the american journal of cancer - cancer...
TRANSCRIPT

THE AMERICAN JOURNAL OF CANCER
A Continuation of The Journal of Cancer Research
VOLUME XXIX MARCH, 1937 NUMBER 3
SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA
ARTHUR PURDY STOUT, M.D.
(From the Surgical Pathology Laboratory of the College of Physicians and Surgeons, Columbia University, and the Department of Surgery, the Presbyterian Hospital, Nrw York C i t y )
INTRODUCTION
During the past three years a very general interest has arisen, especially in the United States, in tumors of the neuromyo-arterial glomus, which are small growths characterized clinically by severe pain, often of a paroxysmal nature. I t has been very generally agreed that these must be one form of the painful subcutaneous tubercle first so designated by William Wood of Edinburgh in 18 12, although previously described by Cheselden, Valsalva, Morgagni, Bisset, Pearson and others in the eighteenth century. But this is not the only lesion which may be called painful subcutaneous tubercle or tuberculum dolorosum as the continental writers named it. In 1854 Virchow first reported that a group of small tumors composed chiefly of smooth muscle and involving the skin of the thoracic wall in the neighborhood of the areola of a thirty-two-year-old man caused exactly the same type of paroxysmal pain as did tubercula dolorosa. Although Verneuil described a case of multiple cutaneous leiomyomas in a cadaver in 1858, and Duhring in 1873 and Kosinski in 1874, cases of undoubted multiple leiomyomas which they mistook for neuromas, the disease did not become well known until 1880, when Besnier published his comprehensive paper. After that, case reports multiplied so that now there are at least 132 cases of multiple dermatomyomas in the lit- erature and the disease is well known in all parts of the world.
During the years after Virchow’s paper, case reports of solitary superficial leiomyomas began to make their appearance. The earlier cases were all pain- less tumors-Forster’s, 1858, in the scrotum; Aufrecht’s, 1868, in a subcu- taneous vein in the side of the foot; Klebs’, 1869, in the neck, Challand’s 1871, in the labium majus and in the scrotum; Sokolow’s, 1873, in the nipple. The first reported case of leiomyomatous tuberculum dolorosum occurred in the subcutaneous tissues of the poet Stranberg’s finger and was described in
435

436 ARTHUR PURDY STOUT
1873 by Axel Key. In the year 1884 Malherbe was able to publish descrip- tions of five solitary painful leiomyomas which had come to his attention dur- ing the preceding nine years. Since these were the only cases of tuberculum dolorosum that he had ever seen, he supposed that the leiomyoma was its only form.
Sufficient information had now accumulated about multiple and solitary cutaneous and subcutaneous leiomyomas to enable Babes to make an excellent summary of the whole subject, which appeared in 1884 in v. Ziemssen’s Hand- buch. Babes was aware that multiple leiomyomas came from either the ar- rectores pilorum muscles, the muscles of the vessel walls, or the muscular ap- paratus which is found in the depths of the skin, especially in the genital sphere (scrotum, labia majora, penis, nipple and areola), in the face, the anal region, the umbilicus and the auricle. He recognized the following classes: ( 1) myomas springing from vessel walls (angiomyoma cutis) ; ( 2 ) hyper- plasias of the arrectores pilorum ( a ) as portions of vascular nevi (Virchow) and ( b ) forming multiple tumors; ( 3 ) neoplasms derived from the deep mus- cular layer of the skin (mybme dartique, Besnier), ( a ) diffuse, as forms of elephantiasis lymphangiectodes and pachydermia myxomatodes, and ( b ) cir- cumscribed; (4) myomas reaching the skin secondarily or originating in mis- placed germs. This admirable summary includes almost all of the types known to us today.
Altogether at least 85 cases of solitary cutaneous and subcutaneous leio- myoma have been recorded to date. I t seems beyond question that many of these neoplasms form an important group of the tubercula dolorosa, although not all leiomyomas of the skin and subcutaneous tissues are painful.
I t may appear superfluous to add to the rather formidable literature al- ready in existence on this subject, but there are several reasons which seem to justify another paper. In the first place, the existence of the solitary superficial leiomyomas cannot be very well known to the English-speaking public, since only three proved cases have been published in that language- two by Americans (Herzog and Ragins) and one by a South African (Wasse- naar). Pearson’s case, published in 1795, is almost certainly a leiomyoma but, of course, lacks histological proof. I t seems worthy of note, also, that no paper on this subject has ever appeared in an English language surgical journal, and exceedingly few in surgical journals in any language, although the tumor usually has been removed by a surgeon. Furthermore, no compre- hensive study of all of the solitary cases recorded has been prepared, although excellent summaries have been made by Saalfeld and Saalfeld, Dietel, and Woringer. The writer has had the opportunity of studying 15 cases, which is three times as many as any one observer has ever reported before. Four- teen of these were seen during the past nine years in the surgical department of the Presbyterian Hospital. During this same period one solitary and three multiple cases, all proved by biopsy, were seen in the dermatological depart- ment. This seems to indicate that the solitary lesion must frequently have been overlooked, and that it is not as uncommon as it is reputed to he.’
1 When Ormsby published his excellent study of leiomyoma cutis in 1925, he included in his summary of 47 patients only 4 solitary cases. This no doubt has served to spread the belief, espe- cially among dermatologists, that the solitary form is much rarer than the multiple form.

SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 43 7
The cutaneous and subcutaneous leiomyoma is a small tumor varying usually from the size of a pea to that of a walnut and only occasionally grow- ing larger, the maximum being the size of a child’s head. The tumor occurs with equal frequency in both sexes and may appear at any age, although more than half have developed after the twenty-ninth year. It is rounded and occasionally pedunculated. Unless fixed in the skin, it is freely movable. The overlying skin is colorless or has a reddish or bluish tint. The tumors are found especially on the extensor surfaces of the extremities, more par- ticularly the lower, and in the scrotum, labia majora, nipple, areola, and cheeks. Less frequently they occur in other parts of the body. They are of slow growth and long duration. Usually they are painless at first but sooner or later many of them become painful and tender, the pain being of paroxysmal character and made worse by pressure, cold, and sometimes other factors. Once the pain starts, it generally grows worse as time progresses. I t seems to be associated with contractions of the smooth muscle forming the tumor. There is good reason for believing that this smooth muscle is derived from one or another of the smooth muscle structures of the skin and subcutaneous tissues.
Histologically the leiomyomas can be divided into two groups: the non- vascular and the angiomatous. The vast majority are benign and are cured by excision. Seven malignant leiomyomas involving skin or subcutaneous tissues have been recorded.
ETIOLOGICAL FACTORS
Sex: I t is generally stated that cutaneous leiomyomas are twice as common among males as among females (Saalfeld). This is true of multiple dermato- myomas, for of 106 cases in which the sex is known, 7 1 were in males and 35 in females. It is not true, however, of the solitary cutaneous and subcu- taneous tumors, for of 88 cases, 43 were in males and 45 in females. The same relative figures are reached if the cutaneous and subcutaneous tumors are separately considered: cutaneous, 2 7 males and 26 females; subcutaneous tissues, 16 males and 19 females.
Con- genital cases are reported by Brugger, Lieber, Marc, Selmi and Wolters, and Soupault and Pommay describe a case which made its first appearance at the age of seventy-five years. The majority of cases, however, appear later in life than do the multiple dermatomyomas. Of 87 cases of multiple tumors in which the age of onset is known, 68, or 78 per cent, appeared before the age of thirty. On the other hand, of 66 cases of solitary leiomyoma, with known age of onset, only 31, or 47 per cent, appeared before the thirtieth year.
Race: With so few cases on record it is dangerous to make any definite statements about racial distribution. I t is to be noted, however, that cases have been reported from almost all of the European countries, from North and South America including one case in an American negress (Case 8), among the Japanese and Chinese (Case 4 ) , and in a South African native (Wassenaar), which suggests that the disease is probably not confined to any racial group.
A g e : Solitary leiomyomas may make their appearance at any age.

43 8 ARTHUR PURDY STOUT
A natomical Situation: Reference to the’ diagram will reveal the anatomical distribution of 95 solitary leiomyomas, including the 15 cases reported in this paper. This shows clearly that there are certain areas in the body where the tumors more commonly appear. Forty-eight or more than half of them have developed on the extensor surfaces of the extremities, especially the lower extremity (37 cases). Seventeen have developed in the genital zones, as follows: nipple and areola 7 , scrotum 5 , penis 1, labium majus 4. Ten have
DIAGRAM I. DISTRIBUTION OF 95 SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMAS
The labium majus cases are shown on the scrotum. INCLUDING REPORTED CASES AND THOSE IN THE AUTHOR’S SERIES
The favored sites are the extensor sur- faces of the extremities 48 (leg 37; arm 11), the scrotum and labium majus 10, the nipple and areola 7, and the cheeks 7.
appeared on the flexor surfaces of the extremities (lower 2, and upper 8) and 7 on the cheeks, The location of the other tumors was as follows: anterior thorax 7 , back 4, eyelid 1, occipital region 1.
In 99 cases the situation of the tumor in regard to the skin is known. Fifty-six, including 4 in the present series, developed in the skin; 43, includ- ing 11 of the present series, were subcutaneous.
Source of the Smooth Muscle in the Tumor: I t occurred to the earliest observers to look for the source of the smooth muscle forming these tumors in the smooth muscle of the skin and subcutaneous tissues. The arrectores pilorum, the sweat gland muscles, and the muscles of blood vessels are found

SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 439
practically everywhere in the skin and the blood vessels in the subcutaneous tissues. In addition there are (1) the muscularis sexualis, bands of smooth muscle bundles paralleling the skin surface in the corium or superficial subcu- taneous tissue of the scrotum, penis, and labium majus; ( 2 ) the muscularis mammillae et areolae in the nipple and areola; ( 3 ) similar muscles in the axilla and anal regions; (4 ) musculi cutis diagonales, irregular findings in the corium of the extensor aspects of the extremities, cheeks,scalp,
FIG. 1. CASE I: SUBCUTANEOUS LEIOMYOMA OF THE DORSAL SURFACE OF THE
FINGER
and forehead
RIGHT MIDDLE
(Hoepke) (Fig. 14). An analysis of the tumors shows that many of them come from one or another of these various sources.
Three cases in the scrotum have been described by Forster and one each by PhCliesse and Challand. Two of the tumors were pedunculated. In addi- tion, Babes noted a marked hyperplasia of the dartos muscle in a child with pachydermia of the scrotum, and Rindfleisch a similar hyperplasia in lymphan- giectatic elephantiasis involving the scrotum. Cases have been reported in the labia majora by Challand, Kramer, Marcano, and Valude. In Marcano’s case the tumor may not have arisen from the muscularis sexualis but rather from the muscle of the rectovaginal septum. Nicolau examined the penis tumor.
The nipple tumors reported by Bauer, Hiebaum, and Kaufmann and the areola tumors described by Driak and Sternberg, Niklas, Sokolow, and the writer (Case 2 ) were all undoubtedly derived from the muscularis sexualis of these parts (Fig. 5 ) . Niklas’s case was pedunculated.2
Of the cases in the cheek, that described by Sehrt was subcutaneous and had a different origin. Herzog’s case probably came from the arrectores mus- cles, but the other 5 (Diss and Lkvy; Hayn and Zieler; Grzybowski; Milian and PCrin and Milian, PCrin and Delarue; and the writer’s Case 13) may very well have been derived from the musculi cutis diagonales of this region.
Klebs suggested that the leiomyoma of the neck which he studied might have developed in connection with a branchial cleft. I t formed a 3.5 cm.
2 I t is of interest that pure leiomyomas also occur in the mammary gland (Klob, 2 cases, Melnick, Mitterstiller, Ribhert, Schauder, Strong, and Driak and Sternberg) but these do not properly belong to the skin or subcutaneous tissues.

440 ARTHUR PURDY STOUT
projection from the neck and was covered with hair. Wassenaar’s tumor of the upper eyelid in a colored native of Pretoria, South Africa, was made up of smooth muscle which may have been derived from Muller’s musc. tarsalis sup. or Riolan’s musc. tarsalis (or ciliaris) .
The number of solitary tumors of the skin which have been ascribed an origin from the arrectores pilorum muscles is relatively small in comparison with the cases of multiple tumors, almost all of which seem to come from these muscles. Audry ( 1898), Diss (Case 1) , Duboucher and Montpellier, Herzog, Levit, Luquet, Simonelli and Wolters are the only reporters of solitary tumors who suggest such an origin.
FIG. 2. CASE 1: PHOTOMICROGRAPII OF T H E W H O L E TUMOR, S H O W I N G ITS MANY THICK-WALLED VESSELS, ITS CAPSULE, AND THE LONGITUDINALLY DISPOSED
VESSELS IMMEDIATELY BENEATH THE CAPSULE
Most of the rest of the skin and subcutaneous tumors have a definite association with the smooth muscle of vessels and are very probably derived from this source. This is true of 30 cases from the literature and 11 cases in the author‘s series. The question of just what kind of vessels is of some interest.
Whether or not the muscle of arteries ever furnishes the source of these tumors is open to question. There are no leiomyomas of recognized arteries on record. Audry believed that his tumor was composed of and derived from arterioles; Babes considered that his tumor came from an abnormal vascular rudiment of mainly arterial nature and Migliorini (1905) thought that the vessels from which his tumor was derived were arteries.
Some of the leiomyomas have developed in the walls of recognized veins. These include the tumors of the saphenous vein in the leg reported by Auf- recht, Ecoffey, and Pearson; Cornil’s case in an unspecified arm vein;

FIG. 3 .
bulk of the tumor.
CASE I: PHOTOMICROGRAPH SHOWING THE MANY SMALL VESSELS The muscle in the walls of some of these is indistinguishable from the muscle forming the
FIG. 4. CASE I : PHOTOMICROGRAPH OF ONE OF THE VESSELS AT THE PERIPHERY OF THE TUMOR, SHOWING A TUMOR-LIKE TIXICKENINC OF THE SMOOTH MUSCLE IN ITS WALL
44 1

442 ARTHUR PURDY STOUT
Niederle’s case in the median basilic vein; and the cases of Neuniann and Schnyder in veins in the foot. Leiomyomas have also been found in the ulnar vein by Boettcher, in the veins of the spermatic plexus by Cernezzi, in the axillary vein by Marri, and in the femoral vein by Natali. Ragins thought that the tumor in the skin of the palm of the left hand which he studied was derived from the muscular coat of veins. The majority of writers whose tumors seemed to them to be of vascular origin did not say whether the vessels were veins or arteries (Diss, Hayn and Zieler, Huppert, Lieber, Marc, Mermet, Moberg, Photinos, Sawada, and del Vivo).
Analysis of this evidence seems to show that leiomyomas can develop in the walls of larger veins but not of arteries. As to the smaller vessels which may be involved, some authors think they are more like arteries, Ragins that they are more like veins, and a larger number are not prepared to say what they are, although all agree that they have muscular walls. A study of our material makes plain the reason for this confusion. The tumor vessels are neither normal veins nor normal arteries. They have thick muscular walls with varying amounts of subintimal and adventitial fibrous thickening. The subintimal thickening may proceed to complete obliteration of the lumen. There is almost no elastic tissue and certainly no elastic lamina. The muscle bundles of the vessel merge with the tumor muscle (Figs. 3 , 10, and 15) so frequently that one cannot avoid the belief that the latter is derived from the former. Although the tumor vessels are never normal, they resemble veins much more than arteries. This is particularly striking at the periphery of some tumors, where vessels which are certainly veins (Fig. 4) are seen enter- ing the tumor. The weight of evidence, therefore, seems to favor an origin from the muscular tissue of typical large or atypical small veins, but not from arteries.
CLINICAL CHARACTERISTICS
Size: The great majority of these leiomyomas are small tumors, varying from 2 to 15 mm. in diameter. Occasionally they grow larger. The tumor in Case 10 measured 9 X 6 X 5 cm., while the dimensions of Blanc and Win- berg’s tumor were 7 X 5 X 3 cm. Devic and Gallavardin’s first patient had a tumor the size of a fetal head and Mermet’s the size of two fists. Other tumors larger than the average are reported by Cornil, Kramer, Huese, Marc, Marcano, Neumann, Santesson, Sokolow, Valude, and Wassenaar.
Shape, Consistency and Color: The tumor is usually rounded, forming a nodule which generally elevates the skin but may be almost imperceptible if it is very small. Pedunculated tumors have been described by Challand on the labium majus and on the scrotum; by Chambard and Gouilloud on the back, Forster on the scrotum, Mermet on the thigh, Niklas on the nipple, and Wassenaar on the upper eyelid. Case 13 on the right naso-labial fold (Fig. 11) is an example in the present group. All of our tumors were quite firm and most of the reported cases are described as firm or hard. In one of Challand’s cases the tumor felt like an empty scrotum; Key’s tumor was called soft and so were those of Huppert, Simonelli, and Zieler.
In contradistinction to the cases of multiple leiomyoma cutis, the majority

SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 443
of the solitary lesions show no discoloration of the skin. This is almost al- ways the case with the subcutaneous tumors. Those that involve the more superficial layers of the skin have been described as brownish (Asai, Du- boucher and Montpellier ) , .brownish-red (Zieler ) , reddish (Brugger, Pearson, Ragins, Case 13), faintly blue (Moberg), and the color of apple jelly (Audry 1898). The skin over one subcutaneous tumor (Audry 1931) is described as
FIG. 5 . CASE 11: PHOTOMICROGRAPH OF THE TUMOR IN THE AREOLA The growth is composed almost exclusively of smooth muscle with a supportive framework
Beneath the tumor are the greatly hypertrophied bundles of fibrous tissue and very few vessels. of the areola smooth muscle, some of which are directly continuous with the tumor muscle.
slightly bluish. Without doubt the color depends upon the distance of the tumor from the epidermis, the degree of redness of the smooth muscle forming it, and its blood content. The brownish tinge noted by some authors seems to be due to melanotic pigmentation of the epidermis.
The subcutaneous tumors are usually freely movable because they are always encapsulated (Figs. 2 and 6) unless the growth has become malignant

444 ARTHUR P U R D Y STOUT
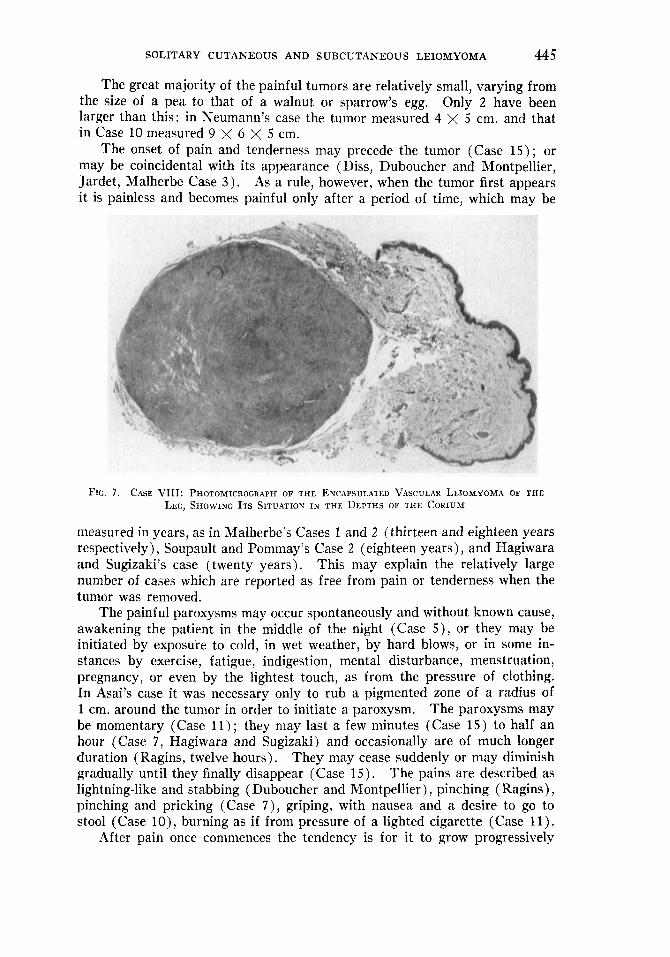
and invasive. The tumors involving the superficial layers of the skin are not encapsulated (Figs. 5 and 12) but those deep in the corium are encapsulated (Fig. 7 ) just as are the subcutaneous tumors.
Pain and Tenderness: The most arresting clini.ca1 feature of these tumors, whether cutaneous or subcutaneous, vascular or non-vascular, is non-radiating pain. Pain or tenderness (or both) was present in 12 of our 15 cases. In one both were absent (Case 13, the pedunculated tumor of the naso-labial fold), and in 2 (Cases 2 and 12) no statement on these features occurs, from
FIG. 6 . CASE Iv: PHOTOMICROGRAPH OF A SECTOR OF THE TuhroR OF TIiE LEG, SHOWING ITS CENTRAL LUMEN AND WALL FORMED ALMOST EXCLUSIVELY OF SMOOTH MUSCLE
which we may infer that they were either absent or inconspicuous. Spon- taneous or induced paroxysmal pain of a more or less marked degree was recorded in 6 cases (Cases 5 , 6, 7, 10, 11, 15); in 3 others there was non- paroxysmal spontaneous pain (Cases 4, 8, 9) and in 3 more there was tender- ness to pressure but no spontaneous pain (Cases 1, 3, 14). Of the cases reported in the literature, 2 7 were characterized by pain or tenderness (18 of a paroxysmal type), in 19 neither pain nor tenderness was present, and in the remaining 39 information is lacking on this point.
SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 445
The great majority of the painful tumors are relatively small, varying from the size of a pea to that of a walnut or sparrow’s egg. Only 2 have been larger than this: in Neumann’s case the tumor measured 4 X 5 cm. and that in Case 10 measured 9 X 6 X 5 cm.
The onset of pain and tenderness may precede the tumor (Case 15) ; or may be coincidental with its appearance (Diss, Duboucher and Montpellier, Jardet, Malherbe Case 3 ) . As a rule, however, when the tumor first appears it is painless and becomes painful only after a period of time, which may be
FIG. 7. CASE VIII: PHOTOMICROGRAPH OF THE EXCAPSULATED VASCULAR LEIOMYOMA OF THE LEG, SHOWING ITS SITUATION IN THE DEPTHS OF THE CORIUM
measured in years, as in Malherbe’s Cases 1 and 2 (thirteen and eighteen years respectively), Soupault and Pommay’s Case 2 (eighteen years), and Hagiwara and Sugizaki’s case (twenty years). This may explain the relatively large number of cases which are reported as free from pain or tenderness when the tumor was removed.
The painful paroxysms may occur spontaneously and without known cause, awakening the patient in the middle of the night (Case 5), or they may be initiated by exposure to cold, in wet weather, by hard blows, or in some in- stances by exercise, fatigue, indigestion, mental disturbance, menstruation, pregnancy, or even by the lightest touch, as from the pressure of clothing. In Asai’s case it was necessary only to rub a pigmented zone of a radius of 1 cm. around the tumor in order to initiate a paroxysm. The paroxysms may be momentary (Case 11) ; they may last a few minutes (Case 15) to half an hour (Case 7 , Hagiwara and Sugizaki) and occasionally are of much longer duration (Ragins, twelve hours). They may cease suddenly or may diminish gradually until they finally disappear (Case 15). The pains are described as lightning-like and stabbing (Duboucher and Montpellier) , pinching (Ragins), pinching and pricking (Case 7 ) , griping, with nausea and a desire to go to stool (Case lo ) , burning as if from pressure of a lighted cigarette (Case 11).
After pain once commences the tendency is for it to grow progressively

446 ARTHUR PURDY STOUT
more intense and for the paroxysms to increase in frequency. Itching with- out any other symptoms is reported by del Vivo. This symptom has been noted also in cases of multiple cutaneous leiomyomas by Goldsmith, Nobl and Wolters.
Observations which have been recorded by some observers lead one to believe that functional activity can occur in these tumors. Challand observed slow, worm-like contractions in a tumor attached to the labium majus even after it had been removed from the body. The large tumor which Kramer removed from a labium majus was observed to undergo slight contractions during the process of removal. The tumor in the left leg which was studied by Hagiwara and Sugizaki seemed to become harder and more elevated if a painful paroxysm was induced by striking the tumor. Ragins reports that the tumor in the left hand, which he described as being the size of a hazelnut, would enlarge and become purplish or bluish when the patient was angry, and an attack of pain would follow. Pearson also noted increased redness and sensible elevation of the tumor during a paroxysm. Similar evidences of functional activity have been recorded in cases of multiple leiomyomata by Duhring, Fiocco, and Nomland. That contraction of the smooth muscle of the tumor is associated with pain was demonstrated by Hagiwara and Sugi- zaki, who found that injection of adrenalin would greatly increase the pain of a paroxysm.
Recog- nized nerve bundles were not seen in the sections of any of our tumors and impregnation with silver according to Rogers’ technic failed to show any neurites in the ten cases in which it was tried. In most instances, however, formalin or Zenker fixation was used, so that we do not regard this negative result as of much significance. Grzybowski, the only writer who has used Cajal’s modified method of silver impregnation, succeeded in demonstrating a great many neurites in his tumor. But whether these were sympathetic nerves or sensory nerves, or what they were, is unknown.
A unique observation is that of Sokolow, who noted that a myoma of the nipple zone twice more than doubled in size during pregnancy, each time decreasing in size following termination of the pregnancy.
Clinical Course: In the great majority of instances the tumors increase somewhat after their appearance, eventually reaching a size somewhere be- tween that of a small pea and a walnut, when growth ceases and no further proliferative activity occurs, although the pain is progressive. Rarely the tumor grows to the maximum size of a child’s head. Spontaneous disappear- ance of a solitary tumor has never been reported but Sannicandro states that some of the multiple angiomatous leiomyomas in a patient whom he studied disappeared spontaneously. Biopsy of one of the remaining nodules showed marked degenerative changes.
Development of Malignant Leiomyomas in the Skin and Subcutaneous Tissue: There are seven undoubted cases of malignant leiomyoma on record. Diss’s second case, in addition to the presence of bizarre cell forms, showed infiltration of the subcutaneous fat. In Devic and Gallavardin’s Cases 1 and 2 and in Luquet’s case the tumor reappeared repeatedly after opera- tion, although there was no suggestion of metastasis. Diss and L6vy’s case,
Jarisch’s patient complained of both pain and itching.
Just what nerves are irritated when pain occurs remains obscure.

FIG. 8. CASE x: PHOTOMICROGRAPII OF THE SUBCUTANEOUS LEIOMYOMA OF THE THIGH, SHOWING
Tumor muscle tissue surrounds these but does not seem to bear any definite relationship t o ITS MANY AREAS OF DEGENERATION AND SOME OF ITS VESSELS
the vascular muscularis.
FIG. 9. CASE x: SOME OF THE TUMOR MUSCLE CELLS WITH THEIR CHARACTERISTICALLY SHAPED
NUCLEI AND MYOFIBRILS (HIGH-POWER)
447

448 ARTHUR PURDY STOUT
which developed in an old lupus lesion in the cheek, caused death by progres- sive infiltration. Two cases with metastases have been reported. Devic and Gallavardin’s third patient had a tumor in the buttock. It was subcutaneous, not adherent, and had been present for several years. Suddenly it began to grow, metastasizing widely, and death ensued. At autopsy metastases were found in the kidneys, liver, lungs, pancreas, and thyroid. Bartkowiak has recently described a tumor in the skin of the dorsum of the foot of a fifty-nine- year-old woman. During a period of about seventeen months it metastasized to the femoral lymph nodes, the liver, and the eleventh dorsal vertebra. Autopsy and careful histological studies make this a convincing case.
A number of cases have been described as malignant solely on the basis of certain suggestive microscopic findings, but this would hardly seem justi- fiable (see p. 45 1 below).
MICROSCOPIC CHARACTERISTICS
There are two principal classes of leiomyomas of the skin and subcutaneous tissues: those that are associated with vessels and those that are not. In the vascular tumors the vessels are usually thick-walled with small, rounded or stellate lumens which occasionally contain blood but more often are empty. The walls are thick and made up of fibrous tissue and smooth muscle which are arranged after no set pattern. Usually there are a subintimal fibrous layer and a more or less complete adventitia. In many sections, however, it can be demonstrated that the adventitia is interrupted and the vascular smooth muscle is continuous with the tumor muscle. The smooth-muscle fibers of the tumor vessels are circularly disposed about the lumen and are associated with variable quantities of collagen fibers (Figs. 10 and 15) . Some- times a vessel is found with smooth muscle paralleling the lumen, and some authors have considered this arrangement as constituting a peculiar type of tumor blood vessel. I t has not been possible for me to believe that this arrangement is other than fortuitous. I t is simply a vessel without muscular walls passing through tumor smooth muscle where the fibers happen to parallel the lumen. These vessels never have an internal elastic lamina such as is found in arteries. Indeed, more often than not there is no elastic tissue in any part of the wall. Only occasionally can one demonstrate a few delicate fibers in the adventitia and still less frequently in the media and subintimal layer. Occasionally some of the tumor vessels at the periphery resemble veins with an unequal distribution of smooth muscle in their walls (Fig. 4).
Not all of the vessels of the vascular forms of leiomyoma have muscular walls; many are of the capillary type with endothelial lining and fibrous walls of varying thickness. When these vessels are widely dilated and do not contain blood, they have been called lymphatics (Key).
These vascular myomas are almost a1way”s found deep in the corium or in the subcutaneous tissues. They are encapsulated, and sections sometimes show the peculiar muscle-walled vessels in the capsule (Figs. 2 , 3 , 4) . In the surrounding tissues one sometimes finds an excess of capillaries or occasionally veins with an unequal distribution of muscle in their walls, but never the bizarre thick-muscled vessels so characteristic of these tumors.

SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 449
The special form of these vascular tumors in which the muscular growth occurs in the media of a vein of sufficient size to gain anatomical and clinical recognition has already been described. I t emphasizes the probable venous origin of most of these lesions.
The bulk of the vascular tumor is composed of smooth muscle and fibrous tissue. These have no definite arrangement but run in bands in various directions, often with an effect of interlacing. Where fibrous tissue is found in large quantities, it seems probable that it represents a fibrous replacement of pre-existing smooth muscle. In such fibrous muscular tumors the bulk of the well preserved smooth muscle is found at the periphery of the tumor. Cal-
FIG. 10. CASE XI: PHOTOMICROGRAPH OF A VASCULAR SUBCUTANEOUS LEIOMYOMA OF THE KNEE REGION, SHOWING THE MANNER IN WHICH VASCULAR MUSCLE AND TUMOR
MUSCLE ARE INDISTINGUISHABLY UNITED
cification of the fibrous areas is rare; it occurred in Malherbe’s second case and in Case 7 of this series.
In the vast majority of instances the smooth muscle of the tumor is quite normal and well differentiated. The elongated, ribbon-like muscle cells with their longitudinally disposed myofibrils have characteristic baton-shaped nuclei with blunted ends (Fig. 9 ) , and each cell is clothed by a delicate reticulin sheath. This fibrous sheath may be much thickened so that the individual muscle cells stand apart. In such areas the cells are apt to be thin and the myofibrils delicate and few. In areas where there is no fibrosis the muscle cells are usually plump and the myofibrils conspicuous.
Unless fixation has been good, it is often difficult to be sure that smooth- muscle cells are present with the hematoxylin and eosin stain. This is par-

450 ARTHUR PURDY STOUT
ticularly true of very vascular or very fibrous tumors. Any good differential fiber stain will suffice to demonstrate myofibrils. We have used phospho- tungstic acid, Masson’s aniline blue, ponceau and acid fuchsin trichrome stain and van Gieson’s stain. Phosphotungstic acid is the best fiber stain, but it can be used only after Zenker fixation.
A second group of leiomyomas is composed principally of smooth-muscle cells, again arranged in interlacing bands with varying amounts of fibrous tissue, but with only a few blood vessels, which obviously are purely nutri- tional and not part of the tumor. This is the common form of the leiomyoma
FIG. 11. CASE XIII: NEVOID PEDUNCULATED LEIOMYOMA OF THE NASO-LABIAL FOLD IN A SIXTY-ONE- YEAR-OLD MAN, WHICH HAD BEEN PRESENT AS LONG AS HE COULD REMEMBER
derived from the skin muscles (Fig. 5 ) . Most of these tumors, although circumscribed, are not encapsulated. Their growth is evidently infiltrative, for hair follicles or skin glands are not infrequently found within the confines of the tumor. Sometimes it is possible to find hypertrophied skin muscles whose fibers are continuous with the tumor muscle (Fig. 5 ) .
A variation of this form is the nevoid leiomyoma in which the smooth muscle is only part of the tumor. Case 13 (Figs. 1 2 and 13), in which sebaceous glands also formed part of the tumor, is an illustration of this group.
The exceptional tumor which is not of the vascular type and which grows to a large size is so unusual that it should perhaps be discussed separately. Case 10 of this series was subcutaneous, encapsulated, and attained dimen- sions of 9 X 6 X 5 cm. I t is an almost pure leiomyoma with only a minimal amount of supportive stroma and few blood vessels. I t has degenerated in many places (Fig. 8). The cells are unusually large but otherwise not re- markable. Nowhere do they show size variation, hyperchromatism, or other features suggestive of malignancy (Fig. 9) . Blanc and Winberg’s skin tumor which attained a size of 7 X 5 X 3 cm. during a period of thirty years is probably a comparable case.
A few cases have shown cellular variation and other microscopic changes which led their reporters to suggest that they were malignant tumors. These changes are especially: variation in the relative size of cells with the formation of bizarre and monster cell forms, swelling and vacuolation of the muscle

SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 45 1
fibers, hemorrhages and necrosis, and increase in the frequency of mitosis. Their presence led Zieler and Hayn, Kopylow, Lieber, Marc, Mermet, Milian and PCrin, Neumann, and Huese to suggest that their cases were ipso facto malignant. It must be remembered, however, that similar pictures are found in leiomyomas of the uterus, especially in the presence of degeneration, and that they do not there necessarily connote malignancy. Without clinical evi- dence of malignancy we cannot accept these as proved malignant tumors.
The presence of nerves in these tumors has never been thoroughly inves- tigated and remains something of a mystery. In 10 of the present series of
FIG. 12. CASE XIII: PHOTOMICRCGRAPR OF A SECTION THROUGH THE FULL THICKNESS OF THE
The nevoid nature of TUMOR WITH THE PEDICLE AT THE RICIIT
The smooth muscle occurs in slender strands throughout the growth. the growth is suggested by the great number of sebaceous glands.
cases in which the fixation had been either Zenker, Bouin or formol, Mrs. A. H. Laidlaw used the Rogers technic in an attempt to demonstrate neurites but failed to blacken any, though this technic was successful in demonstrating the neurites of tumors of the neuromyo-arterial glomus. On the other hand, Grzybowski using Cajal’s modified silver impregnation method succeeded in staining a great many neurites both in and around a cutaneous leiomyoma of the face. The neurites in the tumor were both superficial and deep and ran parallel with the smooth muscle fibers, sometimes in the exact center of a bundle. If this observation is correct it is most important. So far it has not been repeated.

TA
BL
E
I : S
olit
ary
Cut
aneo
us a
nd S
ubcu
tane
ous
Lei
omyo
ma
?
__
_
Ves
sel
Ang
iom
atou
s le
iom
yom
a
Lei
omyo
ma
of ve
ssel
Ves
sel
+
Ves
El<
-' - L
eiom
yom
a ni
th fe
w v
esse
l:
Ang
iom
atou
s le
iom
yom
a M
F
36
40
__
~
F
F
42
47
__
~
Skin
.
Subc
ut.
Leg
, m
id.,
late
ral
Leg
, upp
er,
late
ral
Yes
Yes
Yes
Yes
0.5
0.7
M
M
49%
31
_-
Subc
ut.
Saph
enou
s op
enin
g
Subc
ut.
Kne
e, m
edia
l
Yes
Yes
?
__
~
\:ess
els
Pure
leio
my-
om
a
Ang
iom
atou
s le
iom
yom
a
Subc
ut.
Skin
.
[Vris
t, do
rsum
Nas
olab
ial
fold
? No
Ves
sels
M. c
utis
di
ag.?
Ang
iom
atou
s le
iom
yom
a
Nev
oid
leio
myo
ma
Subc
ut.
Subc
ut.
Ank
le,
ant.,
lat
eral
Leg
, mid
., m
ed.
No
Yes
\-es
Yes
1.5
1.3
x 1.
0 x
0.5
__
__
V
esse
ls
\'ess
els
Ang
iom
atou
s le
iom
yom
a
Ang
iom
atou
s le
iom
yom
a
-
I A
ge
Sex
1 at
Ons
et
Age
at
Obs
er-
vati
on
An
te-o
per
ativ
e D
iagn
osis
Neu
rofi
brom
a
Res
ult
Cas
e N
o.
Sit
e P
ain
~-
M 1 2
2 42
V
esse
ls
1 Ang
iom
atou
s I l
eiom
yom
a I
(191
5)
I1 (
1928
)
Subc
ut.
Fing
er,
dors
um
Not
fol
low
ed
Not
fol
low
ed *
_
__
F
46
50
Sk
in.
Are
ola
of ni
pple
1 ?
Ben
ign
tum
or
Pure
leio
my-
EZ
C /o
ma
FI l9
Se
bace
ous
cyst
N
ot f
ollo
wed
11
1 (1
929)
IV (1
931)
Subc
ut.
No
Subc
ut.
Yes
Leg
, m
id.,
late
ral
Leg
, la
tera
l
21
? N
ot f
ollo
wed
?
__
__
_
M
1 54
V (
1931
) 55
Su
bcut
. L
eg, l
ower
I Ye
s 1 .o
Y
es
I N
euro
lna
. D
ied 4 m
os.
late
r of
Hod
gkin
's d
isea
se
37
I Yes
Subc
ut.
Thu
mb,
dor
sum
Y
es
No
1 0.
5
1.5
x 1
x 0.
5 ~
__
~
? N
ot f
ollo
wed
Not
fol
low
ed
42
I Yes
Skin
. A
nkle
, la
tera
l, po
st..
Fibr
oma
Leio
m yo
ma
I with
few
ves
sel:
Neu
rofi
brom
a A
ngio
mat
ous
I leiom
yom
a V
III
(193
2)
IX (
1932
)
Not
fol
low
ed
Wel
l aft
er 2
54 y
ears
45
49
Neu
rofi
brom
a or
ne
urile
mom
a V
esse
ls
I Angi
omat
ous
X (
1933
)
Yes
0.
8 xO
.6
No
! 9x6x
5
Inca
rcer
ated
fe
mor
al h
erni
a Sy
mpt
om-f
ree
6 w
eeks
52
38
XI
(193
3)
Sym
ptom
-fre
e 43
m
onth
s t
Neu
rom
a
XI1
(19
34)
Not
fol
low
ed
33
61
Gan
glio
n
Papi
llary
nev
us
1.2
NO
1.2
x 1.
Q
XI1
1 (1
934)
M
1 C
hild
- I h
ood
Sym
ptom
-fre
e 3
mon
ths
XIV
(193
6)
Fiii
F
38
Not
fol
low
ed
Sym
ptom
-fre
e 3
mon
ths
Gan
glio
n
Neu
rom
yo-
arte
rial
glo
mus
tu
mor
41
49
XV
(19
36)
* Als
o fi
brom
yom
ata
uter
i. A
lso
neur
ilem
oma
of m
edia
n ne
rve.

SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 45 3
DIAGNOSIS If these tumors are in the symptomless stage, there seems to be little
chance of distinguishing them from other cutaneous and subcutaneous growths. If they are tender and painful, and particularly if the pain is paroxysmal, one may suspect that the growth is either a tumor of the neuromyo-arterial glomus or a leiomyoma. In differentiating between the two it may be recalled that leiomyomas do not occur beneath the nails and glomus tumors have only
FIG. 13. CASE XIII: PHOTOMICROGRAPH SHOWING THE CLOSE RELATIONSHIP OP THE SMOOTII MUSCLE BANDS TO SOME OF THE SEBACEOUS GLANDS
twice been reported outside of the extremities (FernSndez and Monserrat; Touraine, Solente, and Renault) . Moreover, the glomus tumors usually appear more reddish-blue and softer than the leiomyomas. Very little is known about the histology of other forms of tubercula dolorosa. Chandelux described a “ papillary fibroma of a sweat gland ” and a “ tubular epithelioma of a sweat gland ” and Most an “ endothelioma or hemangioendothelioma ” and a “ fibro- sarcoma of lowest malignancy,” all of which had characteristic crises. The small, usually multiple, pointed chondromata of the auricle (first described by Winkler in 1915, according to Nicolas, Massia and Colas) are well known but could hardly be confused with other tumors, because of their situation.

454 ARTHUR PURDY STOUT
A reference to Table I will show that none of the 15 tumors here reported This was due undoubtedly to lack was recognized as such before operation.
of knowledge of the existence of painful leiomyomas.
TREATMENT
Since surgical excision is simple and almost always entirely effective, it is the treatment of choice. The tumors have been treated successfully, how- ever, in other ways. Pearson, for example, destroyed his tumor with the caustic lapis infernalis and Bisset succeeded with two applications of caust. commune fort. In treating multiple cases Weissenbach, Carlu and Martineau have used electrocoagulation with success. Scaduto and Strempel have both reported success with irradiation by x-rays. Some of the nodules disappeared and pain was relieved. Stumpke, however, had no success with x-ray treat- ment. With the solitary tumor it is never necessary to resort to such meas- ures, and excision should be the only treatment.
CASE REPORTS
In the following case reports it should be noted that hematoxylin and eosin sections were prepared in every case and Masson’s aniline blue trichrome stain and the acid orcein stain for elastic fibers were done in all except Case 2 . Rogers’ stain was done in all except Cases 2, 6, 10, 1 2 and 13. Laidlaw silver reticulin stains were used in Cases 1, 5 , 10 and 1 2 , mucicarmine stain in Case 10, and phosphotungstic acid stain in Case 11.
CASE I (S. P. 17723): An Irish married male, aged forty-two years, was admitted Nov. 8, 1915. Twenty years earlier, after injury with a club, he noticed a small swelling of the right middle finger dorsally over the middle phalanx. After fourteen years this began to grow larger and became tender. Since then it had grown but little. There were never any signs of inflammation. The tumor (Fig. 1) formed a nodule, about 1 cm. in diameter, elevated 2 mm. above the skin surface. Peripherally the swelling was soft, with a firm rounded body in the center. This whole mass was excised. The wound healed cleanly in a week and the case was not followed.
The hard tumor nodule is composed of a great many thick blood vessels the walls of which are made up of alternating layers of smooth-muscle and reticulin fibers. The tissue between is also made up of muscle and connective-tissue fibers but without any definite arrangement. At the periphery are longitudinally cut vessels with smooth muscle irregularly disposed in the walls. I t is impossible to say whether these are arteries or veins. Outside of the hard tumor is a mass of fat scattered through which are many thick-walled capillaries. This evidently formed the soft part of the swelling. Although some small nerve bundles were recognized in this surrounding fat, the Rogers stain failed to demonstrate any neurites in the central tumor.
CASE I1 (S. P. 37879): An American housewife, aged fifty years, married, was ad- mitted June 14, 1928. Four years before admission she first noticed in the areola above the left nipple a small nodule which grew slowly. No statement is made as to pain or tender- ness. The tumor was bilobed, measured about 7 X 5 mm., and lay immediately beneath the epidermis, some of which was excised with it. The patient also had fibromyomas of the uterus. The case was not followed.
The tumor is composed of densely packed, interlacing strands of swollen smooth-muscle fibers accompanied by fibrous tissue. The growth is not encapsulated but fills the corium extending up to the subpapillary layer. NO glands or hair follicles are included within the tumor. Deep to the tumor are the bundles of the muscularis areolae. These are extremely

SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 45 5
thick and long, suggesting hyperplasia. Some of them pass directly into the tumor and their muscle fibers intermingle with the muscle fibers of the tumor (Fig. 5 ) .
CASE I11 (S. P. 41783): An American married female, a stenographer, aged twenty- one, was admitted Nov. 12, 1929. She had noticed a small slightly tender nodule on the side of the right leg at about the midpoint for two years, which she thought followed a bruise. The size remained stationary. On examination the nodule was reported to bc firm, slightly tender, and movable except for its attachment to the skin. I t was thought to be a sebaceous cyst. At operation it was reported to be superficially subcutaneous and well encapsulated and was excised. The wound healed and the case was not followed.
FIG. 14. PHOTOMICROGRAPH OF THE SKIN OF THE CHEEK AT THE LEVEL OF THE ANGLE OF THE MOUTH, SHOWING SOME BANDS OF THE MUSCULI DIAGOHALES CUTIS
DEEP IN THE CORIUM In the photograph the muscle bands are pale in contradistinction to the darker bands of
collagen.
The specimen was a pale pink, irregularly rounded, encapsulated nodule 1.3 cm. in diameter. The cut surface showed bands of white fibrous tissue and pale gray semitrans- lucent tissue in approximately equal amounts. Microscopically the fibers of smooth muscle and collagen are approximately equal, although irregularly disposed. The blood vessels pass through the muscle and fibrous tissue sometimes with, but usually without, definite walls and with haphazard arrangement. No elastic tissue and no neurites could be demonstrated.
CASE IV (P. & S. 11804) : An adult Chinese female, single, was admitted Feb. 16, 1931. An 8 mm. nodule had been present in the outer side of the leg for ten years, and had been painful for the past year. I t was superficially subcutaneous and was excised. The result is not known.
Section through it shows a small central lumen 1 mm. in diameter which on one side extends up to the capsule. Microscopically the empty central lumen shows an endothelial lining which rests upon a thin layer of fibrous
The nodule is rounded and encapsulated.

456 ARTHUR PURDY STOUT
tissue containing a few elastic fibers. The rest of the wall of this vessel is made up of a few circularly arranged smooth-muscle fibers which quickly merge with the muscle of the tumor. This consists of irregularly disposed bundles of smooth-muscle fibers supported by fibrous sheaths which run in various directions. Very little elastic tissue is found. In this there are a considerable number of vessels both capillaries and others with muscular walls. In the latter group the vascular muscle merges with the muscle of the tumor. NO neurites are demonstrated (Fig. 6).
CASE V (S. P. 45559) : An Italian male, married, a fruit merchant, aged fifty-five years, was admitted May 18, 1931. The patient was under treatment for Hodgkin’s disease but came complaining of a small painful and tender nodule which had been present on the lateral aspect of the right lower leg for one year. The pain was so great that it kept him awake at night. Examination showed a nodule 1 cm. in diameter, which lay beneath the skin, 5 cm. above the right lateral malleolus. I t was tender and freely movable. The operator reported: “ In the superficial subcutaneous tissues a small, hard, well circumscribed tumor was found about 1 cm. in diameter. . . . At its proximal pole was a small, tough, thread- like structure, similar in appearance to a nerve fiber.” The tumor was excised. The pa- tient died of Hodgkin’s disease after four and a half months.
Microscopically the tumor is found to be composed chiefly of smooth muscle with a generous fibrous stroma about each bundle of myofibrils. There are many capillaries in some areas, fewer in others, and only occasional vessels with definite muscular walls. This muscle merges at the periphery of the vessel with the muscle of the tumor. No elastic fibers or neurites can be demonstrated. In the fibrous capsule an occasional vein is found.
CASE VI (S. P. 46454) : An Italian male, married, a shoemaker, aged thirty-seven years, was admitted Sept. 23, 1931, complaining of a swelling at the base of the thumb on the dorsal surface near the metacarpophalangeal joint. It had been painful and tender for three days. One year before the patient had had a similar attack of pain and tenderness in the lump. The tumor lay beneath the skin, was encapsulated, and shelled out quite easily. The wound healed by first intention and the case was not followed.
It is encapsulated and the cut surface is hard, whitish brown in the center, and shows dilated vessels about the periphery. Micro- scopically the tumor is made up of numerous large and small vessels and some dilated vascular spaces filled with blood. Many of the large vessels have very thick walls made up of much fibrous tissue and scattered smooth-muscle bundles concentrically arranged. The entire circumference of the tumor is composed of several layers of smooth muscle, while the central portion between the vessels is composed of dense fibrous tissue and an occasional stray muscle fiber. The blood in one of the vascular spaces is thrombosed. There is considerable polymorphonuclear leukocytic infiltration in parts of the tumor. The growth is surrounded by a fibrous capsule in which capillaries and veins with imperfectly muscled walls are found, but no nerve bundles are seen. A small number of delicate elastic fibers are found in some of the vessel walls and occasionally in the fibrous tissue of the tumor. Neurite stains were not done.
CASE VII (48128): A married Polish woman, aged forty-two, was admitted April 25, 1932. Two years before she had noticed a small swelling on her left ankle, about one inch posterior to the external malleolus. I t was like a pearl and had caused no pain until two months before admission, a t which time it became larger. Since then it had been very painful a t times. The pain came suddenly, with pinching and pricking sensations. I t would often come on in the morning, lasting half an hour, and then cease until later in the day, when it would return at recurring intervals for short periods of time. The pain was so severe that it would prevent sleep and no medication relieved it. Examination showed an elevated, non-tender area 1 cm. in diameter adherent to the skin. I t was hard, white, and freely movable deeply. I t was excised with the overlying skin. Healing was by first intention. The case was not followed.
The excised tumor measures 5 mm. in diameter. I t is encapsulated and section shows whorls of pale, opaque, whitish tissue mixed with semitranslucent areas. There is one tiny area of calcification. Microscopic examination shows interlacing bands of smooth muscle and collagen fibers in approximately equal amounts. The tumor is very unequally supplied with blood vessels; in some areas they are numerous, in others they are scarce.
The tumor measures 1.5 X 1 X 0.5 cm.

SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 45 7
Most of the vessels are capillaries; occasionally a vessel is found with a small amount of smooth muscle in its wall merging peripherally with the muscle of the tumor. No elastic tissue and no neurites can be demonstrated in the tumor. The tumor capsule contains ves- sels resembling veins, some of which have walls composed in places of smooth muscle and elsewhere of nothing but fibrous tissue. Sweat glands are present in one part of the capsule.
CASE VIII (S. P. 48816) : A colored bath maid, aged forty-five years, and married, was admitted July 12, 1932. For two or three years she had noticed a nodule on the outer aspect of the middle third of the lower leg. I t was only occasionally painful when the pa- tient was walking. I t was always tender to touch, with radiation of pain over the outer aspect of the leg. On examination a tender slightly raised indurated area was found, about 5 mm. in diameter. I t was excised with some of the overlying skin.
FIG. 15. CASE XIV: PHOTOMICROGRAPH OF ONE OF THE PECULIAR VESSELS WlTH A THICK CONCENTRICALLY ARRANGED MUSCULAR COAT WHICH AT THE RIGHT Is INDIS-
TINGUISHABLY INTERTWINED WITH THE SMOOTH MUSCLE OF THE TUMOR Immediately surrounding the lumen is a layer of fibrous tissue.
The tumor is grayish white, dense, and encapsulated. It lies in the deeper layers of the skin. Microscopic preparations show that the growth is composed very largely of interlaced smooth-muscle fibers arranged in bands accompanied by collagen fibers. There are many blood vessels, most of which have thick walls. Many of them have concentrically arranged smooth muscle which merges peripherally with the smooth muscle of the tumor. In the capsule are many capillaries and occasional veins. Capillaries appear in considerable numbers, also, in the corium outside of the capsule. Elastic tissue is found in the veins in the capsule but not in the vessels of the tumor. No neurites are found in the tumor.
CASE I X (S. P. 49883): A Russian Jewess, aged forty-nine years, married, was ad- mitted Nov. 1 2 , 1932. For two years she had noticed a small firm nodule on the outer aspect of the left leg, 5 cm. distal to the knee joint, which had not varied in size since she first found it and which was occasionally painful. On examination a firm, tender, circum- scribed nodule about 8 mm. in diameter was found which was movable with the skin. It

45 8 ARTHUR PURDY STOUT
was excised. The operator stated that it was encapsulated and subcutaneous. The patient also had fibromyomas of the uterus, corpus luteum cyst of the ovary, chronic salpingitis, and abdominal hernia, for which she was operated upon and followed for thirty-five months. As the case history contained no further notes about the leg, it may be assumed that it gave no further trouble.
I t is grayish white and the cut surface has the translucent appearance of smooth muscle. Microscopic preparations show that the growth is largely made up of smooth-muscle fibers which are gathered into interlacing bundles and ensheathed by delicate collagen fibers. The vessels are numerous in some areas and scanty in others. Most of them are capillaries; only a few have muscular walls, but in these the muscle blends with the tumor muscle a t the periphery. No neurites m d no elastic tissue are found.
CASE X (S. P. 50725): An American salesman, aged fifty-two years, married, was ad- mitted March 4, 1933. Two and a half years before admission he first noticed a swelling the size of a marble in the left femoral region. I t grew steadily. occasioning only slight discomfort, until two weeks before admission, when there occurred a sharp, griping pain in the tumor which radiated to the left iliac crest and lasted half an hour. On the day of admission a similar attack occurred. During both these attacks the patient was nauseated and had a desire to go to stool. The mass was believed to be an incarcerated femoral hernia. Operation showed an encapsulated tumor 9 X 6 X 5 cm., which was unusually vascular peripherally. I t seemed to the operator (Dr. R. S. Grinnell), when he cut into it, to be an edematous soft fibroma. It shelled out easily. The base of the tumor lay in the saphenous opening just medial to the femoral vein in the exact position that the neck of a femoral hernia would lie. When cut open the tumor seemed to be made up of fibrous strands running in various directions. In many places were areas of degeneration and small cystic cavities filled with mucoid material. Many small thick-walled vessels were found throughout the tumor.
Microscopically the tumor is composed almost exclusively of well differentiated long smooth-muscle cells with longitudinally arranged myofibrils, which form interlacing bands and are supported only by a minimal amount of delicate collagen fibers. Even in the well preserved parts there are many vacuoles and in the areas of degeneration these coalesce to form large anastomosing spaces filled with a fluid which is not stained by mucicarmine and which retains the fibrous skeleton of the tumor framework but only occasional muscle cells. Mitoses are found only after a long search. The tumor has a capsule which is intact. A number of mast cells are scattered all through the tumor. There are many blood vessels, most of which are capillaries. The larger vessels have a zone of dense fibrous tissue about the lumen, outside of which is smooth muscle arranged a t haphazard and indistinguishable from the tumor muscle, so that it is impossible to say whether or not these vessels have muscular walls. There is nothing to suggest a malignant change. No elastic tissue is found.
CASE X I (S. P. 51377): A married Greek male, a waiter, aged thirty-eight years, was admitted May 22, 1933. Seven years earlier he noticed a small, rounded swelling over the medial side of the left knee. It grew slowly until eighteen months before admission, since which time it had remained stationary. The tumor gave no symptoms unless it was struck, when it would burn momentarily as if a cigarette had been pressed against it. No other similar nodules were present but the patient also had a neurilemoma of the median nerve.3 Both tumors were removed at the same time. The leg tumor was firm, encap- sulated, and lay immediately beneath the skin. It measured 8 X 6 mm. and the cut surface had a pale semitranslucent appearance. Forty-three months after removal there were no symptoms or evidences of recurrence.
Microscopic preparations show an encapsulated tumor composed of smooth muscle and collagen strands arranged in irregular interlacing bundles together with many vessels with very thick walls composed of concentrically arranged smooth muscle, collagen, and varying amounts of elastic tissue. The smooth muscle sometimes blends with the tumor muscle at the periphery. Elastic fibers are found chiefly in the thick-walled vessels and occasionally in the surrounding fibrous stroma. NO neurites could be demonstrated. Only a small amount of the fibrous capsule is shown.
3 Case 29, Stout, A. P.: Peripheral Manifestations of the Specific Nerve Sheath Tumor (Neurilemoma), Am. J. Cancer 24: 751, 1935.
The excised nodule averages 7 mm. in diameter.

SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 459
CASE XI1 (S. P. 54436) : An American printer of Scotch-English parentage, aged thirty- three years, married, was admitted May 25, 1934. A small growth had appeared on the dorsum of the left wrist four years before and steadily increased in size until i t was approxi- mately 2 cm. in diameter. No statement as to pain or tenderness was recorded. It was thought to be a ganglion and several attempts were made to aspirate it without success. One month after the patient was first seen, the tumor was excised. It lay just beneath the skin, toward the ulnar side, and was encapsulated. I t measured 1.2 cm. in diameter and a cutaneous nerve ran over the capsule but was not attached to it. When cut open i t was firm and had a pale gray appearance mottled with brown. The wound healed by first intention and the case was not followed.
Microscopic preparations show a tumor composed of irregularly interlaced bands of smooth muscle and collagen with an area of edema and collagen degeneration toward the center. This region is infiltrated with a good many lymphocytes, leukocytes, and plasma cells. The tumor also contains many blood vessels, both capillaries and others with thick fibrous and muscular walls. Most of the thick-walled vessels are of the venous type either with a small amount of elastic tissue or none at all. Only two arterioles with definite elastic laminae are recognized. In some areas thin-walled anastomosing vascular spaces give the growth the appearance of a cavernous angioma. Vascular and tumor muscle intermingle where they come together. In the capsule are some capillaries. Partly organized clots mark the sites of previous needlings. Neurite stains were not done. There are a number of very delicate elastic fibers in some parts of the tumor, usually in the adventitia of the vessels and fibrous stroma of the tumor.
CASE XI11 (S. P. 55307): A male Russian Jew, aged sixty-one years, married, was admitted Aug. 28, 1934. For as long as he could remember the patient had had a peduncu- lated, smooth, nodular reddish growth in the right naso-labial fold, measuring 1.2 x 1 cm. I t gave no symptoms hut interfered with shaving. I t was excised with a little skin a t the base. I t was not necessary to ligate any vessels. After three months there was no evi- dence of reappearance.
Microscopically the tumor consists of a growth of smooth-muscle fibers arranged in small bundles which run at haphazard in every direction and are accompanied by an even greater quantity of fibrous tissue, the collagen fibers of which not only separate the bundles but surround each of the muscle fibers. The muscle bundles extend from immediately beneath the papillary layer to the base of the pedicle. There are many sebaceous glands and a moderate number of hair follicles. The muscle bundles are often in close relationship with the hair follicles and sebaceous glands and it is not possible to distinguish tumor muscle bundles from the arrectores pilorum. There are many vessels, most of which are capillaries and some of these are widely dilated. Only a few vessels have muscular walls. These are normal in appearance and do not seem to have any relation to the tumor muscle. No nerve bundles are recognized. The normal elastic tissue of the skin is present, but the smooth muscle bundles are devoid of elastic fibers.
CASE XIV (S. P. 60198): An English housewife, aged forty-one years, married, was admitted March 12, 1936. She had noticed a nodule for four years on the antero-medial aspect of the left ankle. At times it was very tender. I t measured 1.5 cm. in diameter and was considered a ganglion. At operation it was found to lie beneath the skin, to be encapsulated, and to have a deep attachment. It was shelled out. The wound healed and the case was not followed.
Microscopic preparations show an encapsulated tumor composed of muscle and collagen fibers arranged in irregularly interlacing bundles. Toward the center the growth is almost all fibrous. There are many capillaries and thick-walled vessels in some areas and very few in others. In some of the large vessels the thick muscle bands join the tumor muscle (Fig. 15). Elastic tissue is found in small quantities in the fibrous tissue about some of the tumor vessels but not elsewhere. .No neurites could be stained. In the capsule are capil- laries and a few irregularly muscled veins.
CASE XV (S. P. 61611): An American housewife, aged forty-nine years, married, was admitted Aug. 10, 1936. Ten or eleven years earlier she first experienced a sharp, sticking sensation in her right leg on walking. At first the pain was not severe nor did it occur every time she walked, but usually a t intervals of two to three days. At times the pain would

460 ARTHUR PURDY STOUT
persist for a short while after the patient sat down, especially if she stretched out her legs. There was moderate tenderness if she touched the painful area. One year before admission all of the symptoms became aggravated, and a tumor was noticed for the first time. Dur- ing this period the pain was much more severe and occurred every time the patient walked or exercised, lasting for the duration of the exercise. Recently it became so severe that she was forced to rest whenever it occurred. When she did so it would gradually disappear. I t was never unbearable and never radiated. I t s onset was sudden and occasionally it disappeared suddenly after resting, but usually it lasted for some time. Recently any sort of pressure, a light touch with the hand or pressure by clothing or bedclothes, would initiate an attack. Occasionally there were paroxysms of pain without any known cause, lasting ten to fifteen minutes and forcing the patient to sit down while they lasted. The pain never awakened her a t night. After the nodule was first noticed it slowly increased in size.
FIG. 16. CASE XV: PATIENT’S RIGHT LEG, SHOWING THE SITUATION OF THE TUMOR
There were no other comparable nodules elsewhere on the body; there was no history of trauma, nothing suggesting sympathetic system disturbance elsewhere, and no familial history. Examination revealed an exquisitely tender tumor lying beneath the epidermis in the anterior crural region. I t was subcutaneous, encapsulated, attached to the skin, but movable deeply. After excision it appeared firm, pale, and fibrous, and measured 1.3 x 1 X 0.5 cm. When seen three months later the patient had no symptoms in her leg. (History taken by Dr. L. W. Sloan.)
Microscopic preparations show an encapsulated tumor composed of masses of smooth muscle and fibrous tissue irregularly disposed and a great many thick blood vessels whose walls are composed of circularly arranged bands of smooth muscle and collagen fibers. Sometimes the fibrous bands are nearest the lumen; sometimes they are outside of the muscle; sometimes either the muscle or the fibrous bands are lacking. Most of the vessels have small lumens which are either empty or contain a few red blood cells. Some have no

SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 46 1
lumen, its place being taken by fibrous tissue. There is no elastic tissue and no neurites were stained. The muscle of these vessels blends at the periphery with the muscle of the tumor. In the capsule veins, arteries and capillaries are found. The arteries are normal but some of the veins approach the structure of the tumor vessels with absence of elastic tissue and irregularly disposed muscle and fibrous tissue.
SUMMARY Fifteen cases of solitary leiomyoma are reported, 4 of which were cutane-
ous and 11 subcutaneous. A review of the literature shows that previously at least 85 solitary and 132 multiple cases of cutaneous and subcutaneous leiomyoma have been recorded. A complete bibliography of these is ap- pended.
The salient clinical features of the solitary tumors include their generally long duration and small size; their peculiar distribution, especially on the extensor surfaces of the upper and lower extremities, the scrotum, labium majus, the nipple and areola, the cheeks, and rarely elsewhere; the charac- teristic pain, often of a paroxysmal nature, so frequently caused by them. That this pain is probably associated with violent contractions of the neo- plastic smooth muscle is indicated by the observations of a number of dif- ferent reporters. Morphologically it is pointed out that they are composed chiefly of smooth muscle derived from one or another of the smooth-muscle structures in the areas involved, and that they develop in two chief forms, one without and the other with peculiar vascular structures which are probably in the nature of veins.
The failure to find any neurites in any of the tumors here reported is admitted and the fact that one observer, Grzybowski, has succeeded in stain- ing a large number in one cutaneous leiomyoma is regarded as suggestive that our own and other attempts have failed because of technical errors.
The opinion is expressed that these tumors, together with the tumors of the neuromyo-arterial glomus, probably form the bulk of the painful subcu- taneous tubercles (tubercula dolorosa) of the older writers of the 18th and 19th centuries, and suggestions for differential diagnosis are made.
The rarity of malignant cutaneous and subcutaneous leiomyomas is pointed out, and the effectiveness of surgical excision as the treatment of choice for the leiomyomas is stressed.
Finally, it is suggested that these solitary tumors contrary to the general impression, are as common as, if not more common than, the multiple cu- taneous leiomyomas, and that a wider knowledge among clinicians of their existence and a more general use of differential fiber staining in pathological laboratories will lead to their more frequent recognition.
BIBLIOGRAPHY
Solitary Cutaneous and Subcutaneous Le iomyoma
ANGELELLI, 0.: Sui miomi cutanei, Policlinico (sez. chir.) 33: 69, 1926. ARNDT, G.: Myoma cutis, Arch. f . Dermat. u. Syph. 112: 381, 1912. ASAI, J.: Ein Fall von solitarem Dermatomyom, Acta dermat. (Kioto) 7: 687, 1926. Abst.
ASAL, W.: Zur Kasuistik der Hautmyome, Deutsch. med. Wchnschr. 51: 221, 1925. in Zentralbl. f. Haut- u. Geschlechtskr. 22: 376, 1927.
462 ARTHUR PURDY STOUT
AUDRY, C.: Note sur un lio-myBme solitaire de la peau, Ann. de dermat. et syph., 3me sCr.
AUDRY, C. : Nodule sous-cutanC iL structure de naevus arteriel lCiomyomateux, Bull. SOC.
AUDRY, C.: Leiomyome solitaire de la peau en rapport avec les arrecteurs, Bull. SOC. franc.
AUFRECHT, E.: Ein Myom der Vena saphena, Virchow’s Arch. f . path. Anat. 44: 133, 1868. BABES: The Myoma of the Skin, in v. Ziemssen, H. : Handbook of Diseases of the Skin,
New York, Wm. Wood and Co., 1885, pp. 607-610. (A translation of the 14th volume of the Handbuch der spez. Path. und Therapie, 1884.)
BARTKOWIAK, Z.: Ein Fall von Sarcoma leiomyoblasticum der Haut, Centralbl. f . allg. Path. u. path. Anat. 65: 179, 1936.
BAUER, T. : Zur normalen und pathologischen Anatomie und Histologie der menschlichen Brustwarze, Beitr. z. path. anat. u. z. allg. Path. 62: 233, 1916.
BLANC AND WINBERG: MyBme dermique ti la cuisse, Ann. de dermat. et syph., 3“’e sCr. 7: 1371, 1896.
BRUGGER, A. G.: Isoliertes Leiomyom, Zentralbl. f . Haut- u. Geschlechtsk. 27: 346, 1928. Ein Fall von Leiomyom, Wien. med. Wchnschr. 78: 330, 1928.
CHALLAND, TH. : Molluscum pendulum de la grande kvre gauche (Fibro-myBme). Mol- luscum pendulum du scrotum (Fibro-myBme), Bull. SOC. anat., Paris 46 (Sme sCr. 6 ) :
CHAMBARD, E., AND GOUILLOUD: Myome xanthomateux dCveloppC dans un molluscum, Ann.
CORNIL: Myome dans les veines du bras, Bull. SOC. Anat., Paris 7 1 (5”’“ sir. 10): 725, 1896. DAGONET, J.: Uber die Entstehung der Hautmyome, Festschrift fur Hans Chiari, 1908, p. 1. DEVIC AND GALLAVARDIN, L. : Contribution A l’dtude du leiomyome malin avec gCnCralisation
DISS, A.: Deux cas de dermatomyome, Bull. SOC. franc. de dermat, et syph. 30: R.S. 20,
DIM, A., AND L%vY, G.: LCiomyosarcome dCveloppC sur un ancien lupus tuberculeux de la
DRIAK, F., AND STERNBERG, H.: Uber Myome der Brustdriise, Deutsche Ztschr. f . Chir.
DUBOUCHER, H., AND MONTPELLIER, J. : Dermatomyome solitaire, Bull. SOC. franc. de
DUBREUILH, W.: Myomes A fibres lisses de la peau, Bull. SOC. franq. de dermat. et syph.
ECOFFEY, M. : FibrolCiomyome tklangiectasique d’une branche de la veine saphkne, Arch. de
F ~ R S T E R : Ueber die weichen Warzen und molluskenartigen Geschwiilste der Haut, Wien.
FORSTER, A. : Handbuch der speciellen pathologischen Anatomie, L. Voss, Leipzig, 1563,
GRZYBOWSKI, M.: Contribution l’ktude de l’histologie des myomas cutanCs, Ann. de
GRZYBOWSKI, M.: Btude des nerfs dans le dermatomyome, Przeglad Dermat. 28: 1, 1933.
HAGIWARA, S., AND SUGIZAKI, K.: Ein Fall von solitarem Dermatomyom, Jap. J. Dermat.
HAREL, L. : Contribution A 1’Ctude des tubercules sous-cutanCs douloureux, Thkse de Paris,
HAYN, FR.: Zur Kenntnis der destruierenden Myome der Haut, Arch. f . Dermat. u. Syph.
HERZOG, M.: A case of myoma of the skin, J. Cutan. Dis. 16: 527, 1898. HIEBAUM, A. : Zur Casuistik der multiplen Cystenbildung in der weiblichen Brustdruse.
Multiple Cysten bei Fibromyom in der Mammilla, Prager med. Wchnschr. 20: 293 and 314, 1895. Abst. in Centralbl. f. allg. Path. u. path. Anat. 7 : 20, 1896.
HUESE, J, F. 0.: Een fibromyoom aan den duim, Nederl. Tijdschr. v. Geneesk. 2 : 2551, 1921.
9: 182, 1898.
franc. de dermat. et syph. 38: 222, 1931.
de dermat. et syph. 38: 1518, 1931.
145-149, 1871.
de dermat. et syph. Zme sCr. 4: 660, 1883.
viscbrale, Rev. de chir. 24: 282, 1901.
1923.
face, Bull. SOC. franc. dermat. et syph. 31: R.S. 108, 1924.
207: 352, 1928.
dermat. et syph. 42: 797, 1935.
28 : 251, 1921.
mCd. expbr. et d’anat. path. 27: 454, 1917.
med. Wchnschr. 8 : 130, 1858.
p. 1042.
dermat. et syph. 7me sCr. 4: 852, 1933.
Abst. in Zentralbl. f . Haut.- u. Geschlechtsk. 46: 196, 1934.
& Urol. 34: Abst. sect. 126, 1933.
1881.
105: 211, 1911.

SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 463
HUPPERT, M.: Zwei Falle von solitaren Myomen der Haut, Centralbl. f . allg. Path. u. path.
JADASSOHN, J. : Dermatomyom, in Lesser's Encyklopadie der Haut-und Geschlechtskrank-
JARDET: Myome sous-cutanC douloureux, Bull. SOC. anat., Paris 59 (4me sCr. 9 ) : 244, 1884. JESIONEK AND WERNER, A. : Naevus myomatosus, Histopathologie eines solitaren Myoms
der Haut, Arch. f . Dermat. u. Syph. 88: 223, 1907. KAUFMANN, E. : (Fibromyoma of the nipple) in Spezielle pathologische Anatomie, Berlin,
Gruyter, vol. 11, 1922, p. 1385. KEY, A , : Fall af myofibroma lymphangiectaticum subcut. dig. I11 och af myofibr. cutis,
Hygiea. Sv. lak. sallsk forhandl., 1873. Abst. Virchow and Hirsch: Jahresbericht Leist. u. Fortschr. ges. Med., xii Jhrg. 1: 271, 1877.
KLEBS, E.: Handbuch der pathologischen Anatomie, A. Hirschwald, vol. I, part 1, 1869. p. 76.
KOPYLOW: Ein Myom der Haut mit tfbergang in ein Sarkom, Russky Wratsch, No. 27, 1908. Abst. in Monatschr. f . prakt. Derm. 47: 637, 1908.
R R ~ M E R : Quoted by Babes. LEVIT, J. : Ein seltener Fall eines aus den Musculi arrectores pili hervorgegangenen solitaren
Leiomyoms, Wien. klin. Rundsch. 28: 2 7 , 1914. Abst. in Arch. f . Dermat. u. Syph. 122: 357, 1918.
LIEBER, K.: tfber die Myome der Haut, Beitr. z. path. Anat. u. z. allg. Path. 60: 449, 1915. LUQUET, G.: Leiomyome malin de la rCgion thoracique, Presse mCd. 38: 89, 1930. MALHERBE, A. : Note sur la structure des tumeurs dites tubercules sous-cutanCs douloureux,
Gaz. mCd. de Nantes 2 : 179, 1884. MARC, S.: Ein Fall von Leiomyoma subcutaneum congenitum nebst einigen Notizen zur
Statistik der Geschwiilste bei Kindern, Virchow's Arch. f . path. Anat. 125: 543, 1891. MARCANO, G.: Fibro-my6me de la grande lCvre, Bull. SOC. anat., Paris 48 (5"" sCr. 6 ) : 388,
1873. MERMET, P. : Qnorme dermato-my6me de la cuisse. DCgCrCresence sarcomateuse. Bull.
SOC. anat., Paris 71 (Sme sCr. 10): 653, 1896; Ann. de dermat. et syph. 3me sCr. 8: 797, 1897.
MIGLIORINI, G.: Fibromioma teleangectode della pelle, Gior. ital. delle mal. ven. 39: 297, 1904.
MIGLIORINI, G. : Mioma perivascolare della pelle (angiomioma), Gior. ital. delle mal. ven. 40: 51, 1905.
MILIAN, G., AND PERIN, L.: Fibro-myome sur lupus, Bull. SOC. franc. de dermat. et syph. 33: 621, 1926; RCV. franc. dermat. et vCn. 3: 152, 1927.
MILIAN, PERIN, L., AND DELARUE: Tumeurs variCes sur lupus, Bull. SOC. franc. de dermat. et syph. 34: 432, 1927.
MOBERG, L. : Fall af solitart hudmyom, Svenska Lokoresollsk. forhandl. p. 282, 1908. Abst. in Dermat. Jahresbericht, 4: 2 5 2 , 1908; Dermat. Stud., Hamburg u. Leipzig, 21: 138, 1910.
NEUMANN, W. : Ueber ein primares leiomyoplastiches Sarkom der Haut, Centralbl. f . allg. Path. u. path. Anat. 52 : 65, 1931.
NICOLAU: Ein Fall von Leiomyom des Penis, Revista Stiinzelor med., Dec. 1909. Abst. in Monatschr. f . prakt. Dermat. 52: 540, 1911.
NIEDERLE, B.: Leiomyoma venae medianae et basilicae cubiti, Cas. 1Ck. Eesk. 51: 169, 1912. NIKLAS: Diss., Wiirzburg, 1889. Quoted by Lindfors. PASSALACQUA, A. : Contribuzione all0 studio del leiomyoma cutis, Riforma med. 2 : 1580,
1890. PEARSON, J. : An account of some extraordinary symptoms which were apparently connected
with certain morbid alterations about the veins and nerves, Medical Facts and Obser- vations 6: 96, 1795.
PH~LIESSE, G.: Contribution i 1'Ctude des myomes de la peau et du tissu sous-cutanC, These de Paris, 1887.
PHOTINOS, P.: Zur Kenntnis und Histologie des Leiomyoms der Haut, Dermat. Wchnschr. 95: 1053, 1932.
Anat. 38: 582, 1926.
heiten, Leipzig, 1900.

464 ARTHUR PURDY STOUT
RAGINS, A. B.: A solitary vascular myoma of the skin, Arch. Dermat. & Syph. 23: 1087, 1931.
RAZUMICHIN, V. S. : Uber Unterhautleiomyome, Vestn. Khir. (russ.) 43/44: 70, 1928.
SANTESSON: Quoted by Key. SAWADA, H.: Angiomyofibroma cavernosum subcutaneum, Acta Dermat. 16: 568, 1931. SCHNYDER, K.: Leiomyom der Vena marginalis lateralis pedis, Centralbl. f . allg. Path. U.
SEHRT, E.: Subkutane Leiomyome der Wange u. ihre Histogenese, Beitr. z. klin. Chir. 54:
SELMI, M. : Angio-fibro-mioma doloroso o forma spuria di morbo di Recklinghausen, Gazz.
SIMONELLI, F. : Contributo allo studio dei miomi cutanei, Dermosifilografo 10: 718, 1035. SOKOLOW : Myoma laevicellulare (Leiomyoma) der rechte Brustwarze, Virchow's Arch. f .
SOUPAULT, R., A N D POMMAY, S.: Les leio-miomes sous-cutanks, Ann. d'anat. path. 1 : 433,
VALUDE, E.: Fibro-myome de la grande livre, Bull. SOC. anat., Paris 59 sCr. 0 ) : 223,
DEL VIVO, G.: Contributo allo studio dei miomi cutanei, Giorn. ital. derniat. et sif. 66: 333,
DEL VIVO, G.: Nuovo contributo allo studio dei miomi cutanei, Arch. ital. dermat. e sif. 2 :
WASSENAAR, T.: Leiomyoma of upper eyelid, J. M. A. South Africa 5 : 818, 1931. WOLTERS, M. : Eigentiimliche Veranderungen der Haut iiber einer meningocele, Dermat.
ZIELER: Ueber ein malignes Myom der Haut, Verhandl d. deutsch. path. Gesellsch. 12: 142,
Abst. in Zentralbl. f . Haut- u. Geschlechtsk 31 : 820, 1929.
path. Anat. 25: 529, 1914.
723, 1907.
d. osp. 52: 871, 1931.
path. Anat. 58: 316, 1873.
1924.
1884.
1925.
373, 1927.
Ztschr. 12: 427, 1905.
1908.
Multiple Leiomyoma of the Skin
ABERASTURY, M. : Contribuci6n para el conocimiento de 10s miomas cutineos, Semana mCd.
ABRAMSON, J. A.: Ueber multiple Leiomyome der Haut, Russky Wratsch, No. 46/47, 1913.
ABRAMSON, J.: Dermatomyomes multiples, Ann. de dermat. et syph. 7111e skr. 4: 322, 1933. ADRIAN: Fall von multiplen Dermatomyomen, Arch. f . Dermat. u. Syph. 117: 887, 1914. ADRIAN AND TILP: Multiple Dermatomyome, D,eutsche med. Wchnschr. 39: 1709, 1913. ANDO, N.: Uber Myomatosis multiplex, Japanese J. Dermat. & Urol. 24: 57, 1924. Abst.
ARNDT, G.: Myoma cutis, Arch. f . Dermat. u. Syph. 112: 381, 1912. ARNDT, G.: Multiple Leiomyome der Wangenhaut, Arch. f. Dermat. u. Syph. 137: 10, 1921. ARNOZAN AND VAILLARD: Mydmes i fibres lisses, multiples, confluents et isolCs de la peau,
Ann. de dermat. et syph. 2"" sCr. 2: 60, 1881; J. de mCd. de Bordeaux 10: 230, 1880-81. BABES, V.: The Myoma of the Skin, in v. Ziemssen, H.: Handbook of Diseases of the Skin,
New York, Wm. Wood & Co., 1885, pp. 607-610. (Trans. of 14th vol. of Handbuch der spez. Path. und Therapie, 1884.)
2: 1105, 1933.
Abst. in Centralbl. f . allg. Path. u. path. 'Anat. 25: 268, 1914.
in Zentralbl. f . Haut- u. Geschlechtskr. 16: 55, 1925.
BALINT, G.: Leiomyoma cutis, Zentralbl. f . Haut- u. Geschlechtsk. 26: 655, 1928. BALZER: Quoted by Babes. BASCH: Fall von Leiomyoma cutis, Arch. f . Dermat. u. Syph. 65: 124, 1903. BASCH: In Discussion of case of v. Marschalk6, Arch. f . Dermat. u. Syph. 72: 253, 1904. BEATTY, W.: A case of multiple leiomyomata of the skin, Brit. J. Dermat. 19: 1, 1907. BECHET: A case for diagnosis, Arch. Dermat. and Syph. 17: 275, 1928. BESNIER, E.: Btudes nouvelles de dermatologie: les tumeurs de la peau. 2 I n * article. Les
Dermatomyomes (Fibromyomes, Liomyomes, ou Myomes CutanCs) , Ann. de dermat. et syph. ZIne sCr. 1: 25, 1880.

SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 465
BESNIER, E. : Contribution i l'histoire des myBmes cutanCs. DermatomyBmes, LiomyBines
DE BIASE, F., AND BIGATTI, A.: Dermatomiomas cutaneos a disposicicin zoniforme del hombro
BOGOLUBOFF, W.: Myomes multiples de la peau, Chirurgia, 1907. Abst. by Abramson, 1933. BOGROFF: Klinitschiskaja Med. M. 56: 38, 1022. Abst. in Zentralbl. f . Haut- u.
BRICIDI, V., AND MARCACCI, G.: Dei miomi cutanei, Imparziale 21: 545 and 577, 1881. See
BROLEMANN: Ein Fall von multiplen Dermatomyomen, Arch. f . Dermat. u. Syph. 70: 163,
BRUHNS, C. : Zur Kenntnis der Dermatomyome, Dermat. Wchnschr. 87/2 : 1344, 1928. BURNIER AND BLOCH, M.: Un cas de liomyomes multiples cutanks, Bull. SOC. franc. de
CANNON, A. B.: Multiple leiomyomas, Arch. Dermat. and Syph. 24: 498, 1931. CAROL, W. L. L.: Myomatosis cutis disseminata, Nederl. Tijdschr. v. Geneesk. 65': 1394,
COLE, H. N., AND DRIVER, J. R.: A case for diagnosis (leiomyoma?), Arch. Dermat. and
CORSI, H.: Leiomyoma cutis multiplex, Proc. Roy. SOC. Med. 22: 1393, 1929. COVISA. J. S.: Los miomas cutineos, Actas dermo-sif. 22: 760, 1930. CROCKER, H. R.: A case of myoma multiplex of the skin, Brit. J. Dermat. 9 : 1, 1897. DOBRONRAVOV, V. N.: Zur Kasuistik der multiplen Leiomyome der Haut, Venerol. i dermat.
6: 3 8 4 6 , No. 10 (abst. in German, p. 47), 1929; Zentralbl. f . Haut- u. Geschlechtskr. 34: 325, 1930.
de la peau, Ann. de dermat. et syph. 2me sbr. 6: 321, 1885.
y brazo izquierdos, Semana mCd. 2 : 208, 1935.
Geschlechtskr. 9: 430, 1924.
also Julien.
1904.
dermat. et syph. 28: 24, 1921.
1921. Abst. in Zentralbl. f. Haut- u. Geschlechtskr. 3: 167, 1922.
Syph. 23: 168, 1931.
DORE AND MORRIS, M.: Myoma multiplex cutis, Brit. J. Dermat. 14: 55, 1902. DOWLING, G. B.: Leiomyoma cutis, Proc. Roy. SOC. Med. 20: 564, 1927. DUHRING, L. A,: Case of painful neuroma of the skin, Am. J . M. Sc., n.s. 66: 413, 1873. ENCEL, E. A,: Un caso di leiomioma cutaneo multiplo, Gior. ital. d. mal. ven. 47: 728, 1912. FINNERUD, C. W.: Leiomyoma cutis, Med. Clin. North America 13: 445, 1929 (Sept.). Frocco: Leiomiomi multipli dolorosi degli arti, Gior. ital. della mal. ven. 65: 1566, 1924. FTSCHER: Ein Fall von multiplen Myomen der Haut, Cluj. med. 2 : 143, 1921.
FISCHER, KL.: Myomatosis cutis, Zentralbl. f . Haut- u. Geschlechtskr. 30: 180, 1929. Fox, C.: Myomata, Brit. J. Dermat. 14: 56, 1902. FRITZ, W.: Fall von Hautmyomen, Arch. f . Dermat. u. syph. 96: 89, 1909. FRITZ, W.: Zwei Falle von multiplen Cutismyomen, Arch. f . Dermat. u. Syph. 99: 45, 1910. FROST, K. P.: A case of multiple cutaneous leiomyoma, J. A. M. A. 83: 906, 1924. FRUHWALD, R.: Multiple Leiomyome der Haut, Zentralbl. f . Haut- u. Geschlechtskr. 15:
GALEWSKY: Demonstr. multipl. Dermatomyome, Arch. f . Dermat. u. syph. 82: 284, 1906. GANS, 0. : Myoblastoma cutis (Cutismyome), in Histologie der Hautkrankheiten, Berlin,
GARIBALDI, G. M.: Un caso di leiomiomi multipli della cute. Contributo clinico ed istolo-
GENEVOIS, E.: Contribution i 1'Ctude des myBmes cutanCs, Thkse de Lyon, 1905. GOLDSMITH, W. N.: A case of leiomyoma, Brit. J. Dermat. & Syph. 44: 211, 1932; also in
GOUGEROT AND ELIASCHEFF, 0. : Dermatomyomes dermiyues multiples des membres, Bull.
GRAHAM-LITTLE, E.: Leiomyoma cutis, Proc. Roy. SOC. Med. 24: 1021, 1931. GUTMANN, C.: Zur Kenntnis der multiplen Dermatomyome, Dermat. Ztschr. 13: 469, 1906.
Patient mit multiplen cutanen Dermatomyomen, Deutsche med. Wchnschr. 32 : 407, 1906.
Abst. in Zentralbl. f . Haut- u. Geschlechtskr. 5: 31, 1922.
410, 1925; 18: 523, 1926.
1928, vol. 2 , p. 439.
gico, Arch. ital. di dermat. sif. 1: 213, 1925.
Proc. Roy. SOC. Med. 2 5 : 672, 1932.
SOC. franc. de dermat. et syph. 3;: 577, 1930.
HACEN: Dermatomyome, Zentralbl. f . Haut- u. Geschlechtskr. 21: 685, 1926. HACENA, G.: Weitere Beitrage zur Kasuistik der multiplen Leiomyome der Haut, Dermat.
Wchnschr. 80: 673, 1925.

466 ARTHUR PURDY STOUT
HARDAWAY, W. A.: Report of a case of multiple myomata of the skin accompanied by severe pain; with remarks (read Am. Dermatological Assoc., August 27 , 1885), Am. J. Med. Sc. 91: 511, 1886.
HARDAWAY, W. A.: A further report of a case of multiple myomata of the skin, J. Cutan. Dis. 2 2 : 375, 1904.
HEIDINGSFELD, M. L.: Myomata cutis, J. A. M. A. 48: 562, 1907. HELLMANN : Dermatomyome, Zentralbl. f. Haut- u. Geschlechtskr. 4 : 100, 1922. HESS, K.: Ein Fall von multiplen Dermatomyomen an der Nase, Virchow's Arch. f . path.
HOPKINS: Myoma, Arch. Dermat. & Syph. 21: 871, 1930. HUBSCHMANN, K.: Diagnosis of multiple dermatoleiomyoma, Ceskb dermat. (supp.) 12 :
HUGENBRUCH: Multiple Leiomyome, Diss. Koln, 1919/1920, 1921. HULDSCHINSKY : Ein Beitrag zur Kenntniss des multiplen Dermatomyome, Freiburg. Inaug.
HYDE, J. E.: A Practical Treatise on Diseases of the Skin, Philadelphia, Lea and Febiger,
JACOBI: Vorstellung eines Falles von multiplen Dermatomyomen, Miinchen med. Wchnschr.
JADASSOHN, J.: Zur Kenntniss der multiplen Myome der Haut, Virchow's Arch. f . path.
JADASSOHN, J.: Dermatomyome, Zentralbl. f . Haut- u. Geschlechtskr. 29: 608, 1929. JAMIN, F.: Ein Fall von multiplen Dermatomyomen, Deutsche Arch. f . klin. Med. 70: 468,
JARISCH, A. : Demonstration eines Falles von multiplen Leiomyomen der Haut, Dermat.
JULIEN: Des myomes cutanks par Vincenzo Brigidi et Giorgio Marcacci, Ann. dermat. et
RISSMEYER: Tilfaelde af multiple myomer (Leiomyomata) i Huden, Hospitaltid. 65 derm.
KLEINSORG, H.: Ein Fall von multiplen Dermatomyomen, Diss. Bonn, 1917. KOSINSKI: Neuroma multiplex: Heilung durch Neurektomie, Centralbl. f . Chir. 1 : 241,
KO~EVNIKOV, P., AND KRAPIRNA, s.: Zahlreiche Leiomyome in der Haut, Med. Mysl' (russ.)
KREIBICH: Naevus leiomyomatosus, Zentralbl. f . Haut- u. Geschlechtskr. 32 : 677, 1930. KRETZMER, E . : Ein Beitrag zur Kenntnis der multiplen Dermatomyome (Kutismyome),
Arch. f . Dermat. u. Syph. 107: 379-386, 1911. KRZYSZTALOWICZ, F. : Przypadek licznych milinikbw skbry (myomata. cutis multiplicia),
Przegl. lek. Krakbw 44: 657, 1905. Abst. in Monatsch. f . prakt. Dermat. 42: 304, 1906. LIEBER, K.: Uber die Myome der Haut, Beitr. z. path. Anat. u. z. allg. Path. 60: 449, 1915. LITTLE, G.: A case of myoma cutis, Brit. J. Dermat. 17: 265, 1905. LOUSTE, L~vY-FRANCKEL AND CAILLIAU : Dermatomyomes a disposition systkmatiske, Bull.
LUKASIEWICZ, W.: Ueber multiple Dermatomyome, Arch. f . Dermat. u. Syph. 24: 33, 1892. MACLEOD, J. M. H.: Case of multiple leiomyoma of the skin, Proc. Roy. SOC. Med. (Dermat.
v. MARS CHALK^, T.: Zur Kenntnis der multiplen Hautmyome, Monatschr. f . prakt. Dermat.
v. MARS CHALK^, T.: Multiple Dermatomyome, Arch. f . Dermat. u. Syph. 72 : 252, 1904. MEIROWSKY, E.: Hautmyome, Zentralbl. f . Haut- u. Geschlechtskr. 24: 577, 1927. MILLER, H. E.: Leiomyoma, Arch. Dermat. & Syph. 2 2 : 135, 1930. MORRIS, M.: Case of multiple myoma, Brit. J. Dermat. 13: 8, 1901. MORROW, MILLER, AND TAUSSIG: Leiomyoma, Arch. Dermat. & Syph. 21: 682, 1930. NEUMANN: Ueber multiple Dermatomyome, Arch. f . Dermat. u. Syph. 39: 3, 1897. NOBL, G.: Myomatosis cutis disseminata, Arch. f . Dermat. u. Syph. 79: 31, 1906. NOMLAND: Leiomyoma, Arch. Dermat. & Syph. 20: 121, 377, 1929.
Anat. 120: 321, 1890.
464, 1931.
Diss., 1901.
3d Ed., 1888, p. 463.
47: 630, 1900.
Anat. 121: 88, 1890.
8th Ed., 1909, p. 566.
1901.
Ztschr. 2: 609, 1895.
syph. 2"le sbr. 3 : 119, 1882.
sec.: 65, 1922. Abst. in Zentralbl. Haut- u. Geschlechtskr. 8 : 261, 1923.
1874.
5: 66. 1928. Abst. in Zentralbl. f . Haut- u. Geschlechtskr. 29: 513, 1929.
SOC. franc. de dermat. et syph. 39: 395, 1932; ibid. 40: 699, 1933.
Sect.) 1: 50, 1907-08; also in Brit. J. Dermat. 20: 84, 1908.
31: 313, 1900.

SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 467
OLESSOV: Multiple generalisierte Dermatomyome, Zentralbl. f . Haut- u. Geschlechtskr. 26 :
OLIVER, FINNERUD, A N D ZEISLER: Leiomyoma, Arch. Dermat. & Syph. 19: 508, 1929. ORMSBY, 0. S.: Leiomyoma cutis, Arch. Dermat. & Syph. 11: 466, 1925; ibid. 2 2 : 172, 1930. ORMSBY, 0. S., AND MITCHELL: Leiomyoma, Arch. Dermat. & Syph. 8: 581, 1923; 9: 656,
OTHAZ, E. L.: Dermatomiomas, Semana mCd. 1 : 1130, 1933. PASINI, A.: A proposito di un caso di mioma angiocavernoso, Gior. ital. delle mal. ven.
PEYRI, J.: Leiomyomatosis cutis. Dermalgia paroxystica, Actas dermosif. 6: 289, 1915.
PHOTINOS, P.: Les myomes de la peau. Etude clinique et histologique i l'occasion du
PRINGLE, J. J.: Case for diagnosis, Brit. J. Dermat. 10: 163, 1898. RACUSIN: Revista dermat. 7: 203 (1930?). RIEGEL, A. : Pi-ispsvek ku kasuistice vzLcnLch nidorfi. Myoma laevicellulare multiplex
ROBERTS, L.: Notes for the study of superficial cutaneous myomata, Brit. J. Dermat. 12:
ROTH, A.: Leiomyoma multiplex dorsi esete, Derm. urol. sek. Budapest Kongs. 1908, 24
RUSCH: Multiple Leiomyome, Zentralbl. f. Haut- u. Geschlechtskr. 35: 32, 1931. SANNICANDRO, G. : Miomi cutanei multipli eruttivi con particularit& cliniche ed istologiche
SASAKAWA, M.: A case of myoma cutis multiplex, Japanese J. Dermat. & Urol. 2 5 : 44, 1925. SATO KUNIO: Multiple Leiomyoma, Japanese J. Dermat. & Urol. 2 7 : 4, 1927. Quoted by
SAVATARD, L.: Leiomyoma, Brit. J. Dermat. 32: 229, 1920. SCADUTO, G.: Dermatomioma della faccia guarito coi raggi X, Policlinico 18 (sez. prat.):
SCHLAMMADINGER, J. : Leiomyosarcoma cutis mit Acanthosis nigricans vergesellschaftet,
SCHOLTZ, M.: Multiple cutaneous leiomyomas. Report of a case, Arch. Dermat. & Syph.
S E G R ~ , G.: Un caso di dermatomiomi multipli, Gior. ital. delle ma1 ven. 47: 300, 1912. SEQUEIRA, J. H.: Case of leiomyoma, Brit. J. Dermat. 26: 331, 1914. SEQUEIRA, J. H. : Case -of leiomyoma (?Epitheliomatous), Proc. Roy. SOC. Med. (Dermat.
SIMONS, A.: Zur Kenntnis der multiplen Cutismyome, Ztschr. f . Krebsforsch. 18: 209, 1921. SMILOVICI, J. : tfber Cutismyome und Keloidbildung im Bereiche einer Acrodermatitis
SOBOTKA, P. : Klinische, histologische und vergleichende Beitrage zur Kenntnis der Cutis-
SOBOTKA, P.: Zur Kenntnis der Myome der Kutis und der Subkutis, Arch. f . Dermat. u.
SPILLMANN, L., A N D MICHON, P.: Les myomes cutanks, Ann. de dermat. et syph. 6"" sCr. 5:
STAVIANICEK, F.: Multiple Myome der Penis, Ztschr. f . Urol. 7 : 635, 1913. STREMPEL: Dermatomyome, Arch. f. Dermat. u. Syph. 155: 322, 1927. STUMPKE: Dermatomyome, Zentralbl. f . Haut- u. Geschlechtskr. 5: 438, 1922. TILP, A.: Multiple Myombildung in Magendarmkanal und in der Haut, Centralbl. f . allg.
TRIMBLE: Dermatomyoma, Arch. Dermat. & Syph. 5: 830, 1922. ULLMANN, K.: Multiple Leiomyome, Arch. f . Dermat. u. Syph. 119/1: 151, 1914. VERNEUIL: Tumeurs cutanCes, Bull. SOC. anat., Paris 33 (Zme sCr. 3 ) : 373, 1858. VIRCHOW, R. : Ueber cavernose (erectile) Geschwiilste und Telangiektasien, Virchow's Arch.
37, 1928.
1924.
41: 588, 1906. Abst. in Monatschr. f. prakt. Dermat. 44: 614, 1907.
Abst. in Dermat. Wchnschr. 62: 78, 1916.
premier cas observC en Grbce, Bull. SOC. franc;. de dermat. et syph. 40: 623, 1933.
cutis reg. mamillae dextrae, Sborn. lCka?sk$ 4, 327, 1891.
115, 1900.
Febr. Dermat. Jarhresbericht 4: 245 and 252, 1908.
sinora non descritte, Dermasifilografo 8: 569, 618, 1933.
Photinos, P.
173, 1911,
Dermat. Wchnschr. 99: 1257, 1934.
10: 173, 1924.
sec.) 7: 261, 1913-1914.
chronica atrophicans, Arch. f. Dermat. u. Syph. 124: 77 , 1917.
myome, Arch. f . Dermat. u. Syph. 89: 209-234, 323-354, 1908.
Syph. 116: 79, 1913.
193, 1924.
Path. u. path. Anat. 18: 769, 1907.
f . path. Anat. 6: 525, 1854.

468 ARTHUR PURDY STOUT
WEISSENBACH, R. J., CARLU, L., AND MARTINEAU, J.: Myomes cutanCs multiples.
WHITE, C. J.: Liomyoma cutis, J. Cutan. Dis. 17: 266, 1899. WHITFIELD: Multiple myoma cutis, Brit. J. Dermat. 1 7 : 267, 1905. WIESINCER: Fibromyome, Arch. f . Dermat. u. Syph. 112: 411, 1912. WOLTERS, M. : Ueber multiple Myome der Haut, Arch. f . Dermat. u. Syph. 25: 413, 1893
WOSYKA, H. : Leiomyoblastoma cutis multiplex in segmentarer Anordnung, Dermat. Wchn-
ZINSSER: Vorstellung eines Falles von multiplen Leiomyomen der Haut, Miinchen med.
Trait- ment par 1’Clectro-coagulation, Bull. SOC. franq. de dermat. et syph. 41 : 1963, 1934.
(Supp.1.
schr. 99: 1110, 1934.
Wchnschr. 66: 733, 1919.
MISCELLANEOUS
BISSET, C.: A case of extraordinary irritable sympathetic tumor, Memoirs Med. SOC. London
BLAND-SUTTON, J.: Notes on some unusual cases of tumours: a curious pedunculated tu-
BORST, M.: Die Lehre von den Geschwiilsten, Wiesbaden, J. F. Bergmann, 1902, 1: 222-
BOETTCHER, A.: Myom einer vena ulnaris, Virchow’s Arch. f . path. Anat. 47: 372, 1869. CERNEZZI, A.: Fibroleiomioma di una vena del plesso spermatic0 posteriore, Gazz. d. osp.
CHANDELUX, A. : Recherches histologiques sur les tubercules sous-cutanCs douloureux, Arch.
CHEVALIER: Thkse de Lyon, 1900. CZERNY, V. : Eine Elephantiasis Arabum congenita mit plexiform Neuromen, Arch. f . klin.
DIETEL, F.: Myoma (myoblastoma cutis), in Handbuch der Haut- u. Geschlechtskr. 12/2,
DRENNAN, M. R.: A fibro-myoma in hernial sac, J. M. A. South Africa 4: 692, 1930. F E R N ~ N D E Z , A., AND MONSERRAT, J. L. E.: Nbdulos doloros de la oreja (Tumor glbmico;
neuro-mio-angioma), Semana mCd. 2 : 1693, 1931. GATTER, G.: Zwei Falle von seltenen Geschwulsten am ausseren Genitale, Zentrnlbl. f .
Gynak. 50: 2769, 1926. GERY, L., AND PILATE: Myome de la cuisse, Bull. et mCm. SOC. anat., Paris 89 (6Ine sCr. 16) :
288, 1919. v. HABERER AND POMMER: Bericht iiber den in letzten Sitzung Vorgestellten Mamma-tumor
und Demonstration des Praparates, Wien. klin. Wchnschr. 2 7 : 962, 1914. HOEPKE, H.: Die Haut in Mollendorff’s Handbuch der mikroskopischen Anatomie des
Menschen, Julius Springer, Berlin, 1927. 111/1, pp. 39-41. JOSEPH, M.: Myome, in Mracek’s Handbuch der Hautkrankheiten 3: 588, 1904. KLOB, M.: Path. Anat. d. weib. Sexualorg., Wien, 1864, p. 492. LEWANDOWSKY, M.: Wirkung des Nebennieren extractes auf die glatten Muskeln der Haut,
LINDFORS, A. 0. : Ueber primare Geschwiilstbildungen der Brustwarze und des Warzenhofs,
MARRI, P.: Sopra un caso di fibroleiomioma della vena ascellare, Arch. ital. di chir. 17: 249,
MELNICK, P. J.: Fibromyoma of breast, Arch. Path. 14: 794, 1932. MITTERSTILLER, S. : Ein Fall von Mammasarkom beim Mann (mit Bemerkungen zur Frage
des Myosarkoms), Deutsche Ztschr. f . Chir. 134: 446, 1915. MOST, A.: Tubercula dolorosa, Beitr. z. klin. Chir. 136: 252, 1926. MUCCI, D., AND PROTTI, G. : Considerazioni sopra un caso di fibrolejomioma (perivascolare)
del piccolo obliquo dell’addome, Tumori 11: 238, 1924. MijLLER, HEINRICH : Uber ein generalisiertes Rhabdomyoblastom der Haut und iiber Stel-
lung der Myoblasten zu den eosinophilen Leukocyten, Zentralbl. Haut- u. Geschlechtskr. 34: 404. 1930.
3: 58, 1792.
mour of the nipple, Practitioner n.s. 6: 460, 1897.
223.
24: 1542, 1903. Abst. in Miinchen med. Wchnschr. 51: 676, 1904.
de physiol. norm. et path., 2me sCr. 9 : 639, 1882.
Chir. 17: 357, 1874.
Berlin, 1932, p. 199.
Centralbl. f . Physiol. 14: 433, 1900.
Monatschr. f . Geburtsh. u. Gynak. 11: 763, 1900.
1927.

SOLITARY CUTANEOUS AND SUBCUTANEOUS LEIOMYOMA 469
M ~ L L E R , HUGO: Fast universelles Rhabdomyoma cutis, Zentralbl. f. Haut- u. Geschlechtskr. Fall zur Diagnose, Zentralbl. f . Haut- u. Geschlechtskr. 32: 174, 1930.
MUSCATELLO, G. : Ueber die angeborenen Spalten des Schidels und der Wirbelsaule, Arch.
NATALI, C.: Su di un caso di fibroleiomioma della vena femorale, Tumori 10: 224, 1923. NICOLAS, J., MASSIA, G., AND COLAS, J.: Nouveau cas de nodule douloureux de l’oreille,
NORA AND KOGAN: Myome de l’urhtre fCminin, J . d’urol. 27: 431, 1929; Bull. SOC. franc.
OTTOW, B. : Zur Kenntnis der gestielten Fibromyome der weiblichen Harnrorhe, Zentralbl.
PERACCHIA, G. C. : Fibrolejomioma della parete del grande obliquo dell’addome, Ann. ital.
POLLAND, G.: Ein Naevus mit quergestreiften Arrectores piloruni, Arch. f . Dermat. u.
RIBBERT, H. : Geschwiilstlehre, Bonn, 1904, p. 3 15. RINDFLEISCH, E. : A Text-book of Pathological Histology, Philadelphia, Lindsay and Blakis-
(Trans. of the 2d German edition Lehrbuch der pathologischen
SAALFELD, U. : Zur dermatologischen Statistik (unter besonderer Beriicksichtigung der Reck-
SAALFELD, E., AND SAALFELD, U. : Die Hautmyome, Handbuch der Haut- u. Geschlechtskr.,
SANDELIN, T . : Ett fall av myom, sannolikt utgiende f r ln ligamentum vesico-umbilicale,
SCHAUDER, H.: Uber Leiomyome der Brustdriise, Deutsch. Ztschr. f . Chir. 205: 58, 1927. SCHUSSLER, H.: Die Myome des Samenstranges, Deutsch. Ztschr. f . Chir. 135: 268, 1916. SPECIALE, F.: Un caso di sarcoma della guaina vascolare del collo, Policlinico {sez. prat.)
STOKES, J. H.: Nevus pilaris with hyperplasia of non-striated muscle, Arch. Dermat. &
STRONG, W. L.: Leiomyoma of the breast, Am, J, Obst. & Gynec. 68: 53, 1913. TOURAINE, A., SOLENTE, AND RENAULT, P.: Tumeurs glomiques multiples du tronc et des
membres, Bull. SOC. franc. de dermat. et syph. 43: 736, 1936. UNNA, P. G. : Die Histopathologie der Hautkrankheiten, in Orth, J. : Lehrbuch der speciellen
pathologischen Anatomie, Erganzungsbd. I1 Theil, pp. 863-866, Berlin, A. Hirschwald, 1894.
32: 26, 1930.
f . klin. Chir. 47: 203, 1894.
Bull. SOC. franq de dermat. et syph. 43: 1437, 1936.
d’urol. 8: 146, 1929.
f . Gynak. 45: 360, 1921.
di chir. 2 : 1279, 1923.
Syph. 109: 497, 1911.
ton, 1872, p. 313. Gewebelehre, W. Engelmann, Leipzig, 1867-69, pp. 324-325.)
linghausenschen Krankheit und der Myome), Dermat. Ztschr. 52 : 399, 1928.
vol. 12/2, Berlin, 1932, p. 55.
Finska Lak.-Sallsk. Handl. 66: 123, 1924.
33: 761, 1926.
Syph. 7: 479, 1923.
VIDAL, E. C.: Myoma, J. Cutan. Diseases 3: 260, 1885. V. WINIWARTER, A.: Die chirurgischen Krankheiten der Haut, Deutsch. Chir., Lief. 23,
Stuttgart, 1892, p. 581. WINKLER, K. : Myoplastische Sarkome, Handbuch d. Haut- u. Geschlechtskr. 12/3: 793-
95, 1933. WOOD, W.: On painful subcutaneous tubercle, Edinburgh M. & S. J. 8: 283, 1812. Further
observations on painful subcutaneous tubercle, Edinburgh M. & S. J. 8: 429, 1812. Observations on painful subcutaneous tubercle with cases and histories of the disease, Tr. Medico-Chirurg. SOC. Edinburgh 3 : 317, 1829.
WORINGER, FR. : Myomes, in Nouvelle Pratique Derniatologique, publike par mm. Darier Sabouraud, Gougerot, Milian, Pautrier, Ravaut, SCzary, ClCment Simon, Masson e t Cie, Paris, 1936, vol. 6, pp. 605-610.
ZURHELLE, E. : Das myoplastiche Sarkom (myoma sarcomatosum), Handbuch d. Haut- u. Geschlechtskr. 12/3: 843, 1933.