the role of exercise in spinal muscular atrophy - … role of exercise in spinal muscular atrophy...
TRANSCRIPT

The Role of Exercise in Spinal Muscular Atrophy
2016 Spinal Muscular Atrophy (SMA) Symposium on Optimizing Care Philadelphia, Pennsylvania
September 30 – October 1, 2016
Jacqueline Montes, PT, EdD, NCS Assistant Professor of Clinical Rehabilitation and
Regenerative Medicine (Physical Therapy) in Neurology SMA Clinical Research Center, Columbia University
PNCR Networkfor SMA

Disclosures
Receives support from Eunice Kennedy Shriver National Institute for Child Health and Human Development (NICHD) 1K01HD084690-01A1 Consultant for Ionis Pharmaceuticals Served on advisory boards for Biogen and Roche Pharmaceuticals

Exercise Topics • Function: Walking, mobility, transfers and balance training • Aerobic exercise
• Walking (treadmill or over ground) • Stationary bicycle / Elliptical machines • Aquatics
• Range of motion exercises: • Active range of motion • Strengthening (concentric, eccentric, isometric) • Passive range of motion • Stretching
No definitive recommendations for exercise in current standard of care. (Wang 2007)

218thth ENMC International Workshop: “Eight years on, revisiting the Consensus Statement of Care in SMA” February 19 -21, 2016
1. Diagnosis and genetics 2. Nutrition, Growth and Bone Health 3. Pulmonary 4. Orthopedic 5. Physical Therapy and Rehabilitation 6. Other organ system involvement 7. Acute care in the hospital setting 8. Ethics and palliative care
Consensus Approach: 1. Literature Review 2. Expert Clinicans, Patient and Pharma Involvement 3. Delphi Technique (2 rounds) 4. Additonal Survey
NORTH AMERICA Jacqueline Montesa
Kristin Krosschell* Allan Glanzman* Richard Gee* Leslie Nelson EUROPE Marion Maina* Elena Mazzonea
Anna-Karin Kroksmark Carole Vuillerot Caron Coleman Agnieszka Stępień APAC Kristy Rose
a Workshop leaders * Participated in original SOC initiative in 2007

Literature Review Summary 54 Articles Identifed
Topic, Study Type, Population, Summary of Findings, Level of Evidence (AAN Classification), Evidence Quality (AAP Classification)
• Contractures and Scoliosis – 10 articles • Function – 17 articles • Hip Dislocation/Subluxation – 3 articles • Intervention - 12 articles • Pain – 1 article • Review – 5 articles (hip subluxation, contractures, scoliosis, care recommendations) • Falls – 1 article • Fatigue – 5 articles
SEARCH TERMS: Spinal Muscular Atrophy, Rehabilitation, Physical Therapy, Occupational Therapy, Exercise

SMA Topic, Level of Evidence and Recommendation
INTERVENTIONS Exercise Topics Aggregate
Evidence Quality Expert Opinion Consensus
Degree of Impact
Recommendations
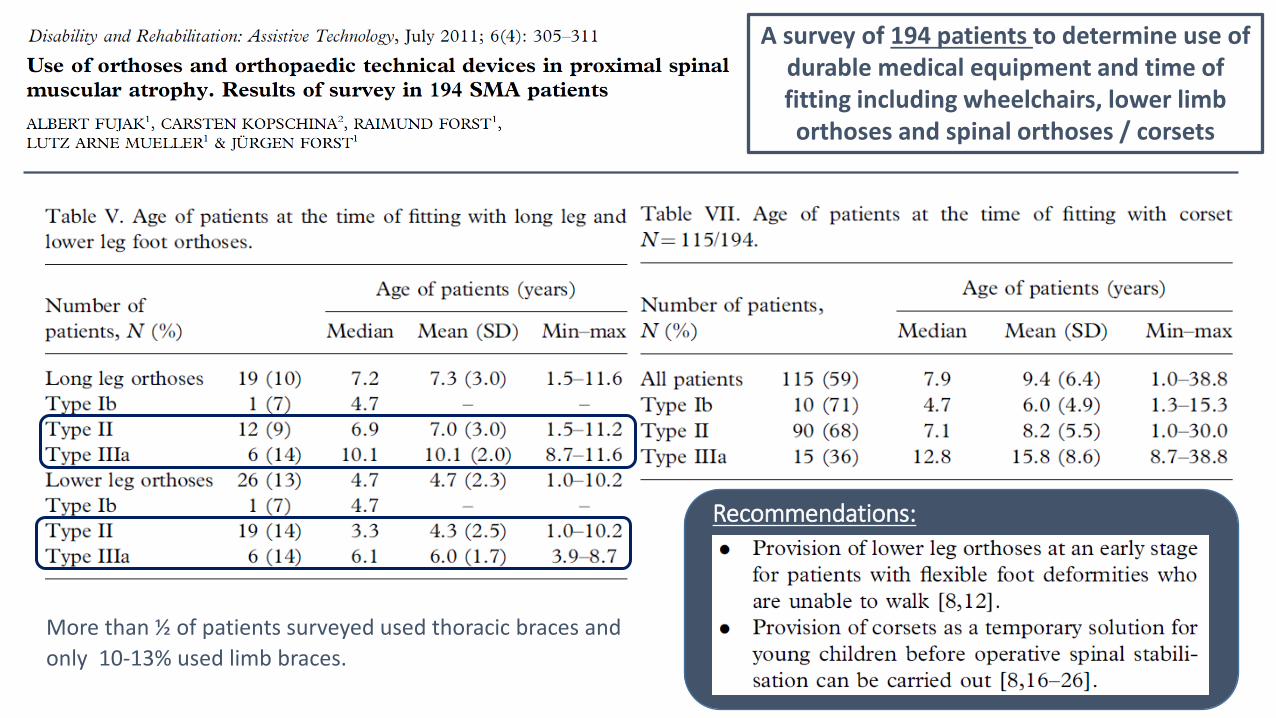
Bracing (sitters) Granata et al. 1987; Fujak et al. 2011
C, C (case series and survey)
Very Strong High No progression of weakness or contractures with early fitting of knee-ankle-foot orthoses.
More than ½ of patients surveyed used thoracic braces and only 10-13% used limb braces.
Aquatic therapy (sitters/walkers) Cunha et al. 1996 Aquatic therapy (walkers) Salem et al. 2010
C (prospective 2 year study) D
Very Strong Very Strong
Mid High
Aquatic therapy may improve daily activities.
Aquatic therapy may improve strength, function and ADLs.
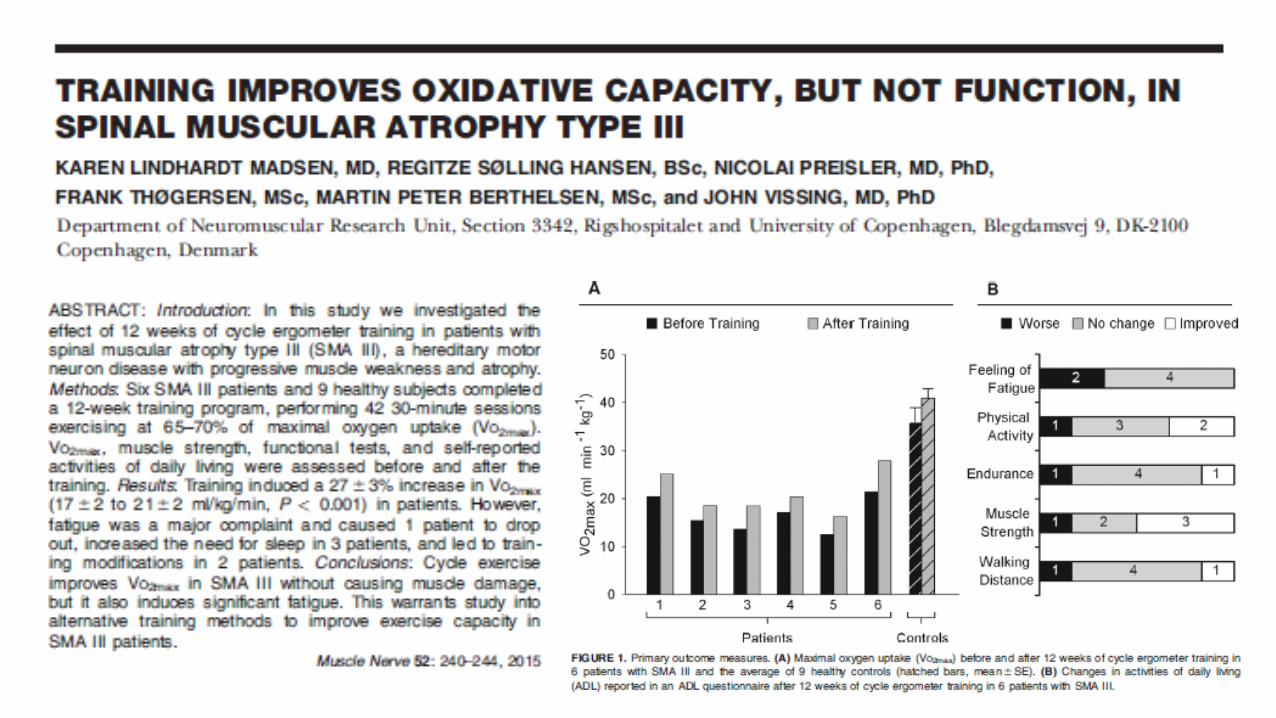
Exercise (sitters) Lewelt et al. 2015; Hartley et al.2013 Exercise (walkers) Montes et al; Lindhardt et al; Lewelt et al. 2015; Hartley et al. 2013
C, D (prospective uncontrolled study and survey) A, B, C, D (4 studies)
Very Strong Very Strong
Mid High
Strengthening is not harmful and has psychosocial benefits.
Strengthening and aerobic conditioning is not harmful, does not improve function, and improves VO2 max and has psychosocial benefits.
Level A = Well designed, randomized, controlled trials Level B = Trials with minor limitations otherwise well designed Level C = Single or few observational studies or multiple studies with inconsistent findings or major limitations Level D -= Expert opinion or case reports Level X = Exceptional situations where validating studies are not possible
Recommendations:
A survey of 194 patients to determine use of durable medical equipment and time of fitting including wheelchairs, lower limb orthoses and spinal orthoses / corsets
More than ½ of patients surveyed used thoracic braces and only 10-13% used limb braces.
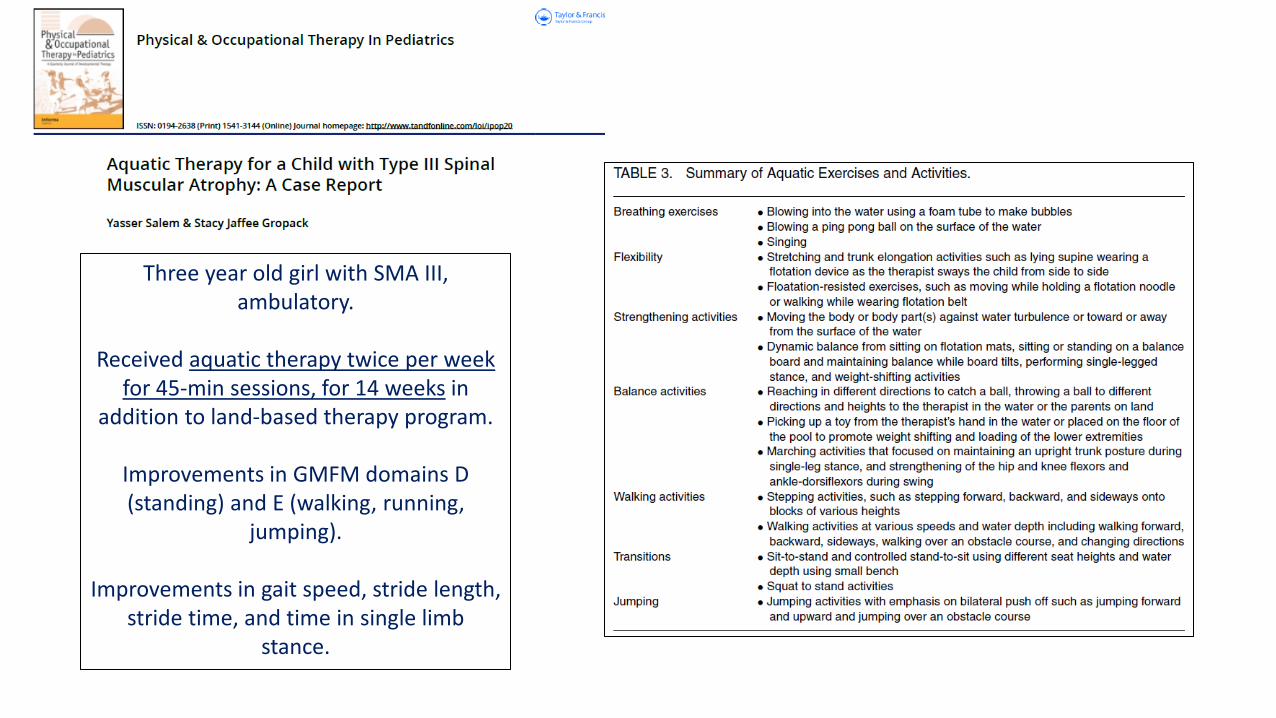
Three year old girl with SMA III, ambulatory.
Received aquatic therapy twice per week
for 45-min sessions, for 14 weeks in addition to land-based therapy program.
Improvements in GMFM domains D (standing) and E (walking, running,
jumping).
Improvements in gait speed, stride length, stride time, and time in single limb
stance.

12--week, supervised, home-based,3 day/week progressive resistance training exercise program.
Well tolerated (no adverse events), safe, and
feasible.

In all participants, there was an improvement in VO2 max with 6
months of exercise.
Percent-predicted VO2 max improved 4.9% in all participants.
Even greater changes (6.6%) were seen in the most compliant participants.
It took nearly 6 months for most patients to achieve the target exercise intensity of
150 minutes / week of aerobic exercise

• 30 participants 11 with SMA
• Power chair soccer teams in children and adults ages 7 -63 years
• Assessed Perceived Exertion (Borg) and volume of oxygen consumption (METs) at rest and during exercise

Table 1c: Topics identified to be important interventions by SMA type and ranked in order of importance.
Rank Interventions Non-Sitters Sitters Walkers More Important
Stretching/ ROM Stretching/ ROM Exercise
Seating Systems / Postural and Positioning Supports
Wheelchairs Transfer and Mobility Training
Play / Toys Play / Toys* Stretching / ROM
Education Bracing Aquatic Therapy
Assistive Technology/ Adaptive Equipment
Seating Systems / Postural and Positioning Supports*
Balance Exercises
Bracing Standers Bracing
Wheelchairs Transfer and Mobility Training
Fatigue Management*
Chest Physical Therapy* Mobile Arm Supports
ADL Management*
Transfer and Mobility Training
Aquatic Therapy Ambulation Devices*
Mobile Arm Supports
Exercise
Less Important
Aquatic Therapy
* Topics with strong agreement but less than the other topics identified.
Exercise topics, including range of motion exercises, were thought to be very
important by an international group of experts for all SMA types.
*******
Revised Consensus Statement for Standards of Care in SMA (2016)
Results from the Delphi Survey Round 2

Exercise Prescription
• Exactly how much exercise is beneficial is still not clear.
• Research to date in both the animal and human models seems to point towards moderate intensity, low resistance exercise as the least harmful and marginally beneficial.

Revised Consensus Statement for Standards of Care in SMA (2016) (in preparation) Stretching and range of motion is applied to maintain joint mobility, prevent or manage contractures, promote function and maintain flexibility. Modalities: orthoses, splints, and aids for supported standing/standing frames, and active-assistive stretching, and positioning techniques such as serial casting. Session duration: For passive stretching and range of motion: * if the aim is to improve length, the stretch needs to be sustained for much longer than 60 minutes. * if the aim is to maintain length, then less time is required however, for stretching to be effective, the end range should be held for at least 30 seconds. Frequency: Stretching and range of motion should be performed during day and/or night time with a minimum frequency of 3-5 times per week and an optimal treatment frequency of 5 times a week to daily.

Bracing: Thoracic bracing is recommended for posture and to promote function. Cervical bracing is used for upright posture or head support. Upper and lower limb orthoses are used to promote function and range of motion. Session duration: To be effective for maintaining and promoting range of motion, orthoses should be applied for more than 60 minutes to overnight. Frequency: The minimum frequency for bracing to be effective is 5 times per week while daily bracing is optimal for sitters. Supported standing: To facilitate lower extremity stretching, promote bone health, enable upright participation, and trunk posture in those with sufficient lower extremity range of motion. Session duration: Optimal standing should be up to 60 minutes. Frequency: Supported standing should be performed 3 – 5 times per week at a minimum while the optimal frequency of supported standing is 5 – 7 times per week.
Revised Consensus Statement for Standards of Care in SMA (2016) (in preparation)

Exercise programs should be encouraged and incorporated into activities of daily living and through age appropriate activities. Strengthening exercise should include concentric and eccentric exercise with and without resistance for proximal, distal, core, and axial, and muscles with at least antigravity strength. For cervical muscles and those with a Medical Research Council Scale (MRC) score less than 3 resistance is not recommended. For muscles with an MRC score less than 3 eccentric exercise is also not widely recommended. Aerobic exercise is recommended and options include: swimming, game-based activities (ie. Wii, Kinect), hippotherapy, upper and or lower extremity ergometry, walking, yoga / pilates, and wheelchair sports. Session duration: The goal for optimal duration for individual bouts of aerobic exercise should be at least 30 minutes. Frequency: The minimal frequency should be 2-3 times per week while the optimal should be 3-5 times per week.
Revised Consensus Statement for Standards of Care in SMA (2016) (in preparation)
Acknowledgments
Darryl C. De Vivo Basil T. Darras Richard Finkel John W. Day Gihan I. Tennekoon Michael McDermott
PNCR Networkfor SMA
Revisiting the consensus statement for standards of care in SMA
Leadership: Richard Finkel, Eugenio Mercuri,
Thomas Sejersen
PT Working Group: Caron Coleman, Richard Gee, Allan Glanzman, Anna-Karin Kroksmark, Kristin Krosschell, Leslie Nelson, Marion Main, Elena
Mazzone, Jacqueline Montes, Kristy Rose, Agnieszka Stępień, Carole Vuillerot
Ying Qian, statistical support
SMA Clinical Research Center