the comprehensive fetal echo protocol - north carolina … · · 2018-02-09the comprehensive...
TRANSCRIPT

The Comprehensive
Fetal Echo Protocol
A PEDIATRIC CARDIOLGY PERSPECTIVE
John Lockhart, BSRT, RDCS
Pediatric and Fetal Echocardiographer
Duke Pediatric Echo Lab
John Lockhart BSRT, RDCS

Why this Talk?
John Lockhart BSRT, RDCS
John Lockhart BSRT, RDCS

John Lockhart BSRT, RDCS

John Lockhart BSRT, RDCS

Diagnosis and
treatment of fetal cardiac disease: A scientific statement from the American Heart Association. Journal Issue: Circulation, 129(21). http://circ.ahajournals.org/content/early/2014/04/23/01.cir.0000437597.44550.5d
John Lockhart BSRT, RDCS

• Create a protocol that satisfies IAC requirements
• Go above minimum protocol and add recommended
views from groups you trust like ASE, AIUM, ISUOG
and AHA
• Revaluate your protocol every few years and make
adjustments
John Lockhart BSRT, RDCS

John Lockhart BSRT, RDCS

Journal of the American Society of Echocardiography Volume 17 Number 7

1. Diagnosis and treatment of fetal cardiac disease: A scientific statement from the
American Heart Association. Journal Issue: Circulation, 129(21).
2. Compares protocols from several sites including their own recommendation
3. Article can be found here.
http://circ.ahajournals.org/content/early/2014/04/23/01.cir.0000437597.44550.5d
J Am Soc
Echocardiogr
2004;17:803-10.
Circulation, 129(21).John Lockhart BSRT, RDCS

Protocol Checklist
• Create a checklist and use
it!
• May want to laminate your
checklist and hang it on
your machine
• Can use dry erase markers
to fill it out
John Lockhart BSRT, RDCS

2. Take the images in the order the baby gives them to you – use
protocol checklist
3. Use ribs and spine as your guide, try to keep cuts true. Try to
keep ribs the same length on both sides when performing
transverse cuts of fetus so you won’t be off axis
4. Try scanning fetus with mom in different positions, try on her
side or reverse Trendelenburg for morbidly obese
5. When your stuck, get the baby to move – find the biggest pocket
of fluid and roll mother on side that will drop the fetus into the
fluid. Wait 5 minutes and roll mom back. Will usually get baby to
move.
John Lockhart BSRT, RDCS

Fetal Cardiac ExamFetal position and cardiac/visceral situs
Vertex or Breech
1. Sweep from cervix to fundus with transducer marker at 3 O'clock to demonstrate
fetal lie in relationship to mother
2. Determine fetal sidedness. I like right hand technique. Bronshtein M1, Gover A, Zimmer EZ.
Sonographic definition of the fetal situs. Obstet Gynecol. 2002 Jun;99(6):1129-30
3. Label head position, posterior/spine and left side of fetus
4. Look for position of heart and cardiac axis
5. Assess location of stomach bubble, liver, descending aorta, IVC and bladder as you
sweep
John Lockhart BSRT, RDCS

Fetal Cardiac ExamFetal position and cardiac/visceral situs
Vertex or Breech
John Lockhart BSRT, RDCS

• Levocardia – heart is in the left chest - Normal
• Dextrocardia – heart is in the right chest
• Mesocardia – heart is in the midline
• Does not necessarily tell you anything about looping or heart disease
• Abnormal position is associated with congenital heart disease
especially with abnormal relationship between cardiac and abdominal
situs-Heterotaxy
• You can have abnormal cardiac position with normal cardiac anatomy,
cardiac malposition can be related to external pressure from masses or
diaphragmatic hernia
John Lockhart BSRT, RDCS

• Should be approximately 45 degrees
• Abnormal cardiac axis is associated with congenital heart disease and increase morbidity
• Study “Abnormal fetal cardiac axis in the detection of intrathoracic anomalies and congenital heart disease” by Crane et al Ultrasound in Obstetrics and Gynecology 10(2):90-3 · August 1997
• Study of 409 fetal patients, 23 of 32 fetuses with abnormal cardiac axis had congenital heart disease
Cardiac Axis
John Lockhart BSRT, RDCS

Transverse fetal position1. If fetus is transverse I prefer Mayo Clinic method – Distinguishing Right From Left: A
Standardized Technique for Fetal Echocardiography JASE January–February, 1994Volume 7, Issue 1, Pages 47–53
2. Sweep from cervix to fundus with transducer marker at 3 O'clock to demonstrate fetal lie in relationship to mother (head maternal right or left)
3. Obtain long axis of the fetal spine with head to right of screen and rotate clockwise 90 degrees
4. Label head position, posterior/spine and left side of fetus and take still frame
John Lockhart BSRT, RDCS
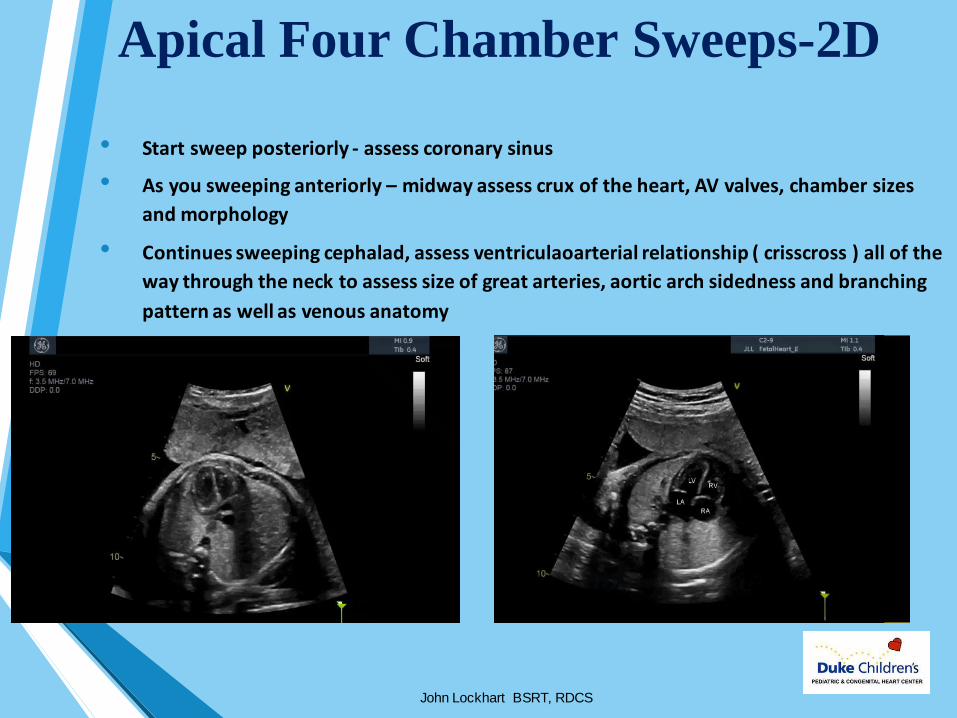
Apical Four Chamber Sweeps-2D
• Start sweep posteriorly - assess coronary sinus
• As you sweeping anteriorly – midway assess crux of the heart, AV valves, chamber sizes
and morphology
• Continues sweeping cephalad, assess ventriculaoarterial relationship ( crisscross ) all of the
way through the neck to assess size of great arteries, aortic arch sidedness and branching
pattern as well as venous anatomy
John Lockhart BSRT, RDCS

Apical Four Chamber Sweeps -Color• Scan the interventricular septum for large ventricular defects,
not a good angle for picking up small defects
• Good angle for picking up MR and TR
• Can pick up pulmonary veins as you sweep through left atrium
• Good view to assess ascending AO and ductus arteriosus by color flow Doppler
John Lockhart BSRT, RDCS

Subcostal Four Chamber Sweep-2D
• Same anatomy as apical view but better at visualizing atrial septum and ventricular septum
• Perform the sweep the same starting with coronary sinus through the head and neck vessels
John Lockhart BSRT, RDCS

Subcostal Four Chamber Sweep-Color
• Scan interventricular septum thoroughly - drop your Nyquist limit into the 50s
• Best view for assess ventricular level shunts
• Pulmonary veins and atrial level shunt are well visualized from this view
• Sweep all the way posteriorly through coronary sinus and anteriorly till you are out of
the heart
John Lockhart BSRT, RDCS

Short Axis Sweep• Start from apex of heart all the way through the arches
• Structures visualized include Ao Arch, Ductal Arch, RVOT, PV ,MPA,
PA branches, AOV, MV and entire ventricular septum
John Lockhart BSRT, RDCS

Short Axis Sweep-Color• Sweep all the way through the ventricular mass and arches
• Drop Nyquist limit to help screen for ventricular septal defect
• Pay attention to color flow in arches for aliasing, ductal restriction
John Lockhart BSRT, RDCS

ClipsApical Four Chamber View
• Crux of the heart – Atrioventricular valve level (MV,TV, common valve)
• Size and morphology of ventricles (moderator band, chordal attachments)
• Size of atria
• 2D of pulmonary veins
• Coronary sinus with posterior angulation
John Lockhart BSRT, RDCS

• Look for atrioventricular valve
regurgitation (MR and TR)
• Usually see at least one
pulmonary vein
ClipsApical Four Chamber View -Color
John Lockhart BSRT, RDCS

• Crux of the heart – primum atrial septal defects, inlet and muscular ventricular septal defects
• Chamber sizes
• Flap of the foramen
• 2D of pulmonary veins
ClipsSubcostal Four Chamber View
John Lockhart BSRT, RDCS
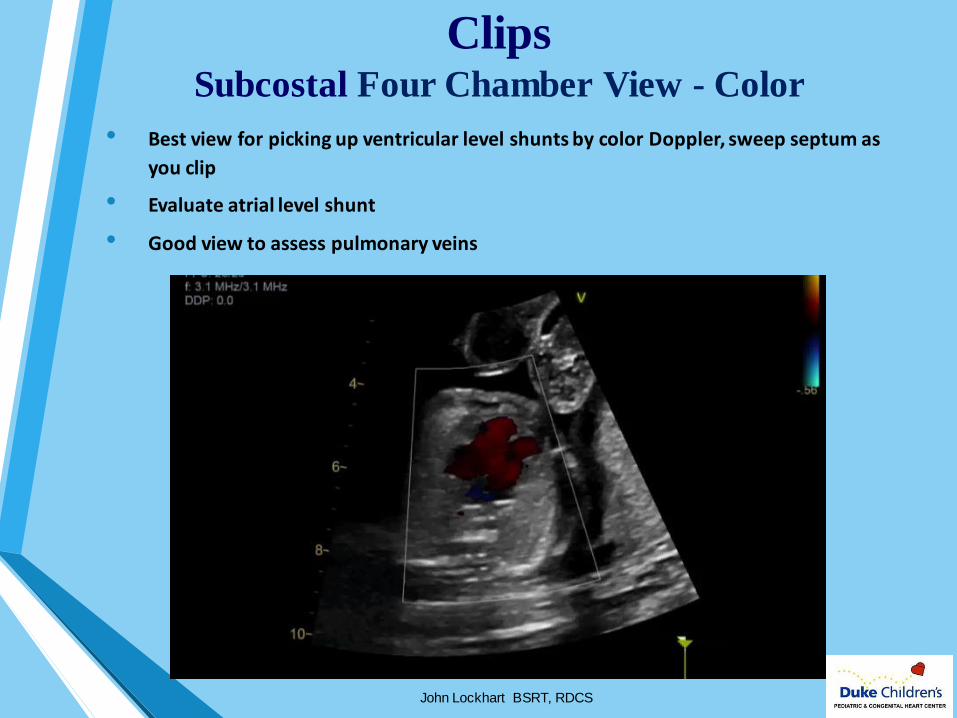
ClipsSubcostal Four Chamber View - Color
• Best view for picking up ventricular level shunts by color Doppler, sweep septum as
you clip
• Evaluate atrial level shunt
• Good view to assess pulmonary veins
John Lockhart BSRT, RDCS

LVOT• Mitral aortic valve continuity
• Size of MV, AOV, and ascending aorta
John Lockhart BSRT, RDCS

ClipsLV and MV SAX
• Assess biventricular function
• Make sure you see anterior leaflet of the MV, rule out a cleft
John Lockhart BSRT, RDCS

RVOT• Assess infundibulum, PV, main pulmonary artery
• Establish that RVOT crosses LVOT
• Short axis view – assess conal septum, infundibulum, PV, MPA and branch pulmonary
arteries (PSAX)
• With slight angulation you should see ductus arteriosus
John Lockhart BSRT, RDCS

ClipsPSAX and AOV
• Zoom on aortic valve and leaflets to assess mobility
John Lockhart BSRT, RDCS

ClipsAortic and Ductal Arches
• Show head vessels on aortic (hairy) arch
• Ductal (bald) arch more hockey stick in appearance
John Lockhart BSRT, RDCS

Aortic and Ductal Arches- Color
• Look for aliasing
John Lockhart BSRT, RDCS

Special Views3 Vessel View
• Structures visualized: Superior Vena Cava and innominate vein, ascending aorta and
isthmus, main pulmonary artery ductus arteriosus and trachea
• Assess size discrepancies between vessels - can be subtle indicator of pathology
• Sweeping will demonstrate arch sidedness, arch branching as well as venous anatomy.
John Lockhart BSRT, RDCS

Special Views3 Vessel View Continued
• Sweeping will demonstrate arch sidedness, arch branching as well as venous anatomy.
• Put color flow on innominate vein to prove it is a venous structure
John Lockhart BSRT, RDCS

Bicaval View
• Structures visualized: Superior Vena Cava, right atrium, inferior vena cava, hepatic veins
John Lockhart BSRT, RDCS

Pulmonary Veins• Must see at least one left and one right pulmonary vein
• Drop Nyquist limit way down to identify pulmonary veins easier.
• Use small sample size and pulse out in parenchyma
• 4 chamber views or short axis views
• Pulsed wave Doppler at least one right and one left pulmonary vein
John Lockhart BSRT, RDCS

• Cone shaped structure that serves to restrict flow and direct it across the atrial septum
• Easily identified by aliasing of color flow Doppler
• Flow profile very important to assess fetal circulatory state and cardiovascular health
• Very small structure so use a small sampling gate when interrogating with PW Doppler, 1 to
2mm
Ductus Venosus
John Lockhart BSRT, RDCS

Ductus Venosus
• Look for decreased A –wave, A-wave reversal sign of increased right atrial pressure
John Lockhart BSRT, RDCS

Ductus Venosus
• Reversal of flow can be an indicator of poor fetal circulatory state
• With certain right heart lesions can be an expected finding, Tr Atr, HRH, due to elevated
right atrial pressure
John Lockhart BSRT, RDCS

RhythmPW Doppler and M-Mode
• We record mechanical PR on every patient (not required)
• Place pulsed wave Doppler sample between MV and AoV in apical 4ch or LAX view, widen Doppler sample so that it covers both part of AoV and MV, about
4mm
• Obtain heart rate from aortic flow clicks
• Assess rhythm from M-Mode
John Lockhart BSRT, RDCS

SVT
John Lockhart BSRT, RDCS
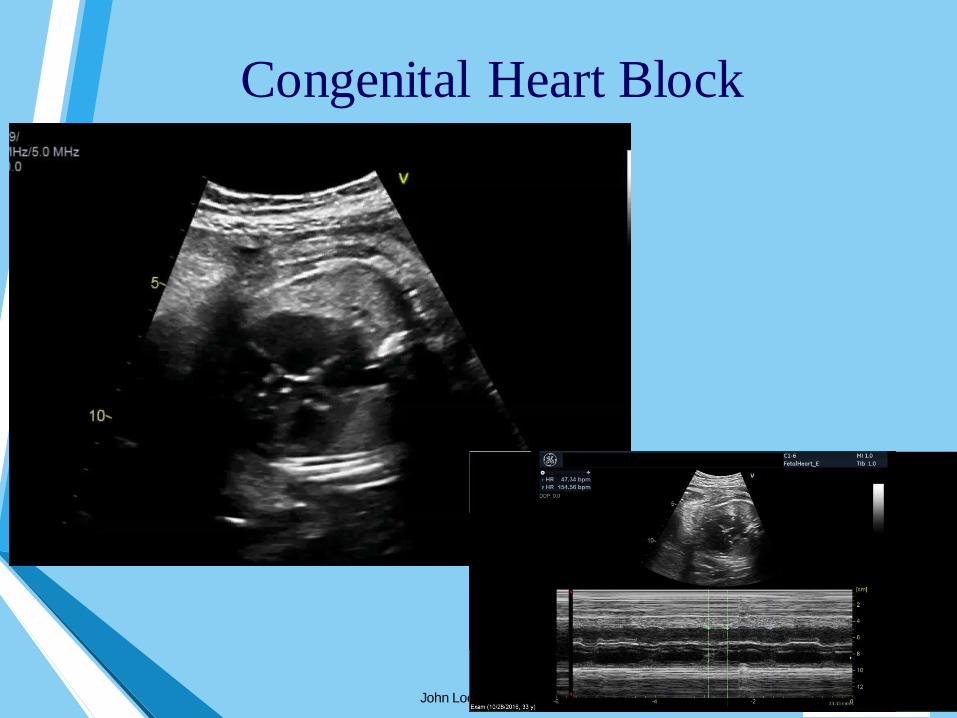
Congenital Heart Block
John Lockhart BSRT, RDCS

Measurements• Measure diameter of all four valves, Boston Z-scores database available at
http://zscore.chboston.org/
• Record Z-scores in report for all valves
• Measure aortic isthmus and ductal isthmus
• 3VV measure MPA and AAO if they look abnormal
• Measure LV and RV length and diameter
John Lockhart BSRT, RDCS

• Increases throughout pregnancy, 11-12 weeks ~ .38, 17 to 20 weeks ~
.45, Term ~ .5
• Should always be . 5 or less
• Predictor of extent of lung compression, poor outcomes
• Critical in patients with severe TR (TV dysplasia, Ebstein’s anomaly)
and often associated with hydrops
• Increased CT ratio often seen with complete heart block~NORMAL EBSTEIN’S CHB
John Lockhart BSRT, RDCS

Gestational Age
1. All our patients are referrals -in cardiology we used to always take gestational age from OB reports
2. Guidelines now require us to measure gestational age ourselves
3. Must obtain a FL, BPD or head circumference
4. We use FL, for us it’s the most reproducible
John Lockhart BSRT, RDCS

Doppler• All four valves, use CW if above Nyquist limit
• Ductus arteriosus and aortic isthmus
• Ductus venosus, umbilical artery, umbilical vein and middle cerebral
artery (MCA)
John Lockhart BSRT, RDCS

Umbilical Vein
• Normal cord has three vessels, two arteries and one vein.
• Two vessel cord has increased risk of congenital anomalies including cardiac
• Pulse a free loop halfway between placenta and insertion
• Gate large enough to capture vein and artery at same time
• Umbilical vein carries oxygenated blood to fetus
• Pulsations in vein can be indicative of cardiac disease
• Diastolic pulsations - cardiac diastolic dysfunction
• Systolic pulsations – severe tricuspid regurgitation
• Use UA for reference for timing
John Lockhart BSRT, RDCS
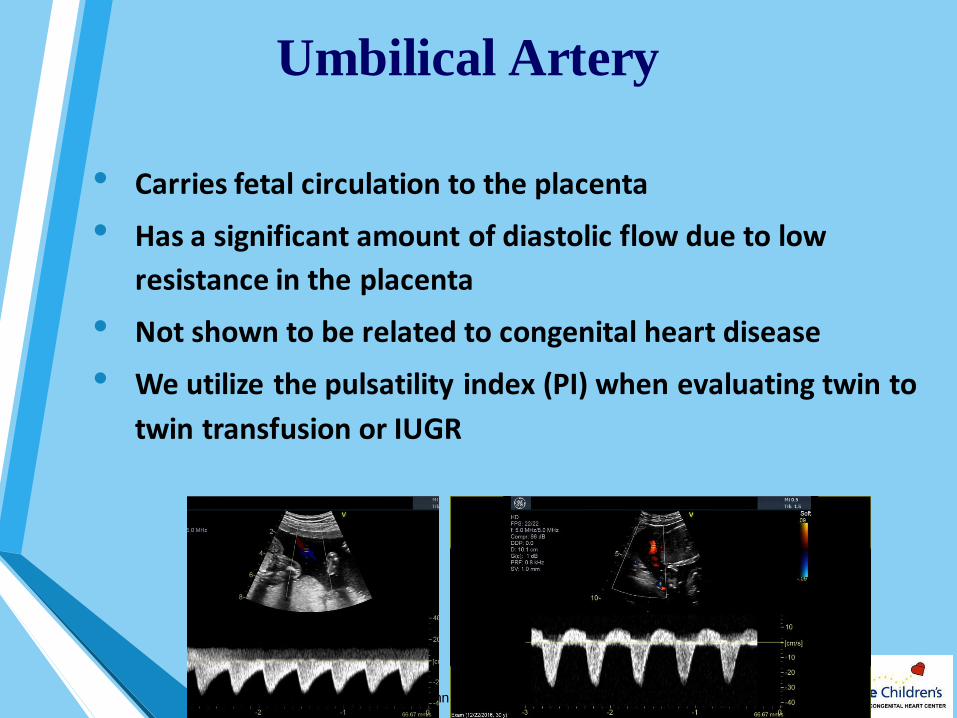
Umbilical Artery
• Carries fetal circulation to the placenta
• Has a significant amount of diastolic flow due to low
resistance in the placenta
• Not shown to be related to congenital heart disease
• We utilize the pulsatility index (PI) when evaluating twin to
twin transfusion or IUGR
John Lockhart BSRT, RDCS
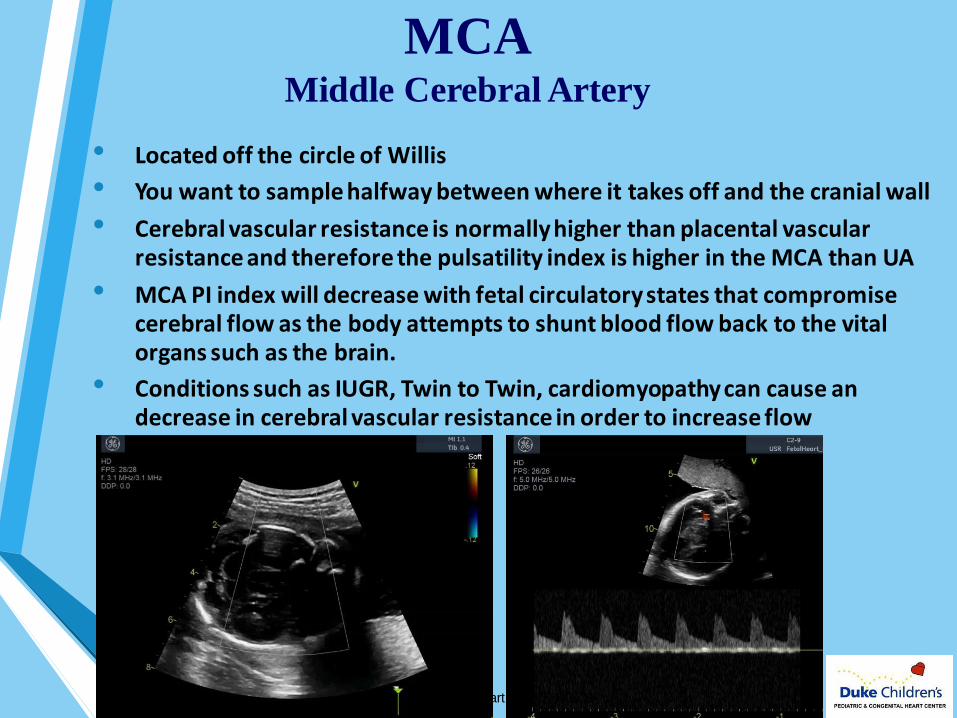
MCAMiddle Cerebral Artery
• Located off the circle of Willis
• You want to sample halfway between where it takes off and the cranial wall
• Cerebral vascular resistance is normally higher than placental vascular resistance and therefore the pulsatility index is higher in the MCA than UA
• MCA PI index will decrease with fetal circulatory states that compromise cerebral flow as the body attempts to shunt blood flow back to the vital organs such as the brain.
• Conditions such as IUGR, Twin to Twin, cardiomyopathy can cause an decrease in cerebral vascular resistance in order to increase flow
John Lockhart BSRT, RDCS

Special ViewsDuctus Venosus
• Cone shaped structure that serves to restrict flow and direct it across the atrial septum
• Easily identified by aliasing of color flow Doppler
• Flow profile very important to assess fetal circulatory state and cardiovascular health
• Very small structure so use a small sampling gate when interrogating with PW Doppler, 1 to
2mm
John Lockhart BSRT, RDCS

Fetal
Hypoplastic Left Heart
Newborn
Hypoplastic Left Heart

Pathology HLH
John Lockhart BSRT, RDCS

John Lockhart BSRT, RDCS

John Lockhart BSRT, RDCS

Normal at 14 1/7 Weeks TOF at 13 1/7 weeks
John Lockhart BSRT, RDCS

Images courtesy of A Moon - Grady, UCSFJohn Lockhart BSRT, RDCS

Images courtesy of A Moon - Grady, UCSFJohn Lockhart BSRT, RDCS

•Be regimented and disciplined in
your protocol
•Use a checklist
•Be stubborn, don’t give up till
you figure out the puzzle
John Lockhart BSRT, RDCS

THANK YOU
John Lockhart BSRT, RDCS
Please feel free to contact me if you have any
questions about a pediatric echo
• Duke University Hospital
• Work Phone # 919-681-5166
• Cell# 214-649-9086