the role of uterine artery embolization in gynecology practice
TRANSCRIPT
The
role of u
uterine a
artery emmbolizati
on in gyynecologgy practicce

Apollo Medicine 2012 SeptemberVolume 9, Number 3; pp. 206e211 Review Article
The role of uterine artery embolization in gynecology practice
S. Kheda Amitha Vikramaa,*, Ramamurthy Chitrab
aConsghatta*CorreReceivCopyrihttp://d
ABSTRACT
Uterine artery embolization (UAE) is a minimally invasive interventional radiological procedure to occlude the arterialsupply to the uterus. UAE has been very useful for controlling hemorrhage following delivery/abortion, in ectopic orcervical pregnancy, gestational trophoblastic disease or carcinoma cervix. Currently it is being mostly used fortreating uterine fibroids. It requires a shorter hospital stay with early resumption to normal activity. This review brieflysummarizes the role of this relatively new technique in gynecologic practice.
Copyright © 2012, Indraprastha Medical Corporation Ltd. All rights reserved.
Keyword: Uterine artery embolization, Hemorrhage, Interventional Radiology
INTRODUCTION
Uterine artery embolization (UAE) is a relatively new, mini-mally invasive interventional radiological technique toocclude the arterial supply to the uterus. UAE has been prac-ticed over more than 20 years for controlling hemorrhagefollowing delivery/abortion, in ectopic or cervical preg-nancy, gestational trophoblastic disease or carcinoma cervix.
Currently, UAE is being used mostly for treating uterinefibroids. UAE is recommended to women with symptom-atic fibroids who wish to retain their uteruses and avoidsurgery. It selectively blocks the feeding arteries that supplyblood to the fibroids and causes ischemic necrosis andsubsequent absorption or expulsion of leiomyoma.1
Worldwide technical success rates reported for UAE are98%e100%.2e4 The decrease in fibroid and uterine size isaround 50% by the end of the first year post procedure. Themajority of patients have reported significant symptomimprovement and improvement in the overall quality oflife following UAE. Pregnancies have been reported afterthe procedure. However, pregnancy outcome was worsewhen compared with that of the general population. Miscar-riage rates are higher; the risk for abnormal placentation isincreased; and an increased incidence of preterm deliveryand postpartum hemorrhage has been reported.
ultant Vascular and Interventional Radiology, bSenior consultant, DeRoad, Bangalore 560076, India.sponding author. email: [email protected]:30.3.2012; Accepted: 29.6.2012; Available online: 5.7.2012ght � 2012, Indraprastha Medical Corporation Ltd. All rights reservedx.doi.org/10.1016/j.apme.2012.06.008
HISTORICAL ASPECTS
UAE was first reported in 1995, by Ravina et al.5 Theynoted that several women with symptomatic leiomyomatawho underwent UAE as a pre-hysterectomy treatment hadsignificant clinical improvement to an extent that hysterec-tomy was no longer required.
SURGERY VERSUS EMBOLIZATION
Few randomized controlled trials have compared UAE withsurgical management. The EMMY trial (EMbolizationversus hysterectoMY) reported similar symptom improve-ment rates between the two groups, and 76.5% of patientsrandomized to UAE were able to avoid surgery.6 The trialby Mara and colleagues compared myomectomy withUAE. Although symptom improvement was similarbetween the two approaches, reproductive outcome wassuperior in the myomectomy group.7
Uterine fibroid embolization has several advantages overconventional hormone suppression (progestogens andGnRHanalogs) and surgical procedures (myomectomy, hysterec-tomy), including avoidance of the side effects of drug therapyand postoperative complications resulting from surgery.8
partment of Obstetrics and Gynaecology, Apollo Hospitals, Banner-
.

The role of uterine artery embolization Review Article 207
The advantages of UAE compared with hysterectomyinclude avoidance of surgical risks, shorter hospitalization,and the potential for maintaining fertility. However, onemust remember that, unlike hysterectomy, UAE is palliativerather than curative.
UAE patients can expect excellent short-term and mid-term results with regards to menorrhagia, pelvic pain,bulk-related symptoms, and reductions in uterine volume.Longer term results are not known.
Recovery is shorter than recovery from hysterectomy oropen myomectomy (7e10 days versus 6 weeks).3,9
INDICATIONS
Symptomatic fibroids, dysfunctional uterine bleeding,adenomyosis; excessive bleeding due to uterine artery pseu-doaneurysm, arterio-venous malformations, trauma andpost curettage.
EMBOLIZATION IN POSTPARTUMHEMORRHAGE
Postpartum hemorrhage remains a major cause of maternalmortality throughout the world.10 Rapid identification ofthe source and control of bleeding are necessary becausethe situation is potentially life threatening. In most cases,primary postpartum hemorrhage can be managed withconservative treatment involving vaginal packing and admin-istration of uterotonic drugs. With persistent bleeding,vascular ligation or hysterectomy may be needed.11 Surgicaltreatment, however, sometimes may be technically difficultto perform and may fail to control hemorrhage. For thesereasons, transcatheter embolization of the uterine arteriesmay represent an interesting alternate technique in the treat-ment of intractable bleeding, preserving future fertility.
Major causes of bleeding include uterine atony, lowergenital tract lacerations or hematoma, retained placentaltissue, placenta accreta or percreta, rupture or inversion ofthe uterus and coagulopathy. Secondary postpartum hemor-rhage occurring more than 24 h after delivery is mainlyrelated to retained gestational products. In a study involving27 cases of primary postpartum hemorrhage, Pelage et al12
reported that selective arterial embolization was successfulin 25 cases after failure of medical management. Emboliza-tion failed in one of the patients with palcenta accreta wholater underwent hysterectomy.
Placenta accreta is one of the major causes of hysterec-tomy after embolization because of persistent bleeding.13
Failures are also likely to occur with unilateral treatmentand in patients who have undergone bilateral ligation ofthe hypogastric artery before embolization.
CONTRAINDICATIONS
Absolute contraindications include active infection andpregnancy. Relative contraindications include coagulop-athy, severe allergy to iodinated contrast, renal insuffi-ciency, prior pelvic irradiation and prior bilateral ligationof iliac arteries. It is also not advisable in women desirousof future pregnancy.
PRE-PROCEDURE EVALUATION
A complete history and physical examination is necessary,as well as ultrasonographic or magnetic resonance imaging(MRI) of pelvis to allow proper treatment. Uterine andfibroid volume measurements provide a baseline for deter-mining the degree of postprocedural reduction in fibroidand uterine volume.
In a preliminary report, Jha et al attached prognosticsignificance to both the location and vascularity of fibroidson MR imaging.14 Mizukami et al also have reporteda possible prognostic value for preprocedural MRI bydemonstrating better response to embolization in patientswith intermediate or high-signal intensity within theirfibroids on T2-weighted images (Fig. 7).15
Laboratory studies include hematocrit, coagulationprofile and serum creatinine.
Withhold GnRH agonist therapy at least 12 weeks prior tothe procedure. Premedication is usually with prophylacticantibiotics, corticosteroids, antiemetics, and analgesics.UAE is usually performed under conscious sedation. Corti-costeroids are well documented to reduce the incidence ofpostembolization syndrome after embolization of solidtumors. John J. Bissler et al16 reported that the use ofa short-term tapering dose of corticosteroid was successfulin reducing postembolization syndrome as compared withthe reported literature and also improved patient comfort.
PROCEDURE
The procedure time is 45e135 min with 90% of the proce-dures lasting from 50 to 75 min. There is an average proce-dural exposure of 20 rad to the ovaries. Most patients aredischarged within 24 h; however, hospitalization for up to48 h is sometimes required for the management of postop-erative pain. The majority of patients return to normal activ-ities within 1 week.17
Common femoral artery is punctured using an 18Gpuncture needle and access secured by a 5F sheath. Usuallythe right common femoral artery is punctured and rarelybilateral punctures may be required. A pigtail catheter ispositioned at the lower abdominal aorta and a flush
208 Apollo Medicine 2012 September; Vol. 9, No. 3 Amitha Vikrama and Chitra
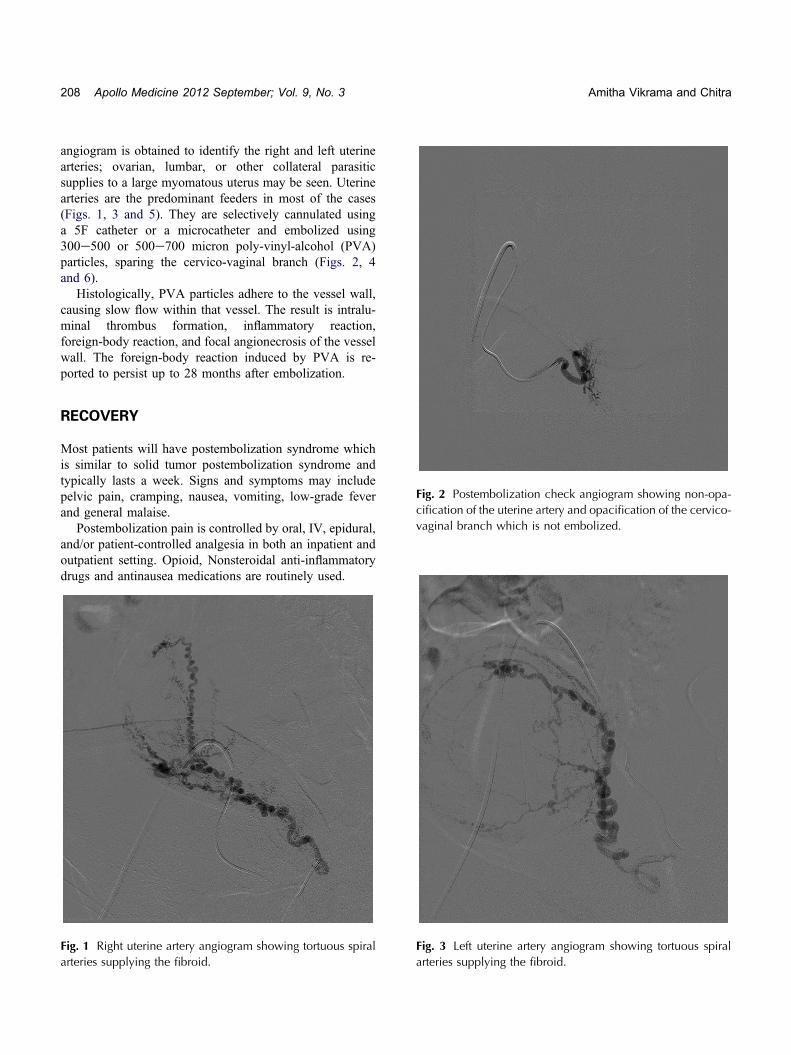
angiogram is obtained to identify the right and left uterinearteries; ovarian, lumbar, or other collateral parasiticsupplies to a large myomatous uterus may be seen. Uterinearteries are the predominant feeders in most of the cases(Figs. 1, 3 and 5). They are selectively cannulated usinga 5F catheter or a microcatheter and embolized using300e500 or 500e700 micron poly-vinyl-alcohol (PVA)particles, sparing the cervico-vaginal branch (Figs. 2, 4and 6).
Histologically, PVA particles adhere to the vessel wall,causing slow flow within that vessel. The result is intralu-minal thrombus formation, inflammatory reaction,foreign-body reaction, and focal angionecrosis of the vesselwall. The foreign-body reaction induced by PVA is re-ported to persist up to 28 months after embolization.
Fig. 2 Postembolization check angiogram showing non-opa-cification of the uterine artery and opacification of the cervico-vaginal branch which is not embolized.
RECOVERY
Most patients will have postembolization syndrome whichis similar to solid tumor postembolization syndrome andtypically lasts a week. Signs and symptoms may includepelvic pain, cramping, nausea, vomiting, low-grade feverand general malaise.
Postembolization pain is controlled by oral, IV, epidural,and/or patient-controlled analgesia in both an inpatient andoutpatient setting. Opioid, Nonsteroidal anti-inflammatorydrugs and antinausea medications are routinely used.
Fig. 1 Right uterine artery angiogram showing tortuous spiralarteries supplying the fibroid.
Fig. 3 Left uterine artery angiogram showing tortuous spiralarteries supplying the fibroid.
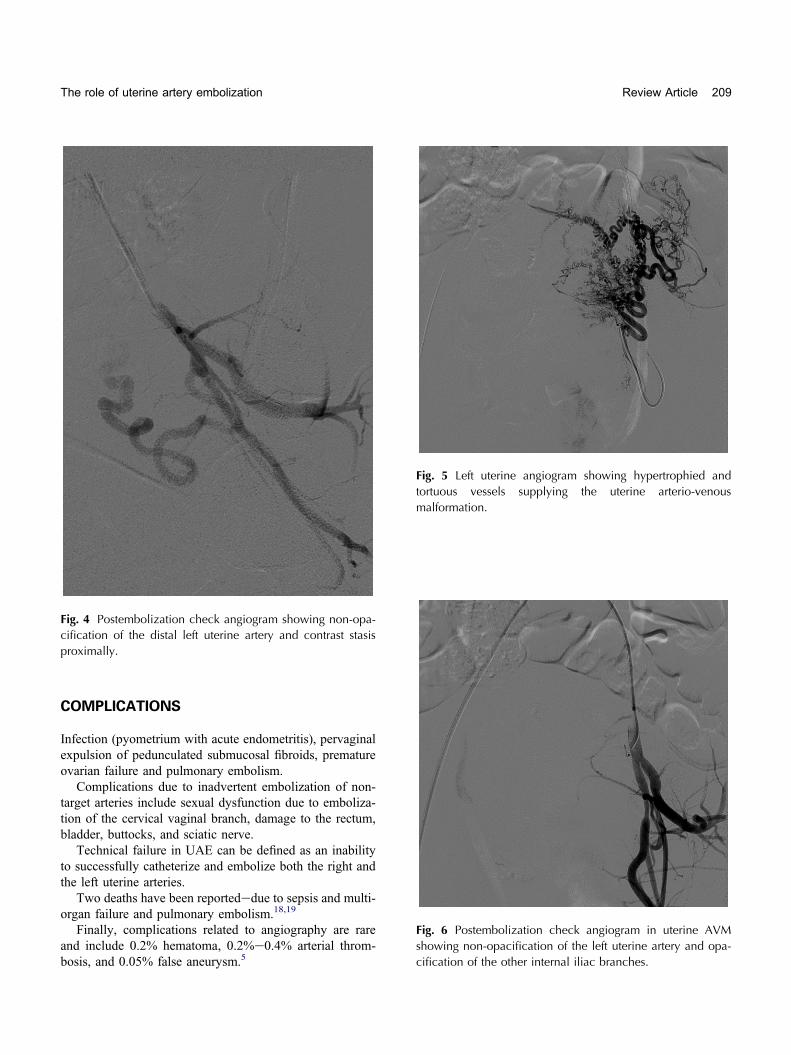
Fig. 4 Postembolization check angiogram showing non-opa-cification of the distal left uterine artery and contrast stasisproximally.
Fig. 5 Left uterine angiogram showing hypertrophied andtortuous vessels supplying the uterine arterio-venousmalformation.
Fig. 6 Postembolization check angiogram in uterine AVMshowing non-opacification of the left uterine artery and opa-cification of the other internal iliac branches.
The role of uterine artery embolization Review Article 209
COMPLICATIONS
Infection (pyometrium with acute endometritis), pervaginalexpulsion of pedunculated submucosal fibroids, prematureovarian failure and pulmonary embolism.
Complications due to inadvertent embolization of non-target arteries include sexual dysfunction due to emboliza-tion of the cervical vaginal branch, damage to the rectum,bladder, buttocks, and sciatic nerve.
Technical failure in UAE can be defined as an inabilityto successfully catheterize and embolize both the right andthe left uterine arteries.
Two deaths have been reportededue to sepsis and multi-organ failure and pulmonary embolism.18,19
Finally, complications related to angiography are rareand include 0.2% hematoma, 0.2%e0.4% arterial throm-bosis, and 0.05% false aneurysm.5

Fig. 7 Sagittal T2W MR image of the pelvis showing a largeintramural fundal fibroid with bright signals within.
210 Apollo Medicine 2012 September; Vol. 9, No. 3 Amitha Vikrama and Chitra
FERTILITY FOLLOWING EMBOLIZATION
Although there is growing literature demonstrating that preg-nancy after UAE is possible, there is not sufficient evidencethat this treatment modality offers advantages over theconventional treatments. Whether UAE is safe for patientswho wish to retain future fertility is controversial. In fact,ACOG Committee Opinion from 2004 states: “.There isinsufficient evidence to ensure its (UAE) safety in womendesiring to retain their fertility, and pregnancy-relatedoutcomes remain understudied. The ACOG considers thisprocedure investigational or relatively contra-indicated inwomen wishing to retain fertility.”. Myomectomy remainsthe standard of care in patients who wish to retain theirfertility. UAE’s effect on fertility and pregnancy needs tobe studied further. Meanwhile, this technique should onlybe used in patients desiring to remain fertile for whom thereare no other feasible options.20
Several pregnancy complications have been reportedafter UAE. In one survey involving 50 published articleson successful pregnancies following UAE, these complica-tions were reported; malpresentations (17%), SGA (7%),cesarean section (56%), preterm delivery (28%), and post-partum hemorrhage (13%).21 The rates of abortions,preterm delivery, malpresentations and postpartum
hemorrhage are significantly higher in patients treatedwith UAE compared to myomectomy group.22
SUMMARY
Uterine artery embolization is a safe and effective treatmentfor haemorrhagic uterine disorders including fibroiddisease. It requires a shorter hospital stay with earlyresumption of normal activities. However, unlike hysterec-tomy, UAE is palliative rather than curative.
CONFLICTS OF INTEREST
All authors have none to declare.
REFERENCES
1. Franz F, Nicolai H, Robert LZ. Histologic features of uterineleiomyomata treated with microsphere embolization. ObstetGynecol. 2003;102:600602.
2. Goodwin SC, Vedantham S, McLucas B, et al. Preliminaryexperience with uterine artery embolization for uterinefibroids. J Vasc Interv Radiol. 1996;8:517e526.
3. Worthington-Kirsch RL, Popky GL, Hutchins FL. Uterinearterial embolization for the management of leiomyomas:quality-of life assessment and clinical response. Radiology.1998;208:625e629.
4. Bradley EA, Reidy JF, Forman RG, et al. Transcatheter uterineartery embolisation to treat large uterine fibroids. Br J ObstetGynaecol. 1998;105:235e240.
5. Ravina JH, Herbreteau D, Ciraru-Vigneron N. Arterial embo-lisation to treat uterine myomata. Lancet. 1995;346:671e672.
6. Hehenkamp WJ, Volkers NA, Birnie E, Reekers JA,Ankum WM. Symptomatic uterine fibroids: treatment withuterine artery embolization or hysterectomyeresults from therandomized clinical Embolisation versus Hysterectomy(EMMY) Trial. Radiology. Mar 2008;246(3):823e832.
7. Mara M, Maskova J, Fucikova Z, Kuzel D, Belsan T, Sosna O.Midterm clinical and first reproductive results of a randomizedcontrolled trial comparing uterine fibroid embolization andmyomectomy. Cardiovasc Intervent Radiol. JaneFeb2008;31(1):73e85.
8. Pelage JP, Le Dref O, Soyer P, et al. Fibroid related menor-rhagia: treatment with superselective embolization of theuterine arteries and mid-term follow up. Radiology.2000;215(2):428e431.
9. Greenberg MD, Kazamel TI. Medical and socioeconomicimpact of uterine fibroids. Obstet Gynecol Clin North Am.1995;22:625e636.

The role of uterine artery embolization Review Article 211
10. Gilbert L, Porter W, Brown VA. Postpartum haemorrhage:a continuing problem. Br J Obstet Gynecol. 1987;94:67e71.
11. Herbert WP, Afalo RC. Management of postpartum hemor-rhage. Clin Obstet Gynecol. 1984;27:139e145.
12. Pelage JP, Le Dref O, Mateo J, et al. Life-threatening primarypostpartum hemorrhage: treatment with emergency selectivearterial embolization. Radiology. 1998;208:359e362.
13. Zelop CM, Harlow BL, Frigoletto FD, Safon LE,Saltzman DH. Emergency periparturm hysterectomy. Am JObstet Gynecol. 1993;168:1443e1448.
14. Jha RC, Imaoka I, Ascher SM. MR imaging of uterineartery embolization for leiomyomas: morphological changesand features predictive of response [ab]. Radiology.1999;213(P):347e351.
15. Mizukami N, Yamashita Y, Matsukawa T. The value of MRimaging in predicting the treatment effect of arterial emboliza-tion therapy for uterine leiomyomas [ab]. Radiology.1999;213(P):348.
16. Bissler John J, Racadio John, Donnelly Lane F, et al. Reduc-tion of postembolization syndrome after ablation of renalangiomyolipoma. Am J Kidney Dis. May 2002;39(5):966e971.
17. Goodwin SC. New horizons in gynecologic embolotherapy:uterine artery embolization for the treatment of uterinefibroids. J Vasc Interv Radiol. 1998;9(1, Pt 2):53e59.
18. Lanocita R, Frigerio LF, Patelli G, et al. A Fatal Compli-cation of Percutaneous Transcatheter Embolization forTreatment of Uterine Fibroids. Abstract. Presented at the2nd International Symposium on Embolization of UterineMyomata. 11th International Conference of the Societyof Minimally Invasive Therapy/Center for InnovativeMinimally Invasive Therapy, Boston, MA, 16e18, Sep1999.
19. Vashisht A, Studd J, Carey A, Burn P. Fatal septicaemia afterfibroid embolisation. Lancet. 1999;354(9175):307e308.
20. Committee on Gynecologic Practice. American College ofObstetricians and Gynecologists. ACOG Committee Opinion:uterine artery embolization. Obstet Gynecol. 2004;103:403e404.
21. Goldberg J, Pereira L, Berghella V. Pregnancy after uterineartery embolization. Obstet Gynecol. 2002;100:869e872.
22. Goldberg J, Pereira L, Berghella V. Pregnancy outcomes aftertreatment of uterine fibromyomata: UAE vs laparoscopicmyomectomy. Am J Obstet Gynecol. 2004;191:18e22.

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/