the art of treating hypertension - everything should be made as simple as possible, but not simpler....
TRANSCRIPT

Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
THE ART OF TREATING HYPERTENSION

www.strokeandhypertension2014.co.za

Lewington et al. Lancet 2002;360:1903–13
Cardiovascular Mortality Risk Doubles with Each
20/10 mmHg Increment in Systolic/Diastolic BP*
Cardiovascular mortality risk
0
2
4
8
115/75 135/85 155/95 175/105
6
Systolic BP/Diastolic BP (mmHg)
*Individuals aged 40–69 years
2X
risk
4X
risk
8X
risk
1X risk

BENEFITS OF LOWERING BP
(12/6 mmHg)
• Stroke ↓ 35-40%
• MI ↓ 20-25%
• CCF ↓ 50%
• Stage 1 with 1 risk factor, SBP ↓ 12 mmHg
for 10 years prevents 1 death for 11 treated
• Stage 1 plus TOD – only 9 patients
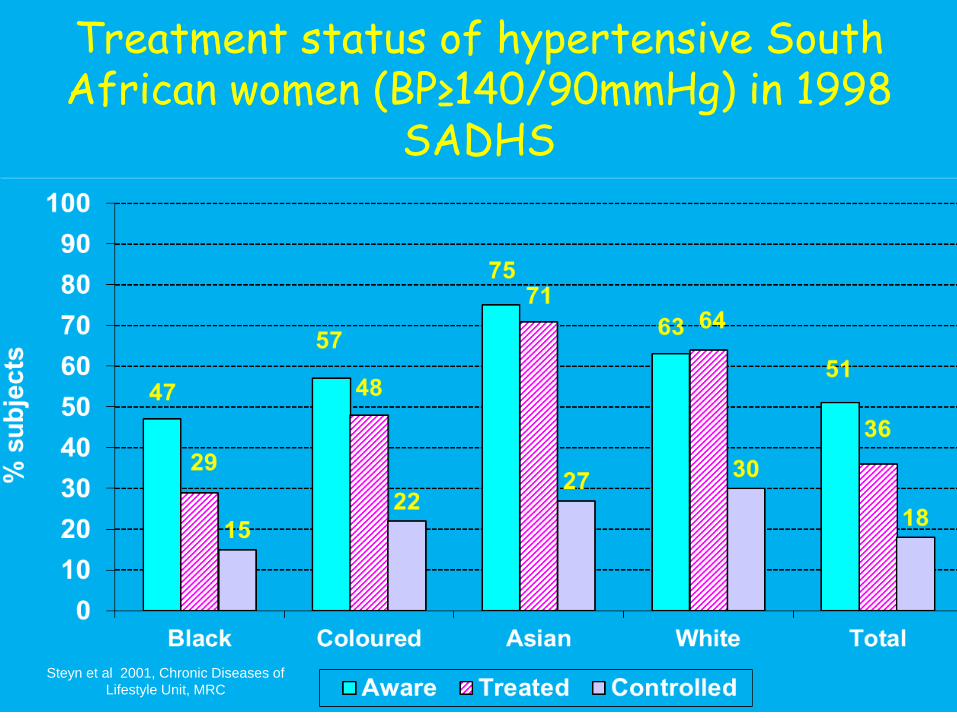
Treatment status of hypertensive South African women (BP≥140/90mmHg) in 1998
SADHS
Steyn et al 2001, Chronic Diseases of
Lifestyle Unit, MRC

Deaths attributable to high blood pressure in males, South Africa 2000
0
1000
2000
3000
4000
5000
6000
7000
30 - 44 45 - 49 60 - 69 70 - 79 80+
Stroke Hypertensive disease Ischaemic heart disease other cardiovascular
Norman et al. 2007 BOD at the MRC

CLINICAL PATHWAY
Evaluation of patient
Appropriate Treatment
BP at goal 65%
BP not at goal
Office hpt
Inadequate treatment
Non-adherence
TRUE RESISTANCE ?
Patient, Funder
or MD failure
Lifestyle
Interfering drugs
Secondary causes Inappropriate
formularies
No fixed drug combinations
Side effects or contraindications to drugs

EXPERIENCE/MADNESS
• Experience is doing the same things over
and over again with increasing confidence
• Madness is doing the same things over and
over again anticipating a different outcome
• Everything should be made as simple as
possible, but not simpler. Einstein
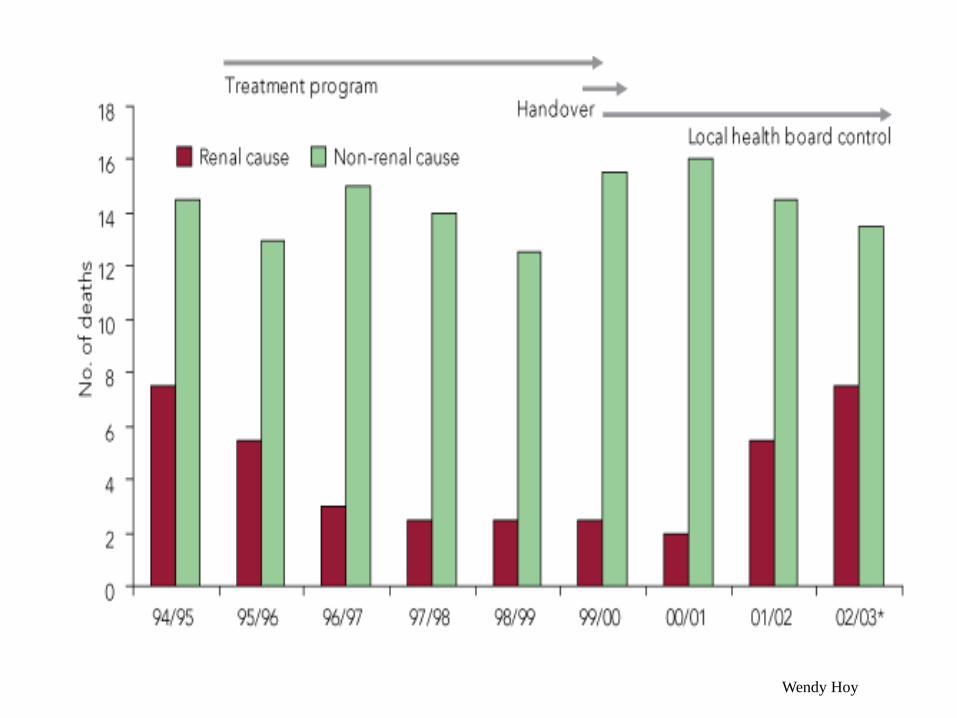
Wendy Hoy

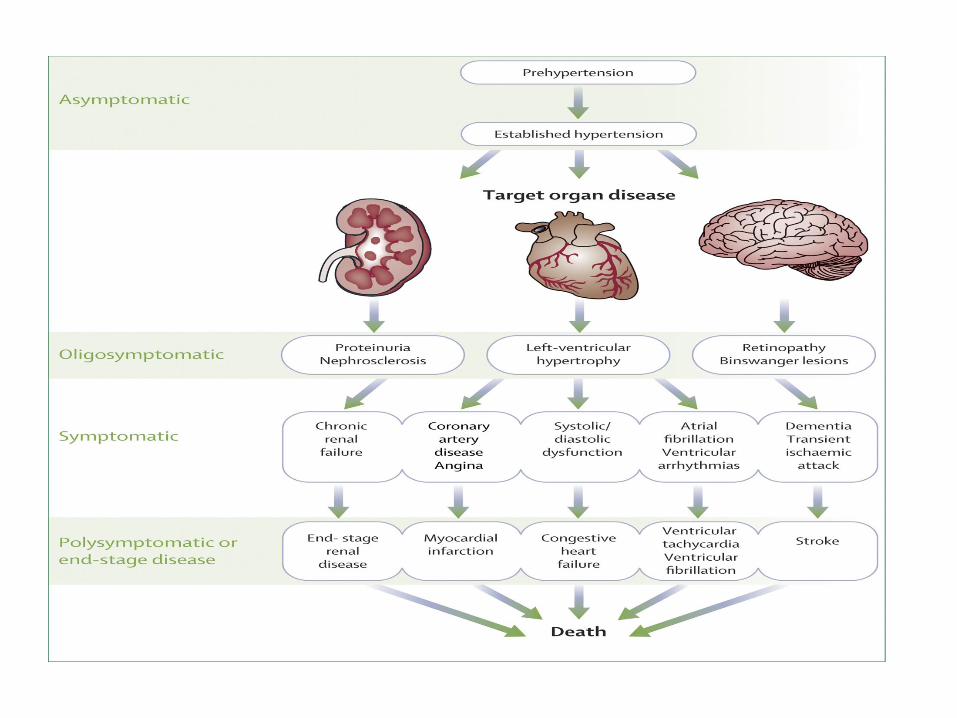
NEW DEFINITION AND
CLASSIFICATION OF HYPERTENSION
• “Hypertension is a progressive cardiovascular syndrome arising from complex and interrelated aetiologies. Early markers of the syndrome are often present before blood pressure elevation is observed; therefore, hypertension cannot be classified solely by discrete blood pressure thresholds. Progression is strongly associated with functional and structural cardiac and vascular abnormalities that damage the heart, kidneys, brain, vasculature, and other organs, and lead to premature morbidity and death”
Giles et al, Hypertension Writing Group, J Clin Hypertens, 2005

DEFINITION OF HYPERTENSION
• Abolish term hypertension, treat overall
CVS risk (Jackson 2005)
• There is no division between normal and
high BP (Pickering, 1972)
• Operational definition – the level (of BP) at
which benefits of action exceed inaction
(Rose 1980)
Kaplan’s Clinical Hypertension 2006

DEFINITION OF
HYPERTENSION (>18 years)
Blood pressure, mm Hg
Category Systolic Diastolic
Optimal <120 and <80
Normal <130 and <85
High-normal 130 - 139 or 85 - 89
Hypertension
Stage 1 140 - 159 or 90 - 99
Stage 2 160 - 179 or 100 - 109
Stage 3 180 or 110

DEFINITIONS OF BLOOD PRESSURE
• Conventional office based measurements
(incorrect measurement, bias, faulty equipment,
variability around mean)
• White coating
• Masking
• Self or home
• 24 Hour ABPM - non-dipping, reverse dipping,
variability or extreme dipping
• Central aortic BP


Arterial Pulse WaveformWhat is it?

Arterial Pulse WaveformWhat is it?

Superiority of ambulatory (nocturnal) BP
for predicting cardiovascular death
Conventional
office BP
Daytime BP
24-hour BP
Nocturnal BP
Systolic BP (mm Hg)
Adju
sted
5-Y
ear
Ris
k o
f
CV
Dea
th (
%)
3.5
3.0
2.5
2.0
1.5
1.0
0.5
90 110 130 150 170 190 210 230
N=5292
Dolan E, et al. Hypertension. 2005;46:156-161.

Mx of Diabetes
Patient 1 2 3
0 month 10.5 27 8.5
1 month 6.8 28 3.1
3 months 12.8 12.5
6 months 7.5 6.8
12 months 15.5 14.5
1. Fasting, pre or post prandial
2. HBA1C
3. 8 or 4 point profiles

WHITE COAT OR OFFICE HYPERTENSION

24-h blood pressure profile in two patientswith hypertension (dipper and non-dipper)
Blood pressure (mm Hg)
7:00 11:00 15:00 19:00 23:00 3:00 7:00
Sleep
Dipper
Non-dipper
Time of day
175
135
115
95
75
55
155
Redman et al, 1976; Mancia et al, 1983; Kobrin et al, 1984; Baumgart et al, 1989; Imai et al, 1990; Portaluppi et al, 1991
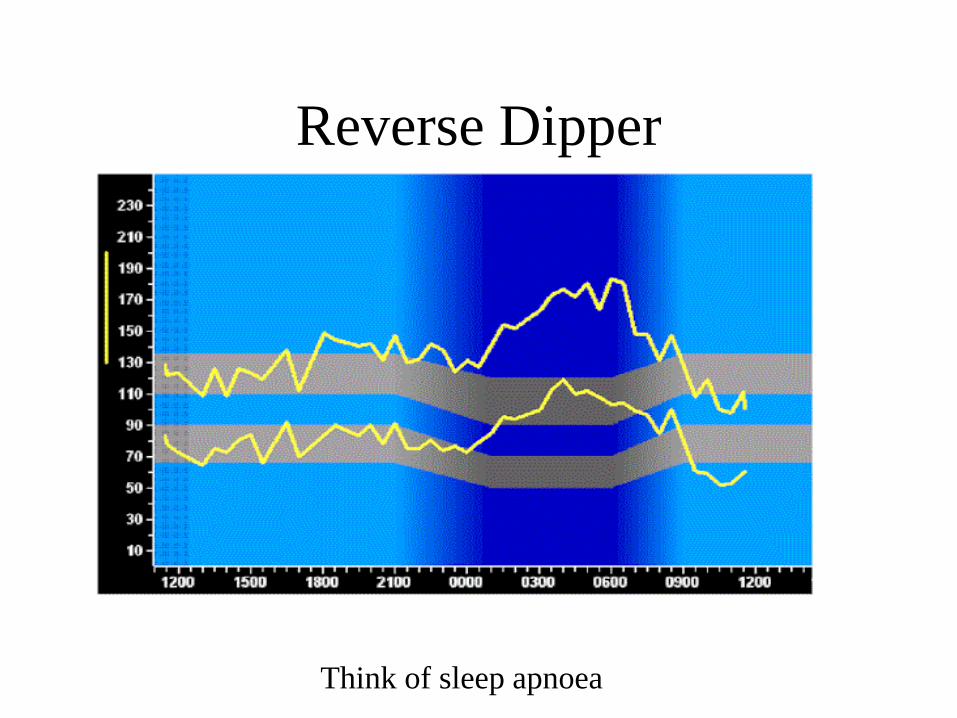
Reverse Dipper
Think of sleep apnoea

Extreme Dipper

Copyright ©2001 American Heart Association
Kario, K. et al. Hypertension 2001;38:852-857
Prevalence of SCIs: shaded area indicates 1 SCI detected by brain MRI per person; solid area, multiple SCIs (defined as >=2 SCIs per person)

Odds ratios (95% confidence intervals [CI]) for cognitive decline associated with the
combination of home systolic blood pressure (BP) value and the SD of the home systolic BP,
after adjusting for sex, age, history of cardiovascular disease, low level of education, baseline
Mini-Mental State Examination (MMSE) score <27, and follow-up duration.
Matsumoto A et al. Hypertension. 2014;63:1333-1338
Copyright © American Heart Association, Inc. All rights reserved.

Mechanistic relationship between increased blood pressure variability and cognitive decline.
Palatini P Hypertension. 2014;63:1163-1165
Copyright © American Heart Association, Inc. All rights reserved.

STROKE
Classical stroke – lenticulostriate artery involving
internal capsule (ischaemic (lacunar)/haemorrhagic)
SCI, cerebral WML, atrophy

MRI of a Practicing Dentist
Presenting with a Facial Palsy
• MRI – bilateral lacunar infarcts in internal
capsule, diffuse cerebral and cerebellar
atrophy due to microvascular changes
• REMEMBER A THIN HYPERTENSIVE
IS A DANGEROUS HYPERTENSIVE

Alzheimer’s and Risk
• ApoEe4 polymorphism
• Hypercholesterolaemia
• Hypertension
• Hyperhomocystinaemia
• Diabetes
• Metabolic S
• Smoking
• Inflammation
• Fat intake and obesity
Casserly I, et al, Lancet 2004

WHITE COAT AND MASKED
HYPERTENSION
White coat or office Masked
↑ BP in office Normal BP in office
Normal BP at home ↑ BP at home
?Regression to mean ?progression to mean
? Pre-hypertensive state ?BP bias, method of
measurement

Incidence of cardiovascular events according to the cross-classification of subjects by
conventional and daytime ambulatory blood pressure in normotensives and in persons with
solated systolic hypertension (ISH) presenting with white-coat hypertension, mask...
Franklin S S et al. Hypertension 2012;59:564-571
Copyright © American Heart Association

RECOGNITION OF MASKING
• Normal office BP but patient has significant
TOD or TOD that is not resolving
• Higher out of office BP readings
• Treatment must be based on self, automated
or ambulatory BP monitoring

Office Self Ambulatory
Predicts outcome + ++ +++
Initial diagnosis Yes Yes Yes
Cut-off BP
(mmHg)
140/90 135/85 Mean day135/85
Mean night 120/70
Evaluation of
treatment
+ ++ +++
Assess diurnal
variation
No No Yes
Limitations No of
readings
Patient bias Expense, inconvenience

Office Automated
office
Self Ambulatory
Predicts
outcome
+ ++ ++ +++
Initial
diagnosis
Yes Yes Yes Yes
Cut-off BP
(mmHg)
140/90 Mean 135/85 135/85 Mean day135/85
Mean night
120/70
Evaluation of
treatment
+ ++ ++ +++
Assess diurnal
variation
No No No Yes
Limitation No of
readings
Does not
completely
eliminate WC
Bias Expense,
inconvenience

Figure 1
FIGURE 1. Proposal for incorporating
automated office blood pressure (mmHg)
into an algorithm for diagnosis of
hypertension using automated
sphygmomanometers.
Copyright © 2012 Journal of Hypertension. Published by Lippincott Williams & Wilkins. 34
The great myth of office blood pressure
measurement
Myers, Martin G.
Journal of Hypertension. 30(10):1894-1898,
October 2012.
doi: 10.1097/HJH.0b013e3283577b05

Systolic Pressures (mean + 95% CI)
Average after 1st year: 133.5 Standard vs. 119.3 Intensive, Delta = 14.2
Mean # Meds
Intensive: 3.2 3.4 3.5 3.4
Standard: 1.9 2.1 2.2 2.3

Figure 4. Incidence of primary outcome (bar graphs) and HR (line graphs; adjusted for
baseline conditions, without propensity score analysis) as a function of SBP and DBP in
patients with and without previous revascularization.
Denardo S J et al. Hypertension 2009;53:624-630
Copyright © American Heart Association


HYPERTENSIVE SMALL VESSEL
DISEASE (kidney, brain, eye)
Sites of auto-regulation
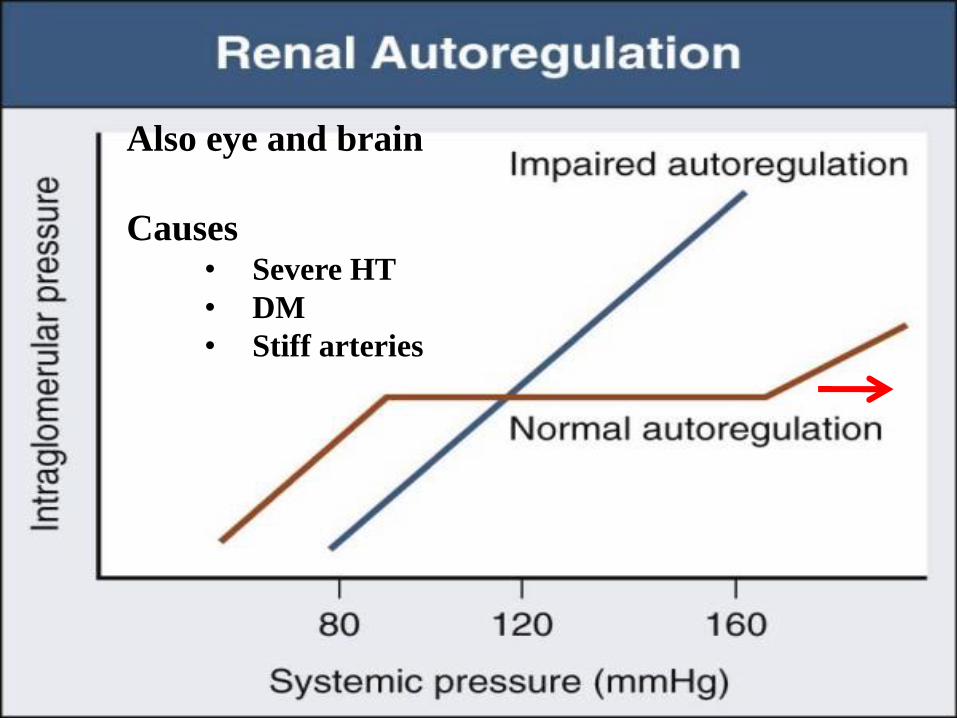
Also eye and brain
Causes • Severe HT
• DM
• Stiff arteries

HYPERTENSIVE EMERGENCY
• Elevation of BP associated with acute and on going organ
damage to kidneys, brain, heart, eyes or vascular system.
•Requires rapid (within minutes to a few hours) lowering of
BP to safe levels.
•Treatment: Hospitalisation in an intensive care unit.
Intravenous antihypertensive therapy – labetalol,
nitroglycerin, nitroprusside
•25% lowering immediately, avoid excessive drops, target
160/100 in first 24 hours, no SL adalat
•Avoid ACEi initially especially if Na < 130
SA Hpt Guidelines, SAMJ 2006

BP > 120-130 diastolic
Renal failure
Dipsticks – protein and blood,
Improves with treatment


LOSS OF AUTOREGULATION
• Endothelial injury
• Increased vascular permeability
• Cell proliferation
• Activation of platelets and coagulation
• Vascular damage, volume depletion and tissue ischaemia
• Activation of RAAS – low K+ often hallmark of malignant hypertension
• Vicious cycle

STROKE
Classical stroke – lenticulostriate artery involving
internal capsule (ischaemic (lacunar)/haemorrhagic)
SCI, cerebral WML, atrophy

HYPERTENSIVE NEPHROSCLEROSIS
Raised creatinine, normal/small echogenic kidneys on U/S,
dipsticks – trace to 1+ protein
Remember NSAIDs

LEFT VENTRICULAR HYPERTROPHY
S4
Pressure overloaded
apex beat
ECG
Echo

>35 – Sokolow-Lyon)
Cornell – (S in V3 + R in aVL + 6 in females) x QRS duration > 2440
Harbinger of death
R in AvL > 11

ECG criteria for LVH
– Sokolow-Lyons >35mm (V1 = V5 or V6)
– R in aVL > 11 mm
– Cornel > 2440 (mm.ms) (S in V3 + R in AvL + 6 in
females) x QRS duration
– LA enlargement = diastolic dysfunction
ESC 2013

MYOCARDIAL INFARCTION

AORTIC ANEURYSM

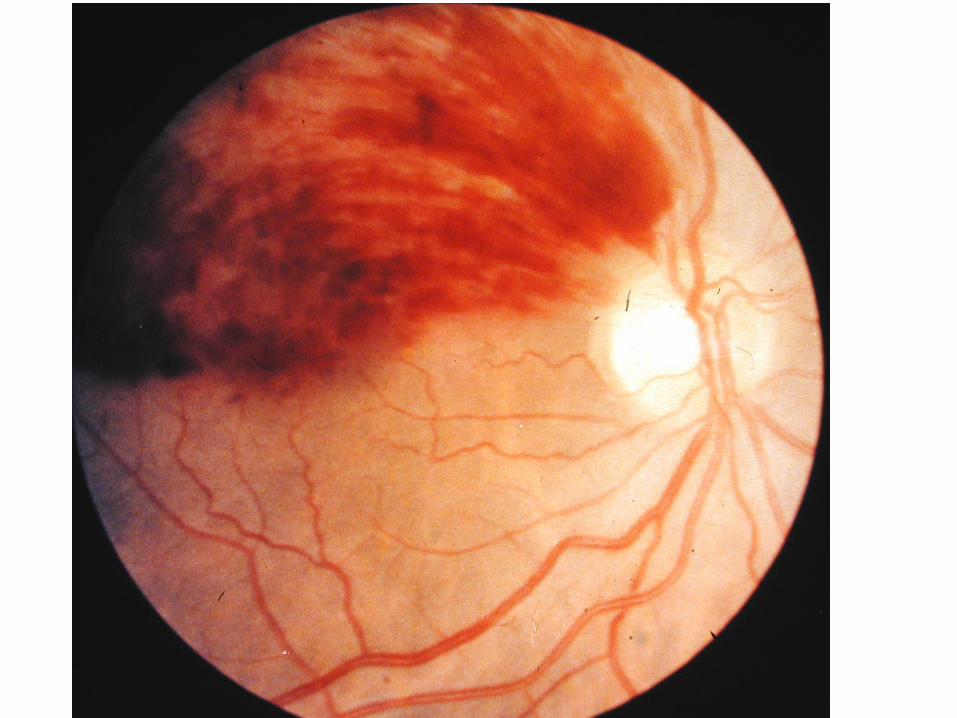
1. Silver wiring
2. Av nipping
3. Hx and exudates
4. Papilloedema


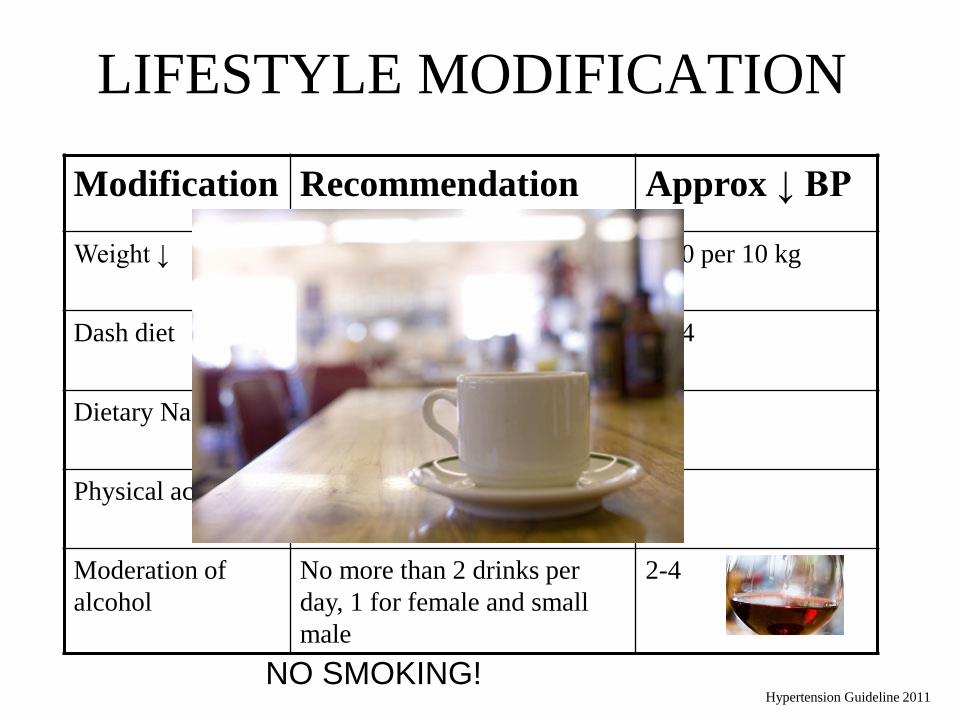
LIFESTYLE MODIFICATION
Modification Recommendation Approx ↓ BP
Weight ↓ BMI 18.5 – 24.9 5-20 per 10 kg
Dash diet ↓ saturated fat and total fat, ↑
fruit and vegetables
8-14
Dietary Na+ <100 mmols or 6 gm
NaCl/day
2-8
Physical activity Brisk walking for 30 minutes
per day most days
4-9
Moderation of
alcohol
No more than 2 drinks per
day, 1 for female and small
male
2-4
Hypertension Guideline 2011
NO SMOKING!

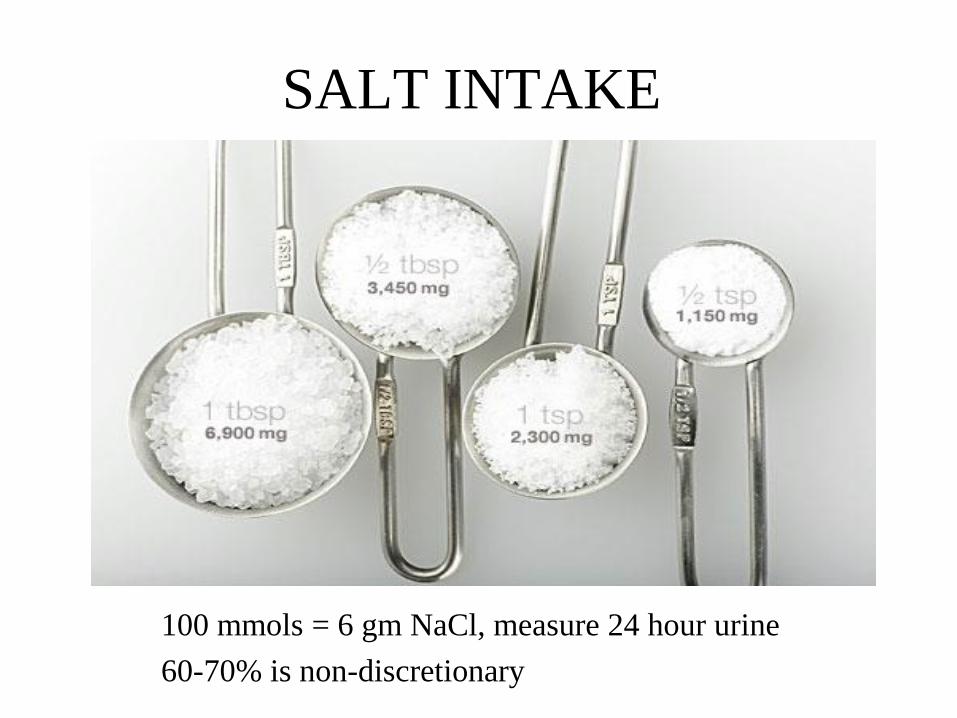
SALT INTAKE
100 mmols = 6 gm NaCl, measure 24 hour urine
60-70% is non-discretionary

CONCLUSIONS
• Hypertension is a complex disorder
requiring a rigorous approach to treatment
• Out of office BP measurement is changing
the landscape of treatment
• Hypertension is also a small vessel disease
and auto-regulation is critically important
• Large vessel stiffening is very important in
the elderly and complicates treatment