the landscape of uterine fibroids · bulk symptoms… the best treatment option for you is a...
TRANSCRIPT

The Landscape of Uterine Fibroids: What Do We Know? What Do We Need? What Do Our Patients Need?
Erica E. Marsh, MD, MSCI, FACOGAssociate Professor and ChiefDivision of Reproductive Endocrinology and InfertilityDepartment of Obstetrics and GynecologyUniversity of Michigan Health SystemUniversity of MichiganAnn Arbor, Michigan
2
Fibroid
Fibroid
Fibroid
Fibroid
Fallopian tube
Ovary
Vagina
Cervix
Uterus

Presentation Overview
• Well circumscribed benign masses
• Single or multiple masses
• Whirled, shiny, white, bulging, rubbery cut surface
• Vary in size up to 100 lb
• Composed of irregular bundles of cells in an extensive connective tissue matrix
• Account for up to $34B annually
Leiomyoma leio (smooth) + myo (muscle) + oma (tumor)
Cardozo ER et al. Am J Obstet Gynecol. 2012;206(3):211.e1-e9.
3
Epidemiology
• Cumulative Incidence of 65% to 70%
• Risk Factors:– Race in AAW
– Obesity
– Hypertension
– Pelvic infections
– Alcohol in women who drink >7 beers/week
– Parity and smoking
Who gets uterine fibroids?
4
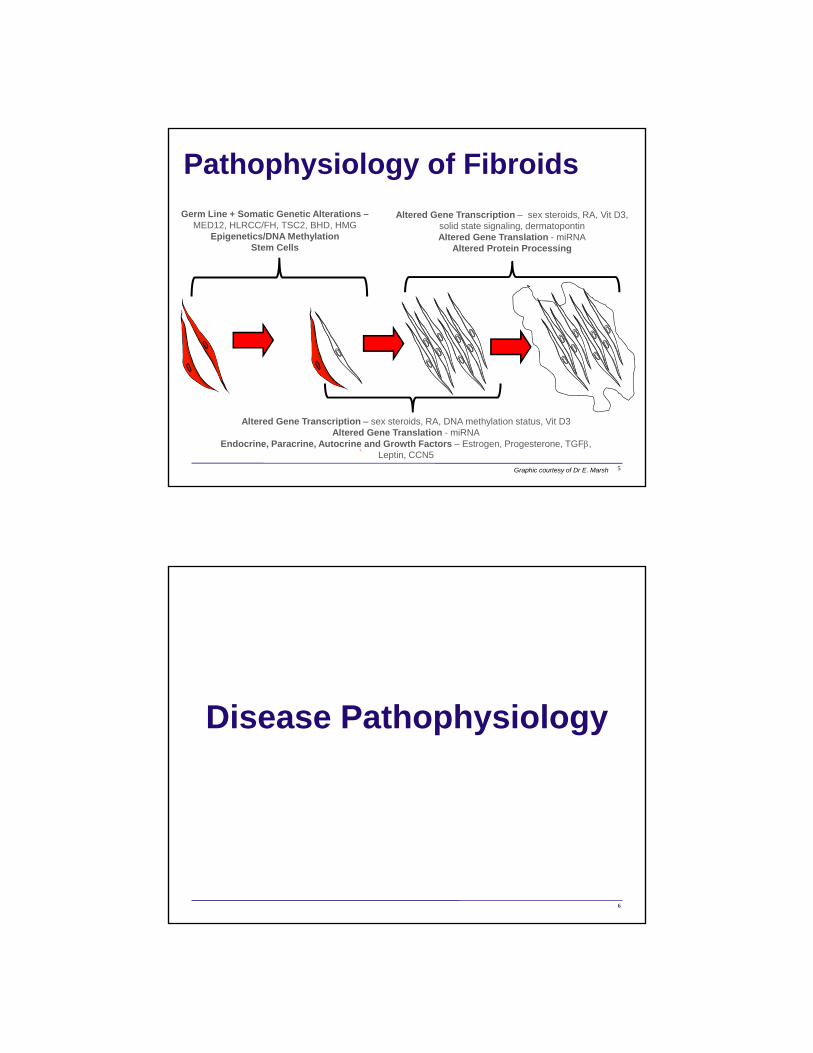
Altered Gene Transcription – sex steroids, RA, DNA methylation status, Vit D3Altered Gene Translation - miRNA
Endocrine, Paracrine, Autocrine and Growth Factors – Estrogen, Progesterone, TGF, Leptin, CCN5
Germ Line + Somatic Genetic Alterations –MED12, HLRCC/FH, TSC2, BHD, HMG
Epigenetics/DNA MethylationStem Cells
Altered Gene Transcription – sex steroids, RA, Vit D3, solid state signaling, dermatopontinAltered Gene Translation - miRNA
Altered Protein Processing
Pathophysiology of Fibroids
5Graphic courtesy of Dr E. Marsh
Disease Pathophysiology
6

Patient Centeredness
Health care that establishes a partnership among practitioners, patients, and their families (when appropriate) to ensure that decisions respect patients' wants, needs, and preferences and that patients have the education and support they need to make decisions and participate in their own care.
Crossing the Quality ChasmInstitute of Medicine, 2001
Institute of Medicine. Crossing the Quality Chasm. Washington, DC: National Academies Press; 2001.
7
“The right care, in the right way, at the right time”
Patient Centeredness
8

Patient Centeredness
"Nothing about me without me"
9
Institute of Medicine
• Core need for health care to be:
– Safe– Effective– Patient centered– Timely– Efficient– Equitable
Institute of Medicine. Crossing the Quality Chasm. Washington, DC: National Academies Press; 2001.
10
Reprinted with permission from the National Academies Press, Copyright 2001, National Academy of Sciences.

Provider Perspective
43-year-old G4P3 with 24-week–sized fibroid uterus, childbearing complete, HMB and bulk symptoms…
The best treatment option for you is a hysterectomy.
11
HMB=heavy menstrual bleeding.
Patient Perspective
“They viewed my uterus like it was a useless organ… They said, ‘Well, why do you want to keep it?’ …and I said, because it’s mine.”
12

Provider Perspective
13
Courtesy of Dr E. Marsh
Patient Perspective
14

Consequences
15
Adapted from Ghant MS et al. J Psychosom Res. 2015;78(5):499-503.
16
Beyond the Physical: A Qualitative Assessment of the Burden of Symptomatic Uterine Fibroids on Women’s Emotional and Psychosocial Health
Consequences
Ghant MS et al. J Womens Health (Larchmt). 2016;25(8):846-852.
17
An Altered Perception of Normal: Understanding Causes for Treatment Delay
in Women With Symptomatic Uterine Fibroids
Altered State of Normal
“…my period lasted for 30 days and it was heavy and it was horrible. I was wearing pads like the size that you get in the hospital after you have a baby, and I was so used to that happening, that at that time I didn’t call anybody because you know it was, like, ‘This is normal’.”
18

Limited Knowledge
“No, I had not. With a bachelor’s degree and a master’s degree in science and chemistry, I had not. Thinking back to anatomy and physiology classes, we talked about having babies, talked about different forms of cancer, but did they ever mention a fibroid?
“I don’t think so.”
19
Avoidance-based Coping Strategies
“…this is what you go through as a woman, and it was like every month you are going to bleed half to death and then the rest of the time you are almost okay. I just went with that… you know, it didn’t kill me, so I would just be stronger.”
20

Patient-Provider Interactions
• Pressure to obtain a hysterectomy
• Lack of discussion of treatment options
• Belittling of symptoms
• Treatment discouragement
21
Eight Dimensions of Patient-Centered Care
Adapted from Registered Nurses’ Association of Ontario. Best Practice Guidelines. Copyright 2015 by National Research Corporation Canada. Picker Institute. Principles of Patient-Centered Care. http://pickerinstitute.org/about/picker-principles/. Accessed July 24, 2017.
The Patient
22

Patient Perspectives
• Treatment Expectations
• Treatment Barriers
• Treatment Recovery and Satisfaction
• Financial Challenges
Sengoba KS et al. J Racial Ethn Health Disparities. 2017;4(2):178-183.
23
Racial/Ethnic Differences in Women’s Experiences With Symptomatic Uterine Fibroids: A Qualitative Assessment
Marsh EE et al. Int J Gynaecol Obstet. 2014;125(1):56-59.
24
Prevalence and Knowledge of Heavy Menstrual Bleeding Among African American Women
Type of ExperienceNo. of
Participants
Clinician seen for HMB 75
Treated for HMB 61
Hospitalized for HMB 35
Presented to emergency department for HMB
34
Type of Treatment% of
Participants
Oral Contraceptives 24.6
Hysterectomy 19.7
Endometrial Ablation 4.9
Depo-Lupron 4.9
Depo-Provera 1.6
Myomectomy 1.6
Other 1.6

Summary• Patient centeredness is 1 of 6 aims identified by the IOM to
address in order to elevate the quality of patient care in the United States
• Fibroids cause emotional and psychological trauma for many patients
• Despite being significantly symptomatic, women are delaying their fibroid treatment
• Many patients report negative provider interactions during their fibroid evaluation—even if they are ultimately comfortable with their care
• Approximately 50% of women in our study reported negative feelings about hysterectomy as a treatment choice
• 28% of women reported being discouraged to pursue any treatment
25
Conclusions• Better and more tailored education is needed for women
regarding fibroid symptoms, diagnosis, and treatment options
• Many women are looking for low risk/no risk treatment options and would rather continue to be severely symptomatic than accept the available treatment options
• There is a disconnect between providers and patients during fibroid counseling and, thus, an opportunity and need to optimize patient-centered care by increasing provider sensitivity and awareness of women’s values, fears, and concerns during their evaluation and by developing research aimed at understanding the health-seeking behaviors and needs of women with fibroids
26

Expanding Medical Treatment Options for Uterine Fibroids
Sukhbir Sony Singh, MD, FRCSC, FACOG (Program Chair)
Associate Professor and Vice‐Chair of Gynecology
Department of Obstetrics and Gynecology
The Ottawa Hospital
University of Ottawa
Ottawa, Ontario, Canada
27
IMPACT OF UTERINE FIBROIDS
28

29
Uterine Fibroids Are TOUGH
• Common and growing problem
• Demand for uterine sparing and fertility preservation procedures increasing
29
Courtesy of Dr S. Singh
Uterine Fibroids Are Common
• Estimated cumulative incidence by age 50– >80% for black women– Almost 70% for white women
• Estimated prevalence of clinically relevant fibroids– 50% of premenopausal black women– 25% of premenopausal white women
Baird DD et al. Am J Obstet Gynecol. 2003;188(1):100-107. 30

Impact of Fibroids
• One of the main reasons for hysterectomy
• By late 40s– 80% of African American– 70% of White
31
Courtesy of Dr S. Singh
Uterine Fibroids are TOUGH
• Surgical risks are REAL
• Skilled and willing surgeons are decreasing
32
Courtesy of Dr S. Singh

S. Singh
33
Adhesions after myomectomy
Adhesions after myomectomy
Courtesy of Dr S. Singh
Fibroids…
34
Courtesy of Dr S. Singh

Fibroids…
35
Courtesy of Dr S. Singh
Fibroids…
36
Courtesy of Dr S. Singh

Fibroids…
37
Courtesy of Dr S. Singh
Fibroids…
38
Courtesy of Dr S. Singh

Fibroids…
39
Courtesy of Dr S. Singh
Fibroids…
40
Courtesy of Dr S. Singh

Fibroids…
41
Courtesy of Dr S. Singh
Uterine Fibroids Are TOUGH
• Pathology Scares Us!
Smooth Muscle Tumor of Uncertain Malignant Potential
42
Courtesy of Dr S. Singh
Courtesy of Dr S. Singh

WHAT IS THE IDEAL THERAPY?
43
The Perfect Treatment Should….
• Manage signs and symptoms
• Offer sustained reduction in size of fibroids
• Preserve fertility
Miller CE. J Minim Invasive Gynecol. 2009;16(1):11-21. 44

Mass effectsrelated to the
size and locationof fibroids
Reproductivedysfunction
Bleedingcomplaints
These have been shown to diminish quality of life
Range of Symptoms Associated With Uterine Fibroids*
Tropeano G et al. Hum Reprod Update. 2008;14(3):259-274; Downes E et al. Eur J Obstet Gynecol Reprod Biol. 2010;152(1):96-102; Viswanathan M et al. Evid Rep Technol Assess (Full Rep). 2007;154:1-122.
*Not all fibroids are symptomatic
Nearly half of women with fibroids have significant and often disabling symptoms
Symptomatic fibroids*
45
Courtesy of Dr S. Singh
Management Options for Fibroids
Fibroid
Fibroid
Fibroid
Fibroid
Fallopian tube
Ovary
Vagina
Cervix
Uterus
UTERUS WITH FIBRO I DS
Fibroid
Fibroid
Fibroid
Fibroid
Fallopian tube
Ovary
Vagina
Cervix
Uterus
UTERUS WITH FIBRO I DS
46
Courtesy of Dr S. Singh

Evaluation
• Evaluate abnormal uterine bleeding
• Imaging to localize fibroids– Transvaginal ultrasound
– Saline infusion hysterography
– MRI
– Hysteroscopy
47
Fibroid
Fibroid
Fibroid
Fibroid
Fallopian tube
Ovary
Vagina
Cervix
Uterus
UTERUS W ITH FIBRO IDS
Fibroid
Fibroid
Fibroid
Fibroid
Fallopian tube
Ovary
Vagina
Cervix
Uterus
UTERUS W ITH FIBRO IDS
Courtesy of Dr S. Singh
PALM‐COEIN Classification of AUB
Leiomyoma Subclassification System
S M – Submucosal 0 Pedunculated Intracavitary
1 <50% Intramural
2 ≥ 50% Intramural
O – Other 3 Contacts endometrium; 100% Intramural
4 Intramural
5 Subserosal ≥50% Intramural
6 Subserosal < 50% Intramural
7 Subserosal Pedunculated
8 Other (specify, eg, cervical, parasitic)
00
22
33
11
44
5566
77
00
2-52-5
0
2
3
1
4
56
7
0
2-5
Polyp
Adenomyosis
Leiomyoma
Malignancy & Hyperplasia
Coagulopathy
Ovulatory Dysfunction
Endometrial
Iatrogenic
Not Yet Classified
Submucosal
Other
Munro MG et al; FIGO Working Group on Menstrual Disorders. Int J Gynaecol Obstet. 2011;113(1):3-13.
AUB=Acute uterine bleeding.
PALM = Visually objective structural criteria
COEI = unrelated to structural anomalies N = entities not yet classified
48Copyright © 2011, Elsevier Ireland Ltd. Reprinted with permission.

The Current State in the United States vs World 2017
USA Current Worldwide
SurgeryMyomectomy and Hysterectomy
InterventionalUterine Artery EmbolizationMRI Focused UltrasoundRadiofrequency Ablation
Medical Management of SymptomsBleeding – Hormonal Suppression and Tranexamic Acid
Pressure – GnRH agonist
X Long‐Term Medical Long‐Term MedicalSelective Progesterone Receptor Modulators
49GnRH=gonadotropin-releasing hormone.
Uterine Fibroid Treatment Algorithm
Singh SS, Belland L. Contemporary management of uterine fibroids: focus on emerging medical treatments. Current Medical Research and Opinion. 2015;31(1):1-12. Reprinted by permission of Taylor & Francis Ltd, http://www.tandfonline.com.
AsymptomaticAsymptomatic
Uterinefibroids
Symptomatic
Fertility notFertility notdesired
Fertilitydesired
Desire to preserveDesire to preserveuteruspreserve uterus
No desire topreserve uterus
Watchfulwaiting
HysterectomyHysterectomyPresurgicalmedical txPresurgicalmedical tx
Long termmedical txLong‐termmedical tx
Myomectomy
Uterine arteryembolizationUterine arteryembolization
Myolysis
EndometrialEndometrialablation
Presurgicalmedical tx
Long termmedical txLong‐termmedical tx
MyomectomyMyomectomy
Long termmedical txLong‐termmedical tx
Presurgicalmedical txPresurgicalmedical tx
Medical treatment includes:1. Fibroid‐directed therapies:
ulipristal acetate and GnRH agonists
2. Symptom‐relieving therapies (eg, OCs, Levonorgestrel IUS,danazol)IUS=Intrauterine system.
50

Symptomatic Fibroids
OPTIONS
Medical
Symptom Management
Targeted Therapy
Interventional Surgery
Myomectomy Hysterectomy
51
Courtesy of Dr S. Singh
Medical
Symptoms
TranexamicAcid
Hormonal Contraception
Targeted Therapy
SPRMsGnRH
Analogues
SPRMs=selective progesterone receptor modulators.
Symptomatic Fibroids
52
Courtesy of Dr S. Singh

Targeted Therapy
SPRMsGnRH
Analogues
Symptomatic Fibroids
53
Courtesy of Dr S. Singh
GnRH Agonists
• 35%–65% uterine/fibroid size
• 3–6 months preoperatively + Fe– Facilitates MIS surgery– Optimizes Hb prior to surgery
• Disadvantages: flare, vasomotor sx, bone loss (6%/ 12mo), grow back
Singh SS, Belland L. Curr Med Res Opin. 2015;31(1):1‐12. 54

GnRH Antagonists
• Novel oral agents that may mimic efficacy of GnRH agonist, but allow for dosing variation
• Elagolix is currently being studied
• Balancing side effect of hypoestrogenism is main challenge
ClinicalTrials.gov. Safety and Efficacy Pre-Menopausal Women With Heavy Uterine Bleeding and Uterine Fibroids. NCT01441635. https://clinicaltrials.gov/ct2/results?term=NCT01441635&Search=Search. Accessed April 28, 2017. 55
Symptomatic Fibroids
Long‐Term Targeted Therapy
SPRMs
56Courtesy of Dr S. Singh

SELECTIVE PROGESTERONE RECEPTOR MODULATORS (SPRMs)*
57*Not currently FDA approved for the treatment of uterine fibroids
Progesterone
Factors Controlling Fibroid Growth
From Walker CL, Stewart EA. Uterine fibroids: the elephant in the room. Science. 2005;308(5728):1589-1592.58
Reprinted with permission from American Association for the Advancement of Science.

Selective Progesterone Receptor Modulators
• First PR antagonist, mifepristone (RU 486), discovered in 1980
• Other PR ligands developed with mixed activity:
– Agonistic and/or antagonistic depending on the tissue (SPRMs):
Bouchard P et al. Fertil Steril. 2011;96(5):1175-1189; Spitz IM. Curr Opin Investig Drugs. 2006;7(10):882-890.
Antagonists AgonistsMesoprogestins
OnapristoneMifepristone
Ulipristal acetateAsoprisnil
Telapristone acetateJ 1042
ProgesteroneR5020 (synthetic
progestin)
59
Courtesy of Dr S. Singh
The SPRM Class
• Bind to progesterone receptors
• Modulate transcription in a positive or negative manner in tissue‐specific ways
• Have short‐term effects on endometrial proliferation
• Inhibit proliferation and induce apoptosis in cultured leiomyoma cells, but not normal myometrial cells
Bouchard P et al. Fertil Steril. 2011;96(5):1175-1189. 60

Vilaprisan Is a Potent Selective Progesterone Receptor Modulator
• Vilaprisan demonstrated a favorable, selective receptor‐binding profile
• Phase 1 and Phase 2 studies have confirmed the results from preclinical models
61
Wagenfeld A et al. Hum Reprod. 2013;28(8):2253-2264; Schütt B et al. Hum Reprod. 2016;31(8):1703-1712; Bradley L et al. Presented at: American Society for Reproductive Medicine Annual Meeting; October 16-20, 2016; Salt Lake City, UT. O-235.
SPRMs*THE KEY POINTS
*AVAILABLE SINCE JULY 2013 IN CANADA
62

Direct action on fibroids, reducing their size through the inhibition of cell proliferation and induction of apoptosis
Direct effect on the endometrium• Stops uterine bleeding• Results in benign and reversible changes in endometrial tissue, “Progesterone Receptor Modulator‐Associated Endometrial Changes” (PAEC)
Direct action on the pituitary, inducing amenorrhea by inhibiting ovulation and maintaining mid‐follicular phase levels of estradiol
Horak P et al. Int J Endocrinol. 2012;2012:436174; Donnez J et al; PEARL I Study Group. N Engl J Med.2012;366(5):409-420; Donnez J et al; PEARL II Study Group. N Engl J Med. 2012;366(5):421-432; Fibristal Product Monograph. Mississauga, Ontario, Canada: Actavis Specialty Pharmaceuticals Co. June 2013
PituitaryEndometriumFibroids
SPRM Mechanism of Action
63
Courtesy of Dr S. SinghCourtesy of Dr S. Singh
Ulipristal Acetate Clinical Trials: Randomized, Phase III
2008 2009 2010 2011 2012 2013 2014
June2012
Dec2014
451 patients in 11 countries
PEARL IV
Double‐blind
Jan2013
Jul2010
209 patients in 4 countries
PEARL III (and extension)
Open‐label
Aug2008
Jun2010
301 patients in 9 countriesPEARL II
• Parallel‐group•Double‐blind•Double‐dummy•Active‐comparator–controlled
Oct2008
Aug2010
• Parallel‐group•Double‐blind• Placebo‐controlled
241 patients in 6 countries
PEARL I
Donnez J et al; PEARL I Study Group. N Engl J Med. 2012;366(5):409-420; Donnez J et al; PEARL II Study Group. N Engl J Med. 2012;366(5):421-432; Donnez J et al; PEARL III and PEARL III Extension Study Group. Fertil Steril. 2014;101(6):1565-1573.e1-e18; Donnez et al. Fertil Steril. 2016;105(1):165-173.e4.
64
All Trials Conducted in Europe
Courtesy of Dr S. Singh

65
Ulipristal Acetate: Canadian Intermittent Dosing Schedule
Fibristal (ulipristal acetate) Canada Product Monograph, Allergan Inc. November 7, 2016.
Repeated intermittent treatment has been studied up to 4 intermittent courses.
Menses
UPA
5 mg 5 mg 5 mg 5 mg 5 mg
3 months on
3 months on
3 months on
3 months on
2 months off
2 months off
2 months off
2 months off
FIBRISTAL® (ulipristal acetate) is indicated for:• Treatment of moderate to severe signs and symptoms of uterine fibroids in adult women of reproductive age, who are
eligible for surgery• Intermittent treatment of moderate to severe signs and symptoms of uterine fibroids in adult women of reproductive ageThe duration of each treatment course is 3 months.
First treatment course begins during first week of menstruation
Treatment‐free intervals for one full menstrual cycle
Re‐treatment courses begin, at the earliest, during first week of second menstruation following previous treatment course
UPA=ulipristal acetate.
Courtesy of Dr S. Singh
Time to Control of Bleeding in Patients With PBAC <75
0
20
40
60
80
100
0 10 20 30 40 50 60 70 80 90 100
Time (days)
Patients (%)
7 days
Bleeding was controlled 7 days from treatment initiation in 75.9% of UPA 5 mg patients and in 82.7% of UPA 10 mg patients
Donnez J et al; PEARL I Study Group. N Engl J Med. 2012;366(5):409-420.
76% at 8 days92% EOT
EOT=end of treatment; PBAC=pictorial blood-loss assessment chart.66Courtesy of Dr S. Singh
UPA 10 mg PlaceboUPA 5 mg
Censored observations (ie, a patient had < 8 days at the end of the treatment period for which the total PBAC score met the criterion).

Time to Control of Bleeding (PBAC <75)
Donnez J et al; PEARL II Study Group. N Engl J Med. 2012;366(5):421-432.
0
20
40
60
80
100
0 10 20 30 40 50 60 70 80 90 100
Time (days)
Patients (%)
7 days 30 days
UPA 10 mg (n = 95) Leuprolide 3.75 mg (n = 93)UPA 5 mg (n = 93)
Uterine bleeding was controlled in 90% of patients on UPA 5 mg, in 98% of those on UPA 10 mg, and in 89% of those on leuprolide acetate
EOT:5 mg: 90% 10 mg: 98% GnRHa: 89%
30 days
67Courtesy of Dr S. Singh
Censored observations (ie, a patient had < 8 days at the end of the treatment period for which the total PBAC score met the criterion).
UPA vs GnRH agonist: Fibroid Volume Reduction
Donnez J et al; PEARL I Study Group. N Engl J Med. 2012;366(5):409-420; Donnez J et al; PEARL II Study Group. N Engl J Med. 2012;366(5):421-432; Donnez J et al; PEARL III and PEARL III Extension Study Group. Fertil Steril. 2014;101(6):1565–1573.e1-e18; Donnez J et al. Fertil Steril. 2016;105(1):165–173.e4.
Median change from baseline in fibroid volume* after each treatment course
• *PEARL I: total fibroid volume; PEARL II, III, IV: combined volume of 3 largest fibroids; †10-mg UPA dose not licensed 68
‐75
‐50
‐25
0
Treatment Course 2
Treatment Course 3
Treatment Course 4
3‐monthFollow‐up
Treatment Course 1
n 130 119 106 96 97207 189 173 160 158
Med
ian change in
fibroid volume (%
)
UPAPEARL IV
UPA†PEARL III
GnRHa (n = 93)
UPA (n = 93)
PEARL II
Placebo (n = 48)
UPA (n = 95)
PEARL I
Courtesy of Dr S. Singh

Ulipristal Acetate 5 mg Clinical Summary
• Rapidly stopped excessive bleeding: 75% normalized menstrual bleeding (7 days), 50% amenorrhea (10 days)
• After 3‐month course: 90%–92% controlled excessive menstrual bleeding, 73%–75% induced amenorrhea
• Significantly reduced volume of the 3 largest fibroids– Maintained for up to 6 months after treatment cessation
Compared to GnRH agonist, UPA:• Controlled bleeding faster• Maintained fibroid volume reduction for up to 6 months• Had a better side‐effect profile
Donnez J et al; PEARL II Study Group. N Engl J Med. 2012;366(5):421-432; Donnez J et al; PEARL I Study Group. N Engl J Med. 2012;366(5):409-420.
69
70

UPA Research in US Population
71
• Venus 1– Simon et al. American Society for Reproductive Medicine (ASRM) 2016
– Phase 3 randomized double‐blind study – UPA (2 doses) vs placebo – n=157, 69% African American
– UPA superior to placebo
Simon JA et al. Ulipristal acetate treatment of uterine fibroids in black and obese women: Venus I Subgroup Analyses [28G]. Obstet Gynecol. May 2017. Presented at: The American College of Obstetricians and Gynecologists; May 6-9, 2017; San Diego, CA.
Venus 1 – ACOG 2017
72
Simon JA et al. Ulipristal acetate treatment of uterine fibroids in black and obese women: Venus I Subgroup Analyses [28G]. Obstet Gynecol. May 2017. Presented at: The American College of Obstetricians and Gynecologists; May 6-9, 2017; San Diego, CA.
BMI=body mass index.© 2017 Allergan. All rights reserved. Used with Permission.

73
Sustainability of Fibroid Volumea Reduction in Subjects Who Did Not Undergo a Procedure
Donnez J et al; PEARL II Study Group. N Engl J Med. 2012;366(5):421-432.
aMeasured by ultrasoundbChange from end of treatment (week 13) to 6‐month follow‐up for UPA 5 mg and UPA 10 mg vs leuprolide p < .05
EOTFollow‐up
EOTFollow‐up
EOTFollow‐up
‐46
‐50
‐45b
‐56
‐17
‐43
‐62
‐57‐55b
3‐mo 6‐mo 3‐mo 6‐mo 3‐mo 6‐mo
LeuprolideUPA 5 mg UPA 10 mg
0
‐10
‐20
‐30
‐40
‐50
‐60
‐70n = 45 n = 46 n = 44
Courtesy of Dr S. SinghUAE=uterine artery embolization.
SPRM Safety Summary
• Safe overall with some nuisance side effects
• No evidence that it leads to endometrial hyperplasia or malignancy
• Progesterone receptor modulator‐associated change
74

Progesterone Receptor Modulator‐Associated ChangeBenign Condition and Completely Reversible
Singh SS, Belland L. Curr Med Res Opin. 2015;31(1):1‐12. 75
Courtesy of Dr S. Singh
Limitations of SPRM Treatment
• Non‐responders– 20% of fibroid volume– <10% bleeding
• Intermittent use
• Effects on surgical planes?
• Reproductive effects long term
76
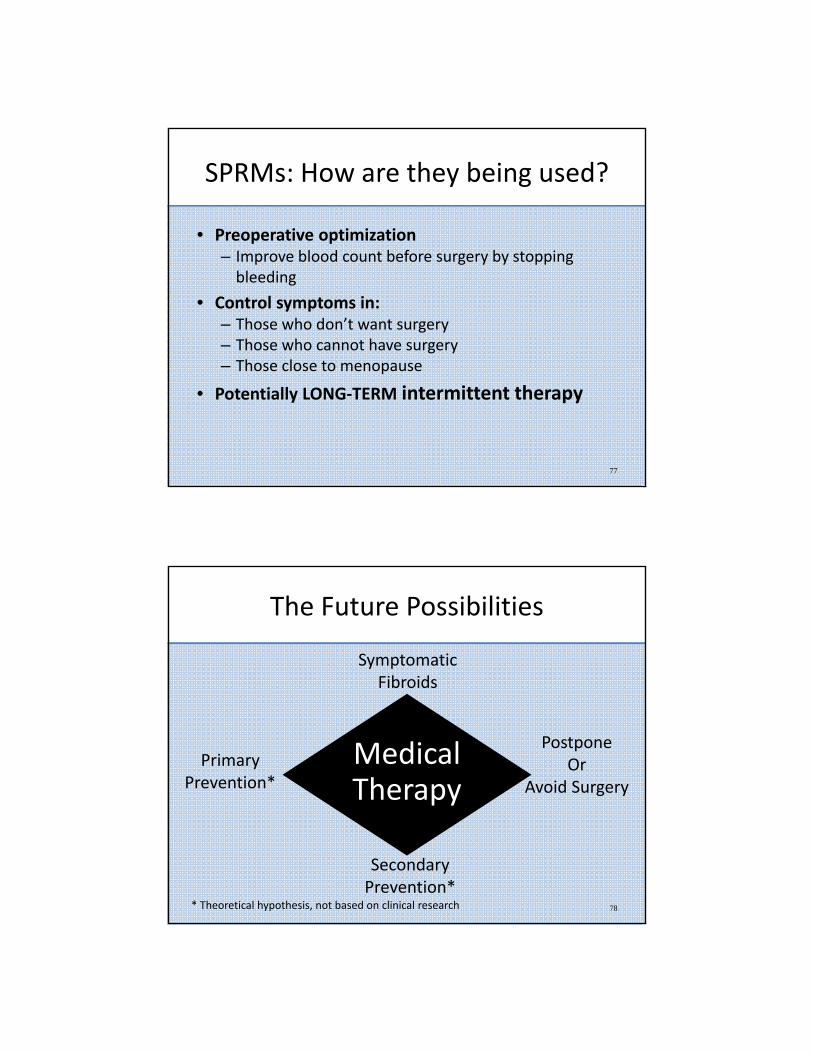
SPRMs: How are they being used?
• Preoperative optimization– Improve blood count before surgery by stopping bleeding
• Control symptoms in:– Those who don’t want surgery– Those who cannot have surgery– Those close to menopause
• Potentially LONG‐TERM intermittent therapy
77
The Future Possibilities
Medical Therapy
78
Symptomatic Fibroids
PostponeOr
Avoid Surgery
PrimaryPrevention*
SecondaryPrevention*
* Theoretical hypothesis, not based on clinical research

79