the effects of glenohumeral joint mobilization
TRANSCRIPT
ABSTRACT
THE EFFECTS OF GLENOHUMERAL JOINT MOBILIZATION INTERVENTIONS VS. INTRA-ARTICULAR CORTICOSTEROID
INJECTIONS IN ADULT PATIENTS WITH EARLY STAGE ADHESIVE CAPSULITIS: A META-ANALYSIS
Objectives: To examine the effects of glenohumeral joint mobilization
interventions on pain and ROM in patients with adhesive capsulitis compared to intra-
articular corticosteroid injections.
Methods: Studies comparing glenohumeral joint mobilizations and corticosteroid
injections for patients with adhesive capsulitis were investigated. These studies
contained similar participants, study time frames, interventions, and outcome measures.
Studies were analyzed to determine the treatment effect and heterogeneity between
studies.
Results: Four studies were included. The combined effect size for pain on VAS
resulted in a moderate effect size of 0.88 largely favoring corticosteroids injection over
joint mobilization for pain relief. On the other hand, the combined effect size for ER
ROM was 0.29 which moderately favored towards the joint mobilization. Heterogeneity
was found between the 4 studies.
Conclusion: A single intraarticular injection of corticosteroid administered during
the early stage adhesive capsulitis, combined with a joint mobilization program, is
effective in improving shoulder pain and disability in patients with adhesive capsulitis.
Supervised physiotherapy in conjunction with the corticosteroid treatment provides faster
improvement in shoulder ROM. Joint mobilization when used alone offer limited efficacy
in the management of adhesive capsulitis due to the weak clinical evidence.
ii
Study Design: A meta-analysis of clinical studies examining the effects of
glenohumeral joint mobilization interventions on pain and ROM in patients with adhesive
capsulitis compared to intra-articular corticosteroid injections.
Justin Lemoine May 2020

THE EFFECTS OF GLENOHUMERAL JOINT MOBILIZATION
INTERVENTIONS VS. INTRA-ARTICULAR CORTICOSTEROID
INJECTIONS IN ADULT PATIENTS WITH EARLY STAGE
ADHESIVE CAPSULITIS: A META-ANALYSIS
by
Justin Lemoine
A project
submitted in partial
fulfillment of the requirements for the degree of
Doctor of Physical Therapy
in the Department of Physical Therapy
College of Health and Human Services
California State University, Fresno
May 2020
APPROVED
For the Department of Physical Therapy:
We, the undersigned, certify that the project of the following student meets the required standards of scholarship, format, and style of the university and the student's graduate degree program for the awarding of the doctoral degree. Justin Lemoine
Project Author
Nupur Hajela (Chair) Physical Therapy
Deborah Walker Physical Therapy
For the University Graduate Committee:
Dean, Division of Graduate Studies
AUTHORIZATION FOR REPRODUCTION
OF DOCTORAL PROJECT
X I grant permission for the reproduction of this project in part or in its
entirety without further authorization from me, on the condition that
the person or agency requesting reproduction absorbs the cost and
provides proper acknowledgment of authorship.
Permission to reproduce this project in part or in its entirety must be
obtained from me.
Signature of project author:
ACKNOWLEDGMENTS
First, I would like to thank my chair Dr. Nupur Hajela and my committee member
Dr. Deborah Walker for their guidance in the development of this meta-analysis. Next, I
would like to thank my parents Kevin and Jamie Lemoine and my brother Michael
Lemoine for instilling in me the values of diligence, grit, and resilience in the face of
adversity. I would also like to give a special thanks to my girlfriend Melissa Orozco for
the constant encouragement, feedback, and moral support. Lastly, I would like to give a
huge thanks to the Fresno State’s DPT class of 2020 for making these last 3 years so
special and memorable.
TABLE OF CONTENTS
Page
LIST OF TABLES .................................................................................................................vii
LIST OF FIGURES ............................................................................................................. viii
BACKGROUND ...................................................................................................................... 1
Introduction ...................................................................................................................... 1
Prevalence and Risk Factors of Adhesive Capsulitis .................................................... 1
Classification and Pathophysiology ................................................................................ 2
Clinical Course and Interventions of Adhesive Capsulitis ............................................ 2
METHODS ............................................................................................................................... 7
Search Strategy................................................................................................................. 7
Eligibility Criteria ............................................................................................................ 7
Definitions ........................................................................................................................ 8
Quality Appraisal ............................................................................................................. 9
Data Collection Process ................................................................................................... 9
Outcome Measures......................................................................................................... 10
Statistical Analysis ......................................................................................................... 10
RESULTS ............................................................................................................................... 12
Study Selection............................................................................................................... 12
Study Characteristics ..................................................................................................... 12
Outcome Assessment ..................................................................................................... 13
Synthesis of Results ....................................................................................................... 14
DISCUSSION......................................................................................................................... 15
Review of Results .......................................................................................................... 15
Limitations of Meta-Analysis........................................................................................ 16
Page
vi vi
Threats to Internal Validity ........................................................................................... 17
Literature Support .......................................................................................................... 19
Clinical Implications ...................................................................................................... 22
Future Research .............................................................................................................. 23
Conclusion ...................................................................................................................... 25
REFERENCES ....................................................................................................................... 26
TABLES ................................................................................................................................. 32
APPENDICES ........................................................................................................................ 39
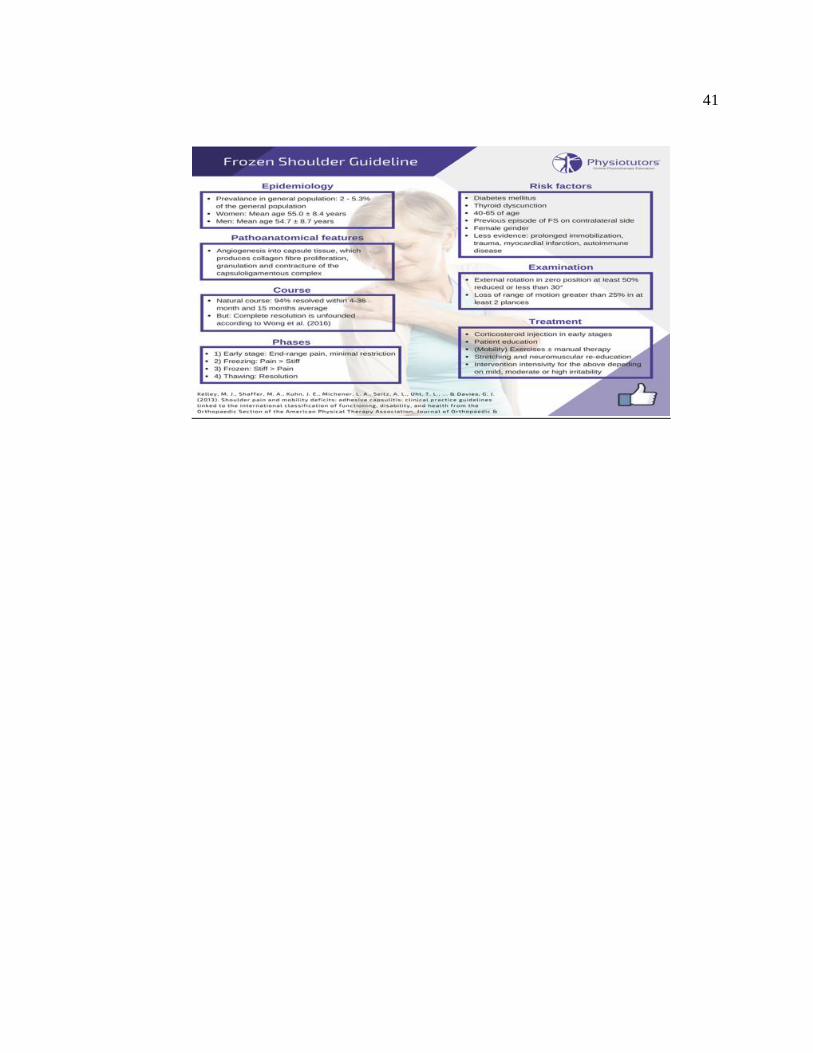
APPENDIX A: FROZEN SHOULDER GUIDELINE ....................................................... 40
APPENDIX B: FROZEN SHOULDER STAGES .............................................................. 42
LIST OF TABLES
Page
Table 1: Study Selection ........................................................................................................ 33
Table 2: PEDro Scores ........................................................................................................... 34
Table 3: Study Characteristics ............................................................................................... 35
Table 4: Pain on VAS ............................................................................................................ 36
Table 5: ER ROM .................................................................................................................. 37
LIST OF FIGURES
Page
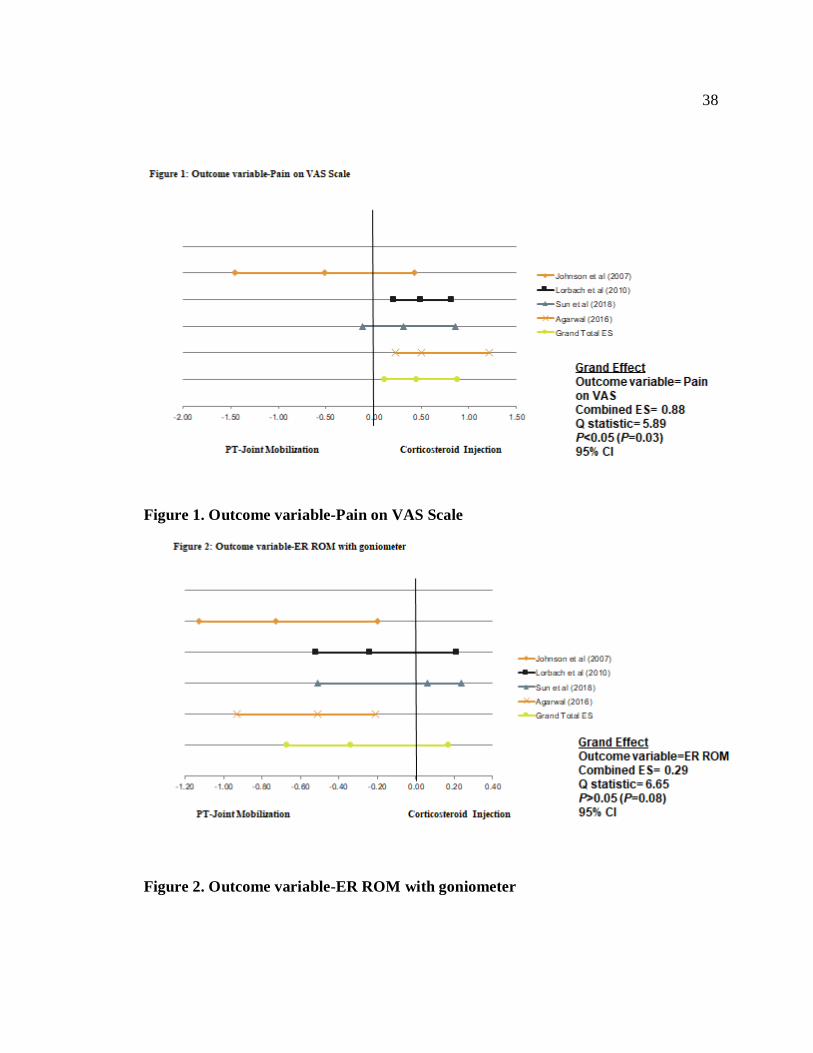
Figure 1. Outcome variable-Pain on VAS Scale .................................................................. 38
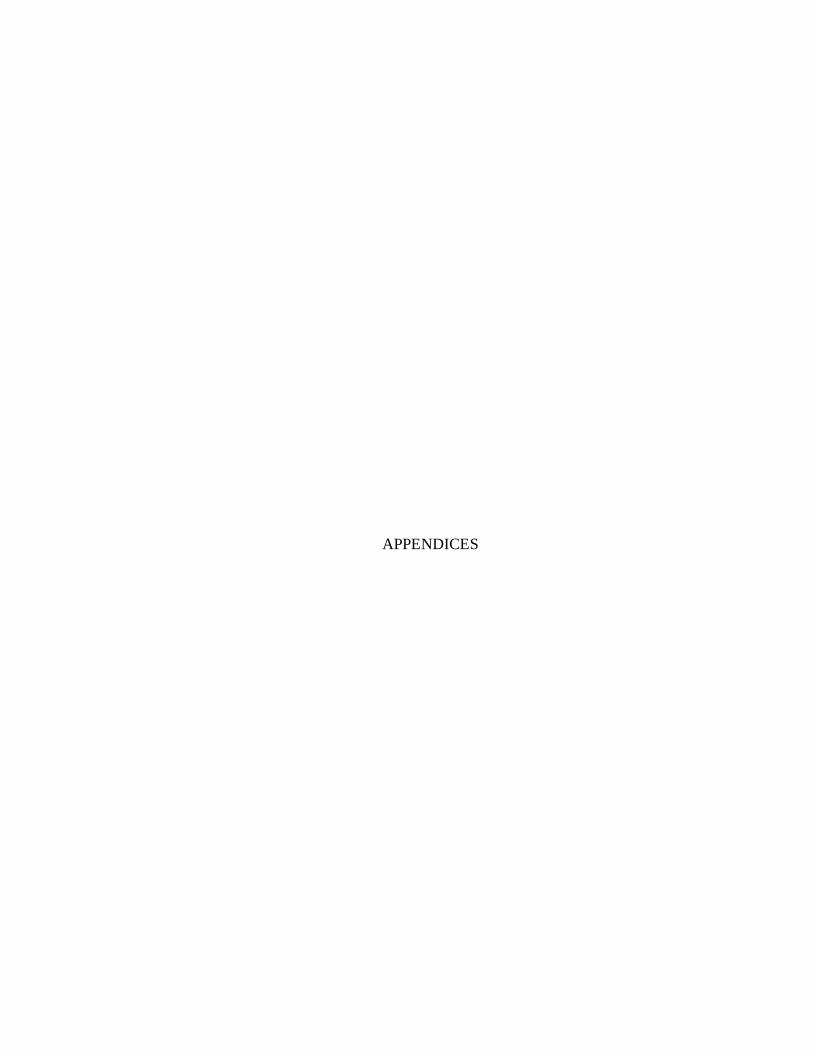
Figure 2. Outcome variable-ER ROM with goniometer...................................................... 38
BACKGROUND
Introduction
The American Shoulder and Elbow Surgeons (ASES) defines adhesive capsulitis
as “a condition of uncertain etiology characterized by significant restriction of both active
and passive shoulder motion that occurs in the absence of a known intrinsic shoulder
disorder”.1 Adhesive Capsulitis (AC) is one of the most commonly known causes of
shoulder pain and disability, a clinical term used for a vague and interchangeable term-
Frozen Shoulder (FS).2 The condition is considered fibrosis of the glenohumeral joint
capsule with a chronic inflammatory response resulting in pain, limited mobility, and
disability of the affected upper-extremity.2,3
Prevalence and Risk Factors of Adhesive Capsulitis
The incidence of adhesive capsulitis is approximately 3 to 5% of the general
population.4 The condition affects females (70%) more than males between the fourth
and sixth decade of life.4 Patients with both Type I and Type II diabetes are 20% more
prone to adhesive capsulitis and have worse measurable functional outcome.2 Around
25% patients following stroke reported adhesive capsulitis as one of the common
complications within 6 months of stroke onset.2 Other risk factors associated for AC are
elevated cytokine levels resulting in synovial inflammation, patients with thyroid disease,
prolonged shoulder immobilization, Dupuytren’s contracture, and female gender.5 It
often involves the non-dominant shoulder, however, involvement of bilateral shoulders
have been reported in about 50% of the cases.6 Rigorous economic evaluation on
shoulder disorders demonstrated that shoulder pathologies are a growing contributor to
the health care costs.7
2
2
Classification and Pathophysiology
The pathophysiology and underlying etiology of AC still remains controversial as
whether to define the disease process as fibrosis contractures or inflammatory changes in
the joint capsule.8 However, it is generally well accepted that the onset of adhesive
capsulitis involves an inflammatory as well as fibrotic process.2,8,9 The underlying
pathology of adhesive capsulitis is considered as a chronic inflammatory response with
fibroblastic proliferation of the joint capsule mediated by cytokines, growth factors, and
immune cells.10 The underlying condition initiates as an immune response that worsens
the inflammatory synovitis and subsequently leads to capsular fibrosis.9,11 The
immunological components such as mast cells, B-lymphocytes, and macrophages have
been reported in the pathogenesis of adhesive capsulitis which proceeds with
inflammatory synovitis and capsular fibrosis.8,11 Diagnostic imaging and arthroscopic
studies have shown that the glenohumeral capsular tissue including the coracohumeral
ligament in the rotator cuff interval is the primary pathological site for adhesive
capsulitis.12
The process of AC passes through several stages, which reflect the series of
processes from capsular inflammation and fibrosis to spontaneous resolution of this
fibrosis.10,11 Adhesive capsulitis can be classified as primary (idiopathic) or secondary.
Primary AC can occur without any known etiology or trauma and results from a chronic
inflammatory changes in the joint capsule.2 Secondary AC can occur as a result of known
shoulder trauma or injury, shoulder surgery complication, post cerebero-vascular injury,
metabolic disease, rotator cuff injuries, and cardio-vascular diseases.2
Clinical Course and Interventions of Adhesive Capsulitis
Adhesive capsulitis is a self-limiting condition with most of the patients achieving
spontaneous recovery within 2-3 years of initial onset.13,14 However, up-to 40% still
reported persistent symptoms such as loss of ER and consistent pain, and around 15%
3
3
had some degree of permanent functional loss of the affected extremity.13,14 The
diagnosis of adhesive capsulitis is usually made on the medical history and clinical
presentation of patient’s symptoms of a painful and stiff shoulder joint with the gradual
lack of active and passive range of motion. Loss of external rotation motion with an intact
rotator cuff musculature is the hallmark sign during the early stages of adhesive
capsulitis.5,6 The restriction of passive shoulder range of motion, particularly in forward
flexion, abduction, external rotation, and internal rotation is the key clinical feature.15 The
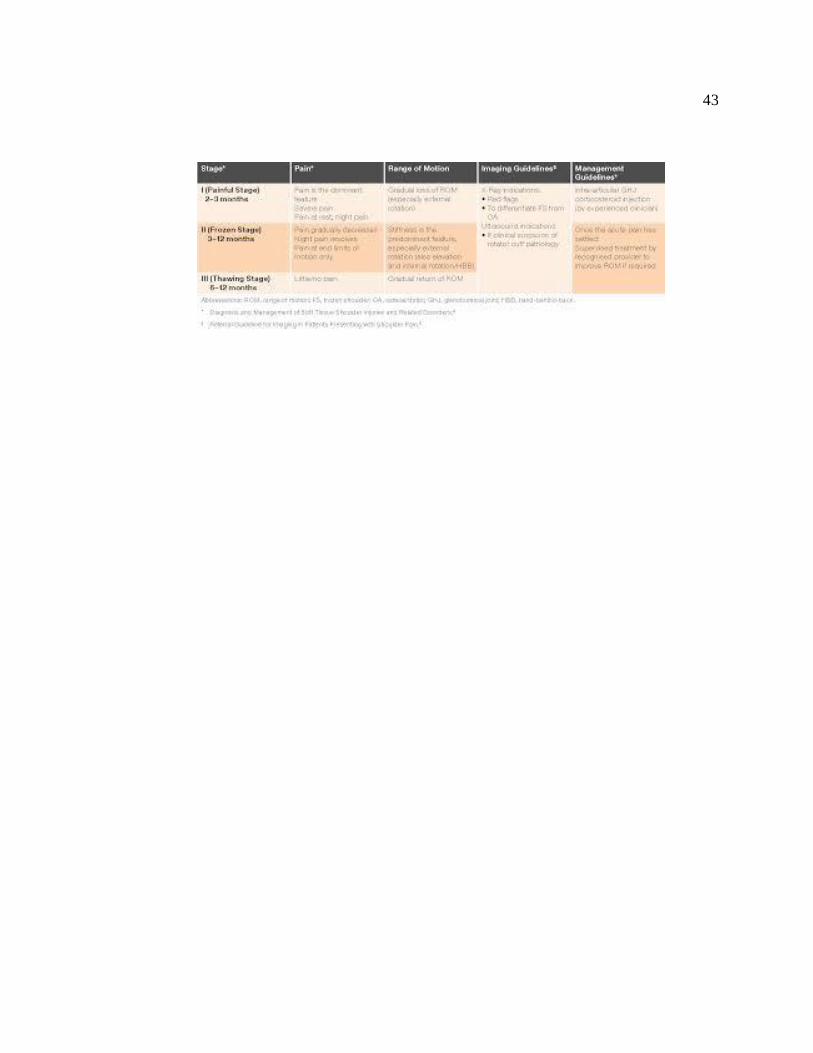
natural course of AC is described in the 4 clinical stages which have been correlated with
clinical and pathological findings.3 The initial stage is referred to as the painful shoulder
phase and symptoms persist for less than 3 months.3,16 This stage is characterized by the
onset of mild aching pain at the deltoid insertion site, inability to sleep on the affected
side, and mild loss of shoulder mobility.3,5,16 This stage sets the basis for vascular
synovitis and capsular hypertrophy of the glenohumeral joint capsule without any
adhesions or capsular contractures.3,16 The second stage, freezing stage is the early stage
and is marked by progressive moderate to severe pain along with loss of active and
passive range of motion, and lasts from 3 to 9 months.3 Early loss of external rotation
ROM with an intact rotator cuff muscle is the hallmark sign of early stages of adhesive
capsulitis.5 Arthroscopic pathological findings in this stage are thickened synovitis and
disorganized collagen deposition.3,16 The third stage, frozen stage is marked by
improvements in pain levels but stiffness and loss of functional mobility still persists.
This stage lasts from 4 to 20 months and is typically followed by 4 th stage (late or
chronic) thawing, the period of recovery marked by gradual improvements in the
mobility and pain levels which can take from 5 to 24 months.3,5 This meta-analysis will
focus on the early stage adhesive capsulitis (stage 1 & 2), since this stage is marked by
significant pain and restriction of all active and passive shoulder movements with at-least
50% loss of external rotation motion, causing impairments in the daily functional
4
4
activities of behind the back and overhead reaching, disturbed sleeping pattern, and lying
on the affected side due to pain.3,5
Various treatment strategies have been advocated in the literature to treat adhesive
capsulitis, aiming at achieving anti-inflammatory and anti-adhesion.13,16–19 Currently,
there are no consensus guidelines describing which treatment is most effective for
adhesive capsulitis.16 The treatment regime follows a course of conservative measures
such as oral analgesics-NSAIDs, intra-articular steroid injections, physical therapy,
manipulation under anesthesia, and rarely includes more invasive surgical approaches-
capsular distention and arthroscopic capsular release.5,13,17,20 The most commonly used
interventions reported in the literature are intra-articular corticosteroid injections and a
course of physical therapy which includes thermotherapy, range of motion exercises,
capsular stretching, manual joint mobilization techniques, and a home based exercise
program.5,16,17,21 Despite several available intervention options, it remains unclear
whether to use 1 specific intervention (CSI, physical therapy, oral NSAID’s,
manipulation under anesthesia) or in combination due to the lack of well-established
clinical evidence.
Conservative treatment approaches including physical therapy, intra-articular
corticosteroid injections and oral Non-Steroidal Anti-inflammatory drugs (NSAID’s)
typically provide short term but limited long-term efficacy for adhesive capsulitis
regardless of the onset or chronicity of condition.13,16,18,21–23 Previous trials and literature
reviews have demonstrated that corticosteroid injections provides pain relief and
improvements in functional mobility on a short term basis up-to 6 weeks, and to a lesser
extent, in the long term.18,21,22,24 Several studies have examined the effect of
glenohumeral joint mobilization-anterior and posterior directed force grade I to IV-and
have found these to be beneficial to regain ROM and alleviate pain by reducing tissue
irritability in patients with AC.25–28 The purpose of joint mobilization is to increase

5
5
shoulder movements by stretching the joint capsule and thereby prevent capsular
contracture16 Clinically, treatment should vary depending on each stage and patient’s
impairment levels. Moreover, most of these studies favored corticosteroid injections over
other conservative interventions due to its immediate pain relief benefits by directly
targeting inflammatory process at the pathological site in the glenohumeral joint.15
A randomized controlled trial by Ranalletta et al (2016) compared corticosteroid
injections with oral NSAIDs on patients with early (freezing) stage AC. This study
showed that a single corticosteroid injection provides faster pain relief and improvements
in the shoulder mobility compared to oral analgesics.29 A systematic review by Blanchard
et al (2010) that compared intraarticular corticosteroid injections and physical therapy
interventions including gleno-humeral joint mobilizations for adhesive capsulitis patients
suggested steroid injections provided greater benefit when compared to physical therapy,
when introduced early in the treatment regime within the first 6 weeks. This study also
noted that the addition of physical therapy with steroid injections in the treatment regime
provided moderate effect on pain, external rotation range of motion and disability at 6
weeks follow-up period. A randomized control trial by Vermeulen et al (2006) compared
high grade (III & IV) gleno-humeral joint mobilization with low grade (I & II) and found
that high grade gleno-humeral joint mobilization was more effective in pain relief and
increasing functional mobility in patients with early stage AC. Johnson et al (2007)
compared anterior vs posterior joint mobilization in patients with adhesive capsulitis
diagnosis with specific restriction of external rotation ROM. Johnson et al (2007) found
that posterior joint glenohumeral mobilization is more effective than anterior to improve
external rotation ROM as well as for pain relief. This study did not compare mobilization
with other forms of treatment and did not assess the effect of mobilization on other
glenohumeral motions.26
6
6
The purpose of this meta-analysis is to determine the effectiveness of
glenohumeral joint mobilization interventions compared with intra-articular
corticosteroid injections in adult patients with early stage adhesive capsulitis, and to
measure the efficacy of long-term benefits of joint mobilization interventions to improve
shoulder functional mobility, specifically external rotation during the early stage AC.
Early stage AC includes stage I and II based on the Neviaser’s adhesive capsulitis
classification. The current review hypothesized that classification based on pathological
stages should be taken into consideration when deciding on various interventions for
adhesive capsulitis. Patient during early stages AC demonstrate increased pain and
functional mobility loss due to a higher level of tissue irritability from increased
inflammatory markers whereas, patients during the later or chronic stages will have low
tissue irritability.10,20 Current available literature has reviewed corticosteroid injections
with physical therapy in general and with oral analgesics, however, lacking direct
comparison of corticosteroid injections with joint mobilization. This review will focus
primarily on the effects of glenohumeral joint mobilization compared to intraarticular
corticosteroid injections for early stage (stage I & II) adhesive capsulitis patients.
This review also hypothesized that glenohumeral joint mobilization interventions
can reduce pain, improve range of motion ER and function in patients with early stage
adhesive capsulitis. Corticosteroid injections when administered during the initial stages
will provide pain relief due to anti-inflammatory effects and will facilitate recovery from
physical therapy interventions. This review may help to bridge the gap in the current
research on selecting the appropriate staging-based interventions for adhesive capsulitis.
METHODS
Search Strategy
The searches were started in August 2019 and concluded in November 2019 on
various databases including PubMed, Cochrane Library, and SportDiscus. The search
protocol and study design were developed in accordance with the Systematic Reviews
and Meta-Analysis (PRISMA) guidelines. The search terms used independently or in
combination for searching the databases are-adhesive capsulitis, frozen shoulder,
adhesive capsulitis interventions, corticosteroid injection, injection and joint
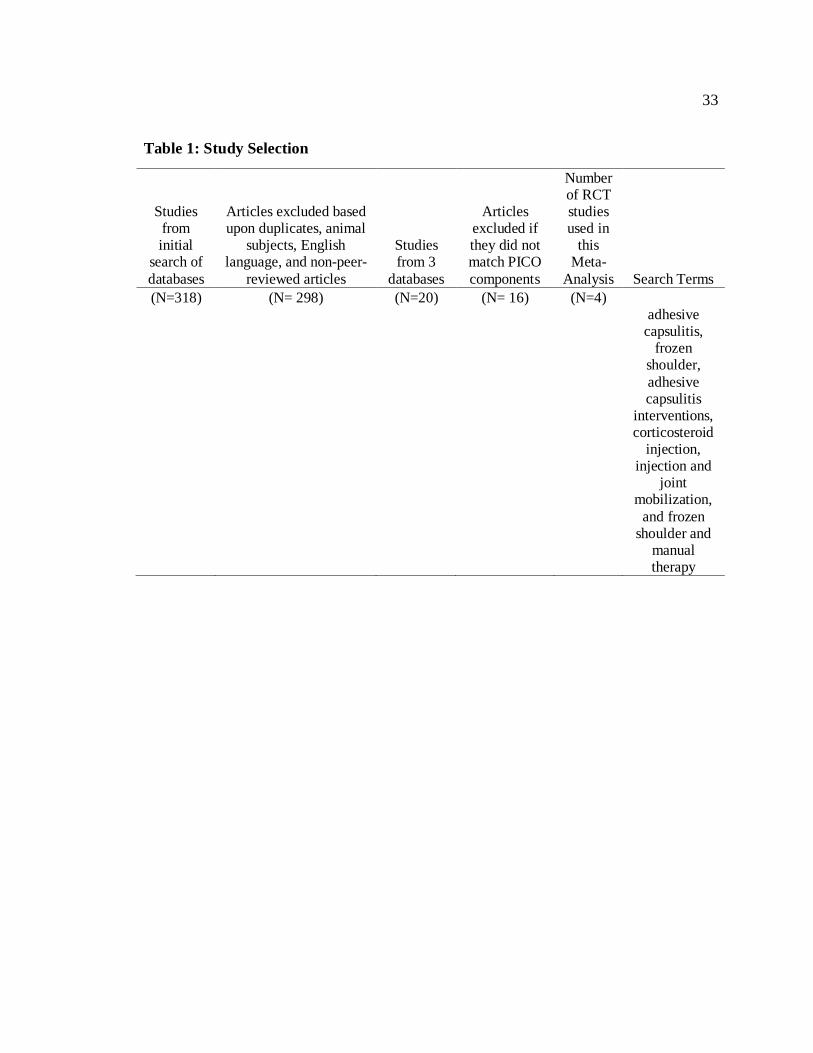
mobilization, and frozen shoulder and manual therapy. Table 1 indicates a comprehensive
list of search terms used to search and narrow the study search. A single reviewer
screened available articles and excluded them based on relevance, title, and abstracts.
Studies deemed to be relevant to the current meta-analysis were retrieved and assessed
independently by the reviewer. The filters applied in the databases for inclusion included
peer reviewed journal articles, English language only, abstracts, and title, human subjects,
and full-text articles were included in the search. A reviewer also performed a secondary
search by reviewing references of systematic reviews, randomized control trials, and
accepted articles.
Eligibility Criteria
The eligibility criteria were set for studies to be included in the current meta-
analysis. The studies were required to be in English language only, must be published in
a peer reviewed journal, and either a level 1, 2 or level 3 research design according to
Oxford Center for Evidence Based Medicine (OCEBM).30 Studies included both men and
women of age 18 to 65 years, with the subjective complaints of unilateral or bilateral
shoulder pain lasting at-least 3 months with associated loss of external rotation range of
motion of the affected shoulder. Due to the lack of a gold standard for diagnosis of
8
8
adhesive capsulitis or frozen shoulder, studies were selected if the participants had
subjective reports of pain and limited mobility in ER and abduction plane. Participants
must have had an established diagnosis of an early stage adhesive capsulitis or frozen
shoulder by a physician or orthopedic surgeon. Early stage adhesive capsulitis included
stage I and stage II by Nevaiser, lasted 3 to 9 months and is characterized as most painful
phase of AC.3 Participants must have reported pain at-least for 3 months but less than 9
months to be classified as an early stage AC. Restriction of both active and passive ER
ROM is also the classical hallmark sign of early stage AC.3,31 Moreover, the studies
needed to compare glenohumeral joint mobilization and intra-articular corticosteroid
injections on external rotation range of motion, pain or both outcome measures.
Studies were excluded if patients had (1) adhesive capsulitis in the late stages III
or IV as defined by pain after 9 months due to AC, (2) prior history of shoulder surgery-
capsulorrhaphy, capsular distension, or manipulation under anesthesia, (3) shoulder pain
and stiffness from dislocation, fracture, or tendon tears, or (4) history of stroke with
hemiparesis or hemiplegia affecting the upper extremity with pain and loss of ROM.
Participants were also excluded if they had a condition in which either one of the
interventions is a contraindication, such as history of severe osteoporosis, joint laxity, and
osteomalacia for joint mobilization, and patients on immunosuppression drugs for cancer,
AIDS, and organ transplant for corticosteroid injections.
Definitions
Data were analyzed for the effect of glenohumeral joint mobilization (grade II to
IV) and single dose of intraarticular corticosteroid injection on external rotation range of
motion and pain over the period of 6 to 8 weeks. Timeline for the interventions was
defined based on the most similar timelines yielded by studies in the literature. The
intraarticular glucocorticoid steroid injections include 40 mg of triamcinolone and 4 ml of
9
9
1% lidocaine administered by the physician during the early stage AC. Similarly,
glenohumeral joint mobilizations (grade II to IV) were rendered by the physical therapist
during the stage I or II AC. The dosage and frequency of joint mobilization were 2 to 3
times per week for 6 to 8 weeks as defined in most of the studies in the available
literature.
Quality Appraisal
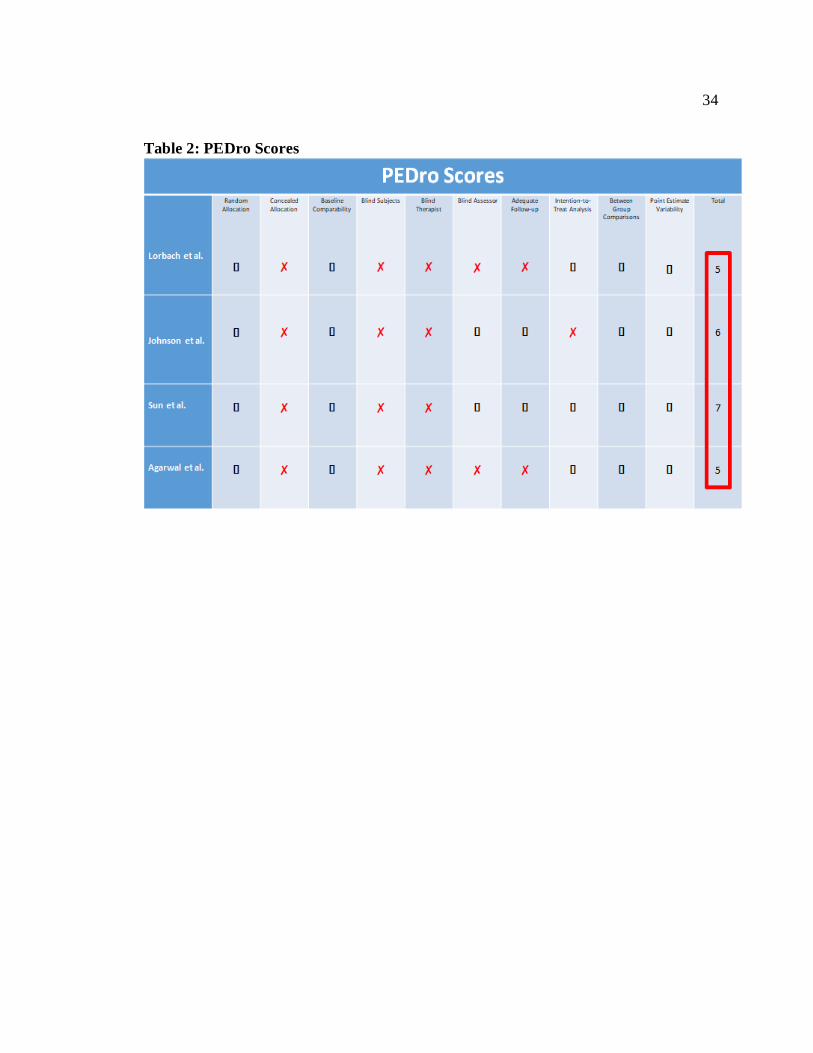
To determine the quality of studies used in this meta-analysis, the PEDro scale
was utilized. The PEDro scale is an 11-point score that assists the user to identify the
potential risks of bias within the studies and also identify flaws that can affect internal
validity.32 The first criterion is used to determine the applicability (inclusion and source)
of the study. As the inclusion and exclusion criteria were listed above, the first criterion
was not used to evaluate the studies. Therefore, the total score for the PEDro is based on
a 10-point scale. A PEDro score of 6-10 is considered high quality; score of 4-5 is
considered fair quality, while a score ≤ 3 is considered poor quality.31 This ensures high
internal validity to be applied in all reviewed studies and PEDro scale has been found to
demonstrate moderate to high reliability thus controlling potential threats to validity.32
Data Collection Process
All data, including the mean, standard deviation, and sample sizes were collected
from tables, figures, and text within the results sections of each study. Statistical analyses
of the studies were conducted to determine the pooled effect sizes of the interventions as
well as heterogeneity and homogeneity between studies. Effect sizes for each intervention
comparison and outcome measure were calculated using the mean differences and
standard deviations.
10
10
Outcome Measures
The Visual Analog Scale (VAS) is a commonly used outcome measure used to
assess patient’s subjective pain.26, 32–34 The VAS is a subjective assessment tool for pain
measurement consisting of a 10 cm line with 0 representing no pain and 10 representing
the worst pain experienced by patients. The patient typically marks on the line indicating
their pain severity based on a cm or mm increment.32-34 In the absence of gold standard
for pain measurement, studies have demonstrated moderate to good reliability for pain on
VAS however, validity can-not be determined.33–35
External rotation range of motion is measured by a qualified physical therapist by
using goniometry and recorded in degrees with the patient in supine and arm abducted to
the side in an available range. The goniometer is one of the most commonly used and
valid tools for measuring active and passive range of motion of major joints in the human
body.36 Studies have established good intra-rater reliability and concurrent validity for
measuring shoulder range of motion by using a standard goniometer.36–38 Standard
protocols for goniometric assessment of shoulder ROM are consistent with regard to
alignment and placement of the goniometer.36 The measurements were taken with the
patients in supine position and with arm abducted to the side, and with the goniometer
moving and stationary arm aligned appropriately to measure both active and passive
ROM. However, for this current review active ER ROM was considered for statistical
analysis. Active ER ROM was reported at baseline and then again at 4, 6, and 8 weeks
following the interventions.26,31,39,40 However, for the current meta-analysis active ER
ROM at 8 weeks will be considered for statistical analysis. Additionally, the patients
were blinded to the reading.
Statistical Analysis
Subjective measures of pain and external rotation ROM for subjects with early
stage adhesive capsulitis at 6 to 8 weeks were extracted from the included studies. Effect
11
11
sizes were calculated to assess the effect of treatment for each intervention and for each
outcome measure. Effect sizes and confidence intervals were calculated for each study
individually as well as combined to yield the grand combined effect size. Effect sizes
were classified as large, moderate, and small based on the correlating values being >0.80
as large, 0.30 to 0.8 moderate, and <0.30 as small respectively based on Cohen’s
conventional values.21 Positive effect sizes on the forest plots indicated beneficial effect
in favor of corticosteroid injections and negative effect sizes indicated benefits towards
glenohumeral joint mobilization. Moreover, to determine the possible homogeneity or
heterogeneity between studies, Cohen Q value was calculated for each study and
combined as well.
In order to determine whether or not to implement the random effects model in
the statistical analysis, a p value was used in the analysis. A random effects model was
used to calculate standardized mean differences and 95% confidence intervals. A random
effect model was utilized in this meta-analysis based on the statistical significance of the
p value. Additionally, forest plots were generated for each outcome measure to present a
visual representation of the results and grand effect size. The results were accepted as
significant if the confidence intervals did not cross zero.
RESULTS
Study Selection
An initial search was conducted by using databases including PubMed, Cochrane
Library, and SportDiscus by using the key terms listed in Table 1. A review of titles and
abstracts yielded a total of 318 studies that were appropriate for an in-depth review to
determine eligibility for inclusion in the meta-analysis. The articles were screened to
match current meta-analysis’s PICO population and non-English language. Articles were
further excluded (N=298) based upon duplicates, animal subjects, and non-peer-reviewed
articles. Of the remaining 20 articles, 16 were further excluded due to not matching the
exclusion/inclusion criteria of the PICO and were not conducted full clinical trials. The 4
remaining studies were reviewed for data comparison for this meta-analysis. These 4
articles were analyzed further by using the PEDro 10-point scale to yield the overall
potential strengths and weaknesses.
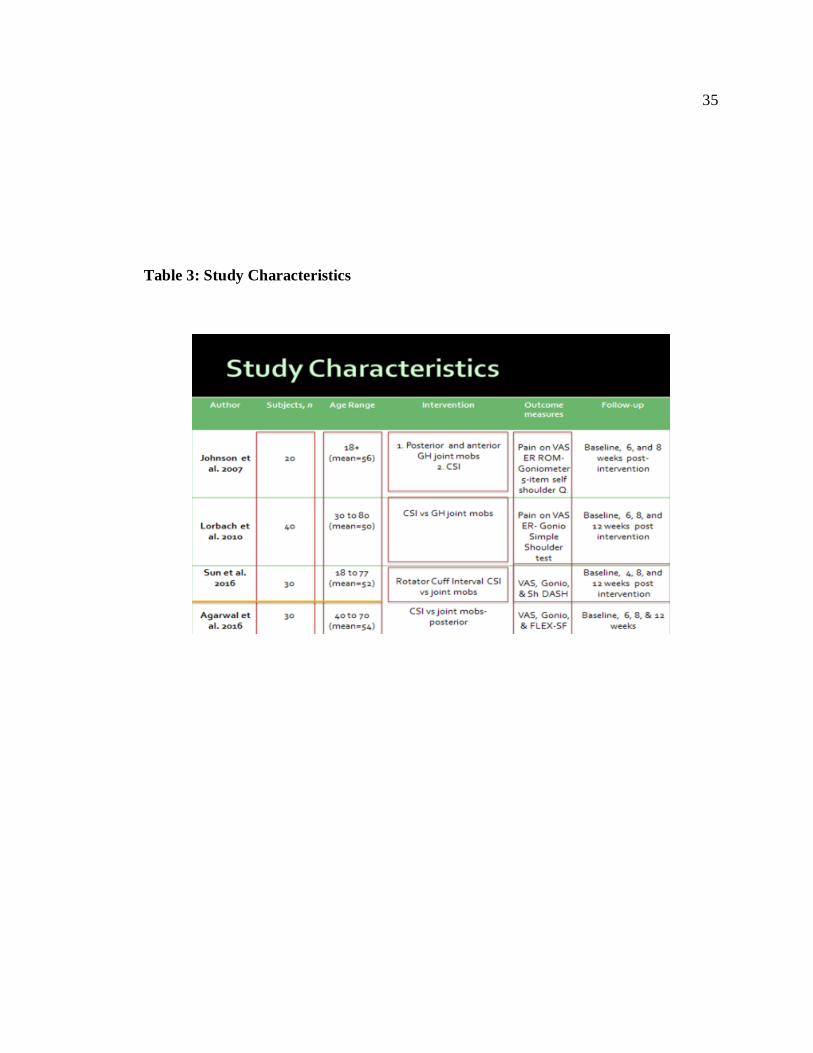
Study Characteristics
Articles included in this meta-analysis are from the following authors, Sun et al.39,
Lorbach et al.31, Agarwal et al.40, and Johnson et al.26 All the studies included in the
meta-analysis meet the requirements of the presented PICO criteria. The PEDro scores of
the 4 studies examined for this meta-analysis were in the ranges from 5-7/10. The study
characteristics are listed in Table 3. All 4 studies measured pain and external rotation
range of motion using the standard VAS and goniometry measurement. All participants
met the early stage adhesive capsulitis criteria as outlined by Neviaser.3 The mean
duration of symptoms was 11 months from the initial onset. Three studies listed an age
range in the inclusion criteria; the mean ages and standard deviations within those means
were above 45.26,39,40 Though the age SD differed across studies, the average age of all
subjects in the studies was 50 years with a range between 40-60 years. The main

13
13
differences identified across all studies included duration of each treatment, frequency of
treatment, amount of total sessions, specific dosage of corticosteroid injection, sample
size, participant mean age, and other associated mobility exercises. There were also
variations in the passive mobilization grades (II to IV), directions (anterior and posterior
directed) and frequencies of joint mobilizations across each of the studies, but they
characteristically included passive joint mobilization with some active therapeutic
exercises. Agarwal et al (2016) and Johnson et al (2007) rendered passive anterior and
posterior directed joint mobilizations to the glenohumeral joint in the mobilization group.
All studies demonstrated a decrease in pain and increase in active or passive ROM with
an intervention, either intra-articular corticosteroid injection or glenohumeral joint
mobilization. All the studies recorded baseline outcomes as well as changes in pain as
well as mobility levels at 6, 8, and 12 weeks following the proposed interventions. Three
of the articles recorded data on pain 8 and 12-weeks post intervention, while 1 article
recorded data 8 and 12 weeks and 6 and 12 months.
Outcome Assessment
A number of outcome measures were utilized across the included studies
including VAS for pain, goniometry for ROM assessment, Shoulder DASH for combined
pain and functional mobility, and shoulder disability index. All 4 studies measured pain
and range of movement at baseline and at 6, 8, and 12 weeks follow-up. All 4 studies
measured pain by a visual analogue scale, although different diurnal and activity pattern
measurements were taken across each of the studies. Alternatively, ROM was measured
in degrees with the exception of 1 study that measured ER ROM in both degrees and by
placing hand behind back, which was calculated by measuring, in inches, the distance
from the tip of the index finger to C7. Both pains on VAS and goniometry assessments
were deemed to be of sufficient comparability to calculate standardized mean differences
14
14
and effect estimates. The outcome measures were recorded at 6, 8, and 12 weeks post
intervention, however, for this meta-analysis, active ER ROM and pain on VAS at 8
weeks will be considered for statistical analysis.
Synthesis of Results
The purpose of this meta-analysis is to measure the effectiveness of glenohumeral
joint mobilization interventions compared with intra-articular corticosteroid injections in
adult patients with early stage adhesive capsulitis. The VAS and ER ROM score changes
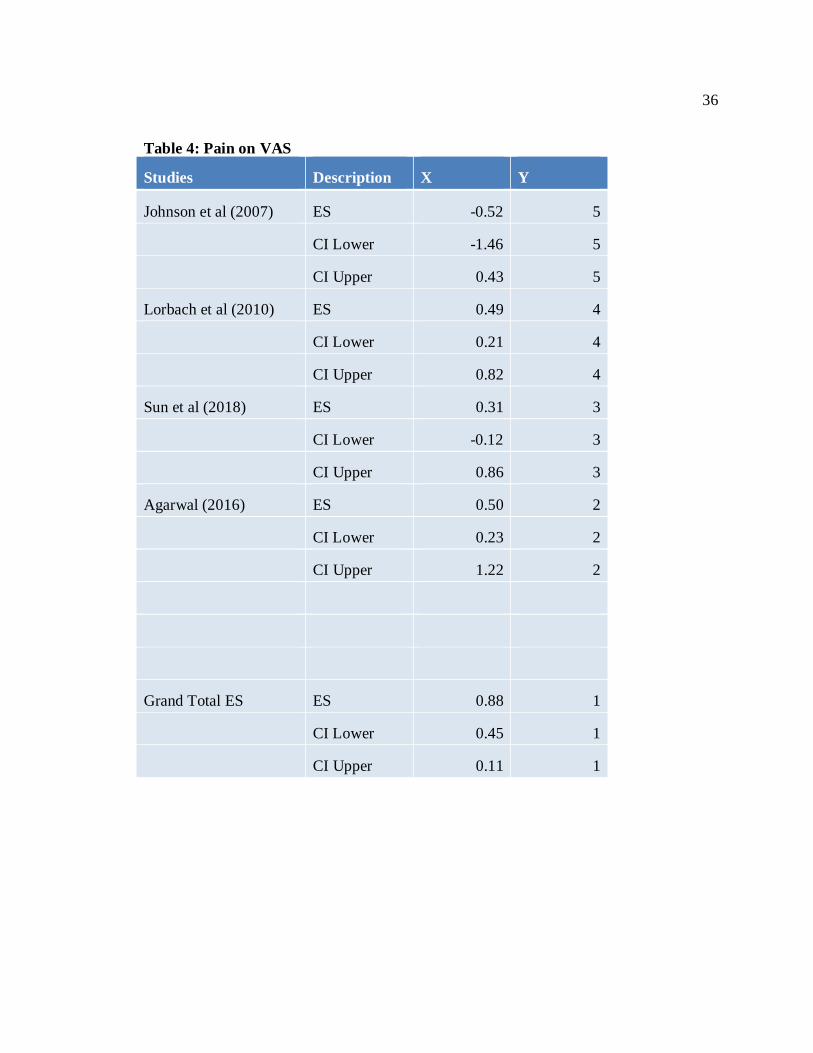
from baseline to 8 weeks are depicted in 2 forest plots (Figure 1 & 2). The effect sizes
and the upper and lower confidence intervals (based on a 95% confidence interval) are
displayed in Table 4 and Table 5. A random effects model was used for all data. The data
were pooled from different studies by pairing comparable means and standard deviations
from all studies. Results of the random effect models statistical analysis demonstrated
heterogeneity for change in VAS (Q= 5.89, p=0.03) and heterogeneity for change in ER
ROM (Q= 6.65, p= 0.08) with 3 degrees of freedom. This indicated that the grouping of
studies measuring pain and ER ROM are heterogenous. The combined effect size for pain
on VAS resulted in a moderate effect size of 0.88 largely favoring corticosteroids
injection over joint mobilization for pain relief. Johnson et al (2007) still favored joint
mobilization over CSI with the ES of -0.52. On the other hand, the combined effect size
for ER ROM was 0.29 indicating low treatment effect of joint mobilization on the ER
ROM.
DISCUSSION
The purpose of this meta-analysis was to determine the effectiveness of
glenohumeral joint mobilization interventions compared with intra-articular
corticosteroid injections in adult patients with early stage adhesive capsulitis. This review
aims to measure the efficacy of long- term benefits of joint mobilization interventions to
improve the shoulder functional mobility, specifically external rotation during the early
stage AC. The intention was to compare intra-articular CSI with the glenohumeral joint
mobilization, a relatively non-invasive safe and efficacious intervention, for the treatment
of early stage adhesive capsulitis. It was hypothesized that joint mobilization would have
superior long-term effect on pain reduction or functional mobility improvement when
compared to CSI, as measured by VAS and goniometric measurements, respectively.
Based on the results of this meta-analysis, the alternative hypothesis is accepted.
Individuals who received CS injections demonstrated improved pain and function when
compared to those who received joint mobilization over the period of 8 weeks. However,
due to heterogeneity of methods between the individual studies and specific study
characteristics, this discussion will include a review of the results, limitations of the
meta-analysis, and current literature support with respect to these outcomes.
Review of Results
The results from this meta-analysis confirmed the alternative hypothesis that CS
injections have superior efficacy in reducing pain and improving functional mobility
when compared to joint mobilization in individuals with adhesive capsulitis. Subjects
receiving CS injection demonstrated reduced pain on the VAS at the 8-week follow up
with a combined effect size of 0.88, indicating a large effect size. The statistical analysis
of this group indicates heterogeneity as measured by the p-value of 0.03 and Q value of
5.89.
16
16
The Q-value of 5.89 from pain on VAS group is greater than the generally
accepted value, Q < degrees of freedom, when determining homogeneity. In this case,
Q=5.89 is greater than the degrees of freedom which equal 3. This is most likely
secondary to the small number of groups (4) included in this meta-analysis.
Nevertheless, heterogeneity was accepted for this group based on the appropriate
significant p-value (P<0.005) and based on observed mean differences between groups.
Despite confidence intervals for CS injections crossing zero (indicating no clear
superiority of CSI), the effect size favors CSI over joint mobilizations for pain on VAS.
Similar to the results of CS injection effects on pain, subjects who received joint
mobilization demonstrated improved functional ER however, not statistically significant
(P>0.005). This was measured with a goniometer at 8-week follow up and resulted in a
combined, small effect size of 0.29. This grouping was also homogenous, supported by p-
value >0.005 (P=0.08), however, heterogeneous based on the greater Q-value of 6.65.
Joint mobilization shows a small effect size in favor as treatment of early stage adhesive
capsulitis for ER ROM. However, these results need to be interpreted with caution due to
the large amount of variation in homogeneity and heterogeneity between the studies.
Limitations of Meta-Analysis
This meta-analysis had several limitations. Study selection was limited to those
published in English. Additionally, there were many search terms used in attempt to
encompass all studies. However, there is a possibility that all the literature was not
reviewed because there was only 1 reviewer.
Studies were excluded if they did not fulfill the PICO comparing CSI to a gleno-
humeral joint mobilization. The literature search yielded 8 studies that examined the
effects of CSI compared to a physical therapeutic intervention-joint mobilization. Of
those 8 studies, 2 studies were excluded due to the inclusion of a therapeutic exercise
17
17
program and 2 were excluded due to the lack of accessibility to the data values. This
meta-analysis only included 4 studies and 2 interventional groups for statistical analysis.
The sample size of the interventional groups was relatively small in each study. This
causes a threat to the external validity and limits the conclusions that can be drawn from
this meta-analysis. Also, a small sample size can result in an underpowered study which
can potentially lead to type II error.41 A larger, multicenter, randomized clinical trial
would be recommended to improve external validity of the results.
Threats to Internal Validity
Lack of Blinding
Blinding allows the researcher to minimize threats to internal validity and
construct validity, thereby strengthening external validity and improving the
generalizability of results.41 Concerns to the internal validity were noted across several
areas, including absence of concealment and blinding of the practitioners providing
treatment. The therapist providing joint mobilization treatments were not blinded and
they may influence the results in favor or against based on their expectations. An
additional internal validity threat is the lack of blinding with patients regarding which
treatment they received. Blinding of patients can be difficult to control with an
experiment comparing 2 different interventions, but future studies can attempt to solve
this problem by providing a sham dosage of treatment.
Sun et al (2018) was the only study to blind their assessors during the
interventions data collection. However, the physician who performed the injections were
not blinded to the injection protocol.39 With all assessors knowing about subject
groupings, this could contain experimenter expectancies via differences in instructing the
subjects while administering the VAS or gathering ER ROM data that introduced biases
in the collection outcomes. The lack of subject, assessor, and therapist blinding, along
18
18
with the concealment of treatment, demonstrate these threats were not addressed. Thus,
future studies must control for the threats in internal validity by blinding all necessary
participants in the process.
Threats to Data Collection
The Visual Analog Scale (VAS) is one of the most commonly chosen outcome
scale across studies used to measure pain. Unfortunately, the VAS has 2 scales for
measurement of pain, measured in mm and cm.33 Agarwal et al.40 used a 100cm scale,
while Sun et al.39, Johnson et al.26 and Lorbach et al.31 all used a 10 cm scale. This can
cause slight variation in data collection as well as cause minor changes in results.
Similarly, another factor that could have resulted in deviated data is the position
in how the experimenter collects data on ER ROM testing. Agarwal et al.40 tested ER
with having subject’s reach their hand behind back and with the posterior inferior iliac
spine considered the starting position.
Threats to External Validity
Small sample sizes are threat to external validity relative to each of the studies.
The studies included in this meta-analysis had small sample sizes ranging from n=10 to
n=30 participants in each experimental group. An appropriate sample renders the research
more efficient as the use of sample size calculation directly influences research
findings.43 Very small samples undermine the internal and external validity of a study.43
Additionally, gender bias samples can be an external validity concern. Adhesive
capsulitis primarily reported a larger prevalence in females,1 and therefore this study is
not generalizable to the entire population of people with early adhesive capsulitis.
19
19
Literature Support
Pain and CSI
This meta-analysis showed a decrease in pain levels as reported by large
combined effect size (0.88) favoring CSI for pain reduction. Literature supports this
finding. Several studies receiving CSI treatments report a significant reduction of pain for
patients with early adhesive capsulitis.21,39,44,45 The findings of this review indicate that
the treatment of early stage adhesive capsulitis with corticosteroid injections is more
effective than joint mobilization in the pain reduction and to a lesser extent for regaining
ER ROM.
A research study by Bal et al. (2008) on a cohort of 80 early stage adhesive
capsulitis patients compared the efficacy of CSI with home exercise program for 12
weeks follow-up. The study demonstrated that intra-articular corticosteroid injections
when administered during the early stages provide an additive effect of rapid pain relief,
and thereby increase patient’s home exercise tolerance.46 The primary limitation
identified in this study was concerns to validity regarding patient’s variability to do home
exercises at their own pace without any supervision thus posing a threat to internal
validity. Another trial by Ranalleta et al (2016) compared CSI with oral analgesics on an
early stage adhesive capsulitis demonstrated that CSI provides faster pain relief (p=
0.001) and improvements in shoulder functional mobility (p=0.002) at 8 weeks follow-
up.29 A review by Blanchard et al (2010) reported that corticosteroid injections were
found to be more effective at improving both range of movement and function at around
6 to 8 weeks only.21 This strengthens the evidence that supports their short-term benefit.
Despite the evidence supporting early benefits of corticosteroid injections for pain relief,
most of the trials and reviews appeared to show minimal differences between
interventions in the long term beyond 8 weeks. This corresponds with the findings of the
20
20
current review wherein early stage adhesive capsulitis favored CSI over joint
mobilization for pain relief during the 8-week follow-up period.
It can be inferred from the studies that in patients with adhesive capsulitis who
have pain symptom predominantly, intraarticular corticosteroid therapy could be advised
concomitantly with exercise. Steroid injection therapy has been advised in adhesive
capsulitis based on the belief that capsular and synovial inflammation plays an important
role in the pathogenesis of this condition.3,9,10 Cytokines are involved in the initiation and
termination of repair processes in multiple musculoskeletal tissues, and their sustained
production has been shown to result in tissue fibrosis.47 Early stage adhesive capsulitis
treatment with intra-articular corticosteroid injections may provide a chemical ablation of
synovial inflammation process, thus limiting the subsequent development of fibrosis and
shortening the natural history of the disease.48
Pain and Joint Mobilization
Several studies have examined the effect of joint mobilization on pain reduction
in patients with early stage adhesive capsulitis, and although there is evidence that it may
be beneficial, there is a weak statistically significant (P<0.005) evidence to support
superior efficacy over other interventions like CSI.5,25,26,40 Bulgen et al compared 4
intervention groups: paired intra-articular and subacromial injections, joint mobilization,
ice/proprioceptive neuromuscular facilitation, and no treatment (pendulum exercises) in a
prospective randomized study of 41 patients with adhesive capsulitis. Patients treated
with joint mobilization and a HEP significantly improved in the first 4 weeks (P<0.005),
but less than patients receiving intra-articular and subacromial injections (P<0.002).
A decrease in pain after joint mobilization has been attributed to various patho-
physiological mechanisms, such as neuro-physiological effects achieved by the
stimulation of type II mechanoreceptors and by inhibition of type IV nociceptors,
21
21
stimulation of Golgi tendon organ activity, and reflex inhibition of the muscle at the end
of the passive joint mobilization.49,50 Joint mobilization also decreases muscle activity,
reducing muscle concentric activation, pain, and muscle tension in periarticular tissue.51
This implies that clinicians may utilize gleno-humeral joint mobilization procedures with
caution in the essence of weak evidence as an adjunct to reduce pain and increase motion
and function in patients with adhesive capsulitis.
External Rotation ROM
Early loss of ER range of motion with an intact rotator cuff muscles is a hallmark
sign of early stage adhesive capsulitis. The current meta-analysis has shown relatively
small effect size for joint mobilization.
Johnson et al (2017) investigated the effectiveness of 2 different joint
mobilization techniques-anterior versus posterior glide mobilization on external rotation
ROM in 20 patients with early stage adhesive capsulitis. Patients treated with posterior
glide mobilization demonstrated significantly greater improvement in ER ROM
compared to those treated with anterior glide mobilization. One of the main limitations
identified in this study is that it compared the effect of 2 directions of mobilization on
external rotation motion but failed to compare mobilization with other forms of treatment
thus creating a bias in the study.
Carette et al performed a randomized controlled prospective study of 93 patients
with early stage adhesive capsulitis and compared 4 different interventions-low grade
joint mobilization, corticosteroid injection, saline injection, and physical therapy home
exercise program (HEP). Patients were assessed at 6 and 8 weeks, 3 months, and 6
months post interventions. This study has shown that at 6 and 8 weeks, a single dose of
intra-articular injection alone or with joint mobilization is more effective in pain
reduction (P=0.0002) and regaining ER ROM (P=0.0003) when compared to 12 sessions
22
22
of joint mobilization or a HEP alone.24 This study had validity threats because of a
significant drop out, 6 in the corticosteroid group (n=23) and 4 in the joint mobilization
(n=21), and 2 in the saline injection group (n=21).
A systematic literature review by Blanchard et al (2010) assessed the
effectiveness of corticosteroid injections compared to physiotherapeutic interventions
including joint mobilization for early stage adhesive capsulitis. This study reported that at
6 to 8 weeks post interventions, there was a medium effect in favor of corticosteroid
injections when compared to physiotherapeutic interventions. Small effects were noted
for the long-term follow up from 12 to 52 weeks post interventions. The study concluded
that corticosteroid injections offer beneficial effects over physiotherapeutic interventions
in the treatment of adhesive capsulitis at short term and to a lesser extent at long term.
Clinical Implications
Current literature states that intraarticular corticosteroids have the additive effect
of providing rapid pain relief and improving mobility in patients with an early stage
adhesive capsulitis. In patients with adhesive capsulitis who have pain symptom
predominantly, intraarticular corticosteroid therapy could be advised concomitantly with
exercises and joint mobilization to improve ROM. Loss of active and passive ER with an
intact rotator cuff is one of the classical hallmark signs of early stage adhesive capsulitis
as the disease progresses. It has been inferred from the review that this short-term
improvement is clinically relevant because pain reduction not only alleviates symptoms
but allows patients to move faster in the stages of rehabilitation and thus return to their
daily life activities more rapidly.
The results of this meta-analysis have shown a decrease in pain levels and
increase in ER ROM primarily with corticosteroid injections over the first 8 weeks,
however, long-term benefits are still questionable. This has been well supported by
23
23
various trials and review studies mentioned throughout this review. Although, the
evidence for joint mobilization is weak for pain relief and gaining ER ROM, there is still
an indication for this treatment specifically for improvements in the ER ROM. According
to Blancahrd et al, Carette et al, and Ryans et al corticosteroid injections are effective
providing an immediate pain relief by easing off an inflammatory response, however, the
effect is short lasting, and physiotherapeutic interventions such as low grade joint
mobilization is effective in improving the range of movement in external rotation. This
indicates that physical therapists should implement non-invasive joint mobilization
techniques as an adjunct to CSI for early stage adhesive capsulitis to achieve pain relief
and ROM. Therefore, if the patient requires short-term relief to continue their daily
functional activities; current evidence supports the use for CSI. However, this should be
taken with caution. If the patient’s occupation or lifestyle requires continued repetition,
stress, optimum shoulder complex’s mobility and strength, it is recommended that one
should find an alternative treatment options, such as physical therapy.
Future Research
Further research is warranted to establish the most effective intervention strategies
with focus on the signs and symptoms associated with each stage for those suffering with
adhesive capsulitis (AC). More high-quality trials and reviews similar to the ones used in
this review could help to substantiate the findings, and thereby provide more definitive
conclusions to be drawn about long-term outcomes beyond 12 weeks. In order to get the
more effective comparisons between different interventions available for AC, a gold
standard diagnostic test as well as standard outcome measure specifically targeting the
signs and symptoms of AC is required.5 The current diagnostic criteria are determined
from history and physical examination of the affected shoulder complex, but imaging
studies can be used to rule out the underlying pathology. The primary purpose for
24
24
diagnosis and classification of shoulder pain is to direct evidence-based intervention and
inform prognosis for AC.5
It is also very important to analyze patients grouped together according to the
stage of their disease, in order to determine whether certain treatments are more effective
at specific times in the disease process. Literature review demonstrated that early stage
AC from onset up-to 12 months is one of the most painful stages with significant loss of
active and passive ROM specifically in the capsular pattern.21,24 Generally, loss of greater
than 25% ROM in at least 2 planes and passive external rotation loss that is greater than
50% of the uninvolved shoulder have been used to define adhesive capsulitis.5,18,24,25,28
Rundquist et al found varying patterns of restriction in adhesive capsulitis patients, but
the most common pattern was a loss of external rotation with the arm at the side followed
by a loss of abduction and internal rotation.55 Impairment-based classification is critical
for matching the intervention strategy that is most likely to provide the optimal outcome
for a patient’s clinical findings.5 However, it is important for clinicians to understand that
patients with shoulder pain often fit more than 1 impairment pattern and that the most
relevant impairments of body function and the associated intervention strategies often
change during the patient’s episode of care.
Multiple interventions have been described for the treatment of adhesive
capsulitis, and there is emerging evidence from high-quality randomized clinical trials
regarding both short and long-term efficacy of these interventions. By far, corticosteroid
injections are administered to suppress the inflammatory response and reduce pain in
patients with adhesive capsulitis. Research into the long term benefits of injection therapy
should be carried out to determine whether or not injections provide a long-benefits
across all stages of AC, and also into the effectiveness of guided vs non-guided
techniques.5 A cost consequence analysis may also be of benefit in order to determine

25
25
whether any additional improvements achieved by combining the 2 interventions would
be large enough to warrant the extra resources required.21
Conclusion
In conclusion, a single intraarticular injection of corticosteroid administered
during the early stage adhesive capsulitis, combined with a joint mobilization program, is
effective in improving shoulder pain and disability in patients with adhesive capsulitis.
Supervised physiotherapy in conjunction with the corticosteroid treatment provides faster
improvement in shoulder ROM. Joint mobilization when used alone offer limited efficacy
in the management of adhesive capsulitis due to the weak clinical evidence. Based on the
evidence provided through this meta-analysis, a large effect size (0.88) for pain reduction
in support of CIS and a small effect size (0.29) for joint mobilization to improve ER
ROM at 8-weeks for the treatment of early stage adhesive capsulitis is indicated.
Therefore, the intra-articular corticosteroid injections combined with joint mobilization
are more effective in providing short-term (8 weeks) pain relief and improved function
compared to shoulder joint mobilization alone. While the results are promising, future
research is needed to develop optimal treatment parameters to further support this
conclusion.

REFERENCES
REFERENCES
1. Zuckerman JD, Rokito A. Frozen shoulder: a consensus definition. J Shoulder Elbow
Surg. 2011;20(2):322-325. doi:10.1016/j.jse.2010.07.008
2. Page P, Labbe A. Adhesive capsulitis: Use the evidence to integrate your
interventions. North Am J Sports Phys Ther NAJSPT. 2010;5:266-273.
3. Neviaser JS. Adhesive Capsulitis of the Shoulder: A Study of the Pathological
Findings in Periarthritis of the Shoulder. JBJS. 1945;27(2):211.
4. Hsu JE, Anakwenze OA, Warrender WJ, Abboud JA. Current review of adhesive
capsulitis. J Shoulder Elbow Surg. 2011;20(3):502-514.
doi:10.1016/j.jse.2010.08.023
5. Kelley MJ, Shaffer MA, Kuhn JE, et al. Shoulder Pain and Mobility Deficits:
Adhesive Capsulitis: Clinical Practice Guidelines Linked to the International
Classification of Functioning, Disability, and Health From the Orthopaedic Section
of the American Physical Therapy Association. J Orthop Sports Phys Ther.
2013;43(5):A1-A31. doi:10.2519/jospt.2013.0302
6. Le HV, Lee SJ, Nazarian A, Rodriguez EK. Adhesive capsulitis of the shoulder:
review of pathophysiology and current clinical treatments. Shoulder Elb.
2017;9(2):75-84. doi:10.1177/1758573216676786
7. Kuye IO, Jain NB, Warner L, Herndon JH, Warner JJP. Economic Evaluations in
Shoulder Pathologies: a systematic review of the literature. J Shoulder Elb Surg Am
Shoulder Elb Surg Al. 2012;21(3):367-375. doi:10.1016/j.jse.2011.05.019
8. Cho C-H, Song K-S, Kim B-S, Kim DH, Lho Y-M. Biological Aspect of
Pathophysiology for Frozen Shoulder. BioMed Research International.
doi:10.1155/2018/7274517
9. Ryan V, Brown H, Minns Lowe CJ, Lewis JS. The pathophysiology associated with
primary (idiopathic) frozen shoulder: A systematic review. BMC Musculoskelet
Disord. 2016;17(1):340. doi:10.1186/s12891-016-1190-9
10. Hand GCR, Athanasou NA, Matthews T, Carr AJ. The pathology of frozen shoulder.
J Bone Joint Surg Br. 2007;89(7):928-932. doi:10.1302/0301-620X.89B7.19097
11. Tamai K, Akutsu M, Yano Y. Primary frozen shoulder: brief review of pathology
and imaging abnormalities. J Orthop Sci Off J Jpn Orthop Assoc. 2014;19(1):1-5.
doi:10.1007/s00776-013-0495-x
12. Zhao W, Zheng X, Liu Y, et al. An MRI Study of Symptomatic Adhesive Capsulitis.
PLOS ONE. 2012;7(10):e47277. doi:10.1371/journal.pone.0047277
28
28
13. Koh KH. Corticosteroid injection for adhesive capsulitis in primary care: a
systematic review of randomised clinical trials. Singapore Med J. 2016;57(12):646-
657. doi:10.11622/smedj.2016146
14. Hand C, Clipsham K, Rees JL, Carr AJ. Long-term outcome of frozen shoulder. J
Shoulder Elbow Surg. 2008;17(2):231-236. doi:10.1016/j.jse.2007.05.009
15. Song A, Higgins LD, Newman J, Jain NB. Glenohumeral corticosteroid injections in
adhesive capsulitis: a systematic search and review. PM R. 2014;6(12):1143-1156.
doi:10.1016/j.pmrj.2014.06.015
16. D’Orsi GM, Via AG, Frizziero A, Oliva F. Treatment of adhesive capsulitis: a
review. Muscles Ligaments Tendons J. 2012;2(2):70-78.
17. Sun Y, Lu S, Zhang P, Wang Z, Chen J. Steroid Injection Versus Physiotherapy for
Patients With Adhesive Capsulitis of the Shoulder. Medicine (Baltimore).
2016;95(20). doi:10.1097/MD.0000000000002469
18. Buchbinder R, Green S, Youd JM. Corticosteroid injections for shoulder pain.
Cochrane Database Syst Rev. 2003;(1):CD004016.
doi:10.1002/14651858.CD004016
19. Baums MH, Spahn G, Nozaki M, Steckel H, Schultz W, Klinger H-M. Functional
outcome and general health status in patients after arthroscopic release in adhesive
capsulitis. Knee Surg Sports Traumatol Arthrosc Off J ESSKA. 2007;15(5):638-644.
doi:10.1007/s00167-006-0203-x
20. Jain TK, Sharma NK. The effectiveness of physiotherapeutic interventions in
treatment of frozen shoulder/adhesive capsulitis: A systematic review. J Back
Musculoskelet Rehabil. 2014;27(3):247-273.
21. Blanchard V, Barr S, Cerisola FL. The effectiveness of corticosteroid injections
compared with physiotherapeutic interventions for adhesive capsulitis: a systematic
review. Physiotherapy. 2010;96(2):95-107. doi:10.1016/j.physio.2009.09.003
22. Maund E, Craig D, Suekarran S, et al. Management of frozen shoulder: a systematic
review and cost-effectiveness analysis. Health Technol Assess Winch Engl.
2012;16(11):1-264. doi:10.3310/hta16110
23. Widiastuti-Samekto M, Sianturi GP. Frozen shoulder syndrome: comparison of oral
route corticosteroid and intra-articular corticosteroid injection. Med J Malaysia.
2004;59(3):312-316.
24. Carette S, Moffet H, Tardif J, et al. Intraarticular corticosteroids, supervised
physiotherapy, or a combination of the two in the treatment of adhesive capsulitis of
the shoulder: A placebo-controlled trial. Arthritis Rheum. 2003;48(3):829-838.
doi:10.1002/art.10954
29
29
25. Vermeulen HM, Rozing PM, Obermann WR, le Cessie S, Vliet Vlieland TPM.
Comparison of high-grade and low-grade mobilization techniques in the
management of adhesive capsulitis of the shoulder: randomized controlled trial. Phys
Ther. 2006;86(3):355-368.
26. Johnson AJ, Godges JJ, Zimmerman GJ, Ounanian LL. The effect of anterior versus
posterior glide joint mobilization on external rotation range of motion in patients
with shoulder adhesive capsulitis. J Orthop Sports Phys Ther. 2007;37(3):88-99.
doi:10.2418/jospt.2007.2307
27. Jewell DV, Riddle DL, Thacker LR. Interventions associated with an increased or
decreased likelihood of pain reduction and improved function in patients with
adhesive capsulitis: a retrospective cohort study. Phys Ther. 2009;89(5):419-429.
doi:10.2522/ptj.20080250
28. Bulgen DY, Binder AI, Hazleman BL, Dutton J, Roberts S. Frozen shoulder:
prospective clinical study with an evaluation of three treatment regimens. Ann
Rheum Dis. 1984;43(3):353-360. doi:10.1136/ard.43.3.353
29. Ranalletta M, Rossi LA, Bongiovanni SL, Tanoira I, Elizondo CM, Maignon GD.
Corticosteroid Injections Accelerate Pain Relief and Recovery of Function
Compared With Oral NSAIDs in Patients With Adhesive Capsulitis: A Randomized
Controlled Trial. Am J Sports Med. 2016;44(2):474-481.
doi:10.1177/0363546515616238
30. OCEBM Levels of Evidence. CEBM. https://www.cebm.net/2016/05/ocebm-levels-
of-evidence/. Published May 1, 2016. Accessed December 7, 2019.
31. Lorbach O, Anagnostakos K, Scherf C, Seil R, Kohn D, Pape D. Nonoperative
management of adhesive capsulitis of the shoulder: oral cortisone application versus
intra-articular cortisone injections. J Shoulder Elbow Surg. 2010;19(2):172-179.
doi:10.1116/j.jse.2009.06.013
32. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the
PEDro scale for rating quality of randomized controlled trials. Phys Ther.
2003;83(8):713-721.
33. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual
Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain),
McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-
MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36
BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP).
Arthritis Care Res. 2011;63(S11):S240-S252. doi:10.1002/acr.20543
34. Carlsson AM. Assessment of chronic pain. I. Aspects of the reliability and validity
of the visual analogue scale. Pain. 1983;16(1):87-101. doi:10.1016/0304-
3959(83)90088-x
30
30
35. Boonstra AM, Schiphorst Preuper HR, Reneman MF, Posthumus JB, Stewart RE.
Reliability and validity of the visual analogue scale for disability in patients with
chronic musculoskeletal pain. Int J Rehabil Res Int Z Rehabil Rev Int Rech
Readaptation. 2008;31(2):165-169. doi:10.1097/MRR.0b013e3282fc0f93
36. Sabari JS, Maltzev I, Lubarsky D, Liszkay E, Homel P. Goniometric assessment of
shoulder range of motion: comparison of testing in supine and sitting positions. Arch
Phys Med Rehabil. 1998;79(6):647-651. doi:10.1016/s0003-9993(98)90038-7
37. Kolber MJ, Hanney WJ. The Reliability and Concurrent Validity of Shoulder
Mobility Measurements Using a Digital Inclinometer and goniometer a technical
report Int J Sports Phys Ther. 2012;7(3):306-313.
38. Mullaney MJ, McHugh MP, Johnson CP, Tyler TF. Reliability of shoulder range of
motion comparing a goniometer to a digital level. Physiother Theory Pract.
2010;26(5):327-333. doi:10.3109/09593980903094230
39. Sun Y, Liu S, Chen S, Chen J. The Effect of Corticosteroid Injection Into Rotator
Interval for Early Frozen Shoulder: A Randomized Controlled Trial. Am J Sports
Med. 2018;46(3):664-670. doi:10.1177/0363546517744171
40. Agarwal S, Raza S, Moiz JA, Anwer S, Alghadir AH. Effects of two different
mobilization techniques on pain, range of motion and functional disability in patients
with adhesive capsulitis: a comparative study. J Phys Ther Sci. 2016;28(12):3342-
3349. doi:10.1689/jpts.28.3342
41. Page SJ, Persch AC. Recruitment, Retention, and Blinding in Clinical Trials. Am J
Occup Ther. 2013;67(2):154-161. doi:10.5014/ajot.2013.006197
42. Clinical Trials: A Practical Approach | Wiley. Wiley.com.
https://www.wiley.com/en-us/Clinical+Trials%3A+A+Practical+Approach-p-
9780471901556. Accessed February 1, 2020.
43. Faber J, Fonseca LM. How sample size influences research outcomes. Dent Press J
Orthod. 2014;19(4):27-29. doi:10.1590/2176-9451.19.4.027-029.ebo
44. Khan AA, Akhtar N, Ayyub A, Aziz T, Iqbal S, Shafaat HK. Intra-Articular
Corticosteroids Versus Physiotherapy in the Management of Adhesive Capsulitis.
Pak Armed Forces Med J. 2018;68(3):565-569.
45. Tariq Aziz, Khan AA, Akhtar N, Ayyub A, Iqbal S, Shafaat HK. Intra-Articular
Corticosteroids Versus Physiotherapy in the Management of Adhesive Capsulitis.
Pak Armed Forces Med J. 2018;68(3):565-569.
46. Bal A, Eksioglu E, Gulec B, Aydog E, Gurcay E, Cakci A. Effectiveness of
corticosteroid injection in adhesive capsulitis. Clin Rehabil. 2008;22(6):503-512.
doi:10.1177/0269215508086179
31
31
47. Border WA, Noble NA. Transforming growth factor beta in tissue fibrosis. N Engl J
Med. 1994;331(19):1286-1292. doi:10.1056/NEJM199411103311907
48. Hannafin JA, Chiaia TA. Adhesive Capsulitis: A Treatment Approach. Clin Orthop
Relat Res. 2000;372:95–109.
49. Lundberg A, Malmgren K, Schomburg ED. Role of joint afferents in motor control
exemplified by effects on reflex pathways from Ib afferents. J Physiol.
1978;284:327-343.
50. Mangus B, Hoffman L, Hoffman M, Altenburger P. Basic Principles of Extremity
Joint Mobilization Using a Kaltenborn Approach. J Sport Rehabil. 2002;11:235-250.
doi:10.1123/jsr.11.4.235
51. Frank C, Akeson WH, Woo SL, Amiel D, Coutts RD. Physiology and therapeutic
value of passive joint motion. Clin Orthop. 1984;(185):113-125.
52. Kivimäki J, Pohjolainen T, Malmivaara A, et al. Manipulation under anesthesia with
home exercises versus home exercises alone in the treatment of frozen shoulder: a
randomized, controlled trial with 125 patients. J Shoulder Elbow Surg.
2007;16(6):722-726. doi:10.1016/j.jse.2007.02.125
53. Ryans I, Montgomery A, Galway R, Kernohan WG, McKane R. A randomized
controlled trial of intra-articular triamcinolone and/or physiotherapy in shoulder
capsulitis. Rheumatol Oxf Engl. 2005;44(4):529-535.
doi:10.1093/rheumatology/keh535
54. Hay EM, Thomas E, Paterson SM, Dziedzic K, Croft PR. A pragmatic randomised
controlled trial of local corticosteroid injection and physiotherapy for the treatment
of new episodes of unilateral shoulder pain in primary care. Ann Rheum Dis.
2003;62(5):394-399. doi:10.1136/ard.62.5.394
55. Rundquist PJ, Anderson DD, Guanche CA, Ludewig PM. Shoulder kinematics in
subjects with frozen shoulder. Arch Phys Med Rehabil. 2003;84(10):1473-1479.
doi:10.1016/s0003-9993(03)00359-9

TABLES
33
33
Table 1: Study Selection
Studies from initial
search of
databases
Articles excluded based upon duplicates, animal
subjects, English language, and non-peer-
reviewed articles
Studies from 3
databases
Articles excluded if they did not match PICO
components
Number of RCT studies used in
this Meta-
Analysis
Search Terms
(N=318) (N= 298) (N=20) (N= 16) (N=4)
adhesive capsulitis,
frozen shoulder,
adhesive capsulitis
interventions, corticosteroid
injection, injection and
joint mobilization,
and frozen shoulder and
manual therapy
34
34
Table 2: PEDro Scores
35
35
Table 3: Study Characteristics
36
36
Table 4: Pain on VAS
Studies Description X Y
Johnson et al (2007) ES -0.52 5
CI Lower -1.46 5
CI Upper 0.43 5
Lorbach et al (2010) ES 0.49 4
CI Lower 0.21 4
CI Upper 0.82 4
Sun et al (2018) ES 0.31 3
CI Lower -0.12 3
CI Upper 0.86 3
Agarwal (2016) ES 0.50 2
CI Lower 0.23 2
CI Upper 1.22 2
Grand Total ES ES 0.88 1
CI Lower 0.45 1
CI Upper 0.11 1

37
37
Table 5: ER ROM
Studies Description X Y
Johnson et al (2007) ES -0.20 5
CI Lower -1.13 5
CI Upper -0.73 5
Lorbach et al (2010) ES -0.24 4
CI Lower -0.52 4
CI Upper 0.21 4
Sun et al (2018) ES 0.06 3
CI Lower -0.51 3
CI Upper 0.24 3
Agarwal (2016) ES -0.21 2
CI Lower -0.93 2
CI Upper -0.51 2
Grand Total ES ES -0.34 1
CI Lower -0.67 1
CI Upper 0.17 1
38
38
Figure 1. Outcome variable-Pain on VAS Scale
Figure 2. Outcome variable-ER ROM with goniometer
APPENDICES

APPENDIX A: FROZEN SHOULDER GUIDELINE
41 41
APPENDIX B: FROZEN SHOULDER STAGES
43 43
Fresno State Non-exclusive Distribution License (Keep for your records) (to archive your thesis/dissertation electronically via the Fresno State Digital Repository)
By submitting this license, you (the author or copyright holder) grant to the Fresno State Digital Repository
the non-exclusive right to reproduce, translate (as defined in the next paragraph), and/or distribute your
submission (including the abstract) worldwide in print and electronic format and in any medium, including
but not limited to audio or video.
You agree that Fresno State may, without changing the content, translate the submission to any medium or
format for the purpose of preservation.
You also agree that the submission is your original work, and that you have the right to grant the rights
contained in this license. You also represent that your submission does not, to the best of your knowledge,
infringe upon anyone’s copyright.
If the submission reproduces material for which you do not hold copyright and that would not be
considered fair use outside the copyright law, you represent that you have obtained the unrestricted
permission of the copyright owner to grant Fresno State the rights required by this license, and that such
third-party material is clearly identified and acknowledged within the text or content of the submission.
If the submission is based upon work that has been sponsored or supported by an agency or organization
other than Fresno State, you represent that you have fulfilled any right of review or other obligations
required by such contract or agreement.
Fresno State will clearly identify your name as the author or owner of the submission and will not make
any alteration, other than as allowed by this license, to your submission. By typing your name and date
in the fields below, you indicate your agreement to the terms of this use. Publish/embargo options
(type X in one of the boxes).
Make my thesis or dissertation available to the Fresno State Digital Repository
immediately upon submission.
Embargo my thesis or dissertation for a period of 2 years from date of graduation. After 2
years, I understand that my work will automatically become part of the university’s public
institutional repository unless I choose to renew this embargo here:
Embargo my thesis or dissertation for a period of 5 years from date of graduation. After 5
years, I understand that my work will automatically become part of the university’s public
institutional repository unless I choose to renew this embargo here:
Type full name as it appears on submission
Date