texas mental health systems transformation and the texas
TRANSCRIPT

Texas Mental Health Systems Transformation and the Texas CANS: implementing TCOM
Marisol Acosta, MEd, LPC-S, Interim Manager of Child and Adolescent ServicesBehavioral Health Services, Health and Human Services Commission
Angela Hobbs-Lopez, D.O., Independent Consultant
October 5, , 2017 TCOM Conference 2017, San Antonio Texas

Objectives
1.Provide an overview of how the children mental health delivery system was redesign using the CANS and TCOM model as the core element of its redesign into the Texas Resilience and Recovery (TRR).
2. Describe the Texas Child and Adolescent Needs and Strengths assessment
3. Discuss lessons learned, barriers/challenges of the implementation of the Texas CANS and the behavioral health system redesign.

Brief Overview of Children’s Community Mental Health in Texas
• Community Mental Health Services for all 254 counties
• Children’s mental health services are currently provided by 39 Local Mental Health Authorities (LMHAs)
• 61,117 children and youth served in fiscal year 2015

Brief Overview of Children’s Community Mental Health in Texas
Children’s Mental Health Service Criteria
Children’s Mental Health serves children ages 3 through 17 with serious emotional disturbance (excluding a single diagnosis of substance abuse, intellectual or developmental disability or autism) who have a serious functional impairment or who:
• Are at risk of disruption of a preferred living or child care environment due to psychiatric symptoms; or
• Are enrolled in special education because of serious emotional disturbance.
Brief Overview of Children’s Community Mental Health in Texas
What are provided for children and their families that are eligible?
Screening
Assessment
Services
Brief Overview of Children’s Community Mental Health in Texas
Funding
• Medicaid
• Texas General Revenue
• SAMHSA Mental Health Block Grant

Unmet Need for Community Mental Health Services
7
(7.0% of total Texas Youth, aged 9 – 17)
Youths Served below 200% FPL
Youth SED Population below 200% FPL
Total Youth SED Population in Texas
Sources: Texas State Data Center, CMHS, SAMSHA, HHS, Census Bureau, DSHS
Estimated Need for Mental Health Services, Texas Youth: FY 2014

Timeline
2004
• RESILIENCY AND DISEASE MANAGEMENT (RDM)
2008
• Review of RDM started
2010
• Re-design was recommended
2012
• New Skills Protocols Available
2013
• Statewide Implementation of TRR and CANS
8

Vision for the Redesign of Children Mental Health Services
Phase 1: Vision and Exploration

Why Redesign?
Challenge’s Facing Children’s Mental Health Care System
Most uninsured children
Low per capita spending for mental health
One of the largest growing child populations
Diverse populations
• Culturally
• Super-urban, urban, suburban, rural , and frontier
Large state
• Population and territory

Why Redesign?
Challenge’s Facing Children’s Mental Health Care System
MH Workforce
• Most bachelor’s level
• High turn-over rate
Child serving systems that did not “talk” to each other
• No common data
• No coordination between systems
Could not compare data with other states
Data did not reflect the comprehensive needs of our populations

Why Redesign?
Challenge’s Facing Children’s Mental Health Care System
Out-dated disease management model
• Diagnosis driven
o “Externalizing” vs. “Internalizing” Disorders
o Medications were prioritized over other forms of treatment
Limited EBPs
Seven Service Packages
• Independent From Each Other
• Most children receiving minimum services
• Too many packages
Why Redesign?
Challenge’s Facing Children’s Mental Health Care System
Poor assessment instrument
• Child & Adolescent: Texas Recommended Assessment Guidelines (TRAG)
o 7 questions
o easily manipulated
• Ohio Youth Problem Severity Scale
• Ohio Youth Functioning Scale

Why Redesign?
Factors that influenced the re-design
LMHAs and Stakeholders Input and Recommendations
State Needs
• Comprehensive assessment
• Age and developmentally appropriate effective treatments
Legislative Requirements: New Outcomes Measures
SAMHSA Requirements of Evidence-based Practices Implementation
National Trends on Mental Health Treatment and Service Delivery System
Vision
Base it on System of Care Values
• Core Values
o Child-Centered, Family Focused
o Community-Based Services
o Cultural Competence
• Principles
o Comprehensive Array of Evidence Based Services & Supports
o Coordination Among Systems
o Involvement of Youth and Families (i.e. Engagement)
Vision
New Level of Care Design
• Intensity Driven: Establishes a Continuum Towards Recovery based on needs & strengths identified
• New Evidence-Based Practices recommended
• Trauma-Informed Care

Vision
Principles of TRR
• Recovery
• Resiliency
• Evidenced Based
• Fidelity

Choosing an Assessment
Workgroup assigned to research assessments:
Needed to match model and vision for TRR
• Align with Systems of Care
• Needs and strengths
• Comprehensive
• Allow for more person-centered/individual care
Needed to match workforce:
• Bachelor’s level
• Ability to train across a large state with high turn-over (i.e. online)
Needed to have fidelity
Needed to have been used and proven up by other states

Choosing an Assessment
Needed to have the following functions:
• Be able to be used as a screening assessment
• Be able to determine a Level of Care
o Algorithms to guide business rules
• Be able to guide treatment planning and selection of EBPs
• Needed to have outcome measurement
Needed to be cost-effective
Why the CANS?
Bottom-line, it met our needs and then some:
• SOC core values are embedded into the CANS
• Based on Needs and Strengths, not diagnosis
• Workforce:
o Can be administered by bachelor’s level staff
o Training available
o Supervision and Super Users

Why the CANS?
• Functions as:
o screening/assessment
o sorting instrument
o comprehensive
ohelps develop individualized treatment plans
oOutcome measure (i.e. Reliable Change Index)
• Cost-effective

Why the CANS?
Outcome Comparison
• CANS—used in 38 states, 16 of which are statewide
• ANSA—Used in 5 states, 3 of which are statewide
Standardized training and certification
• Training & certification required
• Ensures assessments are administered reliably
• i.e. fidelity
Successful pilot in Texas
Why the CANS?
BONUS:
• Dr. John Lyons
DevelopingTexas Resilience and Recovery (TRR): Phase 2 : Plan

Texas Resilience and Recovery (TRR)
Recovery Oriented and Service Intensity Model for Community Mental Health Services
Based on Systems of Care Framework
Focuses on Individual Needs and Strengths
• Person (child)-Centered and Family-Driven services
Implements Evidence-based Practices with Fidelity
Fosters Recovery, Resilience and Hope for Everyone
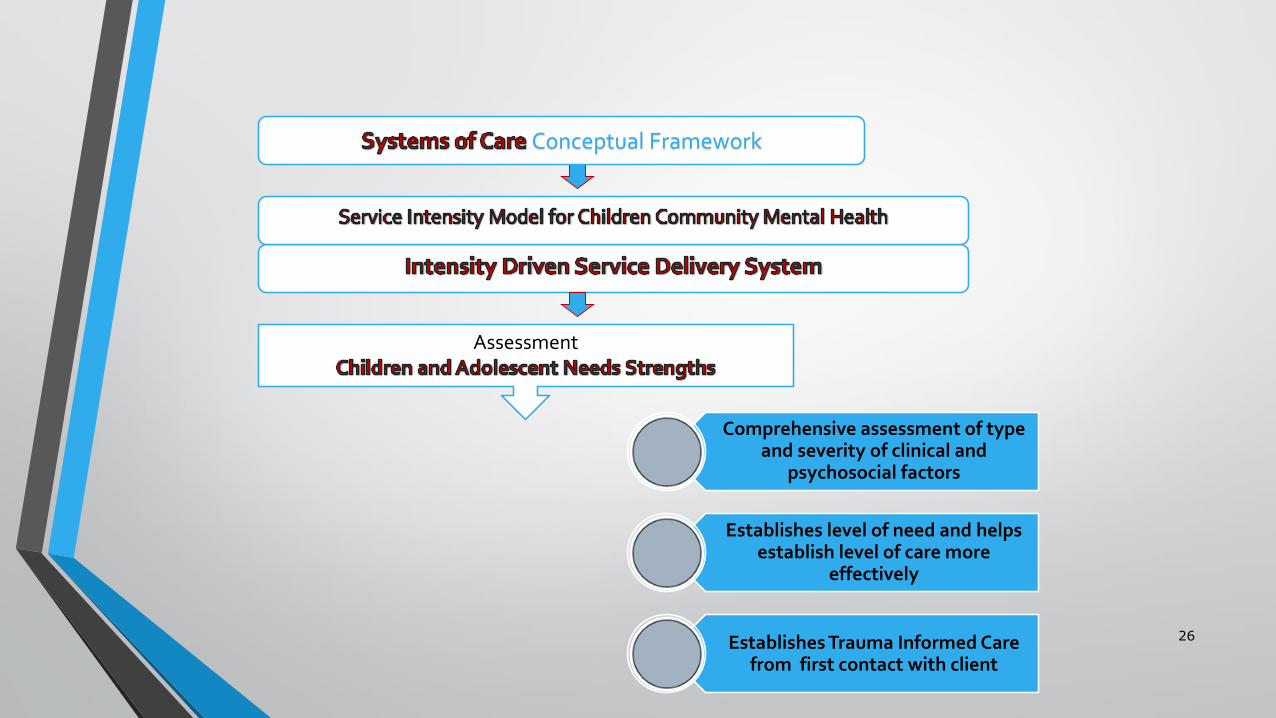
26
Conceptual Framework
Assessment
Comprehensive assessment of type and severity of clinical and
psychosocial factors
Establishes level of need and helps establish level of care more
effectively
Establishes Trauma Informed Care from first contact with client

27
Conceptual Framework
Assessment
Recommended Level of Care
Individualized treatment in the least restrictive setting
EBTs are incorporated
Trauma Informed Care
Facilitate Transitions
Intensity of use of resources responds to level of complexity
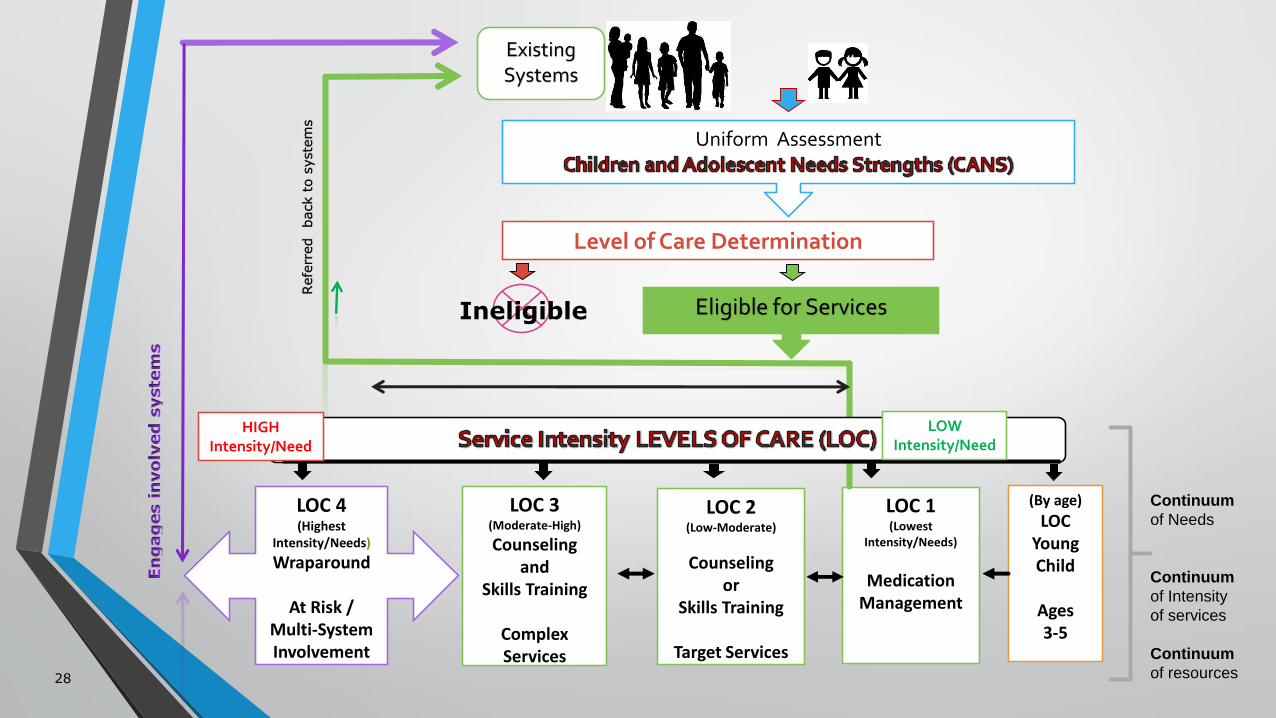
Uniform Assessment
Ineligible Eligible for Services
Level of Care Determination
LOC 4(Highest
Intensity/Needs)
Wraparound
At Risk / Multi-System Involvement
LOC 3(Moderate-High)
Counselingand
Skills Training
Complex Services
LOC 2(Low-Moderate)
Counselingor
Skills Training
Target Services
LOC 1(Lowest
Intensity/Needs)
MedicationManagement
(By age)
LOCYoung Child
Ages 3-5
Refe
rred
back t
o s
yste
ms
ExistingSystems
28
Continuum
of Needs
Continuum
of Intensity
of services
Continuum
of resources
LOW Intensity/Need
HIGHIntensity/Need
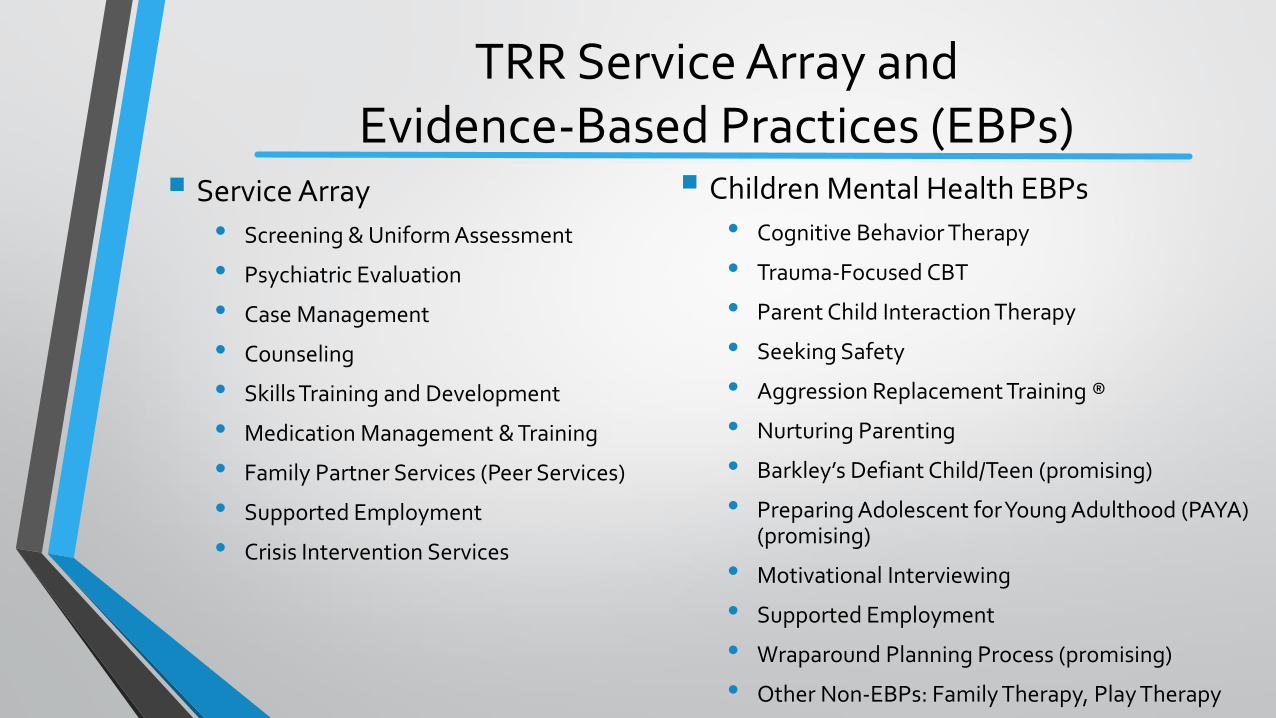
TRR Service Array andEvidence-Based Practices (EBPs)
Service Array
• Screening & Uniform Assessment
• Psychiatric Evaluation
• Case Management
• Counseling
• Skills Training and Development
• Medication Management & Training
• Family Partner Services (Peer Services)
• Supported Employment
• Crisis Intervention Services
Children Mental Health EBPs
• Cognitive Behavior Therapy
• Trauma-Focused CBT
• Parent Child Interaction Therapy
• Seeking Safety
• Aggression Replacement Training ®
• Nurturing Parenting
• Barkley’s Defiant Child/Teen (promising)
• Preparing Adolescent for Young Adulthood (PAYA) (promising)
• Motivational Interviewing
• Supported Employment
• Wraparound Planning Process (promising)
• Other Non-EBPs: Family Therapy, Play Therapy
Developing the Texas CANSPhase 3: Implementation
Phase 1: EXPLORATION (2010)o Existing CANS Versions
Phase 2: PLAN
Phase 3: IMPLEMENTATION• DEVELOPMENT
o Tool & Manualo Algorithms & Business Rules (IT)
• TRAINING & COACHINGo Online Certificationo Training of Trainerso Super Users
• ROLL OUT – Statewide (Sept 2013) FY14
Phase 4: SUSTAINABILITY• SUPERVISION & Super Users• TECHNICAL ASSISTANCE: Webinars & Training• CQI
CANS PHASES OF IMPLEMENTATION

Texas CANS Comprehensive (Domains)
Child Risk Behaviors
Child Behavioral /Emotional
Needs
Child Life Functioning
Child Strengths
Caregiver Strengths &
NeedsCulture
PsychiatricHospital History
Crisis History
2010-2013 (Pilot) 2013 - Present (Roll Out Texas CANS Comprehensive) 2015 (Update) 2016 - CPS (TX CANS 2.0)
Texas CANS: 6-17 Modules
Child Risk Behaviors Domain
• Suicide Risk Module (Suicide Screening)*
• Violence Module
• Sexually Aggressive Behavior Module
• Runaway Module
• Juvenile Justice Module
• Fire Setting Module
Child Emotional/Behavioral Needs Domain
• Trauma Module (Trauma Screening)
• Substance Use Module
Child Life Domain Functioning
• School Module
• Developmental Disability Module
Caregiver Needs & Strengths Domain
• Family/Caretaker Module
Psychiatric History Domain
• Psychiatric Hospitalization Module
Page 34
Texas CANS: 3-5 Modules
Regulatory Functioning Module
Trauma Module
School Module
Developmental Disability Module
Family/Caretaker Module

Total Clinical Outcome Management (TCOM):Grid of Tactics (2011)
Individual Program System
Decision Support
Service PlanningEffective Practices (EBPs)
EligibilityStep-down
Resource ManagementRight-Sizing
Outcome Monitoring
Service Transitions & Celebrations
Evaluation Provider ProfilesPerformance/Contracting
Quality Improvement
Case ManagementIntegrated CareSupervision
QCI/QAAccreditationProgram Redesign
Transformation Business Model Design

Ind
ivid
ual • Service Planning
• Evidence-Based Practices (EBPs)
Pro
gra
m • Eligibility
• Step-down
Sys
tem • Resource
Management
• Right Sizing
TCOM: Decision Support

Ind
ivid
ual• Service Planning
• Evidence-Based Practices (EBPs)
Individualized Recovery Plan guided and supported by CANS scores
Utilization Management Guidelines:• Recommended Decision Tree for EBPs
TCOM: Decision Support
INDIVIDUAL

• Eligibility
• Step Down
Determination of Eligibility• Scores 2 or 3 in
Risk Behaviors orEmotional/Behavioral Needs
Determination of Levels of Care
TCOM: Decision Support
PROGRAM
ProfileChild/Youth
Description of child’s needs, strengths, functioning, recommended core services and transitions.
LOC-A Reasons for Deviation from LOC- Recommended (R)Clinical Judgment/Medical Necessity / Client Refusal / Resource Limitations

Sorting Algorithm Order to DetermineCMH Level of Care (LOC)
Page 39
Clinical Management for Behavioral Health ServicesUse Case Specification: UCS MH 01 Child and Adolescent Uniform Assessment
Version 4.6
LOC 0 • LOC Crisis Services
LOC 4 • LOC Multi-System Involvement
LOC 3 • LOC Complex Services
LOC 1 • LOC Medication Management
LOC 2 • LOC Target Services

Community
CMH Levels of Care Continuum
LOC 1 LOC 2 LOC 3 LOC 4
LOC Residential Treatment Center
LOC Transitioning Age YouthLOC Young
Child
LOC YES Adult
MH
Developmentally Focused LOCs
LOC Early Onset of Psychosis
Strengths/Needs Intensity Driven Levels of Care Continuum
Specialty LOCsLOC – 0
Crisis

Ind
ivid
ual• Resource Management
• Right Sizing
Determine number of staff needed to provider Wraparound Planning Process• LOC 4• LOC Youth Empowerment Services (YES)
TCOM: Decision Support
INDIVIDUAL

Ind
ivid
ual • Service
Transitions
Pro
gra
m • Evaluation
Sys
tem
• Provider Profile
• Performance Measures / Contract
Continuity of Care• Hospitals• RTCs
Improvement
Program Evaluation• Goals• Descriptions• Impact
Outcome Measures
TCOM: Outcomes Monitoring
Outcome Measurement
Reliable Change Index Improvement
• Domain Levelo At least one of the following CANS Domains: Risk Behaviors, Emotional/Behavioral
Needs, Life Functioning, Strengths
• Item Levelo Schoolo Family & Living Situationo Delinquent & Criminal Behavioro Family Partner Services : (Caregivers Domain Items) Family Stress, Involvement with
Care and Knowledge

Ind
ivid
ual • Case Management
• Integrated Care
• Supervision
Pro
gra
m • CQI/QA
• Accreditation
• Redesign Sys
tem • Transformati
on Business
• Model Design
Intensive Case Management : Wraparound• Supervision• Super Users
EBPs Fidelity CQI
• Outcome Measures• Inter-rater reliability
activities at LMHAs by Super Users
Suicide Screening• CSSR-S
CANS Review : Texas CANS 2.0
Transforming Business Operation
TRR: Needs & Strengths
TCOM: Quality Improvement

Implemented by Community Mental Health Services
Implemented by Child Protective Services
2013 Roll Out
Texas CANS
Comprehensive
Developed for Mental Health (MH) Services
All Children entering Mental Health Services
2016Roll Out
Texas CANS 2.0
Developed for MH Services and Child Protective
Services
All Children entering Foster
Care Services
PROGRAM/SYSTEM: QUALITY IMPROVEMENT
Texas CANS 2.0• Improved Manual: Description & Format• Improved Trauma Screening (CANS Trauma) & Suicide Screenings (CSSR-S)• One Assessment Tool for all ages (0-18)• One tool for Mental Health & Child Protective Services)
o Specialized Domains for Systems
Barriers and Challenges Data System
• Roll Out: Clinical Management Behavioral Health Systems (CMBHS)• Multiple IT / Electronic Health Records (EHRs) at the local level• Batching (No Real Time Statewide Data)• Old Data Systems
Funding (State / Local ) Billing : Inability to bill for Uniform Assessment (CANS) Transitioning from a 7 item tool to a 140 items assessment tool Legislative Mandates & Competitive Priorities Workforce : turnover & shortages Inability to make immediate changes or corrections to systems because of
impact to local systems (trickle-down effect) Changes in Leadership Expansion of MCO Providers
Lessons Learned
Leadership: Buy-In and Training• Continuously train and incorporate leadership
Order of CANS Domains (impact to engagement) Need Super Users from the beginning of the implementation Clear definitions in the CANS Manual Needed More Phases of Implementation: Too much elements of implementation rolling out at the same time Incorporate the training of the use of CANS for development of service plan at the
beginning Systems Transformation takes time Systems Transformation is an on-going Continuous Quality Improvement
Initiative

Where are we going?
Implement CSSR-S (Suicide Screening) Incorporate Transforming Collaborative Outcomes Management (TCOM)
• TCOM Implementation Review
Expand access to CMBHS/ CANS electronic to MCO Providers Implement Texas CANS 2.0 Outcome Measures Expand the ability to guide EBP implementation utilizing CANS data Continue CQI
