the reproducibility of colour doppler in chronic ... · pdf file06.08.2010 · the...
TRANSCRIPT

The reproducibility of colour Doppler in chronic cerebrospinalvenous insufficiency associated with multiple sclerosisE. MENEGATTI 1, V. GENOVA 1, M. TESSARI 1, A. M. MALAGONI 1, I. BARTOLOMEI 2,M. ZUOLO 1, R. GALEOTTI 1, F. SALVI 2, P. ZAMBONI 1
1Vascular Diseases Centre, University of Ferrara, Italy.2Bellaria Neurosciences, Bellaria Hospital Bologna, Italy
Aim. Chronic cerebrospinal venous insufficiency (CCSVI)is a syndrome described in multiple sclerosis (MS) patients,characterized by stenosis of the main extracranial veinswith hampered cerebral venous outflow. In the originaldescription echo-colour Doppler demonstrated to be anideal non invasive tool for screening CCSVI patients, butthe reproducibility was not assessed. Aim of this study isto assess the variability coefficient between trained and innot trained echo-colour Doppler operators. Methods. Thirty-six (36) subjects, matched for age and gen-der, were subset in 3 groups (group A, 12 healthy controls,HC; group B, 12 multiple sclerosis patients, MS; group C,12 patients with other neurological disease, OND) under-went echo-colour Doppler screening for CCSVI accordingto an original protocol previously described. The interobserver variability rate was assessed by comparing respec-tively trained vs not trained operators, and trained vs trainedoperators, by using the same echo-colour Doppler equip-ment. In addition, by scanning 15 subjects after one monthfrom the first session, intra observer coefficient was alsoassessed in trained operator. Results. The inter observer variability rate between trainedand not trained echo-colour Doppler operators, were notcompletely satisfactory (K coefficient 0.47 95% CI 0.27-0.68). To the contrary the inter observer agreement betweentrained operators was much more reliable (K coefficient0.80 95% CI 0.59-1.01). Finally, the intra observer variabil-ity rate in trained operators was 0.93, (95% CI 0.80-1.06)confirming a highly satisfactory agreement.Conclusion. Echo-colour Doppler is a powerful, non-inva-sive and reproducible tool for screening CCSVI-MS but itneeds special training.[Int Angiol 2010;29:121-6]
Key words: Cerebrospinal fluid - Venous insufficiency - Mul-tiple sclerosis - Ultrasonography.
A vascular syndrome has been recently describedand defined as chronic cerebrospinal venous insuf-ficiency (CCSVI), characterized by stenosis orobstruction of the internal jugular veins, and/orof the azygous system.
In CCSVI patients, venous stenosis in the maincerebrospinal outflow pathways were never foundto be isolated.
Rather, they were combined in the internal jugu-lar veins, azygous and lumbar systems, definingfour main patterns of distribution.1
Such venous obstructions are partially com-pensated by the activation of extra and intracra-nial collateral circulation, in order to avoidintracranial hypertension.2, 3
Our group recently reported that several venousflow anomalies affecting the internal jugular veins,and the azygous, which are the predominant returnpathways from the brain, occur more frequentlyin multiple sclerosis (MS) patients than in con-trols (P<0.001).1-4
The strength of evidence from the initial cross-sectional study was unexpectedly robust indicat-ing MS patients were 43-fold more likely to haveextracranial cerebral venous return anomalies thatmet pre-defined criteria for CCSVI.1
On the basis of the first description, echo-colourDoppler, examination seems to be an ideal screen-ing tool for CCSVI associated to MS.4
However, the reproducibility of the proposedinvestigation was never been assessed.
The aim of this study was to assess the vari-ability coefficient between trained and in nottrained echo-colour Doppler operators.
Vol. 29, No. 2 INTERNATIONAL ANGIOLOGY 121
This research was supported by a grant of Hilarescere no prof-it Foundation.
This paper has been presented in the poster session of theEuropean Charcot Foundation Symposium, Lisbon November12-14, 2009.
Received on November 18, 2009; accepted for publication onJanuary 10, 2010.
122 INTERNATIONAL ANGIOLOGY April 2010
Materials and methods
Subjects
The subjects under evaluation were 36, blindlyselected by the neurologist (FS), and subdividedinto three groups of 12 subjects each: group A, 12healthy controls, HC; group B, 12 multiple scle-rosis patients, MS; group C, 12 patients with otherneurological disease, OND.
Echo-color Doppler operators and protocol of CCSVIinvestigation
The echo-colour Doppler operators under eval-uation were respectively trained and non-trainedoperators. The trained operator was a vasculartechnician (EM) personally trained by the firstauthor who described the echo-colour Dopplerprotocol for CCSVI (PZ). The non-trained opera-tor was a radiologist, with experience of vascularinvestigations, who simply read and studied thepapers reporting the echo-colour Doppler proto-col (VG).1, 4
A combined transcranial and extracranial echo-colour Doppler provides validated measures ofparameters related to cerebral venous hemody-namics (VH) 1, 4 and enables the assessment ofCCSVI. Cerebral venous return was examined byusing the same echo-colour Doppler equipment
by both trained and non-trained (Esaote-Biosound My Lab Vinco, Genoa, Italy) equippedwith 2.5 and 7.5-13 Mhz transducers, with thesubject positioned on a tilt bed at 90° and 0°, andthe vessels insonated with an angle of 60°.5, 6 Theoperators focused on the detection of five VHpatterns affecting cerebral venous return. Thefollowing specific parameters were also report-ed by both operators in a software of this par-ticular echo-colour Doppler equipment (CCSVImeasurement protocol, Esaote, Genoa-Italy), andsubsequently blindly analyzed by the indepen-dent assessors.
VH Criterion 1
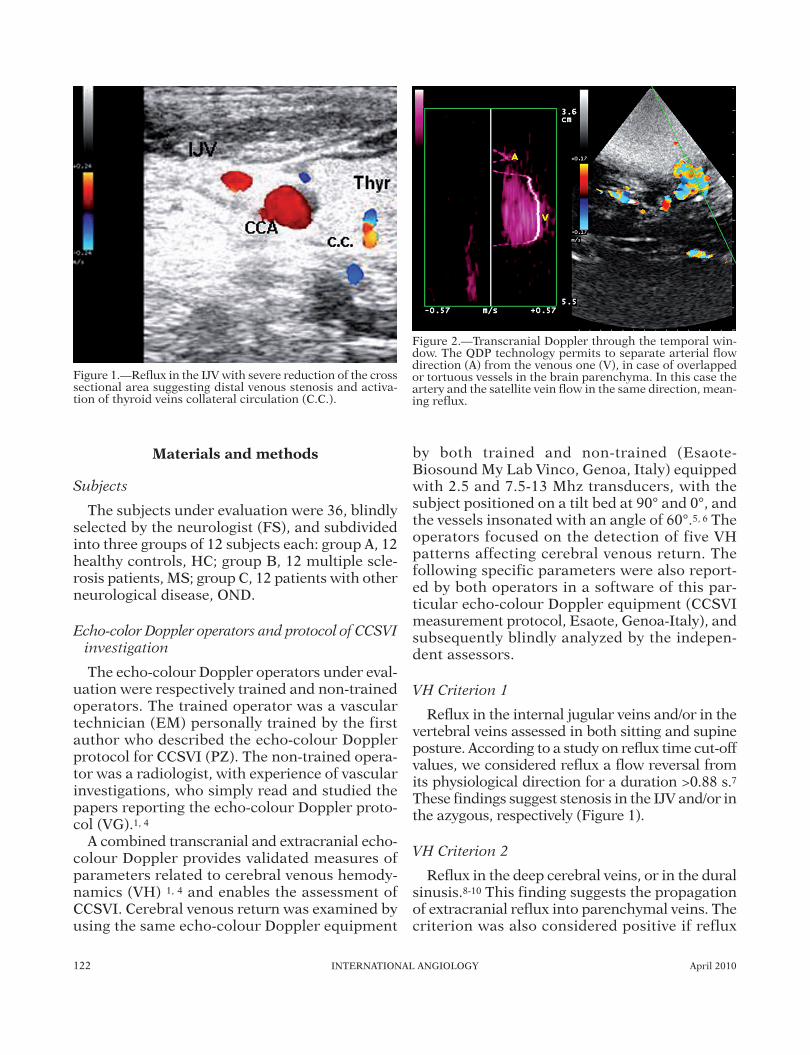
Reflux in the internal jugular veins and/or in thevertebral veins assessed in both sitting and supineposture. According to a study on reflux time cut-offvalues, we considered reflux a flow reversal fromits physiological direction for a duration >0.88 s.7These findings suggest stenosis in the IJV and/or inthe azygous, respectively (Figure 1).
VH Criterion 2
Reflux in the deep cerebral veins, or in the duralsinusis.8-10 This finding suggests the propagationof extracranial reflux into parenchymal veins. Thecriterion was also considered positive if reflux
Figure 1.—Reflux in the IJV with severe reduction of the crosssectional area suggesting distal venous stenosis and activa-tion of thyroid veins collateral circulation (C.C.).
Figure 2.—Transcranial Doppler through the temporal win-dow. The QDP technology permits to separate arterial flowdirection (A) from the venous one (V), in case of overlappedor tortuous vessels in the brain parenchyma. In this case theartery and the satellite vein flow in the same direction, mean-ing reflux.
Vol. 29, No. 2 INTERNATIONAL ANGIOLOGY 123
should be detected only in veins draining the sub-cortical GM into the deep cerebral veins.11 Thedetection of transcranial venous flow is not easyto assess, also in consequence of the high anatom-ical variability of the cerebral veins. In this study,flow detection was facilitated by QDP Technolo-gy (Esaote, Genoa, Italy) inserted in the echo-colorDoppler equipment. QDP mode enables the acqui-sition of the signal of a large number of samplevolumes across one or more blood vessels, mak-ing easier to separate arterial and venous flowDoppler signals and the detection of venous flowdirection (Figure 2).
VH Criterion 3
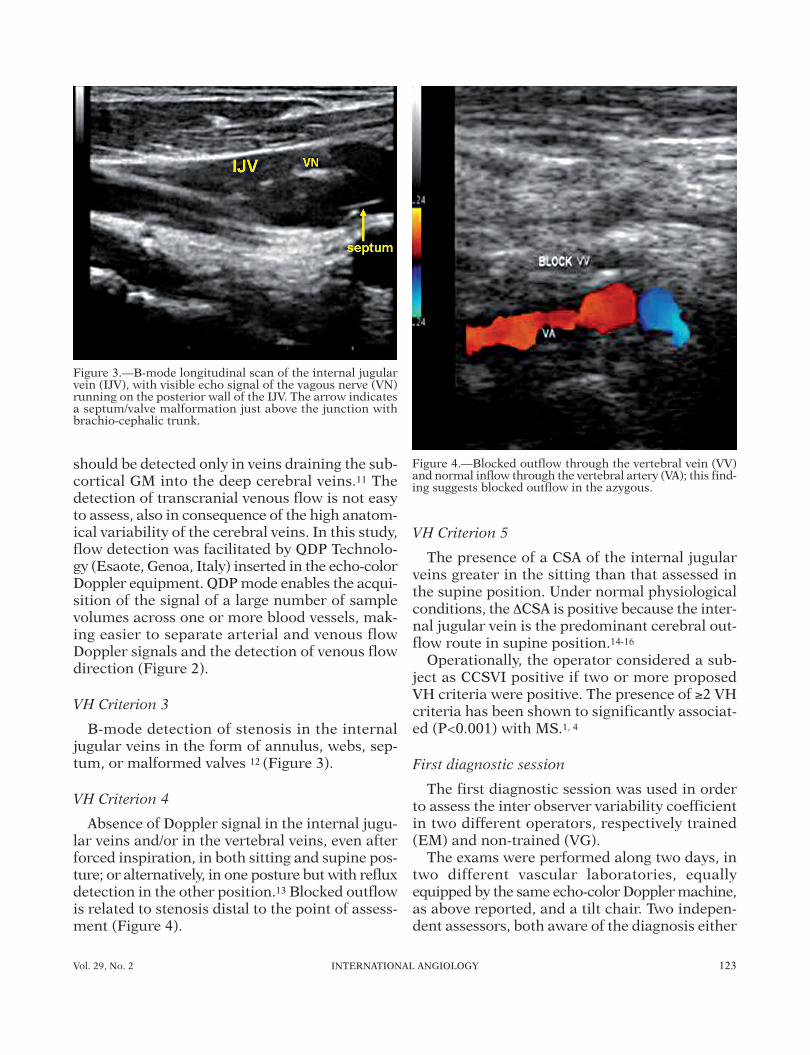
B-mode detection of stenosis in the internaljugular veins in the form of annulus, webs, sep-tum, or malformed valves 12 (Figure 3).
VH Criterion 4
Absence of Doppler signal in the internal jugu-lar veins and/or in the vertebral veins, even afterforced inspiration, in both sitting and supine pos-ture; or alternatively, in one posture but with refluxdetection in the other position.13 Blocked outflowis related to stenosis distal to the point of assess-ment (Figure 4).
VH Criterion 5
The presence of a CSA of the internal jugularveins greater in the sitting than that assessed inthe supine position. Under normal physiologicalconditions, the ∆CSA is positive because the inter-nal jugular vein is the predominant cerebral out-flow route in supine position.14-16
Operationally, the operator considered a sub-ject as CCSVI positive if two or more proposedVH criteria were positive. The presence of ≥2 VHcriteria has been shown to significantly associat-ed (P<0.001) with MS.1, 4
First diagnostic session
The first diagnostic session was used in orderto assess the inter observer variability coefficientin two different operators, respectively trained(EM) and non-trained (VG).
The exams were performed along two days, intwo different vascular laboratories, equallyequipped by the same echo-color Doppler machine,as above reported, and a tilt chair. Two indepen-dent assessors, both aware of the diagnosis either
Figure 3.—B-mode longitudinal scan of the internal jugularvein (IJV), with visible echo signal of the vagous nerve (VN)running on the posterior wall of the IJV. The arrow indicatesa septum/valve malformation just above the junction withbrachio-cephalic trunk.
Figure 4.—Blocked outflow through the vertebral vein (VV)and normal inflow through the vertebral artery (VA); this find-ing suggests blocked outflow in the azygous.

124 INTERNATIONAL ANGIOLOGY April 2010
of CCSVI or neurological (AMM, IB) randomlyassigned the subjects to the two operators, accord-ing to a computer generated list. They did notassist at the echo-color Doppler investigations,and only subsequently assessed the echo-colorDoppler result through the medical report regis-tered into the CCSVI measurement protocol soft-ware. Other two independent assessors (MT, MZ),both unaware of the diagnosis, masked the sub-ject under examination, with sunglasses, hat, andother special dressing consisting in particularshirts, scarf, coloured foulards, in order to makemore difficult to recognize the subjects in the sec-ond session.
Training for non-trained
After the first session the non-trained was specif-ically trained for two weeks by PZ. The trainingconsisted in theoretical lessons on cerebral venousreturn, ultrasonographic cerebral venous anato-my, pathophysiology of CCSVI, specific trainingon echo-color Doppler equipment; the practicalprogram consisted in back to back patient assess-ment in five different sessions of four hours each.Finally, discussion of the cases based on record-ings of the investigation performed together, wasa further integrated part of the program.
Second diagnostic session
After one month from the first session AMMand IB, randomly chosen five subjects from groupA, B and C respectively, being aware of the diag-nosis. MT and MZ provided to exchange amongthe selected subjects the sunglasses, and dress-ings previously used in the course of the first ses-sion. The fifteen subjects were reanalysed by bothtrained, because VG was in the meantime specif-ically trained as above reported.
Statistical analysis
Patient population demographics were com-pared for age, and gender by using one-wayANOVA and c2 test. Differences among group A,B, and C were considered statistically significantwhen P<0.05.
The first session was used to assess the intervariability coefficient rate in trained and non-trained staff. The second session was used toassess the inter observer variability rate between
trained staff. Finally, by comparing the first ses-sion with the session of the trained, we assess theintra observer variability rate. The inter observ-er and the intra observer coefficients were cal-culated by using the Cohen’s K coefficient 17 and95% CI.
Results
The patient population demographics are givenin Table I. No statistically significant differencesamong the 3 groups were found.
Inter observer correlation coefficient was high-er for the trained vs not trained personnel com-parison (K coefficient 0.80 95% CI 0.59-1.01) thanfor the trained x not trained personnel compari-son (K coefficient 0.47 95% CI 0.27-0.68). Final-ly, the intra observer correlation coefficient was0.93, 95% CI 0.80-1.06).
Tables II-III are contingency tables referredrespectively to interobserver variability found indetails pre and after training, respectively. Final-ly, Table IV describes in detail the intraobservervariability test.
Discussion
The echo-color Doppler screening for CCSVI-MS is a valuable tool permitting to recognizeanomalous cerebral venous hemodynamics cor-responding to angiographically demonstrated
TABLE I.—Patients population demographic.
Group A Group B Group CHC MS OND
(N.=12) (N.=12) (N.=12)
AgeMean±SD 38.9±16 41.7±8.7 50.8±19.1
Sex %M 50% 41.6% 58.3M/F 6/6 5/7 7/5
TABLE II.—Interobserver variability assessed between trai-ned and non-trained operators.
Trained Non-trainedoperator 1 operator Total
True 36 17 53False 0 19 19Total 36 36 72

Vol. 29, No. 2 INTERNATIONAL ANGIOLOGY 125
stenosies of the main extracranial and extraver-tebral trunk.1, 4
For instance, venous reflux in any body posture,and/or venous obstruction in any body posture,and/or combination of reflux and obstructionrespectively in sitting and in supine posture cor-responded in the venographic demonstration ofstenosing lesions. Particularly, anomalies detect-ed in the vertebral veins (Figure 4), or reflux com-ing from the extravertebral plexus toward theintravertebral plexus suggest obstruction in theazygous. Such an indirect non-invasive informa-tion is crucial in CCSVI, because approximately70% of CCSVI patients showed obstructions inthe proximal azygous, and about one third in thedistal azygous.18 Azygous system is very difficultto investigate because the cardiac movementsimpairing both MRI and CT scan studies. At pre-sent ECD seems to be the only reliable non-inva-sive screening tool preceding selective venogra-phy.
Moreover, in the internal jugular veins the steno-sis can be directly detected by means of echo-colorDoppler, and as previously reported the mor-phology of these malformations can be of differ-ent shapes.1-4, 18 For instance, in Figure 3 a sep-tum/valve malformation is visible , previouslydetected in 45% of the internal jugular veins, main-ly on the right side.18
However, ultrasound is non-invasive and cheap-er, repeatable but strongly operator dependent.
The main result of this study is the demonstra-tion of a satisfactory agreement between trainedoperators. In contrast, the inter observer vari-ability rate between non-trained and trainedclearly demonstrates the possibility of an amplemargin of error when non-trained screen patientsfor CCSVI. The training program herein experi-mented between the first and the second sessionrepresents a useful basis for educational pro-grams in favour of non-trained operators, whoare interested in screening MS patients forCCSVI.
Finally, the highly satisfactory intra observercoefficient rate measured in trained operators fur-ther confirms the reliability of echo-color Doppler,and the necessity of educational programs.
Conclusions
Echo-color Doppler performed by specificallytrained personnel was highly reproducible toscreen for CCSVI in MS patients. Examinationsperformed by untrained personnel failed to cor-relate with the results obtained by trained per-sonnel.
References
1. Zamboni P, Galeotti R, Menegatti E, Malagoni AM, Tac-coni G, Dall’Ara S et al. Chronic cerebrospinal venousinsufficiency in patients with multiple sclerosis. J NeurNeurosurg Psychiatry 2009;80:392-9.
2. Zamboni P, Consorti G, Galeotti R, Gianesini S, Menegat-ti E, Tacconi G et al. Venous collateral circulation of theextracranial cerebrospinaloutflow routes. Curr NeurovascRes 2009;3:204-12.
3. Singh AV, Zamboni P. Anomalous venous blood flow andiron deposition in multiple sclerosis. J Cereb Blood FlowMetab 2009;Sep 2 [Epub ahead of print].
4. Zamboni P, Menegatti E, Galeotti R, Malagoni AM, Tac-coni G, Dall’Ara S et al. The value of cerebral Dopplervenous haemodynamics in the assessment of multiplesclerosis. J Neurol Sci 2009;282:21-7.
5. Valdueza, JM, Von Munster T, Hoffman O, Schreiber S,Einhaupl KM. Postural dependency of the cerebral venousoutflow. Lancet 2000;355:200-1.
6. Menegatti E, Zamboni P. Doppler haemodynamics of cere-bral venous return. Curr Neurovasc Res 2008;5:259-64.
7. Nedelmann M, Eicke BM, Dieterich M. Functional andmorphological criteria of internal jugular valve insuffi-ciency as assessed by ultrasound. J Neuroimaging2005;15:70-5.
8. Valdueza JM, Schmierer K, Mehraein S, Einhaupl KM.Assessment of normal flow velocity in basal cerebral veins:a transcranial Doppler ultrasound study. Stroke1996;27:1221-5.
9. Stolz DE, Kaps M, Kern A, Babacan SS. Reference datafrom 130 volunteers transcranial color-coded duplex
TABLE III.—Interobserver variability calculated after trai-ning period. The non trained-operator of the first sessionhas been herein defined the trained operator 2, afteraccomplishment of a 2 week specific training.
Trained Trainedoperator 1 operator 2 Total
True 14 13 27False 1 2 3Total 15 15 30
TABLE IV.—Intraobserver variability rate.
Trained Trainedoperator 1 operator 1 Total
True 15 14 29False 0 1 1Total 15 15 30

126 INTERNATIONAL ANGIOLOGY April 2010
sonography of intracranial veins and sinuses. Stroke1999;30:1070-5.
10. Zipper SG, Stolz E. Clinical application of transcranialcolourcoded duplex sonography: a review. Eur J Neurol2002;9:1-8.
11. Zamboni P, Menegatti E, Bartolomei I, Galeotti R, Malag-oni AM, Tacconi G et al. Intracranial venous haemody-namics in multiple sclerosis. Curr Neurovasc Res2007;4:252-8.
12. Lichtenstein D, Saïfi R, Augarde R, Prin S, Schmitt JM,Page B et al. The Internal jugular veins are asymmetric.Usefulness of ultrasound before catheterization. Inten-sive Care Med 2001;27:301-5.
13. Doepp F, Schreiber SJ, von Münster T, Rademacher J,Klingebiel R, Valdueza JM. How does the blood leave thebrain? A systematic ultrasound analysis of cerebral venousdrainage patterns. Neuroradiology 2004;46:565-70.
14. Schreiber SJ, Lurtzing F, Gotze R, Doepp F, KlingebielR, Valdueza JM. Extrajugular pathways of human cere-
bral venous blood drainage assessed by duplex ultrasound.J Appl Physiol 2003;94:1802-5.
15. Schaller B. Physiology of cerebral venous blood flow:from experimental data in animals to normal function inhumans. Brain Res Rev 2004;46:243-60.
16. Gisolf, J, van Lieshout JJ, van Heusden K, Pott F, StokWJ, Karemaker JM. Human cerebral venous outflow path-way depends on posture and central venous pressure. JPhysiol 2004;560:317-27.
17. Cohen J. A coefficient of agreement for nominal scales.Educ. Psycol. Measmnt 1960;20:37-46.
18. Zamboni P, Galeotti R, Menegatti E, Malagoni AM,Gianesini S, Bartolomei I et al. Endovascular treatmentof chronic cerebrospinal venous insufficiency. A prospec-tive open-label study. J Vasc Surg 2009. In press.
Corresponding author: E. Menegatti, Vascular Diseases Cen-ter, University of Ferrara, 44100 Ferrara, Italy. E-mail: [email protected]