the impact of icd-10-cm upon hospital and physician ... · hospital and physician quality...
TRANSCRIPT
The Impact of ICD-10-CM upon
Hospital and Physician
Quality Measurement
A Primer for Physicians and Hospitals
James S. Kennedy, M.D., C.C.S.

2
Faculty
James S. Kennedy, M.D., C.C.S.
Medical School: University of Tennessee, 1979
Residency: Internal Medicine
University of Tennessee, 1980-82
Board Certification: Internal Medicine
Coding Certification: CCS – AHIMA, 2001
Publications:
Physician Query Handbook, 2009
Severity-Adjusted DRGs: an MS-DRG Primer, 2008
Hypovolemia & Dehydration, JAHIMA, 2006
Letter – Annals of Internal Medicine 2006
615-479-7021

3
Goals
• Review the state of the art of physician and hospital profiling
• Explore ICD-10-CM‟s role in severity and risk adjustment
• Define clinical indicators ICD-10-CM coded diagnoses and treatments
• Develop a strategy that improves physician and hospital ICD-10-CM data quality
Like the Phone Book
Interesting Characters – Terrible Plot
Dictionary without
Definitions

ICD-10 Implementation Date
October 1, 2015
5
Diagnoses Procedures
ICD-10-CM
(Clinical Modification)
All entities - providers and
facilities
for diagnoses in all settings:
– Hospital inpatients
– Hospital outpatients
– Physicians offices
– Emergency department
– Home health
– Long-term care
– Rehabilitation facilities
ICD-10-PCS
(Procedure Coding System)
Used by inpatient facilities ONLY
• Includes outpatient facility services
rendered within the prior 72 hours
of writing the inpatient order
• Very different than ICD-9-CM or
CPT
CPT • Physician and
outpatient/observation facility
services still utilize CPT
• CPT does not change!!

ICD-10-CM/PCS Basics
• ICD-10-CM/PCS (and ICD-9-CM) are NOT clinical languages (like SNOMED) – ICD-9-CM and ICD-10-CM/PCS are useful for classifying
healthcare data for administrative purposes, including reimbursement claims, health statistics, and other uses where data aggregation is advantageous
• ICD-10-CM/PCS is based ONLY on provider documentation of clinical language, not on a patient‟s clinical characteristics that are abstracted by a data analyst (e.g. like STS, NCDR, or ATS databases) – The provider must use the magic words that drive ICD-10-
CM/PCS code assignment based upon patient circumstances
6
• Coding is based only on provider
documentation
• If there is a difference between the attending‟s
notes and a consultant‟s notes, particularly at
the time of discharge, the attending‟s
documentation takes precedent in coding.
ICD-10-CM/PCS Basics
• Inpatient coders cannot code from EKG, laboratory, X-ray or pathology reports, even if interpreted by a board-certified physician – Results must be documented as diagnoses in the
physician‟s notes
• Arrow up (h) or down (i) with labs cannot be interpreted as abnormal i Na of 120 meq/liter ≠ hyponatremia i Hct ≠ Anemia
• Physicians must completely describe and document conditions as to be coded
8
ICD-10-CM/PCS Basics
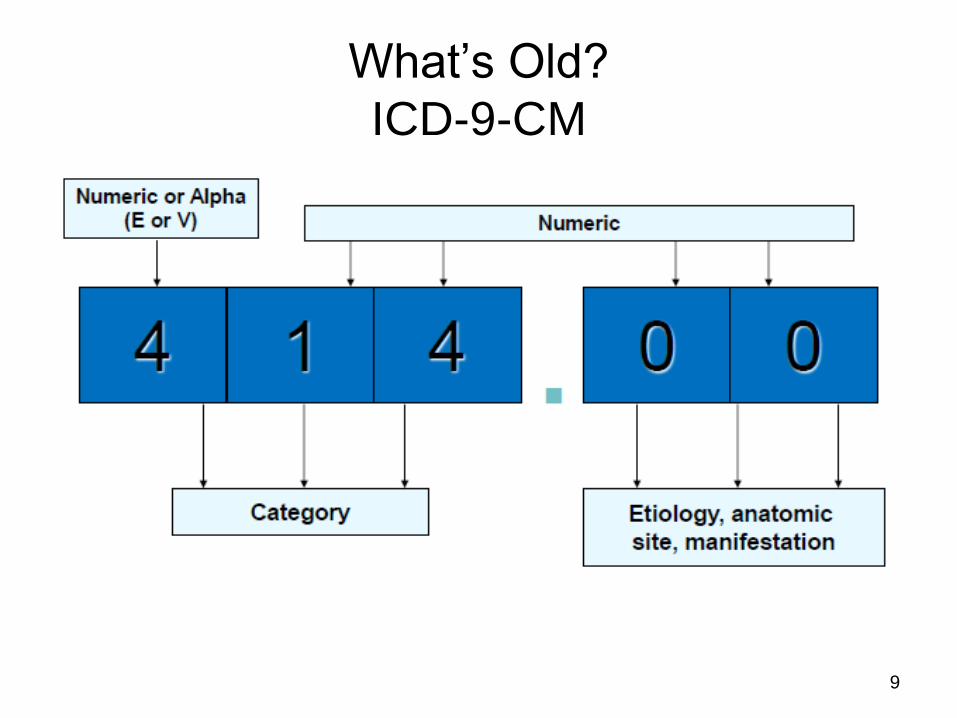
What‟s Old?
ICD-9-CM
9
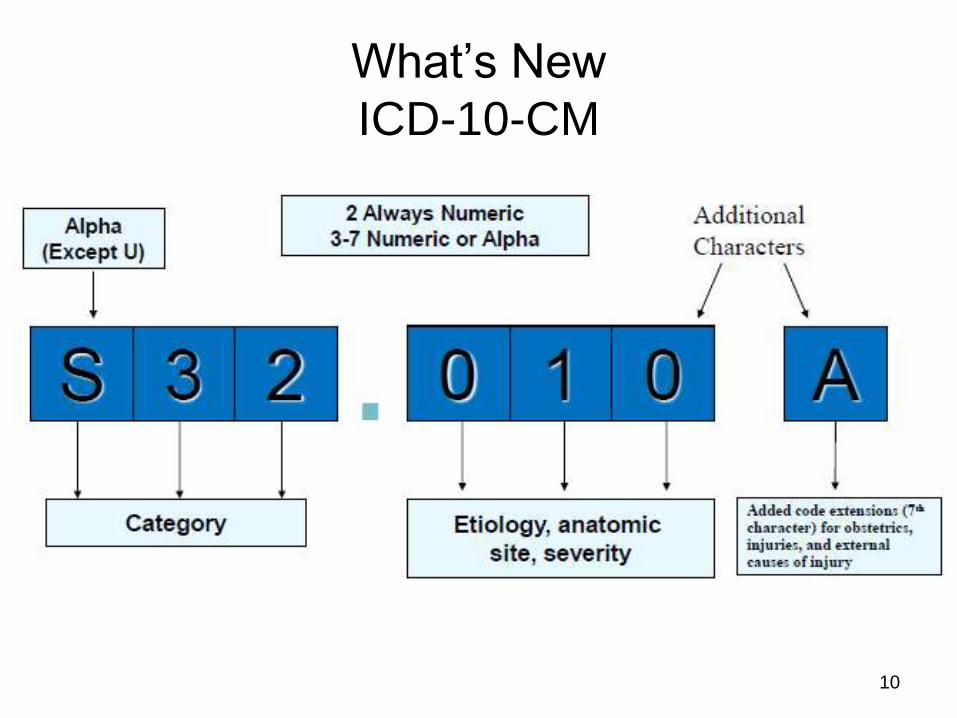
What‟s New
ICD-10-CM
10
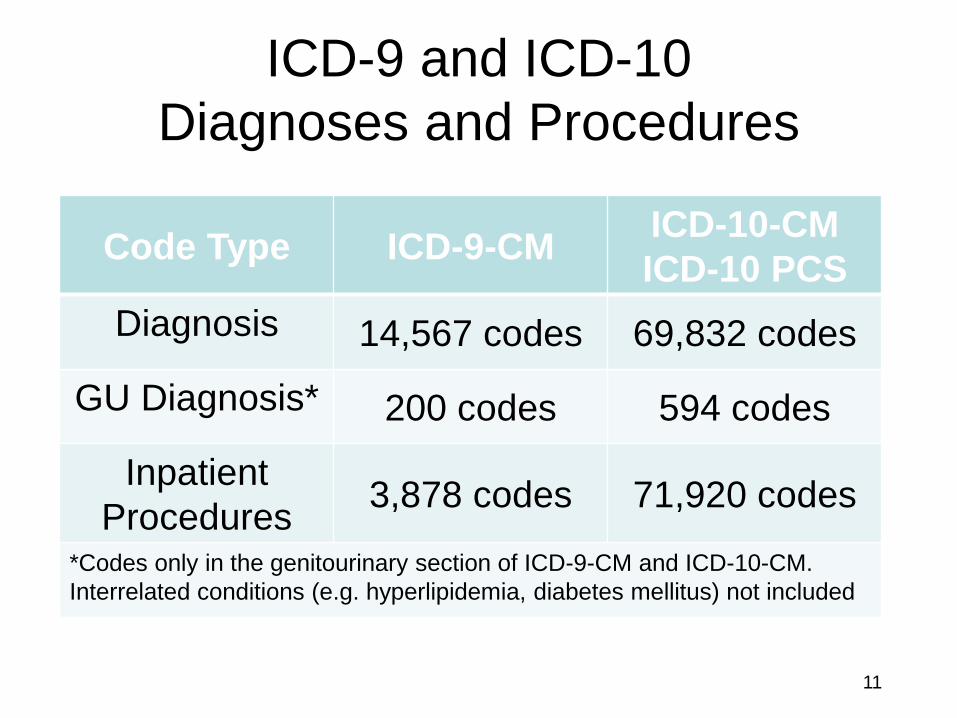
ICD-9 and ICD-10
Diagnoses and Procedures
Code Type ICD-9-CM ICD-10-CM
ICD-10 PCS
Diagnosis 14,567 codes 69,832 codes
GU Diagnosis* 200 codes 594 codes
Inpatient
Procedures 3,878 codes 71,920 codes
*Codes only in the genitourinary section of ICD-9-CM and ICD-10-CM.
Interrelated conditions (e.g. hyperlipidemia, diabetes mellitus) not included
11

Overall Changes
• 34,250 (50%) are related to the musculoskeletal system
• 17,045 (25%) are related to fractures
• 10,582 (62%) of fracture codes to distinguish „right‟ vs. „left‟
• ~25,000 (36%) of all ICD-10 codes to distinguish „right‟ vs. „left‟

Clinical Changes
Expansions and Deletions • Marked expansion of codes
– Trauma, overdoses, or complications treatment phases
– Office encounters
– Asthma
– Diabetes mellitus
– Obstetrics (trimesters)
– Non-pressure ulcer staging
– Myocardial infarction timing and vessel involvement
– Open fractures staging
– Cerebral hemorrhage location
– Ischemic stroke vessel involvement
– Coma (Glasgow Coma Scale)
– Atrial flutter and fibrillation
– Drug underdosing
• Deletion of MD language, such as: – Urosepsis
• Must say “sepsis due to UTI”
– SIRS due to infection • Must say “sepsis” or
“severe sepsis”
– Accelerated or malignant hypertension
• Must describe the organ dysfunction caused by hypertension to measure severity
MD progress notes and DC summaries
must use ICD-10-CM’s language (Index
or Table) as to defend the assigned code

Differences from
ICD-9-CM to ICD-10-CM
ICD-9-CM
Diagnosis Codes ICD-10-CM
Diagnosis Codes
Laterality No Laterality
Laterality –
Right or Left account for 35-40% of codes
Code Construction
3-5 digits 7 digits
First digit is alpha (E or V) or numeric
Digit 1 is alpha; Digit 2 is numeric
Digits 2-5 are numeric Digits 3–7 are alpha or numeric
Decimal is placed after the third character
Decimal is placed after the third character
Placeholders No placeholder characters “X” placeholders
# of Codes 14,000 codes 69,000 codes
Severity Limited Severity Parameters Extensive Severity Parameters
Combination Limited Combination Codes Extensive Combination Codes
Excludes Notes
1 type of Excludes Notes 2 types of Excludes Notes

New Changes
Excludes Notes Excludes1 - A type 1 Excludes note is a pure excludes.
– It means 'NOT CODED HERE!'
– An Excludes1 note indicates that the code excluded should never be used at the same time as the code above the Excludes1 note.
– An Excludes1 is used when two conditions cannot occur together, such as a congenital form versus an acquired form of the same condition.
Excludes2 - A type 2 excludes note represents 'Not included here'.
– An excludes2 note indicates that the condition excluded is not part of the condition it is excluded from but a patient may have both conditions at the same time.
– When an Excludes2 note appears under a code it is acceptable to use both the code and the excluded code together.
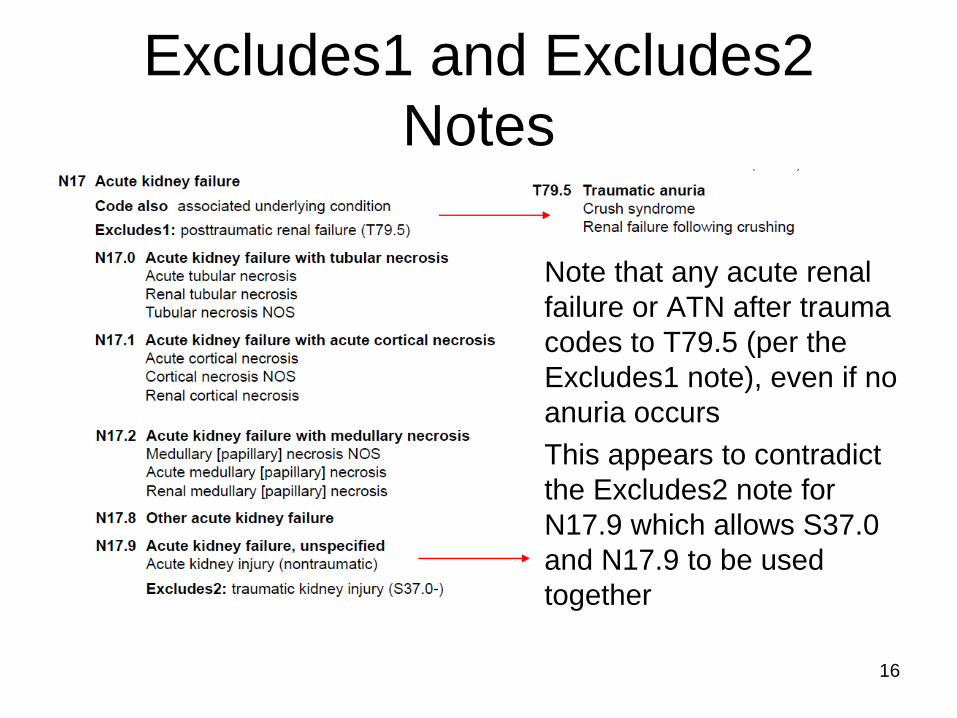
Excludes1 and Excludes2
Notes
Note that any acute renal
failure or ATN after trauma
codes to T79.5 (per the
Excludes1 note), even if no
anuria occurs
This appears to contradict
the Excludes2 note for
N17.9 which allows S37.0
and N17.9 to be used
together
16

New Severity Levels
Emphasis Upon Laterality ICD9 ICD9 Title ICD10 ICD-10 Title
86600 Injury to kidney without mention of open
wound into cavity, unspecified injury
S37001A Unspecified injury of right kidney, initial encounter
S37002A Unspecified injury of left kidney, initial encounter
S37009A Unspecified injury of unspecified kidney, initial encounter
86601
Injury to kidney without mention of open
wound into cavity, hematoma without
rupture of capsule
S37011A Minor contusion of right kidney, initial encounter
S37012A Minor contusion of left kidney, initial encounter
S37019A Minor contusion of unspecified kidney, initial encounter
S37021A Major contusion of right kidney, initial encounter
S37022A Major contusion of left kidney, initial encounter
S37029A Major contusion of unspecified kidney, initial encounter
86602 Injury to kidney without mention of open
wound into cavity, laceration
S37031A Laceration of right kidney, unspecified degree, initial encounter
S37032A Laceration of left kidney, unspecified degree, initial encounter
S37039A Laceration of unspecified kidney, unspecified degree, initial encounter
S37041A Minor laceration of right kidney, initial encounter
S37042A Minor laceration of left kidney, initial encounter
S37049A Minor laceration of unspecified kidney, initial encounter
S37051A Moderate laceration of right kidney, initial encounter
S37052A Moderate laceration of left kidney, initial encounter
S37059A Moderate laceration of unspecified kidney, initial encounter
86603
Injury to kidney without mention of open
wound into cavity, complete disruption of
kidney parenchyma
S37061A Major laceration of right kidney, initial encounter
S37062A Major laceration of left kidney, initial encounter
S37069A Major laceration of unspecified kidney, initial encounter
S37091A Other injury of right kidney, initial encounter
S37092A Other injury of left kidney, initial encounter
S37099A Other injury of unspecified kidney, initial encounter
17

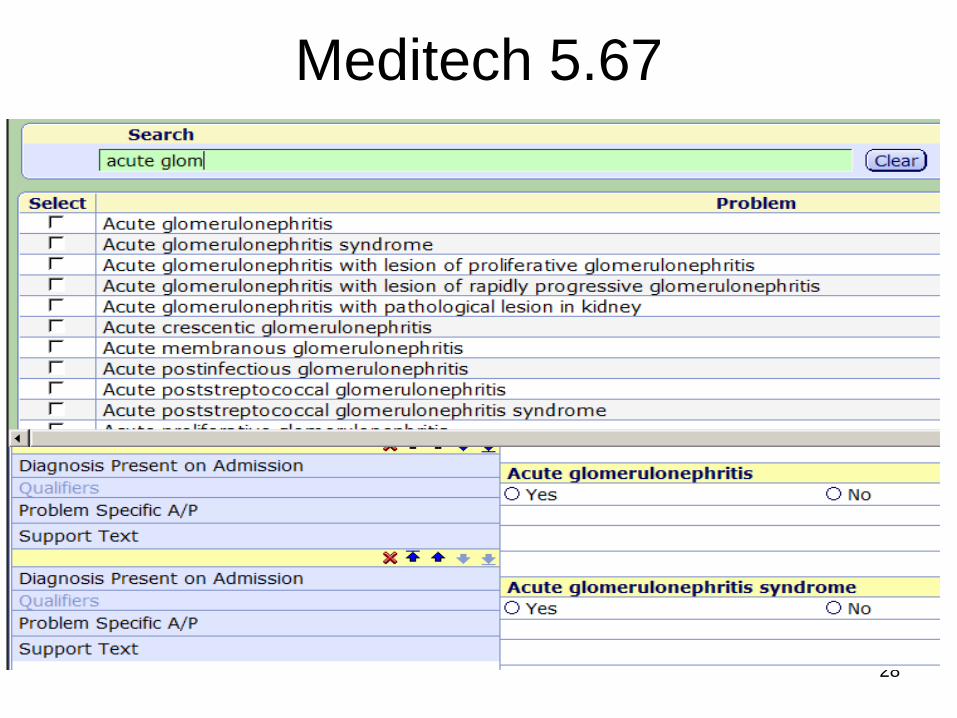
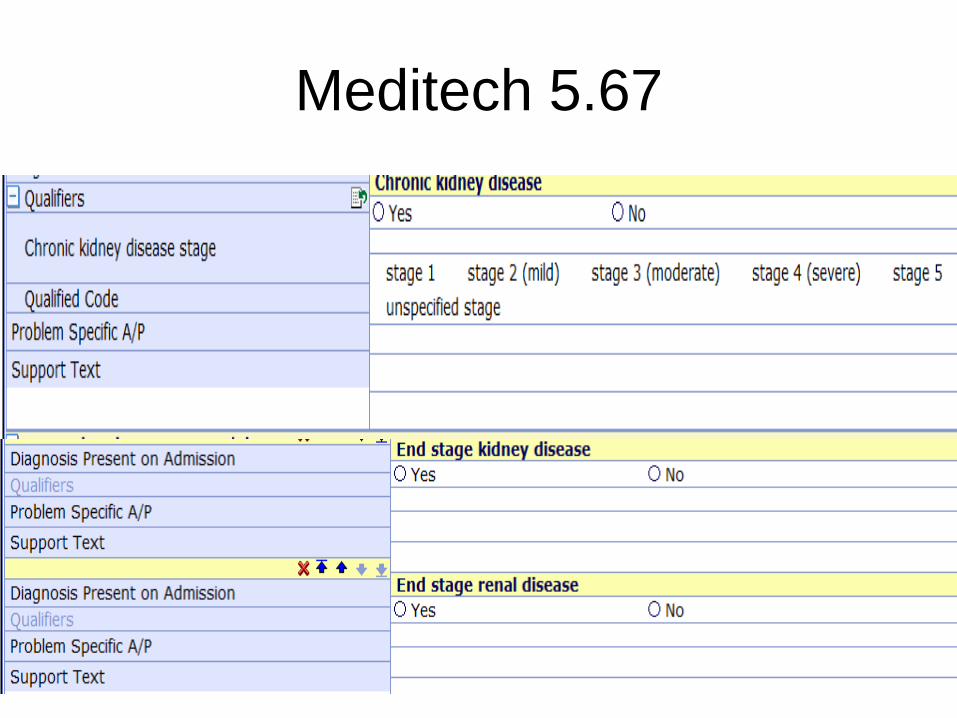
Meditech 5.67
18

Combination Codes
5920 Calculus of kidney N202 Calculus of kidney with
calculus of ureter
I10
combines 2
or more I9
codes
5921 Calculus of ureter N202 Calculus of kidney with
calculus of ureter
I10
combines 2
or more I9
codes
V420 Kidney replaced by transplant Z4822 Encounter for aftercare
following kidney transplant
I10
combines 2
or more I9
codes
V5844 Aftercare following organ
transplant Z4822
Encounter for aftercare
following kidney transplant
I10
combines 2
or more I9
codes
19

Codes with Placeholders
ICD9 ICD9 Title ICD10 ICD-10 Title
27402 Chronic gouty arthropathy without mention of
tophus (tophi)
M1A30X0 Chronic gout due to renal impairment, unspecified
site, without tophus (tophi)
M1A38X0 Chronic gout due to renal impairment, vertebrae,
without tophus (tophi)
M1A39X0 Chronic gout due to renal impairment, multiple
sites, without tophus (tophi)
27403 Chronic gouty arthropathy with tophus (tophi)
M1A30X1 Chronic gout due to renal impairment, unspecified
site, with tophus (tophi)
M1A38X1 Chronic gout due to renal impairment, vertebrae,
with tophus (tophi)
M1A39X1 Chronic gout due to renal impairment, multiple
sites, with tophus (tophi)
20

General Equivalence Mapping
http://www.stjhs.org/documents/ICD-10/2014-ICD-9-CM-to-ICD-10-CM-GEMS.pdf
This exercise will NOT capture new ICD-10 specificities
Validate all mappings using ICD-10 Index, Table, and Guidelines

General Equivalence Mapping
Combination Codes with Hematuria
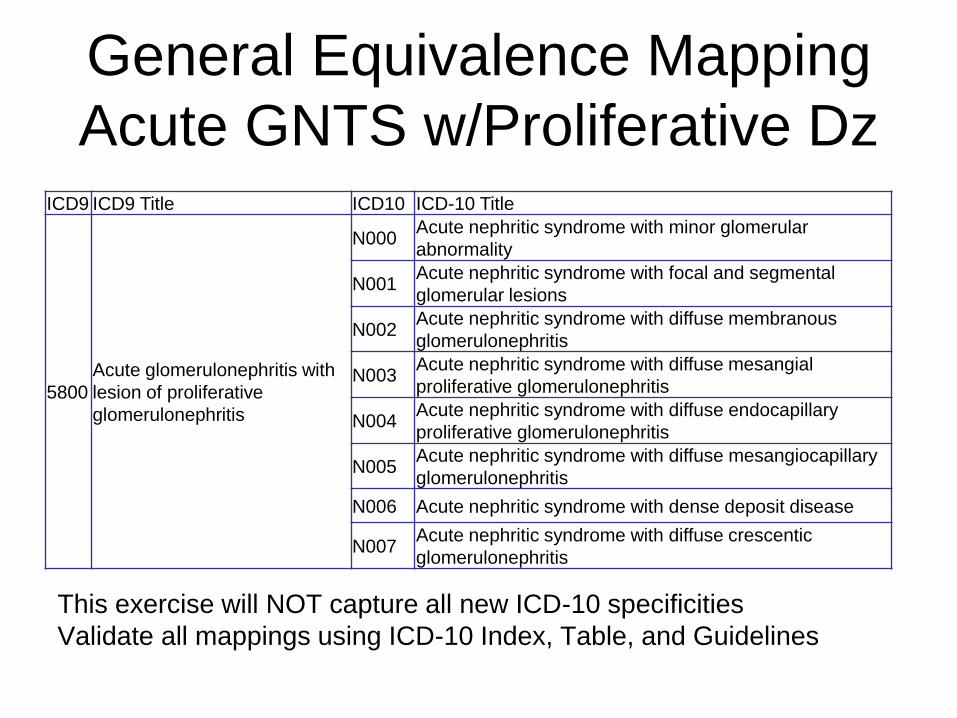
General Equivalence Mapping
Acute GNTS w/Proliferative Dz
This exercise will NOT capture all new ICD-10 specificities
Validate all mappings using ICD-10 Index, Table, and Guidelines
ICD9 ICD9 Title ICD10 ICD-10 Title
5800
Acute glomerulonephritis with
lesion of proliferative
glomerulonephritis
N000 Acute nephritic syndrome with minor glomerular
abnormality
N001 Acute nephritic syndrome with focal and segmental
glomerular lesions
N002 Acute nephritic syndrome with diffuse membranous
glomerulonephritis
N003 Acute nephritic syndrome with diffuse mesangial
proliferative glomerulonephritis
N004 Acute nephritic syndrome with diffuse endocapillary
proliferative glomerulonephritis
N005 Acute nephritic syndrome with diffuse mesangiocapillary
glomerulonephritis
N006 Acute nephritic syndrome with dense deposit disease
N007 Acute nephritic syndrome with diffuse crescentic
glomerulonephritis
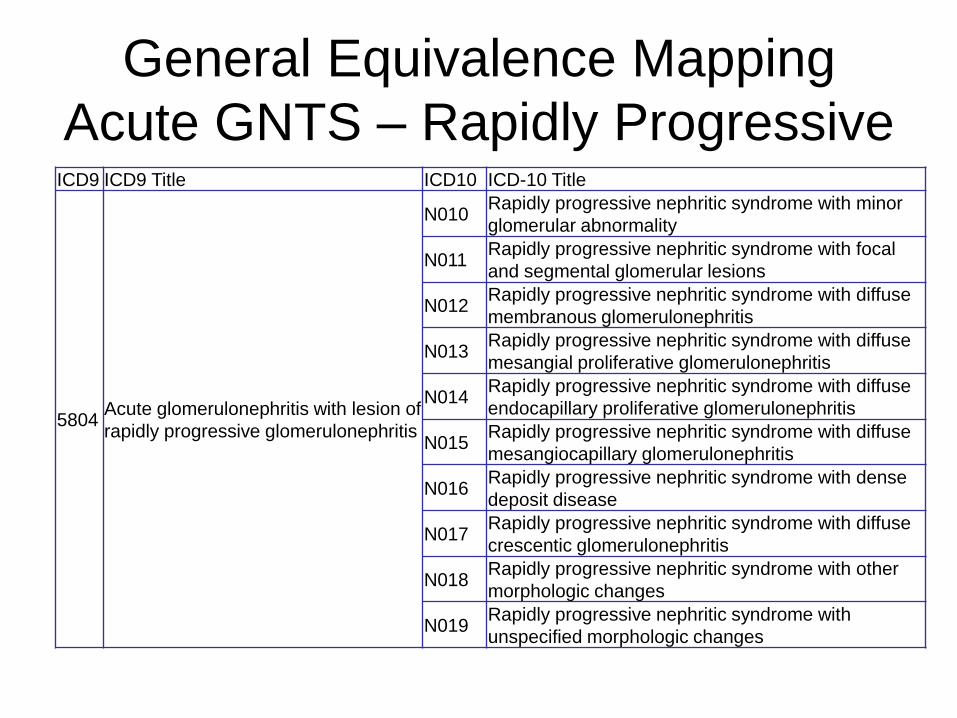
General Equivalence Mapping
Acute GNTS – Rapidly Progressive ICD9 ICD9 Title ICD10 ICD-10 Title
5804 Acute glomerulonephritis with lesion of
rapidly progressive glomerulonephritis
N010 Rapidly progressive nephritic syndrome with minor
glomerular abnormality
N011 Rapidly progressive nephritic syndrome with focal
and segmental glomerular lesions
N012 Rapidly progressive nephritic syndrome with diffuse
membranous glomerulonephritis
N013 Rapidly progressive nephritic syndrome with diffuse
mesangial proliferative glomerulonephritis
N014 Rapidly progressive nephritic syndrome with diffuse
endocapillary proliferative glomerulonephritis
N015 Rapidly progressive nephritic syndrome with diffuse
mesangiocapillary glomerulonephritis
N016 Rapidly progressive nephritic syndrome with dense
deposit disease
N017 Rapidly progressive nephritic syndrome with diffuse
crescentic glomerulonephritis
N018 Rapidly progressive nephritic syndrome with other
morphologic changes
N019 Rapidly progressive nephritic syndrome with
unspecified morphologic changes

Membranous GNTS
5810 Nephrotic syndrome with lesion of
membranous glomerulonephritis
N021 Recurrent and persistent hematuria with
focal and segmental glomerular lesions
N022 Recurrent and persistent hematuria with
diffuse membranous glomerulonephritis
N023
Recurrent and persistent hematuria with
diffuse mesangial proliferative
glomerulonephritis
N041 Nephrotic syndrome with focal and
segmental glomerular lesions
N042 Nephrotic syndrome with diffuse
membranous glomerulonephritis
25

Nephrotic Syndrome w/
Membranoproliferative GNTS
26

Chronic GNTS
• Emphasis
upon
pathology
27
Meditech 5.67
28

Acute Kidney Failure
Chronic Kidney Disease
29
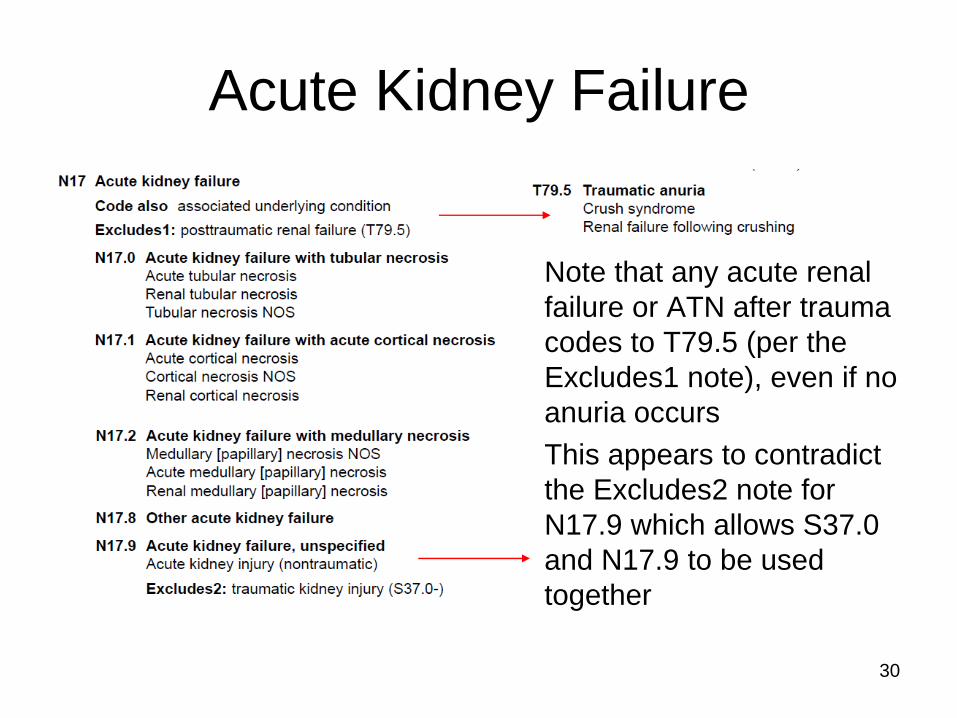
Acute Kidney Failure
Note that any acute renal
failure or ATN after trauma
codes to T79.5 (per the
Excludes1 note), even if no
anuria occurs
This appears to contradict
the Excludes2 note for
N17.9 which allows S37.0
and N17.9 to be used
together
30

Acute Kidney Injury in Meditech
5.67

Acute Kidney Insufficiency
Support Text
Main Term(s) Support Text
acute renal
insufficiency [elevated BUN/creatinine only] [qualifying as acute kidney injury]
azotemia [due to] [hypovolemia] [heart failure]
Elevated blood
urea nitrogen [acute tubular necrosis] [acute interstitial
nephritis] [chronic nephropathy]
High blood urea
nitrogen [shock] [urinary
obstruction] [other] Oliguria
Anuria
Low urine output
32

Acute Kidney Injury
2012 AKI Network
http://www.kdigo.org/clinical_practice_guidelines/pdf/KDIGO%20AKI%20Guideline.pdf
Published 2012
33
34
Acute Renal Failure (MCC)
vs. Azotemia/Insufficiency (not a CC)
• Many physicians document azotemia or
renal insufficiency (an elevation of the
BUN and creatinine) in settings of AKI or
ARF
– “Pre-renal” – due to renal hypoperfusion
– “Renal” – due to intrinsic renal disease
– “Post-renal” – due to renal outflow
obstruction.
Physician definition and documentation is mandatory
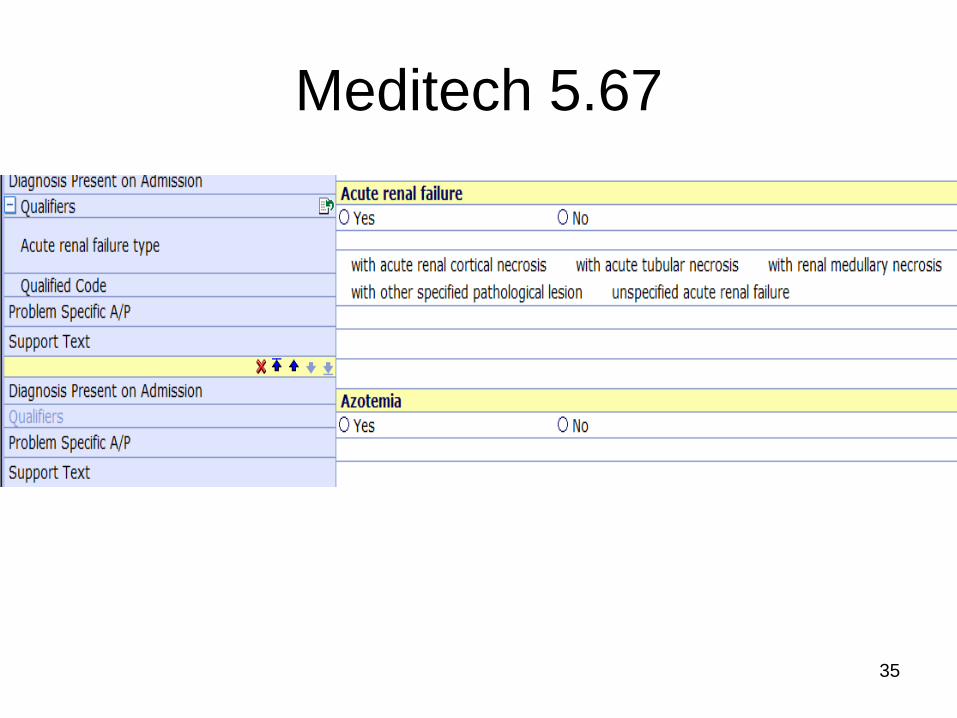
Meditech 5.67
35


Urine Microscopy
• Short of a kidney biopsy, urine
microscopy or prolonged AKI best
supports the diagnosis of ATN
http://www.tinyurl.com/ATNdiagnosis
37
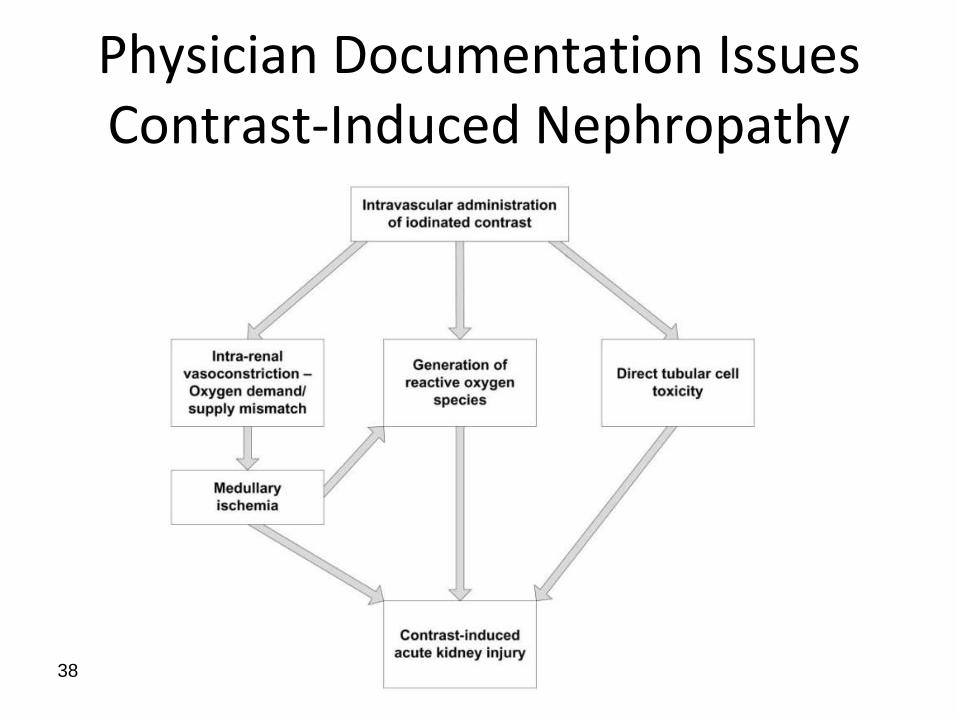
Physician Documentation Issues Contrast-Induced Nephropathy
38
39
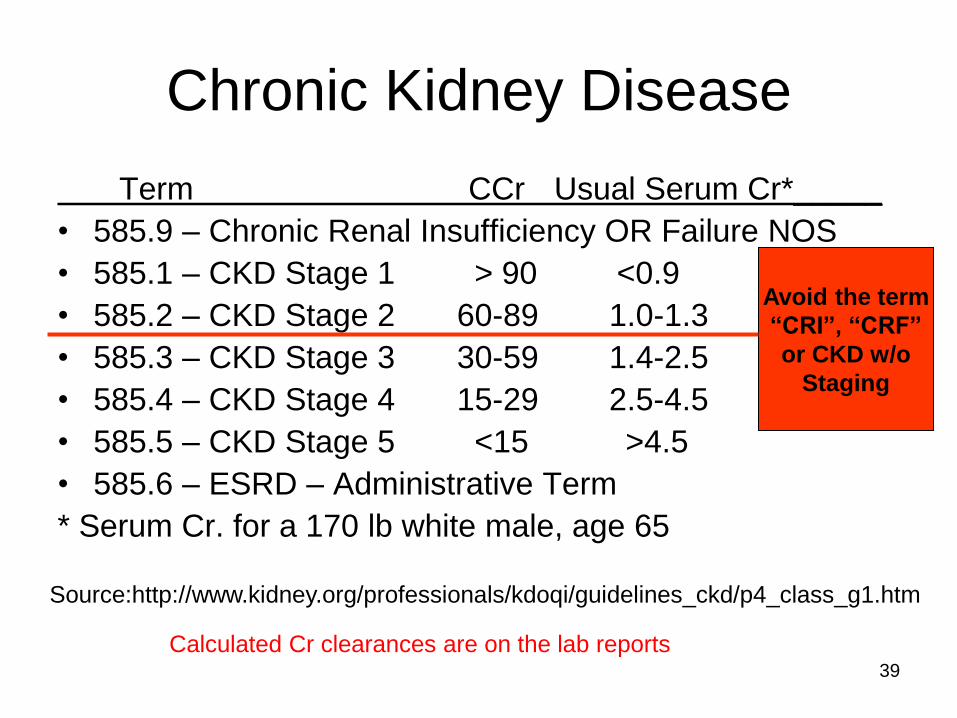
Chronic Kidney Disease
Term CCr Usual Serum Cr*_____
• 585.9 – Chronic Renal Insufficiency OR Failure NOS
• 585.1 – CKD Stage 1 > 90 <0.9
• 585.2 – CKD Stage 2 60-89 1.0-1.3
• 585.3 – CKD Stage 3 30-59 1.4-2.5
• 585.4 – CKD Stage 4 15-29 2.5-4.5
• 585.5 – CKD Stage 5 <15 >4.5
• 585.6 – ESRD – Administrative Term
* Serum Cr. for a 170 lb white male, age 65
Source:http://www.kidney.org/professionals/kdoqi/guidelines_ckd/p4_class_g1.htm
Avoid the term
“CRI”, “CRF”
or CKD w/o
Staging
Calculated Cr clearances are on the lab reports

Diagnoses
ICD-10-CM Official Guidelines
• An essential reference that must be read over and over and over again. Available for free at:
• http://www.tinyurl.com/2015ICD10CMguidelines

2015 ICD-10-CM Official Guidelines
Chronic Kidney Disease
• Hypertensive Chronic Kidney Disease – Assign codes from category I12, Hypertensive chronic kidney disease,
when both hypertension and a condition classifiable to category N18, Chronic kidney disease (CKD), are present. Unlike hypertension with heart disease, ICD-10-CM presumes a cause-and-effect relationship and classifies chronic kidney disease with hypertension as hypertensive chronic kidney disease.
• Chronic kidney disease and kidney transplant status – Patients who have undergone kidney transplant may still have some
form of chronic kidney disease (CKD) because the kidney transplant may not fully restore kidney function.
• Therefore, the presence of CKD alone does not constitute a transplant complication. Assign the appropriate N18 code for the patient‟s stage of CKD and code Z94.0, Kidney transplant status.
– If a transplant complication such as failure or rejection or other transplant complication is documented, see section I.C.19.g for information on coding complications of a kidney transplant.
• If the documentation is unclear as to whether the patient has a complication of the transplant, query the provider.
Meditech 5.67
42
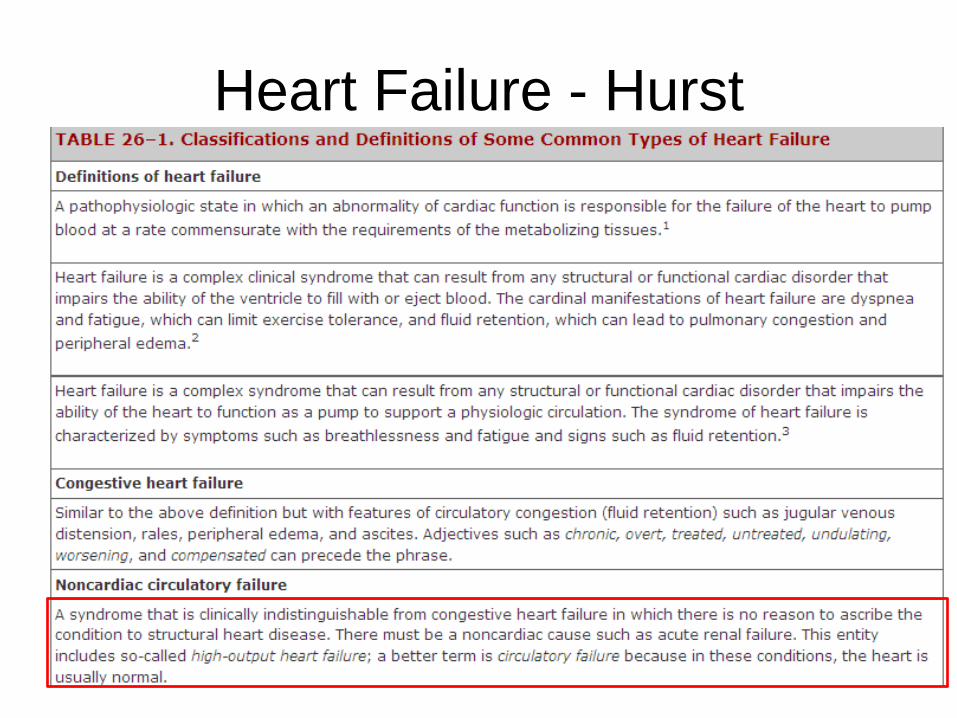
Heart Failure - Hurst
43

Fluid Overload due to
Dialysis Noncompliance • The Coding Clinic Second Quarter 2001 advised to assign code 428.0,
Congestive heart failure, as the principal diagnosis for a patient admitted in
congestive heart failure (CHF) due to fluid overload and noncompliance with
dialysis treatment.
• More recent advice recommended the assignment of code 276.6, Fluid
overload, as principal diagnosis for a patient admitted in fluid overload due
to missed dialysis treatments because the patient had no history or
evidence of CHF.
• At our facility, we had a case where a patient with end stage renal disease
was admitted for treatment of fluid overload due to dialysis noncompliance.
This patient had a history of congestive heart failure. However, the
provider documented, "The patient was successfully dialyzed and had
no evidence of cardiac or pulmonary decompensation other than that
of fluid overload due to dialysis and dietary noncompliance." How
would this case be coded?
Source: Coding Clinic for ICD-9-CM, 3rd Quarter 2007, page 11
Answer
• Assign code 276.6, Fluid overload, as the principal diagnosis. Codes
428.0, Congestive heart failure, unspecified; 585.6, End stage renal
disease; V45.1, Renal dialysis status; and V15.81, Noncompliance
with medical treatment, should be assigned as additional diagnoses.
Assign code 39.95, Hemodialysis, for the dialysis.
• In this case, fluid overload is reported as principal diagnosis since the
provider indicated that the fluid overload was noncardiogenic in
nature and the congestive heart failure was not decompensated. The
provider has clearly addressed the distinction between fluid overload
and CHF in his or her documentation.
Consequently, coders must know if fluid
overload is cardiogenic or noncardiogenic if
the patient has chronic CHF
46
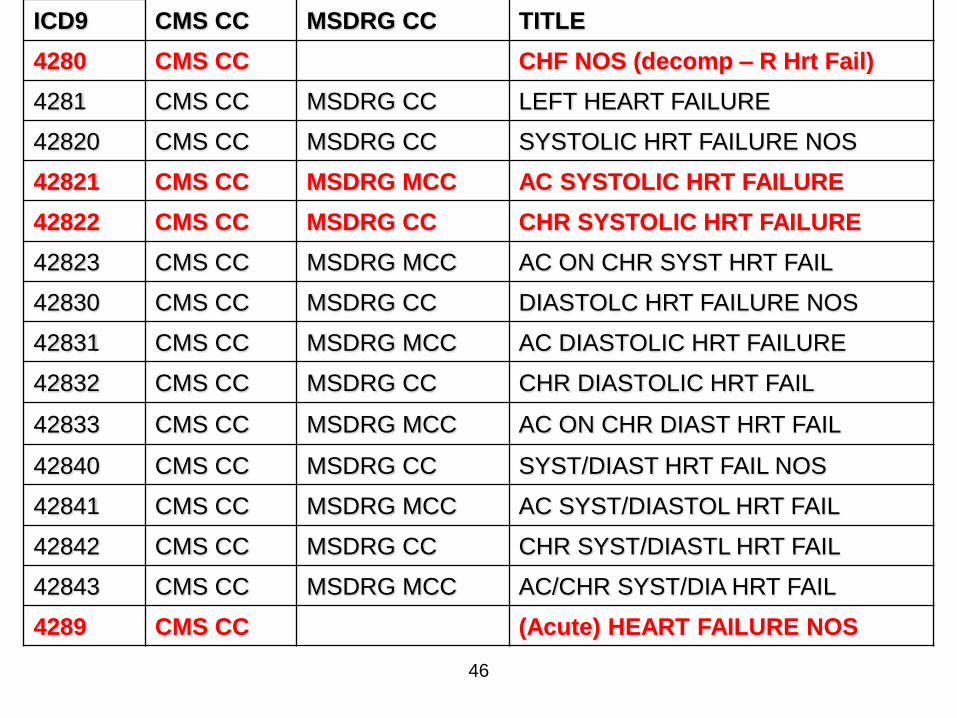
ICD9 CMS CC MSDRG CC TITLE
4280 CMS CC CHF NOS (decomp – R Hrt Fail)
4281 CMS CC MSDRG CC LEFT HEART FAILURE
42820 CMS CC MSDRG CC SYSTOLIC HRT FAILURE NOS
42821 CMS CC MSDRG MCC AC SYSTOLIC HRT FAILURE
42822 CMS CC MSDRG CC CHR SYSTOLIC HRT FAILURE
42823 CMS CC MSDRG MCC AC ON CHR SYST HRT FAIL
42830 CMS CC MSDRG CC DIASTOLC HRT FAILURE NOS
42831 CMS CC MSDRG MCC AC DIASTOLIC HRT FAILURE
42832 CMS CC MSDRG CC CHR DIASTOLIC HRT FAIL
42833 CMS CC MSDRG MCC AC ON CHR DIAST HRT FAIL
42840 CMS CC MSDRG CC SYST/DIAST HRT FAIL NOS
42841 CMS CC MSDRG MCC AC SYST/DIASTOL HRT FAIL
42842 CMS CC MSDRG CC CHR SYST/DIASTL HRT FAIL
42843 CMS CC MSDRG MCC AC/CHR SYST/DIA HRT FAIL
4289 CMS CC (Acute) HEART FAILURE NOS
47
Systolic - Diastolic
Cardiomyopathies • Systolic
– EF usually <40%
– “Dilated” Heart
• Diastolic
– EF usually >40%
– Hypertrophic heart
– HF with preserved systolic function is not coded as diastolic heart failure
• Most patients have both at one time or another
– OK to say “probable systolic-diastolic failure
• Dysfunction ≠ Failure
• Decompensated Systolic or Diastolic CHF can be coded as “Acutely decompensated”
– Does not apply to decompensated CHF not stated as systolic or diastolic
• State the cardiomyopathy
– Hypertensive
– Diabetic
– Alcoholic
– Toxic
– If ischemic, please also state if the others are present

Heart Failure in Meditech 5.67
Altered Mental Status
49

ICD-9-CM and Physician – Pertinent
Disease Categorizations – MUSIC Manifestation
– Nonspecific – Altered Mental Status; Altered Level of Consciousness
– More specific – Delirium, Dementia, Psychosis Stupor, Coma
Underlying Cause – Encephalopathies – Global Brain Dysfunction – (e.g. hypertensive, hepatic)
– Structural Brain Diseases – Neoplasms, Hydrocephalus, Cerebral Laceration
– Ischemic Disease – Transient Ischemic Attack vs. Stroke vs. Late Effect
– Neurodegenerative Disorders – Alzheimer's Disease, Pick‟s Disease
Specificity or Severity – Acute, chronic, or acute on chronic decompensation
Instigating or Precipitating Causes – Acute reasons why the underlying cause or stable conditions get worse
– Includes drug overdoses, head trauma,
Consequences – Acute (on chronic) respiratory failure, Syndrome of Inappropriate Anti-diuretic
Hormone, Rhabdomyolysis, Neurogenic Bladder with incontinence, Aphasia.
Once one element is considered, look for the other four; Linking adds synergy in risk adjustment. Ex: Acute Delirium due to toxic encephalopathy due to levofloxacin given in therapeutic doses resulting in urine incontinence requiring foley catheterization.
17
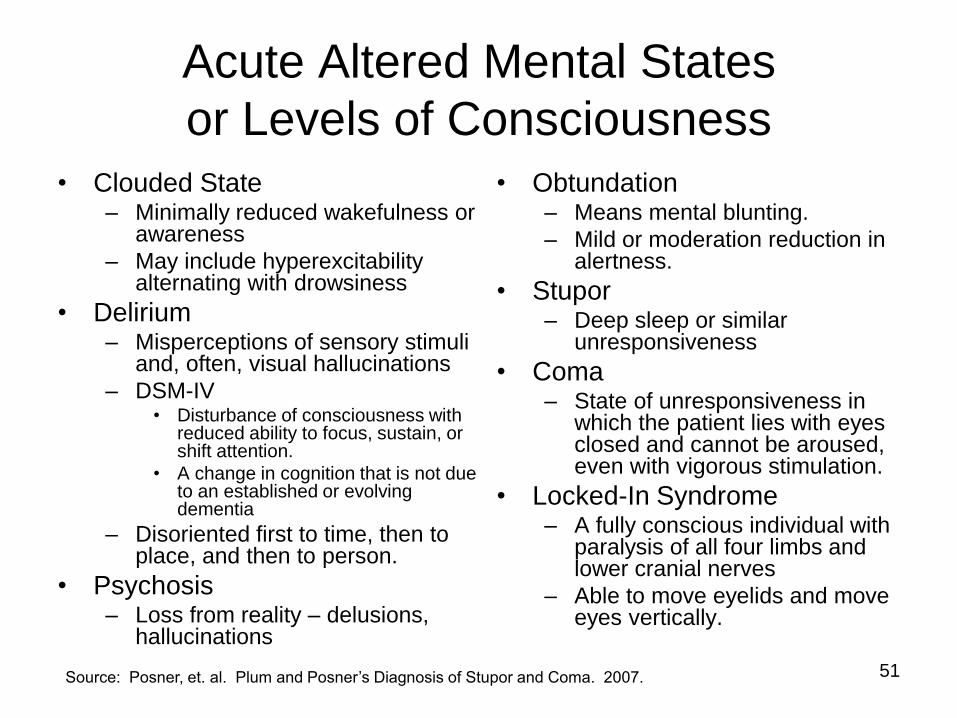
Acute Altered Mental States
or Levels of Consciousness
• Clouded State – Minimally reduced wakefulness or
awareness
– May include hyperexcitability alternating with drowsiness
• Delirium – Misperceptions of sensory stimuli
and, often, visual hallucinations
– DSM-IV • Disturbance of consciousness with
reduced ability to focus, sustain, or shift attention.
• A change in cognition that is not due to an established or evolving dementia
– Disoriented first to time, then to place, and then to person.
• Psychosis – Loss from reality – delusions,
hallucinations
• Obtundation – Means mental blunting.
– Mild or moderation reduction in alertness.
• Stupor – Deep sleep or similar
unresponsiveness
• Coma – State of unresponsiveness in
which the patient lies with eyes closed and cannot be aroused, even with vigorous stimulation.
• Locked-In Syndrome – A fully conscious individual with
paralysis of all four limbs and lower cranial nerves
– Able to move eyelids and move eyes vertically.
51 Source: Posner, et. al. Plum and Posner‟s Diagnosis of Stupor and Coma. 2007.

Underlying Causes
Encephalopathy
• No universal definition of the term.
• NIH Definition: – Encephalopathy is a term for any diffuse disease of
the brain that alters brain function or structure. Encephalopathy may be caused by infectious agent (bacteria, virus, or prion), metabolic or mitochondrial dysfunction, brain tumor or increased pressure in the skull, prolonged exposure to toxic elements (including solvents, drugs, radiation, paints, industrial chemicals, and certain metals), chronic progressive trauma, poor nutrition, or lack of oxygen or blood flow to the brain. The hallmark of encephalopathy is an altered mental state.
Available at: http://tinyurl.com/encephalopathy
52

Physician Literature
http://www.tinyurl.com/TMEncephalopathy
53
Toxic/Metabolic Encephalopathies
Definitions • Toxic and metabolic
encephalopathies are a group of neurological disorders characterized by an altered mental status – That is, a delirium, defined as a
disturbance of consciousness characterized by a reduced ability to focus, sustain, or shift attention
• that cannot be accounted for by preexisting or evolving dementia and that is caused by the direct physiological consequences of a general medical condition.
MS-DRG MCC
APR-DRG
– SOI – 3 of 4
– ROM – 3 of
4
HCC
– No relative
weight
54
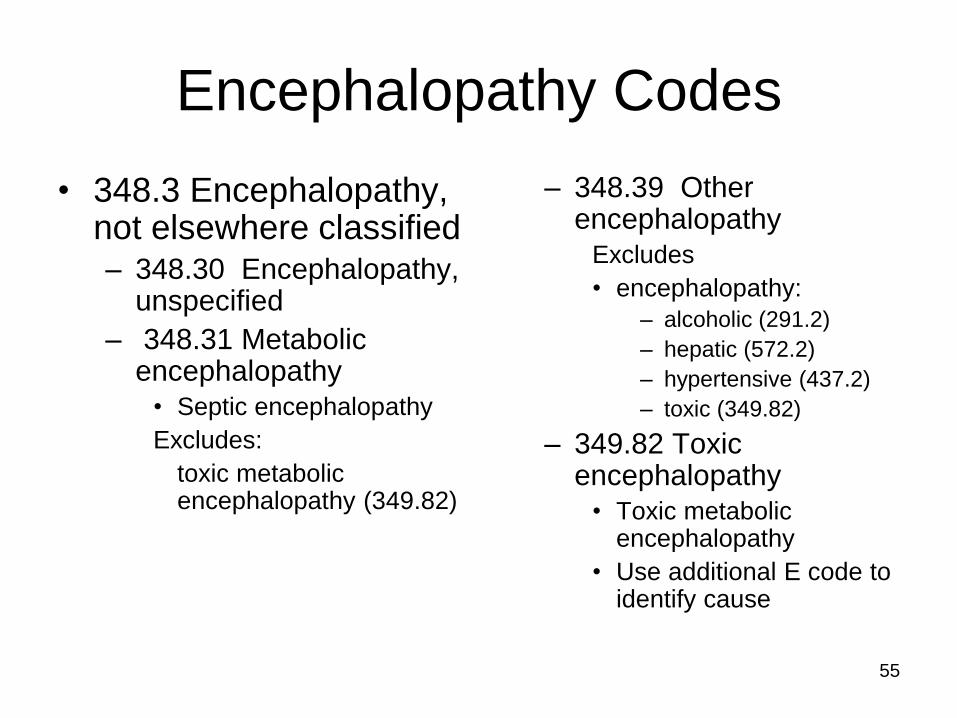
Encephalopathy Codes
• 348.3 Encephalopathy, not elsewhere classified – 348.30 Encephalopathy,
unspecified
– 348.31 Metabolic encephalopathy
• Septic encephalopathy
Excludes:
toxic metabolic encephalopathy (349.82)
– 348.39 Other encephalopathy
Excludes
• encephalopathy:
– alcoholic (291.2)
– hepatic (572.2)
– hypertensive (437.2)
– toxic (349.82)
– 349.82 Toxic encephalopathy
• Toxic metabolic encephalopathy
• Use additional E code to identify cause
55

Thank You
Questions?