the medical decoder fall 2013
DESCRIPTION
Northwestern University's premier undergraduate medical journalTRANSCRIPT

MD THE MEDICAL DECODER
Population Health:
Produced byPhi Delta Epsilon
IL Gamma Volume 2
A Glimpse at Future Health Technologiespg. 4
Making the Career Choice: What are Your
Options?pg. 29
Composure and Compassion: The Medical School Interview
pg. 10
A Call For Value-Based
Healthcare

Features
2 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma
04 A Glimpse at Future Medical TechnologiesAsia Jaros
20 How Baby Boomers Will Change Orthopedic CareHeather Ables
32 Scalp Cryotherapy: Changing the Face of CancerDevora Isseroff
07 Where Does Alternative Medicine Belong?Roy Yu
23 Population Health: A Call for Value-Based HealthcareZach Snow
34 Primetime PrescriptionsRachel Sibley
10 Composure and Compassion: Medical School InterviewBen Fox
26 Emergency Contraception: A Quick Guide to the Morning AfterSarah Smith
40 References
Making the Career Choice: What are Your Options?Varsha Venkatakrishna
29
Cover photo courtesy of www.skeptikai.com
Cour
tesy
ww
w.n
orth
wes
tern
u.tu
mbl
r.com

Editors in ChiefAditya GhoshWCAS ‘15Sarah SmithWCAS ‘15
Associate EditorsSavan PatelSOC ‘13Mahir KhanWCAS ‘15Charlotte ter HaarMEAS ‘14Anthony AnguieraWCAS ‘14Kevin ZhaoWCAS ‘16Devora IsseroffWCAS ‘15Roy YuWCAS ‘16Alex PezeshkiWCAS ‘13
Writing StaffAsia JarosWCAS ‘14Ben FoxWCAS ‘13Zach SnowWCAS ‘14Roy YuWCAS ‘16Rachel SibleyWCAS ‘15Heather AblesWCAS ‘14Varsha VenkatakrishnaWCAS ‘16Devora IsseroffWCAS ‘15
Design StaffBrandon CaldwellWCAS ‘15Jess GuenzlWCAS ‘16
Creative DirectorSvetlana SlavinWCAS ‘16
PhotographerBryan HuebnerWCAS ‘16
ModelsTricia CruzWCAS ‘17Rachel SibleyWCAS ‘15 Roy YuWCAS ‘16Heather AblesWCAS ‘14Asia JarosWCAS ‘14 Kevin ZhaoWCAS ‘16Bethanie WillisWCAS ‘16
Volume 2 ■ Fall 2013 ■ 3
Left to right: Roy Yu, Arpan Patel, Charlotte ter Haar, Asia Jaros, Heather Ables, Rachel Sibley, Svetlana Slavin, Kevin Zhao, Aditya Ghosh, Bryan Huebner (not pictured: Sarah Smith, Savan Patel, Mahir Khan, Anthony Anguiera, Devora Isseroff, Alex Pezeshki, Ben Fox, Zach Snow, Varsha Venkatakrishna, Brandon Caldwell, Jess Guenzl, Trica Cruz, Bethanie Willis)

I n 1990, the US Department of Ecology and
National Institute of Health began its now
world-renowned Human Genome Project. The
project’s mission was to identify over 20,000 genes
in human DNA, sequence over 3 billion chemical
base pairs, and offer innovative treatment and di-
agnostic tools.1 At the time, the idea of sequenc-
ing a genome was a distant dream. Today, nearly
twenty-five years after the initial undertaking of
the project, genomic sequencing is available to the
public at $3,000-5,000
per genome, and costs
continue to decrease as
more efficient techniques
are developed.1
The medical field con-
tinues to move towards
new technologies, facili-
tation of treatments tailored to
the patient, and the use of less invasive medical
procedures. By the time our generation of physi-
cian-hopefuls leaves medical school, a new slew of
technologies and therapies will undoubtedly sup-
plement, if not replace, some of the current meth-
ods. With the advancement of medical care and
higher levels of disease control, researchers and
doctors have now started tackling more complex
pathology issues.
One such issue that Dr. Anthony Atala of Wake
Forest University Center of Regenerative Medicine
battles on a daily basis is the disparity between
organ availability and demand.2 While the exten-
sion of the average human
lifespan is considered
an achievement in the
medical field, Dr. Atala
reminds us of a painful
reality: as human lifes-
pan increases, the num-
ber of patients with fail-
ing organs increases. Yet,
the number of transplants continues to remain
nearly the same despite the higher demand for or-
gans and a low supply. Today, over 116,000 patients
By AsIA JAros
Color- Coded surgery and organ Printing
The medical field con-tinues to move towards new technologies, facili-tation of treatments tai-lored to the patient, and
use of less invasive medical procedures.
4 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma
A Glimpse At Future HeAltH tecHnoloGies

anxiously await a new organ on the national trans-
plant list.2,3 Dr. Atala hopes to offer an innovative
approach to the organ shortage problem with an
unusual solution - organ printing.
At his laboratory, where he performs clinical trials,
Dr. Atala uses a CT scanner to scan the patient’s fail-
ing organ. This allows him to obtain exact dimen-
sions and densities of the specific patient’s organ
and customize the design. He then connects this
scan to a 3-D printer, similar to an ink printer. The
3-D organ printer uses cells extracted from the pa-
tient’s own tissue to recreate a copy of the scanned
organ.2
In his 2011 TED talk, Dr. Atala jokingly likened or-
gan printing to “baking a layered cake.”2 His pecu-
liar analogy rings true upon taking a closer look at
the biomechanics of organ recreation. On average,
the process of printing a complete organ takes ap-
proximately 7 hours.2 It requires a printer that can
elevate from level to level as it builds the organ, cell
by cell, similar to stacking and frosting a layered
cake. Although Dr. Atala has been able to recreate
several major organs including the heart and kid-
ney, his project is still in the clinical trial phase and
the organs have yet to be implanted in humans. His
current challenges are: the design of materials that
are not rejected by the patient’s body, the culturing
of stem cells outside of the patient (i.e. liver, pancre-
atic, and nerve cells which are particularly depen-
dent on a human environment), and tissue integra-
tion once implanted into the patient.2,3
Printed organ implants may not be the only nov-
elty on the medical horizon. Dr. Quyen Nguyen, the
director of surgery at the University of San Diego, is
researching the use of a fluorescent probe to flag
tumors and cancers excised during surgery.4,5 A ma-
jor issue with current tumor removal procedures
involves ensuring complete tumor removal during
surgery. This is generally based on a judgment call
by the surgeon about the margins of the tumor,
which are not easily seen with the
naked eye. Experienced surgeons
judge the extent of the tumor by
its size and location based on prior
imaging evaluation of the area,
proximity to other structures, and
by feeling the tumor. This method-
ology is not only inconsistent, but
also highly inefficient and time-consuming. Often-
times, residual portions of the tumor are left at the
margins of the excision area, and these portions re-
main undetected until the excised tumor has been
In an effort to reduce the number of nerve-related injuries surgeons are creating technology to tag nerves with fluorescent green molecules that can increase the visibility of these nerves drastically.
Cour
tesy
Dis
cove
r Mag
azin
e
Volume 2 ■ Fall 2013 ■ 5

analyzed by a pathologist. If residual, abnormal tu-
mor cells are present at the margins of the removed
mass, a patient may need to undergo multiple ad-
ditional surgeries, chemotherapy, or radiation to
eliminate the rest of the tumor.4
Dr. Nguyen’s approach involves using a molecular
marker made of fluorescently tagged-polycation,
polyanion, and a linker.4,6 Polycationic materials
tend to adhere to all cells, unless they are attached
to a polyanionic component. This polyanionic com-
ponent restricts the polycation from binding to any
cells. The key to tagging only cancerous tissues is a
linker between the polyanion and polycation por-
tions, which contains a specifically engineered cut-
ting site. This site is tailored so that it can only be
cut by tumor-specific enzymes, for example, prote-
ases, that are present only in cancer tissues. When
this three-part molecular marker is injected into a
cancer patient, enzymes within the tumor cut apart
the polycation from its polyanionic counterpart,
allowing it to bind to tissues and fluoresce. Dur-
ing surgery, the operating surgeon is able to see
exactly where the tumorous spots are by simply
observing fluorescent areas and removing them.
Dr. Nguyen’s idea could have a profound impact
on all types of tumor removal, but especially for
tumors that are located in sensitive areas such as
the brain.6
The myriad of simple, yet ingenious medical
technologies doesn’t stop there. In fact, organ
printing and color-coded surgery just scratch the
surface of what is to come. Current research is be-
ing conducted on self-administered, high-speed
voice-based tests to diagnose Parkinson’s disease,
new gamma-ray cameras to detect tiny tumors up
to two-fifths of an inch within dense breast tissue,
implantable, radio-frequency identification chips
for humans that would carry our medical histo-
ries, insurance information, and more.5,7 It is our
responsibility and challenge as future healthcare
professionals to educate ourselves and continue
this legacy of innovation. If we can expand medical
research to incorporate non-traditional fields such
as mathematics, engineering, economics, psychol-
ogy, and other disciplines to supplement current
technologies, the results will definitely exceed our
current expectations and, more importantly, help
save lives.
For more information check out the online TED
Talks series: The Future of Medicine. ■ MD
For references, see page 40.
3D bioprinting holds tremendous potential for dealing with the rise in demand for organ transplants.
Cour
tesy
ww
w.m
arke
tbot
.com
6 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

g rowing up in a Korean-American home
has given me a unique experience that
enables me to find valuable lessons in a variety of
situations. My attitude toward health, for example,
is rather unorthodox because of the way my par-
ents dealt with sickness. Of course, I had my regular
checkups with the pediatrician like everyone else,
but there were several instances where my parents
would provide home remedies. In retrospect, I had
no idea why my parents’ methods worked.
When most people
have indigestion,
they may take an ant-
acid or Alka-Seltzer.
My mom, however,
would use a different home remedy: acupuncture.
First, she would rub my back and arms so that the
blood would flow towards my fingers. Then she
would tie my thumb with a rubber band to constrict
blood flow, prick the part of flesh where the thumb
meets the fingernail, and let the blood out. As she
gently pressed on my thumb, a dark maroon liquid
would ooze out. While the treatment may sound
like it would have no effect, from personal experi-
ence, I can testify that this works like a charm. Af-
ter about fifteen minutes, I would always feel much
better.
As I grew older, I became fascinated and intrigued
by the therapeutic effects of these treatments. Af-
ter doing a bit of research, the best explanation I
could find was based on
the concept of qi in Chi-
nese traditional medi-
cine. Qi (pronounced
“chi”) is the vital force or
energy responsible for controlling the human mind
and body. It flows through the body via channels,
or pathways, which are called meridians. Imbal-
ances in the flow of qi cause illness; correction of
this flow restores the body to balance. Each organ
About 40% of Americans are using some form of alternative medicine.
Where Does
AlternAtiveMeDicine
Belong?
Volume 2 ■ Fall 2013 ■ 7
By Roy Yu

has its own qi, whose activity is characterized by
the organ to which it is attached.1 In the case of an
upset stomach, these energies have collided with
each other. The human hand has certain acupunc-
ture points that are assigned to each qi. Therefore,
pricking the thumb tip sends signals to manage the
unbalanced qi.2
By now, you are likely
thinking that this stuff is
either really interesting or
a bunch of nonsense. How
can releasing a few drops
of blood cure indigestion?
When I try to explain it
to my non-Asian friends,
they look at me suspiciously or even laugh. While
it certainly may be a placebo effect of the interven-
tion, there is emerging literature that acupuncture
and other forms of alternative medicine can be ef-
fective for certain conditions or ailments.3
The National Center for Complementary and Al-
ternative Medicine (NCCAM) notes that the terms
“complementary, alternative, and integrative medi-
cine” refer to health care approaches with a history
of use or origin outside of mainstream medicine.4
They include natural products such as herbs and
supplements, as well as mind and body practices
such as acupuncture and massage.4 Other examples
include homeopathy and naturopathy. Homeopa-
thy is a system
of medicine that
involves treat-
ing people with
highly diluted
substances in
order to trig-
ger the body’s
natural system
of healing. It is based on the doctrine of “like cures
like”, which states that a substance that causes the
symptoms of a disease in healthy people will cure
similar symptoms in sick people.5 Naturopathy, or
naturopathic medicine, is a system of medicine
based on the healing power of nature. Naturopathy
is a holistic system, meaning that naturopathic doc-
tors attempt to find the cause of disease by under-
standing the body, mind, and spirit of the pa-
tient. Most naturopathic doctors use a variety
of therapies and techniques, such as nutrition,
behavior change, and herbal medicine.6
Over the recent years, as knowledge of alter-
native medicine techniques have evolved, the
medical field has started to understand the
Over recent years, as knowl-edge of alternative medicine
techniques have evolved, the medical field has started to understand the inherent
benefits of these techniques and has begun incorporating
it into medical care.
Cour
tesy
ww
w.fl
ickr
.com
8 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

inherent benefits of these techniques and has be-
gun incorporating it into medical care. About 40%
of Americans are using some form of alternative
medicine.4 Many medical schools are also starting
to teach these medicine techniques and theories.7
Several health care providers offer alternative med-
icine in conjunction with conventional therapies,
which is known as “complementary medicine”. The
main difference between alternative and comple-
mentary medicine is that while alternative medicine
is often used instead of conventional techniques,
complementary medi-
cine is used in addition
to them. The combina-
tion of complementary
and alternative medicine
(CAM) with mainstream
medical therapy is called
“integrative medicine.”
Integrative health care
programs are rapidly being incorporated into gen-
eral medical care, as there is new research demon-
strating the immense benefits of this type of care
for the patients. Some cancer treatment centers of-
fer services such as acupuncture and meditation to
help manage symptoms and side effects of conven-
tional cancer treatments, such as chemotherapy.3,4
The scientific basis of medical care emphasizes
that treatments be utilized when they have been
shown to be safe and effective. Some CAM thera-
pies have not shown significant benefit but do not
cause harm and the extent of relief for patients with
a certain therapy may be variable. There is scientific
evidence that supports the use of acupuncture for
cancer related side effects such as nausea, vomiting,
hot flashes, depression and insomnia.3 In another
study, cancer related symptoms of pain, fatigue,
anxiety and depression improved with massage
therapy.8 I am sure that some forms of CAM may
have shown little or no effect. However, research
has clearly shown benefits to certain patients with
use of CAM therapies.
As health care policy
makers decide which
types of treatment are
covered by insurance, I
hope that complemen-
tary and alternative
medicine treatments
are given more consid-
eration in the treatment of the patient. Ongoing
research on CAM can help ensure that patients are
benefited from combining variety of treatment mo-
dalities to ensure the best and sustained long-term
treatment success and health.
■ MD
For references, see page 40.
Integrative health care programs are rapidly be-
ing incorporated into general medical care,
as there is new research demonstrating the im-mense benefits of this
type of care for patients.
Volume 2 ■ Fall 2013 ■ 9

‘r efreshingly finite’ is how I’d describe my
feelings as I traveled home from my medi-
cal school interviews. Although my interviews were
the challenging, final hurdles in an extended and
rigorous application to medical school, I walked out
feeling confident I had done my best in communi-
cating why I deserved a seat in medical school. As
I am now in medical school, and given my experi-
ences with this process, my goal is to communicate
the strategies I used while interviewing in hopes
that it can help improve your own interview per-
formance and allow you to also emerge confident
from your medical school interviews. While there is
certainly an exhaustive amount of published advice
on interviewing, I have boiled it down to the most
essential tips that I have learned over the course of
my application process. I will begin with a short in-
troduction to the interview process and then relate
twelve important tips that greatly improved how I
presented myself on interview day.
ComPosure andCompassion
The MedIcAl school InTervIew
By Ben Fox
10 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

Simply put, interviewing is perhaps the single
greatest opportunity you will have to prove your-
self to a medical school. Admissions officers review
thousands of redundant sounding GPAs, MCAT
scores, and personal statements that can all blur to-
gether after a while. Fortunately, the interview pro-
vides you with a great opportunity to distinguish
yourself from the sea of applicants. The interview
is your best chance for a medical school to ascer-
tain your character, motivation, and determination.
The written material in your AMCAS primary appli-
cation can only go so far in representing you as a
person, unlike interviewing, which provides you a
critical opportunity to relate to someone during the
admissions process. Your ability to interview can be
a deciding factor during the admissions process,
and if approached correctly, will convince medical
schools you are indeed a good fit for them.
Upon receiving your first interview invitation,
feel confident you will succeed, as much of the
pre-screening of applicants has already been per-
formed. Schools sometimes review upwards of ten
thousand applications and must be highly selec-
tive in who they choose to interview. Thus, a large
majority of applicants to most schools don’t receive
interviews - a disappointing but almost inevitable
outcome for many applicants. Do not feel discour-
aged if you are declined an interview by many of
the schools you apply to as almost all applicants
experience the same thing. In my case, I received
only three interviews after applying to thirty-plus
schools total! While frustrating, I made the most of
those three interviews and realized the high de-
cline rate was happening to most other applicants
as well. In reality, receiving an invitation is actually
more difficult than gaining admission after inter-
viewing. An applicant has anywhere from a 33-50%
chance of gaining admission after receiving an invi-
tation to interview. Thus, receiving an invitation is a
huge accomplishment in and of itself and a reliable
indication that the medical school already deems
you a worthy candidate for their program.
Every school is a little different in terms of how
they interview, but generally, interviewing is con-
ducted in three broad ways. The first entails the
‘traditional’ one-on-one interview, where the appli-
cant is paired with a physician, faculty member, or
admissions advisor for anywhere between thirty to
sixty minutes to discuss the applicant’s motivation
for entering medicine. The second type consists
of a ‘panel’ interview where two to five applicants
are paired with one or two interviewers. Usually,
a question is given to all the applicants, who then
answer in turn. The final type of interviewing is the
multiple mini-interviews (MMI), which is a relative-
ly new interviewing style currently used by fewer
than twenty U.S. allopathic medical schools. Broad-
ly, MMIs have applicants answer eight to ten ques-
tions in separate rooms with different interviewers
over the span of an hour. For each room, the appli-
Volume 2 ■ Fall 2013 ■ 11

cant reads a question prompt for two minutes and formulates an answer. The applicant then enters the
room and discusses the answer for six to eight minutes with the interviewer who may provide new infor-
mation to the prompt. At time’s end, the interview repeats the above process until all rooms have been
completed. I encourage you to research the MMI process heavily if you interview at a school that conducts
them. There is definitely much more strategy and information on MMIs than can be related here. Overall,
each interview style presents its own unique challenges. As such, some schools use a combination of in-
terviewing styles or hold multiple interviews. For example, some schools have applicants complete both
a traditional and panel interview, while other schools may have an applicant complete two traditional
interviews with separate faculty.
Whatever the style, I am confident you will find your interview day to be really low-stress and very laid
back. It may feel daunting when twenty to seventy other applicants are interviewing alongside you, but
it is important to calm down either before or during the early stages of your interview. The schools know
interviews are highly stressful, and as such, they take steps to calm you down throughout the day. Many
schools provide a lunch, a Q-and-A session with current students, and a tour around campus. Impor-
tantly, schools do not want you to be distressed by the interview. They have spent a huge amount of time
and energy screening you and thus want to judge your calm and confident self when your motivations
for medicine are clearest. To help you convey your motivation clearly, I will now present the twelve most
important interviewing tips that I feel will help you in developing your interviewing skills. While some tips
seem obvious, you may be surprised when you find yourself making these common mistakes initially, as
many applicants do. However with practice, you will target your weaknesses and eventually become a
more effective and memorable interviewer.
twelve tiPs on mediCal sChool interviewing
1. do not rambleSometimes less is more. Rambling is one of the biggest mistakes made by novice interviewees. It con-
veys that you are nervous or feel unprepared to answer the question. Interviewers are constantly sizing
you up to see whether you would make a competent future colleague of theirs in the medical field where
communicating clearly is of utmost importance. Your goal then is to be logical, clear, and succinct when
speaking. If you do have a tendency to ramble, do not be discouraged as you can easily break the habit. By
12 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

mock interviewing with a friend or family member, you can quickly identify if you ramble and learn how
to break the habit. Importantly, your mock interviewer must be up-front and tell you if you are rambling,
which brings us to a second key point of interviewing preparation.
2. PraCtiCe with Friends and Family You must practice, practice, practice for medical school interviews. You have only one opportunity with
each school, so you will definitely to want prepare and make the most of it. I, along with other applicants
I knew, practiced primarily with friends and family who would give honest feedback about our interview-
ing skills. Either I would tell them a list of questions I wanted them to ask or allow them to surprise me
with their own questions. Importantly, I would explicitly ask them to tell me what they honestly thought
about the interview and where I could improve, no matter how harsh their criticism might be. You NEED
people to help you constructively and not try to sugar coat things.
To further simulate the interview environment, I also tried mirroring the actual conditions of the inter-
view based on descriptions found on studentdoctor.net, a useful resource for interview preparation. This
meant practicing in an unfamiliar environment (not your own living space) and mock interviewing for the
appropriate duration of time (45-60 minutes usually). It was also useful when my mock interviewer and I
would occasionally stop to review a question and determine how I could improve my responses.
3. PrePare For Questions Commonly askedThere are some questions you will encounter again and again while interviewing at different schools.
A list of twelve such questions will be presented in the next edition of the Medical Decoder. These are
questions for which you will certainly need well thought-out answers, and while they may not all be asked
in every interview, they come up on a consistent basis. You must practice what you are going to say for
them or at least have a good idea of how you will answer them. I found it useful to keep a word document
briefly describing my answers for each of the questions. I also wrote down my answers and took the sheet
to each interview for a last minute review.
At the same time, it is extremely important that your answers do not sound rehearsed. The interviewers
know that you have probably practiced for the interview, but they do not want to listen to a memorized
recitation. Your goal is to communicate your predetermined answer as though you have never answered
Volume 2 ■ Fall 2013 ■ 13

the question before - with passion and genuineness. I’ll stress again that you must practice. I had a friend
who hoped to sound more genuine and thoughtful by not practicing. Unfortunately on his interview day,
he became tongue-tied and came off as unprepared. While very intelligent and well qualified, he was
rejected. This goes to show that you cannot anticipate the environment or how you’ll be feeling on the
interview day. While you cannot control these factors, you can control how well you have prepared.
4. review your Primary aPPliCation, esPeCially the Personal statement
Your interviews will often focus on the experiences detailed in your AMCAS primary application. Even
if the interview is “closed,” meaning the interviewer has never reviewed your application, you can still
answer questions based on your experiences. Your college experiences, in some way, should relate to the
pursuit of your dream of becoming a doctor. Therefore, they should be easy to talk about since you are
already passionate about them. In general, for my experiences, I would sum up each one into two or three
important points that I could tie back to medicine and how it strengthened my resolve towards becom-
ing a physician. For instance, I used the time I spent volunteering at a nursing home as one of the college
experiences I brought up while interviewing. During my interview, I told how working with patients with
dementia was initially frustrating; I first arrived to a circle of seemingly asleep residents all in wheelchairs.
I came to realize that they were, in fact, awake, and that the stimulation I provided through fun activities
was important to their well-being. I managed to effectively communicate to my interviewer how each
lesson I learned during that volunteering experience related back to a quality of being a competent doc-
tor. To sum up, know your application. By re-reading your personal statement, and having two to three
important points to discuss for each of your experiences, you will come across as a smoother, more col-
lected, and an altogether more genuine and strong applicant.
5. Familiarize yourselF with issues ConFronting healthCare today
You must show interest in the field you desire to go into, plain and simple. In medicine, this means being
aware and moderately knowledgeable about larger issues facing modern healthcare. For example, I was
14 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

asked for my opinion about Obamacare twice, and it is very possible that depending on your major, i.e.
public health or political science, you could receive more questions on this topic. In general, I recommend
being aware of and retaining some general knowledge in the following healthcare issues: 1) Physician
Shortage and Their Crowded Distribution; 2) The High Costs of Healthcare; 3) Increasing Prevalence of
Chronic Disease; and 4) Understanding the Basic Goals of the Affordable Care Act (ACA). Interviewers do
not expect a 22 year-old premed to provide a panacea to these issues, as they are often complex issues
that have been around for decades now. Rather, they want to see that you are familiar with these issues
and can hold an intelligent conversation about them. It may best to be non-committal with these issues,
by addressing multiple sides that each issue presents and adequately demonstrating your knowledge. In
the end, questions dealing with larger healthcare issues probably will not make or break your interview.
After all, they do less in answering the interview’s overall purpose of why medicine is right for you in com-
parison to other questions. However, I do believe that schools respect an applicant more so if they can
demonstrate basic knowledge of these important health-related issues.
6. stay alert on your interview day Interviews days are not solely for conducting interviews. They may be 7 to 8 hours long and consist of
multiple presentations, a lunch, and a campus tour. While most of the material presented to you is infor-
mation you could easily find on the school’s website, the schools are in the business of attracting you.
After all, medical schools have selected you to interview after sorting through thousands of secondary
applications, and want to show that they offer a quality medical education. That being said, remaining
energized and alert is necessary throughout the interview day.
Generally, not all applicants will interview at the same time - some will be in the morning, some after
lunch, and others late in the afternoon. You have to be prepared to interview at any time of that day. I sug-
gest bringing a bottle of water that you can refill as needed and a quick snack such as a candy or a granola
bar. Another advantage of staying alert and not dozing off through the presentations is that the present-
ers may later be your interviewer! This is especially true in MMI interviews where at least 8-10 interviewers
are needed to fill all question prompts. Overall, the goal here is for you to walk into the interview room
feeling awake, confident, and ready and to give it your best shot.
Volume 2 ■ Fall 2013 ■ 15

7. Provide memorable examPles
Interviewers need something to remember you by. One of my interviewers told me she was my ‘advo-
cate’, and it was her job to present my interview summary to the admissions office. Your advocate should
be able to convey not only their general impression of you but also your memorable and meaningful an-
swers. For example, if asked, “What has prepared you for a career in medicine?” or “What is your greatest
strength?” you should avoid being vague. If you are vague, you risk sounding like another average appli-
cant. Instead, you should focus on a few strong personal examples in some detail that work to distinguish
you in a positive light. Your examples could include a value you stand by, a specific person you’ve worked
with, an interesting class that stuck with you, or an experience from your primary application (that’s why
having 2-3 talking points per experience can be extremely helpful!). Overall, personal examples allow you
to showcase your personality, help you relate better to the interviewer if they’ve had a similar experience,
and above all, give you the best chance of turning the interview into a conversation. If you can develop
stretches of good conversation rather than a question-answer-repeat format, then you will have a suc-
cessful interview.
8. use three talking PointsDuring interview preparation, you will often wonder if your answers are too lengthy, too short, or lack-
ing substance. A great solution that a friend relayed to me is to divide your answer into three talking
points. Her idea was that two points tends to be too short and four points brings the risk of you rambling.
Three points strikes a happy medium, giving you the best chance of being succinct yet complete. While
by no means set in stone, I found using three points to be extremely helpful. For instance, my “why medi-
cine?” answer consisted of three larger points describing my healthcare-related experiences growing up,
in college, and desired ones in the future. Moreover, using three points was essential during my MMI
interview as I had only two minutes to read a question, consider my answer, and formulate what I would
start off presenting, which almost always consisted of three talking points. I simply could not remember
much more than three main points anyway after a quick two minutes.
16 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma
9. answer Questions while aCknowledging all Parties involved
You will want to consider all people’s views in a complicated interview question. Doing so shows you
can relate to others and identify their motivations while being the advocate for the patient, an impor-
tant skill for all physicians. Though you want to apply this advice to all questions, this tip applies very
well to two questions you might encounter. The first concerns a fellow medical student who you know
has cheated on an exam, but no one else does. Instinctively, you might alert the professor immediately;
however, doing so bypasses your classmate, risks your friendship with that person, and potentially blows
the problem out of proportion. In general, you want to handle situations with the least amount of drama
possible. In this case, confronting the classmate privately and encouraging them to seek out the professor
on their own is the advisable action - you have considered and involved them in the decision. Put another
way, what would you want your friend to do if you were the cheater: rat you out or talk to you on his or
her own? The second question you may encounter concerns the hypothetical situation where an elderly
patient is diagnosed with a terminal illness, but a family member does not wish for the patient to know
in fear that the truth will be devastating. Here, you have to balance your patient’s needs along with the
family member’s and be able to recognize what each would stand to gain or lose based on your decision.
No matter how you answer, explore and consider each party’s needs and then adequately communicate
to the interviewer you have done so.
10. ask For time to ColleCt your thoughts“Can I take a few seconds to think about it?” I must have said this a dozen times while interviewing.
While initially practicing, there was always that urge to begin answering right away, and typically, my
responses would be disjointed, as I was using too much effort to both talk and think at the same time.
After a friend suggested that I take time to formulate an answer, my response would almost always come
out better and more logical, showing me that taking time to think was absolutely necessary for difficult
interview questions. Many questions are geared to make you think critically and thereby require time in
order to clarify your thoughts and come up with a coherent answer. Although it initially felt awkward ask-
ing for additional time, my interviewers never had a problem with it and would wait patiently for ten to
fifteen seconds sometimes before I began. By asking for time, you improve your chances of avoiding long
Volume 2 ■ Fall 2013 ■ 17

winded or boring answers that verge on rambling. In my opinion, asking for time is another way you show
poise while interviewing - you come across as a more thoughtful interviewee.
11. ask genuine Follow-uP Questions Again, interview days are both for schools and applicants. Therefore, feel free to ask one to three ques-
tions at your interview’s conclusion to further familiarize yourself with the school. For example, you could
ask about a unique aspect to a particular medical school such as a strong public health component in the
curriculum or interesting summer research opportunities. You could also ask about the student body,
the atmosphere within the school, or life outside the school. While these questions can vary greatly, your
overall goal is to be genuine in your asking. Three well thought out questions can go a long way rather
than tacking on three piecemeal questions at the end.
In general, I would advise preparing one to three genuine questions before arriving at your interview
day. While you do not have to use them, it’s good to have these back-ups if other questions do not come
to mind on the interview day. All in all, asking good questions is another important way to show interest
in the school and that you’ve done your homework on the school’s specific program. This is attractive to
medical schools and lets them know you have seriously considered their program.
12. ComPosure, ComPosure, ComPosure
If I had to summarize what applying to medical school was like, I’d say it was all about maintaining com-
posure. The application process is extensive and must be balanced with other course work and responsi-
bilities. Through it all, you will help yourself by maintaining your composure, especially during interviews.
Some questions are just intended to be tricky and difficult. Indeed, the follow-up questions during my
MMI interview seemed geared to make me second-guess or reconsider my first answer. Generally, I stood
by my first answer since I believed it to be right; however, the more important goal was to maintain my
poise and not appear rattled. I would rationally consider the new information and use it to support my
first answer. This showed self-confidence, which is a quality your interviewer will definitely be looking for.
18 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

ConClusion
Interviewing really is one of the only opportunities to put a face to your application. While GPAs
and MCAT scores certainly weigh heavily, interviewing provides the admissions officers with a
unique perspective of you as a person - one that can be a deciding factor in their decision to accept
you.
On the day of, I think you will find your interview not to be too stressful. Obviously walking into
the room can be daunting to anyone, but you will become comfortable after a little while. From
that point, maintain your composure and be passionate about what you speak of. Try your best to
prove to the interviewer that you are a worthy future colleague of theirs in medicine. Be sure to sit
upright, vary the tone of your voice, answer with an appropriate level of enthusiasm, and turn your
interview into a conversation. By doing these things, you give yourself the best chance of coming
across as likeable yet professional.
I also encourage you to enjoy your interview day and the interviewing experience in general. For
many applicants, interviewing entails traveling to new parts of the country and meeting applicants
from other schools. Talk with these other applicants and have some fun with the process. Not only
will you learn a lot from other applicants, but you will also calm down before your interview.
In the end, medical school interviewing is all about communicating your passion for medicine. If
you can demonstrate your passion for helping others, your interview will be successful, regardless
of whether or not you occasionally stumble on a question. The above tips will hopefully help you
best prepare to communicate this passion in the clearest manner. From here, continue practicing
your interviewing skills and asking your friends and family to critique you while doing so. These tips
are meant to be a foundation for you to build upon. By utilizing these tips and maintaining your
composure, you will undoubtedly succeed during your interview and end your medical school ap-
plication on a resounding high note. ■ MD
Volume 2 ■ Fall 2013 ■ 19

how baby boomers will Change
orthoPediC Care
GPA, MCAT, and the coveted MD. The lives of premed students are flooded with acronyms. At the under-
graduate stage of an aspiring doctor’s life, it is easy to get caught up in the preparations necessary to gain
acceptance into medical school and lose sight of the challenges that we will face when we finally have
become doctors.
While I frantically refresh CAESAR during grade posting time, I also dream of becoming an orthopedic
surgeon. However, it was only recently, after I had a shadowing experience with a physician that I realized
I knew surprisingly little about the future of the profession and the obstacles I might face. This experience
was the first time that I was challenged to look beyond just the task of becoming a doctor and consider
the larger impact that I hoped to have on the medical field. After shadowing, I realized that my responsi-
bilities as a practicing surgeon would depend largely on the patient population that I would be account-
able for.
Those of us who will soon be entering medical school will be responsible for the care of a unique group
of elderly patients: the Baby Boomers. According to the United States Department of Health and Human
Services’ Administration on Aging, in 2009, 12.9% of the total US population was over the age of 65. By
the year 2030, this percentage is expected to rapidly increase to 19% as the Boomers will begin seeking
By heATher ABles
Medical advancements made during Baby Boomers’ lifetimes such as the polio and measles vaccines, as well as new surgical
technologies, have allowed them to live lon-ger and have raised their expectations of
medical care.
20 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

more medical treatments.1 This rise would correlate
with an increase in the number of elderly individu-
als seeking healthcare services in order to manage
chronic pain conditions and combat the woes of
aging.
While the expanding number of healthcare servic-
es that Baby Boomers will require poses a challenge
to medical specialists, this patient population also
brings another challenge due to its unique posi-
tion in history. Medical advancements made during
Baby Boomers’ lifetimes such as the polio and mea-
sles vaccines, as well as new surgical technologies,
have allowed them to live longer and have raised
their expectations of medical care. According to a
2007 report by the American Hospital Association,
new pain management techniques and the option
of joint replacement surgery have allowed aging
Baby Boomers to maintain a more active lifestyle
than their ancestors.2 As a result, these patients are
anticipated to continue to seek orthopedic services
that emphasize mobility and independence.
Unfortunately, it does not appear that the
increase in healthcare services needed by a
growing patient population will be met with an
equal increase in the number of doctors avail-
able to provide them. Between 2000 and 2020
the supply of orthopedic surgeons is predicted
to increase by only 2%, while the demand is ex-
pected to increase by 23%.3 During my recent
shadowing experience, I was surprised by the
number of older patients who sought medical treat-
ment for joint pain. For many, the quick fix seems to
be a minimally invasive cortisone injection about
three or four times a year. For others, whose pain
was more debilitating, the only option to alleviate
their chronic conditions, like arthritis, was joint re-
placement.
This option has only become popular within the
last forty years, but in that time hundreds of pros-
thetic joints have been created, tested, and mar-
Unfortunately, it does not appear that the in-
crease in healthcare services needed by a
growing patient popu-lation will be met with
an equal increase in the number of doctors avail-
able to provide them.
Volume 2 ■ Fall 2013 ■ 21
Cour
tesy
Hea
ther
Abl
es

keted. The rapid evolution of joint replacement and
other surgical techniques will undoubtedly be an
asset over the coming years as the Baby Boomers
steadily age and cause an increase in the average
age of patients seeking treatment. In the future,
surgeons hope to use techniques that will allow for
the treatment of more patients, quicker recovery
times, and shorter hospital stays.2
The Baby Boomers have grown up with a focus on
education, and many have been fortunate enough
to pursue advanced degrees.4 Therefore, this pa-
tient population has tended to be more engaged
in its own medical care than previous generations
have been.4 In fact, throughout my shadowing ex-
perience, the orthopedic surgeon had to explain
to several adamant individuals under the age of
fifty why joint re-
placement should
be postponed for
younger patients
like themselves.
Due to joint re-
placement’s abil-
ity to confer optimal mobility, it can be inferred
that this procedure will appeal to Baby Boomers
as it can drastically reduce pain levels. Studies are
showing that joint replacement surgeries are on
the rise. It is projected that nearly eight times more
knee replacements will be performed in 2030 than
take place today.5 However, prosthetic joints are
not made to sustain intense physical activity. As
surgeons who operate on younger patients are al-
ready seeing, these patients tend to put excessive
stress on the joint, risk wearing it out more quickly,
and need follow-up operations.
It is undoubtedly im-
portant, as future doc-
tors and healthcare pro-
fessionals, to recognize
how our patient popula-
tion will change in the
coming years and re-
spond by appropriately altering our care and deliv-
ery methods. Not only in the field of orthopedics,
but throughout medical practice, a rigorous focus
on wellness and prevention today will be key to
managing the chronic conditions of tomorrow.
■ MD
For references, see page 40.
After shadowing, I realized that my responsibilities as
a practicing surgeon would depend largely on the
patient population that I would be accountable for.
Cour
tesy
Hea
ther
Abl
es
22 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

PoPulation health
In terms of gross domestic product (GDP),
healthcare constituted more than 17.9% of total
U.S. expenditures in 2012, more than the coun-
try’s highly-controversial defense budget.2,3
With medical spending projected to reach
$4.8 trillion by 2020, experts have deemed the
conventional payment structure known as the
“fee-for-service model” as the primary obstacle
to achieving cost-effective healthcare. In fee-
for-service, which is the traditional model for
By ZAch snow
A cAll For vAlue-BAsed heAlThcAre
Volume 2 ■ Fall 2013 ■ 23
How do YOU value good health? How much is
good health worth? The average American spends more than $8,000 in medi-cal expenses each year. That’s nearly two and a half times more spent on healthcare than France, Sweden, or the UK.1

payment in many hospitals and health systems
across the U.S., physicians are paid based on the
number of medical services they provide. The
doctor profits directly from the sheer number of
operations, procedures, and tests ordered; care is
based on quantity but not necessarily quality.4 In
this model, medical professionals financially ben-
efit most from ordering a multitude of services for
temporary fixes to the patients’ conditions, rather
than from designing treatment plans to improve
patient outcomes and keeping sick people out of
the hospital in the fu-
ture.
Considering the
United States’ global
influence in scientific
research and medi-
cal innovation, why
is it so difficult to cre-
ate a workable, cost-effective system for keep-
ing our citizens healthy? Grounded in traditional
approaches for treating patients, what America’s
medical system needs the most is an alternative
business model, one that incentivizes keeping
people healthy rather than solely treating those
who are already ill.
Population health is a term used to describe
a system of care that seeks to assess the health
needs of a target population and proactively
provide services to maintain and improve the
health of that population. This unique approach,
which has recently garnered significant atten-
tion throughout the healthcare industry, differs
considerably from how most healthcare systems
work today.
The principal difference between population
health and the current health care model is that
population health is focused on caring for groups
of patients rather than individuals; it’s more
about the ‘health’ than the ‘care.’ As an alternative
to utilizing the traditional fee-for-service model,
hospitals seeking to
partake in population
health employ a value
rather than volume-
based method of care.
Value-based care means
that federal health plans
such as Medicare and
Medicaid as well as commercial payers such as
Blue Cross Blue Shield fiscally incentivize hospi-
tals and health systems to limit patient volumes.
In this way, both parties profit from the insur-
ance companies’ savings. Financially speaking,
in the fee-for-service model, hospitals will try to
fill beds; in the population health model they will
try to help empty them.5 The health industry is
actively transitioning to a value-based payment
structure that rewards those who do the best job
at keeping their patients healthy.
The doctor profits directly from the sheer number of operations, procedures,
and tests ordered; care is based on quantity but not
necessarily quality.
24 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

But how are they doing this? First, significant
advances in technology have enabled physicians
and medical facilities to extend healthcare out-
side of the traditional acute-care setting. Tele-
health vendors such as Bosch market products
in remote patient monitoring that can monitor
heart rate, glucose levels, blood pressure, and
other vitals all from within the comfort of the
patient’s home.6 IT solutions such as this, in ad-
dition to physician video-conferencing and mo-
bile phone health applications, are extending
care outside the hospital, thereby freeing beds
for patients with more serious conditions, sav-
ing exorbitant urgent-care costs, and maintain-
ing a healthier environment throughout the
entire population. Furthermore, complex analyt-
ics, like those offered by Explorys, a population
health corporation from the Cleveland Clinic, sift
through petabytes of unstructured medical data
from insurance claims, labs, prescriptions, etc., to
evaluate the risk that certain patients will utilize
emergency hospital services in the future. As a re-
sult, medical professionals can intervene early to
reduce the likelihood that these specific patients
become sick, thereby reducing medical costs and
improving overall population health.7
Despite the need for a hefty investment in new
technologies, the most significant obstruction to
transitioning from volume to value-based care
is reluctance on the part of physicians and other
medical professionals to change their ways.
The population health model requires physi-
cians, particularly primary care providers, to per-
form additional activities and make less money
for them. According to experts in the healthcare
industry, physicians must begin to modify much
of what has been hardwired into their current
practices, experimenting with interventions, re-
configuring office workflow, and delegating more
responsibility to an extended care team.
Still, doctors in contention of this value-based
model ought to remind themselves of the under-
lying principle behind good healthcare: to help
their patients get healthy again. In collaboration
with the innovators making America the global
leader in science and industry, physicians have
the opportunity change the health system, re-
duce the national output of medical costs, and
inevitably, make patients better. That’s the value
of a good healthcare system. ■ MD
For references, see page 40.
Volume 2 ■ Fall 2013 ■ 25
The health industry is actively transitioning to a value-based payment structure that rewards those who do the best
job at keeping their pa-tients healthy.

emergenCy ContraCePtion
A QuIck GuIde To The MornInG AFTer
u nprotected sex happens frequently on college campuses and can have a plethora of negative
consequences, from STI transmission to pregnancy. A study by the National College Health Risk
Behavior Survey found that 15% of college students have, at some point, become pregnant during their
college careers.1 Studies have shown that among this high-risk group of college students, knowledge of
emergency contraception is relatively low. While female college students might know of key words like
Plan B or the “morning after pill”, many are unaware of the function and accessibility of an effective means
of pregnancy prevention post-sex.1 Increasing awareness of emergency contraception (types, how they
work, where they can be bought, regulations, etc.) among college-age women is crucial in order to pre-
vent unintended pregnancy.
The following information comes from leading institutions and research journals focused on reproduc-
tive health and emergency contraception research:
By sArAh sMITh
26 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

what is emergenCy ContraCePtion?Emergency contraception (EC) is a form of birth control, used after sexual intercourse to pre-
vent pregnancy. It is both safe and effective, with no long-term or serious side effects.2 In fact,
EC is even considered safe for those whose healthcare providers recommend not using hor-
monal birth controls out of fear of possible side effects including blood clotting and breast
cancer. This is because emergency use of hormones does not carry the same risks associated
with taking daily oral contraceptives.3
Depending on the type, EC can prevent pregnancy up to five days after sex. However, the
longer the time elapsed between having sex and taking the drug, the less effective the drug is.
Therefore, time is of the essence when using emergency contraceptives.
what are my oPtions?There are three main types of emergency contraceptive pills available in the U.S.: progestin-
only, ulipristal acetate, and combined progestin and estrogen pills.2 Plan B, a progestin-only pill,
is likely the most easily accessible type of EC for college students. In June of 2013, after years of
debate, the FDA has finally approved Plan B for over-the-counter sale with no age restrictions,
meaning that Plan B is readily available in most neighborhood drug stores.4 Especially in college
towns where waiting in line at the pharmacy can be a hot spot for running into peers, the abil-
ity to grab Plan B from the shelf and purchase it without having to show ID can come with the
advantage of discretion. It is not uncommon to find women who keep a dose of Plan B available
in their homes before any accident occurs, so that they can be preemptively prepared.
While Plan B is the most recognized brand of EC pills, it is certainly not the only one. Other
brands available in the US include Next Choice One Dose, Next Choice, ella, and more. While
these brands require a prescription (and a visit to a healthcare provider), they also can provide
advantages depending on the circumstance. For example, while Plan B is effective for up to three
days after sex, ella, an ulipristal acetate pill, is effective for up to 5 days after sex. In fact, ella has
been cited as being more effective than Plan B.2 There are multiple brands of EC pills on the mar-
ket, and it is wise explore those options before the need for EC arises.
Certain brands of daily birth control can be utilized for emergency contraception by taking
combinations of pills. Certain brands of combined progestin and estrogen birth control pills can
Volume 2 ■ Fall 2013 ■ 27

how do they work? Much of the controversy that surrounds emergency contraceptives has emerged from questions re-
garding their mechanism of action, i.e. the biological mechanism by which EC prevents pregnancy.
And the truth is, study of the mechanism of action of many emergency contraceptives has not been
100% conclusive. While it has been established that EC works primarily by blocking or delaying ovu-
lation, questions remain regarding their ability to prevent an already fertilized egg from implant-
ing.4 These questions are vital in the debate on ECs, as many believe that blocking the implantation
of a fertilized egg would make emergency contraceptives abortifacients (drugs that induce abortion).
While literature exists arguing both sides of the debate (either affirmative, some kinds of EC can block
implantation or negative, ECs cannot prevent implantation), there is a rising general consensus that these
contraceptives do not prevent the implantation of a fertilized egg, and therefore do not act as abortifa-
cients (note: this is less established in the case of ulipristal acetate and Copper-T IUDs). The inability of
Plan B to prevent implantation and the pill’s non-abortifacient nature have been well established. How-
ever, it is important to note that emergency contraceptives do not protect against transmission of STIs.
ConClusion
Mistakes happen. Emergency contraceptives can offer a simple solution to avoid unwanted pregnancy
in the face of unprotected sex. While avoiding unprotected sex should obviously be a priority, it is also
important to know what to do if a mistake has been made in order to prevent pregnancy. ■ MD
For references, see page 41.
be taken in higher doses to prevent pregnancy.3 However, it is important to consult with a healthcare
provider before utilizing this method as many women experience side effects like nausea and vomiting.3
EC does not come exclusively in pill form; in fact, the most effective form of emergency contraceptive
is the Copper-T intrauterine device (IUD), which is also used by many women as a form of regular birth
control. While a doctor or trained clinician must insert this form of EC into the uterus, he or she can do
so up to 5 days after sex and this has been shown to reduce a woman’s chance of getting pregnant by
more than 99%.3
28 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

Since the 8th grade, I had a wildly idealistic vision for my future. It involved a crisp, white mono-
grammed lab coat, a shiny stethoscope, and a stack of business cards reading Dr. Venkatakrishna.
My parents, of course, were thrilled by the prospect of having a second doctor in the family and heavily
supported my decision. In fact, when I entered Northwestern University as a freshman, it was with their
assurances that lead me to start my collegiate journey as a premed student.
It has been quite a journey. Between finding a new passion for both creative writing and political sci-
ence, to landing a compelling summer internship in a lab, I waned in and out of being premed at least
fifty times during my first year. In fact, having a weekly career crisis was nothing out of the ordinary by the
time spring rolled around. It was torturous living life on the fence, being too hesitant to commit to either
side; however, when I realized I didn’t have to give up one passion for the sake of the other, I was relieved
of my anxiety.
It is estimated that 30% of incoming freshman across the country share my story, entering as a premed,
but switching to other fields as they progress through their college careers.1 While some of these students
choose to switch to entirely different areas of study, others, due to their affinity for the medical field, opt
for medically-related career paths that accommodate their widening interests.
making the Career ChoiCe
By vArshA venkATAkrIshnA
whAT Are your opTIons?
Volume 2 ■ Fall 2013 ■ 29

Career Path Job Description
Education Needed Salary Job Outlook
Health Administrator
•Oversees vari-ous departments to keep up with the fast-paced changes to the medical field•Coordinates quality of care3
•Bachelors in Healthcare Ad-ministration for lower tier jobs•MBA with a background in science or healthcare pre-ferred for upper tier jobs3
•Mean an-nual salary of $104,0003
•Projected 22% growth from 2010 to 20203
Healthcare Attorney
•Oversees risk management and malpractice litigation.•In charge of general corpo-rate manage-ment issues in healthcare5
•A bachelor’s degree and then completion of law school5
•Mean an-nual salary of $102,0005
•Projected 14% growth from 2010 to 2020
Job in Bioethics
•Very wide range of oppor-tunities•Positions in ethics commit-tees • Work for non-profit organiza-tions•Hospital chap-laincy1
•A bachelor’s degree in biol-ogy is required, but a master’s or PhD is prefer-able for higher tier positions13
•Because of the wide range of options in this field, a salary range is difficult to pinpoint13
•Average job growth of 34% from 2010 to 202013
It is understandable why students interested in the medical field would opt out of the traditional route
to medicine (i.e. premed, medical school, residency, etc.). And while I attribute a few of these reasons to
the highly demanding coursework of being premed, many students simply find that their passions lie in
areas apart from medicine after they have been exposed to different academic fields.
Luckily, in today’s job market there are a plethora of options for cross-field careers. I have detailed only a
few of these options below, in regards to job description, level of education required, the salary each path
can provide, and the overall outlook for those career paths.
30 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

Career Path Job Description
Education Needed Salary Job Outlook
Patent Attorney
•Plans and di-rects any legal issues regarding patents•Determines who owns rights to inventions7
•A bachelor’s degree in a sci-ence field and completion of law school. The Patent Bar Exam is required to practice law. 7
•Mean an-nual salary of $212,0007
•Average job growth of 10% from 2010 to 20207
Scientific Consultant
•Conducts research in various fields of biotechnology and other life science-related disciplines to create innova-tions for cus-tomer projects9
•A bachelor’s degree is re-quired for lower tiered jobs, a master’s degree in a science dis-cipline is neces-sary for upper level jobs9
•Mean an-nual salary of $84,0009
•Average job growth of 14% from 2010 to 20209
Forensic Pathologist
•Conducts ap-plied or aca-demic forensic pathology•Uses scien-tific reasoning to help legal matters involv-ing human remains11
•A master’s de-gree or PhD in biological an-thropology11
•Mean an-nual salary of $66,00011
•Average job growth of 5% from 2010 to 202011
The medical field has more options than one would think. If your end goal is to attain the title of MD at
the end of your name, then that is fantastic. It is also important to realize that the medical field has a much
wider range of career paths though; it is flexible, integrative, and multifaceted. In short, you can find a
career path in the medical field that best fits you.
I still have not decided on a career path, and by the end of the month, I may have tossed out another
dozen possibilities. Though the process of choosing a career path still seems daunting as I head into my
sophomore year, it is comforting to know that when I do choose one, I don’t have to sacrifice one interest
for the other. There are still many career opportunities out there, and I have the ability to find a career path
that combines my passions. ■ MD For references, see page 41.
Volume 2 ■ Fall 2013 ■ 31

Scalp cryotherapy: changing the Face oF cancer
A patient facing cancer confronts more than
a battle with a life-threatening illness. Many
patients with cancer must face a battle with the
mirror. Of the 1.6 million Americans who will be di-
agnosed with cancer this year, more than half will
be treated with hair loss-inducing chemotherapy.1
Hair has a distinct function in our society. Hair can
signify health, youth, sexuality, and individuality.
It can enhance body image, self-esteem, and self-
expression. One popular British magazine esti-
mates that the average person spends almost ten
days per year styling their hair!2
Although concerns about hair loss have long
been dismissed as purely cosmetic or superflu-
ous, studies show that hair loss can have a major
psychological impact on patients. Watching your
own hair fall out can be a highly traumatic process
and can cause patients to feel as if they are losing
a part of themselves. One study found that breast
cancer patients are more worried about losing
their hair than losing their breast.3 The loss of hair
takes the privacy out of a patient’s cancer treat-
ment. Patients have described going bald as feel-
ing as if they are wearing a sign that says, “Ask me
about my cancer.” Fear of hair loss is sometimes so
severe that patients will choose not to receive or
prolong a recommended treatment in an effort to
keep their hair.3-5
What many cancer patients and even some phy-
sicians do not know is that there are options cur-
By devorA IsseroFF
32 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma
rently available that can prevent this unfortunate
side effect. Since the 1970s, scalp cryotherapy (lit-
erally, “ice healing”) has been a standard hair loss
prevention method in Europe and Canada.6-8 This
method involves strapping a bulky cap, called a
cold cap, to the scalp of a patient receiving che-
motherapy. Though caps are often cooled to near
0˚C temperatures, they are generally well tolerat-
ed. Major complaints are limited to headache and
sensations of cold, but these complaints rarely
lead to patients discontinuing their cold cap treat-
ment.
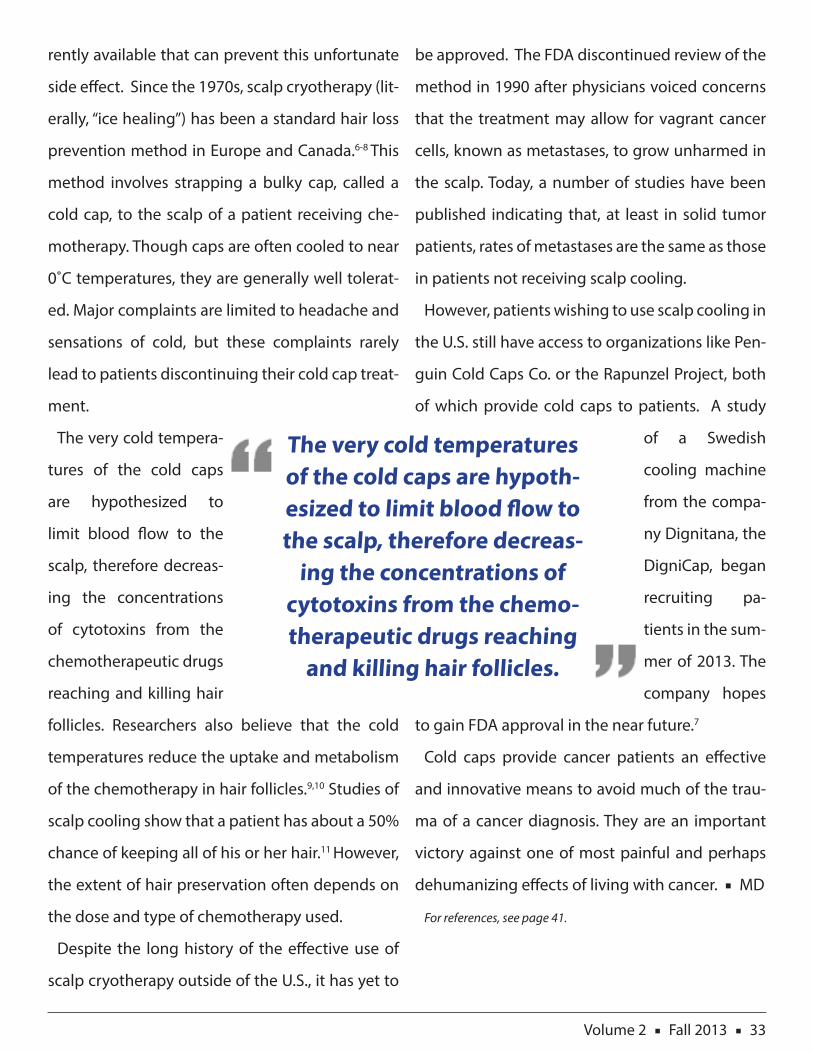
The very cold tempera-
tures of the cold caps
are hypothesized to
limit blood flow to the
scalp, therefore decreas-
ing the concentrations
of cytotoxins from the
chemotherapeutic drugs
reaching and killing hair
follicles. Researchers also believe that the cold
temperatures reduce the uptake and metabolism
of the chemotherapy in hair follicles.9,10 Studies of
scalp cooling show that a patient has about a 50%
chance of keeping all of his or her hair.11 However,
the extent of hair preservation often depends on
the dose and type of chemotherapy used.
Despite the long history of the effective use of
scalp cryotherapy outside of the U.S., it has yet to
be approved. The FDA discontinued review of the
method in 1990 after physicians voiced concerns
that the treatment may allow for vagrant cancer
cells, known as metastases, to grow unharmed in
the scalp. Today, a number of studies have been
published indicating that, at least in solid tumor
patients, rates of metastases are the same as those
in patients not receiving scalp cooling.
However, patients wishing to use scalp cooling in
the U.S. still have access to organizations like Pen-
guin Cold Caps Co. or the Rapunzel Project, both
of which provide cold caps to patients. A study
of a Swedish
cooling machine
from the compa-
ny Dignitana, the
DigniCap, began
recruiting pa-
tients in the sum-
mer of 2013. The
company hopes
to gain FDA approval in the near future.7
Cold caps provide cancer patients an effective
and innovative means to avoid much of the trau-
ma of a cancer diagnosis. They are an important
victory against one of most painful and perhaps
dehumanizing effects of living with cancer. ■ MD
For references, see page 41.
The very cold temperatures of the cold caps are hypoth-esized to limit blood flow to the scalp, therefore decreas-
ing the concentrations of cytotoxins from the chemo-therapeutic drugs reaching
and killing hair follicles.
Volume 2 ■ Fall 2013 ■ 33

“y ou’re turning white,” Dr. House said to
the pale, sickly looking African-American
man lying in the ICU. “What does that mean?” the pa-
tient’s mother asked in a concerned tone. Dr. House
retorted, “It means he doesn’t need football to get a
good job anymore.”
This completely inappropriate yet entertaining
dialogue occurred in an episode of the acclaimed
medical drama House. The show, which features the
brilliant, emotionally unstable, and drug-addicted
character Gregory House, was nominated 159 times
for awards from American television organizations
throughout its 8 seasons, winning two Golden
Globes.1 House is also very popular with students
who are preparing for health professions with 65%
of nursing students and 76% of medical students
tuning into House on a weekly basis, according to a
2008 survey conducted by researchers at the Berman
Institute of Bioethics at Johns Hopkins University.2
Another widely watched medical drama is Grey’s
Anatomy. In the week of March 29, 2013, Grey’s
topped the Thursday rating chart with 8.8 million
viewers.3 The famous medical TV show ER was no
prIMeTIMeprescrIpTIons
Writers are constantly caught in a balancing act between sticking to the facts and bending the truth for the sake of
entertainment.
34 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma
By rAchel sIBley

less popular, winning the People’s Choice Award for
“Favorite Television Dramatic Series” every year from
1995 to 2002.4
Yet, the precedent for hospital dramas on network
TV was set long before ER and Grey’s. The first medi-
cal TV shows began in the 1960s, with Ben Casey and
Marcus Welby, M.D., who earned the title of “Amer-
ica’s family physicians”. In these past five decades,
not one year has gone by without a medical drama
gracing cable television.5 The genre’s unperturbed
success stems from the lure of life and death deci-
sions, blood, gore, mystery, ethics and romance – all
plot components that make for irresistibly compel-
ling television.
However, medical professionals claim that these
medical dramas and others misinform audiences
on most aspects of real-life medicine, from specific
procedures to the interactions between different
members of the healthcare system. But who cares?
Why bother to criticize these shows when they are
grossing millions of dollars and racking in Emmy af-
ter Emmy?
Television writers are the ones responsible for
maintaining medical accuracy in their episodes. In
order to create plot lines and impressive dialogue,
the writers behind these successful shows rely on
consultations from doctors and healthcare experts,
provided by groups such as Health & Society, the
Centers for Disease Control and Prevention, the Na-
tional Institutes of Health, and the USC Annenberg
Norman Lear Center.6 However, writers are constant-
ly caught in a balancing act between sticking to the
facts and bending the truth for the sake of entertain-
ment. Of course, more often than not, they choose to
sacrifice medical accuracy in order to create gripping
television. But how much do they sacrifice and why
is it important?
A plIGhT For nurses
One group that has protested against the inaccura-
cies of medical dramas is nurses. Nurses argue that
hospitals on TV seem to operate completely without
their assistance. Stating that their portrayals are rare-
ly accurate, nurses have observed that these dramas
tend to omit their roles as influential individuals in
the medical setting who make decisions daily that
save lives. Nurses are often absent in medical dramas,
while doctors are shown doing nurses’ jobs. Sandy
Summers, the director of the Center for Nursing Ad-
vocacy, a Baltimore-based non-profit, cites many
television occurrences of physicians acting in the
role of nurses. Summers cites an episode of House in
which a doctor helps a postoperative patient to the
bathroom – a task performed by nurses in real hospi-
Nurses have observed that these dramas tend to omit their roles as influential individuals in the medical setting who make daily decisions that save lives.
Volume 2 ■ Fall 2013 ■ 35

tal settings. In 2006, the Center for Nursing Advocacy
even included Grey’s Anatomy on its list of the “10
Worst Portrayals of Nursing in the Media” during the
Golden Lamp Awards, a ceremony which ranks the
best and worst depictions of nursing in mainstream
media.7 In one episode of the show, the interns mon-
itor a premature infant through the night shift in the
neonatal intensive care unit. Summers pointed out
that trained neonatal nurses are actually responsible
for this job.
One major concern that has propelled the backlash
against medical dramas in the nursing community is
the current nursing shortage in the US. According to
the American Nurses Association (ANA), the current
median age of nurses is 46 and more than fifty per-
cent of the nursing workforce is close to retirement.
The need for more nurses will become even more
apparent in the future. As the baby boom generation
grows older, their health needs will increase, put-
ting a strain on the health system. Additionally, the
new health care reforms have given millions more
people access to medical care, adding to the strain
on hospitals and clinics.8 Nurses partially blame this
shortage on the portrayal of their profession on
the small screen. Rebecca Patton, President of the
American Nurses Association, claimed “Young men
and women are choosing other professions instead
of nursing, in part because of the negative portrayal
of nurses in the media”.7 While some doubt the im-
portance medical dramas’ depiction of nurses has on
this shortage, television has been shown to have a
powerful influence on the careers that today’s young
men and women choose. Annual surveys revealed
that in 2004, forensic medicine ranked 33 on the list
of most popular career choices, while just one year
later in 2005, forensic medicine jumped to 23 on the
list, a dramatic increase in popularity that was attrib-
uted to the late 2004 premiere of CSI: New York.7
The IMpAcT oF hollywood on MedIcAl schools
Unfortunately, nurses are not the only ones nega-
tively impacted by Hollywood hospitals. There is a
growing concern among medical educators that their
students, the young future physicians of America,
are subconsciously using medical TV shows as a type
of informal curriculum. Dr. Elizabeth Sinz, a professor
of anesthesiology at the Penn State Milton S. Her-
shey Medical Center, said “People learn from TV, they
learn from reading, they learn from what I’m teach-
ing in a lecture. It all has to come together.”9 One of
Sinz’s main concerns is that TV shows unrealistically
depict teamwork, especially in emergency settings
where TV doctors often make decisions completely
on their own. In addition, these fictional TV physi-
cians never discuss the concerns that real-life doc-
tors grapple with, such as paying back student loans
or fighting to get Medicare claims reimbursed.9 Ad-
ditionally, medical school professors are worried that
their students might treat these shows as lessons in
36 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

medical ethics. “In a 2008 survey published in the
April Issue of Journal of Medical Ethics, researchers
catalogued 179 depictions of bioethical dilemmas
in 50 episodes of House and Grey’s Anatomy that
aired between fall 2005 and spring 2006. Of those,
49 involved not obtaining informed consent for
treatment from patients or their loved ones. In some
instances (43%), the characters behaved according
to professional codes of conduct, but in most cases
(57%) they missed the mark completely — as when
TV doctors failed to obtain any consent at all for a
procedure or brazenly lied to patients to get them
to sign off (two scenarios particularly common on
House)”.2 Dr. Vineet Arora, the assistant dean at the
University of Chicago’s Pritzker School of Medicine,
has taken action in the classroom to combat the im-
pressions that medical dramas have given medical
students. Dr. Arora created a new class called “Medi-
cal Professionalism in the 21st Century: A Real World
Approach” in which she plays segments from “ER”
that showcase patient-physician interactions. She
then has the class critically discuss the clips after-
wards, highlighting the inconsistencies that many of
these dramas have with the real world of medicine.9
The InTerFerence wITh pATIenT cAre
While medical schools can reach out to their stu-
dents using progressive new curriculums similar
to Dr. Arora’s, it is more difficult to reach out to the
general population of patients. A main misconcep-
tion that patients might have is the survival rate for
cardiopulmonary resuscitation (CPR). In 1996, the
New England Journal of Medicine reported that
CPR occurs successfully in 75% of cases presented
on TV. However, even optimistic real-life estimates
suggest that CPR is successful only 15% of the time.
Some fear that this will give people unrealistic ex-
pectations, although this has not been studied ex-
tensively.9 Medical television has also been shown to
influence viewers’ expectations about their chances
of getting sick. A survey of almost 1,300 participants
presented at the British Psychological Society’s con-
ference in Bath, England revealed that participants
who watched the most medical programs were ten
percent more afraid of falling ill than others. The Brit-
ish Heart Foundation (BHF) also realized that medical
television gives the public unrealistic expectations.
In 2008, BHF cautioned that “Hollywood-style” heart
attacks, in which actors clutch at their chests and fall
to the floor, are misleading and might cause people
to ignore some characteristic symptoms of a heart
attack. In response, BHF produced its own short film
called “Watch Your Own Heart Attack,” combating
television portrayals and publicizing the true symp-
toms of an attack.10
Susan Morgan, associate professor in the Depart-
ment of Communication at Purdue University and
author of Entertainment (Mis)Education, spoke out
regarding what she sees as the most detrimental
effects of inaccurate medical dramas on patients.
Volume 2 ■ Fall 2013 ■ 37

Morgan was the co-author of a study published in
Clinical Transplantation in 2005 that revealed that
the majority of patients who are unenthusiastic, and
even pessimistic, about organ donation frequently
cite television as evidence for their opinions. In-
deed, most TV episodes that feature organ dona-
tion dramatize the situation by including plot lines
about black markets for organs, doctors not saving
potential donors’ lives, or wealthy patients receiv-
ing higher priority on waiting lists.11 Morgan specifi-
cally recalled an episode of Grey’s Anatomy in which
“a patient was prematurely declared brain-dead so
her organs could be procured”.6 Morgan fears that
inaccurate portrayal of organ donation will dissuade
people from becoming donors, an issue which poses
as a major problem because, in the United States
alone, there are roughly 118,000 people on waiting
lists for life-saving transplants.12 Morgan stated: “You
could start drawing this out to real human lives be-
ing lost.”6
However, in 2007, hope came in the form of Do-
nate Life Hollywood (DLH), a campaign specifically
launched to eliminate the “stolen-kidney” story-
line and other inaccuracies in Hollywood related to
the depiction of organ, eye, and tissue donation.
In response to Morgan’s groundbreaking research,
Tenaya Wallace, director of DLH stated: “The organ
and tissue donation and transplant community has
been upset by inaccuracies in the past but we have
not taken action. Now we have hard evidence that
what viewers think about donation is directly related
to what they see in television storylines. This is not
just about creative license. We want Hollywood writ-
ers, producers, and executives to consider the pub-
lic health impact of their donation storylines. That is
why we are launching Donate Life Hollywood.”11 In
order to pursue these goals, DLH discourages writ-
ers and producers from negatively featuring organ
donation by distributing to TV networks a “top 10
list of storylines that are most harmful to the pub-
lic’s perception of the donation process”.11 If a film,
TV episode, or commercial contains any of these
top 10 storylines, DLH recruits volunteers across the
country whose lives have been positively impacted
by organ donation to write letters to those network
executives.11 On the other hand, the campaign also
praises programs that accurately and positively fea-
ture organ donation. For example, one episode of
Extreme Makeover: Home Edition followed the story
of a mother whose son had died in a car crash and
donated his organs. DLH applauded the episode
and “after the show aired, online donor registration
increased 200% in California over the previous week,
a spike the campaign attributed to the show”.6
An AccurATe MedIcAl drAMA show
Thankfully, there is one popular medical drama that
has continually been praised for its accurate repre-
sentations, and it is a show that people might be least
likely to guess: Scrubs. Unlike the shows mentioned
38 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

It is important to remain aware of the inaccuracies that are present in medical dra-mas and differentiate
fact from fiction.
thus far, Scrubs does not deal with life or death sce-
narios in every episode and doesn’t end with a sur-
prise diagnosis – it focuses on ordinary cases. The
show’s narrator and central character is Dr. John “J.D.”
Dorian (played by Zach Braff), and it focuses on his
progression from intern to resident to full-fledged
doctor. In particular, real physicians identify most
closely with J.D.’s portrayal of the ups and downs of
medical residency. He reveals most of his feelings
through his internal monologues. Questions that J.D.
asks in his internal monologues, such as “Am I hurt-
ing the patient? Am I learning what I should? Am I
kissing up too much to the attending?”13 are typical
of the real doubts that go through a resident’s mind,
according to Jonathan Samuels, doctor at the NYU
Hospital for Joint Diseases.13
Scrubs is able to achieve such accuracy because
the show’s creator, Bill Lawrence, based the show
on the experiences of his close friend, Dr. Jonathan
Doris, throughout his internship and residency. Do-
ris is now a cardiologist in LA and a medical advisor
to the show, and many of his experiences from his
residency at Brown University have been featured
in Scrubs episodes. For example, Doris once hid in a
closet in order to avoid being the first doctor at the
scene when a patient was coding. “In the pilot, J.D.
performs a procedure called a paracentesis to drain
fluid from a patient’s distended belly; he turns away
for a moment, then looks back to discover a geyser
of fluid gushing into the air. It happened—just like
that—to a fellow resident at Brown.” 13 Dr. Paul Pir-
raglia, an internist in Providence, Rhode Island and
another resident in Doris’ class explained “Being a
resident is a strange place between officially being
a doctor, which you are, but also really not knowing
it all…You get this level of authority that you don’t
think you deserve. All of a sudden you’re the doctor
and people are going to listen to you.”13
Even though Scrubs has been lauded for its realism,
it remains to be the one of the only major TV produc-
tion that has consistently stuck true to the medical
facts. Next up on the agenda for medical television
series is Hostages, an new drama that aired on CBS
in September of this year. The series stars Toni Col-
lette, a high profile surgeon recruited to operate on
the President of the United States.14 It is clear that
regardless of the plot line, the actor, the location, or
the negative effects of inaccurate representations:
America just can’t get enough of Hollywood hospi-
tals. Whether we like it or not, this television genre
is here to stay. It is important to remain aware of the
inaccuracies that are present in medical dramas and
differentiate fact from fiction. ■ MD For references, see page 42.
Volume 2 ■ Fall 2013 ■ 39

reFerenCes“Color-Coded Surgery and Organ Printing: A Glimpse at Future Health Technologies”
1) About the Human Genome Project.” About the Human Genome Project Information Archive. N.p., 23 July 2013. Web. 30 July 2013.
2) Anthony Atala: Growing New Organs. Dir. Anthony Atala. TED: Ideas worth Spreading. TEDMED, 9 Oct. 2011. Web. 30 July 2013. <http://www.ted.com/talks/an-
thony_atala_growing_organs_engineering_tissue.html>.
3) Bosch, Tory. “How Close Are We to Making Like Salamanders and Regenerating Our Own Organs?” Future Tense. N.p., 9 Nov. 2012. Web. 30 July 2013.
4) Quyen Nguyen: Color-coded Surgery. Dir. Quyen Nguyen. TEDMED, 11 Dec. 2011. Web. 30 July 2013. <http://www.ted.com/talks/quyen_nguyen_color_coded_sur-
gery.html?quote=1236>.
5) Wadhwa, Vivek. “Medicine’s Bright Future.” Washington Post. N.p., 28 July 2011. Web. 30 July 2013.
6) Nguyen, Quyen, and Amy P. Wu, Et Al. “Improved Facial Nerve Identification with Novel Fluorescently Labeled Probe.” National Center for Biotechnology Informa-
tion. U.S. National Library of Medicine, 16 Feb. 2011. Web. 30 July 2013.
7) Deborah Rhodes:A Tool That Finds 3x More Breast Tumors, and Why It’s Not Available to You. Dir. Deborah Rhodes. The Future of Medicine. TEDMED, Jan. 2011.
Web. 30 July 2013. <http://www.sciencedirect.com/science/article/pii/S0025619611629534>.
“Where Does Alternative Medicine Belong?”
1) “The ABCs of Traditional Chinese Medicine and Acupuncture,” Acupuncture Today. <http://www.acupuncturetoday.com/abc>.
2) Kim Soo Kyung and Kim Eun Kyung, “Everyday Application of Meridian,” All That Korean Medicine, 2002, <http://koreanmedicine.net/10news/10news_5.html>.
3) Acupuncture and Cancer. Autonomic neuroscience. David O’Reagan 2010:157(1-2); 96-100.
4) “Complementary, Alternative, or Integrative Health: What’s In a Name?” National Center for Complementary and Alternative Medicine, May 2013. <http://nccam.nih.
gov/health/whatiscam>.
5) “What is homeopathy?” The Society of Homeopaths, August 2013. <http://www.homeopathy-soh.org/about-homeopathy/what-is-homeopathy>.
6) “Naturopathy.” University of Maryland Medical Center. May 2013. <http://umm.edu/health/ medical/altmed/treatment/naturopathy>.
7) “Complementary and Alternative Medicine,” Mayo Clinic, October 2011. <http://www.mayoclinic.com/health/alternative-medicine/PN00001>.
8) Massage therapy for symptoms control: outcome study at a major cancer center. J Pain and Symptom management. Barrie R. Cassileth 2004:28(3); 244-249.
“How Baby Boomers will Change Orthopedic Care”
1) “Aging Statistics.” Administration on Aging. Department of Health and Human Services, 8 May 2013. Web. 20 Sept. 2013.
2) American Hospital Association & First Consulting Group. “When I’m 64: How Boomers Will Change Health Care.” May 2007. Web. 20 Sept. 2013.
3) Boomer Seniors News Conference Keynote Speech Summaries, American Academy of Orthopedic Surgeons, December 20, 2006.
4) U.S. Census Bureau, Current Population Survey, 2005 Annual Social and Economic Supplement. (Table 1: Educational Attainment of the Population 15 Years and
Over, by Age, Sex, Race, and Hispanic Origin: 2005). Internet release date: October 26, 2006; and U.S. Census Bureau, Current Population Survey, 1985 Social and Eco-
nomic Supplement. (Table 1: Years of School Completed by Persons 15 Years Old and Over, by Age, Sex, Race, and Spanish Origin: March 1985, 1984, 1983, and 1982).
5) “Physician Supply and Demand: Projections to 2020,” HRSA, October 2006.
“Population Health: A Call for Value-Based Healthcare”
1) Kane, J. (2012) Health Costs: How the U.S. Compares with Other Countries. October 22, 2012. <http://www.pbs.org/newshour/rundown/2012/10/health-costs-how-
the-us-compares-with-other-countries.html>.
2) Fuchs, V.R. (2013) The Gross Domestic Product and Healthcare Spending. N Engl J Med: 369, 107-109.
3) United States Total Spending Pie Chart for 2013. <http://www.usgovernmentspending.com/united_states_total_spending_pie_chart>.
4) Guan, A. & Chan, A. (2013) Innovating Healthcare Payment Systems: Moving Beyond the Fee for Service Model. May 15, 2013, <http://www.huffingtonpost.com/amy-
guan/innovating-healthcare-pay_b_3211475.html>.
5) Kehoe, B. (2012) Reengineered care delivery and payment models will have a huge impact on hospitals. December 2012, HFM Magazine. <http://www.hfmmagazine.
40 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

com/hfmmagazine/jsp/articledisplay.jsp?dcrpath=HFMMAGAZINE/Article/data/12DEC2012/1212HFM_FEA_TrendsInterview&domain=HFMMAGAZINE>.
6) Frost and Sullivan. (2011). Frost and Sullivan Honors Bosch Healthcare for its Market Share Leadership of the North American Remote Patient Monitoring Market
[Press Release]. <http://www.frost.com/prod/servlet/press-release.pag?docid=249413244>.
7) Explorys. (2013). Trinity Health Selects Explorys’ Big Data Analytics Platform To Support Clinical Integration and Quality Initiatives. [Press Release]. <https://www.
explorys.com/results/news-results/2013/04/29/trinity-health-selects-explorys-big-data-analytics-platform-to-support-clinical-integration-and-quality-initiatives>.
“Emergency Contraception: A Quick Guide to the Morning After”
1) Hickey, MT. 2009. “Female college students’ knowledge, perception, and use of emergency contraception,” Journal of Obstetrics, Gynecology, and Neonatal Nursing,
Vol 38 (4): 399-405.
2) Planned Parenthood Federation of America. Morning-After Pill (Emergency Contraception). <http://www.plannedparenthood.org/healthtopics/emergency-contra-
ception-morning-after-pill-4363.asp>.
3) The Emergency Contraception Website. Princeton University. [cited 2012 Jan 4]. <http://ec.princeton.edu/pills/Dedicated_ECPs.pdf>.
4) Howell, Tom Jr. June, 2013. “Plan B drug maker: FDA approved pill without restrictions,” The Washington Times. <http://www.washingtontimes.com/news/2013/
jun/21/plan-b-drug-maker-fda-approved-pill-without-restri/>.
“Making the Career Choice: What are your options?”
1) Stanford Daily. (2012). Premedical Advising. Retrieved August 13, 2013. <http://www.stanforddaily.com/2012/10/22/pre-med-advising-fails-to-meet-student-needs>.
2) Bureau of Labor Statistics (2013). Retrieved October 4, 2013. <http://www.bls.gov/ooh/images/p02-to-p03/p035-1-jpg.jpg>
3) Bureau of Labor Statistics. (2012). Topics in Brief: Prescription Medical and Health Services Managers. Retrieved August 13, 2013. <http://www.bls.gov/ooh/Manage-
ment/Medical-and-health-services-managers.htm>.
4) Lawcrossing (2011). Retrieved October 4, 2013. <http://www.lawcrossing.com/images/articleimages/Health-Care-Attorney-Jobs.jpg>
5) Education Portal. (2012). Health Care Lawyer: Job Description and Requirements for Starting a Career in Health Care Law. Retrieved August 13,2013. <http://educa-
tionportal.com/articles/Health_Care_Lawyer_Job_Description_and_Requirements_for_Starting_a_Career_in_Health_Care_Law.html>.
6) Taegsang (2012). Retrieved October 4, 2013. <http://taegsang.files.wordpress.com/2010/06/patent-attorney.jpg>.
7) Bureau of Labor Statistics. (2012). Patent work: the other side of invention. Retrieved August 13, 2013. <http://www.bls.gov/opub/ooq/2009/fall/art03.pdf>.
8) Degree Bio (2010) Retrieved October 4, 2012. <http://1degreebio.org/common/files/blogs/6476-1373745719-consulting.jpg>.
9) Science Mag. (2012). Consulting--The Career Path Not (Oft) Taken. Retrieved August 13, 2013. <http://sciencecareers.sciencemag.org/career_magazine/previous_is-
sues/articles/2002_12_13/nodoi.9034383921133532073>.
10) Chron (2012). Retrieved October 4, 2013. <http://work.chron.com/DMResize/photos.demandstudios.com/getty/article/152/134/MD001161.
jpg?w=600&h=600&keep_ratio=1>.
11) ItsGov. (2012). Retrieved August 13, 2013. <http://www.theabfa.org/forstudents.html>.
12) Twin Water Design (2013). Retrieved October 4, 2013. <http://www.twinwaterdesign.com/wp-content/uploads/2011/08/BioEthicsLogo.jpg>.
13) Undergraduate Bioethics Program. (2013). Retrieved August 13, 2013. <http://dev.bioethics.virginia.edu/careers>.
“Scalp Cryotherapy: Changing the Face of Cancer”
1) Cancer Facts and Figures 2013. In: Society AC, editor, 2013.
2) Harding E. “How much time do you spend on your hair, ladies?” Mail Online. England, 2012.
3) Tierney AJ. “Preventing Chemotherapy-Induced Alopecia in Cancer-Patients - Is Scalp Cooling Worthwhile.” Journal of Advanced Nursing. 1987;12: 303-310.
4) Lemenager M, Lecomte S, Bonneterre ME, Bessa E, Dauba J, Bonneterre J. “Effectiveness of cold cap in the prevention of docetaxel-induced alopecia.” European Jour-
nal of Cancer. 1997;33: 297-300.
5) Ron IG, Kalmus Y, Kalmus Z, Inbar M, Chaitchik S. “Scalp cooling in the prevention of alopecia in patients receiving depilating chemotherapy.” Supportive Care in
Cancer. 1997; 5: 136-138.
Volume 2 ■ Fall 2013 ■ 41

6) Van den Hurk CJG, Coebergh JWW, Breed WPM, De Poll-Franse LVV, Nortier JWR. “Scalp cooling in cancer patients receiving chemotherapy in the Netherlands.”
Ejc Supplements. 2007;5: 147-147.
7) Rugo HS, Serrurier K, Melisko M, et al. “The Dignicap (Tm) System to Prevent Alopecia in Women Receiving Chemotherapy for Breast Cancer.” Breast. 2013;22: S119-
S119.
8) Breed WPM. “What is wrong with the 30-year-old practice of scalp cooling for the prevention of chemotherapy-induced hair loss?” Supportive Care in Cancer.
2004;12: 3-5.
9) Lemieux J, Amireault C, Provencher L, Maunsell E. “Incidence of scalp metastases in breast cancer: a retrospective cohort study in women who were offered scalp
cooling.” Breast Cancer Research and Treatment. 2009;118: 547-552.
10) Breed WPM, van den Hurk CJG, Peerbooms M. “Presentation, impact and prevention of chemotherapy-induced hair loss: scalp cooling potentials and limitations.”
Expert Review of Dermatology. 2011;6: 109-125.
11) Grevelman EG, Breed WPM. “Prevention of chemotherapy-induced hair loss by scalp cooling.” Annals of Oncology. 2005;16: 352-358.
“Primetime Prescriptions”
1) “Awards for “House M.D.”” IMDb. IMDb.com, n.d. Web. 12 Sept. 2013. <http://www.imdb.com/title/tt0412142/awards>.
2) O’Callaghan, Tiffany. “The House Effect: Are Real Patients Misled by TV Docs?”
TIME Health & Family. TIME Inc., 9 Apr. 2010. Web. 12 Sept. 2013. <http://content.time.com/time/health/article/0,8599,1978591-1,00.html>.
3)Hibberd, James. “’Grey’s Anatomy’ Tops Thursday Ratings Chart.” Entertainment Weekly. Entertainment Weekly Inc., 29 Mar. 2013. Web. 12 Sept. 2013. <http://in-
sidetv.ew.com/2013/03/29/greys-anatomy-tops-thursday-ratings-chart>.
4)“Awards for “ER”” IMDb. IMDb.com, n.d. Web. 12 Sept. 2013. <http://www.imdb.com/title/tt0108757/awards>.
5)Woo, Steve. “Medicine on the Small Screen.” The New Physician. American Medical Student Association, Nov. 2009. Web. 12 Sept. 2013. <http://www.amsa.org/AMSA/
Homepage/Publications/TheNewPhysician/2009/1109FeatureDrama.aspx>.
6)Van Dusen, Allison. “Playing Doctor: Medical TV Isn’t Always Right.” Forbes. NBCNews.com, 20 Sept. 2007. Web. 12 Sept. 2013. <http://www.nbcnews.com/
id/20895520/ns/health-forbes_com/t/playing-doctor-medical-tv-isnt-always-right/#.UjKGyc2B296>.
7)The Star-Ledger of Newark, N.J. “Nurses Say TV Ignores Them.” Sun Journal [Lewiston, Maine] 13 Jan. 2007, Health sec.: B8. Google News Archives.Google.com. Web.
13 Sept. 2013. <http://news.google.com/newspapers?nid=1914&dat=20070109&id=GwQgAAAAIBAJ&sjid=V2QFAAAAIBAJ&pg=1446,1957933>.
8)“Nursing Shortage.” Nursing World. American Nurses Association, n.d. Web. 12 Sept. 2013. <http://www.nursingworld.org/MainMenuCategories/ThePracticeofProfes-
sionalNursing/workforce/NursingShortage>.
9)Brownstein, Joseph. “Do Doctor Dramas Make for Bad Docs?” ABC News. ABC News Network, 26 Mar. 2009. Web. 12 Sept. 2013. <http://abcnews.go.com/Health/
WellnessNews/story?id=7178967>.
10)Devlin, Kate. “Television Medical Shows Like ER ‘Increase Our Fear of Illness’.” The Telegraph. Telegraph Media Group, 9 Sept. 2008. Web. 12 Sept. 2013. <http://www.
telegraph.co.uk/news/uknews/2711035/Television-medical-shows-like-ER-increase-our-fear-of-illness.html>.
11)“Hollywood Gets It Wrong on Organ Donation.” Washington Regional Transplant Community. Donate Life, 31 July 2007. Web. 13 Sept. 2013. <http://www.beadonor.
org/news-a-events/media-center/press-releases/881-hollywood-gets-it-wrong-on-organ-donation>.
12)“Statistics.” Donate Life America. Donate Life, n.d. Web. 13 Sept. 2013. <http://donatelife.net/understanding-donation/statistics/>.
13)Weiss, Joanna. “Scrubs: Goofy, Cartoonish, and the Most Accurate Portrayal of the Medical Profession on TV.” Slate Magazine. The Slate Group, 6 May 2009. Web. 13
Sept. 2013. <http://www.slate.com/articles/arts/culturebox/2009/05/scrubs.html>.
14)Mullins, Jenna. “5 Fall Shows We Love: Hostages Will Keep You Captivated.” E! Online. E! Entertainment Television, LLC., 12 Sept. 2013. Web. 13 Sept. 2013. <http://
www.eonline.com/news/457866/5-fall-shows-we-love-hostages-will-keep-you-captivated?utm_source=eonline>.
42 ■ The Medical Decoder ■ Phi Delta Epsilon IL Gamma

Thank you For Reading The Medical Decoder:
Presented by Phi Delta Epsilon
IL Gamma!
