the future of clinical microchemical analysis
TRANSCRIPT

The Future
of Clinical
Microchemical
Analysis D A V I D GLICK, (Department o f Physiological Chemistry
University of AAintmsota Medical School
X F CLINICAL chemistry could be dealt with in the least empirical manner, and by the purest of purely academic; approaches, its evolution would fol low the successive developments of cell, tissue, organ, and body chemistry. But the pressure of human need reverses the order. The physician in direct contact ' wi th the sick is concerned first with maintaining the patient as a whole i n the best possible condition. To achieve this e n d he must direct his attention next, in s o far as present limitations permit, to the organ, then to the tissue, and finally to t h e cell. This phrase, in so far as present limitations permit, touches the critical aspect of the matter, and leads us to the thesis of this discussion.
Current medical practice has b e e n able to draw on cell chemistry hardly at all , on tissue chemistry but little more, on organ chemistry a mere beginning, but on body fluid and excretion analysis extensively. This is chiefly the result of the easy availability of the fluids and excrement, and the associated extensive development of
methods and apparatus to deal with these materials in convenient amounts. The value of such analyses is not to be minimized, but in many instances the composition of body fluids and excretion products reflect only poorly the changes to be determined in an organ or tissue for clinical purposes. While it would be better in these cases to obtain samples of the organ or tissue in question directly for analysis, this has not been followed extensively because of the danger to the patient, or the difficulty inherent in obtaining the sample itself.
However, the danger and the difficulty are factors that can be overcome by technical refiniements. Methods have been developed for taking very small biopsies of
tissues in a relatively harmless fashion; of course the smaller the biopsy the less the harm. But most often the limiting factor is the availability in clinical laboratories of methods and techniques for dealing with samples considered very small by 'prevailing standards.
It isn't that we don't know of micro methods that are capable of dealing with quantitative analysis of amounts of tissue small enough to permit histological and even cytological definition. Even in the present primitive state of quantitative histo- and cytochemistry, it is possible to determine sodium, potassium, calcium, phosphorus, nitrogen, chloride, sulfur, various carbohydrates, lipids, proteins, urea, respiratory exchanges, and a number of enzymes and vitamins. It is inevitable that these methods, and new ones, will «be adopted by clinical chemists.
Move Toward Cell Analysis
T h e expansion of clinical chemistry from body fluid and excretion analysis to tissue and cell analysis will elevate its position of usefulness in medical practice, and do its part in bringing the graduate clinical chemist .to a status of something more than a laboratory technician, which is still his role too often.
A n extrapolation into the future of clinical chemistry leads to the greater adoption of rnicroanalytical methods, not
V O L U M E 3 1 , N O . 2 » » J A N U A R Y 1 2 , 1 9 5 3 139
New Text
New Text

Fig. 1. Microscope colorina-eter assembly. ( A ) Mi croscope illuminator, (B ) lens system to give narrow beam of parallel rays, (C ) right-angle prism reflector, ( D ) microscope condenser with top half removed t o reduce convergence, ( E ) objective ( 5 X ) , ( F ) micro-photographic adapter, ( G ) photocell, ( H ) adjustable support [from Malmstrom and Glick ( 3 ) ]
Ifëcaiïsè& these - arèr; requi'Çéti* to .·extehcl .thejfsco^ë/ofl^tÎiè Λγξτ kjto °. tissues .<> and cells^ /Djjt^?also" 'because trie .micro methods are
.Goncerning^t^^last^ppint, -"wje c a n ex— pect^ffia^tn^^ »ό&trie fu— ture · \vill^coriduct$-o routinely,i comple te sets ot blood, cnemistryc'anaiysis'on smgie drops of blood—an advance, already begun in a few laboratories, that will greatly augment the value of clinical chemistry fox infant and other patients from whom it Ls difBcult to ge t the quantities or blood now commonly employed for analysis.
Methodology is Limiting Factor It is not the intention here to extra
polate s o far into the future of c l in ical microchemistry that we get into an H. Gr. Wells fantasy or a "Brave N e w Wor ld ." Rather let us shift our attention from present practice to the horizon still within oixr line of sight. It is not for lack o f concepts and vision that our picture w i l l b e limited; imagination and thought r u n far ahead of t h e presently attainable reality. Our l imiting factor most often w i l l h e methodology, the instrumentation, ancl technique t o draw the horizon to t h e i m mediate, l ike a telescope, a n d bring t h e distant to t h e uses of daily need.
W h o l e fields of science have s t e m m e d from t h e invention and exploitation of a single instrument. Think for a m o m e n t what has come from the microscope. Arid as in t h e past, future great developments wil l also follow methodology. Therefore, on this voyage of extrapolation, w e mirst be drawn b y the currents of methodology. Le t us see where they take u s .
In t h e present consideration we wish "to deal with clinical micro methods o f even
greater refinement than those ingeniously deve loped in such laboratories as those of Sobel and Natelson. In dealing with this matter words like "ultramicro" or "sub-ιτΊαοτο,,> methods, will not be employed b e cause these terms are poor indeed. Certain m e t h o d s that toda} are called "ultra-" or "submicro" in some quarters may be re fined 100O times within a few years. Sxiould we then call the newer methods "iiltra-tiltramicro" or "sub-ultramicro"? Wouldn't it be better to be more explicit and use the terms milligram method, microgram method, and millimicrogram risethod to designate methods for the analysis of milligram, microgram, or millimicrogram quantities? Parenthetically, it could b e added that the invention of addit ional symbols such as y for microgram, a n d λ for microliter are to be deplored w h e n they are not needed and are ac tually less descriptive than the logical standard terms, jug. and μ\.
But let ns steer to the main considerat ion . The chief analytical techniques n o w employed in clinical chemistry laboratories ajre titrimetry, gasimetry, and colorimetry. TTitrimetry, convenient enough for comm o n use, has already been brought close t o the limit of refinement. The burets a n d their modifications developed b y Linderstr0m-Lang and Holter, Scholander, Oi lmont , and others have scale divisions equivalent to O.lyul. ( 3 ) . The buret d e v e l o p e d b y Benedetti-Pichler and c o workers using a micro manipulator with a Txioist chamber on the stage of a microscope was designed for use with volumes o f 0.O5-0.50 ,al. ( θ ) .
Gasimetry has been reduced to the scale where, in instruments such as the Cartesian diver, the total gas volume of •the reaction vessel is as little as 0.1 μλ. %vith a sensitivity of 2 χ 10"° μΐ. (3).
While instruments of this type are roosrt useful in certain researches, they are not convenient enough for routine use in clinical laboratories. Analysis of the blood gases in one drop of "blood has been described by Scholander and Houghton ( θ ) , and more recently by Natelson ( 7 ) , witL· equipment readily adaptable to routine clinical use.
Colorimetry is especially amenable t o clinical chemistry usage, and because o f its great analytical versatility, t h e possibilities of its adaptation t o microchemï-cal work wil l b e discussed in detail. The microcuvette of Lowry and Bessey, fox use with the Beckman spectrophotometex, permits absorption measurements with a 1 cm. light path on volumes of liquid a s little as 50 μ\. ( 3 ) . A further refinement of 10 times is obtained with the microscope colorimeter shown in Fig. 1. This is a modification ( 6 ) of the instrument designed b y Holter and co-workers ( 4 , 5 ) . The cuvette is a glass or plastic capillary tube ( 5 to 15 mm. long with a bore o f 0.5 to 1.5 mm. diameter ) sealed to a microscope slide with a bit of stopcock grease and covered with a niicroscorje
Fig. 2. T w e l v e capillary cuvettes, topped with a glass cover slip, mounted on a m i croscope slide in position for measurement on the stage of the microscope colorimeter
cover glass, Fig. 2. The volumes of liquid used usually range from 5 to ΙΟ μ\. T h e light beam, made monochromatic with an interference filter or a monochromator^ is converted to a parallel beam with a diameter of 0 .2 to 0.4 mm., and it is passed through the center of t h e cuvette to the low power microscope which transmits it to the photocell over the ocular.
T h e observation eyepiece and mechanical stage facilitate the rapid centering of the light beam in the cuvette. Since -the cuvettes are quite inexpensive and easily cleaned, m a n y can h e used simultaneously
C H E M I C A L A N D E N G I N E E R I N G NENX/S 140

to hasten the work. I n Fig. 2, 12 are arranged on a single microscope slide. The cost of the Lowry-Bessey cuvette is about $20. T h e capillary cuvettes cost 50 cents or less.
In order t o extend t h e usefulness of the microscope colorimeter we have converted it into an ultraviolet, visible, and near infrared spectrophotometer and the same instrument is also arranged to b e a fluorimeter. This versatile apparatus, Fig. 3, should serve to make possible a wide variety of analyses of biochemically important constituents in samples of tissue no larger than microtome sections, or fluid samples of a fraction of a drop, with the same degree of accuracy as obtained in the macro procedures. Some of the ancillary equipment employed is illustrated in Figs. 4 and 5.
Emission Spectroscopy for Na-and Κ Flame photometry has established its
value for routine sodium and potassium detenuinations on very small samples of serum. But it will probably be displaced in the future b y emission spectroscopy. The latter holds the unique advantage that a variety of elements can be determined simultaneously on the same small blood sample or tissue biopsy. Recent instru-0
mental improvements and more compacte and convenient equipment are «rapidly* bringing this analytical metKocl to m e . position of practicality for clinical laboratories. The demonstration by, Vallée a'ncL Peattie (8) that spectral lines can be .intensified by surrounding the arc 'witl·^ an^
inert gas such as helium is an important step toward the day when i t will be commonplace to run routine analyses for sodium, potassium, calGium, arid magnesium on the same single drop of serum or bit of tissue which will b e the usual sample.
Less immediately applicable, but already nudging their way to a position of consideration are mass spectrometry and radioactivity analysis. With, reference to the latter, the measurement of Vs1 in connection with thyroid function tests is already a routine matter in some laboratories. Induction of radioactivity for analytical purposes by subjecting biological samples to pile bombardment is now in an experimental stage, and this could become an important method for elementary analysis a t the histological and cytological level. It is not hard to imagine the future establishment of centers to which samples are sent daily for activation analysis by this method.
A technique-of analysis thatkis now being employed in several biochemical research laboratories, and in industry, and one that holds especially intriguing possibilities for quantitative analysis on intact tissues and cells, is x-ray absorption analysis. The principle of 'this technique is
3 *· baseffiofTfrthe absoxpiibn of x-rays of spe-r.yrcïËh< ^S£e 'lejig&hs b y eaUh element. A ' :ipJofo O£ ^Y|ge lërrgÊrï a'gâirTst âbgolptiofi
rgJ2&e§ a ois^nJifXuiiu's ciiw.e as shown in J$& (6: ÎÎhe pjpicylar wave length OVkby) at-wj^sh the absorption j u m p oc-cxjTS^çlia^^cMrizes the ëlërnent. The height
,._*$? Wgi-Jjumpj. ;d^tëi.minieii by âbXorjpiiOn
Fig. 3 . Microscope spectrophotometer-fl^orjmeier|^ with quartz condensing lenses, ( B ) aluminunVfirsYsurf^^^jl^lorS!^^^Illr^^r|g<(rWl^ê) with aligned pin-holes at each end, ( D ) light-tight Housing ccnta ir i in^^ecfernc^l r ^^^ with external control knobs for centering capillary cuvettes with quartz^co^er SHD£ on quartz microscope slide, ( E ) observation eyepiece to aid positioning of cuvette: to place lumen in optical axis, ( F ) replaceable photoelectric unit for absorption measurements sensitive in visible or ultraviolet region depending on requirement, ( G ) photoelectric unit for fluorescence measurements sensitive in visible region, ( H ) amplifier-galvanometer unit for measuring photoeurrent
measurement at waveienguis «*L ea .̂1.1 cugc of die jump (λι and ·λ2), measures the quantity of. the element. Thus identification and quantitation of elements a r e possible in solution in a cuvette, or in situ in the tissue and cell.
Recording of the transmitted x-radiation can be made by photography, Geiger counter, or ionization chamber when samples are in solution in cuvettes. For cells, fibers, or tissue sections photographic recording on fine-grained film is used, Fig. 7. The resolution is about 1μ, and for quantitative work by densitometry of the images on the film the resolution i s about 2 to 3M. Tissue sections 2 to IS/M thick can be used for analysis of nitrogen, carbon, oxygen, phosphorus, and sulfur. Mineral salts in bone sections can also be determined. When cuvettes are employed, volumes of liquid as small as 0.2 μ\. can be used. A feature of the technique is the fact that the sample is not used urp in the analysis so that the same sample can be subjected to repeated analysis for different elements and is still availafcle for morphologic or other studies at t h e end.
The exploitation of x-ray absorption for bjp^chemi calΛ a°nal§ps has derived chiefly from the wffrk oTi^g^r|)_m at the Institute fpr Oeîl· ifegaiféh in giS^ièlrn. I n addition to elkffîëiit&sy iân^^Sii^i)). Engstrôm has emgl£^à ; p r ^ a ^ Ç ^ ^ ^ ( ^ * ^ r the de^er^Mâfâon o£ çfi|f # ^ ^ t e ^ c e l l s and cell parts (ψ). i H t . ^^P^Kpfe '4^Po r n" phshed by using a ^ o ^ ^ ^ ^ g ^ i Q j ^ i n o of soifc x-rays hay;ing ^ p % ^ | n j ^ y ^ r i t ^ e b region of 8A. ftïése Éa^J^^^^M^^Xg,; ab-SjCirbeid b;y the ehM? ^ïjeffijnisyof* Hissue, n a m ^ ^caji^^. p f t ^^K^^3^? | y^ n
i l ^ ^ ^ g e g J ^ | | ^ K ' 1 i j ^ ^ ^ ^ ^ p @ 0 a ? cal-^ ^ & : ^ ^ e - ^ i e W : / ® f e c ^ f p r i t ) . 3fti© S r É ^ f f l ^ ® | i ^ ^ ^ & S ) M ^ ^ i i t s · that oc^ur is- .soffe (Eisin^, i|uisRya"sjj^^phorus, 5\πίΰϊ ; · ,^^^βΜΛςΜΜ^?^^*Ρ 0 "small to
olvent Removal of Lipids from Tissue Measurement of dry weight of tissue
onstituents down to 2 to 3M in size is in :self of limited value, although i t is very seful as a basis of reference for analyses f biochemical substances and as a n index f certain secretory and other cell func-ions. However, more extensive jpossibili-ies exist. The determination of total ciass, before and after treatments designed D remove specific substances, makes vailable analytical methods fox many onstituents. Thus, treatment with selected olvents can be used for the removal, and herefore the analysis, of particular lipids, r specific enzymes can be employed to eniove certain substances for similar ana-ytical purposes.
Other micro techniques already avail-ble will find their way into clinical labor atories. Without attempting to discuss nore of them, we should just mention iaper chromatography. By means of the microscope spectrophotometer artd fluor-meter previously described, quantitative nalysis of the separated spots o£ biolog-2al substances can now be performed in nany new instances.
New Text
New Text
New Text
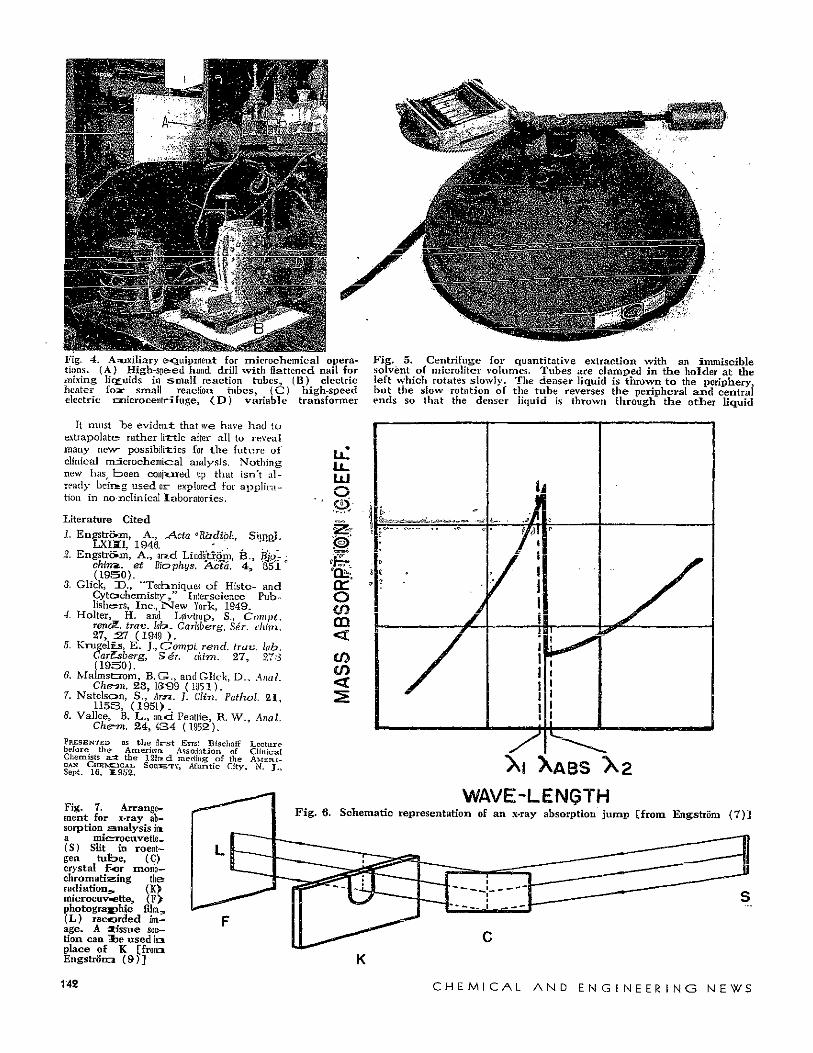
Fig. 4. Auxiliary equipment for microchemical opera- Fig. 5. Centrifuge for quantitative extraction with an immiscible tions. (A) High-sp&ed hand drill with flattened nail for solvent of microliter volumes. Tubes are clamped in the holder at the mixing lic£uids in small reaction tubes^ (B) electric left which rotates slowly. The denser liquid is thrown to the periphery, heater fosr small reaction tubes, (^j) high-speed but the slow rotation of the tube reverses the peripheral and central electric onicrocentrifuge, ( D ) variable transformer ends so that the denser liquid is thrown through the other liquid
It must "be evident: that we have had to extrapolate? rather little after all to reveal many new- possibilities for the future oi clinical mdcrochemical analysis. Nothing new hasp b e e n conjured up that isn't already heir» g used or- explored for application in nonclinical laboratories.
Literature Cited 1. EngstrcVm, Α., J^cta ° Radial·., Sirppi.
LXISI, 1946. · ;. . 2. EngstrcVm, Α., arid Liiidstxôrn, B. , B^- ;
chin*,, et Biophys, 7\cta. 4 , 351 ° ( 1 9 5 0 ) .
3. Glick, D . , "Techniques of Histo- and Cytochemistry / ' Interscience Publishers, Inc., N e w York, 1949.
4. Holter, H. and L0vtrup, S., Compt. rencZ. trav. lab. Carhberg, Sér. cliim. 27, :27 (1949 ) .
5. Krugel£s, E . J., Compt, rend. trav. lab. CarZsberg, Sér. aim. 27 , 27:3 ( 1 9 3 0 ) .
6. Malmsfcrom, B .G. , and Glick, D. , Anal Cherrn. 2 3 , 1(>"99 (1951).
7. Natelson, S., km. } . Clin. Pathol. 21 , 1153 , ( 1 9 5 1 ) .
8. Vallée, Β. L., and Peattie, R. W., Anal. Chew. 2 4 , 4 3 4 (1952).
PBJSSENTED as the flr-st Ernst Bischoff Lecture before the- Americnr*. Association of Clinical Chemists a=t the 122i*d meeting of the A M E R I CAN CHEMCICAL SOCIETY, Atlantic City. Ν. Τ Sept. 16, Ï.9S2.
Fig. 7. Arrangement for x-ray absorption analysis in. a micsrocuvette-(S) Slit in roentgen tufoe, (C> crystal For moiio-chromatizing the radiation.* (K) microcuv«ette, ( F > photographic film, (L) recorded image. A *issue section can Ibe used i n place of Κ [frona Engstrorm ( 9 ) ]
Lu Ο
a: ο en m <
<
WAVE-LENÇTH Fig. 6. Schematic representation of an x-ray absorption jump [from Engstrôm (7)3
142 C H E M I C A L A N D E N G I N E E R I N G N E W S