the role of extracorporeal mechanical assists (ecls et al.) · the role of extracorporeal...
TRANSCRIPT

192 S. M. Ensminger T. Puehler, M. Benzinger, M. Morshuis, L. Kizner, J. F. Gummert
Abbreviations
ECMO Extracorporeal membrane oxygena-tion
MCS Mechanical circulatory support ARDS Adult respiratory distress syndromeECLS Extracorporeal life support
Introduction
After initially disappointing preclinical experi-ments and not particularly encouraging clini-cal results with extracorporeal circulation(ECC), John Gibbon’s pioneer work marksthe start for the development of ECC in thefield of heart surgery. Since 1953 the use ofthe heart-lung machine in cardiac surgery hasbeen steadily increased world-wide and is
Applied Cardiopulmonary Pathophysiology 16: 192-201, 2012
The role of extracorporeal mechanical assists (ECLS et al.)
Stephan M. Ensminger, Thomas Puehler, Michael Benzinger, Michiel Morshuis, Lukasz Kizner, Jan F. Gummert
Herz- und Diabetes-Zentrum NRW, Klinik für Thorax- und Kardiovaskularchirurgie, Univer-sitätsklinikum der Ruhr-Universität Bochum, Bad Oeynhausen, Germany
Abstract
Extracorporeal mechanical assist earlier named extracorporeal circulation (ECC)) has evolvedmarkedly over recent years. ECLS (extra corporeal life support) is employed for the manage-ment of life threatening heart or heart and lung failure, when no other treatment option is like-ly to be successful. Mostly it is instituted in an emergency or urgent situation after failure ofother treatment modalities. ECLS is used as temporary support, usually awaiting the recoveryof organs. It can also be used as a bridge to a more permanent supporting device or cardiactransplantation (bridge-to-decision-patient). ECLS is implanted in a veno-arterial configuration(either peripheral or central cannulation) for the treatment of heart failure. This is usually seenpost-cardiotomy, post-heart transplant and in severe cardiac failure due to almost any othercause (e.g. cardiomyopathy, myocarditis, acute coronary syndrome with cardiogenic shock). In contrast ECMO (extracorporeal membrane oxygenation) is used for respiratory failure andusually involves peripheral cannulation using the femoral veins +/- internal jugular vein if re-quired. The indications for ECMO are respiratory failure, most commonly due to adult respira-tory distress syndrome (ARDS), as a consequence of pneumonia, trauma or primary graft fail-ure following lung transplantation. ECLS is also used for neonatal and paediatric cardiac andrespiratory support. In this review, the technical aspects of ECLS and ECMO cannulation andthe different pump systems are outlined. In addition, indications, complication rates and out-comes are discussed.
Key words: extracorporeal mechanical assist, extracorporeal membrane oxygenation, mechan-ical circulatory support, heart failure, short term support

193The role of extracorporeal mechanical assists (ECLS et al.)
nowadays a standard requisite for moderncardiac surgery. However, during the earlyyears the limiting factor of its use was themassive trauma to the blood componentscaused by oxygenators and pumps includingsignificant hemolysis often followed by multiorgan failure even after a short running timeof less than one hour. Since that time ECChas been steadily improved and in 1971 Hillet al. succeeded in bridging a patient withposttraumatic lung failure for 72 hours withextracorporal membrane oxygenation by us-ing a venous/arterial system which was in-serted through the femoral artery andfemoral vein and this patient could beweaned successfully from ECC (1-4). Alreadyback in 1977 the first series of 28 patients(14 neonates/infants and 14 adults) withECLS-support was published by Bartlett et al.showing respectable results (5). The furtherdevelopment from bubble- to efficient mem-brane oxygenators, from roller- to centrifugal-pumps as well as the minimization of theECLS-systems led to an increased use and anextension of the indications for ECLS therapy.Since 1989 more than 40,000 ECLS and EC-MO implantations in over 170 centres havebeen registered and documented in the Reg-ister of the Extra Corporeal Life Support Or-ganization (6). Today ECLS and ECMO thera-py is used by numerous centers worldwideand adds to a steadily growing cooperationwith other medical departments.
Extracorporeal life support
Modern ECLS-systems have evolved fromminiaturized ECC-systems. The nomenclatureof extracorporeal life support is rather com-plex. ECMO support for lung failure usingveno-venous cannulation should be distin-guished from “extracorporeal life support”(ECLS) for cardiac failure, usually using a cen-trifugal pump combined with an oxygenator(7).
Left ventricular assistance(LVA) and extracorporeal lifesupport (ECLS)
In contrast to left ventricular assistance onlysupporting the patient’s heart ECLS systemscan also if necessary provide additional fulllung support and therefore an additional oxy-genator is integrated to the tube system.ECLS systems are always deployed in a veno-arterial configuration (either peripheral orcentral cannulation) for the treatment of car-diogenic shock. This is usually seen post-car-diotomy, post-heart transplant and in severecardiac failure due to almost any other cause(e.g. cardiomyopathy, myocarditis, acutecoronary syndrome with cardiogenic shock).
ECMO
Veno-venous ECMO is used for respiratoryfailure and usually involves peripheral cannu-lation using the femoral veins +/- internaljugular vein if required. The indications forveno-venous ECMO are respiratory failure,most commonly due to adult respiratory dis-tress syndrome (ARDS), pneumonia, traumaor primary graft failure following lung trans-plantation (8).
Access sites
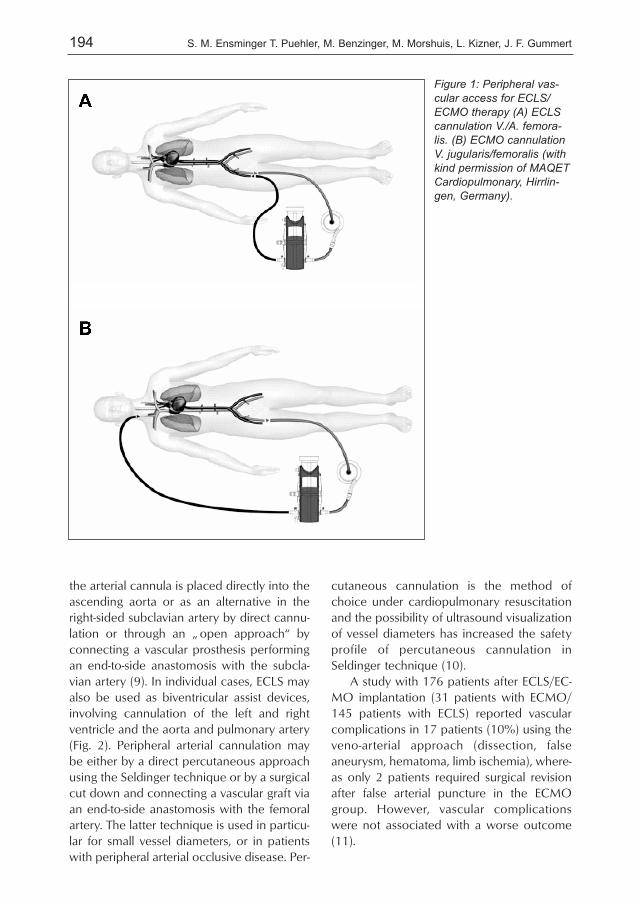
In general for ECLS as well as for ECMO pe-ripheral access is favorable because targetvessels are easy to reach. ECLS devices areused in a veno-arterial fashion (Fig 1 A)whereas ECMO is operated in a veno-ve-nous-fashion (Fig 1B). The venous cannula-tion in veno-venous ECMO is best carried outvia the jugular or the subclavian vein and thefemoral vein on the same site of the patient.For arterial cannulation in the ECLS setting, acentral cannulation is possible via the aortaor peripherally via the femoral arteries. Ingeneral, central cannulation is preferred incase of worse oxygenation combined withheart failure. Technically, after sternotomy
194 S. M. Ensminger T. Puehler, M. Benzinger, M. Morshuis, L. Kizner, J. F. Gummert
the arterial cannula is placed directly into theascending aorta or as an alternative in theright-sided subclavian artery by direct cannu-lation or through an „ open approach“ byconnecting a vascular prosthesis performingan end-to-side anastomosis with the subcla-vian artery (9). In individual cases, ECLS mayalso be used as biventricular assist devices,involving cannulation of the left and rightventricle and the aorta and pulmonary artery(Fig. 2). Peripheral arterial cannulation maybe either by a direct percutaneous approachusing the Seldinger technique or by a surgicalcut down and connecting a vascular graft viaan end-to-side anastomosis with the femoralartery. The latter technique is used in particu-lar for small vessel diameters, or in patientswith peripheral arterial occlusive disease. Per-
cutaneous cannulation is the method ofchoice under cardiopulmonary resuscitationand the possibility of ultrasound visualizationof vessel diameters has increased the safetyprofile of percutaneous cannulation inSeldinger technique (10).
A study with 176 patients after ECLS/EC-MO implantation (31 patients with ECMO/145 patients with ECLS) reported vascularcomplications in 17 patients (10%) using theveno-arterial approach (dissection, falseaneurysm, hematoma, limb ischemia), where-as only 2 patients required surgical revisionafter false arterial puncture in the ECMOgroup. However, vascular complicationswere not associated with a worse outcome(11).
Figure 1: Peripheral vas-cular access for ECLS/ECMO therapy (A) ECLScannulation V./A. femora-lis. (B) ECMO cannulationV. jugularis/femoralis (withkind permission of MAQETCardiopulmonary, Hirrlin-gen, Germany).

195The role of extracorporeal mechanical assists (ECLS et al.)
ECLS/ECMO systems
ECLS/ECMO systems include a driver consist-ing of a controller and a pump. There are dif-ferent types of pumps available on the mar-ket such as roller-, centrifugal and diagonal-pumps. The most frequently used systems arethe Rotaflow system (Maquet Car -diopulmonary, Hirrlingen, Germany) (Fig.3A), available since 1993, a centrifugal-pumpbased system Biomedicus (Medtronic Perfu -sion-Systems, Minneapolis, USA) (Fig. 3C)commercially available since 1973, und theCentriMag system (Levitronix, Zürich,Switzerland) (Fig. 3D) which was approved in2003. In addition the diagonal pumps Delta -stream DP1–DP3 (Medos MedizintechnikAG, Stolwerk, Germany) (Fig. 3B) receivedCE-mark in 2003. These modern powerfulsystems are able to warrant clinically requiredflow rates of 1–4 l/min at 1000 to approx.4000 RPM for several weeks and the respec-tive trauma of blood components has been
minimized in these systems (12). Table 1gives an overview of the technical details ofeach ECMO pump.
Oxygenators
Gas exchange is accomplished by pump driv-en blood flow and a passive oxygen and car-bon dioxide gradient through the micro -porous membranes of the oxygenator tubes.Membrane oxygenators have replaced theformerly used bubble oxygenators as theywarrant a more efficient and stable oxygena-tion of the blood. Membrane oxygenatorsconsist of capillaries with a microporous sur-face structure and gas exchange occurs bydiffusion. However, during long-term usageparticle deposition within the oxygenator oc-curs leading to a creeping „ plasma leakage“(Hydrophylisation). This process ultimately re-sults in insufficient gas exchange and oxy-genator failure. A recent development is the
Figure 2: CentriMag® (Levithronix, Zürich, Switzerland) for biventricular extracorporeal life support(A-D).

196 S. M. Ensminger T. Puehler, M. Benzinger, M. Morshuis, L. Kizner, J. F. Gummert
so-called diffusion-capillary-membrane-oxy-genator. These capillaries are covered withan extra thin layer of silicone or poly-methylpentene which ultimately prevents theloss of plasma components. Oxygentors de-signed in this way are characterised by in-creased durability and therefore of great im-portance for long term ECMO support (12).
Coating of the system/anticoagulation
The most important task of current ECLS/EC-MO therapy is to avoid device related com-plications such as thromboembolic events asa consequence of platelet activation by theartificial surface of the tubes of an ECLS/EC-MO system and bleeding events as a conse-quence of a ridged anticoagulation protocol.Therefore, most of the modern ECLS/ECMO-tubing-systems are coated with heparin, e.g.Rheoparin® (Medos Medizintechnik AG, Stol-
Figure 3: Overview of centrifugal and diogonal pumps: (A) Rotaflow® (Maquet Cardiopulmonary, Hirr-ligen, Germany), (B) DP-2 Deltastream ® (Medos Medizintechnik AG, Stolwerk, Germany), (C) Bio-medicus BP 45 ® (Medtronic, USA), (D) CentriMag ® (Levithronix, Zürich, Switzerland).
Table 1: Technical aspects of the diagonal and centrifugal ECMO pumps (modified from Schmid, CTextbook of Extracorporeal Circulation)
Rotation
(U/min)
Blood flow
(l/min)
Pressure
(mmHg)
Pump
bearing
Coating
Centrifugal pumps
Biomedicus 540,
550 (Medtronic)
0-4.500 0-9.9 0-999 mechanical Carmedia
CentriMag
(Levitronix)
1.500-5.500 0-9.9 0-600 magnetical without
Rotaflow (Maquet) 0-5000 0-9.9 0-750 magnetical Bioline
Diagonal pumps
Deltastream-Pump-
2-3 (DP2-3)
(Medos)
100-10.000 0-8.0 0-600 mechanical Rheoparin

197The role of extracorporeal mechanical assists (ECLS et al.)
werk, Germany) or Bioline® (Maquet Car-diopulmonary, Hirrlingen, Germany) or usephosphorylcholin-coating (Sorin, Milano,Italy) to minimise the contact between bloodcomponents – in particular platelets – andthe artificial surface of the tubes. This resultsin reduced immunological activation of therespective blood components, which in turnenables to reduce the systemic anticoagula-tion with and also tolerate a PTT of about 50-60s (13,14). In particular during the use ofthe interventional lung assist a prospectivestudy was able to show that additional appli-cation of 1.5 mg/kg bodyweight acetylsali-cylic acid (ASS) resulted in improved gas ex-change and longevity of the oxygenators(15,16).
Commercially available ECLS/ECMO-systems
Nowadays there are several CE-certifiedECLS/ECMO-systems commercially availableand approved for in patient use up to 30days. ECLS/ECMO systems such as the Car-diohelp® (Maquet Cardiopulmonary, Hirrlin-gen, Germany) (Fig. 4 A,B), the LifeBridgeB2T® (Lifebridge Medizintechnik AG, Ampf-ing, Germany; Fig. 4C) and the CentriMag®
Left ventricular assist system (LVAS) (Levit-ronix GmbH, Zürich, Switzerland; Fig. 4D)and the Medos-Deltastream-System (MedosMedizintechnik AG, Stolwerk, Germany) are
very well suitable for the use directly at thepatient’s bed. As these systems are rathersmall and have a compact configuration theyare also the device of choice for inter-hospi-tal patient transport by ambulance or heli-copter (17-19). ECLS/ECMO therapy is nowa-days more and more frequently used for thetransport and stabilisation of cardiorespirato-ry unstable patients giving them a chance torelocate in highly specialized centers and torecover with acceptable results. Transporttimes of up to 3 h are described so far(20,21). Furthermore, ECLS/ECMO therapyhas found its place after inhalation and blasttrauma in soldiers from battle zones enablingtheir rescue by plane or helicopter trans-portation (23).
Indications
Although there are nowadays recommenda-tions for the implantation and use ofECLS/ECMO (23), in numerous cases an indi-cation for implantation of an ECLS/ECMOsystem has to be decided on an individual pa-tient base with regard to comorbidities, pa-tient age and the duration of mechanical re-suscitation. Nowadays, this is more or lessthe question to identify a bridge-to-decisionpatient and our strategy is not the conceptthat a long term and permanent deviceshould always be placed in an emergent situ-ation. The bridge-to-decision patient has typ-
Figure 4: Cardiohelp® in use for ECLS helicopter inter-hospital transfer (A) and as ECLS on an inten-sive care unit (B). Lifebridge B2T® system (C) and CentriMag® ECLS for postcardiotomy syndromeon an intensive care unit (D)
198 S. M. Ensminger T. Puehler, M. Benzinger, M. Morshuis, L. Kizner, J. F. Gummert
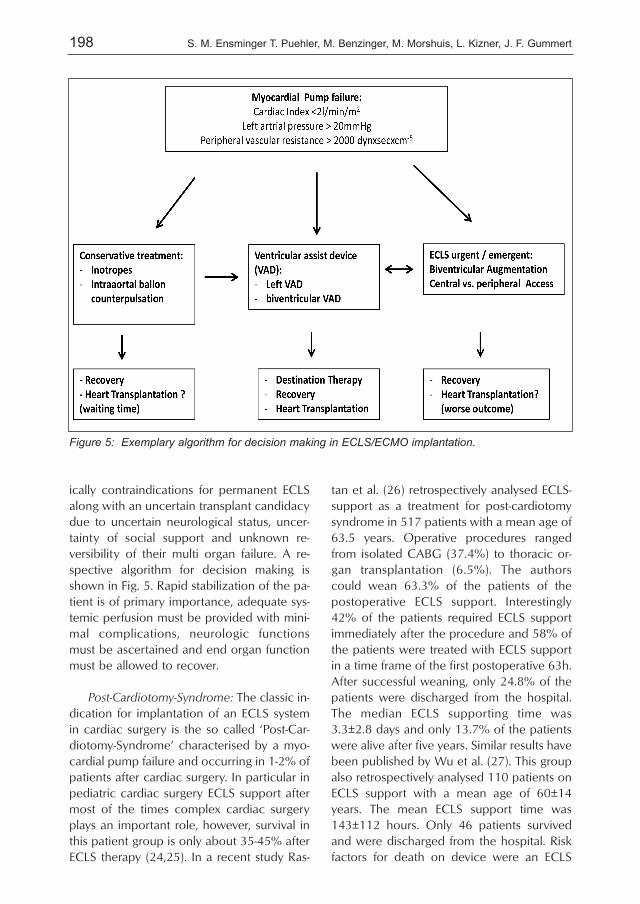
ically contraindications for permanent ECLSalong with an uncertain transplant candidacydue to uncertain neurological status, uncer-tainty of social support and unknown re-versibility of their multi organ failure. A re-spective algorithm for decision making isshown in Fig. 5. Rapid stabilization of the pa-tient is of primary importance, adequate sys-temic perfusion must be provided with mini-mal complications, neurologic functionsmust be ascertained and end organ functionmust be allowed to recover.
Post-Cardiotomy-Syndrome: The classic in-dication for implantation of an ECLS systemin cardiac surgery is the so called ‘Post-Car-diotomy-Syndrome’ characterised by a myo -cardial pump failure and occurring in 1-2% ofpatients after cardiac surgery. In particular inpediatric cardiac surgery ECLS support aftermost of the times complex cardiac surgeryplays an important role, however, survival inthis patient group is only about 35-45% afterECLS therapy (24,25). In a recent study Ras-
tan et al. (26) retrospectively analysed ECLS-support as a treatment for post-cardiotomysyndrome in 517 patients with a mean age of63.5 years. Operative procedures rangedfrom isolated CABG (37.4%) to thoracic or-gan transplantation (6.5%). The authorscould wean 63.3% of the patients of thepostoperative ECLS support. Interestingly42% of the patients required ECLS supportimmediately after the procedure and 58% ofthe patients were treated with ECLS supportin a time frame of the first postoperative 63h.After successful weaning, only 24.8% of thepatients were discharged from the hospital.The median ECLS supporting time was3.3±2.8 days and only 13.7% of the patientswere alive after five years. Similar results havebeen published by Wu et al. (27). This groupalso retrospectively analysed 110 patients onECLS support with a mean age of 60±14years. The mean ECLS support time was143±112 hours. Only 46 patients survivedand were discharged from the hospital. Riskfactors for death on device were an ECLS
Figure 5: Exemplary algorithm for decision making in ECLS/ECMO implantation.

199The role of extracorporeal mechanical assists (ECLS et al.)
supporting time >110 h, a patient age >60years and a serum billirubin concentrationabove 103 µmol/l (>6 mg/dl) (28).
Temporary right heart failure: A further in-dication for short term ECLS support is thetreatment of temporary right heart failurewith respiratory failure after LVAD implanta-tion. The cannules are usually placed in theright femoral vein and the pulmonary artery.If a subcutaneous Dacron conduit connectedto the pulmonary artery is used, this systemcan be weaned and explanted without re-opening of the chest (29).
Prolonged resuscitation: Experiences withECLS support during cardiopulmonary resus-citation are limited to small patient numbers.In particular in children and young adults itsuse is encouraged in the sense of a last op-tion therapy or also called ‘bridge to deci-sion’ therapy until results of further diagnos-tics are available and additional therapeuticoptions can be evaluated (30,31). Examplesinclude drowning accidents, polytrauma, in-toxications and myocardial infarctions withsubsequent cardiogenic shock. Data aboutthe use of a ECLS during cardiopulmonary re-suscitation from the ELSO-Register revealedthat only 27% of the treated patients were fi-nally discharged from the hospital. Braindeath occurred in 28% of the patients whodid not survive and risk factors for deathwere low oxygen partial pressure (paO2),low blood pressure during resuscitation andthe use of hemofiltration during ECLS (28).
Terminal heart failure: During terminalheart failure the following parameters havebeen suggested to help in decision makingwhich patient to support: a cardiac index (CI)<2.0l/min/m2, a capillary wedge-pressure of>20 mmHg and a systolic blood pressure <90mmHg. However, as terminal heart failureusually develops over a certain amount oftime and therefore permanent support andtransplantation play a more important rolethan short term ECLS. In this context – if at all– the ECLS is mainly used as a Bridge-to-
Bridge or rarely as a Bridge-to-Transplantationor permanent support (32,33). In addition,experimental data show that ECLS supportdoes not warrant a completely volume un-loaded left ventricle and wall tension caneven increase (34). Moreover, there are onlyvery few reports about mid and longer termECLS with immobilization of the patient be-ing the major problem (35).
Future perspective
During recent years ECLS/ECMO therapy hasevolved in smaller and more powerful de-vices made increasingly user-friendly. The useof ECLS/ECMO systems during recent yearsexpanded into a variety of disciplines includ-ing cardiac surgery, anesthesia and cardiolo-gy requiring an interdisciplinary treatment ap-proach for these patients aiming for better re-sults. In Germany this led to the formation ofa Working Group for extracorporeal circula-tion in cardiac surgery trying to establishguidelines (36). In addition increasingly bio-compatibilized oxygenators and furtherminiaturization of ECLS/ECMO systems willplay a crucial role for long term ECLS/ECMOsupport. As a consequence of ever increasingnumbers of complex coronary interventionsor catheter based valve replacements in pe-ripheral cardiac catheterization laboratoriescomplications can occur and a prolongeduse of ECLS/ECMO support or prolonged re-suscitation may be a challenge. Especially inthis patient cohort outcomes should be thor-oughly looked at and analysed.
Conclusion
The ECMO is an established therapy optionin severe global respiratory failure to enablelung protective ventilation. Thereby, the sur-vival of these patients has improved by EC-MO therapy.
The ECLS is used in the context of globalcardiopulmonary failure. In particular duringresuscitation, a fast access through the
200 S. M. Ensminger T. Puehler, M. Benzinger, M. Morshuis, L. Kizner, J. F. Gummert
femoral vessels is guaranteed in most of thepatients. In addition, further miniaturizationof ECLS components and new antithrombot-ic surface coatings will result in even moreflexibility of the systems and a reduction ofcomplication rates.
References
1. Gibbon JH. Application of a mechanical heartand lung apparatus to cardiac surgery. MinnMed 1954; 37: 171-185
2. Stoney WS. Evolution of cardiopulmonary by-pass. Circulation 2009; 119 (21): 2844-53
3. Bartlett RH, Fong SW, Burns NE, GazzanigaAB. Prolonged partial venoarterial bypass:physiologic, biochemical, and hematologic re-sponses. Ann Surg. 1974; 180 (6): 850-6
4. Hill JD, O’Brien TG, Murray JJ, Dontigny L,Bramson ML, Osborn JJ, Gerbode F. Pro-longed extracorporeal oxygenation for acutepost-traumatic respiratory failure (shock-lungsyndrome). Use of the Bramson membranelung. N Engl J Med 1972; 286 (12): 629-34
5. Bartlett RH, Gazzaniga AB, Fong SW, JefferiesMR, Roohk HV, Haiduc N. Extracorporealmembrane oxygenator support for cardiopul-monary failure. Experience in 28 cases. J Tho-rac Cardiovasc Surg 1977; 73 (3): 375-86.
6. http://www.elso.med.umich.edu/7. Bartlett RH. Extracorporeal life support: history
and new directions. ASAIO J 2005; 51 (5):487-9
8. Marasco SF, Lukas G, McDonald M, McMillanJ, Ihle B. Review of ECMO (extra corporealmembrane oxygenation) support in critically illadult patients. Heart Lung Circ 2008; 17 Sup-pl 4: S41-7
9. Navia JL, Atik FA, Beyer EA, Ruda Vega P. Ex-tracorporeal membrane oxygenation withright axillary artery perfusion. Ann ThoracSurg. 2005; 79 (6): 2163-5
10. Ganslmeier P, Philipp A, Rupprecht L, Diez C,Arlt M, Mueller T, Pfister K, Hilker M, SchmidC. Percutaneous cannulation for extracorpore-al life support. Thorac Cardiovasc Surg 2011;59 (2): 103-7
11. Bisdas T, Beutel G, Warnecke G, Hoeper MM,Kuehn C, Haverich A, Teebken OE. VascularComplications in Patients Undergoing FemoralCannulation for Extracorporeal MembraneOxygenation Support. Ann Thorac Surg 2011
12. Toomasian JM, Bartlett RH. Hemolysis and EC-MO pumps in the 21st Century. Perfusion2011; 26 (1): 5-6
13. Schmid C, Philipp A. Leitfaden der Extrakorpo-ralen Zirkulation. Heidelberg: Springer Medi-zin Verlag
14. Oliver WC. Anticoagulation and coagulationmanagement for ECMO. Semin CardiothoracVasc Anesth 2009; 13 (3): 154-75
15. Müller T, Philipp A, Luchner A, KaragiannidisC, Bein T, Hilker M, Rupprecht L, LanggartnerJ, Zimmermann M, Arlt M, Wenger J, SchmidC, Riegger GA, Pfeifer M, Lubnow M. A newminiaturized system for extracorporeal mem-brane oxygenation in adult respiratory failure.Crit Care 2009; 13 (6): R205
16. Bein T, Zimmermann M, Philipp A, RammingM, Sinner B, Schmid C, Müller T, Graf B, SchlittHJ, Weber-Carstens S. Addition of acetylsali-cylic acid to heparin for anticoagulation man-agement during pumpless extracorporeal lungassist. ASAIO J 2011; 57 (3): 164-8
17. Mehlhorn U, Brieske M, Fischer U, Ferrari M,Brass P, Fischer JH, Zerkowski HR. LIFEBRIDGEB2T® – A Portable, Modular, Rapidly Available„ Plug-and-Play“ Mechanical Circulatory Sup-port System“. Ann Thorac Surg 2005; 80: 187-192.
18. Maunz O, Horisberger J, von Segesser L.Bridge to life: the Lifebridge B2T extracorpore-al life support system in an in vitro trial. Perfu-sion 2008; 23: 279-82
19. Berdajs D, Born F, Crosset M, Horisberger J,Künzli A, Ferrari E, Tozzi P, von Segesser LK.Superior venous drainage in the „ LifeBox“: aportable extracorporeal oxygenator with a self-expanding venous cannula. Perfusion 2010;25 (4): 211-5
20. Philipp A, Arlt M, Amann M, Lunz D, Müller T,Hilker M, Graf B, Schmid C. First experiencewith the ultra compact mobile extracorporealmembrane oxygenation system Cardiohelp ininterhospital transport. Interact CardiovascThorac Surg 2011
21. Haneya A, Philipp A, Foltan M, Mueller T,Camboni D, Rupprecht L, Puehler T, Hirt S,Hilker M, Kobuch R, Schmid C, Arlt M. Extra-corporeal circulatory systems in the interhospi-tal transfer of critically ill patients: Experienceof a single institution. Ann Saudi Med 2009;29: 110-4
22. Zimmermann M, Philipp A, Schmid FX, DorlacW, Arlt M, Bein T. From Baghdad to Germany:use of a new pumpless extracorporeal lung as-
201The role of extracorporeal mechanical assists (ECLS et al.)
sist system in two severely injured US soldiers.ASAIO J 2007; 53 (3): 4-6
23. Peek GJ, Mugford M, Tiruvoipati R, Wilson A,Allen E, Thalanany MM, Hibbert CL, TruesdaleA, Clemens F, Cooper N, Firmin RK, ElbourneD; CESAR trial collaboration. Efficacy and eco-nomic assessment of conventional ventilatorysupport versus extracorporeal membrane oxy-genation for severe adult respiratory failure(CESAR): a multicentre randomised controlledtrial. Lancet 2009; 374 (9698): 1351-63. Epub2009 Sep 15
24. Rhodes JF, Blaufox AD, Seiden HS, Asnes JD,Gross RP, Rhodes JP, Griepp RB, Rossi AF. Car-diac arrest in infants after congenital heart sur-gery. Circulation 1999; 100 (19 Suppl): II194-9
25. Thourani VH, Kirshbom PM, Kanter KR, SimsicJ, Kogon BE, Wagoner S, Dykes F, FortenberryJ, Forbess JM. Venoarterial extracorporealmembrane oxygenation (VA-ECMO) in pedi-atric cardiac support. Ann Thorac Surg 2006;82 (1): 138-44
26. Rastan AJ, Dege A, Mohr M, Doll N, Falk V,Walther T, Mohr FW. Early and late outcomesof 517 consecutive adult patients treated withextracorporeal membrane oxygenation for re-fractory postcardiotomy cardiogenic shock. JThorac Cardiovasc Surg 2010; 139 (2): 302-11
27. Wu MY, Lin PJ, Lee MY, Tsai FC, Chu JJ, ChangYS, Haung YK, Liu KS. Using extracorporeal lifesupport to resuscitate adult postcardiotomycardiogenic shock: treatment strategies andpredictors of short-term and mid-term survival.Resuscitation 2010; 81 (9): 1111-6
28. Hagiwara S, Yamada T, Furukawa K, Ishihara K,Nakamura T, Ohyama Y, Tamura J, Oshima K.Survival after 385min of cardiopulmonary re-suscitation with extracorporeal membraneoxygenation and rewarming with haemodialy-sis for hypothermic cardiac arrest. Resuscita-tion 2011; 29
29. Strauch JT, Franke UF, Madershahian N,Wahlers T. Right ventricular assist device im-plantation — a new transcutaneous approach.Thorac Cardiovasc Surg 2004; 52 (6): 378-9
30. Arlt M, Philipp A, Voelkel S, Camboni D, Rup-precht L, Graf BM, Schmid C, Hilker M. Hand-held minimised extracorporeal membrane oxy-genation: a new bridge to recovery in patientswith out-of-centre cardiogenic shock. Eur J Car-diothorac Surg 2011; 22
31. Thiagarajan RR, Brogan TV, Scheurer MA,Laussen PC, Rycus PT, Bratton SL. Extracorpo-real membrane oxygenation to support car-
diopulmonary resuscitation in adults. Ann Tho-rac Surg 2009; 87 (3): 778-85
32. Fitzgerald D, Ging A, Burton N, Desai S, ElliottT, Edwards L. The use of percutaneous ECMOsupport as a ‘bridge to bridge’ in heart failurepatients: a case report. Perfusion 2010; 25 (5):321-5, 327
33. Pagani FD, Lynch W, Swaniker F, Dyke DB,Bartlett R, Koelling T, Moscucci M, Deeb GM,Bolling S, Monaghan H, Aaronson KD. Extra-corporeal life support to left ventricular assistdevice bridge to heart transplant: A strategy tooptimize survival and resource utilization. Cir-culation 1999; 100 (19 Suppl): II206-10
34. Bavaria JE, Ratcliffe MB, Gupta KB, WengerRK, Bogen DK, Edmunds LH Jr. Changes in leftventricular systolic wall stress during biventric-ular circulatory assistance. Ann Thorac Surg1988; 45 (5): 526-32
35. Camboni D, Philipp A, Hirt S, Schmid C. Possi-bilities and limitations of a miniaturized long-term extracorporeal life support system asbridge to transplantation in a case with biven-tricular heart failure. Interact Cardiovasc Tho-rac Surg 2009; 8 (1): 168-70
36. Feindt P, Benk C, Boeken U, Bauer A,Mehlhorn U, Gehron J, Markewitz A, Beck-mann A, Beyersdorf F. Use of extracorporealcirculation (ECC) outside the cardiac operatingroom: indications, requirements and recom-mendations for routine practice. Thorac Car-diovasc Surg 2011; 59 (2): 66-8
Correspondence addressProf. Stephan Ensminger, M.A. D.Phil.Klinik für Thorax- und KardiovaskularchirurgieUniversitätsklinikum der Ruhr-Universität BochumGeorgstr. 1132545 Bad OeynhausenGermany [email protected]