the doctor of nursing practice visionary leadership for the practice of nursing evolution and...
Post on 19-Dec-2015
215 views
TRANSCRIPT
The Doctor of Nursing The Doctor of Nursing PracticePractice
Visionary Leadership for the Visionary Leadership for the Practice of NursingPractice of Nursing
Evolution and Current Status of the Evolution and Current Status of the National MovementNational Movement
Overview of PresentationOverview of Presentation
• Introductory Comments on the Present Context and the Development of the DNP
• Discussion Related to the Work of the Road Map Task Force
• Description of the Work of the Essentials Task Force
Focus of Comments Related to the Focus of Comments Related to the Road Map Task ForceRoad Map Task Force
• Comment on the Paradigm Shift Occurring in Graduate Education in Nursing
• Describe the Task Force’s Charge• Comment on Diffusion of Innovations as a
Framework for Looking at what is happening and a Framework for Guiding the Work
• Discuss Frequently Asked Questions and Fears• Comment on Feedback from Regional
Conferences
It is About the FUTURE !!!It is About the FUTURE !!!
Creating the FutureCreating the Future
We have a responsibility to create We have a responsibility to create the future for our patients, for our the future for our patients, for our profession, and for the health of the profession, and for the health of the public.public.
A Paradigm Shift is Underway in A Paradigm Shift is Underway in Graduate Education in NursingGraduate Education in Nursing
• A Number of Factors are Converging to Build Momentum for a Major set of Shifts
• These Include: Aging of the Population; Expansion of Knowledge Underlying Practice; Increased Complexity of Patient Care; Major Concerns about Quality of Care and Patient Safety; Shortages of Nursing Personnel Demanding a Higher Level of Preparation for Leaders Who Can Design and Assess Care and Lead; Shortages of Prepared Nursing Faculty, Leaders in Practice, and Nurse Researchers, and Increasing Educational Expectations for the Preparation of other Health Professionals
Position Statement on the Position Statement on the Practice Doctorate in NursingPractice Doctorate in Nursing
October 2004October 2004
National Academy of Sciences National Academy of Sciences 2005 Report on Nursing Research2005 Report on Nursing Research
• The Report Focuses on Increasing the Number of Nurse Scientists and Increasing the Number of Productive Research Years for Nurses Prepared in PhD Programs

National Academy of Sciences National Academy of Sciences 2005 Report2005 Report
• Calls for a distinction between • “the educational needs and goals of
nursing as a practice profession that require practitioners with clinical expertise from
• Nursing as an academic discipline and science that requires independent researchers and scientists to build the body of knowledge” (p.74)
National Academy of Sciences National Academy of Sciences 2005 Report2005 Report
• “The need for doctorally prepared practitioners and clinical faculty would be met if nursing could develop a new nonresearch clinical doctorate, similar to the M.D. and Pharm.D. in medicine and pharmacy, respectively.”
Development of the Clinical Development of the Clinical Nurse Leader at the Master’s Nurse Leader at the Master’s
LevelLevel
Graduate Education Graduate Education in Nursing in Nursing
20042004
Graduate Education Graduate Education in Nursing in Nursing 2004 - 20102004 - 2010
Members of the Roadmap Task Members of the Roadmap Task ForceForce
• Kathleen Andreoli – Rush University• Debra Davis – University of South Alabama• Carolina Huerta – Univ. of Texas-Pan American• Martha Hill – Johns Hopkins University• Nancy Mosser – Waynesburg College• Robyn Nelson, Cal. State Univ.-Sacramento• Marjorie Lawson – Univ. of Southern Maine• Anna Alt-White – Dept. Veterans Affairs, D.C• Carolyn Williams (Chair) Univ. of Kentucky
Charge of the Roadmap Task ForceCharge of the Roadmap Task Force
• Develop an Implementation Plan that provides a Roadmap for Achieving the Goals of the Position Statement by 2015
• Delineate Key Institutional and Academic Issues that Must be Addressed in Academic Institutions
Charge of the Roadmap Task ForceCharge of the Roadmap Task Force
• Assess Regulatory and/or Legislative Frameworks that Shape Practice Authority, Reimbursement, and/or Academic Authority, and Identify Implications of these Frameworks and
• Identify Actual and/or Potential Challenges and Opportunities Inherent in the Assessments and Make Recommendations
Charge of the RoadmapTask Charge of the RoadmapTask ForceForce
• Map Potential Interfaces and/or Partnerships that can be Created to Assist Undergraduate and Graduate Nursing Programs to Participate in Achieving the 2015 Goal
• Develop Recommendations that Detail Actions and Timelines for Accomplishment with Specific Focus on the Role of AACN in Facilitating the Implementation Process
Rogers ’Diffusion of Innovations as Rogers ’Diffusion of Innovations as a Conceptual Frameworka Conceptual Framework
• A Way of Looking at What is Happening
• A Framework for Guiding Our Work
Diffusion of InnovationsDiffusion of Innovations
• Provides a Conceptual Framework for Understanding the Process of the Adoption of New Technologies or Practices and Social Change
• An Innovation is an idea, practice, or object, that is perceived as new
• The diffusion component is the process by which an innovation is communicated

Diffusion of InnovationsDiffusion of Innovations
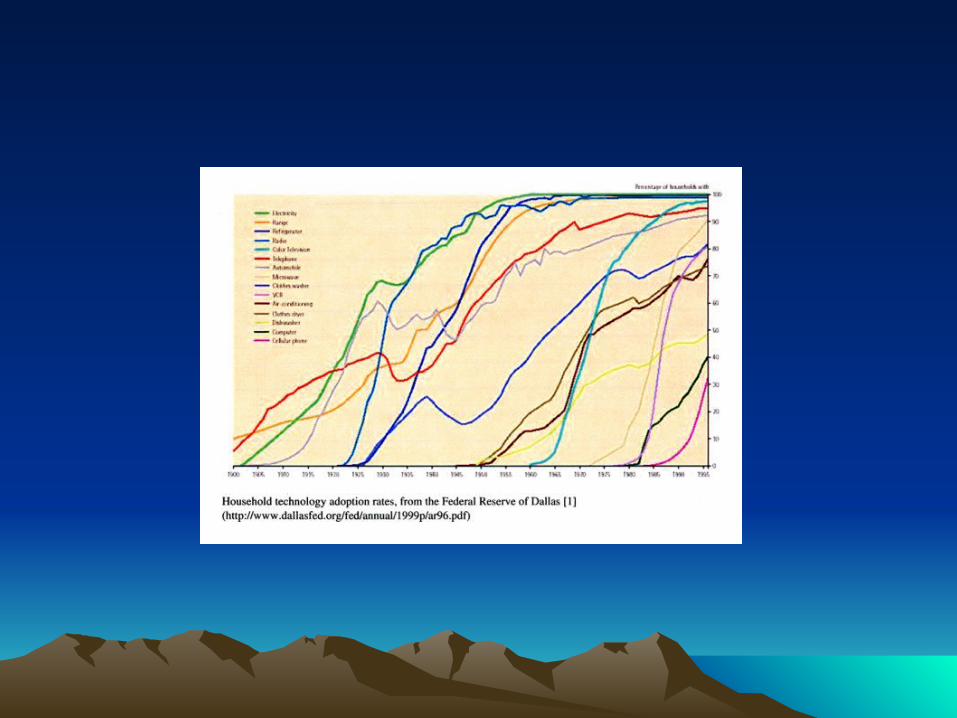
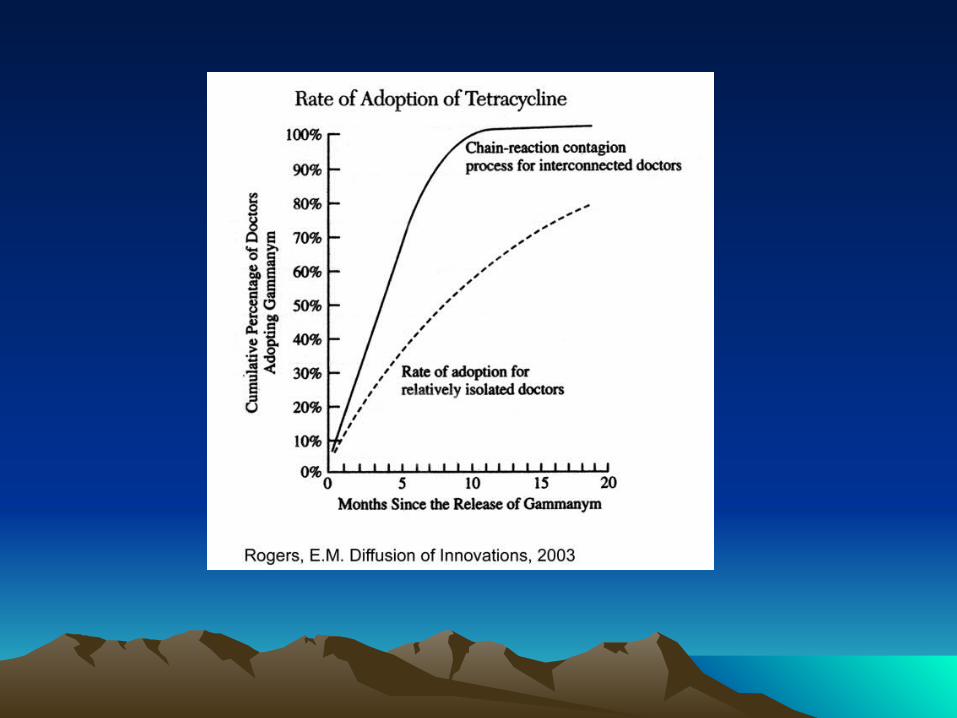
• Generally an innovation moves slowly through a group when it is first introduced. Many are skeptical and resist change, but as the number trying the innovation increases the idea moves at a faster rate especially if the early adopters are pacesetters
• The diffusion phenomenon initially follows an S-shaped curve
Variables Determining the Rate of Variables Determining the Rate of Adoption – Attributes of the Adoption – Attributes of the
InnovationInnovation
• Relative Advantage - Better than Previous Approaches
• Compatibility – Consistent with values/needs
• Complexity – Degree to which it is difficult to Understand or put into place
Varibles Determining Adoption –Varibles Determining Adoption –Attributes of the InnovationAttributes of the Innovation
• Triability – The degree to which an innovation can be experimented with
• Observability – The degree to which the results of an innovation are visible to others
Variables Influencing Rate of Variables Influencing Rate of AdoptionAdoption
• Communication Networks and Opinion Leaders• Extent of Change Agent Efforts/Effectiveness –
key elements include developing contact with “clients”, developing a felt need for change, providing information exchange – effectiveness is increased if there is similarity between the change agents and those they are seeking to influence
Reference on Roger’s Reference on Roger’s WorkWork
Rogers, E.M., (2003). Diffusion of Rogers, E.M., (2003). Diffusion of Innovations. New York, Free Innovations. New York, Free
Press.Press.

Work of the Task ForceWork of the Task Force
• We Understand that our Job is NOT limited to data gathering and getting out a Report - BUT A REPORT WE WILL DO!!!
• We need to Establish Mechanisms for Input from Various Stakeholders
• We need to serve as Change Agents and Encourage Others to Do So
Work of the Task ForceWork of the Task Force
• Development of Communication Opportunities in Various Media
• Regional Conferences in Partnership With Essentials Task Force
• National Nursing Stakeholders Meeting in Partnership With Essentials Task Force
• Participation in Conference Calls with Various Organizations
Work of the Task ForceWork of the Task Force
• As we Think Things Through we also Need to Provide Information About the Innovation and Opportunities to Help the Community of Potential Adopters and other Stakeholders Clarify Their Understanding of the Innovation and Reduce Uncertainty
• This Translates Into Developing Materials and Developing Communication Channels such as Conferences and The Internet
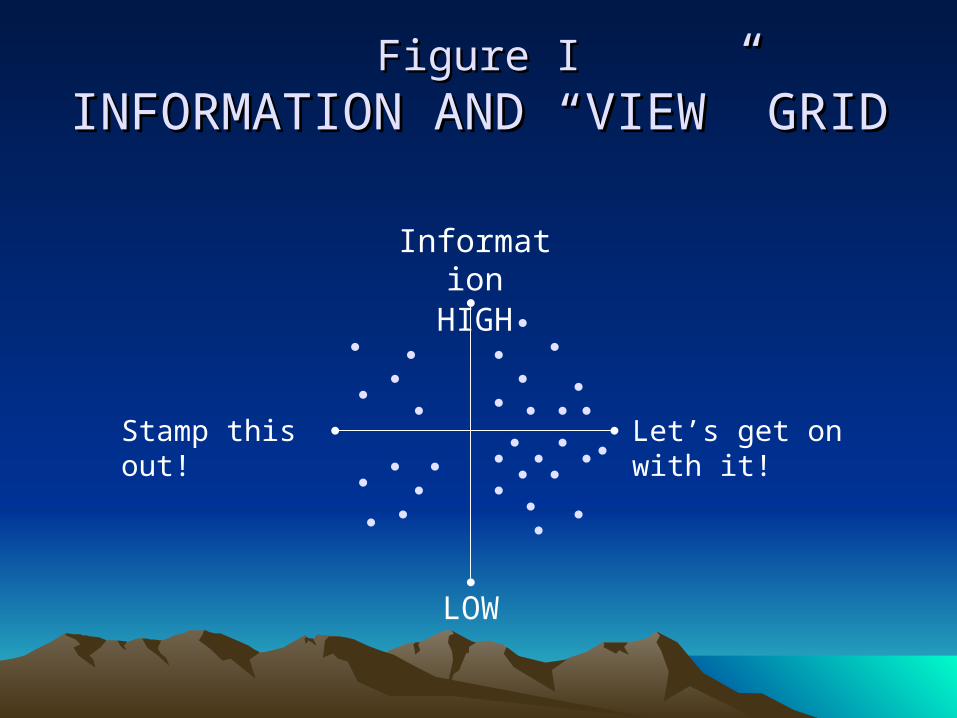
Figure IFigure I
INFORMATION AND “VIEW” GRIDINFORMATION AND “VIEW” GRID
InformationHIGH
LOW
Stamp this out! Let’s get on with it!
Products in ProcessProducts in Process
• Frequently Asked Questions – On Web• Bibliography on the DNP – On Web• Pathways Diagram – On Web• Comparison of DNP and PhD/DNSc/DNS
Programs – Done with Essentials T. Force• Strategy For Growing DNP Faculty• Description of An Institutional Partnering Effort• Possibility of a DNP “Tool Box”
ISSUES IDENTIFIED AT THE ISSUES IDENTIFIED AT THE FOUR REGIONAL FOUR REGIONAL
CONFERENCES, AT THE CONFERENCES, AT THE NATIONAL NATIONAL
STAKEHOLDER’S STAKEHOLDER’S CONFERENCE, AND AT CONFERENCE, AND AT AACN’S FALL MEETINGAACN’S FALL MEETING
FacultyFaculty
• Development of Faculty for DNP Programs
• Preparation of Preceptors
• Credentials Required to Teach in a DNP Program
• The Extent to which Engagement in an Active Practice is Needed
• Definitions of Scholarship
• Tenure Possibilities for DNP Faculty
Program QuestionsProgram Questions
• Could Students be Certified before completing the DNP so they could “Practice” at some level?
• Should Program Models provide for a Jump-out at some point (MSN ? ) to allow for Practice and then Continue to DNP?
• Need for Multiple Pathways• Strategies for Maintaining Quality and
Rigor
Institutional IssuesInstitutional Issues
• Possible Impact on Non-Doctoral Institutions• Possible Effect on an Institution’s Carnegie
Classification• Possibilities for Collaboration Among Various
Institutions • Strategies for Making the Case to the Institution• Distance Learning Partnerships for Rural Areas
Costs/FundingCosts/Funding
• Costs for Students and Return on Investment• Availability of Financial Aid for DNP Students,
including Assistantships• Possibility of National Funding for Paid
Residencies • Possibilities for HRSA Funding• Costs for Institutions• Reimbursement Issues
Market IssuesMarket Issues
• Strategies for Marketing to Students, including those in Rural Areas
• Strategies for Informing the Public, Physicians, and Other Professional Groups
• Nature and Extent of the Market for Graduates - In the Practice Arena and Marketability of DNP Grads to Universities
• Strategies for Countering Misinformation
Master’s ProgramsMaster’s Programs
• Impact on Current Master’s Programs
• What Type of Master’s Programs will Continue?
• Will CCNE Continue to Accredit Master’s Programs?

Licensure and CertificationLicensure and Certification
• Practice Acts May Vary and There May need to be some Changes in Some States
• Clarification of the Future Certification Status for Those Currently Certified who do not obtain a DNP
• Possible Usefulness of a National Definition of Advanced Practice
Political IssuesPolitical Issues
• Extent of Support for Transition from State Regulatory and Educational Bodies
• Impact on Rural Areas• Extent to Which the DNP will Change the
Expected Supply and Demand for Nurses Prepared at the Master’s and Doctoral Levels
• Impact of Retirements on Reaching 2015 Goal• Options for Programs Not Housed in a School of
Nursing• Use of Title “Doctor”
EvaluationEvaluation
• NEED DATA ON :
• Sustainability of Programs
• Graduates
• Value Added
• Career Mobility
• Practice Patterns
Is this program just for primary care providers?Is this program just for primary care providers?
No, the DNP degree prepares individuals for a No, the DNP degree prepares individuals for a variety of roles at the highest level of nursing variety of roles at the highest level of nursing practicepractice
Are there going to be standards for programs?Are there going to be standards for programs?
Yes, the DNP Essentials document will help guide Yes, the DNP Essentials document will help guide development of standards. CCNE has indicated the development of standards. CCNE has indicated the intent to establish accreditation standards.intent to establish accreditation standards.
Is there going to be credentialing for individuals?Is there going to be credentialing for individuals?
Yes, individuals will continue to be credentialed by Yes, individuals will continue to be credentialed by the various specialty organizations.the various specialty organizations.
Frequently Asked QuestionsFrequently Asked Questions
Does the DNP prepare for faculty positions?Does the DNP prepare for faculty positions?
As a professional doctorate, DNP curricula As a professional doctorate, DNP curricula focus on the core discipline of nursing, teaching focus on the core discipline of nursing, teaching content could be incorporated in addition to this content could be incorporated in addition to this core. core.
Will all APN’s have to get a DNP?Will all APN’s have to get a DNP?
Current APN’s will retain their privileges, after Current APN’s will retain their privileges, after 2015 all APN 2015 all APN programsprograms should be offered should be offered through DNP programs.through DNP programs.
Frequently Asked QuestionsFrequently Asked Questions
Will faculty with DNP be eligible for tenure?Will faculty with DNP be eligible for tenure?
Tenure is an institutional prerogative with twoTenure is an institutional prerogative with two
major considerations.major considerations.
1.1. Who is eligible for tenure?Who is eligible for tenure?
If the institution tenures holders of other professional If the institution tenures holders of other professional degrees degrees (EdD, MD, PsyD, PharmD, JD, PTD, AudD, etc.)(EdD, MD, PsyD, PharmD, JD, PTD, AudD, etc.) then DNP then DNP
graduates should also be tenurable.graduates should also be tenurable.
2.2. What are the criteria for tenure?What are the criteria for tenure?
If the institution defines scholarly productivity broadly If the institution defines scholarly productivity broadly to include external funding and publications other than to include external funding and publications other than that associated with only NIH R-Level grants, then the that associated with only NIH R-Level grants, then the DNP graduate should be tenurable.DNP graduate should be tenurable.
Frequently Asked QuestionsFrequently Asked Questions
As a Profession, should we As a Profession, should we let current tenure policies in let current tenure policies in some universities determine some universities determine what is needed in Nursing what is needed in Nursing
Practice, OR should we find Practice, OR should we find ways to help universities ways to help universities
develop policies that support develop policies that support the education of nurses for the education of nurses for
the FUTURE??? the FUTURE???
There are no data to support these programs.There are no data to support these programs.
The Aiken data suggest that health outcomes The Aiken data suggest that health outcomes improve as the educational level of nurses improve as the educational level of nurses increasesincreases
Surveys of graduates indicate they have Surveys of graduates indicate they have acquired new knowledge and skills that have acquired new knowledge and skills that have enhanced their practicesenhanced their practices
Reports from employers are indicating DNP Reports from employers are indicating DNP graduate are bringing added valued to their graduate are bringing added valued to their places places of employmentof employment
Frequently Expressed FearsFrequently Expressed Fears
PhD Program enrollments will decline.PhD Program enrollments will decline.
There is no evidence for this. Those who select the There is no evidence for this. Those who select the DNP appear to be from a population that is not DNP appear to be from a population that is not interested in a PhD and probably would not engage in interested in a PhD and probably would not engage in doctoral study without the emergence of the practice doctoral study without the emergence of the practice doctorate.doctorate.
Frequently Expressed FearsFrequently Expressed Fears
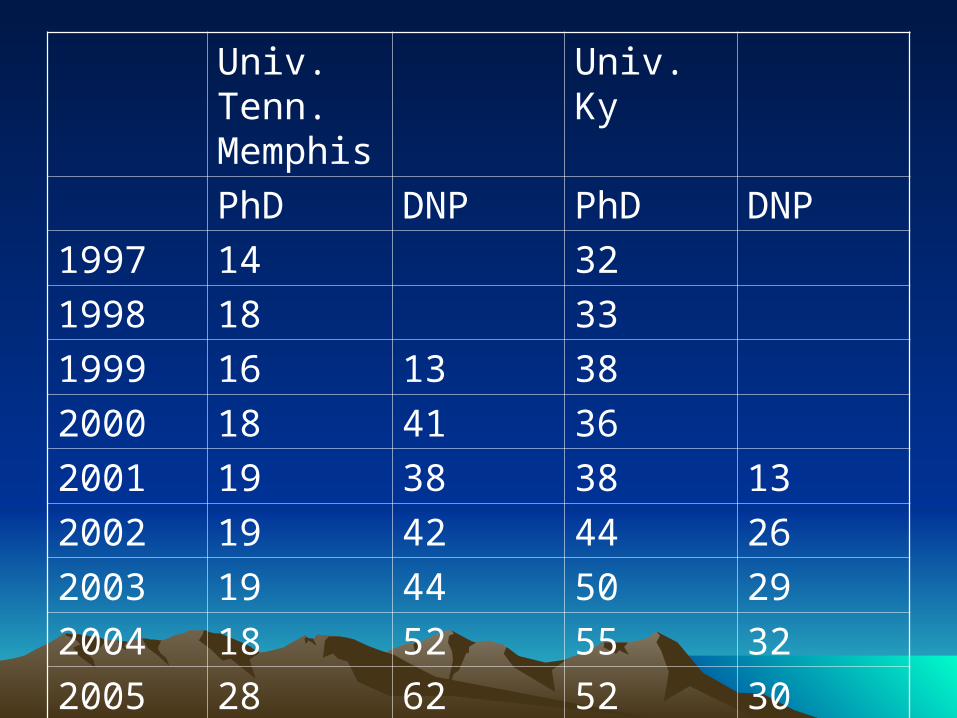
Univ. Tenn. Memphis
Univ. Ky
PhD DNP PhD DNP
1997 14 32
1998 18 33
1999 16 13 38
2000 18 41 36
2001 19 38 38 13
2002 19 42 44 26
2003 19 44 50 29
2004 18 52 55 32
2005 28 62 52 30

Doctoral Students at University of Doctoral Students at University of Tennessee - MemphisTennessee - Memphis
0
10
20
30
40
50
60
70
1997 1998 1999 2000 2001 2002 2003 2004 2005
PhD
DNP
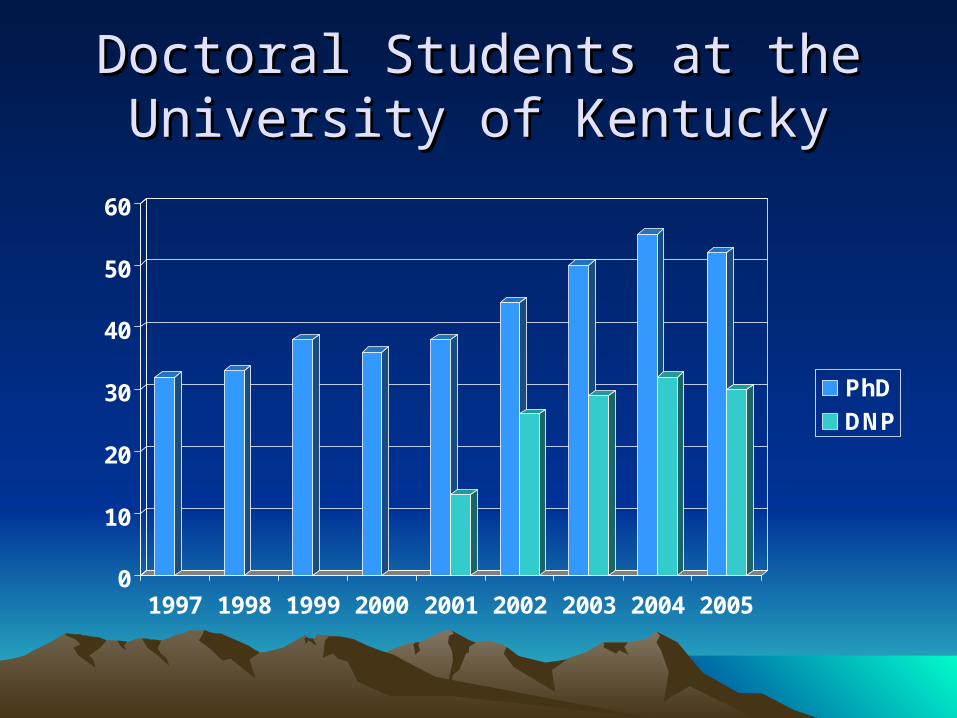
Doctoral Students at the University Doctoral Students at the University of Kentuckyof Kentucky
0
10
20
30
40
50
60
1997 1998 1999 2000 2001 2002 2003 2004 2005
PhD
DNP
FOR THE PROFESSION OF FOR THE PROFESSION OF NURSING IT IS NOT THE NURSING IT IS NOT THE
PhD OR DNP, IT IS BOTH !!!PhD OR DNP, IT IS BOTH !!!
For the Individual, it may be one For the Individual, it may be one or the other, or for a few, it could or the other, or for a few, it could
be both.be both.
What Kind of Individuals What Kind of Individuals are Attracted to the DNP?are Attracted to the DNP?
““I have been waiting for a program like this, I have been waiting for a program like this, I am not interested in a research career, I am not interested in a research career,
but there is more I need to learn but there is more I need to learn to make me a better practitioner.” to make me a better practitioner.”
1960—Boston University opens 11960—Boston University opens 1stst clinical doctorate clinical doctorate1979—Case Western Reserve opens 11979—Case Western Reserve opens 1stst ND program ND program
1999—UTHSC opens DNSc practice doctorate1999—UTHSC opens DNSc practice doctorate2001—University of Kentucky opens First DNP 2001—University of Kentucky opens First DNP
ProgramProgram2002—AACN forms practice doctorate Task Force 2002—AACN forms practice doctorate Task Force 2003—Columbia University admits students2003—Columbia University admits students2004—AACN members approve DNP Position Paper2004—AACN members approve DNP Position Paper2005—(Spring) 8 programs admitting students, 2005—(Spring) 8 programs admitting students,
60 schools considering programs60 schools considering programs2005—(Summer) 80 schools considering programs2005—(Summer) 80 schools considering programs2005—(Fall) 20 programs “approved” 2005—(Fall) 20 programs “approved”
140 schools considering programs 140 schools considering programs
Doctoral Education for Nursing PracticeDoctoral Education for Nursing Practice
An Important Driver is the An Important Driver is the Growing Desire Clinically Growing Desire Clinically Focused Nurses Have in Focused Nurses Have in Advanced Study that will Advanced Study that will
Enhance their Effectiveness Enhance their Effectiveness

Are we at a Tipping Point?Are we at a Tipping Point?
Factors Contributing to the Tipping PointFactors Contributing to the Tipping Point
IOM called attention to problems facing health careIOM called attention to problems facing health care
1999—1999—To Err is HumanTo Err is Human, focused on fragmented nature , focused on fragmented nature of health careof health care
2001—2001—Crossing the Quality ChasmCrossing the Quality Chasm, calls for a , calls for a restructuring of healthcarerestructuring of healthcare
20032003—Health Professions Education: A Bridge to Quality —Health Professions Education: A Bridge to Quality call for educators to prepare health care providers call for educators to prepare health care providers for a new type of practice as members of for a new type of practice as members of interdisciplinary teams that emphasize evidence-interdisciplinary teams that emphasize evidence-based practice, quality improvement, and based practice, quality improvement, and informaticsinformatics
Factors Contributing to the Tipping PointFactors Contributing to the Tipping Point
Expanding length of MSN programsExpanding length of MSN programs
• longer than most masters (many 60+ hrs and 3 yrs)longer than most masters (many 60+ hrs and 3 yrs)
• didactic and clinical increased by 72 and 36 hours didactic and clinical increased by 72 and 36 hours respectively for NP programs between 1995-2000 respectively for NP programs between 1995-2000
(AACN & NONPF 2002)(AACN & NONPF 2002)
• even more content is needed even more content is needed ((eg., information and eg., information and practice management, health policy, risk management, practice management, health policy, risk management, evaluation of evidence, and advanced diagnosis and evaluation of evidence, and advanced diagnosis and managementmanagement))
(Bellack, Graber, O’Neil, Musham, & Lancaster, (Bellack, Graber, O’Neil, Musham, & Lancaster,
1999;1999; Lenz, Mundinger, Hopkins, Clark, & Lin, Lenz, Mundinger, Hopkins, Clark, & Lin,
2002).2002).
Factors Contributing to the Tipping PointFactors Contributing to the Tipping Point
Movement of other disciplines to the doctorateMovement of other disciplines to the doctorate (MD, DDS, PsyD, DPT, PharmD, (MD, DDS, PsyD, DPT, PharmD,
AudD)AudD)
Emerging and active interdisciplinary teamsEmerging and active interdisciplinary teams ““The tipping point for me The tipping point for me
was when I was at a team meeting was when I was at a team meeting and everyone there had a doctorate and everyone there had a doctorate
in their respective fields in their respective fields except the nurse.”except the nurse.”
““Nurses prepared at the doctoral level with a Nurses prepared at the doctoral level with a blend of clinical, organizational, economic and blend of clinical, organizational, economic and leadership skills are most likely to be able to leadership skills are most likely to be able to critique nursing and other clinical scientific critique nursing and other clinical scientific findings and design programs of care delivery findings and design programs of care delivery that are locally acceptable, economically that are locally acceptable, economically feasible, and which significantly impact health feasible, and which significantly impact health care outcomes.”care outcomes.”
The Mission Becomes ApparentThe Mission Becomes Apparent
AACN Position Paper on the Practice DoctorateAACN Position Paper on the Practice Doctorate
““There exists a fleeting and deliriously exciting There exists a fleeting and deliriously exciting moment in the life of an ideamoment in the life of an idea
when it teeters between what one person suspects when it teeters between what one person suspects and what everyone accepts.and what everyone accepts.
In that moment, months or years In that moment, months or years before it exerts any practical influence,before it exerts any practical influence,
the idea holds the greatest potential to inspire and incite.the idea holds the greatest potential to inspire and incite.
Opportunities, implications, and related discoveriesOpportunities, implications, and related discoveriesopen up from it in all directions like a hall of mirrors.”open up from it in all directions like a hall of mirrors.”
(Harvard Business Review, February 2005. (Harvard Business Review, February 2005. Introduction to the years “Best Innovations”)Introduction to the years “Best Innovations”)
Where Does that Put Us Today?Where Does that Put Us Today?

Essentials Task Force MembersEssentials Task Force Members
Janet Allan – University of MarylandJulie Sebastian – University of KentuckyEdward Thompson – University of IowaMaureen Keefe – University of UtahAnn Hamric – University of VirginiaJudy Honig – Columbia UniversityCarol Howe - Oregon Health and Science UniversityElizabeth Lenz – The Ohio State UniversityHeidi Taylor - West Texas A & M UniversitySr. Mary Margaret Mooney – North Dakota State
University
The Essentials of the Doctorate of The Essentials of the Doctorate of Nursing PracticeNursing Practice
Task Force charged to develop the curricular and content requirements for the DNP as well as identify the competencies to be acquired in a DNP program.
The document follows the model of the BSN and Masters Essentials
Provides direction for program development and accreditation.
Charge to Task ForceCharge to Task ForceDevelop the curricular and content requirements for
the DNP as well as identify the competencies to be acquired in a DNP program
Establish a clear strategy for educational changes and transition, and hallmarks that distinguish the DNP from existing programs that offer the Master of Science in Nursing
Identify the critical curricular content that should be present and competencies that should be acquired in the DNP programs in which master’s prepared nurses seek to acquire the DNP
Develop recommendations and strategies for AACN, and the full contingent of AACN’s academic programs to respond to this transition.
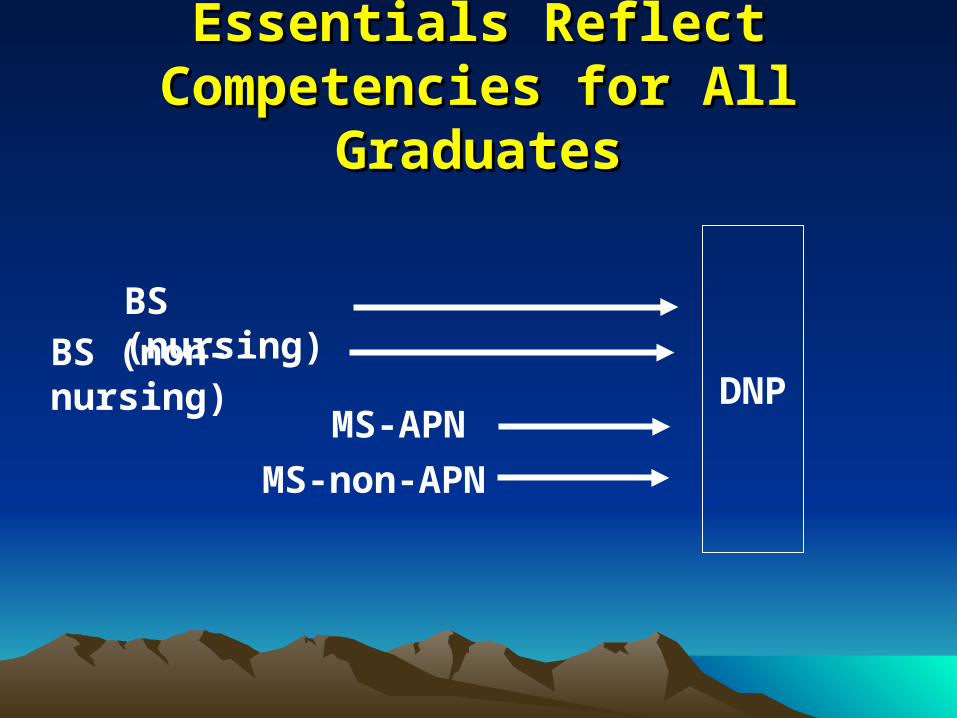
Essentials Reflect Competencies for Essentials Reflect Competencies for All GraduatesAll Graduates
DNPMS-APN
MS-non-APN
BS (nursing)BS (non-nursing)
Task Force StrategyTask Force Strategy
Re-confirm 7 essentials identified by original Practice Doctoral Task Force
Read a lot, and consult constituents and leaders
Discuss and deliberate—8th essential added
“Clinical Prevention and Population Health
for Improving the nation’s Health”
Draft document core—the essential competencies and related curricular content
Hold regional and stakeholder meeting for feedback
Post draft document on web site for feedback
Preliminary Content for the EssentialsPreliminary Content for the EssentialsIntroduction
Background/Trends leading to this paradigm shiftSummary of process and purpose of the document
Context of Graduate Education in NursingRelationship of MSN, DNP, and PhDIntegration of faculty/teaching role in graduate nursing education
Doctoral Education for nursing practiceBroad curricular model—includes links to specialty certifying bodiesDescription of 8 Essentials (document circulated at regionals)Curricular Elements (content circulated at regionals)
DNP Programs in the Academic EnvironmentCurricular parameters (eg, typical length/credit hours)Residency Capstone ProjectFaculty characteristics
Glossary
Format of Section of the DNP Essential Format of Section of the DNP Essential Draft Currently Under ReviewDraft Currently Under Review
Not the complete document or final format—only a section
Introduction
Review of 2004 TF recommendations
Summary of ProcessTask Force creation Regional meetingsDefinition of advanced nursing practice
Curriculum Model
Essential Competencies
Overview of the Curriculum ModelOverview of the Curriculum Model
DNP is a degree preparing individuals for multiple roles.
Seven of the core competencies are for all graduates regardless of role.
Core competencies form the basic foundation for advanced nursing practice (essential 8) where competencies bifurcate with the DNP program of study focusing on either:
Roles involving the direct delivery of care to individuals, families, and/or populations
Roles that influence the delivery of care indirectly through organizational and system
leadership.

Linkage of DNP Curriculum Model Linkage of DNP Curriculum Model to Specialty Practice to Specialty Practice
Specialty specific competency expectations continue to be defined by specialty groups such as NP, administration, CNS, or other specialty practice areas
7 Foundational Core Essential 7 Foundational Core Essential CompetenciesCompetencies
Advanced Nursing Practice Core Essential CompetenciesAdvanced Nursing Practice Core Essential Competencies
Direct Care CompetenciesDirect Care Competencies
Specialty Practice Competency Specialty Practice Competency ExpectationsExpectations
Systems/Organization Systems/Organization CompetenciesCompetencies
OROR
Overview of the Competency Section Overview of the Competency Section
Each of the Eight Essentials includes:• Background information which provides the
rationale for the essential nature of each competency for the highest level of nursing practice.
• A statement regarding the specific competencies for each DNP essential. Includes integration of masters level competencies while adding competencies that reflect the highest level of nursing practice
• Recommended content for each essential
Recommended DNP ContentRecommended DNP Content
Some content overlaps or is noted multiple times due to the synergistic nature of competencies and the utility of some content for more than one essential.
Content ≠ Course

Essential Competencies for DNP GraduatesEssential Competencies for DNP Graduates
1. Scientific underpinnings for practice
Recognizes the philosophical and scientific underpinnings essential for the complexity of nursing practice at the doctoral level.
2. Organizational and systems leadership for quality improvement and system thinking
Recognizes the competencies essential for improving and sustaining clinical care and health outcomes, eliminating health disparities, and promoting patient safety and excellence in care.
Essential Competencies for DNP GraduatesEssential Competencies for DNP Graduates
3. Clinical scholarship and analytical methods for evidence-based practice
Recognizes competencies essential for translation of research into practice, evaluation of practice, practice improvement, and the development and utilization of evidence-based practice.
4. Technology and information for the improvement and transformation of patient-centered health care
Recognizes competencies essential to manage, evaluate, and utilize information and technology to support and improve patient care and systems.
Essential Competencies for DNP GraduatesEssential Competencies for DNP Graduates
5. Health care policy for advocacy in health care
Recognizes the responsibility nurses practicing at the highest level have to influence safety, quality, and efficacy of care, and the essential competencies required to fulfill this responsibility.
6. Interprofessional collaboration for improving patient and population health outcomes
Recognizes the critical role collaborative teams play in today’s complex health care systems and the competencies essential for doctorally prepared nurses to play a central role on these teams.
Essential Competencies for DNP GraduatesEssential Competencies for DNP Graduates7. Clinical prevention and population health for
improving the nation’s health
Added to original competencies in response to:
• IOM 2001 call for transformation “…of health professional education in response to the changing needs of the population and the demands of practice.”
• Health People 2010 support of IOM and objective to include “core competencies in health promotion and disease prevention” in clinical education
• In consideration of nursing’s the longstanding focus on health promotion and prevention
Essential Competencies for DNP GraduatesEssential Competencies for DNP Graduates
8. Advanced nursing practice for improving the delivery of patient care
Recognizes the essential competencies reflective Recognizes the essential competencies reflective of the distinct, in-depth knowledge and skills that of the distinct, in-depth knowledge and skills that form the basis for nursing practice at the highest form the basis for nursing practice at the highest level regardless of practice role.level regardless of practice role.
Essential Competencies for DNP GraduatesEssential Competencies for DNP Graduates
8a. APN or individual and population-focused 8a. APN or individual and population-focused
competencies for the DNP graduate competencies for the DNP graduate
Recognizes the unique competencies associated with the Recognizes the unique competencies associated with the specialized knowledgespecialized knowledge and clinical expertise essential clinical expertise essential for the direct care of individuals, families, or discrete for the direct care of individuals, families, or discrete population aggregates.population aggregates.
8b. Systems or organization-focused competencies for 8b. Systems or organization-focused competencies for
the DNP graduatethe DNP graduate
Recognizes the unique competencies associated with the Recognizes the unique competencies associated with the organizational expertise and specialized knowledge organizational expertise and specialized knowledge essential for leadership of health care delivery systems.essential for leadership of health care delivery systems.
Scheduled Constituent MeetingsScheduled Constituent Meetings
Boston Regional—September 14-1576 attendees from 45 institutions
St. Louis Regional—September 29-30116 attendees from 56 institutions
Washington Stakeholder—October 11
Atlanta Regional—November 3-4Houston Regional—December 8-9San Diego Regional—January 12-13
Regional ProcessRegional Process
Gather input and as clear, consistent messages emerge they will be incorporated
Iterative process with changes made between regional meetings and posted on web site
Less clear or consistent suggestions tracked and reviewed for incorporation following completion of regional meetings
Final changes made and draft completed for submission to AACN Board by summer 2006
Final draft to membership October 2006
Feedback to DateFeedback to DateThe eight essentials are being affirmed
Minor changes and suggestions for wording and format
Need to address teaching expectations for DNP graduates
Support for duality of advanced nursing practice roles (direct care delivery and organizational-systems leadership)
Desire to control length of program is being expressed
Need further clarification of masters and DNP relationship
Feedback to DateFeedback to Date
Need direction regarding residency and capstone project
Redundancy in content across essentials, need to clarify that some content has relevance for multiple competencies.
Clarify that content does not equal course.
Some outcome competencies and content is more reflective of the masters level, need to clarify that the masters essentials have been integrated along with the addition of a higher level of practice competencies.