collection of nuclei related to
altering-arousal system that helps mediate
attention
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Cerebellum
• Spatial organization and memory
• Refining motor control and motor learning
• Vestibular input for balance and spatial
orientation
• Some cognitive functions
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

The 2 visual processing streams
of the brain
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
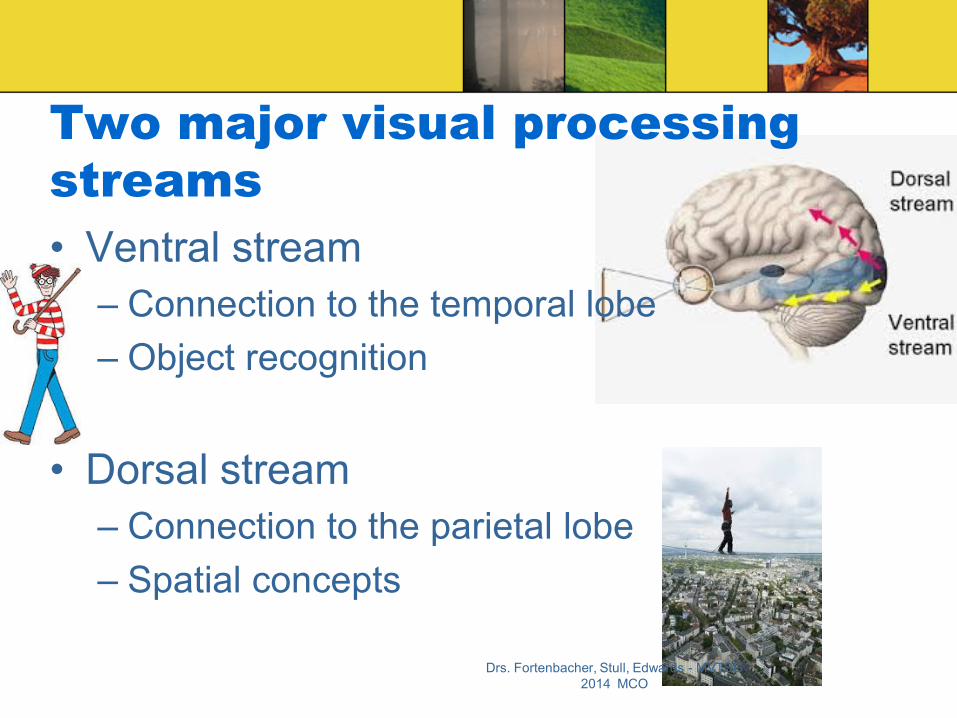
Two major visual processing
streams
• Ventral stream
– Connection to the temporal lobe
– Object recognition
• Dorsal stream
– Connection to the parietal lobe
– Spatial concepts
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Dorsal Stream splits into 3 pathways at
Posterior Parietal Cortex
• Parieto-prefrontal pathway
• Parieto-premotor pathway
• Parieto-medial temporal pathway
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
Each pathway of the PPC controls
different elements of visuo-spatial
function
• Neural nexus of visuo-spatial processing
and intermodal processing
• receives input from
– the auditory cortex
– vestibular input
– other areas of the brain
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Parieto-prefrontal pathway
• Eye movements important for reading
• Spatial working memory
– Important for navigating through new
environment
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Parieto-premotor pathway
• Has projections to both dorsal and ventral
premotor cortex
• Receives vestibular input from cerebellum
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
Parieto-premotor pathway
• Visually guided action
• Navagation
• Integration of body movement and vision
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Parieto-medial temporal pathway
• Connections to limbic areas
• Crucial for navigation
• Most complex, least understood
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Pre-Frontal Cortex –The Conductor
• Eye movements
• Visual attention
• Working memory
• Goal directed behavior Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Effects of mTBI on Prefrontal Cortex
• Oculomotor Dysfunction
– Deficiency in Saccadic Eye movement
• Vergence disorders
• Poor Visual Attention
• Trouble Interpreting visual space
• Poor working memory
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Effects of mTBI on PPC
• Dizziness, loss of balance
• Poor intersensory/intermodal integration
– Poor eye hand coordination
– Visual motor integration (fine motor, gross
motor)
• Clumsiness
– Visual vestibular integration
• Disorientation
• Poor spatial judgments
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Summary
• The visual process is intimately woven
throughout the entire brain
• Even a “mild concussive event” can result
in serious compromise to the neural
substrate, neural software, of the brain
• This can lead to serious visual problems
that require neuro-optometric vision
rehabilitation Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

An effective neuro-optometric vision
rehabilitation model based on the
principles of:
• Learning dependent neuroplasticity
• Top-Down (intrinsic motivation) processing
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
A model based on 5
Elements
1. Intrinsic motivation and engagement
2. Variety and repetition
3. Feedback
4. Motor match to sensory mismatch
5. Intersensory Loading and integration
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Lenses
• The role of the lens
– Refractive correction-
– Aid accommodation- • Influence binocular vision via AC:A
– Aid spatial awareness
– Aid peripheral awareness
– Aid focal-ambient integration • http://maunsell.med.harvard.edu/Downloads/publications/87bMaunsell.pdf
• http://www.oepf.org/jbo/journals/2-1%20Marrone.pdf
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Prisms
• Compensatory
• Spatial
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Yoked Prisms
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Bi-nasal occlusion
• Diplopia management
• Emphasize peripheral
awareness
• Facilitate focal ambient
integration
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

A model based on 5
Elements
1. Intrinsic motivation and engagement
2. Variety and repetition
3. Feedback
4. Motor match to sensory mismatch
5. Intersensory Loading and integration
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Spatial Floor Plan
• Alyson Olmstead, COVT
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Spatial Floor Pattern
• Intersensory Loading-yoked prisms
• Feedback-draw and compare pattern
• Variety and Repetition- complexity of patterns, memory, reverse steps, draw
out patterns Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Modified Marsden Ball Rail Walk
• Monica King, COVT
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
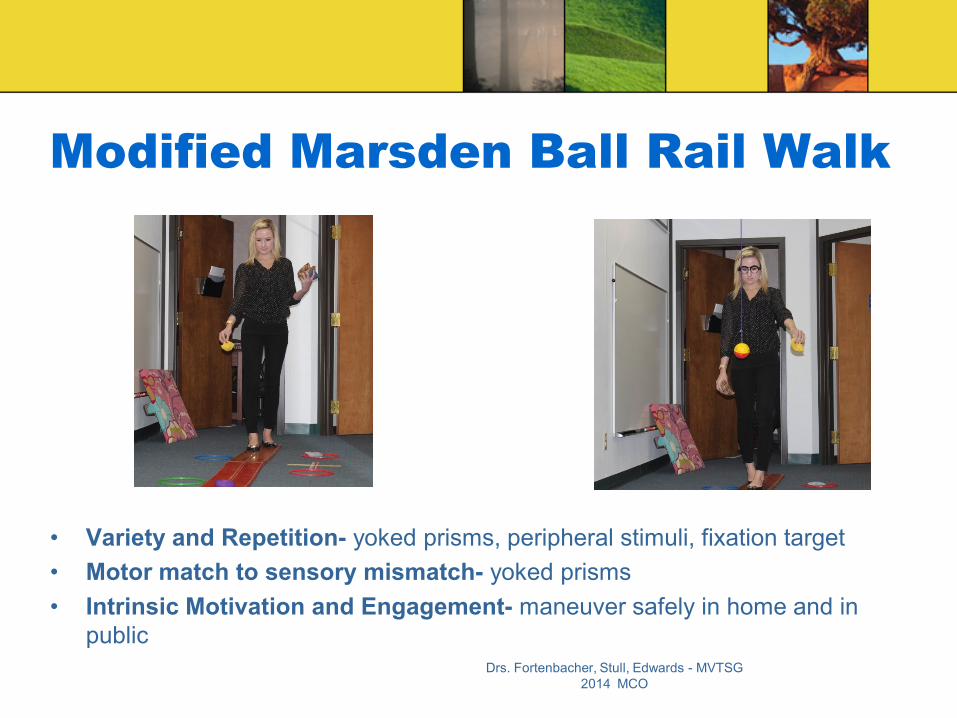
Modified Marsden Ball Rail Walk
• Variety and Repetition- yoked prisms, peripheral stimuli, fixation target
• Motor match to sensory mismatch- yoked prisms
• Intrinsic Motivation and Engagement- maneuver safely in home and in
public
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
Multi-Matrix
• Debra Irwin, COVT
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Multi-Matrix
• Intrinsic Motivation and Engagement- sports vision and competition
• Motor Match to Sensory Mismatch- yoked prism
• Intersensory Loading and Integration- vestibular, auditory, yoked prism
• Variety- patterns, different setup or instructions
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Our patient Thomas
• Age – 17
• Myopia
• Excellent student
• Stellar tennis player- rated in the state
• Suffered head injury from a fall in January
2012
• Dx: Post Concussive Syndrome
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Thomas’ Neuro-optometric
Diagnosis
• Post Trauma Vision Syndrome (PTVS)
• Oculomotor dysfunction
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO
Thomas video before and after
neuro optometric vision rehabilitation
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO

Questions
Drs. Fortenbacher, Stull, Edwards - MVTSG
2014 MCO