the following list includes common outcome measures which ... · inventory (cahai) function icf...
TRANSCRIPT
1
The following list includes common outcome measures which may be used for initial assessment and reassessment(s) post intervention with patients/residents who have increased tone.
Outcome Measures for Spasticity Management
Measure Type Information + website link FLACC (Face, Legs, Arms, Cry, Consolability)
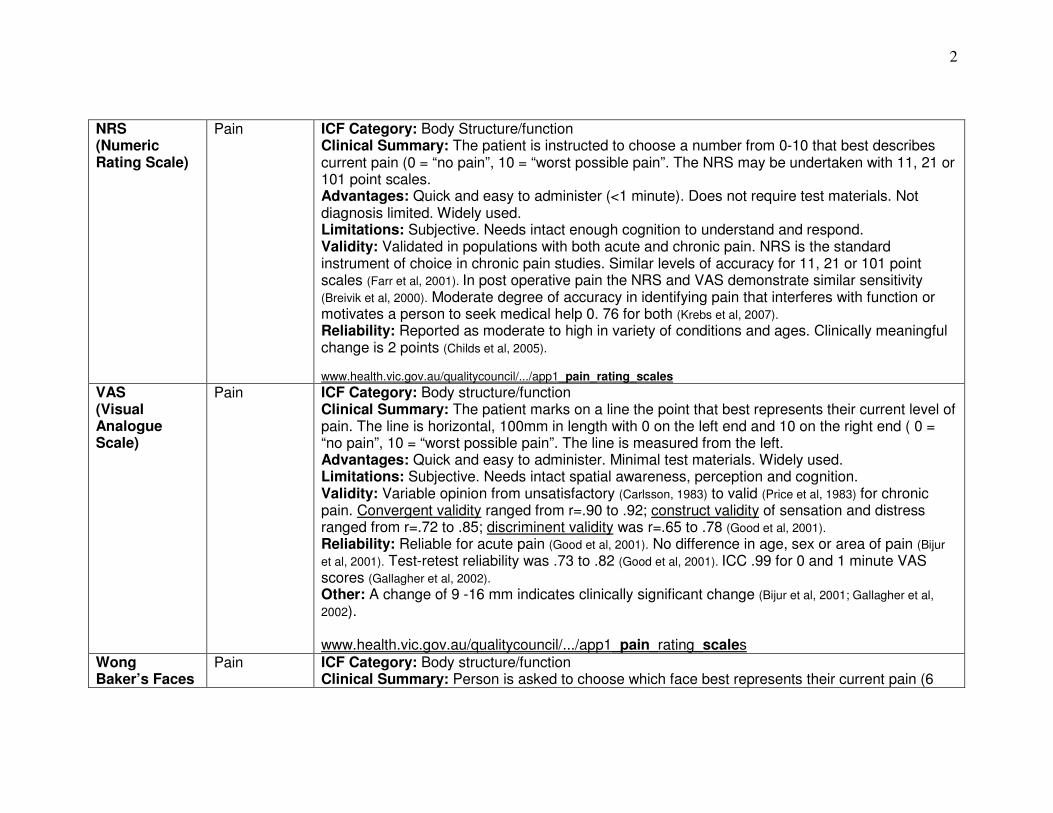
Pain ICF Category: Body structure/function Clinical Summary: Used to evaluate children who have difficulty or are unable to verbalize pain. Used recently in some adult populations. Advantages: Based on testers observations. Does not require compliance / participation from the patient. Minimal test materials required. Limitations: Subjective Validity: Currently validated for children. Demonstrated accuracy for post surgical pain when tested against a child’s self report and for cognitively impaired children (Malviya et al, 2005; Wills et al, 2003). Recent testing on adults in the critical care setting with good results (Voepel-Lewis et al, 2010). Reliability: Good inter-rater reliability for cognitively impaired children. Excellent ICC, adequate k statistic 0.44-0.57 (Malviya et al, 2005) and critically ill adults ICC coefficients of 0.67-0.95 (Voepel-Lewis et al, 2010).
wps.prenhall.com/wps/media/objects/3103/3178396/.../flacc.pdf NOPPAIN (Non-communicative Patient’s Pain Assessment Instrument)
Pain ICF category: Body structure/function, activity, participation Clinical Summary: The Non-Communicative Patient's Pain Assessment Instrument (NOPPAIN) is used to assess pain behaviours in patients with dementia. Daily care activities are rated on a 6 category Likert scale with text and pictures. Advantages: Does not require patient participation/cooperation. Limitations: Currently only validated for patients with dementia. Reliability: Kappa = 0.87 (SE: 0.2; 95% CI: 0.82-0.91) (Snow et al, 2004) www.nmmra.org/resources/download.php?id=1538
2
NRS (Numeric Rating Scale)
Pain ICF Category: Body Structure/function Clinical Summary: The patient is instructed to choose a number from 0-10 that best describes current pain (0 = “no pain”, 10 = “worst possible pain”. The NRS may be undertaken with 11, 21 or 101 point scales. Advantages: Quick and easy to administer (<1 minute). Does not require test materials. Not diagnosis limited. Widely used. Limitations: Subjective. Needs intact enough cognition to understand and respond. Validity: Validated in populations with both acute and chronic pain. NRS is the standard instrument of choice in chronic pain studies. Similar levels of accuracy for 11, 21 or 101 point scales (Farr et al, 2001). In post operative pain the NRS and VAS demonstrate similar sensitivity (Breivik et al, 2000). Moderate degree of accuracy in identifying pain that interferes with function or motivates a person to seek medical help 0. 76 for both (Krebs et al, 2007). Reliability: Reported as moderate to high in variety of conditions and ages. Clinically meaningful change is 2 points (Childs et al, 2005). www.health.vic.gov.au/qualitycouncil/.../app1_pain_rating_scales
VAS (Visual Analogue Scale)
Pain ICF Category: Body structure/function Clinical Summary: The patient marks on a line the point that best represents their current level of pain. The line is horizontal, 100mm in length with 0 on the left end and 10 on the right end ( 0 = “no pain”, 10 = “worst possible pain”. The line is measured from the left. Advantages: Quick and easy to administer. Minimal test materials. Widely used. Limitations: Subjective. Needs intact spatial awareness, perception and cognition. Validity: Variable opinion from unsatisfactory (Carlsson, 1983) to valid (Price et al, 1983) for chronic pain. Convergent validity ranged from r=.90 to .92; construct validity of sensation and distress ranged from r=.72 to .85; discriminent validity was r=.65 to .78 (Good et al, 2001). Reliability: Reliable for acute pain (Good et al, 2001). No difference in age, sex or area of pain (Bijur et al, 2001). Test-retest reliability was .73 to .82 (Good et al, 2001). ICC .99 for 0 and 1 minute VAS scores (Gallagher et al, 2002). Other: A change of 9 -16 mm indicates clinically significant change (Bijur et al, 2001; Gallagher et al, 2002). www.health.vic.gov.au/qualitycouncil/.../app1_pain_rating_scales
Wong Baker’s Faces
Pain ICF Category: Body structure/function Clinical Summary: Person is asked to choose which face best represents their current pain (6

3
faces ranging from a happy smiling face with the words “no hurt” to a crying sad face with the words “hurts worst”. For ages 3 yrs to adult. Advantages: Quick and easy to administer. Minimal test materials. Preferred over other tests in children able to self report and in adults with limited cognition. Limitations: Subjective. Need the ability to interpret facial expression. Validity: Numerous studies report it is valid in children (Luffy et al, 2003; Garra et al, 2010). Less data available for adults but good validity in comparison to other scales such as the VAS and NRS (Jowers Ware et al, 2006; Li, 2007) Reliability: Generally, authors report good reliability (Luffy et al, 2003; Garra et al, 2010; Jowers Ware et al, 2006; Li, 2007). However, Jastrzab et al (2009) reported that 52-55% of nurses were unable to describe the correct use of the scale, even after education. www.painknowledge.org/physiciantools/.../Wong-Baker_Scale.pdf
JAMAR Grip Dynamometer
Strength ICF Category: Body structure/function Clinical Summary: Quantifies isometric grip strength Advantages: Relevant in clinical practice and research; simple and commonly used test of general strength level; well researched; norms available. Limitations: Equipment required; The dynamometer must be adjusted for hand size – this affects the accuracy of the measurement. Validity: Generally considered the gold standard; 0.75 with sphygmanometer (Hamilton et al, 1992) Reliability: Good r=0.81 (Hamilton et al, 1992); ICC values 0.85-0.98 (Peolsson et al, 2001) Other: It is also useful to record whether the person is left or right handed, as this may help in the interpretation of results. The non-dominant hand usually scores about 10% lower. The forearm muscles are easily fatigued, so the best scores are usually achieved in the first or second trial. http://www.youtube.com/watch?v=y9r6jqy6tdE
Action Research Arm Test (ARAT)
Function ICF Category: Body structure/function; activity Clinical Summary: There are 4 subtests: Grasp, Grip, Pinch, Gross Movement. The ARAT measures specific changes in limb function among individuals who sustained cortical damage resulting in hemiplegia. Advantages: Time to administer is an average of 6 to 30 minutes. Norms for Adolescent: 13-17 years; Adult: 18-64 years; Elderly adult: 65+. Researched in Multiple Sclerosis; Stroke; Traumatic Brain Injury populations. Limitations: Price € 870 (euros). Standardized equipment is required.

4
Validity: Concurrent. adequate to excellent correlations with the Box and Block Test (BBT) and the Nine-Hole Peg Test (NHPT) at pre and post-treatment (Lin et al, 2010). Construct: 7 excellent correlations with Brunnstrom-Fugl-Meyer test; the upper extremity subscale of the Motor Assessment scale; the Motricity Index; the upper extremity movement of Modified Motor Assessment Chart; the Box and Block Test, the motor function subscore of the Fugl-Meyer test, the Hemispheric Stroke Scale, and upper extremity strength and grasp speed. Adequate correlations with the passive joint motion/joint pain of the Fugyl-Meyer test, the FIM and spasticity. Poor correlations with the Fugyl-Meyer test, the Ashworth scale, the Modified Barthel Index, the NIHSS, light touch sensation, and pain. Reliability: Excellent internal consistency Cronbach's α = 0.98 (Nijland et al, 2010) Excellent test-retest reliability for each subscale ICC = 0.89 and rho = 0.89 at a minimum and for the test as a whole, ICC = 0.96 and rho = 0.96 (Platz et al, 2005) excellent intra-rater reliability using Spearman rho correlation, intraclass correlation coefficients (ICC) and weighted kappa. Excellent inter-rater reliability - minimum ICC = 0.92 (Platz et al, 2005; Yozbatiran et al, 2008; Nijland et al. 2010). Minimally Clinically Important Difference = 5.7 Minimal Detectible Change: satisfactory (6%) http://www.ncbi.nlm.nih.gov/pubmed/19556333
http://www.medicine.mcgill.ca/strokengine%2Dassess/module_arat_quick-en.html Information on the ARAT can be obtained in the study by Lyle (1981), Hsieh et al. (1998), van der Lee et al. (2002), Rabadi & Rabadi (2006), and Yozbatiran et al. (2008) and at the website: http://www.aratest.eu/Index_english.htm
Arm Activity Measure (ArMA)
Function ICF Category: Body structure/function/activity Clinical Summary: This is a measure of real time functional performance in the hemiparetic arm. The measure is designed to be reflective of real life or actual performance. May be administered by patient or carer. Advantages: 10 minutes; free access; Validity: No information located. Reliability: No information located. http://www.researchrom.com/masterlist/view/2
Chedoke Arm and Hand Inventory (CAHAI)
Function ICF Category: Activity Clinical Summary: The original CAHAI consists of 13 functional items that are non-gender specific, involve both upper limbs, and incorporates a range of movements and grasps that reflect stages of motor recovery following stroke. The shortened versions have 7, 8 or 9 items. Each item

5
of the CAHAI is scored on a 7-point quantitative scale, similar to the scale used in the Functional Independence Measure (FIM) (Keith et al, 1987). The time to administer and score the CAHAI is approximately 25 minutes (Barreca et al., 2004; Barreca et al., 2006). Advantages: Easy to administer and score. Training video available. Limitations: Need to assemble the required materials in advance. Validity: Excellent convergent validity with the ARAT and the CMSA; excellent known groups validity - CAHAI was the best measure to detect change among patients with mild/moderate impairment from patients with severe impairment (Barreca 2004, 2005, 2006, 2006b). Reliability: Excellent internal consistency, test-retest, and inter-rater reliability 0.96- 0.98 (Barreca, et al, 2004; Barreca et al, 2005; Barreca et al, 2006) Minimal detectable change: 6.3 points http://www.cahai.ca
Jebsen Test of Hand Function
Function ICF Category: Activity Clinical Summary: Standardized, timed test of unilateral and bilateral hand use: writing, card turning, small object manipulation, simulated feeding, manipulation of large, light and heavy objects. Advantages: Adult norms established for age groups 20-59, 60-94; and 60-69, 70-79, and 80-89. (Children’s norms also established from age 6 up.) Test requires 15 to 45 minutes to complete using simple, inexpensive, readily available test materials. Test can be used for clients with multiple diagnoses: arthritis, hemiparesis, quadriplegia, head trauma. Limitations: Assesses the speed but not the quality of the movement Validity: Concurrent validity: In patients with RA the scores on the Jebsen correlated significantly with scores on the AIMS dexterity items (r=0.43), the AIMS ADL items (r=0.47), the AIMS household activity items (r=0.58), grip strength (r=0.56) and the HAQ (r=0.37) (Vliet Vlieland et al, 1996). All of the subscales except writing correlated with the HAQ (r=0.49-0.55) and joint deformity (r=0.38-0.83) (Sharma et al, 1994). Discriminative validity: The Jebsen was shown to discriminate between subjects with and without different physical disabilities (Jebsen et al, 1969;VlietVlieland et al, 1996). Reliability: Interrater reliability: r = 0.82 (Vliet Vlieland et al, 1996); interrater reliability r=0.91 (Vliet Vlieland et al, 1996). ICCs ranged from 0.82 to 1.00 (Hackel et al, 1992); Test-retest reliability r=0.84-0.85 (Vliet Vlieland et al, 1996). http://www.scireproject.com/outcome-measures/jebsen-hand-function-test

6
Motor Assessment Scale – Upper Limb (UL-MAS)
Function ICF Category: Body structure/function; activity Clinical Summary: Has 3 sections with 6 components each: Upper Arm Function, Hand Movements and Advanced Hand Activities. Patients perform each task 3 times and the best performance is recorded. Some are timed. Advantages: Well researched test. 45-60 minutes to administer. Limitations: Not recommended for patients with aphasia. Validity: Criterion– Correlations between MAS items and corresponding Fugl-Meyer Assessment items were excellent (ranging from r = 0.65 to r = 0.93). The MAS Balance score correlations with the Fugl-Meyer Assessment-Sensation scores of light touch and position sense were excellent (r = 0.64 and r = 0.67, respectively) (Malouin et al, 1994; Poole and Whitney (1988). Reliability: Reliability assessed only in stable patients – excellent r = 0.95 except for tone scale. (Carr et al,1985; Poole & Whitney,1988). http://www.medicine.mcgill.ca/strokengine%2Dassess/module_mas_indepth-en.html http://www.cptrehab.com/agencyforms/CPT%20forms/Motor_Assessment_Scale.pdf
Nine Hole Peg Test
Function ICF Category: Body structure/function Clinical Summary: The Nine Hole Peg Test (NHPT) was developed to measure finger dexterity, also known as fine manual dexterity. It can be used with a wide range of populations, including clients with stroke, multiple sclerosis, and musculoskeletal disorders. Advantages: Administration time ~10 minutes. Limitations: Performance on the 9-Hole Peg Test may be sensitive to practice effects – recommend practice trials in advance of baseline assessment. Validity: Concurrent validity: the NHPT, ARAT and BBT were found to have adequate to excellent correlations at pre-treatment (ranging from rho=-0.55 to -0.80) and post-treatment (ranging from rho=-0.57 to -0.71) (Lin et al, 2010). Construct validity: The correlation between NHPT and Motricity Index (Demeurisse et al., 1980) was excellent (r = 0.82) (Parker, Wade, & Hewer 1986). When considering both the results of responsiveness and validation components of the study, the ARAT and BBT (Box and Block Test) are believed to be more appropriate than the NHPT for evaluating dexterity (Lin et al, 2010). Reliability: Excellent inter-rater reliability (Heller et al, 1987; Mathiowetz et al, 1985). http://www.nationalmssociety.org/for-professionals/researchers/clinical-study-measures/9-hpt/index.aspx http://www.medicine.mcgill.ca/strokengine%2Dassess/module_nhpt_psycho-en.html The NHPT instructions can be obtained in the study by Mathiowetz et al. (1985) and Wade (1992). Standardized
7
equipment can be obtained at the website: http://www.sammonspreston.com/Supply/Product.asp?Leaf_Id=A8515
Rivermead Motor Assessment (RMA)
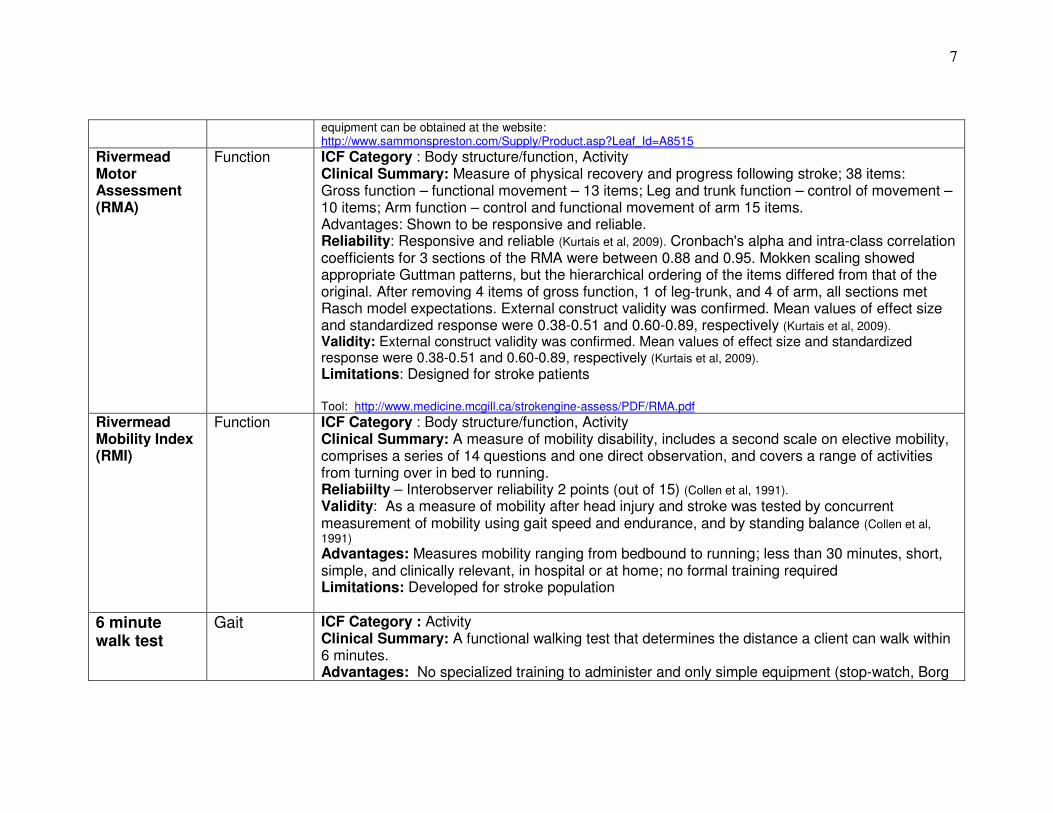
Function ICF Category : Body structure/function, Activity Clinical Summary: Measure of physical recovery and progress following stroke; 38 items: Gross function – functional movement – 13 items; Leg and trunk function – control of movement – 10 items; Arm function – control and functional movement of arm 15 items. Advantages: Shown to be responsive and reliable. Reliability: Responsive and reliable (Kurtais et al, 2009). Cronbach's alpha and intra-class correlation coefficients for 3 sections of the RMA were between 0.88 and 0.95. Mokken scaling showed appropriate Guttman patterns, but the hierarchical ordering of the items differed from that of the original. After removing 4 items of gross function, 1 of leg-trunk, and 4 of arm, all sections met Rasch model expectations. External construct validity was confirmed. Mean values of effect size and standardized response were 0.38-0.51 and 0.60-0.89, respectively (Kurtais et al, 2009). Validity: External construct validity was confirmed. Mean values of effect size and standardized response were 0.38-0.51 and 0.60-0.89, respectively (Kurtais et al, 2009). Limitations: Designed for stroke patients Tool: http://www.medicine.mcgill.ca/strokengine-assess/PDF/RMA.pdf
Rivermead Mobility Index (RMI)
Function ICF Category : Body structure/function, Activity Clinical Summary: A measure of mobility disability, includes a second scale on elective mobility, comprises a series of 14 questions and one direct observation, and covers a range of activities from turning over in bed to running. Reliabiilty – Interobserver reliability 2 points (out of 15) (Collen et al, 1991). Validity: As a measure of mobility after head injury and stroke was tested by concurrent measurement of mobility using gait speed and endurance, and by standing balance (Collen et al, 1991) Advantages: Measures mobility ranging from bedbound to running; less than 30 minutes, short, simple, and clinically relevant, in hospital or at home; no formal training required Limitations: Developed for stroke population
6 minute walk test
Gait ICF Category : Activity Clinical Summary: A functional walking test that determines the distance a client can walk within 6 minutes. Advantages: No specialized training to administer and only simple equipment (stop-watch, Borg

8
Scale, and pulse oximeter when necessary) plus a 100-ft, quiet, indoor, flat, straight rectangular hallway. The walking course must be 30m long and marked every 3m with coloured tape. Limitations: Does not assess balance, quality of movement, use of assistive devices and amount of physical assistance needed (Barak & Duncan, 2006). Stroke-specific impairments (ie muscle weakness, spasticity, balance, hemiparesis) may influence distance walked (Barak & Duncan, 2006). Validity: a) concurrent- Vo2 max in patients with stroke (r = 0.66).(Eng et al., 2004; Pang et al, 2005). Five Meter Walk Velocity for preferred (r = 0.79), and fast speed (r = 0.82) (Tang et al, 2006) Discharge locomotion (walk) FIM scores (Spearman r = 0.69), and discharge locomotion (walk) + stairs FIM scores (Spearman r = 0.69) (Keith et al, 1987). b) predictive - A predictor of mean steps per day (r = 0.68; P = 0.001). (Fulk et al, 2010) c) convergent- Correlation between 2MWT and 6 MWT plus 12MWT and 6MW. (Kosak & Smith, 2005) Relationship reported between Berg Balance Scale and the 6MWT (r = 0.69) (Patterson et al, 2007); the 6MWTand quadriceps strength (r = 0.57) (Patterson et al. 2007); the Reintegration to Normal Living Index (RNL) and 6MWT (r = 0.35) (Pang et al, 2007). Reliability: Excellent reliability for distance covered in meters (ICC = 0.99) and for the submaximal exercise variable Vo2 (ml/kg.min) (ICC = 0.96). (Eng et al, 2004); (ICC = 0.99) (Flansbjer et al, 2005);
(ICC = 0.97) (Fulk et al, 2008); (ICC = 0.98) (Liu et al, 2008) 2 minute and 12 minute walk tests also available. http://www.medicine.mcgill.ca/strokengine%2Dassess/module_6mwt_psycho-en.html
10 meter walk test
Gait ICF Category : Activity Clinical Summary: Assesses short duration walking speed (m/sec) i.e. measures the time required to walk 10 meters. Used in various populations including stroke, Parkinson’s, general neurological movement disorders and SCI. It is performed using a “flying start” - the patient walks 14 meters and the time is measured for the intermediate 10 meters. Individual walks at his preferred walking speed and wears regular footwear. An assistive device can be used if necessary. Advantages: Suitable test for clients who can ambulate in household settings. Takes 30 sec to administer, and does not require advanced training. Can be administered in clinical setting or community. 14 m and a stopwatch required.

9
Limitations: 14 m corridor can be difficult to find in a home setting. Does not consider amount of physical assist required, assistive devices required or endurance. Test is conducted in controlled environment and cannot be directly translated to other environments. Inconsistencies in the literature re: standardized distance used 10 m vs 14m Validity: Excellent correlation with 6 MWT. Intercorrelation (.93) with 2 min walk and Rivermead Mobility Index (van Hedel, Wirz,Dietz 2005) Reliability: Intrarater reliability for SCI ( r =.983, P<.001) Interrater reliability (r=.974, P<.001) van Hedel, Wirz,Dietz (2005,2006,2008,2009) http://www.scireproject.com/outcome-measures/10-meter-walking-test-10mwt
Frenchay Activities Index
IADL ICF Category : Activity Clinical Summary: A measure of instrumental activities of daily living (IADL) for use with patients recovering from stroke. Provides a broad measurement of actual activities patients have undertaken in recent past. Completed through an interview. Advantages: Interview taking 5 minutes (with or without the patient's family). Chinese (translated and validated), Dutch (translated). Used for longitudinal studies. No ceiling effect. Limitations: Floor effect for individuals examined at 6 months post-stroke. A moderate ability to detect change (in patients 6-12 months post-stroke) Validity: Construct validity supported by correlations with Barthel index and Sickenss Impact Scale (Pedersen et al, 1977). Criterion: Spearman's correlation of r = 0.94 was found between mailed questionnaire FAI scores and face-to-face interview FAI scores., however individual differences on scores ranged widely between mailed and postal responses taken 10 days later (Carter et al. 1997) Construct: Sickness Impact Profile (r = -0.56 to -0.73) (Bergner et al, 1981) ; Barthel Index (r = 0.66) (Wade & Collin, 1988); Functional Independence Measure (Motor subscale) (r = 0.63) (Keith et al, 1987); Stroke Adapted Sickness Impact Profile (van Straten et al, 1997) Reliability: Excellent internal consistency ( Schuling et al 1993; Tooth et al, 2003, Miller et al. 2004) Test-retest reliability - overall agreement of individual items was variable eg. heavy housework, local shopping, walking outside and travel outings failed to reach statistical significance, while other items demonstrated excellent agreement (r = 0.80) (Wade et al. 1985). Inter-rater reliability with mixed results depending upon items assessed. Spearman's correlation for FAI totals of rater B versus rater A was r = 0.93 (Piercy et al, 2000)
Barthel Index Activity ICF Category: Activity

10
(BI) Clinical Summary: Original version (1965) identifies the level of independence of an individual with a neuromuscular or musculoskeletal disorder in ten areas of ADL. Each item is rated “with help” or “independent”; has scoring guide with definitions for each category. Score based on the time and amount of physical assistance required. Score ranges from 0 to 100 points. Modified version - (1988) added 2 intermediate scoring categories for 8 of 10 ADL items; 5 response categories: “unable to perform task”, “attempts task but unsafe”, “moderate help required”, minimal help required” and “fully independent”. Alternate forms of the BI available including: Modified 10-item version (MBI) (Collin et al., 1988), 5-item short form (Hobart & Thompson, 2001), The expanded 15-item version (Granger et al., 1979; Fortinsky & Granger, 1981), The extended BI (EBI) (Prosiegel, Bottger, & Schenk, 1996), The 3-item BI (Ellul, Watkins, & Barer, 1988), Self-rating BI (SB) (Hachisuka, Ogata, Ohkuma, Tanaka, & Dozono, 1997; Hachisuka, Okazaki, & Ogata, 1997; McGinnis et al., 1986). The original and 10-item and 15-item modifications are most commonly used. Advantages: Easy to use with training; Completed in 2 - 5 minutes by self-report and up to 20 minutes by direct observation. (Finch, Brooks, Stratford, & Mayo, 2002). Metric rating system to reflect overall functional ability and to assess progress over time. Tested on many chronic conditions including stroke, spinal injuries, dementia, arthritis, and multiple sclerosis Limitations: Does not take into account contextual or individualized factors; Items assessed may not reflect the client’s real priorities (Dewing, 1992). It should be used with caution as it is insensitive to change at higher scores with persons with mild stroke (Wade & Hewer, 1987; Skilbeck, Wade, Hewer, & Wood, 1983). Validity: Original version: Construct validity: Comparable with other measures of functional ability but not sensitive to change in functional ability related to general health, communications status, and psychosocial status. (Granger et al, 1979). Modified version has excellent concurrent validity (r = 0.73-0.77) with a measure of motor ability (Wade & Hewer, 1987); demonstrates predictive validity for predicting progress and recovery following stroke (Patel, Coshall, Lawrence, Rudd, & Wolfe, 2001; Sze, Wong, Leung, & Woo, 2001; Tilling, Sterne, Rudd, Glass, Wityk, & Wolfe, 2001). Reliability: Original version: Inter-rater reliability between items k = 0.53 (adequate) - 0.94 (excellent) in a study at four points post stoke. ICC 0.94 (excellent), T internal consistency was excellent, ranging between 0.89-0.92 (Hsueh et al., 2002).
http://www.medicine.mcgill.ca/strokengine-assess/PDF/barthel.pdf

11
Clinical Outcome Variables Scale (COVS)
Activity ICF: Activity Clinical Summary: Used to assess movement from one postural position to another or from one location to another, within walking or wheeling distance. Conducted via in-person interviews or over the telephone (TCOVS). 10 mobility tasks quantified using a 7-point scale ranging from 1(fully dependent mobility) to 7 (normal independent mobility). Scores range from 13 to 91 with higher scores indicating better physical functioning. Advantages: Patient population: stroke, traumatic brain injury, amputations, and musculoskeletal injuries (Barker et al. 2007).Applied in acute, inpatient/outpatient rehabilitation, and community settings. Telephone interview takes 5 minutes (subjects are given the questions ahead of time). In-person assessment takes 35 minutes Limitations: Not Free COVS 2000 packages: $85.00, Guidelines Booklet: $30.00 While a widely used instrument, more validation work needs to be completed Validity: Construct: Comparable with other measures of functional ability (Salter et al, 2010, Hajek et al, 1997Sacks L et al, 2010) Predictive validity – predictive of length of hospital stay, discharge destination (Ekstrand et al, 2008) Reliability: Test-retest Reliability: Excellent correlation between tool administered in-person and tool administered over the telephone (Composite score ICC = 0.98, General mobility subscale ICC=0.97, Ambulation subscale CC 0.99)( Barker et al, 2007). Intrarater/Intrarater Reliability: Excellent interrater, ICC=0.97 (1 to 2 days between assessments) and excellent intrarater reliability, agreement on all items >85%, 4 items tend to have lower but still acceptable agreement (Seaby, 1989) Internal Consistency: Excellent, alpha = 0.93 Available for purchase at http://www.irrd.ca/covs/
Functional Independence Measure (FIM)
Activity ICF Category: Activity Clinical Summary: Systematic measurement of the level of a patient's disability. Scored on the basis of how much assistance is required. Contains 18 items: 13 motor tasks 5 cognitive tasks (considered basic activities of daily living). Tasks are rated on a 7 point ordinal scale that ranges from total assistance to complete independence. Scores range from 18 (lowest) to 126 (highest) indicating level of function. Patient population researched: stroke, brain injury, spinal cord injury, multiple sclerosis, stroke, orthopaedic conditions including low back pain, geriatrics Advantages: Metric rating system used to identify a baseline and to compare progress in basic ADLs; easily reproducible; internationally recognized outcome measure of disability. Limitations: In patients with MS and stroke, total and motor scales have small floor and ceiling
12
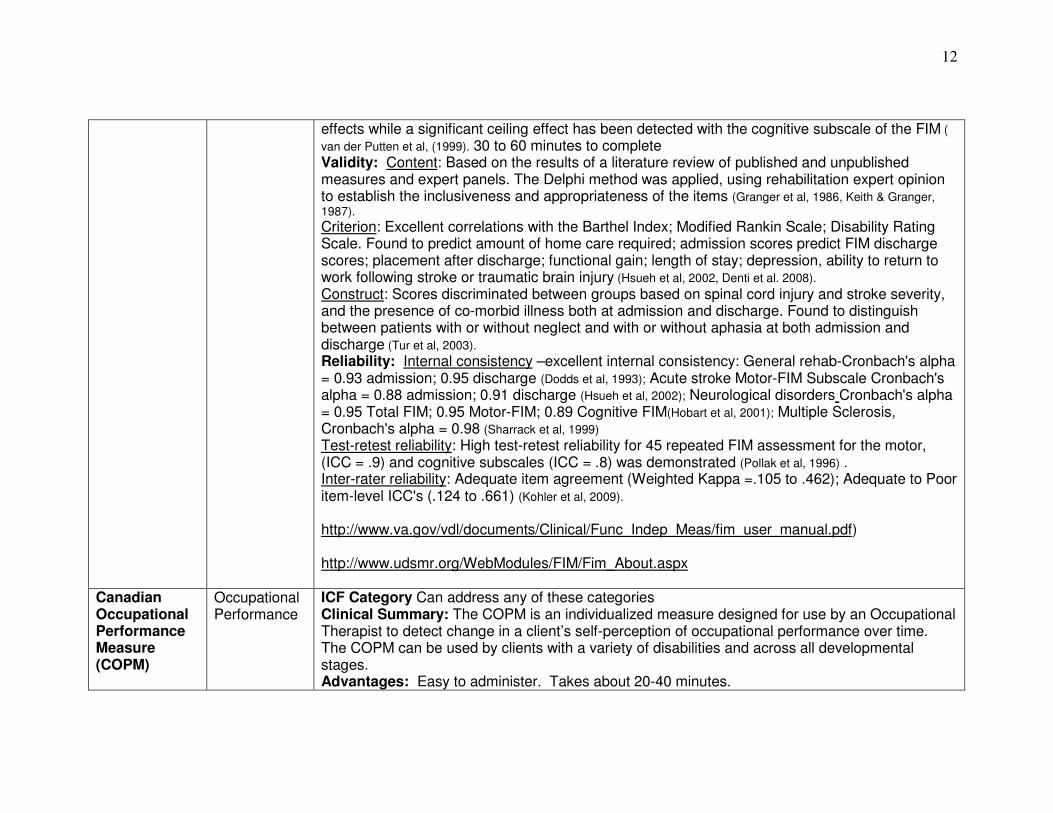
effects while a significant ceiling effect has been detected with the cognitive subscale of the FIM ( van der Putten et al, (1999). 30 to 60 minutes to complete Validity: Content: Based on the results of a literature review of published and unpublished measures and expert panels. The Delphi method was applied, using rehabilitation expert opinion to establish the inclusiveness and appropriateness of the items (Granger et al, 1986, Keith & Granger, 1987). Criterion: Excellent correlations with the Barthel Index; Modified Rankin Scale; Disability Rating Scale. Found to predict amount of home care required; admission scores predict FIM discharge scores; placement after discharge; functional gain; length of stay; depression, ability to return to work following stroke or traumatic brain injury (Hsueh et al, 2002, Denti et al. 2008). Construct: Scores discriminated between groups based on spinal cord injury and stroke severity, and the presence of co-morbid illness both at admission and discharge. Found to distinguish between patients with or without neglect and with or without aphasia at both admission and discharge (Tur et al, 2003). Reliability: Internal consistency –excellent internal consistency: General rehab-Cronbach's alpha = 0.93 admission; 0.95 discharge (Dodds et al, 1993); Acute stroke Motor-FIM Subscale Cronbach's alpha = 0.88 admission; 0.91 discharge (Hsueh et al, 2002); Neurological disorders Cronbach's alpha = 0.95 Total FIM; 0.95 Motor-FIM; 0.89 Cognitive FIM(Hobart et al, 2001); Multiple Sclerosis, Cronbach's alpha = 0.98 (Sharrack et al, 1999) Test-retest reliability: High test-retest reliability for 45 repeated FIM assessment for the motor, (ICC = .9) and cognitive subscales (ICC = .8) was demonstrated (Pollak et al, 1996) . Inter-rater reliability: Adequate item agreement (Weighted Kappa =.105 to .462); Adequate to Poor item-level ICC's (.124 to .661) (Kohler et al, 2009). http://www.va.gov/vdl/documents/Clinical/Func_Indep_Meas/fim_user_manual.pdf) http://www.udsmr.org/WebModules/FIM/Fim_About.aspx
Canadian Occupational Performance Measure (COPM)
Occupational Performance
ICF Category Can address any of these categories Clinical Summary: The COPM is an individualized measure designed for use by an Occupational Therapist to detect change in a client’s self-perception of occupational performance over time. The COPM can be used by clients with a variety of disabilities and across all developmental stages. Advantages: Easy to administer. Takes about 20-40 minutes.

13
Limitations: Although there are different studies in which the validity and/or reliability of the COPM have been investigated, some studies have only focused on specific diagnoses, and in other studies small study populations are investigated, so there is still a lack of info about the psychometric properties of the COPM (Dedding 2004). Validity: No clear description of the psychometric properties of the COPM can be found in the literature (Dedding 2004). Reliability: The test-retest reliability for the performance and satisfaction scores of the COPM, calculated using inter-class correlation coefficients, were 0.63 for performance and 0.84 for satisfaction (Law, 1994). Other: In clinical practice the COPM scoring for performance and satisfaction for a particular problem can still be useful, since this reflects the perception of the client and offers the possibility to detect change from the client’s point of view (Dedding 2004). http://www.caot.ca/copm/description.html
Associated Reaction Rating Scale
Tone ICF Category: Body structure/function Clinical Summary: Measures 4 key characteristics of associated reactions in the hemiplegic upper limb, developed for stoke clients Advantages: Reliability for stroke patients is encouraging (Macfarlane, 2002). Limitations: Results apply to observations made during standardized tasks of “sit to stand” (Macfarlane, 2002). Validity: Under review. Reliability: Good correlations between the two raters in total (rho 0.89 p< 0.005) and modal scores (rho 0.88 p < 0.005). Reliability testing of each item revealed moderate to very good inter-rater agreement (weighted kappa values 0.43–0.85) and good to very good intra-rater agreement (weighted kappa values 0.61–0.87). (Macfarlane et al, 2002). Weblink for article: http://cre.sagepub.com/content/16/7/726.abstract or http://www.ncbi.nlm.nih.gov/pubmed/12428821
Australian Spasticity Assessment Scale (ASAS)
Tone ICF category: Body structure/function Clinical Summary: Quantifies amount of spasticity present via measurement of “spastic catch” Advantages: Relevant in clinical practice and research. Almost complete agreement with instrumental measures. Limitations: Tested mainly with children. The presence of muscle contractures may influence the reliability of ASAS. Limited publications. Validity: Has face validity (Gibson, Love, & Blair, 2008)

14
Reliability: Kappa = 0.71 (95% CI 0.67 to 0.75) (Gibson, Love, & Blair, 2008) http://physiotherapy.asn.au/congress10/images/Abstracts/PDF_NPG/Gibson,%20N.pdf
Ashworth and Modified Ashworth (MAS)
Spasticity ICF Category: Body structure/function Clinical Summary: Assess single-joint resistance to passive ROM or a velocity dependent stretch reflex. Doesn’t address spasm frequency or severity, differentiate between phasic and tonic components of spasticity. Overall construct of spasticity is best measured with a battery of tests including the Ashworth or MAS (SCIRE http://www.scireproject.com/outocme-measures/ashworth-and-modified-ashworth) Original Ashworth Scale: Tests resistance to passive movement about a joint with varying degrees of velocity. Scores range from 0-5; 0= no resistance; 4= rigidity Modified Ashworth Scale: Similar to Ashworth, but add a 1+ scoring category to indicate resistance through less than half of the movement (Bohannon & Smith, 1987). Populations tested: adults & children with lesions of the Central Nervous System, traumatic brain injury, multiple sclerosis. Advantages: Clinical gold standard for SCI. Easily interpretable with discrete categories Adds an additional grade at the lower end of spasticity. Correlates well with self rating VAS for spasticity and SCATS (Priebe et al. 1996). Limitations: Adequate training is required to ensure inter-rater reliability. Evidence suggests that the resistance to passive movement is not an exclusive measure of spasticity (http:www.rehabmeasures.org/Lists/RehabMeasures/DispForm.aspx?ID=902). Validity: Conflicting evidence regarding validity. Insufficient validity and reliability and no longer recommended for use to describe spasticity (Fleuren et al, 2009). Adequate concurrent validity (Allison & Abraham, 1995); excellent convergent validity (Katz, 1992) (http:www.rehabmeasures.org/Lists/RehabMeasures/DispForm.aspx?ID=902). Reliability: 2 studies involving subjects with SCI report adequate to excellent reliability, validity, and/or responsiveness (Taciser, 2011).*Note conflicting findings by researchers. Inter-rater agreements were very good for both MAS and MMAS, with weighted kappa values of 0.868 and 0.892, respectively (Taciser, 2011). Link to article http://journals.lww.com/intjrehabilres/Abstract/2011/03000/Inter_rater_reliability_of_the_Modified_Ashworth.8.aspx. Website for tool: http://www.scireproject.com/outcome-measures/ashworth-and-modified-ashworth

15
Spinal Cord Assessment Tool for Spastic reflexes (SCATS-SC)
Spasticity ICF Category Body structure/function Clinical Summary: Evaluates 1. Ankle clonus, 2. Flexor reflex and 3. Extensor reflex Advantages: Assesses multiple joint spasticity Limitations: Requires trained clinicians to quantitatively measure angles; not widely used Validity: Valid measure of 3 distinct types of spastic motor behaviors in SCI and provides a complementary tool for measuring spastic hypertonia (Benz 2005) Reliability: r =0.22–0.49, 19 repeated measures in 8 individuals (Heish 2008). Significant correlations observed between the SCATS extensor spasms and the Ashworth scores for hip and knee flexors and for ankle plantarflexors (ρ=.98, .88, .61, respectively). Also, SCATS flexor spasms and SCATS clonus scores correlated significantly with some of the Ashworth scores. Only SCATS clonus scores correlated significantly with spasm frequency measures (ρ=.59, P<.05) (Benz 2005) Links to articles: http://www.archives-pmr.org/article/S0003-9993(04)00297-7/abstract http://www.nature.com/sc/journal/v46/n2/fig_tab/3102125t1.html
Tardieu Spasticity ICF Category Body structure/function Clinical Summary: The Tardieu Scale involves performing passive muscle stretch at 2 velocities, slow and fast. The rater derives 2 parameters; the Spasticity Angle X is the difference between the angles of arrest at slow speed and of catch-and-release or clonus at fast speed; the Spasticity Grade Y is an ordinal variable that grades the intensity (gain) of the muscle reaction to fast stretch. (Gracies 2010) Advantages: Relevant in clinical practice & research. Sensitive to change post Botox (Boyd & Graham, 1999) Limitations: Developed for children with Cerebral Palsy Validity: Some studies have identified the Tardieu Scale to be more sensitive than other measures, to change following treatment with botulinum toxin (Haugh et al, 2006) Reliability: Excellent intrarater and interrater reliability - nonexperienced raters had mean ± SD intrarater and interrater agreement rates of 80%±14% and 74%±16%, respectively. experienced raters, intrarater and interrater agreement 90%±8% and 81%±13%, respectively, after training (Gracies 2010) Links to articles: : http://informahealthcare.com/doi/abs/10.1080/09638280500404305 : http://www.archives-pmr.org/article/S0003-9993(09)00984-8/abstract
16
Leeds Arm Spasticity Impact
Impact of spasticity
ICF Category: Activity Clinical Summary: Disability and carer scale to measure impact of upper limb spasticity. Consists of 8 items (cleaning the palm, cutting fingernails, putting the paretic arm through sleeves, cleaning under the armpit, cleaning around the elbow, standing balance, walking balance, ability to perform a home UE PT Program and carer burden scale (cleaning the palm, cutting the fingernails, dressing, cleaning under the armpit). All based on a 5 point Likert scale from “no difficulty” to “cannot do” the task) based on most difficult over the preceding week. Item scores summated and divided by number of items answered giving a summary disability score Advantages: Assessment of everyday functional skills Limitations: No information on reliability or validity found .Subjective assessments by client and carer on function. Validity: No numerical values found Reliability: No numerical values found
Spinal Cord Injury Spasticity Evaluation Tool (SCI-SET)
Impact of spasticity on function
ICF Category: Activity/ Participation Clinical Summary: The SCI-SET is a 7-day recall self-report questionnaire that takes into account both the problematic and useful effects of spasticity on daily life in people with SCI. Advantages: Easy to administer and score. Definitions of ‘spasm’ and the scale response are clearly outlined in the instructions. Time to administer is 6.8+/-2.6 minutes; in person or over the phone. Limitations: Not applicable for intervention purposes. Validity: Good face validity. Construct validity was supported by correlations (r range, -.48 to .68; p<.01) between SCI-SET scores and theoretically meaningful constructs (Adams, 2007) Reliability: The internal consistency and correlation coefficient of the SCI-SET were .90 and .91 respectively (Adams, 2007) Other: Number of items: 35. Spasticity is known to be highly variable, fluctuating on a daily and even hourly basis. A 7 day recall of impact of spasticity may be overshadowed by current levels of spasticity. Repeated administration may therefore be necessary to provide a more accurate picture of the impacts spasticity has on daily life. http://www.scireproject.com/outcome-measures/spinal-cord-injury-spasticity-evaluation-tool-sci-set
Penn Spasm Frequency Scale (PSFS)
Frequency and severity of spasticity
ICF Category: Body Function Clinical Summary: A self-report measure that assess the frequency and severity of muscle spasms. The PSFS is composed of 2 parts. (1) A self report measure with items on 5 point scales developed to augment clinical ratings of spasticity to provide a more comprehensive

17
assessment of spasticity. (2) A 3-point scale assessing the severity of spasms. Advantages: The PSFS is easy to understand presents minimal patient burden (easy to administer during routine clinical visits). Quick to administer. No training required, however, understanding spasticity likely improves the scale’s utility. Free of cost. Limitations: Population tested only on spinal cord injured population Validity: Predictive/concurrent validity: Chronic SCI: (Hornby et al, 2003; n = 12; mean age = 39.2 (range = 24 to 67) years; mean time since injury = 8.9 years; injury at the 8th thoracic spinal cord level or higher); Mean Penn scores:
• Patients taking anti-spastic medication = 3.0 (median = 3.0) points • Patients not taking medication = 2.17 (median = 2.0) points
Reliability: Test-rest reliability: Chronic SCI: (Adams et al, 2007) excellent (assessed 3 times over 3 consecutive weeks; ICC = 0.91). Interrater/intrarater reliability: has not been established for PSFS in SCI (Hsieh et al, 2008) Other: The scale is subject to concomitant subclinical conditions such as fullness of the bladder, development of a symptomatic urinary tract infection, anxiety level, room temperature, subject comfort and many other conditions. In general, self-report measures of spasticity correlate only moderately with clinical examination suggesting that the elements of spasticity evaluated in physical examination do not represent what is important to persons with SCI spasticity. http://www.rehabmeasures.org/Lists/RehabMeasures http://www.scireproject.com/outcome-measures/penn-spasm-frequency-scale-psfs
GAS Goal Attainment Scale
Can be designed to address specific types eg. Pain, function, activity etc.
ICF Category: Can be designed to address any of these categories Clinical Summary: A method of scoring the extent to which a patient’s individualized goals are achieved in the course of an intervention. Each patient has their own outcome measure but it can be scored in a standardized way to enable statistical analysis Advantages: More sensitive to change for a specific individual than standardized outcome measures; minimizes floor and ceiling effects; grading of goal attainment; versatility across populations, interventions, and fields, encourages patient/family and team collaboration; ability to adapt to any ICF category (Schlosser, 2004) Limitations: Dependent upon the quality of the initial goal Validity: Effect size 1.29; relative efficiency 53.7 (Gordon et al, 1999) * as the GAS is designed to detect change in status rather than current status, it is unreasonable to compare this tool to standardized outcome measures (Schlosser, 2004); no equipment required

18
Reliability: k> 0.8 (Stolee et al, 1992: Rockwood et al, 1993); generally good e.g >0.8 (Schlosser, 2004) Other: In a residential setting, the GAS was found to be more responsive to change than other standardized outcome measures (Gordon et al, 1999) (website): None identified
References Adams M, Martin Ginis K, Hicks A. (2007). The Spinal Cord Injury Spasticity Evaluation Tool: Development and Evaluation. Archives of Physical Medicine and Rehabilitation. 88:1185-1192
Barreca SR, Gowland CK., Stratford PW (2004). Development of the Chedoke Arm and Hand Activity Inventory: Theoretical constructs, item generation, and selection. Topics in Stroke Rehabilitation, 11(4), 31- 42.
Barreca, SR, Stratford PW, Lambert CL, Masters, LM, & Streiner, DL. (2005). Test-retest reliability, validity, and sensitivity of the Chedoke Arm and Hand Activity Inventory: a new measure of upper-limb function for survivors of stroke. Archives of Physical Medicine and Rehabilitation, 86, 1616-1622.
Barreca SR, Stratford PW, Masters LM, Lambert CL, Griffiths J, McBay C. (2006a). Validation of three shortened versions of the Chedoke Arm and Hand Activity Inventory. Physiotherapy Canada, 58, 148-156.
Barreca SR, Stratford PW, Masters LM, Lambert CL, & Griffiths J (2006b) Comparing two versions of the Chedoke Arm and Hand Activity Inventory with the Action Research Arm Test. Physical Therapy, 86(2), 245-253. Barker RN, Amsters DI, Kendall MD, Pershouse KJ, Haines TP. (2007). Reliability of the Clinical Outcome Variables Scale when administered via telephone to assess mobility in people with spinal cord injury. Archives of Physical Medicine and Rehabilitation. 88: 632-7. Bhakta B, Cozens JA, Chamberlain MA. (2000) Impact of botulinum toxin type A on disability and carer burden due to arm spasticity after stroke: a randomised double blind placebo controlled trial .Journal of Neurology and Neurosurgery Psychiatry;69:217-221. Bijur PE, Silver W, Gallagher EJ. (2001). Reliability of the Visual Analog Scale for Measurement of Acute Pain. Academic Emergency Medicine December 2001, 8, (12): 1153-1157. Bohannon RW, Smith MB. (1987). Interrater reliability of a modified Ashworth scale of muscle spasticity. Physical Therapy. 67(2):206-7. Boyd R & Graham K. (1999). Objective measurement of clinical findings in the use of Botox Type A for the management of children with Cerebral Palsy. European Journal of Neurology. 6(suppl 4) S23-35. Bovend Eerdt TJH, Dawes H, Johansen-Berg H, Wade DT. (2004). Evaluation of the Modified Jebsen Test of Hand Function and the University of Maryland Arm Questionnaire for Stroke. Clinical Rehabilitation.18: 195-202. Breivik EK, Bjornsson G A, Slovlund E. (2000). A comparison of Pain Rating Scales by Sampling From Clinical Trail Data. The Clinical Journal of Pain, 16(1): 22-28. Campbell J, Kendall M. (2003) Investigating the suitability of the Clinical Outcome Variables Scale (COVS) as a mobility outcome measure in spinal cord in jury rehabilitation. Physiotherapy Canada.55:135-144. Carr, JH, Shepherd RB, Nordholm L, Lynne, D. (1985). Investigation of a new motor assessment scale for stroke patients. Physical Therapy. 65, 175-180. Childs JD, Piva SR, Fritz JM. (2005). Responsiveness of the numeric pain rating scale in patients with low back pain. Spine, 30(11): 1331-1334. Collen FM, Wade DT, Robb GF, Bradshaw CM. (1991). The Rivermead Mobility Index: a further development of the Rivermead Motor Assessment. Disability and Rehabilitation. 13(2), 50-54.
19
Collin C, Wade DT, Davies S, Horne V. (1988). The Barthel ADL Index: a reliability study. International Disability Study, 10, 61-63.
Dedding C, Cardol M, Eyssen IC, Dekker J, Beelen A. (2004). Validity of the Canadian Occupational Performance Measure: a client-centred outcome measurement. Clinical Rehabilitation. 18:660-7.
Demeurisse G., Demol O, & Robaye E. (1980). Motor evaluation in vascular hemiplegia. European Neurology, 19(6), 382-389.
Denti, L, Agosti M, Franceschini M. (2008). Outcome predictors of rehabilitation for first stroke in the elderly. European Journal of Physical Rehabilitation Medicine. 44(1): 3-11. Dewing, Jan (1992) Clinical Review: A critique of the Barthel Index. British Journal of Nursing, 1 (7): 325-9. Dodds, TA., Martin, DP, Stolov WC, Deyo RA.(1993). A validation of the functional independence measurement and its performance among rehabilitation inpatients. Archives of Physical Medicine and Rehabilitation. 74: 531-536. Ekstrand, E, Ringsberg, K.A, Pessah-Rasmussen H. (2008). The physiotherapy clinical outcome variables scale predicts length of hospital stay, discharge destination and future home facility in the acute comprehensive stroke unit. Journal of Rehabilitation Medicine. 40(7): 524-528.
Ellul, J., Watkins, C., Barer, D. (1998). Estimating total Barthel scores from just three items: The European Stroke Database 'minimum dataset' for assessing functional status at discharge from hospital. Age and Ageing, 27(2), 115-122. Eng J, Chu K, Dawson A, Kim CM, Hepburn K. (2002). Functional Walk Tests in Individuals with Stroke Relations to Perceived Exertion and Myocardial Exertion. Stroke. 33:756-761. Farrar JT, Yound JP, MaMoreaux L, Werth JL. (2001). Clinical Importance of changes in chronic pain intensity on an 11 point numerical pain rating scale. Pain 92(2): 149-158.
Finch, E., Brooks, D., Stratford, P. W., Mayo, N. E. (2002). Physical Rehabilitations Outcome Measures. A Guide to Enhanced Clinical Decision-Making (2nd ed.), Canadian Physiotherapy Association, Toronto.
Fleuren JFM, Voerman GE, Erren-Wolters, CV, Snoek GJ, Rietman JS, Hermens JF, Nene AV. (2010). Stop using the Ashworth Sclae for the assessment of spasticity. Journal of Neurology & Neurosurgical Psychiatry. 81: 46-52.
Fortinsky, RH, Granger, CV, Seltzer GB. (1981). The use of functional assessment in understanding home care needs. Medical Care, 19, 489-497. Gallagher J, Bijur PE, Latimer C, Silver M. (2002). Reliability and validity of a visual analog scale for acute abdominal pain in the ED. The American Journal of Emergency Medicine. 20(4): 287-290. Garra G, Adam J. Singer MD, Breena R. Taira MD, Chohan J, Cardoz H, Chisena E, Thorde HC. (2010). Validation of the Wong-Baker FACES Pain Rating Scale in Pediatric Emergency Department Patients. Academic Emergency Medicine.17(1) 50-54. Good M, Stiller C, Zausniewski JA, Anderson GC, Anderson GC, Stanton-Hicks M, Grass JA. (2001). Sensation and Distress of Pain Scales: Reliability, Validity, and Sensitivity. Journal of Nursing Measurement. 9(3): 219-238. Gordon JE, Powell C, Rockwood K. (1999). Goal attainment scaling as a measure of clinically important change in nursing-home patients. Age & Aging. 28: 275-281. Gracies JM, Burke K, Clegg NJ, Browne R, Rushing C, Fehlings D, Mathews D. (2010). Reliability of the Tardieu Scale for assessing spasticity in children with cerebral palsy. Archives of Physical Medicine and Rehabilitation. 91(3): 421-8. Granger CV, Dewis LS, Perters NC, Sherwood CC, Barrett JE (1979). Outcome of comprehensive medical rehabilitation: measurement of PULSES Profile and the Barthel Index. Archives of Physical Medicine and Rehabilitation. 60: 145-54.
Granger CV, Hamilton BB, Keith RA, Zielezny M, Sherwins FS. (1986). Advances in functional assessment for medical rehabilitation. Topics in Geriatric Rehabilitation, 1, 59-74.

20
Hachisuka K, Ogata H, Ohkuma H, Tanaka S, Dozono K. (1997). Test-retest and inter-method reliability of the self-rating Barthel Index. Clinical Rehabilitation, 11(1), 28-35.
Hachisuka K., Okazaki T., Ogata H. (1997) Self-rating Barthel index compatible with the original Barthel index and the Functional Independence Measure motor score. J UOEH, 19(2), 107-121.
Hackel ME, Wolfe GA, Band SM, Canfield JS. (1992). Changes in hand function in the ageing adult as determined by the Jebsen Test of Hand Function. Physical Therapy; 72:373-7. Hamilton GF, McDonald C, Chenier TC. (1992). Measurement of grip strength: Validity and reliability of the sphygmanometer and Jamar Grip Dynamometer. Journal of Orthopaedic and Sports Physical Therapy. 16(5): 215-219.
Hajek V, Gagnon S, Ruderman JE. (1997). Cognitive and functional assessments of stroke patients: an analysis of their relation. Archives of physical medicine and rehabilitation. 78(12): 1331-1337.
Haugh AB, Pandyan AD, Johnson GR. (2006). A systematic review of the Tardieu Scale for the measurement of spasticity” Disability and Rehabilitation, 2006, Vol. 28, No. 15 , Pages 899-907.
Heller A, Wade DT, Wood VA, Sunderland ., Hewer R, & Ward E. (1987). Arm function after stroke: measurement and recovery over the first three months. Journal of Neurology, Neurosurgery & Psychiatry, 50(6), 714- 719.
Hobart JC, Thompson AJ. (2001). The five item Barthel index. Journal of Neurology, Neurosurgery & Psychiatry, 71, 225-230 Holbrook M., Skilbeck C. E. (1983). An activities index for use with stroke patients. Age and Ageing, 12(2), 166-170.
Hornby T, Rymer W et al (2003). Windup of flexion reflexes in chronic human spinal cord injury: a marker for neuronal plateau potentials. Journal of Neurophysiology. 89(1): 416.
Hsieh CL., Hsueh IP, Chiang F, & Lin P. (1998). Inter-rater reliability and validity of the action research arm test in stroke patients. Age and Ageing, 27, 107-113. Hsieh JTC, Wolfe DL, Miller WC, Curt A.(2008). Spasticity outcome measures in spinal cord injury: Psychometric properties and clinical utility.Spinal cord. 46(2), 86-95.
Hsueh I, Lin J, Jeng JS, Hsieh CL.(2002). Comparison of the psychometric characteristics of the functional independence measure, 5 item Barthel index, and 10 item Barthel index in patients with stroke. Journal of Neurology, Neurosurgery & Psychiatry 73(2): 188. Jastrzab G, Kerr S, Fairbrother G. (2009). Misinterpretation of the Faces Pain Scale-Revised in adult clinical practice. Acute Pain.11( 2): 51-55.
Jebsen RH., Taylor N, Trieschmann RB., Trotter MJ., & Howard LA. (1969). An objective and standardized test of hand function. Archives of Physical Medicine and Rehabilitation, 50, 311-319. Jowers Ware L, Epps CD, Herr KH, Packard A. (2006). Evaluation of the Revised Pain Scale, Verbal Descriptor Scale, Numeric Rating Scale, and Iowa Pain Thermometer in Older Minority Adults. Pain Management Nursing. 7(3): 117-125. Keith RA,Granger CV, Hamilton BB, Sherwin FS. (1987). The functional independence measure: a new tool for rehabilitation. Advances in Clinical Rehabilitation. 1: 6-18. Kohler F, Dickson, H, Redmond H, Estell J, Connolly C. (2009). Agreement of functional independence measure item scores in patients transferred from one rehabilitation setting to another. European Journal of Physical and Rehabilitation Medicine. Krebs EE, Carey TS, Weinberger M. (2007). Accuracy of the pain numeric rating scale as a screening test in primary care. Journal of General Internal Medicine 22(10): 1453-1458. Kurtais Y, Kucukdeveci A, Elhan A, Yilmax A, Kalli T, Tur BS, Tennant A. (2009). Psychometric properties of the Rivermead Motor Assessment: its utility in stroke. Journal of Rehabilitation Medicine. 41(13): 1055-61.
21
Law M, Polatajko H, Pollock N, Carswell A, Baptiste S, & McColl, M. (1994). Canadian Occupational Performance Measure. CAOT Publication come measures in spinal cord injury: psychometric properties and clinical utility. Spinal Cord 46(2): 86-95. Li L, Liu X, Herr K. (2007). Postoperative Pain Intensity Assessment: A comparison of four scales in Chinese adults. Pain Medicine. 8(3): 223-234.
Lin K-C., Chuang L-L., Wu C-Y., Hseih Y-W. & Chang W-Y. (2010). Responsiveness and validity of three dexterous function measures in stroke rehabilitation. Journal of Rehabilitation Research and Development, 47(6), 563-572. Low Choy N, Kuys S, Richards M and Isles R (2002); Measurement of functional ability following traumatic brain injury using the Clinical Outcomes Variable Scale: A reliability study. Australian Journal of Physiotherapy.48: 35-39.
Lyle, R.C. (1981). A performance test for assessment of upper limb function in physical rehabilitation treatment and research. International Journal of Rehabilitation and Research, 4, 483-492.
Macfarlane A, Turner-Stokes L, De Souza L. (2002). The Associated Reaction Rating Scale: a clinical tool to measure associated reactions in the hemiplegic upper limb. Clinical Rehabilitation.16(7):726-35
Malouin F., Pichard L., Bonneau C., Durand A., Corriveau D. (1994). Evaluating motor recovery early after stroke: comparison of the Fugl-Meyer Assessment and the Motor Assessment Scale. Archives of Physical Medicine and Rehabilitation. 75(11), 1206-1212.
Mathiowetz V., Weber K., Kashman N., & Volland, G. (1985). Adult norms for the nine hole peg test of finger dexterity. Occupational Therapy Journal of Research, 5, 24 -33.
McGinnis G. E., Seward M. L., DeJong G., Osberg, J. S. (1986). Program evaluation of physical medicine and rehabilitation departments using self-report Barthel. Archives of Physical Medicine and Rehabilitation. 14, 61-65. Mossberg KA. (2003). Reliability of a timed walk test in persons with acquired brain injury. Archives of Physical Medicine and Rehabilitation .82:385-390. Patel M., Coshall C., Lawrence E. G., Rudd A, Wolfe,C. D. (2001). Recovery from poststroke urinary incontinence: Associated factors and impact on outcome. Journal of the American Geriatrics Society, 49(9), 1229-1233 Pedersen PM, Jorgensen HS, Nakayama H, Raaschou HO, Olsen TS. (1997). Comprehensive assessment of activities of daily living in stroke. The Copenhagen Stroke Study. Archives of Physical Medicine and Rehabilitation, 78, 161-165. Peolsson A, Hedlund R, Öberg B (2001). Intra- and inter-tester reliability and reference values for hand strength. Journal of Rehabilitation Medicine. 33 (2001), 36–41. Pollak, N., Rheault, W., Stoecker JL. (1996). Reliability and validity of the FIM for persons aged 80 years and above from a multilevel continuing care retirement community. Archives of Physical Medicine and Rehabilitation 77: 1056-1061.
Poole JL., Whitney SL. (1988). Motor assessment scale for stroke patients: concurrent validity and interrater reliability. Archives of Physical Medicine and Rehabilitation, 69(3), 195-197.
Priebe MM, Sherwood AM, Thornby JI, Kharas NF, Markowski J. (1996). Clinical assessment of spasticity in spinal cord injury: a multidimensional problem. Archives of Physical Medicine and Rehabilitation. 77:712-16.
Prosiegel M., Bottger S., Schenk T. (1996). Der Erwertiertr Barthel Index (EBI)-eine neue Skala zur Erfassung von Fahigkeitsstorungen bei neurologischen patieneten. Neurological Rehabilitation. 1, 7-13. Rockwood K, Stokee P, Howard K, Mallery I. (1996). Use of goal attainment scaling to measure treatment effects in an anti-dementia drug trial. Neuroepidemiology; 15: 330-8. Rossier P, Wade DT. (2001). Validity and Reliability Comparison of 4 Mobility Measures in Patients Presenting with Neurological Impairment. Archives of Physical Medicine Rehabilitation. 82: 9-13.
22
Sacks L, Yee K, Huijbregts M, Miller P, Aggett T, Salbach N. Validation of the Activity Inventory of the Chedoke-McMaster Stroke Assessment and the Clinical Outcome Variables Scale to evaluate mobility in geriatric clients. Journal of Rehabilitation Medicine (Stiftelsen Rehabiliteringsinformation) [serial on the Internet]. (2010), [cited May 30, 2011]; 42(1): 90-92.
Salter K, Jutai J, Foley N, Teasell R. (2010). Clinical Outcome Variables Scale: A retrospective validation study in patients after stroke. Journal of Rehabilitation Medicine. 42(7):609-13. Schlosser RW. (2004). Goal attainment scale as a clinical measurement technique in communication disorders: A critical review. Journal of Communication Disorders. 37(3): 217-239. Schuling J, de Haan R, Limburg M, Groenier KH. (1993). The Frenchay Activities Index. Assessment of functional status in stroke patients. Stroke. 24;1173-1177.
Seaby, L. and Torrance, G. (1989). Reliability of a physiotherapy functional assessment used in a rehabilitation setting. Physiotherapy Canada. 41: 264-271.
Sharma S, Schumacher HR, McLellan AT. (1994). Evaluation of the Jebsen Hand Function Test for use in patients with rheumatoid arthritis. Arthritis Care Research, 7:16–9.
Sharrack, B, Hughes, RA, Soudain S, Dunn G. (1999). The psychometric properties of clinical rating scales used in multiple sclerosis. Brain. 122 ( Pt 1): 141-159. Skilbeck C. E., Wade D. T., Hewer R. L., Wood V. A. (1983). Recovery after stroke. Journal of Neurology and Neurosurgical Psychiatry, 46, 5-8. Snow AL, Weber JB, O’Malley KJ, Cody M, Beck C, Bruera E, Ashton A, Kunik ME. (2004). NOPPAIN: A Nursing Assistant-Administered Pain Assessment Instrument for Use in Dementia. Dementia and Geriatric Cognitive Disorders. 17:240-246. Steffen TM, Hacker TA, Mollinger L. (2002). Age and Gender Related Test Performance in Community Dwelling Elderly People: 6 minute walk test, Berg Balance Scale, Timed Up and Go Test and Gait Speeds. Physical Therapy. 82:128-137. Stolee P, Rockwood K, Fox RA, Streiner DL (1992). The use of goal attainment scaling in a geriatric care setting. Journal of the American Geriatric Society. 40:574-78.
Sze K. H., Wong E., Leung H. Y., Woo J. (2001). Falls among Chinese stroke patients during rehabilitation. Archives of Physical Medicine and Rehabilitation. 82(9), 1219-1225.
Taciser K, Goksel KA, Gunaydin R, Koc, A, Eltundal E. (2011). Inter-reater reliability of the Ashworth Scale and Modified Ashworth Scale in assessing poststoke elbow flexor spasticity. International Journal of Rehabilitation. 34(1): 59-64.
Tilling, K., Sterne, J. A. C., Rudd, A. G., Glass, T. A., Wityk, R. J., Wolfe, C. D. A. (2001). A New Method for Predicting Recovery After Stroke. Stroke, 32, 2867.
Tur, B. S., Gursel, Y. K., et al. (2003). Rehabilitation outcome of Turkish stroke patients: in a team approach setting. International Journal of Rehabilitation Research. 26(4): 271-277.
Wade D. T., Hewer R. L. (1987). Functional abilities after stroke: measurement, natural history, and prognosis. Journal of Neurology and Neurosurgical Psychiatry. 50, 177-182. Williams N, Love S, Gibson N, Blair E. Reliability of the Australian Spasticity Assessment Scale. (2008). Proceedings of the International CP Conference, Sydney, Australia.
van der Lee J.H, Beckerman H., Lankhorst G.J., Bouter L.M. (2001a). The responsiveness of the Action Research Arm Test and the Fugl-Meyer Assessment Scale in chronic stroke patients. Journal of Rehabilitation Medicine, 33, 110-113.
23
Van der Putten, JJMF, Hobart JC, Freeman JA, Thompson AJ. (1999).Measuring change in disability after inpatient rehabilitation: comparison of the responsiveness of the Barthel Index and the Functional Independence Measure. Journal of Neurology and Neurosurgical Psychiatry. 66:480-484. Van Hedel HJ Wirz M, Dietz V. (2005). Assessing Walking Ability in Subjects with Spinal Cord Injury: Validity and Reliability of 3 Walking tests. Archives of Physical Medicine and Rehabilitation. 86:190-196. Vliet Vlieland TPM, van der Wijk TP, Jolie MM, Zwinderman AH (1996). Determinants of hand function in patients with rheumatoid arthritis. Journal of Rheumatology; 23:835-40. Voepel-Lewis T, Malviya S. (2003). FLACC Behavioral Pain Assessment Scale: a comparison with the child’s self report. Pediatric Nursing. 29(3). Voepel-Lewis T, Zanotti J, Dammeyer JA, Merkel S. (2010). Reliability and Validity of the FACE, Legs, Activity, Cry, Consolability Behavioral Tool in Assessing Acute Pain in Critically Ill Patients. American Journal of Critical Care. 19(1): 55-61. Wyller, T.G. (1998). Early discharge after stroke. British Medical Journal (Intl Ed); 316:1168-1169.
Yozbatiran N., Der-Yerghiaian L., & Cramer S.C. (2008). A standardized approach to performing the action research arm test. Neurorehabilitation & Neural Repair, 22(1), 78-90. Compiled by: Jacqueline Behr, Jeanette Boily, Nancy Cho, Alison Hoens, Deirdre Lee, Sandy Leznoff, Tina Moran, Sarah Rowe