“the faculty practice plan & our strategic partnership
TRANSCRIPT

“The Faculty Practice Plan & Our Strategic
Partnership with BJC”
Department of Pediatrics Leadership Development Program
February 28, 2018
Paul J. Scheel, MD
Assoc. Vice Chancellor for Clinical Affairs
CEO, Washington University Physicians Faculty Group Practice

2
Depends on Who You Ask ?

3
What is BJC ?
BJC is an Integrated Health Care Delivery System
Initially formed as merger between Barnes, Jewish, Christian hospitals
BJC Hospitals Include: Alton Memorial, St Peters, Progress West, Christian,
Parkland, Missouri Baptist, Barnes, St Louis Children’s, Belleville
Memorial , Boone, West County
Goldfarb School of Nursing
BJC Homecare
BJC Medical Group

4
Institutional Relationships
Washington University
Teaching Hospitals:• BJH
• SLCH
• BWC
Board of Trustees
Chancellor
School of
Medicine
Dean & Executive Faculty
Faculty Group
Practice
BJC Health Care
Board of Directors
CEO
Community
Hospitals
Affiliation
Agreement

5
WUSM-Teaching Hospital Affiliation Agreement
WUSM:
• Provides medical staff and medical direction for hospital clinical programs
• Supervises BJH/SLCH resident and fellowship training programs
• Limits its hospital practice activities to BJH/SLCH exclusively unless the parties agree
otherwise
• Assigns to BJH/SLCH/BJWCH the right to own and operate most outpatient technical
services offered on the WUMC campus
In Exchange, WUSM receives:
• Partial payment for GME supervision costs ($7.9m in CY15)
• Above-line medical coverage payments for pathology, anesthesiology, hospitalists, and
emergency medicine professional services
• 45% of teaching hospital operating margins (BJH/SLCH/BJWCH)

6
Hospital Support Funds Flow
30%Unrestricted
(BLS)GME Payment ($7.9M)
BLS = 45% of Op Margin
45% Dean
55% FPP Clinical
Program Development
Distributed to Clinical Depts based on set
allocation formula
15% Strategic
Investment Fund

7
WU Physicians Clinical Practice
• Ranks in top 5 of the nation’s 123 academic group practices
1,433 full-time faculty physicians (76 sub-specialties)
228 Nurse Practitioners, 36 PA’s, 124 CRNA’s plus PT, OT & Audiology
69 employed primary care providers thru WUCA (Washington University Clinical Associates)
3,768,961 total patient encounters in FY16 including:
1,082,665 outpatient visits & 1,114,682 procedures
65,268 surgeries
90,878 hospital discharges
Account for 98% of discharges from BJH & SLCH
• 67% of clinical activity on Washington University Medical Center
Campus
• 33% of clinical activity occurs at 49 off-campus clinical program sites
8
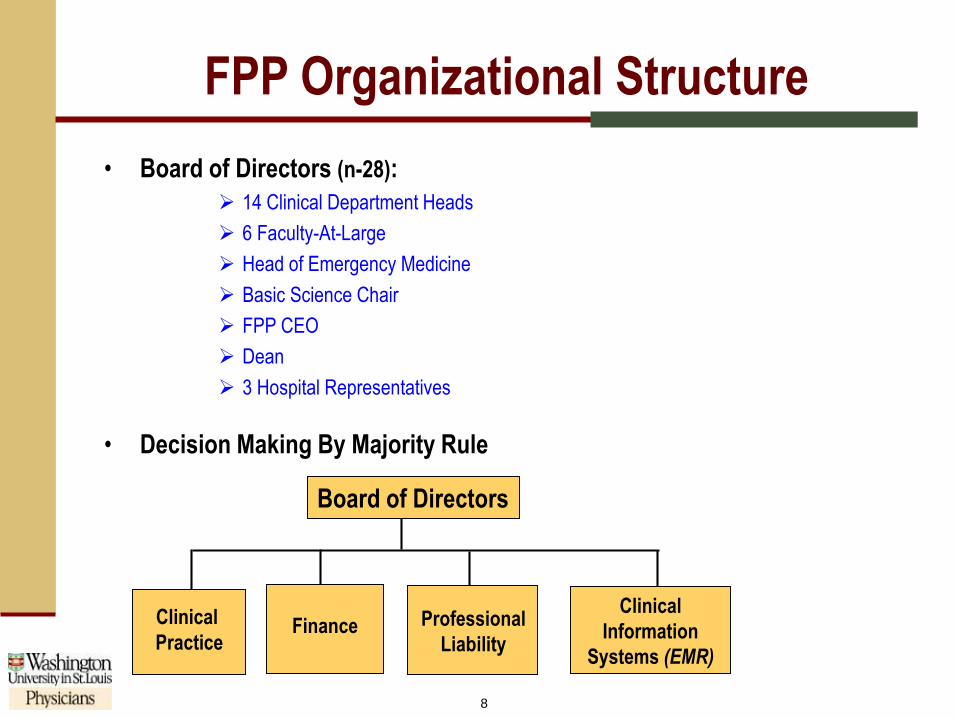
FPP Organizational Structure
Board of Directors
Clinical
Information
Systems (EMR)
Professional
Liability
Clinical
PracticeFinance
• Board of Directors (n-28):
14 Clinical Department Heads
6 Faculty-At-Large
Head of Emergency Medicine
Basic Science Chair
FPP CEO
Dean
3 Hospital Representatives
• Decision Making By Majority Rule

9
358 381 407 455
499 539 553
603 637
689 753
809 875
958
1,070 1,147
10.2
3.96.7
17.9
26.8
48.8
37.2 38.4 4037.1
57.354.3
58.6
70.775.9 73.8
9.2 21.9
21.4 24.9
27.2
-8.2 -8.5
16.4
3.4
11.0
20.2 22.5
11.1
17.7 17.3
5.6
-10
0
10
20
30
40
50
60
70
80
90
(100)
100
300
500
700
900
1,100
FY02 FY03 FY04 FY05 FY06 FY07 FY08 FY09 FY10 FY11 FY12 FY13 FY14 FY15 FY16 FY17
Clin
ical
Pra
ctic
e M
arg
in &
Pre
miu
ms
(mill
ion
s)
Clin
ical
Pra
ctic
e R
even
ue
(mill
ion
s)
Clinical Practice Revenue
Clinical Practice Margin
Premiums
Clinical Practice Revenue, Margin & Premiums
WUSM CLINICAL PRACTICE REVENUE, NET INCOME & PROFESSIONAL
LIABILITY COSTS1
In Millions
1 Margin in graph include rebates. Clinical Practice Margin includes Occupational Therapy, Physical Therapy, Physician Billing Services, Endowment Spending Distribution and Investment Income.2 CAGR = Compound Annual Growth Rate
Source: WUSM Finance, based on Hyperion reporting
FY02-FY17 Revenue CAGR2 = 8.1%
FY02-FY17 Margin CAGR2 = 14.1%
FY02-FY17 Premiums CAGR2 = -3.3%

10
Primary Functions
1) Provides key services & infrastructure for clinical departments
2) Serves as the focal point for establishing strategic direction and coordinating clinical program activities across WUSM’s 14 clinical departments and with our major teaching affiliates
3) Oversees annual allocation of Clinical Program Development Funds
4) Establishes school-wide clinical practice policies
5) Public policy advocacy (ex: tort reform, safety net sustainability)
Washington University PhysiciansFaculty Practice Plan

11
Core FPP Services
Billing &Collections
Services
Communications & Marketing
Patient Access & Service
Quality
Clinical Strategic& Operational
Planning
WUSM Clinical Practice
Managed CareContracting
ReferringPhysician
Relationships
ClinicalInformation
Systems(EMR, etc)

12
Prior Uses of CPD Funds
1 Includes professional liability insurance cost relief, clinical practice space build out and clinical equipment requests,
time-limited clinical staff support, primary care loan forgiveness program, CAM TI Allowance, South County Phase 1
construction costs, WUCA expansion, ICD-10, CAM Expansion, South County Phase 2 construction costs and
Sleep Medicine Center construction costs.
Category Allocated
Dollars
(millions)
% of Total # of
Funded
Recruits (&/or
Proposals)
Faculty Recruitment $80.3 70% 283
EMR Infrastructure Support $14.1 12% 12
One-Time Clinical Practice O/H1 $20.5 18% 25
TOTAL $114.9m 100%
12 Year History

13
FPP Key Clinical Priorities

14
FPP Key Clinical Priorities
1) Work collaboratively with BJH and SLCH to develop and implement a plan for
Hospital Facility Expansion and Renewal on the WUMC campus
• Reconfigure SLCH’s bed platform to expand the critical care bed base, create private rooms
and meet the growing demand for pediatric diagnostic and treatment services
• Create an innovative, integrated Women’s and Infants Program
• Expand adult medical oncology inpatient bed platform on the north campus
• Expansion of the CAM to the BJH Center for Outpatient Health (COH)
2) Work in partnership with BJH and SLCH to expand our off-campus ambulatory
programs:
• South County Phase 1 Facility - SCC Satellite (opened Jan 7, 2013)
• New West County Pediatric Ambulatory Satellite (June 2015)
• South County – Phase 2 Ambulatory Program (April 19, 2016)
• Expansion of BJSPH SCC (mid 2016)
• Further Ambulatory Expansion and Hospital Replacement at BJWCH (late 2018)
• Planning new SCC satellites in North County and in Shiloh, Illinois

15
9.6% 12.5% 13.8% 8.8% 29.3% 29.5%% Change from
Previous Year
$21.7$24.4
$27.8$30.2
$39.1
$50.7
$0
$4
$8
$12
$16$20
$24
$28
$32
$36$40
$44
$48
$52
$56
FY12 FY13 FY14 FY15 FY16 FY17
Off-Campus Activity Drives Significant Profit
• Off-campus clinical activity accounted for 34.6% of WUSM’s total revenue in FY17 and
generated a premium of $50.7M in incremental income as compared to an equivalent volume
and mix of services on the WUMC campus
Source: WUSM PBS Reporting Services
Off-Campus Incremental Net Income (millions)
FY12-FY17 CAGR – 18.2%
14

16
FPP Key Clinical Initiatives
3) Secure and expand WUSM’s primary care physician referral base
4) Implement new EHR
5) Increase access
6) Improve patient experience
7) Safety

17
6 Key Revenue Challenges
1) Flat market size, making it more difficult to grow clinical volumes
2) 1% per year expected shift from commercial payors to Medicare until 2030 as the “baby
boomer” generation ages
3) Potential erosion of historical referral patterns due to physician employment by
competitor hospitals
4) Growth in uncompensated care costs due to increase in charity care & below cost
reimbursement from Medicare and Medicaid
5) Changes in private sector health benefit designs and health plan market consolidation:
• High deductible health plan designs
• Narrow network and tiered network products
• Steerage programs
• Defined contribution health insurance models
• Insurance market consolidation
6) Shift from FFS to Value-Based Payment models with downside risk

18
36.1% 36.8% 37.3%
14.1% 13.6% 13.4%
3.8% 3.9% 4.3%
19.2% 19.9% 20.3%
21.3% 20.8% 20.2%
5.1% 4.6% 4.2%
0.4% 0.3% 0.3%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
FY15 FY16 FY17
Commercial
Other
PPO
HMO
Self Pay
Medicaid
Medicare
“Baby Boomer” Payor Mix Shift
• Medicare now accounts for 37.3% of WUSM’s total payor mix, up 0.5% from the
prior year
Based on billed charges; Other includes transplant, international, hospital contracts, and workers compensation; Includes insurance co-payments; Managed Medicaid is included in Medicaid percentage.
Source: WUSM PBS Reporting Services
50.4%50.2% 50.7%

19
% To WUSM
Total Charges0.3% 1.9% 20.2% 20.3% 2.3% 6.3% 4.3% 37.3% 7.1%
148% 153%
139% 136%
99% 90%
59% 67%
53%
0%
20%
40%
60%
80%
100%
120%
140%
160%
180%
Commercial Global TX PPO HMO Other Managed
Medicaid
Self Pay Medicare Traditional
Medicaid
Payor Reimbursement as a Percent of Clinical Practice Costs
• Medicare and Traditional Medicaid reimbursement is below the fully loaded cost of providing these services, covering 67%
and 53% of costs, respectively.
Government Payors Do Not Cover the Cost of Care
Payor Trends Relative to WUSM Clinical Practice Costs (FY17)
1Other includes Special Contracts; Non-contracted HMO, PPO, and POS; Workers Comp; Railroad employees; TRICARE; and Medicaid Appeals.
WUSM cost as a percent of Medicare RBRVS = 1/0.67 = 150%
Source: WUSM PBS Reporting Services44.4% of total charges
Breakeven
Point

20
Uncompensated Care Trends
On a cost-basis, WUSM provided $97.9M in uncompensated care during FY17, an 15.9% increase over FY16
Under-reimbursed care for Medicare and Medicaid patients accounted for $84.1M of the total, a 13.2% increase
from FY16
Bad debt increased 11.8% in FY17 to $7.8M while charity discounts increased from $3.2M to $6.0M
$61.8$74.3
$84.1
$2.1
$3.2
$6.0
$7.8
$7.0
$7.8
$71.8
$84.5
$97.9
$0
$20
$40
$60
$80
$100
$120
FY15 FY16 FY17
Under-Reimbursed Care Charity Discounts Bad Debt

21
How Do We Survive ?
- Increase market share commercial business
- Expand primary market
- Focus on regional, national, international referrals

22

23