the international federation of gynecology and obstetrics
TRANSCRIPT

Int J Gynecol Obstet 2019; 145 (Suppl. 1): 1–33 wileyonlinelibrary.com/journal/ijgo | 1© 2019 International Federation of Gynecology and Obstetrics
DOI: 10.1002/ijgo.12802
S U P P L E M E N T A R T I C L E
The International Federation of Gynecology and Obstetrics (FIGO) initiative on pre- eclampsia: A pragmatic guide for first- trimester screening and prevention
Liona C. Poon1,* | Andrew Shennan2 | Jonathan A. Hyett3 | Anil Kapur4 | Eran Hadar5 | Hema Divakar6 | Fionnuala McAuliffe7 | Fabricio da Silva Costa8 | Peter von Dadelszen2 | Harold David McIntyre9 | Anne B. Kihara10 | Gian Carlo Di Renzo11 | Roberto Romero12 | Mary D'Alton13 | Vincenzo Berghella14 | Kypros H. Nicolaides15 | Moshe Hod5
1DepartmentofObstetricsandGynecology,PrinceofWalesHospital,TheChineseUniversityofHongKong,Shatin,HongKongSAR2Department of Women and Children's Health, School of Life Course Sciences, Faculty of Life Sciences and Medicine, King's College London, London, UK3DisciplineofObstetrics,GynecologyandNeonatology,FacultyofMedicine,UniversityofSydney,Sydney,NSW,Australia4WorldDiabetesFoundation,Bagsværd,Denmark5HelenSchneiderHospitalforWomen,RabinMedicalCenter,PetahTikva,andSacklerFacultyofMedicine,TelAvivUniversity,TelAviv,Israel6DivakarsSpecialityHospital,Bangalore,India7DepartmentofObstetricsandGynecology,TheNationalMaternityHospital,Dublin,Ireland8DepartmentofGynecologyandObstetrics,RibeirãoPretoMedicalSchool,UniversityofSãoPaulo,SãoPaulo,Brazil9UniversityofQueenslandMaterClinicalSchool,Brisbane,QLD,Australia10AfricanFederationofObstetricsandGynaecology,Khartoum,Sudan11CenterofPerinatalandReproductiveMedicine,DepartmentofObstetricsandGynecology,UniversityofPerugia,Perugia,Italy12PerinatologyResearchBranch,DivisionofObstetricsandMaternal-FetalMedicine,DivisionofIntramuralResearch,Eunice Kennedy ShriverNationalInstituteofChildHealthandHumanDevelopment,NationalInstitutesofHealth,USDepartmentofHealthandHumanServices,Bethesda,MD,andDetroit,MI,USA13ObstetricianandGynecologistin-Chief,ColumbiaUniversityIrvingMedicalCenter,NewYork-Presbyterian14DivisionofMaternal-FetalMedicine,DepartmentofObstetricsandGynecology,SidneyKimmelMedicalCollegeofThomasJeffersonUniversity,Philadelphia,PA,USA15FetalMedicineResearchInstitute,King‘sCollegeHospitalLondon,London,UK
*CorrespondenceLionaC.Poon,DepartmentofObstetricsandGynecology,PrinceofWalesHospital,TheChineseUniversityofHongKong,Shatin,HongKongSAR.Email:[email protected]
Funding InformationPerkinElmerInc
[Correctionaddedon18June2019,afterfirstonlinepublication:theaffiliationforMaryD’Altonhasbeencorrectedinthisversion.]

2 | Poon ET AL.
ACKNOWLEDGMENTS
ThisprojectwasfundedbyanunrestrictededucationalgrantfromPerkinElmerInc,Waltham,USA,representedbyYvonneParker,VPMarketDevelopment,ReproductiveHealth,PerkinElmerInc.
CONFLICTS OF INTEREST
Theauthorshavenoconflictsofinteresttodeclare.
CONTRIBUTORS
Inadditiontotheauthors,thefollowingpeopleprovidedimportantcontributionsduringthecreationofthedocument.Thanksgotothefollow-inginternationalexperts:ThePregnancyandNCDCommitteemembers:MosheHod,HemaDivakar,MarkHanson,AnilKapur,HaroldDavidMcIntyre,MaryD‘Alton,AnneB.Kihara,RonaldMa,FionnualaMcAuliffe,GianCarloDiRenzo,andCNPurandare.Special thanks forFIGOguidanceandcoordinationgotoPresidentCarlosFuchtner,Past-PresidentCNPurandare,Past-ChairoftheSMNHCommitteeGerardVisser,alongwithJessicaMorrisandRachelGooden(FIGOProjectManagerandCoordinator).InadditiontotheFIGOExecutiveBoard,variousFIGOCommitteesandWorkingGroupscontributedtoandsupportedthedocument.
| 3Poon ET AL.
CONTENTS
1. Executivesummary
2. TargetaudienceoftheFIGOinitiativeonpre-eclampsia
3. Assessmentofqualityofevidenceandgradingofrecommendations
4. Pre-eclampsia:background,definition,riskfactors,maternalandperinatalmorbidityandmortalityassociatedwithpre-eclampsia
5. Firsttrimesterpredictionofpre-eclampsia
6. Firsttrimesterpreventionofpre-eclampsia
7. Resource-basedapproachtoscreening
8. Cost-effectivenessofpre-eclampsiascreening
Supporting Information
AdditionalsupportinginformationmaybefoundonlineintheSupportingInformationsectionattheendofthearticle.
Appendix S1. Formulas for calculation of multiple of the median (MoM) values at 11–13weeks of gestation. Algorithm for prediction ofpre-eclampsia.

4 | Poon ET AL.
LIST OF ABBREVIATIONS/ACRONYMS
ACOG AmericanCollegeofObstetricsandGynecologyAPS AntiphospholipidsyndromeART AssistedreproductivetechnologiesASPRE Combinedmultimarkerscreeningandrandomizedpatienttreatmentwithaspirinforevidence-basedpre-eclampsiapreventionAUC AreaunderreceiveroperatingcharacteristiccurveBMI BodymassindexCI ConfidenceintervalCRL Crown–rumplengthdBP DiastolicbloodpressureDR DetectionrateFGR FetalgrowthrestrictionFIGO InternationalFederationofGynecologyandObstetricsGI GastrointestinalGWAS Genome-wideassociationstudiesHELLP Hemolysis,elevatedliverenzyme,lowplateletHR HazardratioIAD InterarmdifferenceICSI IntracytoplasmicsperminjectionIGF Insulin-likegrowthfactorIQ IntelligencequotientISSHP InternationalSocietyfortheStudyofHypertensioninPregnancyIUFD Intrauterine fetal deathIUI IntrauterineinseminationIVF InvitrofertilizationMAP MeanarterialpressureMoM MultipleofmedianNCDs Noncommunicable diseasesNHFA NationalHeartFoundationofAustraliaNICE NationalInstituteforHealthandCareExcellenceNICU Neonatal intensive care unitOR OddsratioPAPP-A Pregnancy-associatedplasmaproteinAPE Pre-eclampsiaPLGF Placental growth factorPOC Point of careRR RelativerisksBP SystolicbloodpressureSD StandarddeviationSGA SmallforgestationalageSLE Systemic lupus erythematosusUA UmbilicalarteryUTPI UterinearterypulsatilityindexVEGF-R1Vascularendothelialgrowthfactorreceptor1VEGF Vascularendothelialgrowthfactor

| 5Poon ET AL.
1 | EXECUTIVE SUMMARY
Pre-eclampsia (PE) is a multisystem disorder that typically affects2%–5% of pregnant women and is one of the leading causes of mater-nal and perinatal morbidity and mortality, especially when the condi-tionisofearlyonset.Globally,76000womenand500000babiesdieeach year from this disorder. Furthermore,women in low-resourcecountriesareatahigherriskofdevelopingPEcomparedwiththoseinhigh-resourcecountries.
Although a complete understanding of the pathogenesis of PEremainsunclear,thecurrenttheorysuggestsatwo-stageprocess.Thefirststageiscausedbyshallowinvasionofthetrophoblast,resultingininadequateremodelingofthespiralarteries.Thisispresumedtoleadto the second stage, which involves the maternal response to endo-thelialdysfunctionandimbalancebetweenangiogenicandantiangio-genicfactors,resultingintheclinicalfeaturesofthedisorder.
Accurate prediction and uniform prevention continue to eludeus.ThequesttoeffectivelypredictPE inthefirsttrimesterofpreg-nancyisfueledbythedesiretoidentifywomenwhoareathighriskofdevelopingPE, so thatnecessarymeasurescanbe initiatedearlyenoughto improveplacentationandthuspreventorat leastreducethefrequencyofitsoccurrence.Furthermore,identificationofan“atrisk”groupwillallowtailoredprenatalsurveillancetoanticipateandrecognizetheonsetoftheclinicalsyndromeandmanageitpromptly.
PE has been previously defined as the onset of hypertensionaccompanied by significant proteinuria after 20weeks of gestation.Recently,thedefinitionofPEhasbeenbroadened.Nowtheinterna-tionallyagreeddefinitionofPEistheoneproposedbytheInternationalSociety for the Study of Hypertension in Pregnancy (ISSHP).
Accordingtothe ISSHP,PE isdefinedassystolicbloodpressureat≥140mmHgand/ordiastolicbloodpressureat≥90mmHgonatleast two occasions measured 4 hours apart in previously normoten-sivewomenandisaccompaniedbyoneormoreofthefollowingnew-onsetconditionsatorafter20weeksofgestation:
1. Proteinuria (i.e. ≥30mg/mol protein:creatinine ratio;≥300mg/24hour; or ≥2+dipstick);
2. Evidenceofothermaternalorgandysfunction,including:acutekid-ney injury (creatinine ≥90μmol/L; 1 mg/dL); liver involvement (elevated transaminases, e.g. alanine aminotransferase or aspartate aminotransferase>40IU/L)withorwithoutrightupperquadrantor epigastric abdominal pain; neurological complications (e.g.eclampsia,alteredmentalstatus,blindness,stroke,clonus,severeheadaches, and persistent visual scotomata); or hematological com-plications (thrombocytopenia–platelet count <150000/μL, dis-seminatedintravascularcoagulation,hemolysis);or
3. Uteroplacentaldysfunction(suchasfetalgrowthrestriction,abnor-malumbilicalarteryDopplerwaveformanalysis,orstillbirth).
It is well established that a number of maternal risk factors areassociated with the development of PE: advanced maternal age; nulli-parity; previous history of PE; short and long interpregnancy interval; useofassistedreproductivetechnologies;familyhistoryofPE;obesity;
Afro-CaribbeanandSouthAsianracialorigin;co-morbidmedicalcondi-tionsincludinghyperglycemiainpregnancy;pre-existingchronichyper-tension; renal disease; and autoimmune diseases, such as systemic lupus erythematosusandantiphospholipidsyndrome.Theseriskfactorshavebeendescribedbyvariousprofessionalorganizationsfortheidentifica-tionofwomenatriskofPE;however,thisapproachtoscreeningisinad-equateforeffectivepredictionofPE.
PEcanbesubclassifiedinto:
1. Early-onset PE (with delivery at <34+0weeks of gestation);2. PretermPE(withdeliveryat<37+0weeksofgestation);3. Late-onsetPE(withdeliveryat≥34+0weeksofgestation);4. TermPE(withdeliveryat≥37+0weeksofgestation).
Thesesubclassificationsarenotmutuallyexclusive.Early-onsetPEisassociatedwithamuchhigherriskofshort-andlong-termmaternalandperinatal morbidity and mortality.
Obstetricians managing women with preterm PE are faced with the challengeofbalancing theneed to achieve fetalmaturation inuterowiththeriskstothemotherandfetusofcontinuingthepreg-nancy longer.These risks include progression to eclampsia, devel-opmentofplacentalabruptionandHELLP(hemolysis,elevatedliverenzyme,lowplatelet)syndrome.Ontheotherhand,pretermdeliveryis associated with higher infant mortality rates and increased morbid-ityresultingfromsmallforgestationalage(SGA),thrombocytopenia,bronchopulmonarydysplasia,cerebralpalsy,andanincreasedriskofvariouschronicdiseasesinadultlife,particularlytype2diabetes,car-diovasculardisease,andobesity.WomenwhohaveexperiencedPEmayalsofaceadditionalhealthproblemsinlaterlife,astheconditionisassociatedwithanincreasedriskofdeathfromfuturecardiovas-culardisease,hypertension,stroke,renalimpairment,metabolicsyn-drome,anddiabetes.ThelifeexpectancyofwomenwhodevelopedpretermPEisreducedonaverageby10years.Thereisalsosignifi-cantimpactontheinfantsinthelongterm,suchasincreasedrisksof insulin resistance, diabetes mellitus, coronary artery disease, and hypertensionininfantsborntopre-eclampticwomen.
TheInternationalFederationofGynecologyandObstetrics(FIGO)broughttogetherinternationalexpertstodiscussandevaluatecurrentknowledgeonPEanddevelopadocument to frame the issuesandsuggestkeyactionstoaddressthehealthburdenposedbyPE.
FIGO'sobjectives,asoutlined in thisdocument,are: (1)To raiseawarenessofthe linksbetweenPEandpoormaternalandperinataloutcomes,aswellastothefuturehealthriskstomotherandoffspring,anddemandaclearlydefinedglobalhealthagendatotacklethisissue;and (2) To create a consensus document that provides guidance for the first-trimesterscreeningandpreventionofpretermPE,andtodissem-inate and encourage its use.
Based on high-quality evidence, the document outlines currentglobal standards for the first-trimester screening and prevention ofpretermPE,whichisinlinewithFIGOgoodclinicalpracticeadviceonfirsttrimesterscreeningandpreventionofpre-eclampsiainsingletonpregnancy.1

6 | Poon ET AL.
Itprovidesboth thebestand themostpragmatic recommenda-tions according to the level of acceptability, feasibility, and ease ofimplementationthathavethepotential toproducethemostsignifi-cant impact indifferent resource settings. Suggestionsareprovidedforavarietyofdifferentregionalandresourcesettingsbasedontheirfinancial,human,andinfrastructureresources,aswellasforresearchprioritiestobridgethecurrentknowledgeandevidencegap.
To deal with the issue of PE, FIGO recommends the following:Public health focus:Thereshouldbegreater internationalatten-
tiongiventoPEandtothelinksbetweenmaternalhealthandnon-communicable diseases (NCDs) on the Sustainable Developmental Goals agenda. Public health measures to increase awareness, access, affordability, andacceptanceofpreconceptioncounselling, andpre-natal and postnatal services forwomen of reproductive age shouldbeprioritized.Greatereffortsarerequiredtoraiseawarenessofthebenefitsofearlyprenatalvisitstargetedatreproductive-agedwomen,particularlyinlow-resourcecountries.
Universal screening:Allpregnantwomenshouldbescreenedforpreterm PE during early pregnancy by the first-trimester combinedtestwithmaternal risk factorsandbiomarkersasaone-stepproce-dure. The risk calculator is available free of charge at https://fetal-medicine.org/research/assess/preeclampsia. FIGO encourages all countriesanditsmemberassociationstoadoptandpromotestrate-gies to ensure this. The best combined test is one that includes mater-nalriskfactors,measurementsofmeanarterialpressure(MAP),serum
placental growth factor (PLGF), and uterine artery pulsatility index(UTPI). Where it is not possible to measure PLGF and/or UTPI, the baselinescreeningtestshouldbeacombinationofmaternalriskfac-torswithMAP,andnotmaternalriskfactorsalone.Ifmaternalserumpregnancy-associatedplasmaproteinA(PAPP-A)ismeasuredforrou-tinefirst-trimesterscreeningforfetalaneuploidies,theresultcanbeincludedforPEriskassessment.Variationstothefullcombinedtestwouldleadtoareductionintheperformancescreening.Awomanisconsideredhighriskwhentheriskis1in100ormorebasedonthefirst-trimestercombinedtestwithmaternal risk factors,MAP,PLGF,and UTPI.
Contingent screening: Where resources are limited, routinescreeningforpretermPEbymaternalfactorsandMAPinallpregnan-cies and reserving measurements of PLGF and UTPI for a subgroup of thepopulation(selectedonthebasisoftheriskderivedfromscreen-ingbymaternalfactorsandMAP)canbeconsidered.
Prophylactic measures: Following first-trimester screening forpretermPE,womenidentifiedathighriskshouldreceiveaspirinpro-phylaxis commencing at 11–14+6weeks of gestation at a dose of~150mgtobetakeneverynightuntil36weeksofgestation,whendelivery occurs, orwhen PE is diagnosed. Low-dose aspirin shouldnot be prescribed to all pregnant women. In women with low calcium intake(<800mg/d),eithercalciumreplacement(≤1gelementalcalci-um/d)orcalciumsupplementation(1.5–2gelementalcalcium/d)mayreducetheburdenofbothearly-andlate-onsetPE.

| 7Poon ET AL.
2 | TARGET AUDIENCE OF THE FIGO INITIATIVE ON PRE- ECLAMPSIA
This document is directed at multiple stakeholders with the inten-tionofbringingattentiontoPE,whichisapreventablebutcommonandpotentiallylife-threateningcomplicationofpregnancywithgraveconsequencesforboththemothersandtheoffspring.ThisdocumentproposestocreateaglobalframeworkforactionforearlyscreeningandpreventionofPE.
The intended target audience includes:
• Healthcare providers:Allthosewhoarequalifiedtocareforpreg-nantwomenandtheirnewborns,butinparticularthoseresponsi-bleforscreeningforhigh-riskwomen(obstetricians,maternal-fetalmedicine specialists, internists, pediatricians, neonatologists, gen-eral practitioners/family physicians, midwives, nurses, advancepractice clinicians, nutritionists, pharmacists, community healthworkers,laboratorytechnicians,etc.)
• Healthcare delivery organizations and providers: governments, federalandstatelegislators,healthcaremanagementorganizations,health insurance organizations, international development agen-cies,andnongovernmentalorganizations.
• Professional organizations: international, regional, and nationalprofessional organizations of obstetricians and gynecologists,internists, family practitioners, pediatricians, neonatologists, andworldwidenationalorganizationsdedicatedtothecareofpregnantwomen with PE.
3 | QUALITY ASSESSMENT OF EVIDENCE AND GRADING OF STRENGTH OF RECOMMENDATIONS
Inassessing thequalityofevidenceandgradingof strengthof rec-ommendations, thedocument follows the terminologyproposedbythe Grading of Recommendations, Assessment, Development andEvaluation(GRADE)workinggroup(http://www.gradeworkinggroup.org/).Thissystemusesconsistentlanguageandgraphicaldescriptionsforthestrengthandqualityoftherecommendationsandtheevidenceonwhichtheyarebased.Strongrecommendationsarenumberedas1andconditional(weak)recommendationsarenumbered2.Forthequalityofevidence,cross-filledcirclesareused:⊕OOO denotes very low-qualityevidence;⊕⊕OO lowquality;⊕⊕⊕Omoderatequality;and ⊕⊕⊕⊕high-qualityevidence(Tables1and2).
T A B L E 1 Interpretationofstrongandconditional(weak)recommendationsaccordingtoGRADE.a,b
Implications1=Strong recommendation phrased as “we recommend” 2=Conditional (weak) recommendation phrased as “we
suggest”
Forpatients Nearlyallpatientsinthissituationwouldaccepttherecommendedcourseofaction.Formaldecisionaidsarenotneededtohelppatientsmakedecisionsconsistentwiththeir values and preferences
Mostpatientsinthissituationwouldacceptthesuggestedcourseofaction
For clinicians Accordingtotheguidelinesperformanceoftherecom-mendedactioncouldbeusedasaqualitycriterionorperformanceindicator,unlessthepatientrefuses
Decisionaidsmayhelppatientsmakeamanagementdecision consistent with their values and preferences
Forpolicymakers Therecommendationcanbeadaptedaspolicyinmostsituations
Stakeholdersneedtodiscussthesuggestion
aReprintedwithpermissionoftheAmericanThoracicSociety.©2019AmericanThoracicSociety.SchunemannHJ,JaeschkeR,CookDJ,etal.AnofficialATSstatement:gradingthequalityofevidenceandstrengthof recommendations inATSguidelinesandrecommendations.Am J Respir Crit Care Med 2006;174:605–614.TheAmericanJournalofRespiratoryandCriticalCareMedicineisanofficialjournaloftheAmericanThoracicSociety.bBothcaregiversandcarerecipientsneedtobeinvolvedinthedecision-makingprocessbeforeadoptingrecommendations.
T A B L E 2 InterpretationofqualityofevidencelevelsaccordingtoGRADE.a
Level of evidence Definition
High ⊕⊕⊕⊕
Weareveryconfidentthatthetrueeffectcorrespondstothatoftheestimatedeffect
Moderate ⊕⊕⊕O
Wearemoderatelyconfidentintheestimatedeffect.Thetrueeffectisgenerallyclosetotheestimatedeffect,butitmaybeslightlydifferent
Low ⊕⊕OO
Ourconfidenceintheestimatedeffectislimited.Thetrueeffectcouldbesubstantiallydifferentfromtheestimatedeffect
Verylow ⊕OOO
Wehaveverylittleconfidenceintheestimatedeffect.Thetrueeffectislikelytobesubstantiallydifferentfromtheestimatedeffect
aAdaptedwithpermissionfromBalshemetal.GRADEguidelines:3.Ratingthequalityofevidence.J Clin Epidemiol2011;64:401–6.©Elsevier(2011).

8 | Poon ET AL.
4 | PRE- ECLAMPSIA: BACKGROUND, DEFINITION, RISK FACTORS, MATERNAL AND PERINATAL MORBIDITY AND MORTALITY ASSOCIATED WITH PRE- ECLAMPSIA
4.1 | Introduction
Pre-eclampsia(PE) isamultisystemdisorderofpregnancypreviouslydefinedbytheonsetofhypertensionaccompaniedbysignificantpro-teinuriaafter20weeksofgestation.Recently,thedefinitionofPEhasbeen broadened.2–5 PE typically affects2%–5%ofpregnantwomenand is one of the leading causes of maternal and perinatal morbidity and mortality,especiallywhentheconditionisofearlyonset.6,7 Globally, 76 000 women and 500 000 babies die each year from this disorder.8 Furthermore,womeninlow-resourcecountriesareatahigherriskofdevelopingPEcomparedwiththoseinhigh-resourcecountries.
PEcanbesubclassifiedinto:
1. Early-onset PE (with delivery at <34+0weeks of gestation);2. PretermPE(withdeliveryat<37+0weeksofgestation);3. Late-onsetPE(withdeliveryat≥34+0weeksofgestation);4. TermPE(withdeliveryat≥37+0weeksofgestation).
Thesesubclassificationsarenotmutuallyexclusive.Early-onsetPEisassociatedwithasubstantialriskofbothshort-andlong-termmaternaland perinatal morbidity and mortality.9,10
Although a complete understanding of the pathogenesis remainsunclear,thecurrenttheorysuggestsatwo-stageprocess.Thefirststageiscausedbyshallowinvasionofthetrophoblastresultingininadequateremodeling of the spiral arteries.11–13 This is presumed to lead to the second stage, which involves the maternal response to endothelial dys-functionandimbalancebetweenangiogenicandantiangiogenicfactors,resultingintheclinicalfeaturesofthedisorder.11–13Inlate-onsetdisease,placentationisusuallynormal;however,feto-placentaldemandsexceedsupply,resultinginaplacentalresponsethattriggerstheclinicalphenotype.WhilsttheplacentacertainlyplaysanessentialroleinthedevelopmentofPE, there is a growing body of evidence that the maternal cardiovascular systemmayhaveasignificantcontributiontothedisorder.14
WhileknowledgeofthecomplexpathophysiologyofPEisimproving,accuratepredictionanduniformpreventioncontinuetoeludeus.ThequesttoeffectivelypredictPEinthefirsttrimesterofpregnancyisfueledbythedesiretoidentifywomenwhoareathighriskofdevelopingPE,sothatnecessarymeasurescanbeinitiatedearlytoimproveplacentationandreducetheprevalenceofthedisease.Furthermore,identificationofan“atrisk”groupwillfacilitatetailoredprenatalsurveillancetoanticipateandrecognizetheonsetoftheclinicalsyndromeandmanageitpromptly.
4.2 | Definition of pre- eclampsia
PEisbroadlydefinedasdevelopmentofhypertensionandproteinu-riainapreviouslynormotensivewoman.Thedifficultyininterpreting
epidemiologicalstudiesofPEisduetothewidevariationinthedefi-nitionsofthedisease.Thereareseveraldefinitionsforthediagnosisof PE that have been reported in published literature and proposed byvariousprofessionalbodies.Consequently,thishasresultedinsev-eraldifferentguidelinesproducedbyprofessionalbodiesworldwidefor the diagnosis and management of PE.2,15–17 However, an inter-nationallyagreeddefinitionofPEisthatoftheInternationalSocietyfor the Study of Hypertension in Pregnancy (ISSHP)5(Box1),whichisendorsed by FIGO.
Gestationalhypertensionisdefinedassystolicbloodpressure(sBP)at≥140mmHgand/ordiastolicbloodpressure(dBP)at≥90mmHgon at least two occasionsmeasured 4hours apart developing after20weeksofgestationinpreviouslynormotensivewomen.
PE is defined as gestational hypertension accompanied by≥1of the following new-onset conditions at or after 20weeksofgestation:
1. Proteinuria (i.e. ≥30mg/mol protein:creatinine ratio;≥300mg/24hour; or ≥2+dipstick);
2. Othermaternal organdysfunction, including: acute kidney injury(creatinine ≥90μmol/L; 1 mg/dL); liver involvement (elevated transaminases, e.g. alanine aminotransferase or aspartate ami-notransferase>40IU/L)withorwithout rightupperquadrantorepigastricabdominalpain;neurologicalcomplications(e.g.eclamp-sia, alteredmental status,blindness, stroke, clonus, severehead-aches, and persistent visual scotomata); or hematological complications (thrombocytopenia–platelet count <150000/μL, disseminatedintravascularcoagulation,hemolysis);or
3. Uteroplacental dysfunction (such as fetal growth restriction,abnormal umbilical artery Doppler waveform analysis, or stillbirth).
4.3 | Risk factors
Itiswellestablishedthatanumberofmaternalriskfactorsareasso-ciated with the development of PE. These risk factors have beendescribedbyvariousprofessionalorganizationsfortheidentificationofwomenatriskofPE.3,4,16,18,19
4.3.1 | Maternal age
Advanced maternal age, defined as age greater than or equal to35years at the time of delivery, is associated with 1.2 to 3-foldincreased risk of developing PE.19–22 Predictive probability of PEincreases when maternal age is greater than 35 years and the prob-ability further increases rapidly when maternal age is greater than
FIGO adopts the definition of PE as provided by theInternational Society for the Study of Hypertension inPregnancy (ISSHP).

| 9Poon ET AL.
40 years.19Onestudyhasevaluatedthematernalageassociatedriskaccording to the severity of PE. Using multivariate logistic regres-sionanalysis,adjustingforconfounders,theriskforlate-onsetPEhasbeenshowntoincreaseby4%withevery1-yearincreaseinmaternalage above 32 years.23 However, maternal age is not associated with increasedriskofearly-onsetPE.23
4.3.2 | Parity
Innulliparouswomen,the increasedriskofdevelopingPEhasbeenwidelyreported.OnesystematicreviewreportedthattheriskofPEis increased three-fold in nulliparouswomen.24 Another systematicreviewthat included26studiesreportedthatthis increasedriskforPEpersistsevenafteradjustingforotherriskfactors,suchasmaternalage,race,andbodymassindex(BMI)andthesummaryadjustedoddsratio (OR)was 2.71 (95%CI, 1.96–3.74).25 Parous women without priorhistoryofPEhavereducedriskofPE;however,thisprotectiveeffectislostwhentheconceptionpartnerisdifferent.26
4.3.3 | Previous history of PE
Alargepopulation-basedstudyincluding763795nulliparouswomenwithafirstdeliverybetween1987and2004showedthattheriskofPEwas4.1%inthefirstpregnancyand1.7%inlaterpregnanciesoverall.However,theriskwas14.7%inthesecondpregnancyforwomenwithahistoryofPEintheirfirstpregnancyand31.9%forwomenwhohadPEintheprevioustwopregnancies.TheriskofPEforparouswomenwithoutahistoryofPEwas1.1%.TheseobservationssuggestthattheriskofPEisgreaterinnulliparousthanparouswomenwithoutapriorhistoryofPE.Amongparouswomen,theriskofPEinsubsequentpreg-nancies depends on a prior history of PE.27Thisrelativeriskforsubse-quentPErangesfrom7to10timeshigherinasecondpregnancy.28–30
Astudy focusingonPEaccording to severityofdiseaseshowedthat a history of PE doubled the risk of developing early-onset PE(<32weeks) in a subsequent pregnancy as opposed to late-onsetPE.31 Other studies have reported a 5% to 17% recurrence risk ofearly-onsetPE (<34weeks) in the indexpregnancy for thosewith aprior historyof early-onsetPE.32,33A systematic reviewof11 stud-iesincluding2377womenshowedthatthepooledrecurrenceriskofearly-onsetPEisapproximately8%inwomenwhorequiredeliveryatlessthan34weeksfollowingthedevelopmentofearly-onsetPEinthefirstpregnancy.33
4.3.4 | Pregnancy interval
Both short and long interpregnancy intervals are associatedwith anincreased risk of PE.34–36 A recent large multicentric retrospectivestudy of 894 479 women reported that interpregnancy intervals of less than 12 months or greater than 72 months are associated with higherriskofPEdevelopmentcomparedwithinterpregnancyintervalsof 12–23 months.37 It has been observed that the longer the interval, thehighertheriskofdevelopingPE.Thereasonsfortheassociationbetween short interpregnancy interval and PE are unclear, but several
hypotheses have been proposed, including factors related to socioeco-nomicstatus,postpartumstress,malnutrition,and inadequateaccesstohealthcareservices.Meanwhile,theincreasedPEriskinwomenwithlonginterpregnancyintervalsmightbeattributedtoadvancedmaternalage,infertility,andunderlyingmaternalmedicalconditions.38,39
4.3.5 | Assisted reproduction
Several studieshave reported that theuseofassisted reproductivetechnologies (ART) doubles the risk of PE.40–43 In a cohort study ofmore than1million pregnantwomen, the risk of havingPEwasincreased in women exposed to hyperestrogenic ovarian stimula-tionmedications regardlessofART typecomparedwith thosewithspontaneousconception (ORs ranging from1.32 to1.83).44 In con-trast, the use of nonhyperestrogenic ovarian stimulationdrugswas
Box 1 Diagnosis of hypertensive disorders in pregnancy according to ISSHP.a
Gestational hypertension• Persistentdenovohypertension(sBP≥140mmHgand/ordBP≥90mmHgafter20weeksofgestationintheabsenceoffeatures of PE.
PE de novo• Gestationalhypertensionaccompaniedby≥1ofthefollowingnew-onsetconditionsatorafter20weeksofgestation:- Proteinuria:24-hurineprotein≥300mg/dorspoturineprotein/creatinineratio≥0.30mg/mgorurinedipsticktesting≥1+
- Othermaternalorgandysfunction: Acutekidneyinjury(creatinine≥90μmol/L; 1 mg/dL) Liver involvement (elevated alanine aminotransferase or
aspartate aminotransferase >40 IU/L) with or without rightupperquadrantorepigastricpain)
Neurologicalcomplications(includingeclampsia,alteredmentalstatus,blindness,stroke,ormorecommonlyhyperreflexiawhenaccompaniedbyclonus,severeheadaches, and persistent visual scotomata)
Hematologicalcomplications(thrombocytopenia–plateletcount<150000/μL, disseminated intravascular coagula-tion,hemolysis)
Uteroplacentaldysfunction(fetalgrowthrestriction,abnormal umbilical artery Doppler waveform or stillbirth).
Superimposed PE on chronic hypertension• WomenwithchronicessentialhypertensiondevelopanyoftheabovematernalorgandysfunctionsconsistentwithPE
• Increaseinbloodpressureperseisnotsufficienttodiagnosesuperimposed PE
• Intheabsenceofpre-existingproteinuria,new-onsetproteinuriainthesettingofariseinbloodpressureissufficientto diagnose superimposed PE
In women with proteinuric renal disease, an increase in proteinuria duringpregnancyisnotsufficientpersetodiagnosesuperim-posed PE
aSource:Brownetal.5

10 | Poon ET AL.
not associatedwith an increased risk of PE.44 High estrogen levels during implantationmay lead to impairedplacentationand reduceduteroplacentalcirculationaswellasdecreasednumberofuterinespi-ral arteries with vascular invasion.44–46 Women conceiving by intrau-terineinsemination,inparticularbydonorsperm,areatagreaterriskof developing PE.47–51 Those who have undergone donor ovum in vitrofertilization(IVF)appeartohaveahigherriskofPEthanthosewhohavehadautologousovumIVF.52Evidencefrom IVFpregnan-cieswithovumdonationsuggeststhattherearealteredextravilloustrophoblast and immunological changes in decidua basalis, which may impedethemodificationofthespiralarteries.53
4.3.6 | Family history of PE
AlthoughmostcasesofPEaresporadic,afamilialsusceptibilitytoPEhas been documented. Daughters or sisters of women with PE are 3–4timesmorelikelytodeveloptheconditionthanwomenwithouta family history.54–56Themodeofinheritanceseemstobecomplex,includingnumerousvariants,whichindividuallyhavesmalleffects,butcollectively contribute to an individual's susceptibility to the disor-der.Genome-wideassociationstudies(GWAS)usingsib-pairanalysishaveidentifiedplausible,yetconflicting,positionalcandidatemater-nal susceptibility genes forPE.GWASofPE affected families havedemonstratedsignificantlinkagetochromosomes2p,2q,4p,7p,9p,10q,11q,and22q.57 However, no other study has reproduced these significantorsuggestiveloci.
4.3.7 | Obesity
Thereissubstantialevidencetoshowthatobesity(BMI≥30kg/m2) con-fersa2to4-foldhigherriskforPE.58–64Theexactmechanismslinkingoverweight/obesityandPEremainunclear.Obesityisknownasastateofchronic,low-gradeinflammation,alsocalled“meta-inflammation”.65,66 Low-gradeinflammationcaninduceendothelialdysfunctionandplacen-tal ischemia by immune mediated mechanisms, which in turn lead to pro-ductionofinflammatorymediatorsresultinginanexaggeratedmaternalinflammatoryresponseanddevelopmentofPE.67
4.3.8 | Race and ethnicity
There is extensive evidence in the literature demonstrating theassociation between race and ethnicity and PE. Large populationstudies suggest that the risk of PE in Afro-Caribbean women isincreased by 20%–50%.68–72TheriskofPEisalsohigherinwomenofSouthAsianoriginthan inthoseofnon-Hispanicwhitewomen(adjustedOR1.3;95%CI,1.2–1.4).73 IncreasedriskofPEreflectsthemetabolic profiles of nonpregnantwomen associatedwith anincreased susceptibility to cardiovascular disease.74–76 BothAfro-CaribbeanandSouthAsianwomenaremoresusceptibletodevel-oping chronic hypertension, diabetes mellitus, and cardiovascular disease.Inalargeprospectiveobservationalcohortstudyofmorethan 79 000 singleton pregnancies recruited in London, UK, the risk of PE was significantly higher in women of Afro-Caribbean
andSouthAsian racialorigincomparedwithwhitewomen.77 The increasedriskremainssignificantevenafteradjustingforothercon-foundingriskfactorsforPE.
4.3.9 | Comorbidities
Therearecertainmedicalconditionsthatpredisposewomentodevel-oping PE. These include hyperglycemia in pregnancy (pre-pregnancytype 1 and type 2 diabetes mellitus, overt diabetes in pregnancy, and gestational diabetes requiring insulin treatment), pre-existing chronichypertension, renal disease, and autoimmune diseases such as sys-temiclupuserythematosus(SLE)andantiphospholipidsyndrome(APS).Recently,asystematicreviewandmeta-analysisevaluatedclinicalriskfactorsat less thanorequal to16weeksofgestation in25356655pregnant women in 27 countries.78PatientswithahistoryofchronichypertensionhaveahigherriskofdevelopingPEthanthosewithoutthiscondition(relativerisk[RR]5.4;95%CI,4.0–6.5).Pre-existingdia-betesmellitus,APS,SLE,andchronickidneydiseasearealsoassociatedwithanincreasedriskofdevelopingPE(RR3.7;95%CI,3.1–4.3;RR2.8;95%CI,1.8–4.3;RR2.5;95%CI,1.0–6.3;andRR1.8;95%CI,1.5–2.1,respectively).78
Interestingly,pre-existingdiabetesmellitusandPEsharemanyriskfactors including advanced maternal age, nulliparity, pre-pregnancyobesity, nonwhite racial propensity, and multiple pregnancy.79,80 Several common pathological pathways are present in both condi-tions.Theseincludeendothelialdysfunction(e.g.lowerflow-mediateddilatation),81,82 imbalance of angiogenic factors,81,83 increasedoxida-tivestress(e.g.lowtotalantioxidantstatus,highfreeradicals),84 and dyslipidemia (e.g. increased triglycerides).85,86 PE is a risk factor forfuture type 2 diabetes.87–90Thisrelationshipisstillevidentevenwhenwomenwho have PEwith gestational diabetes are excluded. Bothconditionsareassociatedwithinsulinresistance91–97 and women with PEhaveanincreasedriskofmetabolicsyndromeafterdelivery.98–100
4.4 | Maternal and perinatal morbidity and mortality associated with pre- eclampsia
4.4.1 | Maternal morbidity and mortality
The most common cause of death in women with PE is intracranial hemorrhage.101Otherseriouscomplicationsincludeplacentalabrup-tion,HELLPsyndrome,acutepulmonaryedema,respiratorydistresssyndrome, and acute renal failure.102
Chesley et al.103werethefirsttoproposetheconceptthatpreg-nancyisastresstest,basedontheobservationthatpregnantwomenwho have never developed PE have a lower risk of cardiovasculardisease than the general female population; whereas women witheclampsiahaveasimilarriskofcardiovasculardiseasein later lifeas
FIGOacknowledgesthemanymaternalriskfactorsthatareasso-ciated with the development of pre-eclampsia, which must betakenintoconsiderationforscreeningpractices.

| 11Poon ET AL.
appropriately matched women with unknown pregnancy history.Therefore, while PE may not directly cause cardiovascular disease in later life, pregnancy itself acts as a challenge test to reveal under-lying metabolic risk factors for atherosclerosis and cardiovasculardisease.103 Evidence in support of this hypothesis is that PE and car-diovasculardiseasesharemanyrisksfactors,includingobesity,insulinresistance, diabetes mellitus, underlying hypertension, and dyslipid-emia.103–106A recentmeta-analysis demonstrated thatwomenwithpreviousPEhaveaRRof3.13(95%CI,2.51–3.89)forfuturedevelop-mentofchronichypertension,anORof2.28(95%CI,1.87–2.78)forfuturecardiovasculardisease,andanORof1.8(95%CI,1.43–2.21)for cardiovascular accident.107 It has been observed that the earlier the onsetofPE,themoreseveretheconditionandthehighertheriskofdevelopingsubsequentcardiovasculardisease.108
Compared with normotensive women, women with PE are also more likely to havemicroalbuminuria (amarker of renal damage) at3–5years after delivery.109 PEmay adversely impact future kidneyfunction sinceglomerular endotheliosis—a typical renal lesion inPEthatwas previously thought to resolve soon after delivery—can beobservedlongafterpregnancyinsomewomenwhohadPE.110Apro-spectivecohortstudyreportedanassociationbetweenPEandsubse-quentend-stagerenaldisease(RR4.7;95%CI,3.6–6.1).111PatientswithahistoryofPEshouldbeawareofthe increasedriskoffuturecardiovascular disease,107,108 metabolic syndrome,112,113 and chronic or end-stage renal disease.111 It remains to be determined whether lifestylemodificationsaswellasclosemonitoringforsignsandsymp-tomsofmetabolicsyndromesafterdeliveryamongpatientswithPEcanreducetheserisks.114
4.4.2 | Perinatal morbidity and mortality
PEisassociatedwithanumberofshort-andlong-termperinatalandneonatal complications, including death (Table3). These aremostlyrelatedtobirthweightandgestationalageatdeliveryandarethere-foremainlyattributedtoearly-onsetPE.
PE is commonly associated with placental lesions. The underly-ingvascularmanifestationsandthepresenceofoxidativestressandendothelial damage can lead to fetal growth restriction (FGR)withunderlyinghypoxiaandacidosis.Amulticenterprospectivestudyof30 639 unselected women with singleton pregnancies demonstrated
that in 614 (2%) women who developed PE there was an inverse signif-icantassociationbetweenthegestationalageatdeliveryandpreva-lenceofsmallforgestationalage(SGA)(r=−0.99,P<0.0001).Aswouldbeexpected,theprevalenceofSGAwithPEwas82%,47%,and30%inthosedeliveredatlessthan34weeks,between34and37weeks,andgreaterorequalto37weeks,respectively.ThefrequencyofSGAinpregnancieswithoutPEwas44%,21%,and8%,respectively.115
GiventhepresenceofunderlyinghypoxiainPE,andthefrequentassociationswithFGR,theincidenceoffetaldistressbeforeorduringlabor is also increased. This is partly related to the reduced fetal reserves available to withstand the stress of labor. This is supported by severalstudiesinwhichlevelsofmarkersofchronichypoxia(suchaserythropoietinandnucleatedredbloodcells)incordbloodoffetusesborn to women with PE were shown to be elevated.116,117
The most important complication that requires great attentionthrougheffectivepredictionandpreventionofPEisintrauterinefetaldeath(IUFD).TheriskofIUFDvarieswidelydependingonthepop-ulation,severityofPE,andthepresenceofcomorbidfactors.118 For womenwith PE, infant mortality is three-times higher in low- andmiddle-incomecountriesthaninhigh-incomecountries.119 The under-lyingcausesofIUFDsrelatedtoPEincludeacuteandchronichypoxia,placental insufficiency, FGR, and placental abruption.A prospectivestudy of 113 415 singleton pregnancies in the UK reported 396 (3.5 per 1000) prepartum IUFDs, of which 230 (58%) were secondary to impairedplacentation (PE,FGR,placental abruption)and166 (42%)wereduetootherorunexplainedcauses.120
Infants born to mothers suffering from PE are at risk of beingborn prematurely, as delivery is the only cure for PE. In women with early-onsetor severePE, the risk ismuchhigher.About25%ofPEcases require delivery before 37weeks of gestation. It is estimatedthat about one-third of preterm births aremedically indicated, andthatPEistheprimaryindicationforiatrogenicpretermdelivery.121,122 Infantsbornprematurelyareathigherriskofneonatalmortalityandmorbidity, including necrotizing enterocolitis, retinopathy of prema-turity, bronchopulmonary dysplasia, intraventricular hemorrhage, and neurodevelopmental impairments compared with term infants. These tendtobeinverselyrelatedtogestationalageatbirth.
In summary, several fetal complications are associatedwith PE,especially when the disease is severe or has an early onset. These include FGR, oligohydramnios, IUFD, preterm delivery, nonreassur-ingfetalheartrate(FHR)duringlabor,lowApgarscores,andneedforadmission to a neonatal intensive care unit (NICU).118 Poor neonatal outcomes can be either related solely to prematurity or as a direct consequenceofPE.Moreoftenthannot,bothareatplay,particularlyincasesofsevere,early-onsetPE.
Regarding early childhood and school-age neurodevelopmentalimpairment, several investigators have reported outcomes of largepopulation-based or geographic cohorts of infants born extremelypremature.TheEpicureStudyexaminedschoolageoutcomesofallinfantsbornatlessthan26weeksofgestationoverafive-yearperiodin England.123Cerebralpalsyaffected6%ofthesurvivors,whereas41% had IQ tests that were more than two standard deviations(SDs) below the mean compared with schoolmates. Investigators
T A B L E 3 Short-andlong-termperinatalandneonatalcomplicationsrelatedtopre-eclampsia.
Short- term complications Long- term complications
Fetalgrowthrestriction(FGR) Cerebral palsy
Oligohydramnios Low IQ
Intrauterine fetal death (IUFD) Hearing loss
Preterm birth Visualimpairment
LowApgarscore Insulin resistance
NonassuringFHRduringlabor Diabetes mellitus
Need for NICU admission Coronary artery disease
Hypertension

12 | Poon ET AL.
fromBritishColumbiareportedprovincialoutcomesforinfantsbornbetween22and25weeksover17years (n=341).124 Some 20% of survivors hadmoderate disability (defined as cerebral palsy, or IQ2–3 SDs below the mean, or sensorineural hearing loss corrected with aids or visual impairment worse than 20/70), whereas 10% of survivors had severe disability (defined as nonambulatory cerebralpalsy, IQ more than three SDs below the mean, hearing loss not cor-rected, or legal blindness).
Regarding impact in adult life, the publication byOsmond andBarker125 suggested that the in-uteroenvironmentcould influenceadult health and disease state. Their hypothesis states that sub-optimal in-uteronutrient supply, as seen inplacental insufficiency,through metabolic and hormonal adaptations and altered organmorphology, leads to increased risksof insulin resistance,diabetes
mellitus, coronary artery disease, and hypertension. Thus, both the short-termandlong-termconsequencesofPE,intermsofimpactonindividualhealth, thefinancial costs inproviding theneededacuteintensivecare,andthelong-termconsequencestohealthandhumancapital,justifyeffortstofindeffectiveearlypredictionandpreventivestrategies.
FIGOrecommendsandsupportsthecallforgreaterattentionandfocus on the links between maternal health and NCDs in theSustainable Developmental Goals agenda, including efforts toensure early screening for all pregnant women for pre-existingNCDsortheirriskfactors.

| 13Poon ET AL.
5 | FIRST TRIMESTER PREDICTION OF PRE- ECLAMPSIA
5.1 | Problems with existing methods of screening
ThecurrentapproachtoscreeningforPEistoidentifyriskfactorsfrommaternal demographic characteristics and medical history (maternalrisk factors).2–4,15,16,126,127 There are two key recommendations thathaveevolvedovertime.AccordingtotheNationalInstituteforHealthandClinicalExcellence(NICE)intheUK,womenshouldbeconsideredtobeathighriskofdevelopingPEiftheyhaveanyonehigh-riskfac-tor (hypertensive disease in previous pregnancy, chronic hypertension, chronic renal disease, diabetes mellitus, or autoimmune disease) or anytwomoderate-riskfactors(nulliparity,age≥40years,BMI≥35kg/m2, family history of PE, or interpregnancy interval >10 years).16 In the USA, the American College of Obstetricians and Gynecologists(ACOG)issuedtheHypertensioninPregnancyTaskForceReportrec-ommendingdailylow-doseaspirinbeginninginthelatefirsttrimesterforwomenwithahistoryofearly-onsetPEandpretermdeliveryatlessthan34weeksofgestation,orforwomenwithmorethanonepriorpregnancy complicated by PE.128 The US Preventive Services TaskForcepublishedasimilarguideline,althoughthelistofindicationsforlow-doseaspirinusewasmoreexpansive.129AnupdatedversionoftheUSPreventiveServicesTaskForceguidelinehasnowbeenendorsedbyACOG,theSocietyforMaternal-FetalMedicine,andtheAmericanDiabetes Association.130 Low-dose aspirin prophylaxis at 81mg/dfrom12and28weeksofgestation(optimallyat<16weeksofgesta-tion),continueddailyuntildelivery,shouldbeconsideredforwomenwithoneormorehigh-riskfactors(historyofPE,renaldisease,auto-immune disease, type 1 or type 2 diabetes, and chronic hypertension) ormore than one of several moderate-risk factors (first pregnancy,age of ≥35years, BMI >30kg/m2, family history of PE, sociodemo-graphiccharacteristics,andpersonalhistoryfactors).128 The approach recommendedbyNICEandACOGessentiallytreatseachriskfactorasaseparatescreeningtestwithadditivedetectionrateandscreen-positiverate.Althoughrecognitionofmaternal risk factorsmightbeuseful inidentifyingat-riskwomeninclinicalpractice, it isnotasuf-ficienttoolfortheeffectivepredictionofPE.131 In screening with use ofNICEguidelines,thedetectionrateis39%forpretermPEand34%fortermPEat10.3%false-positiverate.TherespectivedetectionratesinscreeningwithuseoftheUSPreventiveServicesTaskForcerecom-mendationswere90%and89%,at64.3%false-positiverate.132
5.2 | Screening with biomarkers
AnalternativeapproachtoscreeningforPE,whichallowsestimationofindividualpatient-specificrisksofPErequiringdeliverybeforeaspeci-fiedgestation,istouseBayestheoremtocombinetheaprioririskfrommaternalcharacteristicsandmedicalhistorywiththeresultsofvariouscombinationsofbiophysicalandbiochemicalmeasurements.Extensiveresearchinthelastdecadehasledtotheidentificationoffourpotentiallyusefulbiomarkersat11–13weeksofgestation:meanarterialpressure(MAP),uterinearterypulsatilityindex(UTPI),serumpregnancy-associated
plasmaproteinA(PAPP-A),andserumplacentalgrowthfactor(PLGF).The algorithm was originally developed from a study of 58 884 single-tonpregnanciesat11–13weeksofgestation,including1426(2.4%)thatsubsequentlydevelopedPE.TheestimateddetectionratesofpretermPEandallcasesofPE,atfixedfalse-positiverateof10%,were77%and54%.133Subsequently,datafromprospectivescreeningin35948single-tonpregnancies,including1058pregnancies(2.9%)thatexperiencedPE,wereusedtoupdatetheoriginalalgorithm.Thedetectionratesofpre-termPEandtermPEwere75%and47%,respectively,atfalse-positiverate of 10%.134Thepredictiveperformanceofthisalgorithmwasexam-inedinaprospectivemulticenterstudyof8775pregnancies,including239(2.7%)casesthatdevelopedPE.ThedetectionratesofpretermPEandtermPEwere75%and43%,respectively,atfalse-positiverateof10%.135InthescreenedpopulationintheASPREtrial,involving26941singletonpregnanciesfrom13maternityhospitalsinsixcountries(UK,Spain,Italy,Belgium,Greece,Israel),thedetectionratesofpretermPEandtermPE,afteradjustmentfortheeffectofaspirin,were77%and43%,respectively,atfalse-positiverateof9.2%.136
In the latest National Institute for Health Research (UK) com-missionedprospectivevalidationstudyoftheBayes-basedmodel in16 747 pregnancies, including 473 (2.8%) women who developed PE, thescreen-positiveratebytheNICEmethodwas10.3%,thedetectionrateforallPEwas30%,andforpretermPEitwas41%.Thedetectionrateofthemini-combinedtest(maternalfactors,MAP,andPAPP-A)for all PE was 43%, which was superior to that of the NICE method by 12.1% (95% CI, 7.9–16.2). In screening for preterm PE by a combina-tionofmaternalfactors,MAP,UTPI,andPLGF,thedetectionratewas82%, which was higher than that of the NICE method by 41.6% (95% CI, 33.2–49.9).137TheadditionofPAPP-Atothiscombinedmodeldidnot improve the overall screening performance.
Datafromthreereportedprospectivenoninterventionscreeningstudies at11–13weeksof gestation in a combined total of61174singleton pregnancies, including 1770 (2.9%) that developed PE, have demonstrated that screeningbyacombinationofmaternal risk fac-tors,MAP,PLGF, andUTPI andusing a risk cut-offof 1 in 100 forpretermPE inwhitewomen, the screen-positive ratewas10%anddetectionratesforearly-onset,preterm,andtermPEwere88%,69%,and40%,respectively.Withthesamemethodofscreeningandriskcut-offinwomenofAfro-Caribbeanracialorigin,thescreen-positiveratewas34%anddetectionratesforearly-onset,preterm,andtermPEwere100%,92%,and75%,respectively.138
AsecondaryanalysisofdatafromtheASPREtrialofatotalof34573womenwithsingletonpregnancieswhounderwentprospectivescreen-ing for preterm PE, including 239 (0.7%) cases of preterm PE, has shown thatinACOGorNICEscreen-positivewomenwhoarescreennegativebytheBayes-basedmethod,theriskofpretermPEisreducedtowithinorbelowbackgroundlevels.ThestudydemonstratedthatatleastoneoftheACOGcriteriawasfulfilledin22287(64.5%)pregnanciesandtheincidence of preterm PE was 0.97% (95% CI, 0.85–1.11). In the subgroup thatwasBayes-methodscreenpositive,theincidencewas4.80%(95%CI,4.14–5.55); inthosethatwerescreennegative itwas0.25%(95%CI,0.18–0.33%),andtherelativeincidenceinBayes-methodnegativetoBayes-methodpositivewas0.051(95%CI,0.037–0.071).In1392(4.0%)
14 | Poon ET AL.
pregnanciesatleastoneoftheNICEhigh-riskcriteriawasfulfilledandinthis group the incidence of preterm PE was 5.17% (95% CI, 4.13–6.46). InthesubgroupsofscreenpositiveandscreennegativebytheBayesmethod the incidence of preterm PE was 8.71% (95% CI 6.93–10.89%) and0.65%(95%CI,0.25–1.67),respectively,andtherelativeincidencewas 0.075 (95% CI, 0.028–0.205). In 2360 (6.8%) pregnancies with at leasttwooftheNICEmoderate-riskcriteria,theincidenceofpretermPEwas1.74%(95%CI,1.28–2.35).InthesubgroupsofscreenpositiveandscreennegativebytheBayesmethodtheincidencewas4.91%(95%CI,3.54–6.79)and0.42%(95%CI,0.20–0.86),respectively,andtherelativeincidence was 0.085 (95% CI, 0.038–0.192).139 These results provide furtherevidencetosupportrisk-basedscreeningusingbiomarkers.
Thereisnowasubstantialbodyofevidencetosupportrisk-basedscreeningforpretermPEusingvariousbiomarkers.ThisapproachtoscreeninghasalsobeenvalidatedprospectivelyincountriesotherthanEurope.140–143Achecklist-basedmethodofscreeningusinginforma-tionfrommaternalhistorydoesnotperformaswellandcannolongerbeconsideredsufficientforpredictingpretermPEeffectively.
5.3 | Recommendations
FIGOrecommendsthefollowingfirst-trimesterscreeningproceduresfor singleton pregnancies.
5.3.1 | Maternal characteristics and medical history
Best practice recommendation: Maternal characteristics, medicalhistory and obstetric history (as shown inBox2)must be recordedaccurately.
Quality of evidenceStrength of recommendation
High ⊕⊕⊕⊕ Strong
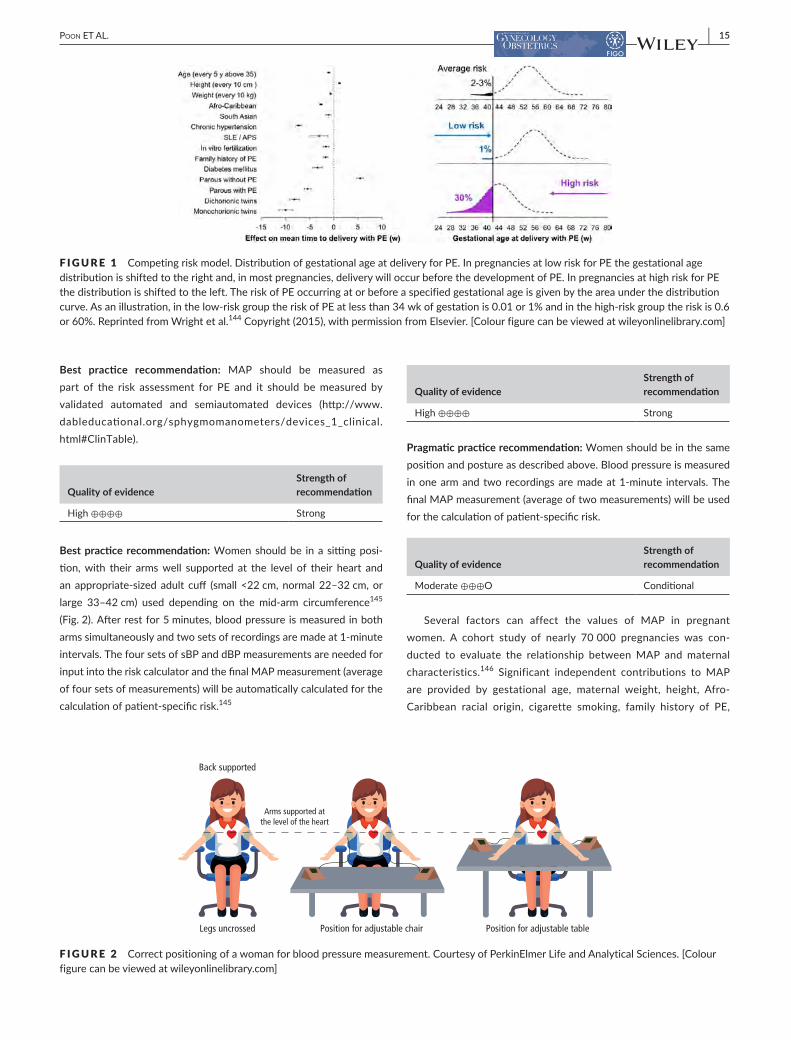
Evidencetosupporttheinclusionoftheabove-listedmaternalriskfactorsinamultivariateregressionalgorithmoriginatesfromascreeningstudyof 120492 singletonpregnancies at 11–13weeks of gestation,including 2704 (2.2%) pregnancies that experienced PE.A competingriskmodelhasbeenutilizedtoproducerisksforPE,basedonacontin-uousmodel for thegestationalageatdeliverywithPE, treatingbirthsfromcausesotherthanPEascensoredobservations.144 This approach assumesthat,ifthepregnancyweretocontinueindefinitely,allwomenwouldexperiencePEandthatwhethertheydosoornotbeforeaspeci-fiedgestationalagedependsoncompetitionbetweendeliverybeforeorafterdevelopmentofPE.Theeffectofvariablesfrommaternalcharacter-isticsandhistoryistomodifythedistributionofgestationalageatdeliv-erywithPEsothatinpregnanciesatlowriskforPEthegestationalagedistributionisshiftedtotherightwiththeimplicationthat,inmostpreg-nancies, delivery will actually occur before development of PE (Fig. 1). In high-riskpregnanciesthedistributionisshiftedtotheleftandthesmallerthemeangestationalagethenthehighertheriskforPE(Fig.1).
Inthisriskfactor-basedmodel,increasedriskforPE,withaconse-quent shift in the Gaussian distribution of the gestational age at
delivery with PE to the left, is related to advancing maternal age,increasingweight,Afro-CaribbeanandSouthAsianorigin,medicalhis-toryofchronichypertension,diabetesmellitusandSLEorAPS,familyhistoryandpersonalhistoryofPE,andconceptionbyIVF.TheriskforPE decreases with increasing maternal height and in parous women withnopreviousPE;inthelatter,theprotectiveeffect,whichisrelatedinverselytotheinterpregnancyinterval,persistsbeyond15years.Atascreen-positiverateof11%,asdefinedbyNICE,thenewmodelpre-dicted40%and48%ofcasesofallPEandpretermPE,respectively.144 Theriskfactor-basedmodelhasbeenfurtherimprovedwiththeinclu-sionofgestationalageatdeliveryinthepreviouspregnancy.136
5.3.2 | Measurement of blood pressure
FIGOsupportstheuseofrisk-basedscreeningusingbiomarkersfor first-trimester prediction of pre-eclampsia over screeningmethodsthatusematernaldemographiccharacteristicsandmedi-calhistory(maternalriskfactors)only.
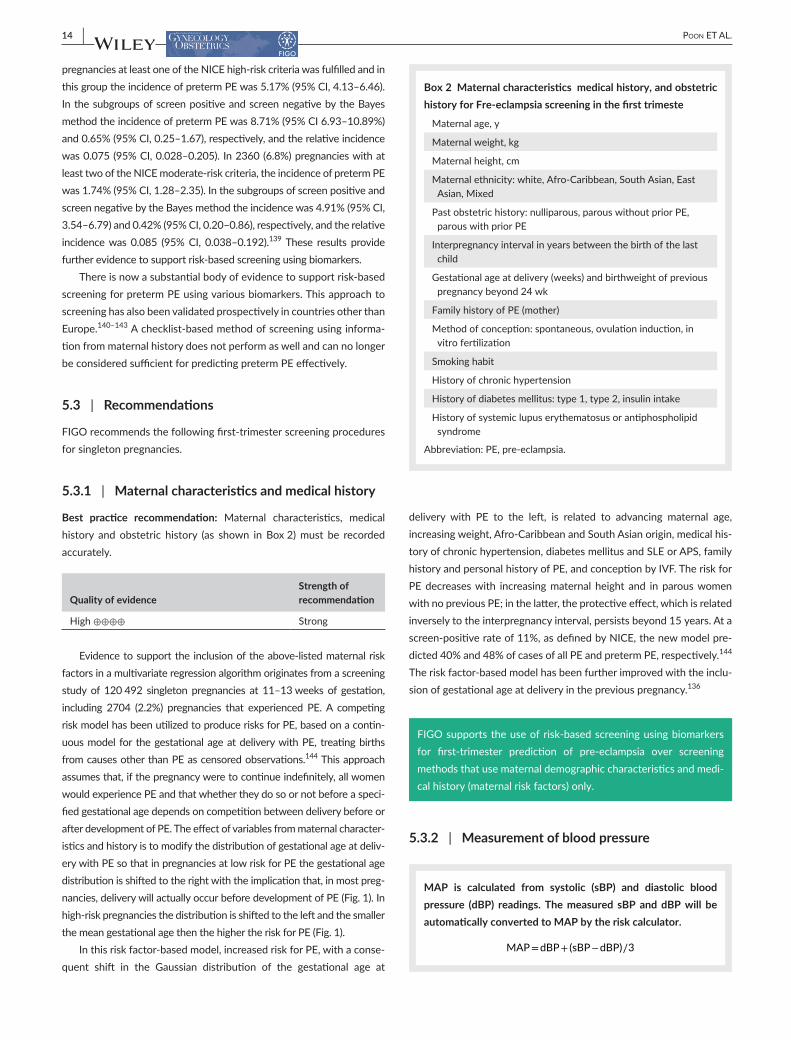
MAP is calculated from systolic (sBP) and diastolic blood pressure (dBP) readings. The measured sBP and dBP will be automatically converted to MAP by the risk calculator.
MAP=dBP+ (sBP−dBP)∕3
Box 2 Maternal characteristics, medical history, and obstetric history for pre- eclampsia screening in the first trimester.
Maternal age, y
Maternalweight,kg
Maternal height, cm
Maternalethnicity:white,Afro-Caribbean,SouthAsian,EastAsian,Mixed
Past obstetric history: nulliparous, parous without prior PE, parous with prior PE
Interpregnancy interval in years between the birth of the last child
Gestationalageatdelivery(weeks)andbirthweightofpreviouspregnancybeyond24wk
Family history of PE (mother)
Methodofconception:spontaneous,ovulationinduction,invitrofertilization
Smokinghabit
History of chronic hypertension
Historyofdiabetesmellitus:type1,type2,insulinintake
Historyofsystemiclupuserythematosusorantiphospholipidsyndrome
Abbreviation:PE,pre-eclampsia.
| 15Poon ET AL.
Best practice recommendation: MAP should be measured aspart of the risk assessment for PE and it should bemeasured byvalidated automated and semiautomated devices (http://www.dableducational.org/sphygmomanometers/devices_1_clinical.html#ClinTable).
Quality of evidenceStrength of recommendation
High ⊕⊕⊕⊕ Strong
Best practice recommendation:Womenshouldbe inasittingposi-tion,with their armswell supported at the level of their heart andanappropriate-sizedadult cuff (small<22cm,normal22–32cm,orlarge 33–42cm) used depending on the mid-arm circumference145 (Fig.2).Afterrestfor5minutes,bloodpressureismeasuredinbotharmssimultaneouslyandtwosetsofrecordingsaremadeat1-minuteintervals.ThefoursetsofsBPanddBPmeasurementsareneededforinputintotheriskcalculatorandthefinalMAPmeasurement(averageoffoursetsofmeasurements)willbeautomaticallycalculatedforthecalculationofpatient-specificrisk.145
Quality of evidenceStrength of recommendation
High ⊕⊕⊕⊕ Strong
Pragmatic practice recommendation: Women should be in the same positionandpostureasdescribedabove.Bloodpressureismeasuredinonearmandtworecordingsaremadeat1-minute intervals.ThefinalMAPmeasurement(averageoftwomeasurements)willbeusedforthecalculationofpatient-specificrisk.
Quality of evidenceStrength of recommendation
Moderate ⊕⊕⊕O Conditional
Several factors can affect the values of MAP in pregnantwomen. A cohort study of nearly 70000 pregnancies was con-ducted to evaluate the relationship betweenMAP andmaternalcharacteristics.146 Significant independent contributions toMAPare provided by gestational age, maternal weight, height, Afro-Caribbean racial origin, cigarette smoking, family history of PE,
F I G U R E 1 Competingriskmodel.DistributionofgestationalageatdeliveryforPE.InpregnanciesatlowriskforPEthegestationalagedistributionisshiftedtotherightand,inmostpregnancies,deliverywilloccurbeforethedevelopmentofPE.InpregnanciesathighriskforPEthedistributionisshiftedtotheleft.TheriskofPEoccurringatorbeforeaspecifiedgestationalageisgivenbytheareaunderthedistributioncurve.Asanillustration,inthelow-riskgrouptheriskofPEatlessthan34wkofgestationis0.01or1%andinthehigh-riskgrouptheriskis0.6or60%.ReprintedfromWrightetal.144Copyright(2015),withpermissionfromElsevier.[Colourfigurecanbeviewedatwileyonlinelibrary.com]
F I G U R E 2 Correctpositioningofawomanforbloodpressuremeasurement.CourtesyofPerkinElmerLifeandAnalyticalSciences.[Colourfigurecanbeviewedatwileyonlinelibrary.com]

16 | Poon ET AL.
history of PE in the previous pregnancy, interpregnancy interval, chronic hypertension, and diabetes mellitus. Consequently, themeasurementofMAPisconvertedtoamultipleofmedian(MoM),adjusting for these associated maternal characteristics and gesta-tional age146(AppendixS1).
Poon et al.147firstreportedthevalueofMAPmeasuredbyvalidatedautomatedbloodpressuredevicesaccordingtoastandardizedproto-colat11–13weeksofgestationforthepredictionofPE.148 Maternal blood pressure was determined in 5590 singleton pregnant women by automated devices and appropriately trained doctors. For MAPaloneand incombinationwithmaternalhistory, thedetectionratesforPE,at10%false-positive rate,were38%and63%, respectively.A follow-up study ofmore than 9000 pregnancies at 11–13weeksof gestation compared the screening performance of sBP, dBP, andMAP.149AlthoughsBP,dBP,andMAPwereallfoundtoberaisedinwomenwhosubsequentlydevelopedPE,MAPperformedbestasamarker,withadetectionrateforearly-onsetPE,increasingfrom47%(basedonmaternalfactorsalone)to76%(basedonacombinationofmaternalfactorsandMAP)atafalse-positiverateof10%.149
Methodologically, based on the protocol of theNationalHeartFoundation of Australia (NHFA),148 blood pressure is measured in botharmsandaminimumoftworecordingsaremadeatone-minuteintervalsuntilvariationsbetweenconsecutivereadingsfalltowithin10mmHg in sBPand6mmHg indBP inbotharms.148 When this point of stability is achieved, the average of the last two stable mea-surements of the left and right arms is calculated and the higherof these two measurements from the two arms is used. However, in order to achieve the necessary point of blood pressure stability according to theNHFAprotocol, it has been shown that it is nec-essary to perform two measurements in both arms in about 50% of cases, three measurements in 25% of cases, and four measurements or more in 25%.145 In addition,whether blood pressure should betaken on the left or right arm remains controversial.The evidencesupportingsimultaneousmeasurementofbotharmsisderivedfromthe study published by Poon et al.150 In this study, the prevalence of bloodpressure interarmdifference (IAD),definedas IADofgreaterthan 10mmHg of sBP and dBPwas determined in 5435womenduringthefirsttrimesterofpregnancy.TheIADofsBPanddBPwasfoundin8.3%and2.3%ofnormalpregnantwomen,respectively.150 Asimplifiedprotocolforbloodpressuremeasurement(asdescribedabove) has been developed through a study of 25 505 singleton preg-nancies where blood pressure measurements were made using a val-idatedautomaticdeviceat11–13weeksofgestation.145 The results demonstrated that performance of screening for PE by taking theaverage of two measurements from both arms is comparable with theNHFAprotocol.
5.3.3 | Measurement of biochemical markers
Best practice recommendation:Infirst-trimesterscreening,thebestbiochemical marker is PLGF. PAPP-A is useful if measurements ofPLGF and UTPI are not available.
Quality of evidenceStrength of recommendation
High ⊕⊕⊕⊕ Strong
MaternalserumconcentrationsofPLGFandPAPP-Aaremeasuredby one of three commercially available automated devices. Quality control shouldbeappliedtoachieveconsistencyofmeasurementofbiomarkers.
5.3.3.1 | Placental growth factorPLGFisaglycosylateddimericglycoproteinsecretedbytrophoblasticcells and is part of the angiogenic vascular endothelial growth factor (VEGF)family.ItbindstoVEGFreceptor1(VEGFR-1),whichhasbeenshowntoincreaseduringpregnancy.PLGFissynthesizedinvillousandextravillous cytotrophoblasts, and has both vasculogenic and angio-genetic functions. Its angiogenetic abilities havebeen speculated toplay a role in normal pregnancy, and changes in the levels of PLGF or its inhibitory receptors have been implicated in the development of PE.151–153SeveralstudieshaveshownthatwomenwhosubsequentlydevelopPEhavesignificantlylowermaternalPLGFconcentrationsinthefirsttrimesterthanthosewithnormalpregnancies.154–157 This bio-markeralonehasadetectionrateof55%and33%,respectively,at10%false-positiverate,fortheidentificationofbothearly-andlate-onsetPE.158Asystematicreviewandmeta-analysisdemonstratedthatPLGFis superior to theotherbiomarkers forpredictingPE.159Specifically,maternalPLGFconcentrationsaloneachieveadetectionrateof56%at9%false-positiverateforthepredictionofearly-onsetPE.159
Several factorsaffect thevaluesofPLGF inpregnantwomen.Acohort study of more than 42 000 pregnancies, including 33 147 mea-suredbytheDELFIAXpresssystem(PerkinElmerLifeandAnalyticalSciences,Waltham,MA, USA), 7065measured by the Cobas e411system (Roche Diagnostics, Risch-Rotkreuz, Switzerland), and 2143measured by the B·R·A·H·M·S KRYPTOR compact PLUS (ThermoFisherScientific,Waltham,MA,USA),wasconductedtoevaluatetherelationship of PLGFwith analyzers andmaternal characteristics.138 Significant independent contributions to PLGF values are providedbythethreeanalyzersas listedabove,aswellasbygestationalage,maternalage,weight,racialorigin,cigarettesmoking,ahistoryofPEinthepreviouspregnancy,diabetesmellitus,andIVF.
5.3.3.2 | Pregnancy- associated plasma protein APAPP-Aisametalloproteinaseinsulin-likegrowthfactor(IGF)bindingprotein secretedby the syncytiotrophoblast thatplays an importantrole in placental growth and development. It enhances the mitogenic functionoftheIGFs.PEhasbeenshowntobeassociatedwithalowlevelofcirculatingPAPP-A,which ispresumablyduetothereducedavailabilityofunboundIGFstofulfiltheirfunctionalroleonacellularlevel.PAPP-Aisawell-establishedbiochemicalmarkerinthescreeningof trisomies21,18,and13. Ineuploidpregnancies,aPAPP-AMoMvalueatlessthanthe5thpercentile(0.4MoM)ispresentin8%–23%ofwomenwithPE.Therefore,asasinglemarkeritisnotanaccuratepredictive test for PE.160–162 A recent systematic review andmeta-analysis, including eight studies involving 132 076 pregnant women in

| 17Poon ET AL.
thefirsttrimester,demonstratedthatthematernalPAPP-Aconcentra-tionoflessthanthe5thpercentileisassociatedwiththeriskofdevel-opingPEwithanORof1.94(95%CI,1.63–2.30). Ithasadetectionrateof16%(9%–28%)at8%false-positiveratetopredictPE.163
In a cohort study of more than 94 000 pregnancies, the rela-tionship between PAPP-A,measured by theDELFIA Xpress system(PerkinElmerLifeandAnalyticalSciences),andmaternalcharacteristicswas evaluated.164 Significant independent contributions to PAPP-Aareprovidedbygestationalage,maternalweight,height,racialorigin,cigarettesmoking,diabetesmellitus,methodofconception,previouspregnancywithorwithoutPE,andbirthweightZ-scoreoftheneonatein thepreviouspregnancy.ThemeasurementsofPLGFandPAPP-AshouldbeconvertedtoMoMs,adjustingfortheseassociatedmaternalcharacteristics,analyzers,andgestationalage138(AppendixS1).
5.3.4 | Measurement of uterine artery pulsatility index
Best practice recommendation: Where feasible UTPI should be measured.Atransabdominalultrasoundscanshouldbedoneat11+0 to 13+6weeks of gestation (corresponding to fetal crown–rumplength (CRL) of 42–84mm). Gestational age must be determinedfromthemeasurementofthefetalCRL.Thesamescanisutilizedforthemeasurementoffetaltranslucencythicknessanddiagnosisofanymajorfetaldefects.ForthemeasurementofUTPI,asagittalsectionof the uterus is obtained and the cervical canal and internal cervical osareidentified.Subsequently,keepingthetransducerinthemidlineitisgentlytiltedtothesideandcolorflowmappingisusedtoidentifyeachuterinearteryalongthesideofthecervixanduterusattheleveloftheinternalos(Fig.3).Pulsed-waveDopplerisusedwiththesam-plinggatesetat2mmtocoverthewholevesselandcareistakentoensurethattheangleofinsonationislessthan30°.Whenthreesimi-larconsecutivewaveformsareobtained(Fig.3),theUTPIismeasuredandthemeanUTPIoftheleftandrightarteriesiscalculated.165 The measurement of UTPI must be carried out by sonographers who have received the appropriate certificate of competence from the FetalMedicineFoundation(FMF)(www.fetalmedicine.org).
Quality of evidenceStrength of recommendation
High ⊕⊕⊕⊕ Strong
TheDopplerultrasoundassessingtheresistancetobloodflowinthe uterine arteries correlates with both histological studies and clin-ical severityofPE.Thisbiophysicalmarkerprovidesausefulnonin-vasivemethod for the assessmentof theuteroplacental circulation.Studies have shown that a significant decrease of resistance in thespiral arteries occurswith advancing gestation,which is in keepingwith physiological changes throughout pregnancy.166,167 Persistent high impedance to flow in the uterine arteries is evidence of poorplacentation thatmanifests itself in the formof abnormal uteropla-centalflowvelocitywaveforms.HistologicalexaminationofplacentalbedbiopsiesofpregnanciesaffectedbyPEhasshownthatabsenceofphysiological changes of the spiral arteries is found more commonly in cases with high UTPI.168
Methodologically, the measurement of UTPI at the level of the internalosduringthefirsttrimesterismorereproduciblethanthoseobtained at the level of external iliac vessels crossover.169 In addi-tion,UTPIcanbeachievedattheleveloftheinternalcervicalosinagreaterproportionofwomenthanatthelevelofexternaliliacvesselcrossover.169
SeveralfactorscanaffectthevaluesofUTPIinpregnantwomen.Acohortstudyofmorethan83000pregnancieswasconductedtoevaluatetherelationshipbetweenUTPIandmaternalcharacteris-tics.138SignificantindependentcontributionstoUTPIareprovidedbygestationalage,maternalage,weight,racialorigin,ahistoryofPE in the previous pregnancy, and type 1 diabetes. Hence, before comparing the values between affected and unaffected groups,the UTPI value needs to be adjusted for these associated mater-nal characteristicsandgestational agebyconverting it toaMoM(AppendixS1).
Alargemeta-analysisoffirst-trimesterUTPImeasurementfortheprediction of PE included eight studies for the prediction of early-onsetPE(n=41692women)andelevenstudiesforthepredictionofPEofanygestation(n=39179women).170Thefirst-trimesterabnor-malUTPI isdefinedasgreaterthanthe90thpercentile,achievingadetectionrateof48%,at8%false-positiverate,fortheidentificationof early-onset PE. The detection rate for predicting late-onset PEreducesto26%ata7%false-positiverate.
[Correctionaddedon18June2019,afterfirstonlinepublication:Secondlastsentence‘Thefirst-trimesterabnormalUTPIisdefinedasgreaterthanthe90thpercentile’hasbeencorrectedforaccuracy inthisversion.]
F I G U R E 3 Identification of the uterine artery at the level of the internal os (left) and typical waveforms of the uterine artery Doppler in the firsttrimesterofpregnancy.CourtesyoftheFetalMedicineFoundation.[Colourfigurecanbeviewedatwileyonlinelibrary.com]

18 | Poon ET AL.
The International Society of Ultrasound in Obstetrics andGynecology(ISUOG)hasrecentlypublisheditspracticeguidelineontheroleofultrasoundinscreeningforandfollow-upofPE.165
FIGOacknowledgesandendorsestheguidancefromISUOGwithregard to UTPI measurement methodology.
5.3.5 | Combined risk assessment
Best practice recommendation: Published algorithms should be used forconvertingthemeasuredvaluesofMAP,PLGF,andUTPI,withorwithoutPAPP-A, intoMoMsasdetailed above.Patient-specific riskforpretermPEiscalculatedusingtheBayes-basedmethod.Theriskcalculatorisavailablefreeofchargeonthewebpagehttps://fetalmedi-cine.org/research/assess/preeclampsia and on the FMF mobile app. It isalsoavailableonmedicalrecordssoftware.Awomanisconsideredhighriskwhentheriskisgreaterthanorequalto1in100basedonthefirst-trimestercombinedtestwithmaternal riskfactors,MAP,PLGF,and UTPI.1,136,171
Quality of evidenceStrength of recommendation
High ⊕⊕⊕⊕ Strong
Best practice recommendation:Basedonexistingevidence,thefirst-trimestercombinedtestismostpredictiveofpretermPEbutnottermPE. Thebestmodel is theone that combinesmaternal risk factors
withMAP,PLGF,andUTPI.Theperformanceofscreeningforpre-term PE of various combinations of the first-trimester test, basedondatafromthreepreviouslyreportedprospectivenoninterventionscreening studies, including a combined total of 61 174 singleton pregnancies, including 1770 (2.9%) that developed PE, is illustrated in Table 4.
Quality of evidenceStrength of recommendation
High ⊕⊕⊕⊕ Strong
Pragmatic practice recommendation: Where it is not possible to measurethebiochemicalmarkersand/orUTPI,thebaselinescreeningtestshouldbeacombinationofmaternalriskfactorswithMAP,andnotmaternalriskfactorsalone.PAPP-AisusefulifmeasurementsofPLGFandUTPI arenot availableThesevariations to the combinedtestwouldleadtoareductionintheperformancescreening.
Quality of evidenceStrength of recommendation
Moderate ⊕⊕⊕O Conditional
Asdemonstratedabove,biomarkersarebestusedinthecombina-tionstrategyforthepredictionofPE.Arecentsystematicreviewhasbeen conducted to evaluate theperformanceof simple riskmodels
T A B L E 4 Detectionrates,atscreen-positiverateof10%,ofpretermPEandtermPEbymaternalfactors,biomarkers,andtheircombination.a
Method of screeningRisk cut- off for PE <37 wk
Preterm PE Term PE
AUC DR % (95% CI) AUC DR % (95% CI)
Maternalriskfactors 1 in 62 0.788 44.8 (40.5–49.2) 0.735 33.5 (31.0–36.2)
Maternalriskfactorsplus
MAP(baseline) 1 in 61 0.841 50.5 (46.1–54.9) 0.776 38.2 (35.6–40.9)
UTPI 1 in 60 0.853 58.4 (54.0–62.7) 0.733 35.2 (32.6–37.8)
PAPP-A 1 in 61 0.810 48.5 (44.1–52.9) 0.734 35.2 (32.7–37.9)
PLGF 1 in 62 0.868 60.6 (56.3–64.9) 0.745 34.5 (32.0–37.2)
MAP,UTPI 1 in 61 0.891 68.4 (64.1–72.3) 0.772 41.4 (38.8–44.2)
MAP,PAPP-A 1 in 60 0.855 55.8 (51.4–60.1) 0.774 39.1 (36.4–41.8)
MAP,PLGF 1 in 65 0.895 66.1 (61.8–70.2) 0.777 39.3 (36.7–42.0)
UTPI,PAPP-A 1 in 60 0.861 59.2 (54.8–63.5) 0.735 36.3 (33.7–39.0)
UTPI, PLGF 1 in 62 0.892 66.9 (62.7–70.9) 0.744 36.9 (34.3–39.6)
PLGF,PAPP-A 1 in 62 0.869 63.5 (59.2–67.6) 0.745 35.7 (33.1–38.4)
MAP,UTPI,PAPP-A 1 in 61 0.896 68.2 (63.9–72.1) 0.773 40.6 (37.9–43.3)
MAP,PAPP-A,PLGF 1 in 65 0.896 67.3 (63.1–71.3) 0.777 39.3 (36.7–42.0)
MAP,UTPI,PLGF 1 in 66 0.915 74.8 (70.8–78.5) 0.776 41.0 (38.3–43.7)
UTPI,PAPP-A,PLGF 1 in 63 0.892 68.2 (63.9–72.1) 0.745 36.9 (34.3–39.6)
MAP,UTPI,PAPP-A,PLGF 1 in 66 0.916 74.8 (70.8–78.5) 0.777 41.3 (38.7–44.1)
Abbreviations:PE,pre-eclampsia;AUC,areaundercurve;DR,detectionrate;MAP,meanarterialpressure;UTPI,uterinearterypulsatilityindex;PAPP-A,pregnancy-associatedplasmaproteinA;PLGF,placentalgrowthfactor.aAdaptedwithpermissiongrantedbyWiley,fromTanetal.138

| 19Poon ET AL.
(maternalcharacteristicsonly)versusspecializedmodelsthatincludespecialized tests such as the measurement of MAP, UTPI, and/ormaternalbiochemicalmarkersforthepredictionofPE.Seventymod-elsfrom29studieshavebeenidentified(17modelstopredictPE,31modelstopredictearly-onsetPE,and22modelstopredictlate-onsetPE).Amongthem,22weresimplemodelswhile48wereclassifiedasspecializedmodels.Comparingthesimpleandspecializedmodels,thelatterperformedbetterthanthesimplemodelsinpredictingearly-andlate-onsetPE,achievinganadditional18%(95%CI,0–56)indetectionrate for the predictionof PE at a fixed false-positive rate of 5%or10%.172Therefore,acombinationofvarioustestsratherthanasingletestisrecommendedforthepredictionofPE.
5.3.6 | Contingent screening
Pragmatic practice recommendation: Where resources are limited, routinescreeningforpretermPEbymaternal factorsandMAPinallpregnancies and reserving measurements of PLGF and UTPI for a sub-groupofthepopulation,selectedonthebasisoftheriskderivedfromscreeningbymaternalfactorsandMAPalonecanbeconsidered(Fig.4).
Quality of evidenceStrength of recommendation
Moderate ⊕⊕⊕O Conditional
In a prospective screening study including more than 120000singleton pregnancies, the performance of screening for preterm PE by this two-stagestrategywasexamined.Atafixedscreen-positiverateof10%,adetectionrateof71%wasachievedbythistwo-stagescreening,withscreeningbymaternalfactorsandMAP,basedontheabove-described combined algorithm, at 11+0–13+6weeks of gesta-tioninthefirststageandreservingmeasurementofPLGFandUTPIforthesecondstageandfor30%ofthepopulation.173
5.3.7 | Multiple pregnancies
Pragmatic practice recommendation: Thesamefirst-trimestercom-bined test for PE in singleton pregnancies can be adapted for screen-ingintwinpregnancies.ItleadstothedetectionofnearlyallaffectedcasesofPEbutatahighscreen-positiverate.
Quality of evidenceStrength of recommendation
Moderate ⊕⊕⊕O Conditional
InaprospectivescreeningstudyforPEin2219twinpregnanciesundergoingroutinefirst-trimestercombinedscreeningforaneuploidyand subsequently delivering two phenotypically normal live or still-bornbabiesatgreaterthanorequalto24weeksofgestation,theinci-dence of PE in dichorionic and monochorionic twin pregnancies was shown to be increased by four-fold and three-fold, respectively.174 IntwinpregnanciesthatdevelopedPE,thevaluesofMAPandUTPIwereincreasedandthevaluesofPLGFandPAPP-Aweredecreased.Thedistributionsoflog10MoMvaluesofbiomarkerswithgestationalage at delivery were similar to those that were previously reported in singleton pregnancies and it was therefore decided that the same first-trimestercombinedtestforsingletonpregnanciescouldbeappli-cabletotwinpregnancies.Inamixedpopulationofsingletonandtwinpregnancies,combinedscreeningbymaternalfactors,MAP,UTPI,andPLGFandatariskcut-offof1in75forpretermPE,thedetectionratesof preterm PE and all PE in singleton pregnancies were 77% and 57%, respectively, at a screen-positive rate of 13%; the respective ratesfortwinpregnancieswere99%and97%,atascreen-positiverateof75%.174TheadditionofPAPP-Adidnotimprovetheperformanceofscreening.
F I G U R E 4 Two-stagescreeningstrategyforpretermPEinwhichthewholepopulationundergoesfirst-stagescreeningbymaternalfactorsandMAPandaselectedproportionofthoseconsideredtobeatintermediateriskundergosecond-stagescreeningbyPLGFandUTPI.AdaptedwithpermissiongrantedbyWiley,fromWrightetal.173
Total population
First-stage screening
Screen positive
Screen positive
Second-stage screening
Screen negative
Screen negative

20 | Poon ET AL.
6 | FIRST TRIMESTER PREVENTION OF PRETERM PRE- ECLAMPSIA
The current approach to prevention of PE is to commence low-dose aspirin at 75mg or 81mg daily in high-riskwomen as locallydefined.2–4,16,128Low-doseaspirintreatmentinpregnancyisthoughttoprevent thedevelopmentofPEby inhibiting thebiosynthesisofplacentalthromboxaneA2withminimaleffectsonvascularprostacy-clin levels.175TheenzymecyclooxygenaseplaysapivotalroleintheproductionofbothprostacyclinandthromboxaneA2.Aspirin inhib-its endothelial cyclooxygenase176 and this process is irreversible in platelets,where theenzyme is inhibited for their entire lifespan. Incontrast,whentheenzyme is resynthesized inendothelialcells, theprostacyclinproductionisre-establishedrelativelyrapidly.Thisselec-tive inhibitionof cyclooxygenaseand the resultingalteration in theprostacyclintothromboxaneA2ratiointheplacentaformsthebasisof using aspirin to prevent or delay the onset of PE.
Crandon and Isherwood177 demonstrated that nulliparous women whohadtakenaspirinmorethanonceafortnightthroughoutpreg-nancyhad a lower risk of PE than thosewhohadno reportedhis-toryofaspirinconsumption.In1985,anopen-labelrandomizedtrialshowedthatamongwomenatriskforPEorFGR,basedonobstetrichistory, pregnancies in women who received 300 mg of dipyridamole and150mgofaspirinbeginningat12weeksofgestationuntildeliv-erywerenotcomplicatedbyPE,fetalloss,andsevereFGRcomparedwiththoseinthenoninterventiongroup.178Alandmarkmeta-analysis,including 31 randomized trials of PE prevention, including 32217pregnancies, showed that patientswho received antiplatelet agentsespeciallyaspirinforthepreventionofPE,hada10%reductionofPE(RR0.90;95%CI,0.84–0.97),pretermbirthbefore34weeksofgesta-tion,andseriousadversepregnancyoutcomes(PE,delivery<34weeksofgestation,SGAbabies, fetalormaternaldeath).179Bujoldetal.180 showedthatlow-doseaspirinstartedatlessthanorequalto16weeksofgestationinwomenatriskofPEhadasubstantialreductionintherateofPE(RR0.47;95%CI,0.34–0.65).However,aspirinstartedafter16weeksofgestationdidnotdecreasetherateofPE(RR0.81;95%CI, 0.87–1.10).180 Subsequent meta-analyses consistently showedthatadministrationoflow-doseaspirin(50–150mg/d)atlessthanorequalto16weeksofgestationtowomenatriskofPEhadasignificantreduction inPE, in particular pretermPE (RR0.22; 95%CI, 0.080–0.567).181 Additionally, these meta-analyses highlighted that addi-tionalbenefitsfromearlyaspirinprophylaxisincludea50%reductionintheriskofFGRanda60%reductionintheriskofperinataldeath.180 TheseresultshavestimulatedtheneedforaprospectiverandomizedtrialtoevaluatethepotentialbenefitofaspirininpreventingPE.
This evidence has been provided by the ASPRE trial (Project#601852; EudraCT number 2013-003778-29; ISRCTN13633058;www.aspre.eu).TheASPREtrialshowsthattherateofdeliverywithpretermPEcanbereducedby62%byaspirinstartedat11–14weeksofgestationinhigh-riskwomen.182TheASPREtrialwasdesignedtotest the hypothesis that aspirin at a dose of 150 mg per night from 11to14weeksuntil36weeksofgestation,comparedwithplacebo,
would result inhalving the incidenceofpretermPE. In thismulti-center,double-blind,placebo-controlledtrial,womenwithsingletonpregnanciesidentifiedasbeingathigh-riskofpretermPEbymeansof the first-trimester combined test were randomized to receiveaspirin (150mgpernight)versusplacebo from11–14weeksuntil36weeksofgestation.PretermPEoccurredin1.6%(13/798)ofpar-ticipantsintheaspiringroup,comparedwith4.3%(35/822)intheplacebogroup (OR intheaspiringroup,0.38;95%CI,0.20–0.74).However,therewasnosignificantreductionintherateoftermPEwith theuseofaspirinprophylaxis (OR in theaspiringroup,0.95;95%CI,0.57–1.57).Theproportionofprescribedtabletstakenwasusedasanoverallmeasureofadherence.Adherencewasgood,withreportedintakeofmorethan85%oftherequirednumberoftabletsin 80% of participants. Therewere no significant between-groupdifferencesinadverseevents.Therewasnostatisticallysignificantdifferenceintherateofvaginalbleeding(3.6%vs2.6%)anduppergastrointestinal(GI)symptoms(7.4%vs7.1%)betweenplaceboandaspiringroups. Inparticular, theratesofvaginalbleeding (4.8%vs2.9%)andupperGIsymptoms(6.8%vs6.4%)werenotsignificantlydifferentinwomenwhowereofnormalweightversuswomenwhowere overweight in the aspirin arm.
Further, a secondary analysis of data of 1620 participants with1571 liveborn neonates showed that the total length of stay in NICU wassubstantiallylongerintheplacebothanintheaspiringroup(1696vs531days).ThisreflectedsignificantlyshortermeanlengthsofstayinbabiesadmittedtotheNICUintheaspiringroupcomparedwiththeplacebogroup(11.1vs31.4days;areductionof20.3days).183 Overall, inthewholepopulation,includingzerolengthsofstayforthosethatwerenotadmittedtotheNICU,themeanlengthofstaywaslongerintheplacebothanintheaspiringroup(2.06vs0.66days;reductionof1.4days).Thiscorrespondedtoareductioninlengthofstayby68%.183
ResultsfromtheASPREtrialprovidedefinitiveevidencethateffec-tivescreeningforpretermPEcanbeachievedwithacombinedtestofmaternalfactorsandbiomarkersat11–13weeksandaspirintreatmentfromthefirsttrimesterofpregnancycansignificantlyreducetheriskofdevelopingpretermPE.Furthermore,inpregnanciesathighriskofpretermPE,administrationofaspirinreducesthelengthofstayintheNICUby68%.Thefindingshaveimplicationsforbothshort-andlong-term savings as well as infant survival, disability, and human capital.
FIGOmakes the following recommendation forearlypreventionof preterm PE:
Best practice recommendation:Followingthefirst-trimesterscreen-ing and assessment for preterm PE, women identified at high riskshould receive aspirin prophylaxis commencing at 11–14+6weeksof gestation at a dose of ~150mg to be taken every night untileither 36weeks of gestation,when delivery occurs, orwhen PE isdiagnosed.171
Quality of evidenceStrength of recommendation
High ⊕⊕⊕⊕ Strong

| 21Poon ET AL.
This recommendation is supported by the evidence from theASPRE trial.182 The choice for recommending night-time consump-tionof low-doseaspirin isbasedon the results froma randomized,double-blind,placebo-controlled,chronotherapytrialon350high-riskwomen.Thistrialdemonstratedthatwomentakinglow-doseaspirinat100mg, comparedwithplacebo,hada significantly lowerhazardratio (HR)ofseriousadverseoutcomes,acompositeofPE,pretermbirth,FGR,andIUFD(HR0.35;95%CI,0.22–0.56)andthattheeventrate of serious adverse outcomeswas significantly lower inwomentakinglow-doseaspirinintheevening,comparedwithinthemorningandafternoon(HR0.19;95%CI,0.10–0.39).184
The latest systematic reviewandmeta-analysis,which included16 randomized controlled trial studies for a totalof18907partic-ipants, demonstrated that administration of aspirinwas associatedwithareduction intheriskofpretermPE(RR0.62;95%CI,0.45–0.87).However,therewasnosignificanteffectontermPE(RR0.92;95% CI, 0.70–1.21). Only the subgroup in which aspirin was started at less thanorequal to16weeksofgestationatadoseofgreaterthan or equal to 100mg/dwas associatedwith a reduction in thefrequency of pretermPE (RR 0.33; 95%CI, 0.19–0.57;P=0.0001). Aspirinstartedafter16weeksoradministeredinadailydoseoflessthan100mgwasnotassociatedwithasignificantreductioninratesof preterm or term PE.185 Suggested aspirin dosages are provided in Table 5.
Low-doseaspirin isdefinedasdosageof less than300mg/d. In1979, Masotti etal.186 demonstrated that aspirin 2.5–3.5mg/kg isthe required dosage to produce a consistent inhibition of plateletaggregation with slight inhibition of prostaglandin production. Therecommendeddosageof150mg/dwouldbesufficientforanaveragewomanwithaweightof65kgatbooking.
Pragmatic practice recommendation: Where it is not possible to source the above suggested aspirin regime, the minimum dosage of aspirintobeprescribedtohigh-riskwomenshouldbe100mg/d.
Quality of evidenceStrength of recommendation
Moderate ⊕⊕⊕O Conditional
Best practice recommendation:High-riskwomenmustbe informedand counselled about the importance of treatment adherence and assessed for compliance at each prenatal visit.
Quality of evidenceStrength of recommendation
High ⊕⊕⊕⊕ Strong
InasecondaryanalysisofdatafromtheASPREtrial,theinflu-enceofadherenceonthebeneficialeffectofaspirininpreventionofpretermPEwasevaluated.Thechoiceofcut-offforgoodcom-pliancewasredefinedasgreaterthan90%,whichwasbasedonanexploratoryanalysisof the treatmenteffect.PretermPEoccurredin 5/555 (0.9%) participants in the aspirin groupwith adherence
greaterthanorequalto90%,in8/243(3.3%)ofparticipantsintheaspirin group with adherence less than 90%, in 22/588 (3.7%) of participants in theplacebo groupwith adherence greater thanorequalto90%,andin13/234(5.6%)ofparticipantsintheplacebogroupwithadherence lessthan90%.TheORintheaspiringroupfor preterm PE was 0.24 (95% CI, 0.09–0.65) for adherence more than 90% and 0.59 (95% CI, 0.23–1.53) for adherence less than 90%.The beneficial effect of aspirin in preventing preterm PE isdependent on adherence.187Inaddition,therewasnoevidenceofheterogeneity intheaspirineffect insubgroupsdefinedaccordingtomaternal characteristics and obstetric history,with the excep-tionofchronichypertension.Inwomenwithchronichypertension,preterm PE occurred in 10.2% (5/49) in the aspirin group and in 8.2%(5/61)intheplacebogroup(adjustedOR1.29;95%CI,0.33–5.12);therespectivevaluesinthosewithoutchronichypertensionwere 1.1% (8/749) in the aspirin group and 3.9% (30/761) in the placebogroup(adjustedOR0.27;95%CI,0.12–0.60).Prophylacticaspirin may not be as effective in lowering preterm PE risk inwomenwith chronic hypertension comparedwith other high-riskgroups. Further, in women with adherence of more than 90% the adjustedORintheaspiringroupwas0.24(95%CI,0.09–0.65), inthe subgroup with chronic hypertension it was 2.06 (95% CI, 0.40–10.71), and in those without chronic hypertension it was 0.05 (95% CI, 0.01–0.41).
Pragmatic practice recommendation: If vaginal spotting occurs itmust be duly assessed but does not necessitate stopping aspirin prophylaxis.
Quality of EVIDENCEStrength of recommendation
High ⊕⊕⊕⊕ Strong
Several systematic reviews of randomized controlled trials havedemonstrated that the use of low-dose aspirin during pregnancy isnot associatedwith hemorrhagic complications.179,188,189 The study bytheUSPreventiveServicesTaskForce,whichincludedmorethan23000 pregnantwomen, showed that the risk of placental abrup-tion (RR1.17;95%CI,0.93–1.48) andpostpartumhemorrhage (RR1.02;95%CI,0.96–1.09)didnotsignificantly increasewith theuse
T A B L E 5 Proposedaspirinregimeforpretermpre-eclampsiaprevention.
Maternal weight, kg
Daily required dosage, mg Administration, mg
<40 100 1 × 100
≥40 ~150 2 × 60 2 × 75 2 × 81 1×100+½×100(discardtheother half) ½×300(discardtheotherhalf)

22 | Poon ET AL.
of aspirin.188Inaddition,womenwhowereexposedtolow-doseaspi-rin during pregnancy had similar mean blood loss to those who were notexposedtolow-doseaspirin.188Arecentmeta-analysisinvolving12 585 pregnant women showed that the use of aspirin at less than 100mg/dorgreaterthanorequalto100mg/d,regardlessof initia-tiontime (≤16or>16weeks),wasnotassociatedwithan increasedriskofplacentalabruptionorprepartumhemorrhage.190IntheASPREtrial,womenexposedtoaspirindidnothaveincreasedriskofbleedingadverse events.136Duringthetrial,womenwithvaginalspottingwerenotadvisedtostopthetrialmedication.
Best practice recommendation: Inwomenwith low calcium intake(<800mg/d),eithercalcium replacement (≤1gelemental calcium/d)orcalciumsupplementation(1.5–2gelementalcalcium/d)mayreducetheburdenofbothearly-andlate-onsetPE.191
Quality of evidenceStrength of recommendation
Low ⊕⊕OO Conditional
PEwasreducedconsistentlywithlow-dosecalciumwithorwith-outco-supplements(ninetrials,2234women,RR0.38;95%CI,0.28–0.52),aswellasforsubgroups:low-dosecalciumalone(fourtrials,980women,RR0.36;95%CI,0.23–0.57); low-dosecalciumplus linoleicacid (twotrials,134women,RR0.23;95%CI,0.09–0.60); low-dosecalciumplusvitaminD(twotrials,1060women,RR0.49;95%CI,0.31–0.78);andatrendforlow-dosecalciumplusantioxidants(onetrial,60women,RR0.24;95%CI,0.06–1.01).Overallresultswereconsistentwiththesinglequalitytrialoflow-dosecalciumalone(171women,RR0.30;95%CI,0.06–1.38).Forhigh-dosecalcium,theaverageriskofhighbloodpressurewasreducedwithcalciumsupplementationversusplacebo(12trials,15470women,RR0.65;95%CI,0.53–0.81).TherewasareductionintheaverageriskofPEassociatedwithcalciumsup-plementation(13trials,15730women,RR0.45;95%CI,0.31–0.65).Theeffectwasgreatest forwomenwith lowbaselinecalcium intake(eight trials,10678women,RR0.36;95%CI,0.20–0.65)andthoseselectedasbeingathighrisk(fivetrials,587women,RR0.22;95%CI,0.12–0.42).Thevariablemethodsofselectingwomenasbeingathighrisklimittheclinicalusefulnessofthesepooledresults.191
Pragmatic practice recommendation:Inhigh-riskwomenwhoaresen-sitiveorallergictoaspirin,andintheabsenceofotherproveninter-ventions,closevigilandexpectantmanagementareappropriate.Theseinclude frequent clinic blood pressure and/or home blood pressuremonitoringtoensureearlydiagnosisofPE.Thepurportedbenefitofother treatments, such as heparin, vitamins C and E, magnesium, folate, metformin,andstatinforprophylaxisofpretermPEisnotyetbasedoncredibleevidenceandtheirusesolely for thepurposeofpreventingpretermPEinpregnancyisneitherjustifiednorrecommended.192–198
Quality of evidenceStrength of recommendation
VeryLow⊕OOO Conditional
Pragmatic practice recommendation: Inwomenwithmultiplepreg-nancies,theuseoflow-doseaspirinforthepreventionofPEmaybeconsidered;however,moreresearchisrequiredtodemonstrateahighlevel of evidence.
Quality of evidenceStrength of recommendation
VeryLow⊕OOO Conditional
Thelatestsystematicreviewandmeta-analysisofsixrandomizedcontrolled trials, including 898 pregnancies, demonstrated a signifi-cantreductionintheriskofPE(RR0.67;95%CI,0.48–0.94)andmildPE(RR0.44;95%CI,0.24–0.82)butnotseverePE(RR1.02;95%CI,0.61–1.72)with low-doseaspirin.TheriskofSGAwasnotchanged(RR1.09;95%CI,0.80–1.47).ThereductionofPEwasnotdifferentbetweenwomenrandomizedbefore(RR0.86;95%CI,0.41–1.81)orafter16weeksofgestation(RR0.64;95%CI,0.43–0.96;P=0.50). The authorsconcludedthatthereisalowlevelofevidencesupportingtheuseoflow-doseaspirinforthepreventionofPEandSGAneonatesinmultiplegestations.199
TheFIGOinitiativeforPEismeanttoprovideapracticalandprag-maticguidefornationalassociationstoadoptandpromoteauniformapproachtopredictingandpreventingpretermPEforallcountriesandregionsbasedontheirfinancial,human,andinfrastructureresources.A pathway for preterm PE prevention and screening is shown inFigure 5.
• FIGO adopts and supports the Fetal Medicine Foundationpositionthatallpregnantwomenshouldbescreenedforpre-termpre-eclampsiabythefirst-trimestercombinedtestwithmaternal risk factors, mean arterial pressure, uterine arterypulsatility index, and placental growth factor as a one-stepprocedure.
• FIGOadoptsandsupportstheFetalMedicineFoundationposi-tionthatinhigh-riskwomen,definedbythefirst-trimestercom-bined test, aspirin ~150 mg/night should be commenced at 11–14+6weeksofgestationuntileither36weeksofgestation,whendeliveryoccurs,orwhenpre-eclampsiaisdiagnosed.
• Giventheresourceconstraintsinlow/middle-incomecountries,variationsofthefirst-trimestercombinedtestshouldbeconsid-eredbutthebaselinetestshouldbematernalriskfactorscom-bined with mean arterial pressure.
• FIGOencouragesallcountriesanditsmemberassociationstoadapt and promote strategies to improve access to prenatal ser-vicesandencourageearlybooking.
• FIGOencouragesallcountriesanditsmemberassociationstoensure that risk assessment and resource-appropriate testingforpretermpre-eclampsiabecomean integralpartof routinefirst-trimesterevaluationprotocolofferedatallmaternalhealthservices.

| 23Poon ET AL.
F I G U R E 5 Pathwayofpretermpre-eclampsiascreeningandprevention.

24 | Poon ET AL.
7 | RESOURCE- BASED APPROACH TO SCREENING
Implementation of guidelines is a constant challenge. The reality isthat most low-resource countries around the world are unable toimplementafirst-trimesterscreeningprogramforpretermPEbasedon the combined test.
Recommendationsthatarerigidandimpracticalinreal-lifesettingsare unlikely to be implemented andhencemayproduce little or noimpact.Ontheotherhand,pragmaticbutlessthanidealrecommen-dations may produce significant impact owing to morewidespreadimplementation.
The FIGO approach is three pronged: (1) to promote, encourage, and advocate ideal evidence-based guidance; (2) to offer pragmatic options for resource-constrained situations based on local experience backed by less than optimal evidence; and (3) to promote research aimed at improving the evidence base in both well-resourced and resource-constrained contexts.
FIGOrecommendationsarebasedonavailableresourcesatcoun-trylevelandevidenceoflocalpractice.Countriesworldwidefallintofour resource categories. There are also variations seenwithin anycountry.Anaffluentcountrymayhavepocketsofpoorlyfundedcareand,conversely,alow-ormiddle-resourcecountrymayhave“stateoftheart”careintheprivatesectorforaselectedfew.
High-resource countries:IncludescountriesorregionslikeNorthAmerica,WesternEurope,Japan,SouthKorea,Australia,etc.
Upper/middle-resource countries: Includes countries like Brazil,China,Colombia,Hungary,Malaysia,Mexico,Romania,SouthAfrica,Turkey,etc.
Low/middle-resource countries: Includes countries like India,Indonesia,Pakistan,Nigeria,Egypt,Vietnam,thePhilippines,etc.
Low-resource countries: Includes countries like Bangladesh,Nepal, Cambodia, Kenya, Tanzania, Uganda, Ethiopia, Congo, SierraLeone, etc.
Inlow-andmiddle-incomecountrieswhereresourcesarelimited,variationsofthefirst-trimestercombinedtestcanbeconsideredbutthebaselinetestisonethatcombinesmaternalriskfactorswithMAP.Intheabsenceofoneortwoofthebiomarker(s),riskcalculationcanstillbedonebutthedetectionratesforpretermPEwillbereduced,inturnleadingtoareductioninthetreatmenteffectsizebyaspirinprophylaxisbutmaymakethetreatmenteconomicallyfeasible.
As99%ofseriousmorbidityoccursinlow-andmiddle-incomesettings,anypredictionandpreventionstrategiesneedtobeappliedin these settings to impact on the global burden. An estimated70000 women die each year from PE. Low- and middle-incomecountries are disproportionately affected by avoidable maternaldeaths,with84%ofmortalitiesoccurringinSub-SaharanAfricaandSouthern Asia.200 Regional variation in hypertension disorders inpregnancy as a cause of maternal mortality is also seen, with the highest burden in LatinAmerica and the Caribbean,where thesedisorders are responsible for 22% of deaths compared with 14% globally.Foreverywomanthatdies,another20sufferlife-alteringmorbidity.
PredictionandpreventionofPE isan importantgoal inreducingavoidable mortality and morbidity on a global scale but enabling this in diversehealthsystemsremainsachallenge.Predictionmodelsbasedonearlymaternalcharacteristicstoimproveriskstratificationrequirecontactwith healthcare services in the first trimester.A systematicanalysis of early prenatal care visits between 1990 and 2013 showed that although worldwide coverage increased by 40%, in 2013 only 24% ofvisitswere in low-income countries comparedwith 82% in high-income countries.201Althoughprogressincoverageofprenatalcareisimprovingovertime,itremainsfarfromuniversal.Furtherunderstand-ing of contextual factors influencing barriers to prenatal care suchasacceptability,affordability,andgeographicalaccessibility iscrucialwhenconsideringapproachestoimprovequalityandcoverageofcare.
Communityoutreachstrategiessuchasmobileclinicsareanexam-pleofattemptstoincreasecoverage;however,qualityofcareinthesesettingshasrarelybeenevaluated.Across-sectionalstudycomparingqualityofprenatalcarebetweenfixedandmobileclinicsinHaitifoundlow referral rates, with 95% of women found to be hypertensive not being referred to a higher level of care to screen for proteinuria.202 This highlightstheneedtofocusonprovidereducation,consistentadher-ence to clinical guidelines, and improvement in referral pathways.
A health systems approach must be advocated for, particularlyin low- and middle-income countries where systems are weakest.Concentrating solely ondeliveryof health servicesor new technol-ogiesaimedatriskpredictionisunlikelytoworkalonetoreducetheburden of mortality and morbidity. However, it remains an import-ant goal and must be accompanied by necessary pathways to deliver effectiveprophylaxis,suchaswithaspirin.Althoughaffordable,edu-cationandprescribing/deliverypathwaysmustbeestablished if thisstrategy is tobeeffective.Workforce,availabilityofessentialdrugs,informationsystems,governance, andfinancing thereforemustalsobe addressed.
Prioritiesforunder-resourcedsettingsmaybefocusedaroundtheavailabilityofaccurate,functionalbloodpressuremonitoringdevices;facilityforassessmentofrisksuchasproteinuria;trainingofstaff(par-ticularlyifultrasoundistobeusedforscreening),includingforappro-priateescalationandmanagement;ensuringreliablesupplychainsfortheprovisionofaspirin,antihypertensives,andmagnesiumsulphate;and the availability of laboratory services. This will need to be in paral-lelwithanystrategytoimplementprevention.
Cost-effectiveness of an early PE prediction and preventionapproach has been evaluated in high-income countries and hasshown substantial cost saving.203 However, in low- and middle-income countries,multiple system-level barriers exist that impactimplementation,evaluation,andsustainabilityofsuchapproaches.Economic analysis of basic screening devices such as blood pres-suremonitors andurinedipsticks foruse in low-resource settingshasshownthatsimpledevicesaremostcost-effective.204 The more sophisticated tools for first-trimester screening must be evalu-atedinthiscontext.Moreworkisrequiredtoevaluatethebalancebetweenbetterdetectionversuscostofscreeningwithcurrentsuc-cessfulpredictionalgorithms,andtreatmentpathwayswhenappliedtoalow-incomesetting.

| 25Poon ET AL.
A key barrier to early prediction and prevention of PE in low-resource settings is the delayed first prenatalvisit or even contactwithahealthcareworker.Further, inmanyplacesbloodpressure isnot beingmeasured at all.More efforts to raise awareness of thebenefitsof an early prenatalvisit (targeted atwomenof reproduc-tive age, primary healthcare workers, women's self-help groups,etc.), coupled with skills development of primary healthcare pro-viders on risk assessment, accurate blood pressure measurement,counsellingskills,andensuringaspirinavailabilityandadherencetotreatment and follow-upwill have a far greater impact onPE out-comesthanmakingmoreadvancedtestingtechnologyandprotocolsavailable.IntegratingPEriskassessmentasanintegralpartofbasic
first-trimester evaluation protocol (measuring weight, blood pres-sure, hemoglobin, blood sugar, etc.) will go a long way to improve implementation.
• All countries have an obligation to implement the best pre-eclampsiatestingandmanagementpracticestheycan.
• FIGOacknowledgesthatforglobalprogresstobemade,India,China,Nigeria,Pakistan,thePhilippines,Indonesia,Bangladesh,Brazil,andMexicomustbekeytargetsforfocusedpre-eclamp-siaattention.

26 | Poon ET AL.
8 | COST- EFFECTIVENESS OF PRE- ECLAMPSIA SCREENING
Itiswellestablishedthatsignificanthealthcareresourceshavetobeinvested to prevent morbidity and mortality related to PE and that, as a consequence, bothmaternal and neonatal costs are inflatedcompared with an uncomplicated pregnancy. Given the relativefrequencyofPE,thesecostsaresignificantforthehealthcaresys-temandthewidespreadimplementationofaprediction/preventionstrategywouldhelpeasethisburden.Asthebesttestsforpredic-tion involve a multivariate model that includes several investiga-tivetools,manyconsiderscreeningtobecomplexandexpensive.ItisthereforeimportanttofirstrecognizethecurrentcostsofPE,and the potential benefit in spending a fraction of the sum thatwouldberecoupedthrougheffectivepreventiononcomprehensivescreening.
The reported costs of PE do vary depending on the jurisdic-tion.ExamplesofcostsincludethosereportedwithintheUSAandIrish healthcare systems.A reviewof billing data collected by theCalifornianMedi-Calhealthcareprogramestimated thecostofanuncomplicated vaginal delivery to be US $4500 in 2011 (US $4900 based on Consumer Price Index to 2017).205 The average incre-mental cost for a pregnancy complicated by hypertensive disease was US$8200, with an estimated total incremental cost for allCalifornian births of more than US $200 million. Costs were high-est forwomenwhohad severedisease requiringdelivery at early(<34weeks) gestations. In this cohort, the incremental cost wasUS$70100 per pregnancy. Although costs for an uncomplicateddelivery were reported to be lower in Ireland (US $3000) there was asimilarincreaseincostforpregnanciesaffectedbyPE(incrementof US $3300).206
Throughlinkageofthematernalandneonataldatasets,itispossi-ble to show that the predominant driver for increased costs in preterm birth is neonatal care.207While costs ofmaternal care rise 2.7-foldforwomenwhoneedtobedeliveredbefore32weeksofgestation,costsofneonatalcareincrease35-fold.Pretermbirthimpactsjust8%of thepopulationbut it is responsible for61%ofallcosts.Deliverybefore32weeksofgestationaffectsjust1%ofinfantsbutisresponsi-blefor36%ofobstetriccosts.AthirdCaliforniandatasetshowedthatthese margins hold true for PE as well as other adverse outcomes. In thisseriesthecostburdenwasUS$1311at36weekscomparedwithUS$150000at26weeksofgestation.208 The authors suggested that theannualburdenofPEtotheUSAin2012,includingcareofmotherandchildforthefirst12monthsafterdelivery,wasUS$2.18billion.
Asystematicreviewofthe literatureshowedthatthereareonlyfour cost-effective analyses that focus on interventions for preven-tionofPE.Threeoftheseexaminedtheimpactofaspirin,thefourthfocusedonthepotentialvalueofcalciumsupplementation.
Thefirstpaper toassess theeconomicvalueof a comprehensivefirst-trimester screening tool (usingmaternal characteristics, the bio-markersplacentalprotein13andPLGFandUTPI)describedthreeendpoints: theprevalenceofPE, costs until discharge afterdelivery, andincrementalcostperquality-adjustedlife-year(QALY)toavoidperinatal
death.209Theauthorswerenotprescriptiveabouttheintervention,sug-gestingthatlow-doseaspirin,calcium,orvitaminsupplementationcouldbeused—eitheraloneorincombination—andusingsensitivityanalysistodemonstratedifferentialeffect.Theauthorsdefinedcostsbasedonthe Israelihealthcaresystemandalsodemonstratedthatcostbenefitwasaffectedbyprevalenceofdisease.Usingthesemodels,theauthorsconcludedthatscreeningforPEwaseffectiveinvariousscenarios.
Werner et al.210 used a decision model to determine which one of fourpotentialstrategiesforpreventionofPEwasmostcost-effective.Treatment involved either no prophylaxis, provision of aspirin towomendeemedhighriskinaccordancewithACOGguidelinesortheUS Preventative ServicesTask Force recommendations, or universalprophylaxis.17,129 Costs were based on US healthcare prices. The model showedthatboththeUSPreventativeServicesTaskForceapproachanduniversalprophylaxis ledtoasimilarandsignificantreductionintheprevalenceofPE;themajordifferencebeingthat76.5%ofwomenwould not be prescribed aspirin using the former approach. The authors suggested rolling out either of these policies to all four million pregnant womenintheUSAasthiswouldresultincostsavingsofapproximatelyUS $370 million (similar using either approach).
Thecheapnatureof the intervention (aspirin)makesapolicyofuniversal screening attractive and easy to advocate. It is, however,importanttorecognizethatalthoughaspiriniscurrentlyrecommendedforprophylaxis,onlyaminorityofhigh-riskwomenaretreated,withmedicationstartingatanappropriatetimepoint.211 Secondly, there is nohigh-qualityevidencedemonstrating that apolicyofuniversalprophylaxisworks.Thirdly,manypregnantwomenprefertoavoidtak-ingmedicationswhen theyarepregnantandcompliance is likely tobepoor.Whilethesafetyprofileforaspirinisgood,recentepidemi-ological data suggest that this drug may be associated with a small increaseintheriskofhavinganinfantaffectedbycerebralpalsy.212 Therelativeriskforcerebralpalsyismuchlowerthanthatassociatedwith preterm birth, so this does not impact pregnancies deemed to be highriskthroughformalmultivariatescreeningprograms,butitshouldmakecliniciansmorecircumspectaboutuniversalprescription.
TheASPREtrialdidnotshowasignificantreductioninadmissionratestotheNICU(6.8%incontrolsvs6.2%inhigh-riskwomenwhowereprescribed aspirin) but did showa significant reduction in thelengthofstay(31.4daysvs11.1days,respectively).183Thisequatedtoa68%reductioninthelengthofstayfortheaspirin-treatedgroupand an equivalent reduction in neonatal costs,which, as previouslydescribed, are the dominant costs in these models.
Prior to introducing first-trimester screening for PE, a Canadiangroupexamined thepotential costbenefitof screeningwithaspirinprophylaxis in high-riskwomen.203 The group used a decision anal-ysismodelassigningprobabilitiesandassociatedcostsateachnodebasedonlocalpublisheddataandpublicdatabases.TheinterventionmimickedthatdescribedinASPREandthiswascomparedtocurrentstandardofcare(prescriptionof81mgaspirinbasedonmaternalhis-tory).Sensitivityanalysiswasperformedtovarytheuptakeofscreen-ing and the probability of being prescribed aspirin if found to be in a high-risk group. The model showed that first-trimester screeningandprescriptionofaspirintohigh-riskwomenledtobothareduction

| 27Poon ET AL.
inprevalenceofdiseaseandaCAD$14.4millioncostsavingtotheCanadian healthcare system. This saving was demonstrated despite theconservativenatureofsomeofthecostings.Thecostofamother/infant being delivered at less than 34weeks of gestationwas onlycostedatCAD$13268.21,thereforethecostsavingsfrompreventionofearly-onsetPEmaybeunderestimated.Thecostoffirst-trimesterscreeningwasestimatedatCAD$668.84;however,incircumstanceswherefirst-trimesteraneuploidyscreeningisperformedthis is likelylower(CAD$100pertest),whichwouldleadtoacostreduction(andfurthersavingtothehealthsystem)ofanadditionalCAD$220millionper year.
Afourthcost-effectivenessanalysis focusedoncalciumprophy-laxisandusedadecisionanalyticmodeltoexaminetheimpactofthistreatment ifprescribedtoallpregnantwomen, towomen identifiedasbeinghighriskforPE,ortowomenwithlowdietaryintakeofcal-cium.213Thesethreemodels ledtocorrespondingreductionsofdis-easeprevalenceof25%,8%,and13%,respectively—alldemonstratingcost savings ranging from €2 to 4.6 million per 100 000 pregnancies. Onceagain,thelowcostoftheinterventionmakesuniversalprophy-laxisappealing.
None of these models have adequately considered the long-term health effects of PE.Whilematernal cerebrovascular eventsare rare, Pourat et al.205estimateda lifetimecostofUS$659156
for such an event in a 25-year-oldwoman. Similarly,womenwhohadPEhavehigherrisksofothercardiovascularpathologiesinmid-dleagethatmaybeavoidedthrougheffectivefirst-trimesterscreen-ingandprophylaxis.Preterminfantshavesignificantriskofcerebralpalsyandneurodevelopmentaldelay—disabilitiesthathaveanasso-ciated estimated cost of US$38250 per year.205 These children/youngadultsalsohavehigherrisksofhypertension,type2diabetes,andmetabolicsyndrome—allassociatedwiththeirownburdensandhealthcare costs.
Further cost-effective analyses are needed to demonstrate thevalueoffirst-trimesterscreeningindifferentpopulations,withdiffer-entdiseaseprevalenceanddifferentmodels/costsofmedicalcare.Tothis point, allmodels have suggested that the introduction of first-trimester prediction and prevention dominates current screeningstrategies. This is largely driven by the cost savings associated with reductionofpretermdelivery.
• FIGO considers early screening to be a measure that would mostlikelyincreasesavingstothehealthsystem.
• FIGOcallsformorecost-effectiveanalysestobeconductedtoshowthisbenefittopolicymakers.
28 | Poon ET AL.
REFERENCES
1. FIGOWorkingGrouponGoodClinicalPractice inMaternal–FetalMedicine. Good clinical practice advice: First trimester screeningandpreventionofpre-eclampsiainsingletonpregnancy.Int J Gynecol Obstet. 2019;144:325–329.
2. Tranquilli AL, Dekker G, Magee L, et al. The classification, diag-nosis and management of the hypertensive disorders of preg-nancy:A revised statement from the ISSHP.Pregnancy Hypertens. 2014;4:97–104.
3. Magee LA, PelsA, HelewaM, Rey E, vonDadelszen P; CanadianHypertensive Disorders of Pregnancy (HDP) Working Group.Diagnosis,evaluation,andmanagementof thehypertensivedisor-ders of pregnancy. Pregnancy Hypertens. 2014;4:105–145.
4. LoweSA,BowyerL,LustK,etal.SOMANZguidelinesfortheman-agement of hypertensive disorders of pregnancy 2014. Aust N Z J Obstet Gynaecol. 2015;55:e1–e29.
5. Brown MA, Magee LA, Kenny LC, et al. The hypertensive disor-ders of pregnancy: ISSHP classification, diagnosis &managementrecommendations for international practice. Pregnancy Hypertens. 2018;13:291–310.
6. VillarJ,SayL,GulmezogluAM,etal.Eclampsiaandpre-eclampsia:Ahealthproblemfor2000years.In:CritchlyH,MacLeanA,PostL,WalkJ,eds.Pre-Eclampsia.London:RCOGPress;2003:189–207.
7. RonsmansC,GrahamWJ.Maternalmortality:Who,when,where,and why. Lancet. 2006;368:1189–1200.
8. Kuklina EV, Ayala C, CallaghanWM. Hypertensive disorders andsevere obstetric morbidity in the United States. Obstet Gynecol. 2009;113:1299–1306.
9. LisonkovaS,JosephKS.Incidenceofpreeclampsia:Riskfactorsandoutcomes associated with early- versus late-onset disease. Am J Obstet Gynecol. 2013;209:544.
10. LisonkovaS,SabrY,MayerC,YoungC,SkollA,JosephKS.Maternalmorbidityassociatedwithearly-onsetandlate-onsetpreeclampsia.Obstet Gynecol. 2014;124:771–781.
11. Redman CW, Sargent IL. Latest advances in understanding pre-eclampsia. Science. 2005;308:1592–1594.
12. JimB,KarumanchiSA.Preeclampsia:Pathogenesis,prevention,andlong-termcomplications.Semin Nephrol. 2017;37:386–397.
13. Chaiworapongsa T, Chaemsaithong P, Yeo L, Romero R. Pre-eclampsia part 1: Current understanding of its pathophysiology. Nat Rev Nephrol. 2014;10:466–480.
14. Thilaganathan B. Pre-eclampsia and the cardiovascular-placentalaxis.Ultrasound Obstet Gynecol. 2018;51:714–717.
15. WorldHealthOrganization.WHO Recommendations for Prevention and Treatment of pre-Eclampsia and Eclampsia. Geneva: WHO; 2011.
16. National Collaborating Centre for women's and Children's Health(UK). Hypertension in Pregnancy: The Management of Hypertensive Disorders During Pregnancy.London:RCOGPress;2010.
17. AmericanCollegeofObstetriciansandGynecologists;TaskForceonHypertensioninPregnancy.Hypertensioninpregnancy.Reportof the American College of Obstetricians and Gynecologists’Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013;122:1122–1131.
18. LoweSA,BrownMA,DekkerGA,etal.Guidelinesforthemanage-ment of hypertensive disorders of pregnancy 2008. Aust N Z J Obstet Gynaecol. 2009;49:242–246.
19. KhalilA,SyngelakiA,MaizN,ZinevichY,NicolaidesKH.Maternalage and adverse pregnancy outcome: A cohort study.Ultrasound Obstet Gynecol. 2013;42:634–643.
20. Lamminpaa R, Vehvilainen-Julkunen K, Gissler M, Heinonen S.Preeclampsia complicated by advanced maternal age: A registry-based study on primiparous women in Finland 1997-2008. BMC Pregnancy Childbirth. 2012;12:47.
21. YogevY,MelamedN,BardinR,Tenenbaum-GavishK,Ben-ShitritG,Ben-HaroushA.Pregnancyoutcomeatextremelyadvancedmater-nal age. Am J Obstet Gynecol. 2010;203:558.e1–558.e7.
22. Balasch J, Gratacos E. Delayed childbearing: Effects on fertil-ity and the outcome of pregnancy. Curr Opin Obstet Gynecol. 2012;24:187–193.
23. PoonLC,KametasNA,ChelemenT,LealA,NicolaidesKH.Maternalriskfactorsforhypertensivedisordersinpregnancy:Amultivariateapproach. J Hum Hypertens. 2010;24:104–110.
24. Duckitt K, Harrington D. Risk factors for pre-eclampsia at ante-natal booking: Systematic review of controlled studies. BMJ. 2005;330:565.
25. LuoZ-C,AnN,XuH-R,LaranteA,AudibertF,FraserWD.Theeffectsandmechanismsofprimiparityontheriskofpre-eclampsia:Asys-tematicreview.Paediatr Perinat Epidemiol. 2007;21(Suppl.1):36–45.
26. Robillard PY, Hulsey TC, Alexander GR, Keenan A, de Caunes F,PapiernikE.Paternitypatternsandriskofpreeclampsia inthe lastpregnancyinmultiparae.J Reprod Immunol. 1993;24:1–12.
27. Hernandez-Diaz S, Toh S, Cnattingius S. Risk of pre-eclampsia infirst and subsequent pregnancies: Prospective cohort study.BMJ. 2009;338:b2255.
28. CampbellDM,MacGillivray I,Carr-HillR.Pre-eclampsia in secondpregnancy. Br J Obstet Gynaecol. 1985;92:131–140.
29. Sibai BM, el-Nazer A, Gonzalez-Ruiz A. Severe preeclampsia-eclampsia in young primigravid women: Subsequent preg-nancy outcome and remote prognosis. Am J Obstet Gynecol. 1986;155:1011–1016.
30. LieRT,RasmussenS,BrunborgH,GjessingHK,Lie-NielsenE,IrgensLM. Fetal and maternal contributions to risk of pre-eclampsia:Populationbasedstudy.BMJ. 1998;316:1343–1347.
31. Odegard RA, Vatten LJ, Nilsen ST, Salvesen KA, Austgulen R.Risk factors and clinical manifestations of pre-eclampsia. BJOG. 2000;107:1410–1416.
32. vanRijnBB,HoeksLB,BotsML,FranxA,BruinseHW.Outcomesofsubsequentpregnancyafterfirstpregnancywithearly-onsetpre-eclampsia. Am J Obstet Gynecol. 2006;195:723–728.
33. LangenveldJ,JansenS,vanderPostJ,WolfH,MolBW,GanzevoortW.Recurrenceriskofadeliverybefore34weeksofpregnancyduetoanearlyonsethypertensivedisorder:Asystematicreview.Am J Perinatol. 2010;27:565–571.
34. Rousso D, Panidis D, Gkoutzioulis F, Kourtis A, Mavromatidis G,KalahanisI.Effectoftheintervalbetweenpregnanciesonthehealthof mother and child. Eur J Obstet Gynecol Reprod Biol. 2002;105:4–6.
35. King JC.The risk ofmaternal nutritional depletion and poor out-comes increases in early or closely spaced pregnancies. J Nutr. 2003;133:1732S–1736S.
36. Conde-AgudeloA,Rosas-BermudezA,Kafury-GoetaAC.Effectsofbirthspacingonmaternalhealth:Asystematicreview.Am J Obstet Gynecol. 2007;196:297–308.
37. MigniniLE,CarroliG,BetranAP,etal. InterpregnancyintervalandperinataloutcomesacrossLatinAmericafrom1990to2009:Alargemulti-countrystudy.BJOG. 2016;123:730–737.
38. WinikoffB.Theeffectsofbirthspacingonchildandmaternalhealth.Stud Fam Plann. 1983;14:231–245.
39. KlebanoffMA.Theintervalbetweenpregnanciesandtheoutcomeofsubsequentbirths.N Engl J Med. 1999;340:643–644.
40. JacksonRA,GibsonKA,WuYW,CroughanMS.Perinataloutcomesinsingletonsfollowinginvitrofertilization:Ameta-analysis.Obstet Gynecol. 2004;103:551–563.
41. TrogstadL,MagnusP,MoffettA,StoltenbergC.Theeffectofrecur-rentmiscarriageand infertilityontheriskofpre-eclampsia.BJOG. 2009;116:108–113.
42. Pandey S, ShettyA, HamiltonM, Bhattacharya S, Maheshwari A.Obstetricandperinataloutcomesinsingletonpregnanciesresulting

| 29Poon ET AL.
fromIVF/ICSI:Asystematicreviewandmeta-analysis.Hum Reprod Update. 2012;18:485–503.
43. Thomopoulos C, Tsioufis C, Michalopoulou H, Makris T,PapademetriouV, Stefanadis C. Assisted reproductive technologyand pregnancy-related hypertensive complications: A systematicreview. J Hum Hypertens. 2013;27:148–157.
44. MartinAS,MonsourM,KawwassJF,BouletSL,KissinDM,JamiesonDJ. Risk of preeclampsia in pregnancies after assisted reproduc-tive technology and ovarian stimulation. Matern Child Health J. 2016;20:2050–2056.
45. AlbrechtED,BonaguraTW,BurleighDW,EndersAC,AberdeenGW,PepeGJ.Suppressionofextravilloustrophoblastinvasionofuterinespiral arteries by estrogen during early baboon pregnancy. Placenta. 2006;27:483–490.
46. Imudia AN, Awonuga AO, Doyle JO, et al. Peak serum estradiollevel during controlled ovarian hyperstimulation is associatedwith increased risk of small for gestational age and preeclamp-sia in singleton pregnancies after in vitro fertilization. Fertil Steril. 2012;97:1374–1379.
47. Fisher SJ. Why is placentation abnormal in preeclampsia? Am J Obstet Gynecol. 2015;213:S115–S122.
48. SmithGN,WalkerM,TessierJL,MillarKG. Increased incidenceofpreeclampsiainwomenconceivingbyintrauterineinseminationwithdonorversuspartnerspermfortreatmentofprimaryinfertility.Am J Obstet Gynecol. 1997;177:455–458.
49. HoyJ,VennA,HallidayJ,KovacsG,WaalwykK.Perinatalandobstet-ricoutcomesofdonor inseminationusingcryopreservedsemen inVictoria,Australia.Hum Reprod. 1999;14:1760–1764.
50. SalhaO, SharmaV,DadaT, et al.The influence of donated gam-etes on the incidence of hypertensive disorders of pregnancy. Hum Reprod. 1999;14:2268–2273.
51. NeedJA,BellB,MeffinE,JonesWR.Pre-eclampsiainpregnanciesfromdonorinseminations.J Reprod Immunol. 1983;5:329–338.
52. Simeone S, Serena C, Rambaldi MP, Marchi L, Mello G, MecacciF. Risk of preeclampsia and obstetric outcome in donor oocyteand autologous in vitro fertilization pregnancies.Minerva Ginecol. 2016;68:9–14.
53. NakabayashiY,NakashimaA,YoshinoO, et al. Impairment of theaccumulationofdecidualTcells,NKcells,andmonocytes,andthepoor vascular remodeling of spiral arteries, were observed in oocyte donationcases,regardlessofthepresenceorabsenceofpreeclamp-sia. J Reprod Immunol. 2016;114:65–74.
54. Arngrimsson R, Bjornsson S, Geirsson RT, Bjornsson H, WalkerJJ, Snaedal G. Genetic and familial predisposition to eclampsiaand pre-eclampsia in a defined population. Br J Obstet Gynaecol. 1990;97:762–769.
55. Cincotta RB, Brennecke SP. Family history of pre-eclampsia as apredictor forpre-eclampsia inprimigravidas. Int J Gynaecol Obstet. 1998;60:23–27.
56. WilliamsPJ,BroughtonPF.Thegeneticsofpre-eclampsiaandotherhypertensive disorders of pregnancy. Best Pract Res Clin Obstet Gynaecol. 2011;25:405–417.
57. Zintzaras E, Kitsios G, Harrison GA, et al. Heterogeneity-basedgenome search meta-analysis for preeclampsia. Hum Genet. 2006;120:360–370.
58. CnattingiusS,BergstromR,LipworthL,KramerMS.Prepregnancyweightandtheriskofadversepregnancyoutcomes.N Engl J Med. 1998;338:147–152.
59. WeissJL,MaloneFD,EmigD,etal.Obesity,obstetriccomplicationsandcesareandeliveryrate–apopulation-basedscreeningstudy.Am J Obstet Gynecol. 2004;190:1091–1097.
60. LeungTY,LeungTN,SahotaDS,etal.TrendsinmaternalobesityandassociatedrisksofadversepregnancyoutcomesinapopulationofChinese women. BJOG. 2008;115:1529–1537.
61. SyngelakiA, Bredaki FE,Vaikousi E,MaizN,NicolaidesKH.Bodymassindexat11-13weeks’gestationandpregnancycomplications.Fetal Diagn Ther. 2011;30:250–265.
62. LiuL,HongZ,ZhangL.Associationsofprepregnancybodymassindex and gestational weight gain with pregnancy outcomesin nulliparous women delivering single live babies. Sci Rep. 2015;5:12863.
63. RahmanMM,AbeSK,KandaM, et al.Maternal bodymass indexandriskofbirthandmaternalhealthoutcomesinlow-andmiddle-incomecountries:Asystematicreviewandmeta-analysis.Obes Rev. 2015;16:758–770.
64. WeiY-M,YangH-X,ZhuW-W,etal.Riskofadversepregnancyout-comesstratifiedforpre-pregnancybodymassindex.J Matern Fetal Neonatal Med. 2016;29:2205–2209.
65. Catalano PM. Obesity, insulin resistance, and pregnancy outcome. Reproduction. 2010;140:365–371.
66. GregorMF,Hotamisligil GS. Inflammatorymechanisms in obesity.Annu Rev Immunol. 2011;29:415–445.
67. SpradleyFT,PaleiAC,GrangerJP.Immunemechanismslinkingobe-sity and preeclampsia. Biomolecules. 2015;5:3142–3176.
68. Mittendorf R, Lain KY,WilliamsMA,Walker CK. Preeclampsia. Anested, case-control study of risk factors and their interactions. J Reprod Med. 1996;41:491–496.
69. KnuistM,BonselGJ,ZondervanHA,TreffersPE.Riskfactorsforpre-eclampsiainnulliparouswomenindistinctethnicgroups:Aprospec-tivecohortstudy.Obstet Gynecol. 1998;92:174–178.
70. MostelloD,CatlinTK,RomanL,HolcombWLJ,LeetT.Preeclampsiain the parous woman: Who is at risk? Am J Obstet Gynecol. 2002;187:425–429.
71. CaugheyAB,StotlandNE,WashingtonAE,EscobarGJ.Maternaleth-nicity, paternal ethnicity, and parental ethnic discordance: Predictors of preeclampsia. Obstet Gynecol. 2005;106:156–161.
72. GhoshG,Grewal J,MannistoT, et al. Racial/ethnic differences inpregnancy-relatedhypertensivediseaseinnulliparouswomen.Ethn Dis. 2014;24:283–289.
73. RussellRB,GreenNS,SteinerCA,etal.Costofhospitalizationforpreterm and low birth weight infants in the United States. Pediatrics. 2007;120:e1–e9.
74. BurtVL,WheltonP,RoccellaEJ,etal.PrevalenceofhypertensionintheUSadultpopulation.ResultsfromtheThirdNationalHealthand Nutrition Examination Survey, 1988-1991. Hypertension. 1995;25:305–313.
75. KestenbaumB,SeligerSL,EasterlingTR, et al.Cardiovascular andthromboembolic events following hypertensive pregnancy. Am J Kidney Dis. 2003;42:982–989.
76. BellamyL,CasasJ-P,HingoraniAD,WilliamsDJ.Pre-eclampsiaandrisk of cardiovascular disease and cancer in later life: Systematicreviewandmeta-analysis.BMJ. 2007;335:974.
77. KhalilA,RezendeJ,AkolekarR,SyngelakiA,NicolaidesKH.Maternalracial origin and adverse pregnancy outcome: A cohort study.Ultrasound Obstet Gynecol. 2013;41:278–285.
78. BartschE,MedcalfKE,ParkAL,RayJG.Clinicalriskfactorsforpre-eclampsia determined in early pregnancy: Systematic review andmeta-analysisoflargecohortstudies.BMJ. 2016;353:i1753.
79. MuddLM,OweKM,MottolaMF,PivarnikJM.Healthbenefitsofphysical activity during pregnancy: An international perspective.Med Sci Sports Exerc. 2013;45:268–277.
80. SchneiderS,FreerksenN,RohrigS,HoeftB,MaulH.Gestationaldia-betesandpreeclampsia–similarriskfactorprofiles?Early Hum Dev. 2012;88:179–184.
81. Conti E, Zezza L, Ralli E, et al. Growth factors in preeclampsia:A vascular disease model. A failed vasodilation and angiogenicchallenge from pregnancy onwards?. Cytokine Growth Factor Rev. 2013;24:411–425.

30 | Poon ET AL.
82. Guimaraes MF, Brandao AHF, Rezende CA, et al. Assessment ofendothelial function in pregnant women with preeclampsia andgestationaldiabetesmellitusbyflow-mediateddilationofbrachialartery. Arch Gynecol Obstet. 2014;290:441–447.
83. Kane SC, Costa Fda S, Brennecke S. First trimester biomarkers inthe prediction of later pregnancy complications. Biomed Res Int. 2014;2014:807196.
84. KaracayO,Sepici-DincelA,KarcaaltincabaD,et al.Aquantitativeevaluationof total antioxidant statusandoxidativestressmarkersinpreeclampsiaandgestationaldiabeticpatientsin24-36weeksofgestation.Diabetes Res Clin Pract. 2010;89:231–238.
85. WiznitzerA,MayerA,NovackV,etal.Associationoflipidlevelsduringgestation with preeclampsia and gestational diabetes mellitus: Apopulation-basedstudy.Am J Obstet Gynecol. 2009;201:482.e1–e8.
86. ZhouJ,ZhaoX,WangZ,HuY.Combinationoflipidsanduricacidinmid-secondtrimestercanbeusedtopredictadversepregnancyoutcomes. J Matern Fetal Neonatal Med. 2012;25:2633–2638.
87. EngelandA,BjorgeT,DaltveitAK,etal.Riskofdiabetesaftergesta-tionaldiabetesandpreeclampsia.Aregistry-basedstudyof230,000women in Norway. Eur J Epidemiol. 2011;26:157–163.
88. FeigDS,ShahBR,LipscombeLL,etal.Preeclampsiaasa risk fac-tor for diabetes: A population-based cohort study. PLoS Med. 2013;10:e1001425.
89. LibbyG,MurphyDJ,McEwanNF,etal.Pre-eclampsiaandthelaterdevelopment of type 2 diabetes in mothers and their children: An intergenerational study from theWalker cohort. Diabetologia. 2007;50:523–530.
90. MannistoT,MendolaP,VaarasmakiM,etal.Elevatedbloodpres-sureinpregnancyandsubsequentchronicdiseaserisk.Circulation. 2013;127:681–690.
91. ParrettiE, LapollaA,DalfraM, et al. Preeclampsia in leannormo-tensive normotolerant pregnant women can be predicted by simple insulinsensitivityindexes.Hypertension. 2006;47:449–453.
92. Sierra-LaguadoJ,GarciaRG,CeledonJ,etal.Determinationofinsu-linresistanceusingthehomeostaticmodelassessment(HOMA)anditsrelationwiththeriskofdevelopingpregnancy-inducedhyperten-sion. Am J Hypertens. 2007;20:437–442.
93. LegroRS.Insulinresistanceinwomen'shealth:Whyitmattersandhowtoidentifyit.Curr Opin Obstet Gynecol. 2009;21:301–305.
94. Ryan EA, Imes S, Liu D, et al. Defects in insulin secretion andaction inwomenwith a history of gestational diabetes.Diabetes. 1995;44:506–512.
95. D'Anna R, Baviera G, Corrado F, et al. Adiponectin and insu-lin resistance in early- and late-onset pre-eclampsia. BJOG. 2006;113:1264–1269.
96. Soonthornpun K, Soonthornpun S, Wannaro P, Setasuban W, ThamprasitA.Insulinresistanceinwomenwithahistoryofseverepre-eclampsia.J Obstet Gynaecol Res. 2009;35:55–59.
97. FuhMM-T,YinC-S,PeiD,etal.Resistancetoinsulin-mediatedglu-coseuptakeandhyperinsulinemiainwomenwhohadpreeclampsiaduring pregnancy. Am J Hypertens. 1995;8:768–771.
98. Ray JG. Dysmetabolic syndrome, placenta-mediated diseaseand future risk of cardiovascular disease. Fetal Matern Med Rev. 2004;15:231–246.
99. HarborneL,FlemingR, LyallH,SattarN,NormanJ.Metforminorantiandrogeninthetreatmentofhirsutisminpolycysticovarysyn-drome. J Clin Endocrinol Metab. 2003;88:4116–4123.
100. GirouardJ,GiguereY,MoutquinJ-M,ForestJ-C.Previoushyperten-sivediseaseofpregnancyisassociatedwithalterationsofmarkersofinsulin resistance. Hypertension. 2007;49:1056–1062.
101. BeckDW,MenezesAH.Intracerebralhemorrhageinapatientwitheclampsia. JAMA. 1981;246:1442–1443.
102. Zhang J, Meikle S, Trumble A. Severe maternal morbidity associ-ated with hypertensive disorders in pregnancy in the United States. Hypertens Pregnancy. 2003;22:203–212.
103. Chesley LC, Annitto JE, Cosgrove RA. The remote prognosis ofeclamptic women. Sixth periodic report.. Am J Obstet Gynecol. 1976;124:446–459.
104. KaajaR.Insulinresistancesyndromeinpreeclampsia.Semin Reprod Endocrinol. 1998;16:41–46.
105. Garovic VD, Hayman SR. Hypertension in pregnancy: An emerg-ing risk factor for cardiovascular disease. Nat Clin Pract Nephrol. 2007;3:613–622.
106. CraiciI,WagnerS,GarovicVD.Preeclampsiaandfuturecardiovas-cularrisk:Formalriskfactororfailedstresstest?Ther Adv Cardiovasc Dis. 2008;2:249–259.
107. Brown MC, Best KE, Pearce MS, Waugh J, Robson SC, Bell R.Cardiovasculardiseaseriskinwomenwithpre-eclampsia:Systematicreviewandmeta-analysis.Eur J Epidemiol. 2013;28:1–19.
108. McDonald SD, Malinowski A, Zhou Q, Yusuf S, Devereaux PJ.Cardiovascular sequelae of preeclampsia/eclampsia: A systematicreviewandmeta-analyses.Am Heart J. 2008;156:918–930.
109. McDonald SD, Han Z, Walsh MW, Gerstein HC, Devereaux PJ.Kidneydiseaseafterpreeclampsia:Asystematic reviewandmeta-analysis. Am J Kidney Dis. 2010;55:1026–1039.
110. Fisher KA, LugerA, Spargo BH, LindheimerMD. Hypertension inpregnancy:Clinical-pathologicalcorrelationsandremoteprognosis.Medicine (Baltimore). 1981;60:267–276.
111. Vikse BE, Irgens LM, Leivestad T, Skjaerven R, Iversen BM.Preeclampsiaandtheriskofend-stagerenaldisease.N Engl J Med. 2008;359:800–809.
112. CallawayLK,LawlorDA,O'CallaghanM,WilliamsGM,NajmanJM,McIntyreHD.Diabetesmellitus in the21years after apregnancythatwascomplicatedbyhypertension:Findingsfromaprospectivecohort study. Am J Obstet Gynecol. 2007;197:492.e1–e7.
113. Carr DB, Newton KM, Utzschneider KM, et al. Preeclampsia andrisk of developing subsequent diabetes. Hypertens Pregnancy. 2009;28:435–447.
114. CartyDM,DellesC,DominiczakAF.Preeclampsiaandfuturemater-nal health. J Hypertens. 2010;28:1349–1355.
115. Yu CK, Khouri O, Onwudiwe N, Spiliopoulos Y, Nicolaides KH.Prediction of pre-eclampsia by uterine artery Doppler imaging:Relationshiptogestationalageatdeliveryandsmall-for-gestationalage. Ultrasound Obstet Gynecol. 2008;31:310–313.
116. TeramoKA,HiilesmaaVK, Schwartz R, ClemonsGK,Widness JA.Amnioticfluidandcordplasmaerythropoietinlevelsinpregnanciescomplicatedbypreeclampsia,pregnancy-inducedhypertensionandchronic hypertension. J Perinat Med. 2004;32:240–247.
117. AaliBS,MalekpourR,SedigF,SafaA.Comparisonofmaternalandcordbloodnucleated redblood cell count betweenpre-eclampticand healthy women. J Obstet Gynaecol Res. 2007;33:274–278.
118. Yucesoy G, Ozkan S, Bodur H, et al.Maternal and perinatal out-come in pregnancies complicated with hypertensive disorder of pregnancy:Asevenyearexperienceofa tertiarycarecenter.Arch Gynecol Obstet. 2005;273:43–49.
119. DuleyL.Theglobal impactofpre-eclampsia andeclampsia.Semin Perinatol. 2009;33:130–137.
120. YerlikayaG,AkolekarR,McPhersonK,SyngelakiA,NicolaidesKH. Prediction of stillbirth from maternal demographic and pregnancy characteristics. Ultrasound Obstet Gynecol. 2016;48:607–612.
121. Moutquin J-M. Classification and heterogeneity of preterm birth.BJOG. 2003;110(Suppl):30–33.
122. Ilekis JV, Reddy UM, Roberts JM. Preeclampsia–a pressingproblem: An executive summary of a National Institute ofChild Health and Human Development workshop. Reprod Sci. 2007;14:508–523.
123. Marlow N, Wolke D, Bracewell MA, Samara M. Neurologic anddevelopmentaldisabilityatsixyearsofageafterextremelypretermbirth. N Engl J Med. 2005;352:9–19.
| 31Poon ET AL.
124. KhashuM, NarayananM, Bhargava S, Osiovich H. Perinatal out-comesassociatedwithpretermbirthat33to36weeks’gestation:Apopulation-basedcohortstudy.Pediatrics. 2009;123:109–113.
125. OsmondC,BarkerDJ.Fetal,infant,andchildhoodgrowtharepredic-tors of coronary heart disease, diabetes, and hypertension in adult men and women. Environ Health Perspect. 2000;108(Suppl):545–553.
126. Bibbins-Domingo K, Grossman DC, Curry SJ, et al. Screening forpreeclampsia:USPreventiveServicesTaskForceRecommendationStatement. JAMA. 2017;317:1661–1667.
127. Committee Opinion No. 638: First-trimester risk assessment forearly-onsetpreeclampsia.Obstet Gynecol. 2015;126:e25–e27.
128. ACOGCommitteeOpinionNo.743Summary:Low-doseaspirinuseduring pregnancy. Obstet Gynecol. 2018;132:254–256.
129. LeFevreML.Low-doseaspirinuse for thepreventionofmorbidityandmortalityfrompreeclampsia:U.S.PreventiveServicesTaskForcerecommendationstatement.Ann Intern Med. 2014;161:819–826.
130. American Diabetes Association. 13. Management of diabetes inpregnancy: Standards ofMedical Care inDiabetes-2018.Diabetes Care. 2018;41:S137–S143.
131. WallenburgHC.Preventionof pre-eclampsia: Status andperspec-tives2000.Eur J Obstet Gynecol Reprod Biol. 2001;94:13–22.
132. O'GormanN,WrightD, Poon LC, et al.Multicenter screening forpre-eclampsiabymaternalfactorsandbiomarkersat11–13weeks’gestation:ComparisonwithNICEguidelinesandACOGrecommen-dations.Ultrasound Obstet Gynecol. 2017;49:756–760.
133. AkolekarR,SyngelakiA,PoonL,WrightD,NicolaidesKH.Competingrisksmodel inearlyscreening forpreeclampsiabybiophysicalandbiochemicalmarkers.Fetal Diagn Ther. 2013;33:8–15.
134. O'GormanN,WrightD,SyngelakiA,etal.Competingrisksmodelinscreening for preeclampsia bymaternal factors and biomarkers at11-13weeksgestation.Am J Obstet Gynecol. 2016;214:103.e1–103.e12.
135. O'Gorman N, Wright D, Poon LC, et al. Accuracy of competing-risksmodelinscreeningforpre-eclampsiabymaternalfactorsandbiomarkers at 11-13weeks’ gestation.Ultrasound Obstet Gynecol. 2017;49:751–755.
136. RolnikDL,WrightD,PoonLCY,etal.ASPREtrial:Performanceofscreening for preterm pre-eclampsia. Ultrasound Obstet Gynecol. 2017;50:492–495.
137. TanMY,WrightD,SyngelakiA,etal.Comparisonofdiagnosticaccu-racy of early screening for pre-eclampsia by NICE guidelines anda method combining maternal factors and biomarkers: Results ofSPREE.Ultrasound Obstet Gynecol. 2018;51:743–750.
138. TanMY, SyngelakiA, Poon LC, et al. Screening for pre-eclampsiaby maternal factors and biomarkers at 11-13 weeks’ gestation.Ultrasound Obstet Gynecol. 2018;52:186–195.
139. Poon LC, Rolnik DL, Tan MY, et al. ASPRE trial: Incidence ofpretermpre-eclampsia inpatients fulfillingACOGandNICE crite-riaaccording to riskbyFMFalgorithm.Ultrasound Obstet Gynecol. 2018;51:738–742.
140. ParkFJ,LeungCHY,PoonLCY,WilliamsPF,RothwellSJ,HyettJA.Clinicalevaluationofafirst trimesteralgorithmpredictingtheriskof hypertensive disease of pregnancy. Aust N Z J Obstet Gynaecol. 2013;53:532–539.
141. OliveiraN,MagderLS,BlitzerMG,BaschatAA.First-trimesterpre-dictionofpre-eclampsia:Externalvalidityofalgorithmsinaprospec-tivelyenrolledcohort.Ultrasound Obstet Gynecol. 2014;44:279–285.
142. LoboGA,NowakPM,PanigassiAP,etal.ValidationofFetalMedicineFoundationalgorithmforpredictionofpre-eclampsiainthefirsttri-mesterinanunselectedBrazilianpopulation.J Matern Fetal Neonatal Med. 2019;32:286–292.
143. RochaRS,AlvesJA,MaiaEHolandaMouraSB,etal.Simpleapproachbased on maternal characteristics and mean arterial pressure forthepredictionofpreeclampsiainthefirsttrimesterofpregnancy.J Perinat Med. 2017;45:843–849.
144. Wright D, Syngelaki A, Akolekar R, Poon LC, Nicolaides KH.Competing risks model in screening for preeclampsia by mater-nal characteristics and medical history. Am J Obstet Gynecol. 2015;213:62.e1–62.e10.
145. Poon LC, Zymeri NA, Zamprakou A, Syngelaki A, Nicolaides KH.Protocolformeasurementofmeanarterialpressureat11-13weeks’gestation.Fetal Diagn Ther. 2012;31:42–48.
146. WrightA,WrightD,IspasCA,PoonLC,NicolaidesKH.Meanarte-rialpressureinthethreetrimestersofpregnancy:Effectsofmater-nal characteristics andmedical history.Ultrasound Obstet Gynecol. 2015;45:698–706.
147. PoonLC,KametasNA,PandevaI,ValenciaC,NicolaidesKH.Meanarterialpressureat11(+0)to13(+6)weeksinthepredictionofpre-eclampsia. Hypertension. 2008;51:1027–1033.
148. NationalHeartFoundationofAustralia.HypertensionManagementGuide for Doctors. 2004. [website] www.heartfoundation.org.au.AccessedApril1,2006.
149. Poon LC, Kametas NA, Valencia C, Chelemen T, Nicolaides KH.Hypertensive disorders in pregnancy: Screening by systolic diastolic andmean arterial pressure at 11-13weeks.Hypertens Pregnancy. 2011;30:93–107.
150. Poon LC, Kametas N, Strobl I, Pachoumi C, Nicolaides KH. Inter-arm blood pressure differences in pregnant women. BJOG. 2008;115:1122–1130.
151. MaynardSE,MinJ-Y,MerchanJ,etal.Excessplacentalsolublefms-liketyrosinekinase1(sFlt1)maycontributetoendothelialdysfunc-tion, hypertension, and proteinuria in preeclampsia. J Clin Invest. 2003;111:649–658.
152. LevineRJ,MaynardSE,QianC,etal.Circulatingangiogenicfactorsandtheriskofpreeclampsia.N Engl J Med. 2004;350:672–683.
153. AhmadS,AhmedA.Elevatedplacentalsolublevascularendothelialgrowthfactorreceptor-1inhibitsangiogenesisinpreeclampsia.Circ Res. 2004;95:884–891.
154. Chau K, HennessyA,MakrisA. Placental growth factor and pre-eclampsia. J Hum Hypertens. 2017;31:782–786.
155. WortelboerEJ,KosterMP,KucS,etal.Longitudinaltrendsinfeto-placental biochemicalmarkers, uterine artery pulsatility index andmaternal blood pressure during the first trimester of pregnancy.Ultrasound Obstet Gynecol. 2011;38:383–388.
156. Tidwell SC, Ho HN, ChiuWH, Torry RJ, Torry DS. Low maternalserum levels of placenta growth factor as an antecedent of clinical preeclampsia. Am J Obstet Gynecol. 2001;184:1267–1272.
157. Thadhani R, Mutter WP, Wolf M, et al. First trimester placentalgrowthfactorandsolublefms-liketyrosinekinase1andriskforpre-eclampsia. J Clin Endocrinol Metab. 2004;89:770–775.
158. AkolekarR,ZaragozaE,PoonLC,PepesS,NicolaidesKH.Maternalserumplacentalgrowthfactorat11+0to13+6weeksofgesta-tion in thepredictionofpre-eclampsia.Ultrasound Obstet Gynecol. 2008;32:732–739.
159. ZhongY,ZhuF,DingY. Serumscreening infirst trimester topre-dictpre-eclampsia, small forgestationalageandpretermdelivery:Systematic review and meta-analysis. BMC Pregnancy Childbirth. 2015;15:191.
160. Smith GC, Stenhouse EJ, Crossley JA, Aitken DA, Cameron AD,ConnorJM.Earlypregnancylevelsofpregnancy-associatedplasmaprotein a and the risk of intrauterine growth restriction, prema-ture birth, preeclampsia, and stillbirth. J Clin Endocrinol Metab. 2002;87:1762–1767.
161. SpencerK,YuCK,CowansNJ,OtigbahC,NicolaidesKH.Predictionof pregnancy complications by first-trimester maternal serumPAPP-Aandfreebeta-hCGandwithsecond-trimesteruterinearteryDoppler. Prenat Diagn. 2005;25:949–953.
162. Dugoff L, Hobbins JC, Malone FD, et al. First-trimester maternalserumPAPP-Aand free-betasubunithumanchorionicgonadotro-pin concentrations and nuchal translucency are associated with

32 | Poon ET AL.
obstetric complications: A population-based screening study (theFASTERTrial).Am J Obstet Gynecol. 2004;191:1446–1451.
163. Morris RK, Bilagi A, Devani P, Kilby MD. Association of serumPAPP-A levels infirst trimesterwith small for gestational age andadversepregnancyoutcomes:Systematicreviewandmeta-analysis.Prenat Diagn. 2017;37:253–265.
164. WrightD,SilvaM,PapadopoulosS,WrightA,NicolaidesKH.Serumpregnancy-associated plasma protein-A in the three trimesters ofpregnancy:Effectsofmaternalcharacteristicsandmedicalhistory.Ultrasound Obstet Gynecol. 2015;46:42–50.
165. SotiriadisA,Hernandez-AndradeE,daSilvaCostaF,etal. ISUOGPractice Guidelines: Role of ultrasound in screening for and fol-low-upofpre-eclampsia.Ultrasound Obstet Gynecol. 2019;53:7–22.
166. CarbillonL,PerrotN,UzanM,UzanS.Dopplerultrasonographyandimplantation:Acriticalreview.Fetal Diagn Ther. 2001;16:327–332.
167. CarbillonL,ChallierJC,AlouiniS,UzanM,UzanS.Uteroplacentalcirculation development: Doppler assessment and clinical impor-tance. Placenta. 2001;22:795–799.
168. Olofsson P, Laurini RN,Marsal K.A high uterine artery pulsatilityindexreflectsadefectivedevelopmentofplacentalbedspiralarter-ies in pregnancies complicated by hypertension and fetal growth retardation.Eur J Obstet Gynecol Reprod Biol. 1993;49:161–168.
169. LefebvreJ,DemersS,BujoldE,etal.Comparisonoftwodifferentsitesof measurement for transabdominal uterine artery Doppler velocim-etryat11-13weeks.Ultrasound Obstet Gynecol. 2012;40:288–292.
170. VelautharL,PlanaMN,KalidindiM,etal.First-trimesteruterinearteryDopplerandadversepregnancyoutcome:Ameta-analysisinvolving55,974 women. Ultrasound Obstet Gynecol. 2014;43:500–507.
171. Magee LA, Dadelszen PV, Stones WM. The FIGO Textbook of Pregnancy Hypertension. An Evidence-Based Guide to Monitoring, Prevention and Management. London: The Global Library of Woman's Medicine; 2016.
172. Al-RubaieZ,Askie LM,RayJG,HudsonHM, Lord SJ.Theperfor-manceof risk predictionmodels for pre-eclampsia using routinelycollectedmaternalcharacteristicsandcomparisonwithmodelsthatincludespecialisedtestsandwithclinicalguidelinedecisionrules:Asystematicreview.BJOG. 2016;123:1441–1452.
173. Wright D, Gallo DM, Gil Pugliese S, Casanova C, Nicolaides KH. Contingentscreeningforpretermpre-eclampsia.Ultrasound Obstet Gynecol. 2016;47:554–559.
174. Francisco C, Wright D, Benkő Z, Syngelaki A, Nicolaides KH.Competing-risks model in screening for pre-eclampsia intwin pregnancy according to maternal factors and biomark-ers at 11–13 weeks’ gestation. Ultrasound Obstet Gynecol. 2017;50:589–595.
175. SibaiBM.Thrombophilia andseverepreeclampsia:Time to screenandtreatinfuturepregnancies?Hypertension. 2005;46:1252–1253.
176. Dekker G, Sibai B. Primary, secondary, and tertiary prevention ofpre-eclampsia.Lancet. 2001;357:209–215.
177. CrandonAJ, IsherwoodDM.Effectofaspirinon incidenceofpre-eclampsia. Lancet. 1979;1:1356.
178. Beaufils M, Uzan S, Donsimoni R, Colau JC. Prevention of pre-eclampsiabyearlyantiplatelettherapy.Lancet. 1985;1:840–842.
179. Askie LM,Duley L,Henderson-SmartDJ, Stewart LA.Antiplateletagentsforpreventionofpre-eclampsia:Ameta-analysisofindividualpatientdata.Lancet. 2007;369:1791–1798.
180. BujoldE,RobergeS,NicolaidesKH.Low-doseaspirinforpreventionofadverseoutcomesrelatedtoabnormalplacentation.Prenat Diagn. 2014;34:642–648.
181. RobergeS,GiguereY,VillaP,etal.Earlyadministrationoflow-doseaspirin for thepreventionof severeandmildpreeclampsia:Asys-tematicreviewandmeta-analysis.Am J Perinatol. 2012;29:551–556.
182. Rolnik DL, Wright D, Poon LC, et al. Aspirin versus placebo inpregnancies at high risk for preterm preeclampsia.N Engl J Med. 2017;377:613–622.
183. WrightD,RolnikDL,SyngelakiA,etal.AspirinforEvidence-BasedPreeclampsiaPreventiontrial:Effectofaspirinonlengthofstayinthe neonatal intensive care unit. Am J Obstet Gynecol. 2018;218:612.e1–612.e6.
184. Ayala DE, Ucieda R, Hermida RC. Chronotherapy with low-doseaspirinforpreventionofcomplicationsinpregnancy.Chronobiol Int. 2013;30:260–279.
185. Roberge S, Bujold E,NicolaidesKH.Aspirin for the prevention ofpretermandtermpreeclampsia:Systematicreviewandmetaanaly-sis. Am J Obstet Gynecol. 2018;218:287–293.e1.
186. Masotti G, Galanti G, Poggesi L, Abbate R, Neri Serneri GG.Differentialinhibitionofprostacyclinproductionandplateletaggre-gationbyaspirin.Lancet. 1979;2:1213–1217.
187. Wright D, Poon LC, Rolnik DL, et al. Aspirin for Evidence-BasedPreeclampsiaPreventiontrial:Influenceofcomplianceonbeneficialeffectofaspirininpreventionofpretermpreeclampsia.Am J Obstet Gynecol. 2017;217:685.e1–685.e5.
188. HendersonJT,WhitlockEP,O'ConnerE,SengerCA,ThompsonJH,RowlandMG. Low-Dose Aspirin for the Prevention of Morbidity and Mortality From Preeclampsia: A Systematic Evidence Review for the U.S. Preventive Services Task Force [Internet].Rockville,MD:Agency forHealthcareResearchandQuality(US);2014.
189. DuleyL,Henderson-SmartDJ,MeherS,KingJF.Antiplateletagentsfor preventing pre-eclampsia and its complications. Cochrane Database Syst Rev. 2007;(2):CD004659.
190. Roberge S, Bujold E, Nicolaides KH. Meta-analysis on theeffect of aspirin use for prevention of preeclampsia on placen-tal abruption and antepartum hemorrhage. Am J Obstet Gynecol. 2018;218:483–489.
191. Hofmeyr GJ, Lawrie TA, Atallah AN, Torloni MR. Calcium sup-plementation during pregnancy for preventing hypertensivedisorders and related problems. Cochrane Database Syst Rev. 2018;(10):CD001059.
192. RodgerMA,GrisJ-C,deVriesJIP,etal.Low-molecular-weighthep-arin and recurrent placenta-mediated pregnancy complications: Ameta-analysisofindividualpatientdatafromrandomisedcontrolledtrials. Lancet. 2016;388:2629–2641.
193. MastroliaSA,NovackL,ThachilJ,etal.LMWHinthepreventionofpreeclampsiaandfetalgrowthrestrictioninwomenwithoutthrom-bophilia.A systematic reviewandmeta-analysis.Thromb Haemost. 2016;116:868–878.
194. ChiswickC,ReynoldsRM,DenisonF,etal.Effectofmetforminonmaternalandfetaloutcomesinobesepregnantwomen(EMPOWaR):Arandomised,double-blind,placebo-controlledtrial.Lancet Diabetes Endocrinol. 2015;3:778–786.
195. KalafatE,SukurYE,AbdiA,ThilaganathanB,KhalilA.Metforminforthe prevention of hypertensive disorders of pregnancy inwomenwith gestational diabetes and obesity: A systematic review andmeta-analysis.Ultrasound Obstet Gynecol. 2018;52:706–714.
196. RumboldA, Ota E, Nagata C, Shahrook S, Crowther CA.VitaminC supplementation in pregnancy. Cochrane Database Syst Rev. 2015;(9):CD004072.
197. Rumbold A, Ota E, Hori H, Miyazaki C, Crowther CA. VitaminE supplementation in pregnancy. Cochrane Database Syst Rev. 2015;(9):CD004069.
198. WenSW,WhiteRR,RybakN,etal.Effectofhighdosefolicacidsup-plementationinpregnancyonpre-eclampsia (FACT):Doubleblind,phase III, randomised controlled, international, multicentre trial.BMJ.2018;362:k3478.
199. Bergeron TS, Roberge S, Carpentier C, Sibai B, McCaw-Binns A,Bujold E. Preventionof preeclampsiawith aspirin inmultiple ges-tations: A systematic review and meta-analysis. Am J Perinatol. 2016;33:605–610.
200. SayL,ChouD,GemmillA,etal.Globalcausesofmaternaldeath:AWHOsystematicanalysis.Lancet Glob Health. 2014;2:e323–e333.

| 33Poon ET AL.
201. MollerA-B,PetzoldM,ChouD,SayL.Earlyantenatalcarevisit:Asystematicanalysisofregionalandgloballevelsandtrendsofcover-age from 1990 to 2013. Lancet Glob Health. 2017;5:e977–e983.
202. PhillipsE,StoltzfusRJ,MichaudL,PierreGLF,VermeylenF,PelletierD.Domobileclinicsprovidehigh-qualityantenatalcare?Acompar-isonofcaredelivery,knowledgeoutcomesandperceptionofqual-ity of care betweenfixed andmobile clinics in centralHaiti.BMC Pregnancy Childbirth. 2017;17:361.
203. OrtvedD,HawkinsTL,JohnsonJA,HyettJ,MetcalfeA.Thecost-effectiveness of first trimester screening and early preventativeuseof aspirin inwomenathigh riskofearlyonsetpre-eclampsia.Ultrasound Obstet Gynecol. 2019;53:239–244.
204. McLarenZM,SharpA,HessburgJP,etal.Costeffectivenessofmed-icaldevicestodiagnosepre-eclampsiainlow-resourcesettings.Dev Eng. 2017;2:99–106.
205. PouratN,MartinezAE,JonesJM,etal.Costs of Gestational Hypertensive Disorders in California: Hypertension, Preeclampsia, and Eclampsia. Los Angeles,CA:UCLACenterforHealthPolicyResearch;2013.
206. FoxA,McHughS,BrowneJ,etal.Estimatingthecostofpreeclamp-siainthehealthcaresystem:Cross-sectionalstudyusingdatafromSCOPE Study (screening for pregnancy end points). Hypertension. 2017;70:1243–1249.
207. PhibbsCS,SchmittSK,CooperM,etal.BirthHospitalizationCostsand Days of Care for Mothers and Neonates in California, 2009–2011. J Pediatr. 2019;204:118–125.e14.
208. StevensW,ShihT, IncertiD,etal.Short-termcostsofpreeclamp-sia to the United States health care system. Am J Obstet Gynecol. 2017;217:237–248.e16.
209. ShmueliA,MeiriH,GonenR.Economicassessmentofscreeningforpre-eclampsia.Prenat Diagn. 2012;32:29–38.
210. WernerEF,HauspurgAK,RouseDJ.Acost-benefitanalysisoflow-doseaspirinprophylaxis for thepreventionofpreeclampsia in theUnited States. Obstet Gynecol. 2015;126:1242–1250.
211. HelouA,WalkerS,StewartK,GeorgeJ.Managementofpregnanciescomplicated by hypertensive disorders of pregnancy: Could we do better?Aust N Z J Obstet Gynaecol. 2017;57:253–259.
212. PetersenTG,LiewZ,AndersenAN,etal.Useofparacetamol,ibupro-fenoraspirininpregnancyandriskofcerebralpalsyinthechild.Int J Epidemiol. 2018;47:121–130.
213. Meertens LJE, Scheepers HCJ, Willemse JPMM, SpaandermanMEA, Smits LJM. Shouldwomen be advised to use calcium sup-plementsduringpregnancy?AdecisionanalysisMatern Child Nutr. 2018;14:e12479.