the muscular system. a.function of muscles muscles are responsible for four functions 1. p roduce...
TRANSCRIPT

The Muscular The Muscular SystemSystem

A.A. Function of MusclesFunction of MusclesMuscles are responsible for four functions1.1. Produce movementProduce movement
Contraction!Skeletal: Run away from danger, smile in flirtation
Smooth: peristalsis of digestionCardiac: beat of heart
2.2. Maintain postureMaintain postureUpright/seated – fight downward pull of gravity

3.3.StabilizStabilize jointse joints Tendons attaching muscles to
bones of joints for stabilization

4. Generate heat By-product of muscle activity
produces heat As ATP (adenosine triphosphate)
is used to power contraction, ¾ energy released as heat
Maintains normal body temperature (homeostasis!)
Skeletal muscle (40% body mass) most responsible

B.B. Types of MusclesTypes of MusclesThree basic muscle types are found in the bodyi. Skeletal muscle - attached
to bonesii. Smooth muscle - hollow
visceral (internal) organsiii. Cardiac muscle – heart


i. Skeletal MusclesMost are attached by tendons to bonesCells are multinucleate (many nuclei in one cell)
Striated – have visible bandingVoluntary – subject to conscious control
Cells are surrounded and bundled by connective tissue

Muscle fiber = muscle cellEndomysium – around
single muscle fiberFascicle = bundle of fibersPerimysium – around a
fascicleTypical skeletal muscle =
bundle of fasciclesEpimysium – covers the
entire skeletal muscleFascia – on the outside of
the epimysiumFigure 6.1
“Packaging” of Skeletal Muscles

Epimysium blends into a connective tissue attachmentTendon – cord-like structureAponeuroses – sheet-like structure
Sites of muscle attachmentBonesCartilagesConnective tissue coverings
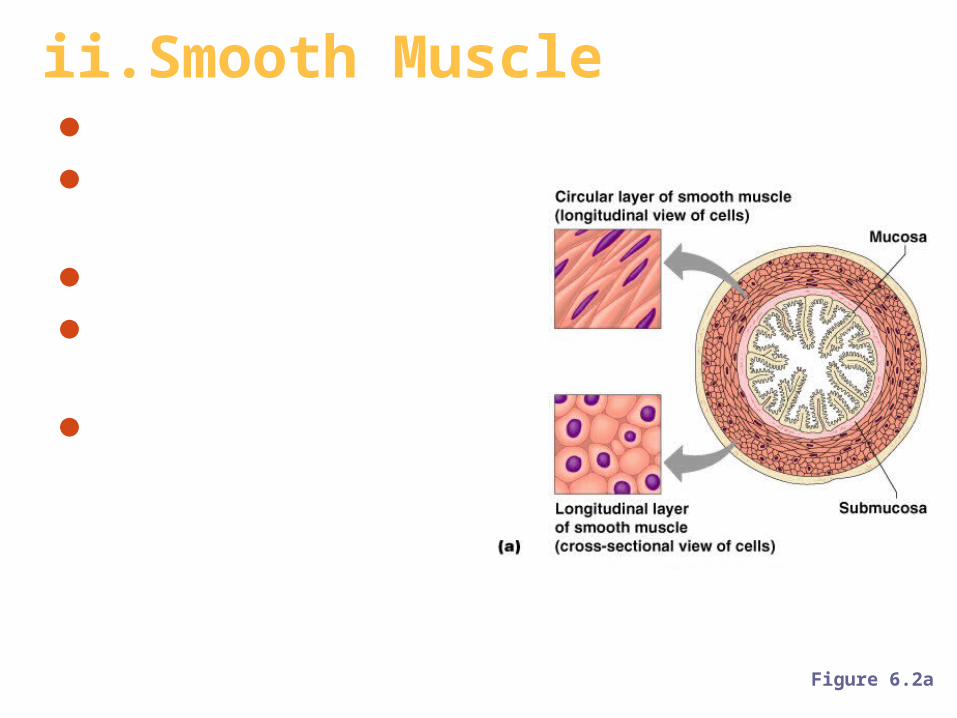
ii. Smooth MuscleHas no striationsSpindle-shaped cells
Single nucleusInvoluntary – no conscious control
Found mainly in the walls of hollow organs
Figure 6.2a

iii.Cardiac MuscleHas striationsUsually has a single nucleus
Joined to another muscle cell at an intercalated disc
InvoluntaryFound only in the heart
Figure 6.2b


C. Anatomy of Skeletal Muscle
Cells are multinucleate (many nuclei per cell)Nuclei (oval-shaped) are just beneath the sarcolemma (specialized plasma membrane)
Contain sarcoplasmic reticulum (specialized smooth endoplasmic reticulum [ER]) for Ca2+ storage
Figure 6.3a

Figure 6.3a
One muscle fiber (muscle cell) is made of a bundle of myofibrils (organelles) that nearly fill cytoplasm

One myofibril (organelle) is made of chains of tiny contractile units called sarcomeres (Z disc to Z disc)
SARCOMERE

one sarcomere is made of two myofilaments (protein filaments): actin (thin) and myosin (thick)

Thick filamentsComposed of the protein myosinHas ATPase enzymes which break ATP bonds to make energy for muscle contraction!
Thin filamentsComposed of the protein actin
Figure 6.3c

Myosin filaments have heads (extensions, or cross bridges which look like golf club heads) that move
Myosin and actin overlap somewhat
Figure 6.3d

Site of muscle contraction


Figure 6.3b
Alignment of myofibrils in sarcomere creates banding patternI band (light band) = absence of myosin
A band (dark band) = concentration of myosin

Z disc =Area where actin joins other actin molecules, forms Z-shaped pattern
H zone (bare zone) = area that lacks thin filaments
M line = center of H zone that contains tiny protein rods that hold adjacent myosin proteins together

Banding pattern changes shape during contraction when each sarcomere segment gets shortened (H zone gets smaller)

D.Muscle Activity: Contraction
Muscle has two functional properties that are necessary for contraction:1.Irritability – ability to receivereceive and
respondrespond to a stimulus (nerve to muscle)
2.Contractility – ability to shortenshorten when an adequate stimulus is received via sliding filament theory (inside muscle)

1. Irritation: Nerve Stimulus to Muscles
Skeletal muscles must be stimulated by a nerve
Motor units are responsible for stimulating a few to hundreds of muscle cells. Consist ofOne neuronAll muscle cells stimulated by that one neuron
Figure 6.4a
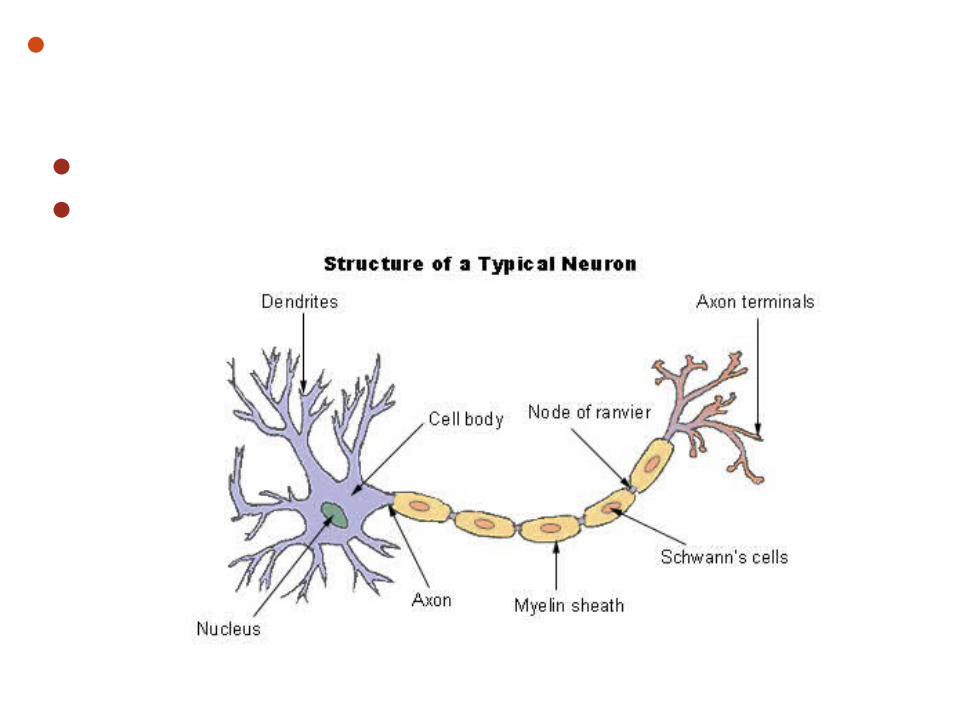
Neuron (nerve cell) relays message through electrical and chemical signals. Consists ofCell body (with dendrite fingers)Axon or nerve fiber (with axon terminal projections)

Axon terminals approach (never physically touch) muscle’s sarcolemma via neuromuscular junctionsGap between axon terminals and muscle cells called synaptic cleftFilled with interstitial (“between tissues”) fluid
Figure 6.5b

1.Electrical nerve impulse reaches dendrites
Steps of Nerve Stimulation

2.Signal moves down cell body, to axon terminals, signals vesicles with chemical neurotransmitter called acetylcholine (ACh) to move to nerve membrane

3.ACh is released via exocytosis into synaptic cleft (space between nerve and muscle)
4.ACh attaches to receptors on the sarcolemma membrane
5.Triggers Na+/K+ (sodium/potassium) pumps to open, making sarcolemma permeable to Na+ (Na+ rushes in, K+ rushes out)

6.Rapid change in ion movement (sodium in, potassium out of the cell) is called depolarization which generates an electrical current called action potential
7.Action potential will start, muscle contraction which cannot be stopped travels over entire surface of sarcolemma

In the meantime, ACh is now broken down by enzyme (AChase) to acetic acid and cholineThis is why one nerve impulse produces one contraction

Steps of Nerve Stimulation 1. Nerve cell receives electrical stimulus
through dendrites2. Stimulus send down cell body, out
through axon terminals as chemical signal
3. ACh neurotransmitter released from vesicles into synaptic cleft
4. Receptors on sarcolemma receive ACh5. Sarcolemma now permeable to Na+ ions
= Na+ rushes in, K+ rushes out6. Depolarization of muscle cells creates
action potential

2. Contraction: The Sliding Filament Theory
Activation by nerve causes myosin heads (cross bridges) to attach to binding sites on the thin (actin) filament
Myosin heads then bind to the next site of the thin filament due to Ca2+ and ATP
Figure 6.7
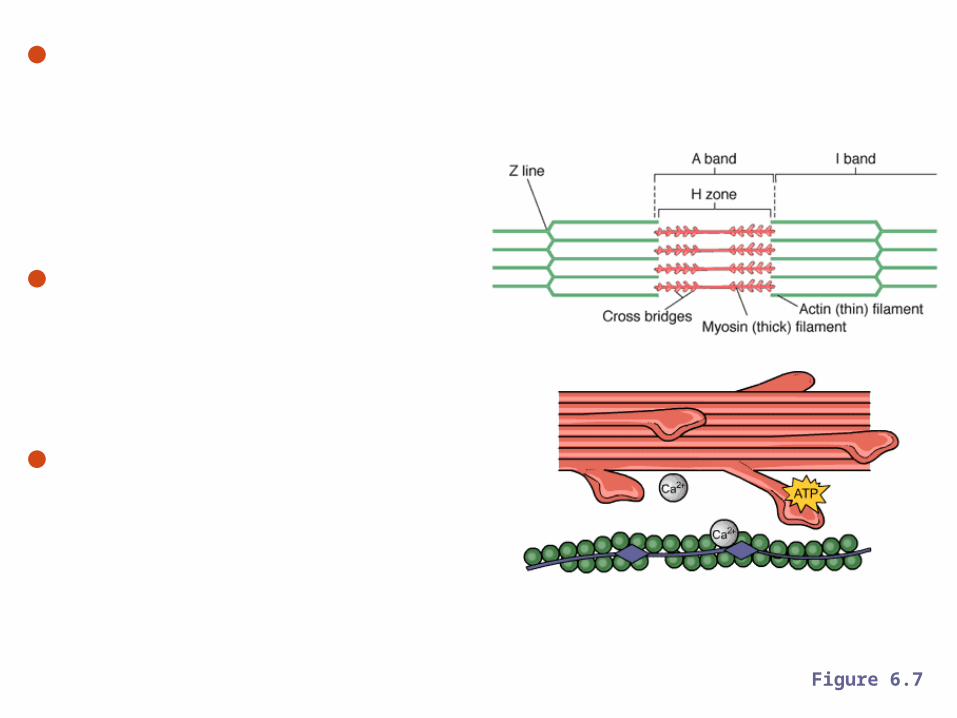
Ca2+ from sarcoplasmic reticulum which was triggered to release Ca2+ as a result of action potential
This continued action causes a sliding of the myosin along the actin
The result is that the muscle is shortened (contracted) Figure 6.7


Figure 6.8




Muscle cell relaxes again when:1. diffusion of K+ ions out of cell2. Na+/K+ pump brings ions back to original state (Na+ back out, K+ back in)

1. Action potential triggers sarcoplasmic reticulum to release Ca2+
2. Action potential causes myosin heads to attach to binding sites on actin filament
3. Ca2+ with ATP triggers myosin heads to attach to neighbor binding sites on same actin filament, causing actin to move toward each other = contraction!
Sliding Filament Sliding Filament Contraction RecapContraction Recap

Muscle fiber contraction is “all or none”Within a skeletal muscle, not all fibers may
be stimulated during the same intervalDifferent combinations of muscle fiber
contractions may give differing responsesGraded responses – different degrees of
skeletal muscle shortening
Contraction Responses

Types of Graded Responses1.Twitch
Single, brief contractionNot a normal muscle function
Figure 6.9a–b

2.Tetanus (summing of contractions)
One contraction is immediately followed by another
The muscle does not completely return to a resting state
The effects are added (summed)
Figure 6.9a–b

3. Fused (complete) tetanusNo evidence of relaxation before the
following contractionsThe result is a sustained muscle contraction
Figure 6.9c–d

Muscle force depends upon the number of fibers stimulated
More fibers contracting results in greater muscle tension
Muscles can continue to contract unless they run out of energy

Muscle Fatigue and Oxygen Debt
When a muscle is fatigued, it is unable to contract
The common reason for muscle fatigue is oxygen debtOxygen must be “repaid” to tissue to remove oxygen debt
Oxygen is required to get rid of accumulated lactic acidBreathing heavy!
Increasing acidity (from lactic acid) and lack of ATP causes the muscle to contract less

Types of Muscle ContractionsIsotonic contractions
Myofilaments are able to slide past each other during contractions
The muscle shortens (movement)Ex: bending knee, smiling
Isometric contractionsTension in the muscles increasesThe muscle is unable to shorten (no movement)Ex: lifting 400-lb table alone, push
against wall

Muscle ToneSome fibers are contracted even in a
relaxed muscleDifferent fibers contract at different times
to provide muscle toneThe process of stimulating various fibers
is under involuntary control

E. Body MovementsMovement is attained due to a muscle moving an attached bone
Muscles are attached to at least two pointsInsertion – attachment to a moveable bone
Origin– attachment to an immovable bone
Figure 6.12

Ordinary Body MovementsFlexion – decreases angle of joint &
brings two bones closer togetherExtension – opposite of flexion
(increases angle, bones farther apart)Rotation – movement of bone around
longitudinal axisAbduction – move AWAY from midlineAdduction – move TOWARD midlineCircumduction – proximal end of
bone stationary, distal end moves in circle
oppo
site
sop
posi
tes
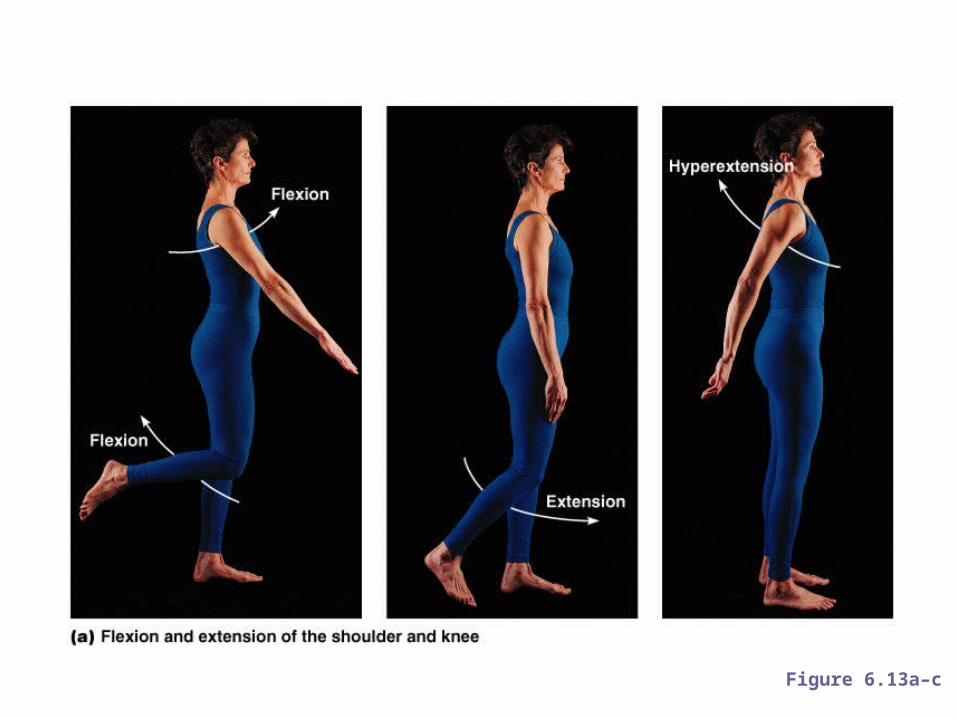
Figure 6.13a–c


Figure 6.13d

Special MovementsDorsiflexion – lifting foot so its superior
surface approaches shin (decrease angle)Plantar flexion – pointing toes away from
shin (increase angle)Retraction – moving bone slightly
backwardProtraction – moving bone slightly forward
oppo
site
sop
posi
tes

Inversion – move sole of foot up and inward
Eversion – move sole of foot up and outward
oppo
site
s

Supination – radius and ulna are parallel (palm up)
Pronation – radius rotates over ulna (palm down)
Opposition –thumb touching tip of other fingers
oppo
site
s

F. Types of MusclesPrime mover (agonist) – muscle with the major responsibility for contracting
Antagonist – muscle that opposes or reverses a prime mover (relaxes)
Synergist – muscle that aids a prime mover in a movement and helps prevent rotation
Fixator – stabilizes the origin of a prime mover
Agonist vs. Antagonist Muscle

Naming of Skeletal MusclesDirection of muscle fibers
Example: rectus (straight)
Relative size of the muscleExample: maximus (largest)

Location of the muscleExample: many muscles are named for bones (e.g., temporalis)

Number of originsExample: triceps (three heads)

Location of the muscle’s origin and insertionExample: sterno (on the sternum)
Shape of the muscleExample: deltoid (triangular)

Action of the muscleExample: flexor and extensor (flexes or extends a bone)


Head and Neck Muscles
Figure 6.15

Trunk Muscles
Figure 6.16

Deep Trunk and Arm Muscles
Figure 6.17

Muscles of the Pelvis & Hip
Figure 6.19c

Muscles of the Thigh

Muscles of the Lower Leg
Figure 6.20

Muscles of the Arm

Muscles For Injections

Superficial Muscles: Anterior
Figure 6.21

Superficial Muscles: Posterior
Figure 6.22

G.Muscular Development
In embryo, muscular system develops quicklyMuscles have to cover and move bones of limbs
Nervous system invades muscles to allow conscious control
Skeletal movements occur by 16th week of developmentFetus will start moving around 14th weekSucking thumb, tugging, kicking

Fetus at 16 weeks

Development occurs in:cephalic/caudal direction (head to toe)
Can raise its head before it can sit upCan sit up before it can walk
Proximal/distal directionCan wave “bye-bye” before it can hold a pencil

Due to rich blood supply, skeletal muscles are resistant to infectionable to repair/regenerate selves very efficiently
Aging will alter muscle ability and can lead to atrophyAmount of connective tissue increases, muscle tissue decreasesLeads to stringy/sinewy musclesLeads to decreased body weight/mass
Muscle strength decreases by about 50% by age 80
Continued or new dedication to weight-bearing exercise (pumping iron) will offset or reverse effects

Jack LaLanne, at age 83 (left), and 93 (right)Often referred to as the Godfather of Fitness, Jack
Lalane was a pioneer in American fitness. He advocated healthy eating and daily weight training exercises starting in the 1930s.

H. Diseases/Homeostatic Imbalances
Two major diseases affect muscles:Muscular dystrophy: genetic disease group in which muscles degenerate due to fat and connective tissue deposits
Myasthenia gravis: autoimmune disease in adults of general weakness and fatigability as a result of shortage of ACh receptors

Muscular Dystrophy (MD)Nine different types of muscular dystrophy in which all are genetic and result in degeneration of voluntary and sometimes involuntary muscles
Most common (and most serious) type is Duchenne’s MD X-linked (affects males almost always)
Diagnosed between ages 2 – 6

Active, normal-appearing children become clumsy and begin to fall as muscles start to weakenFirst muscles stricken are around hips, pelvis, thighs, and shoulders
By early teens, attacks involuntary muscles like heart and respiratory muscles

A group of interdependent proteins along the membrane surrounding each fiber helps to keep muscle cells working properly. When one of these proteins, dystrophin, is absent, the result is Duchenne muscular dystrophy; poor or inadequate dystrophin results in Becker muscular dystrophy.

Myasthenia Gravis (MG)
Chronic autoimmune neuromuscular disease characterized by varying degrees of weakness of the skeletal (voluntary) muscles of the body.
First signs are weakness in head and neck muscles droopy eyelids (orbicularis oculi), difficulty chewing (masseter), swallowing & talking
May eventually lead to difficulty breathing

Result of shortage of ACh receptors available to receive AChAntibodies bind to ACh receptors which prevent them from binding AchBody thinks receptors are foreign body so produces antibodies to fight it off
Receptors not triggered lead to weakened contractions


Test Wednesday, November 23
The End