the chocolate balloon - ici...
TRANSCRIPT

The Chocolate Balloon
David Planer, MD

• I, David Planer, MD, DO NOT have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context of the subject of this presentation.

Inflation with conventional balloons can result in vessel trauma — which often leads to dissection.
Intended for illustrative purposes only.
Torsional Stress: Twisting
Radial Stress: Expanding
Longitudinal Stress: Elongating
CHALLENGE: Acute Vessel Trauma

Acute vessel trauma with POBA
• POBA can cause dissections, vessel wall trauma, and edge injury

Controlled dilatation with Chocolate • Predictable luminal gain with unique pillows and grooves
design 1,2
• Reduced dog-boning and edge injury 3
• Demonstrated low rates of dissection & bailout stenting 2
1 Predictable: less dissection and less bailout stenting 2 Chocolate BAR interim results 3 Cadaver data on file at TriReme Medical, LLC

Chocolate Balloons
Non-coated Drug-coated
Co
ron
ary
Pe
rip
he
ral
PTCA
PTA

N=174
No Flow Limiting Dissection 97%
(219/226)
Achieved <30% Diameter Stenosis
physician visual estimate
94%
(212/226)
Freedom from Bail-Out Stenting 96%
(218/226))
Dissection Rates
3%
8%
12%
Chocolate BAR Odink, PTA
Study
Bosiers, PTA
Arm
Bail-Out Stenting Rates
4% 5%
12% 14%
20%
Chocolate
BAR
Schmidt
BTK DEB
Bosiers,
PTA Arm
Schmidt
BTK PTA
Odink,
PTA Study
How
does this
compare?
Odink H, van den Berg A, Winkens B. Technical and clinical long-term results of infrapopliteal percutaneous transluminal angioplasty for critical limb ischemia. J Vasc Inter radio. Apr 2012: 23(4):461-467 Boisers M, Scheinert D, Peetrs P, Torsello G, Zeller T, Delosse K, Schmidt A, Tosserek J, Vinck E, Schwartz L. Randomized comparison of everolimus-eluting versus bare-metal stents in patients with critical limb ischemia and infrapopliteal arterial occlusive disease. J Vasc Surg Feb 201255(2):390-398 Schmidt A, Piorkowski M, Werner M, Ulrich M, Bausback Y, Braunlich S, Ick H, Schuster J, Botsios S, Kruse H, Varcoe R, Scheinert D. First Experience with Drug-Eluting Balloons in Infrapopliteal Arteries. JACC Sep 2011 58(11): 1105-1109 Schmidt A, Ulrich M, Winkler B, Klaeffling C, Bausback Y, Braunlich S, Botsios S, Kruse H, Varcoe R, Scheinert D. Angiographic Patency and Clinical Outcome After Balloon-Angioplasty for Extensive Infrapopliteal Arterial Disease.
Chocolate BAR: BTK Procedural Success

Outcomes
Chocolate BAR BTK
Cohort PTA
Balloon
Literature BTK
References PTA *
Procedural Outcomes
Bail-Out stent placement 3.5% 9.9%
30-Day Outcomes
Target lesion revascularization 2.2% 8.1%
Major amputation 1.3% 4.4% - 6.6%
Mortality 0.9% 1.7% - 3.3%
6-Month Outcomes
Target lesion revascularization 9.0% 16.0%
Major amputation 3.2% 11.8%
Mortality 2.9% 7.7% *References:
Razavi MK, Mustapha JA, Miller LE. Contemporary systematic review and meta-analysis of early outcomes with percutaneous treatment for infrapopliteal atherosclerotic disease. Jour of Vasc and Intervent Radiol : JVIR 2014;25:1489-96, 96 e1-3.
Romiti M, Albers M, Brochado-Neto FC, Durazzo AE, Pereira CA, De Luccia N. Meta-analysis of infrapopliteal angioplasty for chronic critical limb ischemia. J Vasc Surg 2008;47:975-81.
Boisers, Marc on behlaf of AMS investigators. 6-Month Analysis AMS INSIGHT—Absorbable Metal Stent Implantation for Treatment of Below-the-Knee Critical Limb Ischemia: 6-Month Analysis. Cardiovasc Intervent Radiol (2009) 32:424–435 (PTA control group)
Chocolate BAR: BTK Clinical Outcomes

Chocolate PTCA Case Dr. William Gray, Columbia Medical Center, NY
• LCx/OM1 bifurcation (Medina 1,1,1) • Chocolate® into the OM1 branch; first 2.5mm
and then 3.0mm (12 atm for 90 secs) • DES in main vessel – excellent final result
73 year old female Previous PCI
Pre-intervention After Chocolate® Post-intervention
In this complex case, the angiographic outcome after the use of Chocolate PTCA was exceptional. - Dr. William Gray

Chocolate PTCA Case Dr. Manish Parikh, Columbia Medical Center, NY
Chocolate is the ideal balloon for vessel preparation because it offers predictable luminal gain even in calcified lesions. - Dr. Manish Parikh
Pre-intervention
• Two de novo lesions in the RCA • Moderate tortuosity and moderately calcified (Type B).
• 2.5mm x 20mm Chocolate® PTCA Balloon Catheter was used to predilate both lesions (16 ATM for 20 sec each)
• DES to cover both lesions – excellent final result
60 year old male Stable Angina Previous PCI
Inflated Chocolate® Post-intervention

Chocolate Touch
Chocolate platform for controlled inflation
• Predictable luminal gain with unique pillows and grooves design 1,2,3
• Reduced dog-boning and edge injury 4
• Demonstrated low rates of flow-limiting dissection and bail out stenting 2,3
1 Predictable: less dissection and less bailout stenting 2 Chocolate BAR interim results 3 ENDURE interim results 4 Cadaver data on file at TriReme Medical, LLC
Long term effect of paclitaxel
• Clinically proven anti-proliferative agent to inhibit neointimal hyperplasia
• 3 µg/mm2 dose of paclitaxel
• Crystalline paclitaxel coating with hydrophilic excipient developed in collaboration with InnoRa GmbH
+

Core Lab Adjudicated Data (N=70)
Flow Limiting Dissections (0 / 69) 2
>50% Diameter Stenosis 1.4% (1/69) 2
Bail-out Stenting 1 Per protocol stent was permitted with flow-limiting dissection or >50% stenosis
1.4% (1/69) 2
1 Additional non-bail-out stents were placed per operator discretion. In all cases in which these stents were placed the Chocolate Touch balloon was adjudicated to be undersized less than 1:1
2 Post Chocolate Touch inflation assessment could not be completed in one patient
• This study did not require pre-dilatation. The IN.Pact global registry, which also did not require pre-dilatation, reported 24.7% provisional stenting.
• Many other DCB studies exclude suboptimal pre-dilatation outcomes from enrollment
ENDURE Study Procedural Review

Per Protocol
Clinically driven TLR 1
Amputation 0
Death 0
Other
TLR (Asymptomatic) 3 *
Thrombosis 0
ENDURE Interim Results at 6 months
Major Adverse Events Patency
(N=54)
All Patients 88.9%
(48/54)
Patients Treated per Protocol
90.0%
(45/50)
* Interventions performed during 6 month follow-up angiogram with no reported clinical symptoms Patency based upon Duplex Ultrasound Review by the DUS Corelab (Vascore, Boston MA) Study Follow-up and Event adjudication is on-going

-0.1
0
0.1
0.2
0.3
0.4
0.5
0.6
(N=49)
Mean 0.16
Std Dev ±0.72
Lutonix®
Stellarex™
Chocolate® Touch
IN.PACT®
Based upon Angiogram QVA analysis by the QVA Corelab (Yale University, New Haven, CT ) Study Follow-up and Data Review is on-going (4 patients still missing) Comparisons based on these studies: PACIFIER (IN.Pact), ENDURE (Chocolate Touch), LEVANT I (Lutonix), ILLUMENTAE (Stellarex)
0.54 0.45
0.16 -0.01
ENDURE Interim Results at 6 months
Late Lumen Loss LLL compared to other DCBs

ENDURE Case: Pre-intervention

ENDURE Case: Post-intervention

ENDURE Case: 6-mo follow-up

Patient Characteristics Per patient
Age Average (Range)
59 years (34-76 years)
Male 72.7% (14/19) Diabetes 47.4% (9/19)
Tobacco Use 31.6% (6/19)
Calculated BMI Average (Range)
29.5 (22.0 – 37.5)
History of Hypertension
100% (19/19)
History of Hyperlipidemia
63.2% (12/19)
History of Myocardial Infarction
52.6% (10/19)
A total of 19 patients have been enrolled between April & Aug 2015
Site Reported Data (N=19)
Vessel Involvement
2 Vessels Treated
1 Vessel Treated
36.8% (7/19) 63.2% (12/19)
Target Vessel
LCX
RCA
LAD
Ramus
36.8% (7/19)
31.6% (6/19)
26.3% (5/19)
5.3% (1/19)
Calcification* Mild
Moderate
84.2% (16/19)
15.8% (3/19)
Lesion Complexity*
Type A
Type B
Type C
36.8% (7/19)
42.1% (8/19)
5.3% (1/19)
Lesion Length*
12.1 mm (3 -18mm)
Pre-treatment Post- Treatment
% DS * 69.3% ±15.9 18.0% ±8.5
Lesion Characteristics
Population Chocolate Heart: First in Human

Procedural Complications in Chocolate Heart FIH study:
Historical PTCA Balloon Procedural Complications:
Bail out stent placement 0% (0/19)
Significant Dissection 0% (0/19)
Abrupt Closure 0% (0/19)
Sub-Acute Occlusion 0% (0/19)
Bail out CABG 2.7 – 10.1%
Dissections (Types not specified)
29.0 – 35.0%
Abrupt Closure 1.7 – 9.4%
1: The Bypass Angioplasty Revascularization Investigation (BARI) Investigators. Comparison of coronary bypass surgery with angioplasty in patients with multivessel disease. N Engl J Med. 1996 Jul 25;335(4):217-25. Erratum in: N Engl J Med 1997 Jan 9;336(2):147. PubMed PMID: 8657237. 2: King SB 3rd, Lembo NJ, Weintraub WS, Kosinski AS, Barnhart HX, Kutner MH, Alazraki NP, Guyton RA, Zhao XQ. A randomized trial comparing coronary angioplasty with coronary bypass surgery. Emory Angioplasty versus Surgery Trial (EAST). N Engl J Med. 1994 Oct 20;331(16):1044-50. PubMed PMID: 8090163. 3: Black AJ, Namay DL, Niederman AL, Lembo NJ, Roubin GS, Douglas JS Jr, King SB 3rd. Tear or dissection after coronary angioplasty. Morphologic correlates of an ischemic complication. Circulation. 1989 May;79(5):1035-42. PubMed PMID: 2523763. 4: Bredlau CE, Roubin GS, Leimgruber PP, Douglas JS Jr, King SB 3rd, Gruentzig AR. In-hospital morbidity and mortality in patients undergoing elective coronary angioplasty. Circulation. 1985 Nov;72(5):1044-52. PubMed PMID: 2931211. 5: Ellis SG, Roubin GS, King SB 3rd, Douglas JS Jr, Weintraub WS, Thomas RG, Cox WR. Angiographic and clinical predictors of acute closure after native vessel coronary angioplasty. Circulation. 1988 Feb;77(2):372-9. PubMed PMID: 2962787
Procedural Outcomes
Chocolate Heart: First in Human
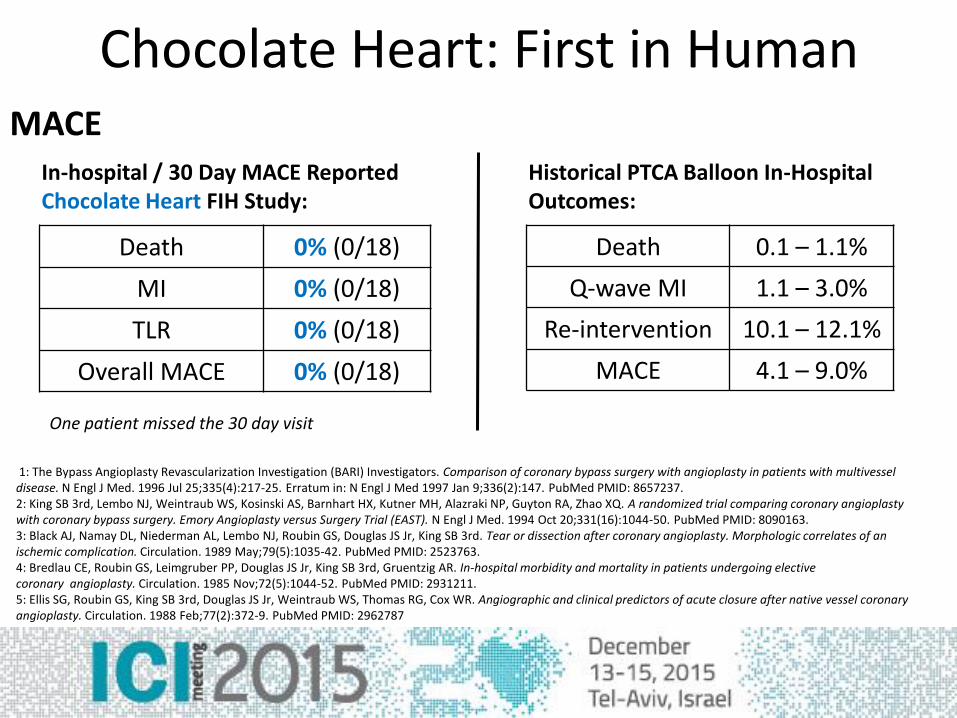
Death 0% (0/18)
MI 0% (0/18)
TLR 0% (0/18)
Overall MACE 0% (0/18)
Death 0.1 – 1.1%
Q-wave MI 1.1 – 3.0%
Re-intervention 10.1 – 12.1%
MACE 4.1 – 9.0%
1: The Bypass Angioplasty Revascularization Investigation (BARI) Investigators. Comparison of coronary bypass surgery with angioplasty in patients with multivessel disease. N Engl J Med. 1996 Jul 25;335(4):217-25. Erratum in: N Engl J Med 1997 Jan 9;336(2):147. PubMed PMID: 8657237. 2: King SB 3rd, Lembo NJ, Weintraub WS, Kosinski AS, Barnhart HX, Kutner MH, Alazraki NP, Guyton RA, Zhao XQ. A randomized trial comparing coronary angioplasty with coronary bypass surgery. Emory Angioplasty versus Surgery Trial (EAST). N Engl J Med. 1994 Oct 20;331(16):1044-50. PubMed PMID: 8090163. 3: Black AJ, Namay DL, Niederman AL, Lembo NJ, Roubin GS, Douglas JS Jr, King SB 3rd. Tear or dissection after coronary angioplasty. Morphologic correlates of an ischemic complication. Circulation. 1989 May;79(5):1035-42. PubMed PMID: 2523763. 4: Bredlau CE, Roubin GS, Leimgruber PP, Douglas JS Jr, King SB 3rd, Gruentzig AR. In-hospital morbidity and mortality in patients undergoing elective coronary angioplasty. Circulation. 1985 Nov;72(5):1044-52. PubMed PMID: 2931211. 5: Ellis SG, Roubin GS, King SB 3rd, Douglas JS Jr, Weintraub WS, Thomas RG, Cox WR. Angiographic and clinical predictors of acute closure after native vessel coronary angioplasty. Circulation. 1988 Feb;77(2):372-9. PubMed PMID: 2962787
One patient missed the 30 day visit
In-hospital / 30 Day MACE Reported Chocolate Heart FIH Study:
Historical PTCA Balloon In-Hospital Outcomes:
MACE
Chocolate Heart: First in Human

Thank You תודה