the bidirectional ‘rendezvous’ endoscopic technique in the management of impassable strictures...
TRANSCRIPT
The bidirectional ‘Rendezvous’ endoscopic technique in the management of impassable
strictures following radical chemo-radiotherapy for head and
neck/oesophageal SCCMr A Madhavan
Mr AW PhillipsMr SM Dresner

Introduction
• Oesophageal strictures common complication post chemo-radiotherapy for advance neck and thoracic malignancies (1,2)
• Incidence 3.4% patients receiving radiotherapy alone, 18-26% receiving chemo-radiotherapy (2,3)
• Affect cervical oesophagus– Dysphagia– Risk of aspiration

Introduction
• Subsequent fibrosis, tissue fragility and altered anatomy – Difficulty identifying oesophageal lumen
• Management challenging – Conventional endoscopy difficult• Location – Cervical oesophagus
– “Blind” use of guide wire/balloon dilatation – false lumen or frank perforation (4)

Method• Retrospective review between 2011 – 2013• Standard Anterograde-retrograde approach• Total of 7 patients– 6 patients with oropharyngeal carcinoma– 1 patient with distal oesophageal carcinoma
• All patients had PEG prior to adjuvant treatment• Pre-procedure investigations– Barium Swallow +/- CT neck/thorax
• All patients complete obstruction at level of stricture
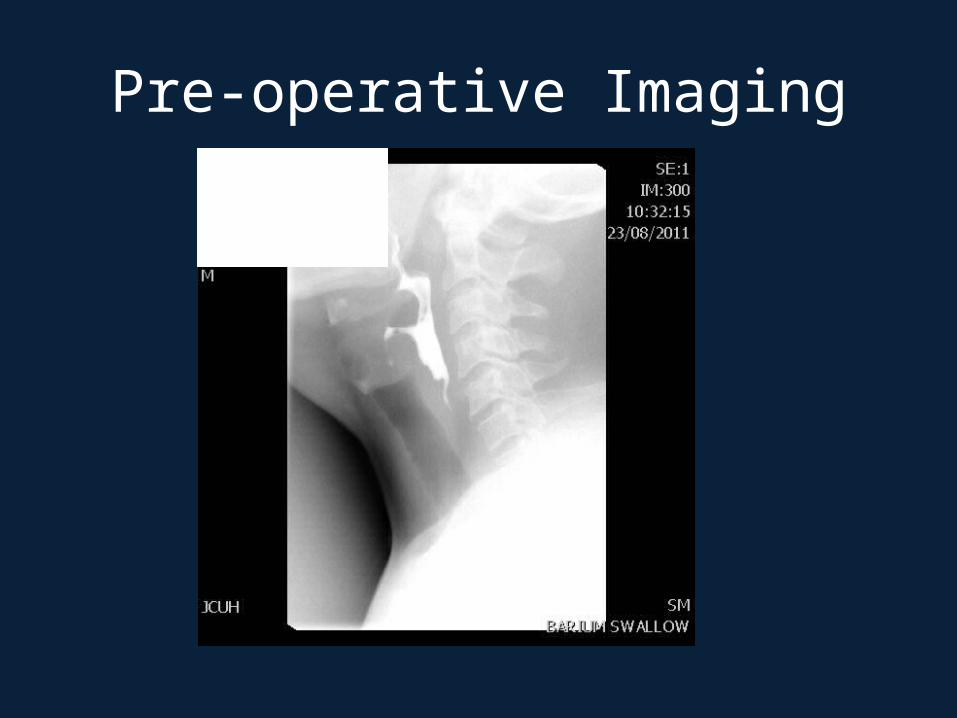
Pre-operative Imaging
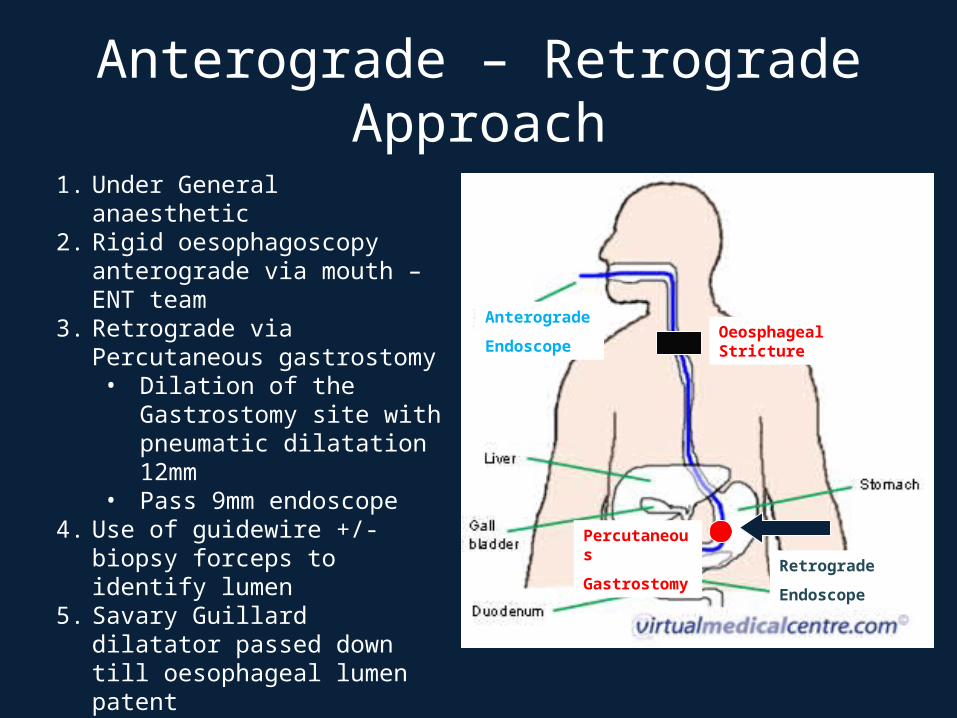
Anterograde – Retrograde Approach
1. Under General anaesthetic2. Rigid oesophagoscopy anterograde
via mouth – ENT team3. Retrograde via Percutaneous
gastrostomy• Dilation of the Gastrostomy
site with pneumatic dilatation 12mm
• Pass 9mm endoscope 4. Use of guidewire +/- biopsy forceps
to identify lumen5. Savary Guillard dilatator passed
down till oesophageal lumen patent6. NG is left in, PEG replaced7. Diet introduced gradually
Oeosphageal Stricture
Anterograde
Endoscope
Retrograde
Endoscope
Percutaneous
Gastrostomy


ResultsTotal of 7 patients• Male : Female – 5:2• Age – 59 (42 – 71)
•6 patients with oropharyngeal carcinoma• 2 patients had total laryngectomy • Adjuvant Treatment• 4 patients – chemoradiotherapy• 2 patients – radiotherapy
•1 patients with oesophageal carcinoma•Length of stay – 6 (4-20)
Results
Intra-operative complication• 1 patient – stomach detached from abdominal
wall at gastrostomy site following dilatation• Required laparoscopy for repair
Post operative •Follow up with ENT team •All patients tolerating soft diet

Discussion• Anterograde-retrograde rendevous technique
described Van Tisk et al in 1998 (5)
• Boyce et al (6)– 25 year experience with endoscopic lumen restoration
(ELR), Median F/U – 22 months– Standard approach, tri-plane fluroscopy, retrogarde
dilatation, swallowing rehab therapy– 33 patients with head/neck cancers– Successful cannulation + procedure 39/33 (91%)– Return to soft diet 15/30 (50%), 10/30 (33%) unsafe
swallow due to neuromotor defecit– Complications 5/30 (17%), anastomotic fistula 2/30 (6.7%)

Discussion
• Use of guidewire and bougie dilatation• Long stenosis use of blunt instrument +/- CO2
laser (7) • Retrograde approach use of rigid
bronchoscope (7)• Use of ERCP catheter for cannulation of
stricture (8)

Conclusion• Safe approach for patients with oesophageal
strictures post radio-chemotherapy• Individual cases may need variation in
technique• Good outcomes– 6/7 patients able to soft diet– Positive impact quality of life
• Swallowing rehabilitation post treatment

References1. De Boer et al. Rehabilitation Outcomes of longterm survival treated for head and
neck cancers. Head Neck. 1995; 17 503-5152. Laurell et al. Stricture of the proximal oesophagus in head and neck carcinoma
patients after radiotherapy. Cancer 2003; 97:1693-17003. Lawson et al. Frequency of oesophageal stenosis after simultaneous modulated
accelerated radiation therapy and chemotherapy for head and neck cancer. American journal of Otolaryngology 2008:29; 13-19
4. Banergee et al. Intrathoracic oesophageal perforation following bougienage: a protocol for management. Aust N Z Journal Surg. 1989;59: 563-6
5. Van Twisk et al. Retrograde approach to pharyngo-oesophageal obstruction. Gastrointestinal Endoscopy 1998; 48:296-9
6. Boyce et al. Endoscopic lumen restoration for obstructive aphagia: outcomes of a 25-year experience Gastrointest Endosc. 2012 Jul;76(1):25-31. doi: 10.1016/j.gie.2012.02.037.
7. Kos et al. Anterograde-Retrograde rendevous approach for radiation-induced complete upper oesophageal sphincter stenosis: case report and literature review. Journal of Laryngology and Otology 2011, 125, 761-764
8. Takeshi et al. Successful endoscopic dilatation of a severe stricture of the cervical oesophagus after defintive combined chemotherapy plus radiotherapy for oesophageal cancer. Oesophagus 2012 9;252-256