the role of early detection in improving … · chief of breast center at hospital moinhos de vento...
TRANSCRIPT

THE ROLE OF EARLY DETECTION IN IMPROVING TREATMENT OUTCOMES FOR BREAST CANCER PATIENTS IN LMICS IMPACT OF TWO INDEPENDENT STRATEGIES TO PROMOTE DOWNSTAGING IN BRAZIL
MAIRA CALEFFI, MD, PH.D CHIEF OF BREAST CENTER AT HOSPITAL MOINHOS DE VENTO
PORTO ALEGRE, BRAZIL
VOLUNTEER PRESIDENT OF FEMAMA
UICC BOARD MEMBER

STRATEGY 1
Núcleo Mama Porto Alegre (NMPA) u A Private Public Partnership with the support of a IMAMA NGO;
u 9,218 women above 15 years-old from a specific area in Porto Alegre;
u Accrual from March 2004 to March 2006;
u Asymptomatic 40-69 years-old women entered the annual clinical examination and mammographic screening cohort;
u Women out of this age range did their routine exams in the primary health care facilities. In case of any breast complaint, they were referred immediately to NMPA.


7 DAYS
ZERO
14 DAYS
21 DAYS
35 DAYS
NMPA
MMG
BIOPSY
SURGERY
CHEMO
PHCF
PATIENT’S JOURNEY
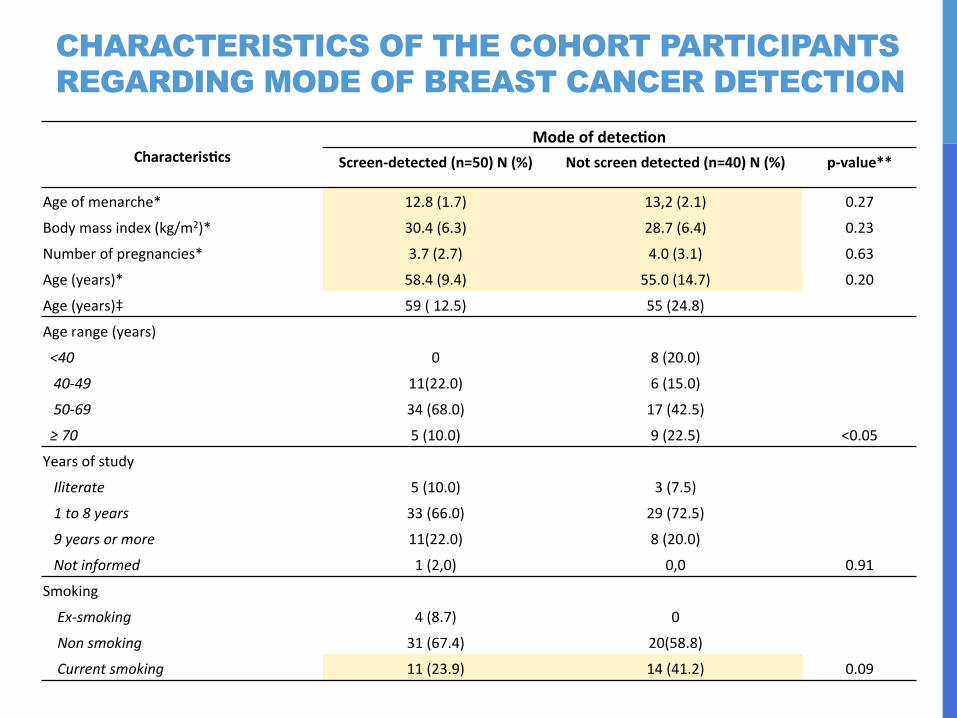
CHARACTERISTICS OF THE COHORT PARTICIPANTS REGARDING MODE OF BREAST CANCER DETECTION
Characteris*cs Mode of detec*on
Screen-‐detected (n=50) N (%) Not screen detected (n=40) N (%) p-‐value**
Age of menarche* 12.8 (1.7) 13,2 (2.1) 0.27
Body mass index (kg/m2)* 30.4 (6.3) 28.7 (6.4) 0.23
Number of pregnancies* 3.7 (2.7) 4.0 (3.1) 0.63
Age (years)* 58.4 (9.4) 55.0 (14.7) 0.20
Age (years)‡ 59 ( 12.5) 55 (24.8)
Age range (years)
<40 0 8 (20.0)
40-‐49 11(22.0) 6 (15.0)
50-‐69 34 (68.0) 17 (42.5)
≥ 70 5 (10.0) 9 (22.5) <0.05
Years of study
Iliterate 5 (10.0) 3 (7.5)
1 to 8 years 33 (66.0) 29 (72.5)
9 years or more 11(22.0) 8 (20.0)
Not informed 1 (2,0) 0,0 0.91
Smoking
Ex-‐smoking 4 (8.7) 0
Non smoking 31 (67.4) 20(58.8)
Current smoking 11 (23.9) 14 (41.2) 0.09

PARTICIPATION RATE OF WOMEN IN MAMMOGRAPHIC SCREENING IN 18 MONTHS, ACCORDING TO AGE - NMPOA

PATHOLOGIC FEATURES OF SCREEN-DETECTED AND NOT SCREEN DETECT BREAST CARCINOMAS. 2004-2013
Characteris*cs Mode of detec*on
Screen-‐detected (N=50) N (%) Not screen detected (N=40) N (%) p Tumor size (mm)* 16.7 (10.0) 18.5 (15.4) 0.54 Tumor size (mm)‡ 15.0 (10.0) 15.5 (17.5) Tumor size categories < 20 mm 28 (65.1) 23 ( 63.9) >20-‐50 mm 14 (32.6) 6 (30.6) >50 mm 1 (2.3) 2(5.6) 0.75 Tumor type IDC 38 (80.0) 32 (77.5) ILC 2 (2.0) 1 (5.0) Mixed 3 (4.0) 0 (2.5) Other 2 (2.0) 1 (5.0) DCIS 4 (12.0) 6 (10,0) 0.54 Stage** I 21 (47.7) 13 (38.2) II 19 (43.2) 14 (41.2) III 4 (9.1) 6 (17.6) IV 1 (2.9) 0 0.53 Grade** Grade 1 10 (29.4) 2 (8.0) Grade 2 19 (55.9) 13 (52.0) Grade 3 5 (14.7) 10 (40.0) 0.03

Official data (2011): u 10% STAGE I AND 53% STAGE III AND IV
u 51.3% of cancer patients had their 1st treatment between 60 and 120 days.
Cohort Nucleo Mama Porto Alegre Data (2014):
u According to our research, 43% of the patients were STAGE I and 15% of patients were STAGE III and IV.
u The tumor size was not statistically different among the two studied groups (screened and not screened)
u The average time to 1st treatment in our cohort was 21 days.
FINDINGS
u Based on the NMPA prospected study, we can infer that:
(1) an efficient health care system with well trained and committed u Based on the NMPA prospected study, we can infer that: (1) an efficient health care system with well trained and committed health professionals and (2) intensive community and primary care physicians awareness may be as good as annual screening mammography to promote breast cancer
in LMICs. changes in public policies in order to achieve cancer control.
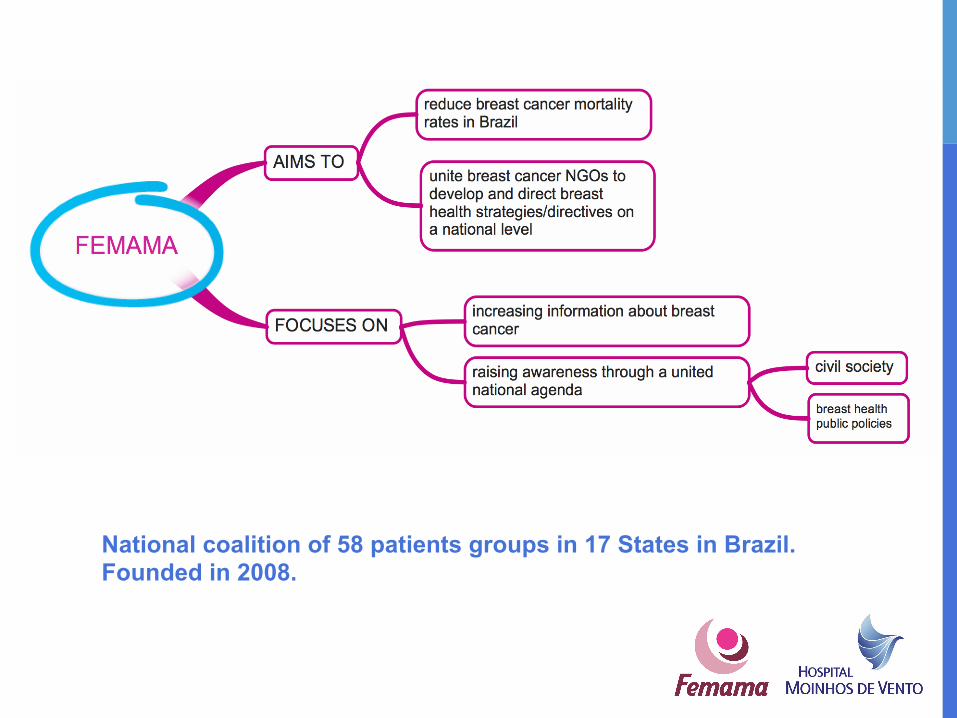
National coalition of 58 patients groups in 17 States in Brazil. Founded in 2008.

– CIVIL SOCIETY’S ROLE TOWARDS BREAST CANCER SURVIVAL IMPROVEMENT DUE TO EARLY DETECTION FEMAMA’S ACHIEVEMENTS SINCE 2008 ACHIEVEMENTS SINCE 2008
75% of mammography
coverage
Law of Mammography after 40 years-old #11.664/2008 -
March 23, 2012. National Program for Quality in Mammography INCA
30 days maximum time between
1st consultation and treatment initiation
certification for providers of SUS services and
supplementary
100%
May 23, 2013. Law #12.732 - Period of 60 days to start cancer treatment after diagnosis (pathological report)
March 23, 2011. Cervical and Breast Cancer Control National Plan

PATIENT’S PATH

30 days LAW PROJECT
# PL 5722/13 for exams when cancer is suspected indicated by the physician # PL 5722/13
approval of the Law of 30 days during the Pink October 2013; u Participation in 2 Public Audiences with request to approve the Law of 30
days in House of Representatives; u Request for Congressman to vote urgently the Law of 30 days;
u Institutional events held manifestation of agreement with the Law of 30 days:
2) Forum to Fight Cancer Woman 1) National Congress All Together Against Cancer 2) Forum to Fight Cancer Woman

ADVOCACY CAMPAIGN #OTEMPOCORRECONTRA #TIMERUNSAGAINST
Hot Site
Folders Banners

ADVOCACY CASE: LOBBY DAY

THANK YOU! Maira Caleffi, MD, Ph.D Chief of Breast Center at Hospital Moinhos de Vento
Volunteer President of FEMAMA
UICC Board Member