the editors' perspectives
TRANSCRIPT

THE JOURNAL OF PEDIATRICS DECEMBER 2002 1A
THE JOURNAL OFPEDIATRICSCopyright 2002 by Mosby, Inc.
THIS MONTH IN
THE EDITORS’ PERSPECTIVES
MATERNAL ALCOHOL METABOLISM AND THE
FETAL ALCOHOL SYNDROME
Although the fetal alcohol syndrome (FAS) is the most com-mon cause of brain injury, many fetuses exposed to alcoholdo not have the FAS. Alcohol is metabolized in the liver toacetaldehyde by alcohol dehydrogenase, and the toxicacetaldehyde is metabolized to acetate by aldehyde dehydro-genase. The different alleles for alcohol dehydrogenase yieldenzymes with different activities, and the distribution of alle-les also differs by race. In this issue of The Journal, Stoler etal asked, in a high-risk population, if there was an associationbetween maternal genotype for alcohol dehydrogenase,maternal history of alcohol use during pregnancy, and theclinical diagnosis of FAS in the newborn. One genotype pre-dicted both increased alcohol consumption and a greater riskof having an infant with FAS. The suggestion is that the genet-ic potential of a person to metabolize alcohol may promoteexcessive alcohol use and thus increase the risk for FAS.
—Alan H. Jobe, MD, PhDPage 780
The Journal of Pediatrics (ISSN 0022-3476) is published monthly by Mosby. Corporate and editorial offices: 11830 Westline Industrial Dr, StLouis, MO 63146-3318. Accounting and circulation offices: Mosby, 6277 Sea Harbor Dr, Orlando, FL 32887-4800. Periodicals postage paid atOrlando, FL 32862, and at additional mailing offices. 2002 subscription rates: domestic, $152.00 for individuals and $386.00 for institutions.Printed in USA. POSTMASTER: Send address changes to The Journal of Pediatrics, Mosby, Periodicals Department, 6277 Sea Harbor Dr,Orlando, FL 32887-4800.
HOW DO WE FEEL ABOUT ENROLLING OUR
PATIENTS IN CLINICAL TRIALS?
The randomized controlled clinical trial has become the goldstandard for developing evidence to advance clinical practice.At the start of a clinical trial there should be equipoiseregarding the risks and benefits of the interventions beingused. At the end of a trial, and particularly if more than onetrial produce consistent significant results, the interventionthat is better should be implemented in clinical practice. Thisis simple in theory but sometimes complicated in practice.For a successful trial, patients must be enrolled as subjectsand complete the study. This is different from standard clini-cal practice where the clinician provides the patient with thebest clinical therapy. Clearly we want the results from clinicaltrials, but how do we feel about enrolling patients in trials?
In this issue of The Journal, Caldwell et al examine the issueof pediatricians’ attitudes about clinical trials. They found thatpediatricians perceive both benefits and risks from havingpatients participate in clinical trials. The benefits include sci-entific advancement and improved patient care. The risksinclude potential risk to the patient and harm to the doctor-patient relationship. They also found that there may be a lackof equipoise or an inability to admit equipoise as pediatri-cians’ personal treatment preferences hindered support fortrials.
These results suggest that there is work to be done as westrive for increasingly evidence-based clinical practice.Education is needed for investigators to better understandthe barriers to completion of a trial; primary care physiciansto better accept the concept of equipoise and the role of clin-ical trials in answering important clinical questions; andpatients and their families to accept clinical trial participationas leading to the best clinical practice for themselves and oth-ers.
—Stephen R. Daniels, MD, PhDPage 798

2A DECEMBER 2002 THE JOURNAL OF PEDIATRICS
INDUCED SPUTUM AS A NEW OUTCOME MEASURE
IN CYSTIC FIBROSIS
Measuring the degree of airway inflammation in cystic fibro-sis (CF) is a useful outcome measure for clinical trials ofantibiotic and anti-inflammatory agents. Earlier approacheshave usually involved bronchoscopy to obtain bronchoalveo-lar lavage fluid for analysis, and this approach has been usefulbut is limited in the pediatric age group by clinical and ethicalconsiderations. A relatively new approach in CF is to analyzesputum that has been induced by inhaling hypertonic saline.This technique has been validated in clinically stable childrenwith CF and the results are published in an article by Sagel etal. Several markers of airway inflammation, such as inter-leukin-8, neutrophil elastase activity, total cell count, andneutrophil count, were negatively correlated with the pul-monary function measurement forced expiratory volume inone second (FEV1). By contrast, the density of bacteria insputum did not correlate significantly with either FEV1 ormarkers of inflammation in induced sputum, possibly reflect-ing a relatively small sample size. The induced sputum tech-nique offers a noninvasive way to obtain repeated samplesfrom the lower respiratory tract and assess airway infectionand inflammation in relation to a clinical trial.
—Robert W.Wilmott, MDPage 811
THERAPEUTIC MAGIC BULLETS
New therapies for difficult-to-treat diseases continue to bedeveloped. When new therapies are first available, enthusi-asm for them often tends to overlook treatment failures. Inperinatal medicine, the most effective therapies—antenatalsteroids and postnatal surfactant—do not uniformly preventor effectively treat respiratory distress syndrome. The newmagic bullet is nitric oxide (NO) for the treatment of pul-monary hypertension of the newborn. Although NO is oftenvery effective, almost half of the infants treated with it do notrespond adequately. Kelly et al report in this issue of TheJournal that infants who do not respond to NO, whichincreases intracellular cyclic GMP, may respond toaerosolized prostacyclin (PGI2), which increases intracellularcyclic AMP. Although intravascular PGI2 is approved for thetreatment of pulmonary hypertension, its use in infants hasbeen limited by systemic hypotension. Aerosolized PGI2effectively targets the lungs and may be a new therapeutic bul-let for infants with pulmonary hypertension who do notrespond to NO.
—Alan H. Jobe, MD, PhDPage 830
THE JOURNAL OF PEDIATRICS DECEMBER 2002 3A
WHAT DOSE OF L-THYROXINE TO USE FOR
CONGENITAL HYPOTHYROIDISM?
The use of L-thyroxine to treat congenital hypothyroidism isone of the great advances in pediatrics. It is well known thatearly detection and prompt treatment preserves optimumneurodevelopmental outcome. However, the optimum doseof L-thyroxine has been controversial. In this issue of TheJournal, Selva et al report on a randomized controlled clinicaltrial of 3 dosing schedules. They found that initial dosing of 50µg/day (12-17 µg/kg/day) raised serum thyroxine (T4) and freeT4 levels to the target range in 3 days, and normalized thy-roid-stimulating hormone by 2 weeks, of therapy. They alsorecommend a higher target range for T4 and free T4 duringthe first 2 weeks of treatment. However, careful follow-up ofgrowth and neurodevelopment will be necessary to confirmthe relative risks and benefits of this strategy.
—Stephen R. Daniels, MD, PhDPage 786
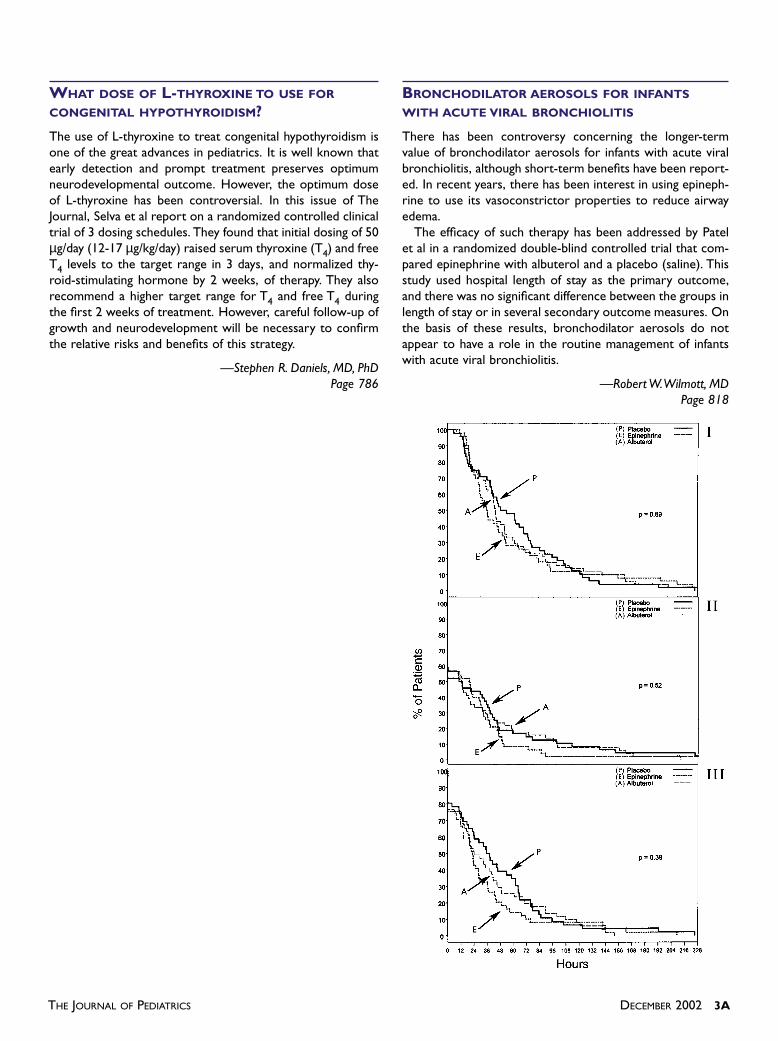
BRONCHODILATOR AEROSOLS FOR INFANTS
WITH ACUTE VIRAL BRONCHIOLITIS
There has been controversy concerning the longer-termvalue of bronchodilator aerosols for infants with acute viralbronchiolitis, although short-term benefits have been report-ed. In recent years, there has been interest in using epineph-rine to use its vasoconstrictor properties to reduce airwayedema.
The efficacy of such therapy has been addressed by Patelet al in a randomized double-blind controlled trial that com-pared epinephrine with albuterol and a placebo (saline). Thisstudy used hospital length of stay as the primary outcome,and there was no significant difference between the groups inlength of stay or in several secondary outcome measures. Onthe basis of these results, bronchodilator aerosols do notappear to have a role in the routine management of infantswith acute viral bronchiolitis.
—Robert W.Wilmott, MDPage 818