the construction of community holistic care - unescap.org · the concept of community-holistic care...
TRANSCRIPT

The Construction of Community Holistic Care
by the comparative analysis of Korea and
Japan’s systems
2011.11.4
Duk SUNWOO, Ph.D
Korea Inatitute for Health Social Affairs

CONTENTS
I. Introduction
II. The Major Characteristics of LTC Insurance
System of Korea and Japan
III. The Concept of Community-Holistic Care
System and Its Implication
IV. Applicability to Korea’s LTCI of Community-
Holistic Care System
V. Conclusion
I. Introduction
� Korea & Japan are providing social LTC services by the type of social insurance method.
� Japan: April of 2000
� Korea: July of 2008
� Germany: 1996(home care), 1995(institutional care)
� Both countries face financial pressure in LTCI .
� Increase in beneficiaries, especially low(mild) level
� Increase in home & institutional benefit level
� Limit of continuous raise in premiums

� What is alternatives to financial stabilization?
� Firstly, avoidance of excessively care-centered services
for beneficiaries with low level
� Secondly, intensification of community & home care-
centered system
� Thirdly, continuum of health care and welfare
services for supporting home care and the prevention
of physically & cognitively functional disability

II. Major Characteristics of LTCI
: Korea and Japan
Beneficiary
Korea(June of 2011)
Japan(May of 2011)
Total population aged 65 and over(persons) (A) 5,518,711 29,070,943
Total recognized persons as to LTC recipient (persons) (B) 296,427 4,932,639
(B)/(A)x100(%) 5.4 17.0
Rate of elderly people (%)
Persons aged 65 & over(2010) 11.3 23.1
Persons aged 75 & over(2010) 4.3 11.2
Beneficiary
� Problems
� Increase in persons with low level in both countries, who they have no nearly the needs of self-care
� Korea: level 3
� Japan: yo-kai-go 1, yo-shi-en 1, 2
� In the case of Korea, the over-supply of service providers give rise to increase in persons with low level
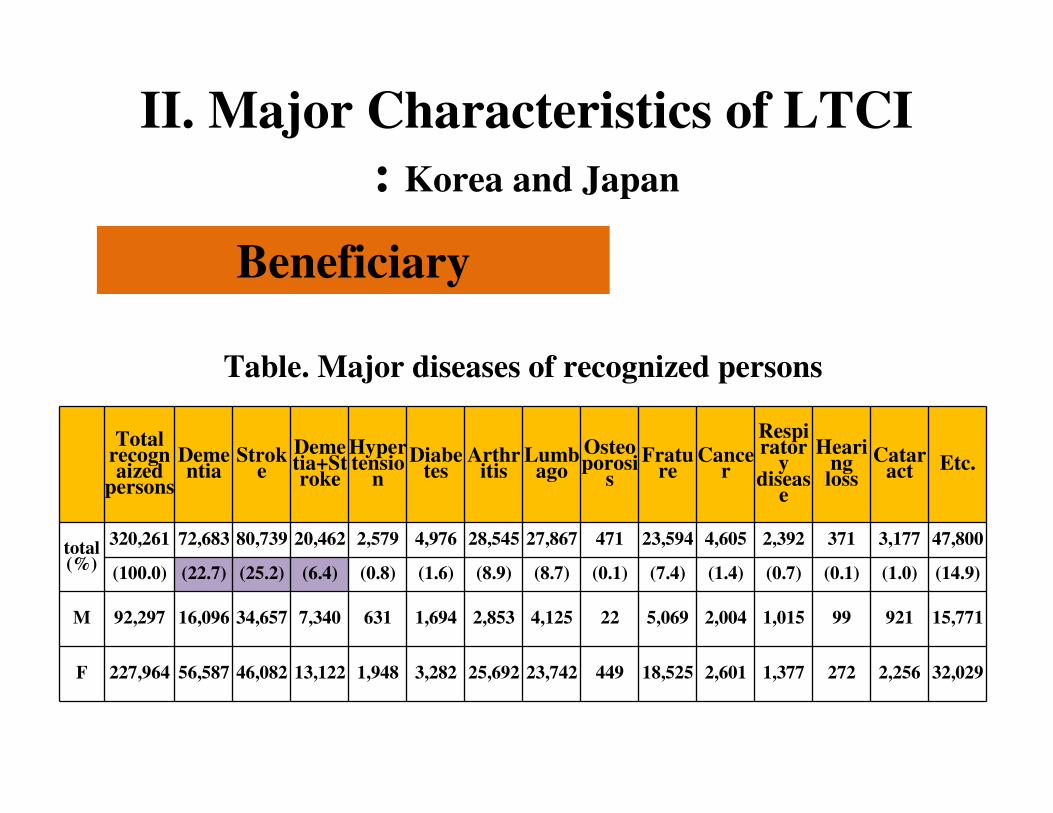
II. Major Characteristics of LTCI
: Korea and Japan
Beneficiary
Total recognaized
persons
Dementia
Stroke
Demetia+Stroke
Hypertensio
n
Diabetes
Arthritis
Lumbago
Osteoporosi
s
Frature
Cancer
Respirator
y diseas
e
Hearing loss
Cataract Etc.
total(%)
320,261 72,683 80,739 20,462 2,579 4,976 28,545 27,867 471 23,594 4,605 2,392 371 3,177 47,800
(100.0) (22.7) (25.2) (6.4) (0.8) (1.6) (8.9) (8.7) (0.1) (7.4) (1.4) (0.7) (0.1) (1.0) (14.9)
M 92,297 16,096 34,657 7,340 631 1,694 2,853 4,125 22 5,069 2,004 1,015 99 921 15,771
F 227,964 56,587 46,082 13,122 1,948 3,282 25,692 23,742 449 18,525 2,601 1,377 272 2,256 32,029
Table. Major diseases of recognized persons
Beneficiary
� Problems
� Most of underlying causes of the needs in LTC services are avoidable diseases through preventive medical care or health promotion programs, excluding natural ageing
� Those causes are similar to persons who were not recognized as a beneficiary.
� Therefore, the preventive services are necessary to stabilize finances of LTCI

Benefit
� Problems
� In the case of Korea, the continuum of medical care services is lacking in LTC services
� Nursing home : lack of physician & rehabilitative services
� Home care : lack of physician, RNs & rehabilitative services
� Most of home care benefits centered on home-help services � Home-help services tend to concentrate in domestic services, for
example, laundry, cleaning or cooking
� Therefore, the desire to admit to nursing home is very high because of various types of care services and being cared all the day

Benefit
Services recognized as a insurance benefit
Not-
covered
services
(B)
Not-covered quantities (A)
The covered services

Benefit
� Reason that not-covered quantities or services are occurred
� In the case of home care services, a monthly maximum amount to be spent is set previously
� LTC services are focused on self-care and domestic services
� Therefore, hotel costs like accommodation costs, food expenses are excluded from the benefit coverage
� Voluntary services can’t be provided for persons who are recognized as a recipient by LTCI
� Problems
� Continuous increase in insurance premium
� Premium rate (2011): 6.55% of health insurance premiums
� It’s about 0.37% of average income
� If the enlargement of coverage of recognition or the raise of unit cost plans to be performed, premium will be raised continuously
� Also, the higher continuum of health care and long-term care services results in increase in LTC expenditures and raise of premium
Financing

Governance
� Problems
� The separated system of the responsibility for LTC and community services for the elderly in case of Korea
� LTC services: National Health Insurance Corporation
� Community services for the elderly: local government
� Therefore, local governments have no incentives to constrain LTC expenditures through the preventive services
� Also, NHIC has no interest in persons who aren’t recognized as a recipient, but they become ones in the near future.

III. The Concept of Community-Holistic
Care System and Its Implication
Background
� Increase in the oldest-old people aged 75 or 85 and over
� Increase in elderly households, especially comprised of single or spouse only
� Increase in demented older persons
� Insufficiency of supply of professional (formal) care-workers

(1) Increase in the oldest-old people
� In the year of 2020, baby-boomers start to be persons aged 65 and over.
� The oldest-old persons tend to be more needs in long-term care than any other age group.
� The oldest-old persons tend to reside in the familiar living environment, called ‘ageing in place’, especially their own houses.
� Therefore, it can be said that community-based care system is appropriate for the elderly
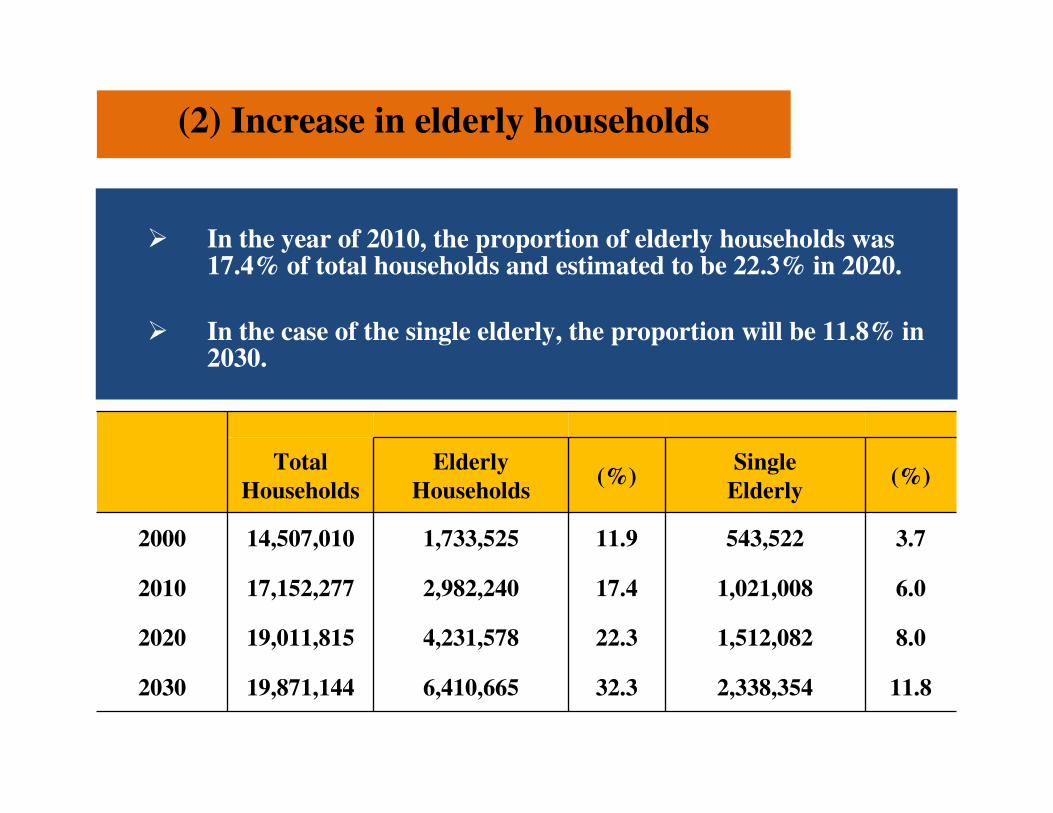
(2) Increase in elderly households
� In the year of 2010, the proportion of elderly households was 17.4% of total households and estimated to be 22.3% in 2020.
� In the case of the single elderly, the proportion will be 11.8% in 2030.
Total
Households
Elderly
Households(%)
Single
Elderly(%)
2000 14,507,010 1,733,525 11.9 543,522 3.7
2010 17,152,277 2,982,240 17.4 1,021,008 6.0
2020 19,011,815 4,231,578 22.3 1,512,082 8.0
2030 19,871,144 6,410,665 32.3 2,338,354 11.8

(3) Increase in demented older persons
� In the year of 2010, the dementia prevalence was estimated to be8.8% of the total elderly persons.
� For the demented elderly persons it is not good to make them move to other place and also the cognitive ability may be down.
2008 2009 2010 2020 2030 2040 2050
Elderly persons
aged 65 & over5,016 5,193 5,357 7,701 11,811 15,041 16,156
The demented
persons aged 65 &
over
421 445 469 750 1,135 1,685 2,127
Prevalence (%) 8.4 8.6 8.8 9.7 9.6 11.2 13.2
(4) Insufficiency of supply of professional (formal) care-workers
� Professional care workers are being trained during 240 hours and should pass a national examination for the license of formal care-worker.
� The present issues for formal care-worker
� Lower wages compared with other service employees
� Much more working hours
� Socially wrong reputation
� Informal care-givers are not utilized properly
The concept of community-holistic care system
� What is community-holistic care?
� In order to support safe, reliable and healthy daily living for the elderly,
� Only LTC services are not enough.
� Therefore, besides LTC services they need other types of health and welfare as well as housing services
The concept of community-holistic care system
� Conditions for the construction of community-holistic care
①①①① Coordination between LTC and health care services, for example, around-the-clock home health care
②②②② Reinforcement of LTC-home care, for example, around-the-clock home-help
③③③③ Ex ante prevention of functional disability
④④④④ Providence of living-support services, for example, caring, meal service, shopping
⑤⑤⑤⑤ Right-protection
⑥⑥⑥⑥ Barrier-free housing

What is community-based integrated care?
21
� The term “community-based integrated care” used in Japan is a mix of two concepts: c
ommunity-based care and integrated care.
� Recently, the debate around the possible merging of these two concepts is intensifying i
n various countries around the world.
� However, very few countries have tried to implement both of the system at the same tim
e. Holland is one of them, but the community-based integrated care system is sometime
considered as a myth or compared to a Tower of Babel in health care.

Definition by research committee of
community-based integrated care system
Definition of a community-based integrated care systemDefinition of a community-based integrated care system
Communities are delimited imaginarily as “an area of
approximately 30 minutes from a certain point” and can be pictured
as the district surrounding, for example, a middle school.
Delimiting the area of each communityDelimiting the area of each community
Community-based integrated care system is “a system within a given
community that provides the appropriate medical and long-term care
but also welfare services and various support services for the daily life
(the sphere of daily activities) of all the residents and according to their
needs”
Source: MHLW, Community-based Integrated Care Research Committee paper, p.6.Source: MHLW, Community-based Integrated Care Research Committee paper, p.6.

Japan’s Case: Three phases, two paradigm shifts : the true reasons
First paradig
m shifts
First paradig
m shifts
Second parad
igm shifts
Second parad
igm shifts
Reducing non-medic
al hospitalization
Reducing non-medic
al hospitalization
Extra expansion citiz
en’s needs for long-te
rm care service (espe
cially home care)
Extra expansion citiz
en’s needs for long-te
rm care service (espe
cially home care)

Characteristics of “care by community”
in community–based integrated care system of Japan

Daily living area level
((((smaller than school ar
ea))))
Town/Village lev
elapprox. 200,000
population
approx. 50,
000 popula
tion
C地区
Area C: Population: 70,000
• Many solitary houses in a sub
urb
• Longtime and aging residents
Area B: Population: 50,000
• Population aging in residen
tial complex• High needs for long-term c
are
Area A: Population: 70,000
• New residential area aroun
d the railway station
• High fluidity of residents
• High needs for child-raising assistance
It is necessary to construct the support base by assessing each community’s needs and u
tilizing its social resources/social capital because societal characteristics differ by region.
Area A Integrated Community S
upport Center
Area B Integrated Community
Support Center
Area C Integrated Community
Support Center
Construction of the support base based on
the community assessment by daily living areas
What are community needs?
What sort of social resources are there?How can social resources be utilized?

IV. Applicability to Korea’s LTCI of
Community-Holistic Care System
� The current system
� Persons who are recognized as a beneficiary
� Persons who are not recognized and they have a mild disability mainly.
� The former, beneficiaries by LTCI
� The latter, users by community-based elderly care service, called no-in-dol-bom services
They include health and welfare services which
are provided by various types of public center
or NPO in community

� The preparations for Korea’s community-holistic care system are
� Construction of the integrated health care system
(especially, medical care by physician)
� Construction of an available home care system around the clock
� Construction of elderly housing support system

Thank you very much for
your attention