the 8 “must haves” for perinatal safety - 2014
TRANSCRIPT
The 8 “Must Haves” For Perinatal Safety - 2014
Larry Veltman, MD
HASC Perinatal Safety Tract
March 11, 2014

What’s Coming: Accountability
• The public expects it
• Your hospital expects it
• The payers expect it

Think about your organization’s biggest perinatal challenges

Here are 8 essentials, “must haves”, to meet and overcome these
challenges

8 “Must Haves”
• Overarching 1. Work toward high reliability - the culture of safety 2. Establish and grow physician champions
• Fetal monitoring 3. Implement the fetal monitoring bundle
• Reduce Cesarean deliveries in NTSV 4. No cervical ripening for elective inductions 5. Ensure an adequate trial of labor
• Reduce EED < 39 weeks 6. Establish/maintain the infrastructure of scheduling inductions and the hard
stop
• Proactive evidence-based, policies, procedures, practices, and accountability
7. Fetal Compromise– oxytocin, tachysystole, resuscitation, signal ambiguity 8. Maternal conditions– post partum hemorrhage, hypertension

1. High Reliability

Characteristics of HROs
1. Safety oriented culture
2. Operations are a team effort; flattened hierarchy
3. Communications are highly valued; civility rules
4. Always prepared for the unexpected
5. Multidisciplinary review of near- misses and adverse outcomes
6. The “top brass” endorses the culture and provides the resources to make it work

Safety Oriented Culture
• Protocols
• Checklists
• Redundancy
• Simplification
• Standardization - reduced variability
• Attention to human factors
• Accountability

2. Physician Champions
What’s a Physician Champion?
Primary Characteristics Has a wide peer and social network and an extensive knowledge of how his/her
colleagues interact with each other Perceived as credible and is respected by peers Highly knowledgeable and stays connected to his/her area of expertise through a
variety of sources Willing to share knowledge with others Willing to support and advocate for process changes Willing to implement new guidelines and serve as a resource for others Easy to talk to or deal with, welcomes contact by others, makes time to attend to
their issues and shows an interest in their views Is flexible and controlled in the face of stress, leading others by example Is not afraid to speak his/her mind or of trying to influence others, but does so in a
way that respects the personal boundaries of others
(www.hsag.com/App_Resources/Documents/Physician_Potential_G.doc)

What’s a Physician Champion?
Secondary Characteristics Able to defend self against aggressive incursions and foster self-control and
respect in others Able to discern mutual goals beyond apparent differences in order to build
consensus among opposing parties Holds that all people should be treated as equals Recognizes, perceives, and directly relates to the emotions of others Communicates truthfully and does not withhold relevant information Shows appreciation for the efforts and contributions of others Follows through with duties and takes the time necessary to get the job done
correctly Able to wait patiently and recognizes the importance of “timing” when initiating
change
(www.hsag.com/App_Resources/Documents/Physician_Potential_G.doc)

If You Don’t Have One, Make One!

3. Fetal Monitoring Bundle
Fetal Monitoring Bundle
1. A Credentialed Staff
2. An Escalation Policy
3. A Known and Available Responsible Party
4. Capability for Rapid Response

Yale Department of OB/GYN: Credentialing
“All medical staff and employees responsible for fetal monitoring interpretation (resident and attending obstetricians, midwives, and labor room and antepartum nurses) were obligated to take this examination within 1 year of employment and pass within 18 months.”
(Pettker CM, Thung SF, Norwitz ER, et al. Impact of a comprehensive patient safety strategy on obstetric adverse events.
Am J Obstet Gynecol 2009;200:492.e1-492.e8.):

A New Approach: Script Concordance Testing
Is It Really Fetal Distress? Category II Tracings

The Basic Question:
• What is the likelihood of the fetus developing significant acidemia prior to delivery?
• Moderate variability or accelerations = absent fetal acidemia at the point of observation
• 16 footnotes – must be read – E.g., Treat minimal to absent variability as one
entity.

Escalation Policy Chain of Command
Communication issues that cannot be solved
Charge Nurse
Nursing manager
Medical staff leader
Department Chair
Contacts physician Executive committee
Credentials committee
QA committee
Board of Trustees

The Responsible Party
• Any hospital providing an obstetric service should have the capability of responding to an obstetric emergency.
• The required personnel, including nurses, anesthesia personnel, neonatal resuscitation team members, and obstetric attendants, should be in the hospital or readily available.
Guidelines for Perinatal Care, 7th Edition, 2012

The Responsible Party: Stay Connected

Assuring The Rapid Response

4. Reduce Cesarean Delivery for NTSV – Failed Nulliparous Inductions
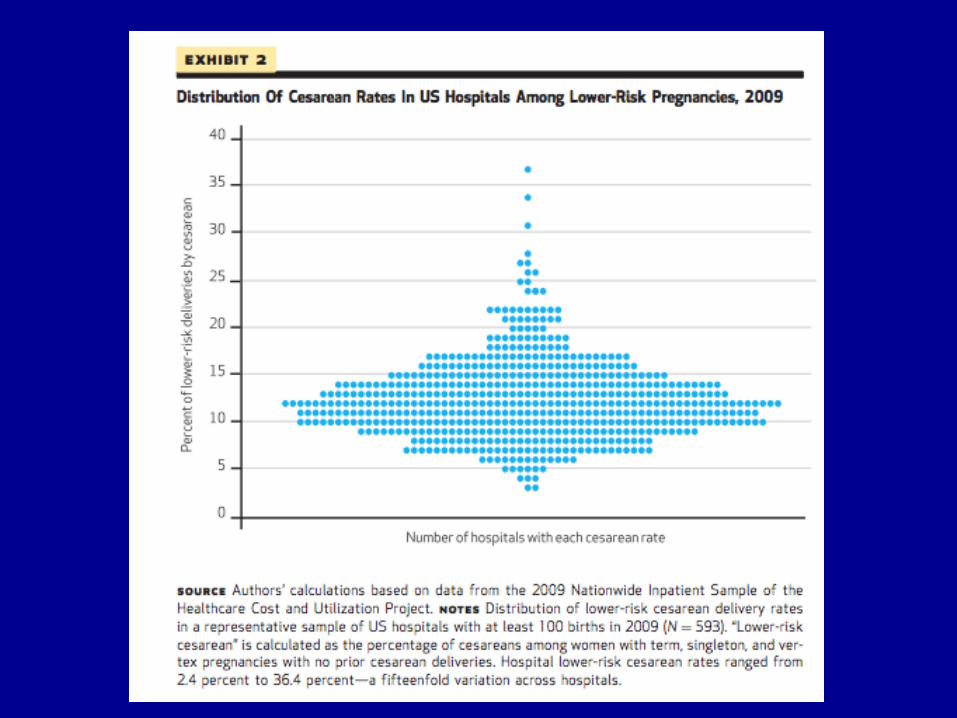

Clark, AJOG, Feb, 2009
Cervical “Ripeness” and Cesarean Rate

Nulliparous Cesarean Rate
With Cervical Ripening
47.1 %
Without Cervical Ripening
26.9 %

5. Reduce Cesarean Delivery for NTSV – Adequate Trial of Labor


CONCLUSION: “The active phase of labor may not start until 5 cm of cervical dilation in multiparas and even later in nulliparas. A 2-hour threshold for diagnosing labor arrest may be too short before 6 cm of dilation, whereas a 4-hour limit may be too long after 6 cm.” (Zhang, et al., Obstet Gynecol 2010;115:705–10)
Six Is The New Four


Induced Labor

MFMU Network
Conclusion: “Almost 40% of the women who remained in the
latent phase after 12 hours of oxytocin and membrane rupture were delivered vaginally.
Therefore, it is reasonable to avoid deeming labor
induction failure in the latent phase until oxytocin has been administered for at least 12 hours after membrane rupture.” (Obstetrics and Gynecology 2011;117:267-72)

6. EED < 39 weeks
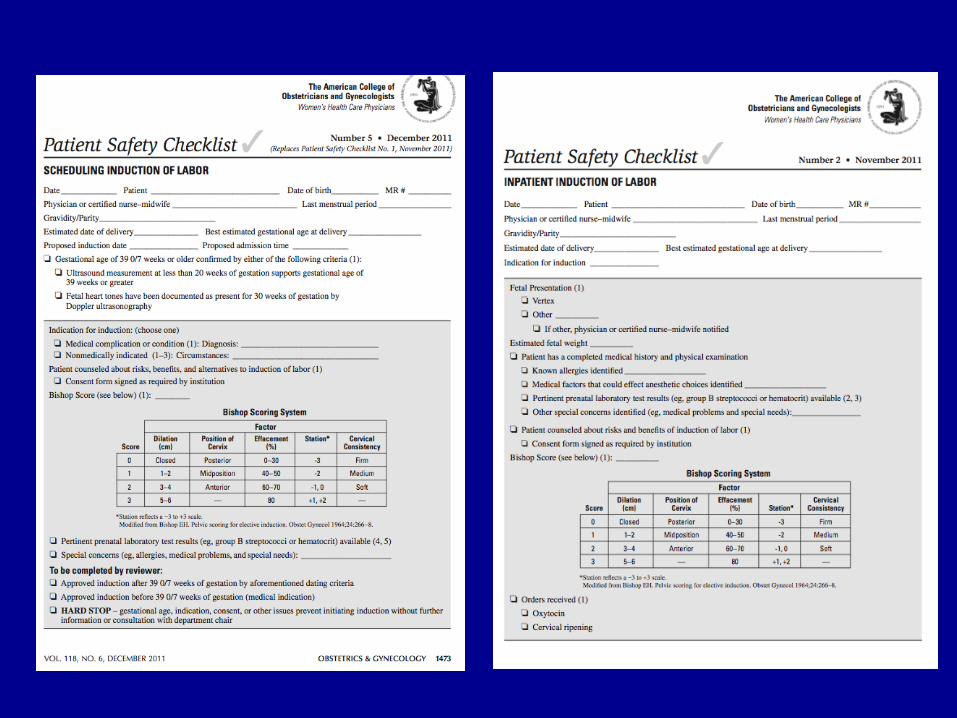

PSTV Elective Inductions Include:
• Post dates < 41 weeks • Macrosomia without documented previous shoulder dystocia • AFI > or equal to 6 • History of fast labors • Prodromal or impending labor • Previous maternal pelvic floor injury (e.g., 4th degree laceration) • Psychosocial issues
– Husband out of town – Family in town – Maternal exhaustion or discomforts – Psychiatric issues (anxiety or depression) – Physician convenience – Adoption/surrogacy

“Hard Stop” “Soft stop” Peer review
Education only

7. Fetal Compromise

“Turn Up The Pit!”
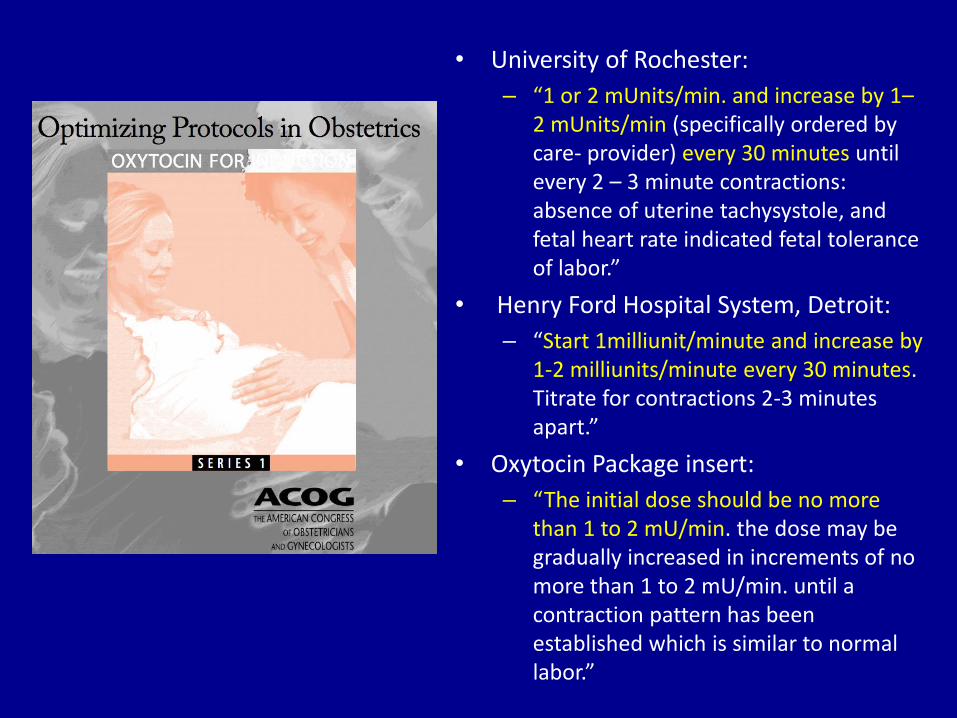
• University of Rochester:
– “1 or 2 mUnits/min. and increase by 1– 2 mUnits/min (specifically ordered by care- provider) every 30 minutes until every 2 – 3 minute contractions: absence of uterine tachysystole, and fetal heart rate indicated fetal tolerance of labor.”
• Henry Ford Hospital System, Detroit:
– “Start 1milliunit/minute and increase by 1-2 milliunits/minute every 30 minutes. Titrate for contractions 2-3 minutes apart.”
• Oxytocin Package insert:
– “The initial dose should be no more than 1 to 2 mU/min. the dose may be gradually increased in increments of no more than 1 to 2 mU/min. until a contraction pattern has been established which is similar to normal labor.”

Standardize Approach to Tachysystole
ACOG PB, Nov 2010

NRP 2012
Intubation (Guidelines for Perinatal Care)

Resuscitation: The List
• Any FHR concerns • Prematurity • Fetal malpresentation (e.g., breech) • Multiple pregnancy • Any operative vaginal delivery • Meconium stained amniotic fluid • Any significant fetal anomaly • Concerns about a potential shoulder dystocia (e.g. previous
shoulder dystocia, macrosomia) • Significant maternal medical conditions (e.g., eclampsia,
thyroid storm, diabetic ketoacidosis) • Any additional concerns by the obstetrician, labor and
delivery nurse or resident. • Note that any member of the obstetrical team with a concern
can call for the neonatal resuscitation team.
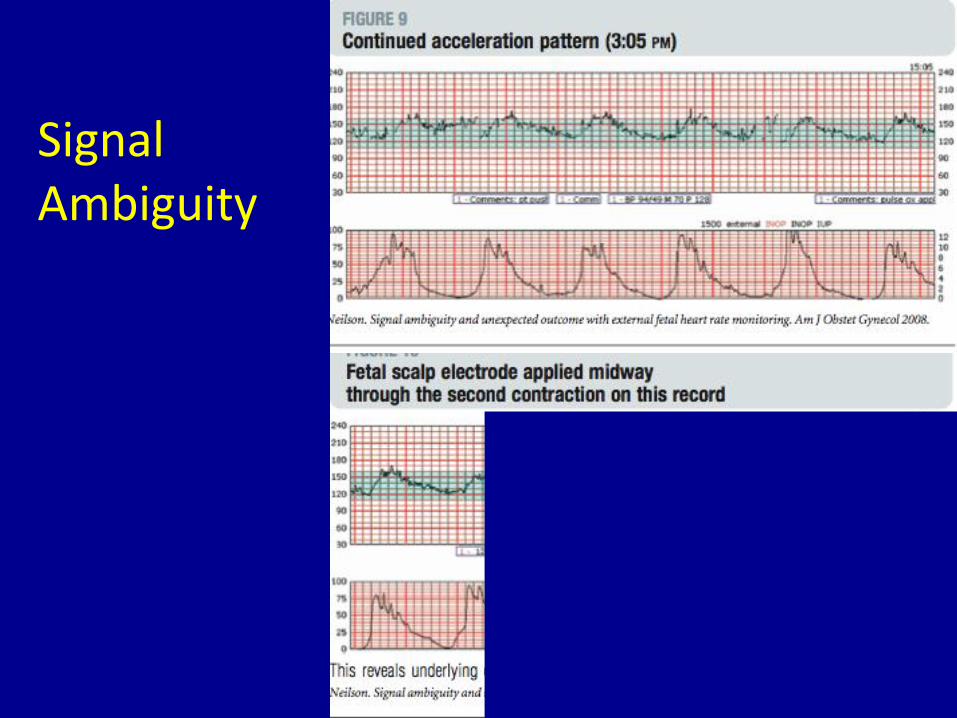
Signal Ambiguity

8. Maternal Emergencies – Post Partum Hemorrhage / Hypertension
Obstetrics and Gynecology, February, 2012





2014
