the quebec palliative sedation guidelines
TRANSCRIPT
The Quebec Palliative Sedation Guidelines
Rose DeAngelis, N, MSc(A), CHPCN (C) CHPCA Conference September 2017
Conflict of Interest Statements
• There is no financial or in-kind support for this presentation.
• There are no biases to be mitigated.
• I do not have any relationships with any pharmaceutical company nor do I benefit from any mention of their medications in this presentation.
2

In this session, we’ll review
• The key elements of guidelines themselves
• Indications for the use of Palliative Sedation
• Pre-sedation steps
• Selecting medication options
• Standardized assessment tools used
• Documentation requirements
• Discussion challenges
3
Palliative Sedation (or forms of it) have been called:
• Sedation • Terminal sedation • Sedation for intractable distress in the imminently dying • End-of-life sedation • Total sedation • Sedation in the terminal or final stages of life • Controlled sedation • Palliative sedation therapy • Proportional Palliative Sedation - PPT • Palliative sedation to unconsciousness – PSU • Continuous palliative sedation therapy-CPST
Annals Internal Medicine, 2009
4

Practice Guide
5 www.cmq.org/publications-pdf/p-1-2016-08-29-en-sedation-palliative-fin-de-vie.pdf

Palliative Sedation
Is the intentional induction of
sedation to relieve intractable
symptoms and suffering, when all other therapeutic interventions have
failed.
Heal, sometimes
Relieve, often
Comfort, always
Anonymous 16th century
Goal and intention of the sedation is to relieve distress
The patient is unconscious and can be for hours, days or weeks until the advancing disease, not the combination of medications given, causes the patient’s death.
7
Pereira, J. (2013), Pallium Palliative Pocketbook, 18-1
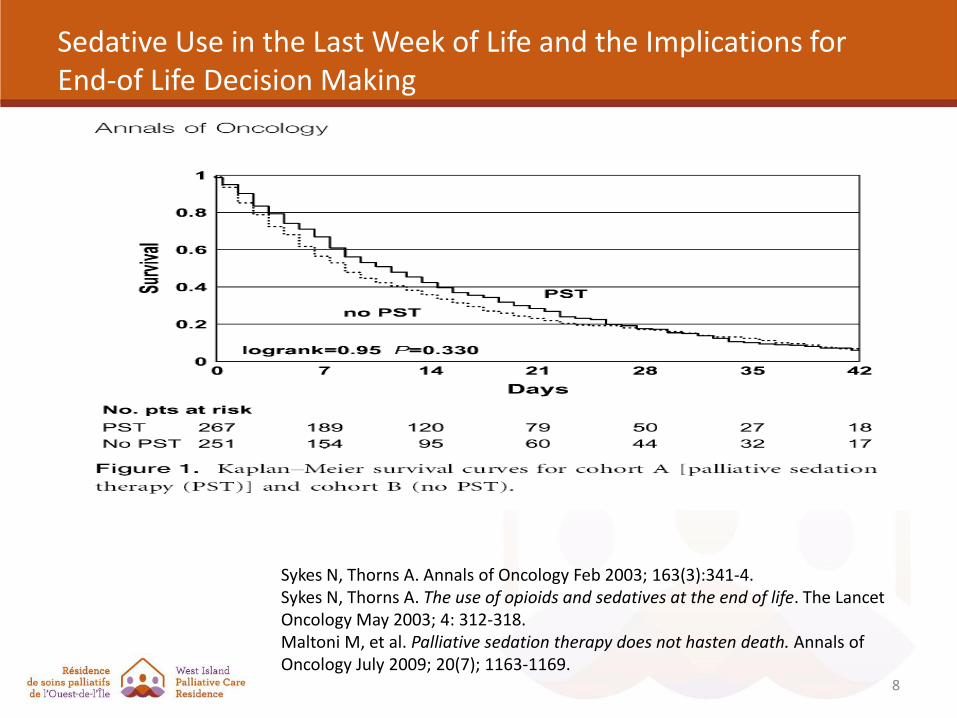
Sedative Use in the Last Week of Life and the Implications for End-of Life Decision Making
8
Sykes N, Thorns A. Annals of Oncology Feb 2003; 163(3):341-4. Sykes N, Thorns A. The use of opioids and sedatives at the end of life. The Lancet Oncology May 2003; 4: 312-318. Maltoni M, et al. Palliative sedation therapy does not hasten death. Annals of Oncology July 2009; 20(7); 1163-1169.
Palliative Sedation is a rare event
It is a relatively rare phenomenon that occurs in about 3-5% of patients who
are in palliative care settings.
9
The decision to use Palliative Sedation is based on :
the presence of refractory and intolerant symptoms
the inability of standard therapies to provide adequate relief within an acceptable time frame
10
Indications for the use of Palliative Sedation
• Hyperactive delirium with uncontrolled agitation
• Recurrent episodes of severe respiratory distress
• Progressive and intractable dyspnea
• Refractory seizures
• Intolerable and untreatable pain
• Hemorrhagic distress
• Intractable nausea and vomiting
• Copious and refractory bronchial secretions
• Refractory psychological or existential distress that severely compromises comfort
11
Imminence of Death
There must be evidence to support the fact that death is
imminent.
12

Who can be offered Palliative Sedation?
13
The patient’s disease must be irreversible, far-advanced, and death expected in less than 2 weeks.
The patient (or proxy) determines himself that he has intolerable suffering as a symptom that he does not wish to endure.
Cherny, N.I., and R.K. Portenoy. 1994. Sedation in the management of refractory symptoms: Guidelines for evaluation and treatment. Journal of Palliative Care 10(2): 31–38.
Consent & Pre-Infusion Discussion
• The physician must obtain free and informed consent
• Explain the following: A review of the diagnosis/prognosis
The irreversible nature of the sedation
That the procedure will not cause death
What the procedure entails/monitoring requirements
The anticipated duration of the sedation
That the patient will remain unconscious/cannot interact
Its benefits and risks
Any other possible options
Consequences of a refusal of the palliative sedation
What death with/without palliative sedation is anticipated to look like
The non-provision of nutrition (and hydration) in most cases*
14
We suggest to …
• Negotiate the start time of the infusion with the patient/family.
• Ensure the presence of interdisciplinary team members as decision is being made.
• Document observations of the patient/family understanding of and reactions to the decisions taken.
15

The decision to sedate is not a unilateral decision
• Be culturally sensitive
• Discuss with patient/family to assess the following:
The value and meaning given to pain, suffering, death, dying?
The importance of consciousness in the dying process?
The value and meaning placed on food, hydration?
The communication pattern in the family? (truth telling, disclosure, and hope system)
Is the decision consistent with patient’s values and wishes?
Perception by the patient/family of the role of the health care practitioners
16
Purnell L. The Purnell Model for Cultural Competence. J of Multicultural Nursing and Health (Summer 2005)
General principles for physicians starting Palliative Sedation
• Choose the most appropriate medication(s) More than 1 medication may be required, especially if more than 1
refractory symptom is present
• Restrict the number of agents used It’s not logical to use 2 benzodiazepines or 2 neuroleptics
• Begin slow/low Use the minimum amount of medication that relieves the symptom(s)
• Consider changing to another class of medications if they are not effective or if there are too many side effects
• Check cross compatibility
• Ensure physician presence at the start of the sedation
17
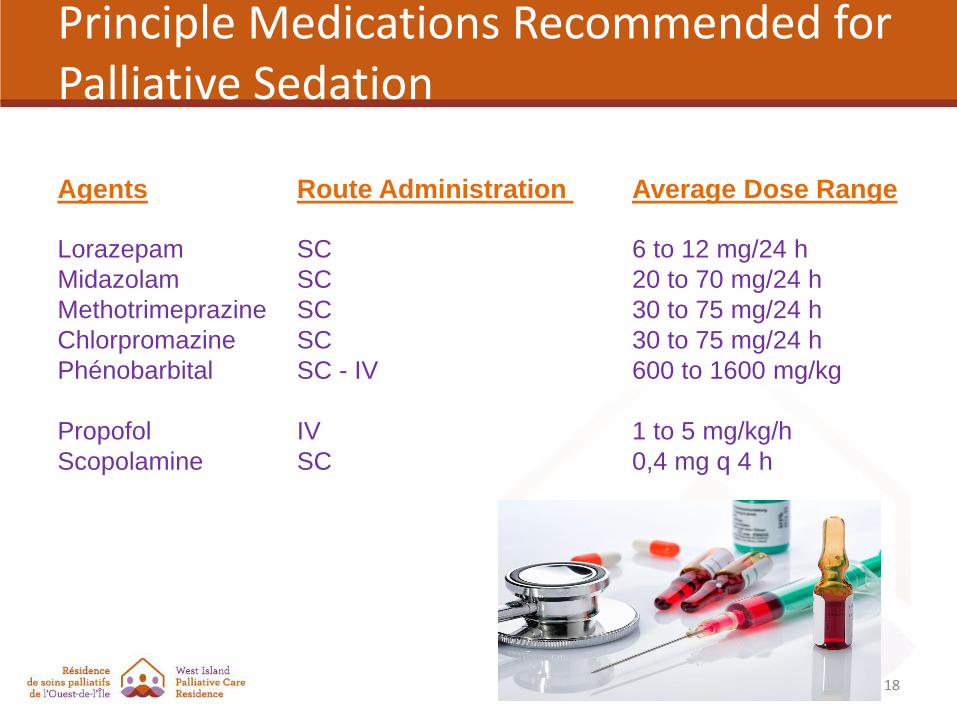
Principle Medications Recommended for Palliative Sedation
Agents Route Administration Average Dose Range
Lorazepam SC 6 to 12 mg/24 h
Midazolam SC 20 to 70 mg/24 h
Methotrimeprazine SC 30 to 75 mg/24 h
Chlorpromazine SC 30 to 75 mg/24 h
Phénobarbital SC - IV 600 to 1600 mg/kg
Propofol IV 1 to 5 mg/kg/h
Scopolamine SC 0,4 mg q 4 h
18
Monitoring has 3 main components:
The level and depth of sedation
The comfort level and symptom relief obtained
The presence of any adverse side effects
19
‘Scales’ for other refractory symptoms?
Since there is no objective assessment scale for many of the refractory symptoms such as seizures
hemorrhagic distress
psychological or existential distress
intractable nausea and vomiting, etc.
it is agreed that the most accurate description possible must written in the nurse’s notes concerning the targeted symptom and/or of any side effects observed.
20
There are 3 suggested validated assessment tools
• To assess the depth of sedation
• Richmond Agitation-Sedation Scale (RASS)
• Goal is a score of -3, -4
• To assess the level of pain and discomfort
• Nociception Coma Scale (Vinay Scale)
• Goal is a score of 8 or less.
• To assess the degree of respiratory distress
• Respiratory Observation Distress Scale (RDOS)
• Goal is a score of 4 or less.
21
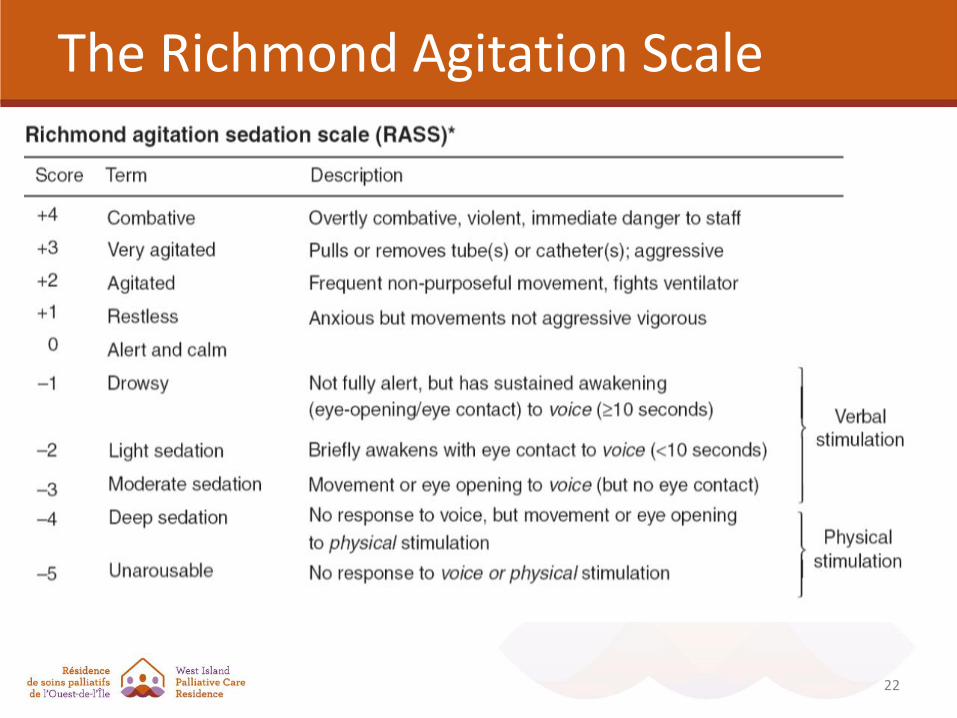
The Richmond Agitation Scale
22

Nociception Coma Scale (Adapted by Vinay 2011)
23

Nociception Coma Scale (Adapted by Vinay 2011)
Measures pain relief by assessing the following:
Facial expression-tense/relaxed
Presence of tears, moaning
Limb stiffness/relaxed
Movements calm/agitated
Respiration ≤ ≥ 19
Pulse ≤ ≥ 110
24

Respiratory Distress Observation Scale (RDOS) (Campbell, 2008, 2010)
25
26
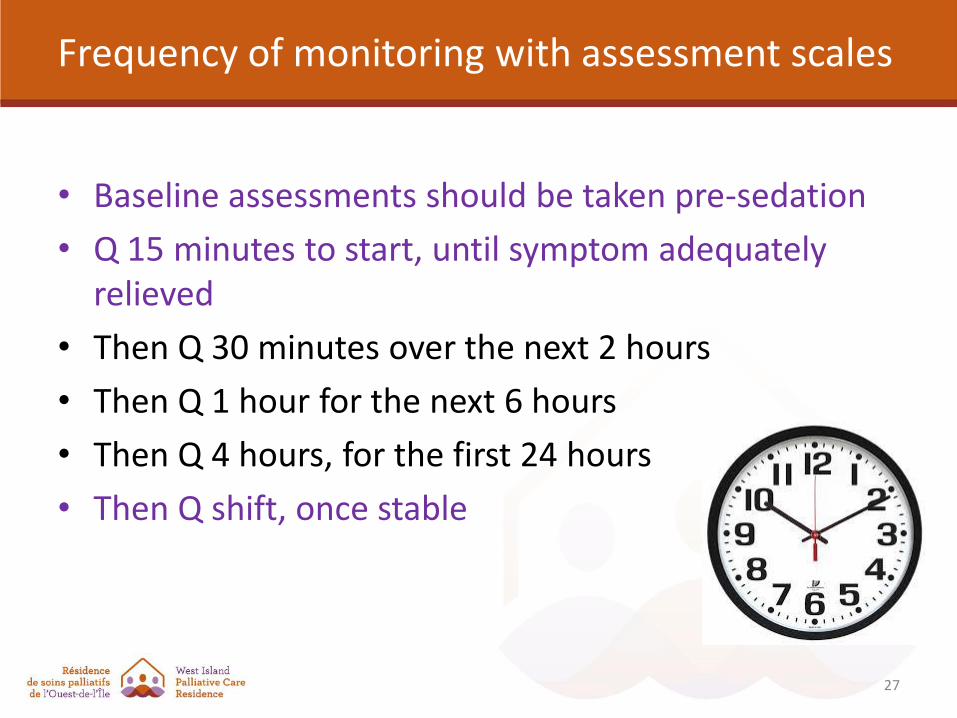
Frequency of monitoring with assessment scales
• Baseline assessments should be taken pre-sedation
• Q 15 minutes to start, until symptom adequately relieved
• Then Q 30 minutes over the next 2 hours
• Then Q 1 hour for the next 6 hours
• Then Q 4 hours, for the first 24 hours
• Then Q shift, once stable
27
Monitoring for Side Effects
• Since comfort is the overriding goal of palliative sedation, any parameters observed are mainly comfort-oriented.
28
• So what about measuring the following? – Blood pressure
– Temperature
– Oxygen saturation
– Respiratory rate
– Myoclonus
– Miotic pupils
Nursing Responsibilities • Document drug, dose and titration process clearly
• Document sedation, respiratory and comfort level and titrate medication(s) until symptoms are controlled
• Assess the need for placing a Foley catheter in if sedation is expected to last more than 12-24 hours
• Maintain airway patency
• Continue analgesics if they were required pre-sedation
• Continue all routine comfort measures including turning, positioning, bathing, good skin and
mouth care, massaging bony
prominences, toileting, explaining
any nursing action to the patient, etc.,
29

Supportive Care Responsibilities • Support family during the process
• Emotional support
• Informational support
• Reinforce goals of care
• Convey consistent messaging amongst all family members
• Support the health care team
• Ensure the staff is all on the same page
• Help them to understand process/decisions taken/reasoning
• Let them vent!
30
31
The West Island Palliative Care Residence Mission Statement: To provide active and compassionate care in order to comfort and support terminally ill patients and their loved ones and to continue as a leader in palliative care within Quebec and Canada.