tendon and ligament injury - aaep¬‚exor tendon (ddft) overstrain injuries often re-main...
TRANSCRIPT

Tendon and Ligament Injury
Roger K. W. Smith, MA, VetMB, PhD, DEO, Diplomate ECVS, MRCVS
Author’s address: The Royal Veterinary College, University of London, United Kingdom; e-mail:[email protected]. © 2008 AAEP.
1. Diagnosis of Tendon Injury
The most frequently injured tendons and ligamentsin the horse are those on the palmar or plantaraspect of the distal limb. For this reason, this se-ries of presentations will focus on these injuries.Diagnosis of strain-induced tendon injuries of theequine distal limb are based on history (usually apreceding period of exercise) and the development ofthe signs of inflammation (pain, heat, swelling, andlameness) over the affected structure. Confirma-tion and semi-objective assessment of severity isprovided by diagnostic ultrasound.
2. Physical Examination
Lameness, which is often severe in the early stages,may not always be present when a patient is pre-sented to a clinician, and it tends to be related to thedegree of inflammation rather than the degree ofdamage. Similarly, after the inflammatory phasehas passed in 1–2 wk, lameness usually resolvesrapidly; however, the injury takes much longer toheal. Additionally, some tendon and ligament in-juries do not follow this pattern. Deep digitalflexor tendon (DDFT) overstrain injuries often re-main persistently and markedly lame, and sus-pensory ligament (SL) desmitis, especiallyproximally in the hindlimb, can result in lowergrade but persistent lameness.
Initial Examination—Non-Contact Observation
Observation of the limb before palpation can providea considerable amount of information on the injuredstructure (nature and location of the swelling) andseverity of the injury (alteration in the posture andfunction of the limb).
Swelling for superficial digital flexor tendon(SDFT) is most apparent when assessing the verypalmar contour of the limb. It is often centered justdistal to the mid-metacarpal region, but it can alsobe in the proximal metacarpal region (high bow) ordistal within the digital sheath (low bow). In sub-tle cases, this swelling may only be apparent whenthe hair is clipped from the limb. Deep digitalflexor tendinopathy rarely, if ever, occurs in theextra synovial portion of the tendon. Thus, injuriesto this tendon are invariably associated with digitalsheath distension and swelling in the pastern re-gion. Desmitis of the accessory ligament of theDDFT (ALDDFT) occurs in the proximal one-half ofthe metacarpal region and is located immediatelydorsal to the SDFT. It is often confused with DDFTenlargement, because it wraps around the tendon.Suspensory desmitis results in swelling over theaffected area. It can occur proximally because ofthe presence of the splint bones; swelling may beminimal, especially in hindlimbs. It can also occurmore distally in areas dorsal to the flexor tendons.Swelling of the body and branches of the SL is found
AAEP PROCEEDINGS � Vol. 54 � 2008 475
IN-DEPTH: TENDON AND LIGAMENT INJURY
NOTES

medially and/or laterally and is immediately palmarto the metacarpal bone.
Resting metacarpophalangeal (MCP) joint angleis often normal with superficial digital flexor tendi-nopathy because of the action of the other support-ers of this joint (SL and DDFT). Additionally, painwill result in a reduced loading of the limb. How-ever, in cases of severe superficial digital flexor ten-dinopathy, the affected limb shows greater thannormal overextension of the MCP joint when theload on the limb increases (e.g., when the contralat-eral limb is raised or when walking). Severe dam-age to the SL will have a greater effect on MCP jointextension. ALDDFT desmitis rarely affects limbposture unless adhesions occur between it and theflexor tendons. In that case, the limb can take onthe appearance of a flexural deformity.
Palpation
In a case of suspected flexor tendon injury, carefulpalpation of the tendons and ligaments in the limbshould be made both when the limb is bearingweight and not bearing weight (flexed). Whenweight bearing, enlargement is assessed by compar-ison with the contralateral limb; however, bilateraldisease is common. With the limb raised, the flexortendons become slack. Careful attention should begiven to pain response, subtle enlargement, whichoften manifests as an indistinct border to the ten-don, and consistency of the structure (soft after re-cent injury and firm after healing). The horse mustbe relaxed so that muscle activity does not tense thetendons and make them appear artificially firm.This assessment should also include the contralat-eral limb, because many strain-induced injuries arebilateral; however, one limb is usually more severelyaffected than the other limb.
Swelling of the ALDDFT is detected by proximalswelling, usually predominantly laterally, becausethis is where the body of the ligament is situated.Enlargement is best identified with the limb flexedand palpated between the flexor tendon bundle andthe SL in the proximal metacarpal region.
The same evaluation should be made for the SL.Unfortunately, the proximal region is impossible topalpate in the weight-bearing limb, especially in thehindlimb, because it is covered by the heads of thesplint bones and the taut flexor tendons. The prox-imal SL in the forelimb can be palpated in the raisedlimb by moving the flexor tendons to one side andpressing between the heads of the splint bones.A comparison should be made between sides, be-cause some normal horses may respond.
Percutaneous tendon injuries are usually associ-ated with moderate to severe lameness and may ormay not have a concurrent wound. If a wound ispresent, it should be initially cleaned and then ex-plored digitally with sterile gloves to find the dam-aged structures. Small wounds may hinder fullevaluation, because the tendon laceration site, sus-tained under full weight-bearing load, is unlikely to
be visible in the wound when the horse is severelylame. In such cases, concurrent ultrasonographicexamination is very helpful. Penetration injuriesor partial severance of a tendon will not alter thefunction of the tendon, and therefore, other thanlameness, there will be little alteration in limb confor-mation. Complete transection, however, is associ-ated with significant alterations in limb conformationunder loading.
SDFT is the overextension of the MCP joint underweight-bearing load.
SDFT � DDFT is the overextension of the MCPjoint at rest and when weight bearing; the toe iselevated from the ground when weight bearing.
SDFT � DDFT � SL is the MCP joint on theground.
If the laceration is complete, the proximal part of alacerated tendon often recoils and can become re-flected on itself. It is also necessary to assess if anysynovial structures have been penetrated. This is acommon complication of trauma to the distal limbsand will frequently lead to synovial sepsis.
3. Ultrasonography
Indications for Ultrasonographic Evaluation of the Tendonand Ligament Injuries
1. DiagnosisAlthough most metacarpal/metatarsal tendon andligament injuries are easily detectable by palpation,palpation provides a poor objective assessment ofthe severity. A base-line scan can provide an as-sessment of severity that may relate to prognosis.It is usually performed 7–10 days after injury, be-cause injuries can worsen initially. In the pas-tern, however, non-specific fibrosis that commonlyaccompanies soft tissue injuries in this regionmakes accurate determination of the injuredstructure difficult. Therefore, ultrasonography isessential for establishing an accurate diagnosis inthis region.
2. ManagementFollow-up ultrasonographic examinations (ideallyevery 2–3 mo) are used to optimize managementdecisions during the rehabilitation phase.
Ultrasonographic Technique
The limb should ideally be prepared by clipping astrip of hair from the palmar aspect of the limb.For the proximal SL in the hindlimb, it is useful toextend this clipped area to the medial aspect toincrease the size of the ultrasonographic “window.”The body of the SL is usually also evaluated from thepalmar aspect; however, this only enables the axialone-third of the ligament to be examined. There-fore, a more complete examination can be achievedby increasing the clipped area for transducer place-
476 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY
ment to the medial and lateral aspects of the limb.Because the branches cannot be adequately exam-ined from the palmar/plantar aspect of the limb,these are evaluated with the transducer placed di-rectly over the branches on the medial and lateralaspects of the limb.
Careful preparation of the area is essential if gooddiagnostic images are to be obtained. After clip-ping, the area should be cleaned. Ideally, a surgi-cal scrub should initially be used followed bysurgical spirit, which degreases the skin and re-moves the bubbles created by the surgical scrub.Any excess is wiped from the limb, and then, high-viscosity contact gel is rubbed well into the skin.While scanning, the horse should be standingsquare so that both limbs are evenly loaded. Seda-tion may be necessary, although usually low doses of�-2 agonists (detomidine or romifidine) are used tominimize swaying. Both limbs should be exam-ined, because many cases of strain-induced tendoninjury have bilateral components. The contralat-eral limb can also serve as a comparison to helpdifferentiate lesions from normal anatomical vari-ants, which are usually bilaterally symmetrical.
There is no standardized technique, but a systemof seven levels or zones is recommended; each hascharacteristic anatomical features.1,2 The palmar/plantar pastern region is also divided into 3–5 levelsor zones. The distal two zones correspond to themore distal position that can sometimes be achievedwith a small footprint transducer; however, a moredistal examination can be achieved with caudal limbposition that hyperextends the distal interphalan-geal joint. At least one longitudinal level is usuallyachievable with a linear transducer depending onthe relative size of transducer and pastern. Easieraccess can be achieved by raising the foot on a block.Because a number of structures pass obliquelyacross the first phalanx, oblique 45° views should beused to perform a complete examination.
4. Principles of Interpretation—UltrasonographicPathology of Tendons and Ligaments
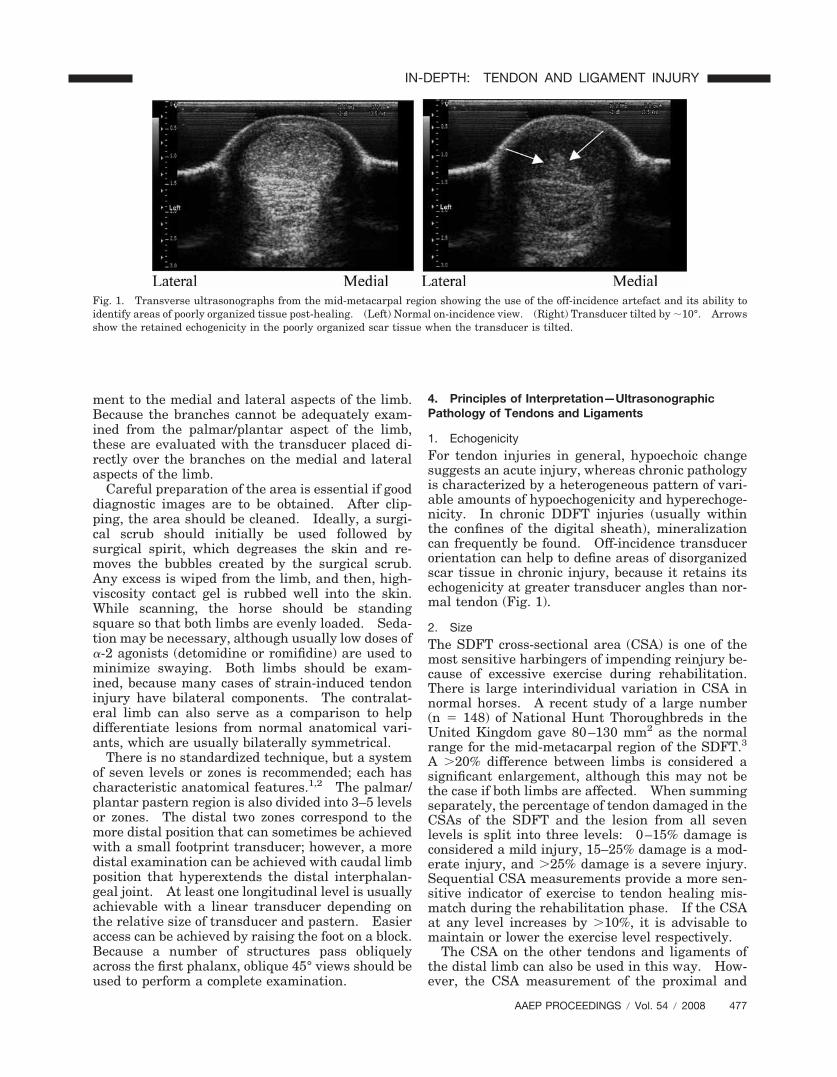
1. EchogenicityFor tendon injuries in general, hypoechoic changesuggests an acute injury, whereas chronic pathologyis characterized by a heterogeneous pattern of vari-able amounts of hypoechogenicity and hyperechoge-nicity. In chronic DDFT injuries (usually withinthe confines of the digital sheath), mineralizationcan frequently be found. Off-incidence transducerorientation can help to define areas of disorganizedscar tissue in chronic injury, because it retains itsechogenicity at greater transducer angles than nor-mal tendon (Fig. 1).
2. SizeThe SDFT cross-sectional area (CSA) is one of themost sensitive harbingers of impending reinjury be-cause of excessive exercise during rehabilitation.There is large interindividual variation in CSA innormal horses. A recent study of a large number(n � 148) of National Hunt Thoroughbreds in theUnited Kingdom gave 80–130 mm2 as the normalrange for the mid-metacarpal region of the SDFT.3
A �20% difference between limbs is considered asignificant enlargement, although this may not bethe case if both limbs are affected. When summingseparately, the percentage of tendon damaged in theCSAs of the SDFT and the lesion from all sevenlevels is split into three levels: 0–15% damage isconsidered a mild injury, 15–25% damage is a mod-erate injury, and �25% damage is a severe injury.Sequential CSA measurements provide a more sen-sitive indicator of exercise to tendon healing mis-match during the rehabilitation phase. If the CSAat any level increases by �10%, it is advisable tomaintain or lower the exercise level respectively.
The CSA on the other tendons and ligaments ofthe distal limb can also be used in this way. How-ever, the CSA measurement of the proximal and
Fig. 1. Transverse ultrasonographs from the mid-metacarpal region showing the use of the off-incidence artefact and its ability toidentify areas of poorly organized tissue post-healing. (Left) Normal on-incidence view. (Right) Transducer tilted by �10°. Arrowsshow the retained echogenicity in the poorly organized scar tissue when the transducer is tilted.
AAEP PROCEEDINGS � Vol. 54 � 2008 477
IN-DEPTH: TENDON AND LIGAMENT INJURY

body regions of the SL is not possible, because theultrasound “window” is narrower than the width ofthe ligament.
3. Pattern
In the longitudinal view, the tendon appears as aseries of striations that relate to the linearity of thecollagen fibers. Because tendon function reliesheavily on this arrangement, the fiber alignment isimportant in assessing the current and, to someextent, the future functionality of healing tendon.The fiber alignment score (FAS) gives a semi-objec-tive assessment between 0 (normal) and 3 (no stri-ations visible).
4. Shape
Alterations in shape will occur with almost any ten-don or ligament injury, but it can be an importantindicator of subtle tendon pathology when the CSAis within the normal range. In addition, both per-cutaneous trauma, which tends to cause focal dam-age to the palmar surface of the SDFT, and focaladhesions in the tendon sheath can also distort thetendon shape.
5. Position
The SDFT becomes medially displaced with severesuperficial digital flexor tendinopathy because oflengthening of the tendon. Adhesions can also al-ter the position of a tendon within tendon sheaths.In the case of the SDFT, complete transection of onebranch in the pastern region results in a shift inposition toward the side of the intact branch proxi-mally (Fig. 2).
6. Margination
Within tendon sheaths, individual adhesions cansometimes be visualized when surrounded by fluid(normal mesotenon/synovial plicae). Poor tendonborder definition has been suggested to be a sign ofadhesions, but it can lead to their overestimation.Optimally, it should be determined by tenoscopy.Real-time imaging while the limb is flexed and ex-tended will allow the ultrasonographer to assess thedegree of the movement of the tendons and liga-ments relative to one another and therefore, identifyadhesion between adjacent structures.
Longitudinal tears in the DDFT within the digitalsheath, easily observed tenoscopically, are oftenpoorly discernible ultrasonographically. Greatersensitivity in detecting these tears can be made byusing an oblique transducer position to assess thelateral and medial borders (Fig. 3). In contrast,some central defects may extend to the surface of thetendon without penetrating the epitenon and thus,may not be visible tenoscopically.
7. Vascularity
The blood flow within healing digital flexor tendonscan be assessed using Doppler with the limb raised(Fig. 4). Normal digital flexor tendons usually have
minimal discernible blood flow, whereas a pro-nounced vascular pattern is usually visible afterinjury. Hypervascularity is normal in the healingprocess but should subside as healing progresses.
Fig. 2. Transverse ultrasonograph from the distal metatarsalregion in a horse suffering a pastern laceration that had com-pletely transacted the lateral branch of the SDFT. Note thealtered medial position of the SDFT proximal to the metatarso-phalangeal joint.
Fig. 3. Oblique transverse ultrasonograph from the palmarolat-eral aspect of the limb immediately proximal to the metacarpo-phalangeal joint showing a tear in the lateral margin of theDDFT. (Arrow) These are not always visible ultrasonographi-cally. Note the echogenic material to the lateral side of thetendon that is a non-specific sign of such tears. This materialcan be torn tendon fibers or thicken synovial plicae, which canalso be the site of fibrous mass formation is chronic cases.
478 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY

This technique is particularly useful for identifyingexacerbations during the healing phase.
5. Ultrasonographic Appearance of the MetacarpalRegion and Pastern Regions
SDFTProximally, the tendon lies within the carpal sheathas a semi-circular structure that is palmaromedialto the DDFT (Figs. 5 and 6). As the tendon runsdistally, it reduces in the CSA and adopts a roundedmedial contour and sharper lateral border. In thedistal metacarpal region, it thins in a dorsopalmardirection and extends a ring of tissue around theDDFT (the manica flexoria). Tearing of the attach-ment of this structure to the SDFT can cause lame-ness (especially in hindlimbs), although diagnosingthis ultrasonographically is difficult.
Distal to the fetlock, the SDFT continues as a thinstructure that then divides into two branches in themid-pastern region. Before its division, the distal“manica,” another ring of the SDFT surrounding theDDFT, is usually visible deep to the DDFT. It is auseful landmark, but contrary to its more proximalsister, it is rarely significantly injured. The twoSDFT branches run abaxially to insert through thethick fibrocartilagenous middle scutum onto theproximopalmar aspect of the middle pha-lanx. These branches are best observed ultrasono-graphically as comma-shaped structures with thetransducer on the palmarolateral and palmarome-dial aspects.
DDFTIn the proximal forelimb, the DDFT lies dorsolateralto the SDFT. As the tendon runs distally, it be-comes more circular and also reduces in the CSA.In the mid-metacarpal level, the ALDDFT joins theDDFT on its dorsal surface and becomes enclosed inthe one paratenon. However, the fibers of the AL-
DDFT can be identified, separated from the DDFTby a hypoechoic curved line, for an appreciable dis-tance distally. In the distal metacarpal region, theDDFT increases in the CSA and becomes oval inshape at the level of the MCP joint. In the hind-limb, the dorsal surface of the DDFT usually has awell-circumscribed hypoechoic region within it inthe proximal limit of the digital sheath that isnormal.
Within the pastern region, the DDFT will fre-quently contain a dorsal hypoechoic region immedi-ately distal to the ergot caused by off-incidenceartefact from the change direction in the DDFT.As the DDFT runs distally, it adopts a bilobedappearance.
The DDFT can be examined further distally, butthis requires a small footprint (e.g., curvilinear)probe that can be placed in the longitudinal planebetween the bulbs of the heel. This allows identi-fication of the DDFT distally to the level of theproximal border of the navicular bone, but it is offincidence. The DDFT overlying the navicular boneand inserting onto the solar surface of the distalphalanx can be seen when scanning through thefrog; however, only the central portions of the ten-don are visible.
ALDDFT
This ligament arises from the palmar carpal liga-ments where it lies on the dorsal surface of thecarpal sheath. It runs from a deep position proxi-mally to a more superficial position distally where itjoins onto the dorsal surface of the DDFT in themid-metacarpal region. Proximally, it is a discretestructure that is separate from the other structureson the palmar aspect of the limb with a prominentlongitudinal striated pattern. It runs in a slightlyoblique angle compared with the flexor tendons, andits on-incidence echogenicity tends to be at a slightlydifferent probe orientation to the flexor tendons.Thus, the flexor tendons or the ALDDFT can appearbrighter than the other depending on probe orienta-tion. As it runs distally, it starts to conform to thedorsal surface of the DDFT. The majority of theligament is laterally positioned so that the trans-ducer has to be moved to a palmarolateral positionto view the entire ligament.
SL
At its origin, the echogenicity can be very variable,and it can include central hypoechoic regions. Thesenormal variants are caused by areas of looser connec-tive tissue within the ligament that contain fat andvascular elements. They are usually bilaterally sym-metrical, but the presence of hypoechoic areas in thisregion should only be interpreted in the light of clinicalexamination and diagnostic analgesia. The dorsalborder of the ligament is usually distinct and sepa-rated from the underlying palmar aspect of the meta-carpus by a small anechoic gap. This hypoechoic area
Fig. 4. Longitudinal ultrasonograph from the mid-metacarpalregion from a horse with a damaged SDFT that showed increasedvascularity with color-flow Doppler in a non–weight-bearing limb.
AAEP PROCEEDINGS � Vol. 54 � 2008 479
IN-DEPTH: TENDON AND LIGAMENT INJURY

becomes obliterated when the ligament is enlargedthrough pathology.
Both proximal and body regions of the forelimb SLare rectangular in shape in transverse images, butthis only represents the middle one-third of the lig-ament because of the size of the ultrasonographicwindow. The medial and lateral borders can only
be visualized by tilting the transducer onto the pal-maromedial and palmarolateral aspects proximallyand then positioning the transducer directly overthe medial and lateral borders in the mid-metacar-pal region where the splint bones are smaller. Be-cause of the variable presence of muscle within theproximal and body (but not the branches) of the SL,
Fig. 5. Diagram representing the ultrasonographic anatomy of the metacarpal region. (A) Transverse images. (B) Longitudinalimages. (From Smith RKW, Webbon PM. Diagnostic imaging—musculoskeletal ultrasonography. In: Hodgson DR, Rose R, eds.The athletic horse. 1992.)
480 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY

the longitudinal striated pattern of the SL is morecoarse than seen in the flexor tendons.
The proximal SL in the hindlimb is more triangularin shape, and it is closely associated with the largehead of the fourth metatarsal (lateral splint) bone andthe smaller head of the second metatarsal (medialsplint) bone. This area is difficult to evaluate and canbe improved by one of the following two actions:
1. Move the transducer to the medial aspect ofthe limb. The ultrasonographic window islarger in this location because of the smallhead of the second metatarsal bone. Amore complete evaluation of the proximalSL can be obtained in this location; however,edge refraction artefacts from the prominentblood vessels superficially in this region caninduce shadows within the proximal SL.
2. Use a curvilinear transducer or “compound-ing,” which provides a wider view of thedeeper areas.
In longitudinal views, the proximal SL has a stri-ated pattern, and the majority of the ligament isattached to the proximal palmar/plantar metacar-pus/metatarsus. The most superficial portion ofthe ligament, however, continues and inserts moreproximally.
In the distal one-third of the metacarpal region,the SL adopts a dumbbell shape in transverse im-ages as it divides into two separate branches. Be-cause of edge refraction shadowing from the bordersof the flexor tendons, the branches cannot be visu-alized adequately from the palmar aspect of thelimb, and therefore, the transducer needs to bemoved so that it lies directly over the medial andlateral SL branches. These branches increase inthe CSA in a proximodistal direction and are a tear-drop shape. They lie immediately adjacent to theskin. Any pathology in these branches results infibrosis between the branch and the skin, whicheffectively “moves” the branch away from the skin.
Fig. 5. (continued)
AAEP PROCEEDINGS � Vol. 54 � 2008 481
IN-DEPTH: TENDON AND LIGAMENT INJURY
Corresponding longitudinal images should also beobtained starting with the most distal of these lon-gitudinal images where the attachment site of the
SL branch onto the abaxial surface of the proximalsesamoid bone appears as an S-shaped surface; thishas been termed, descriptively, the “ski-jump view.”
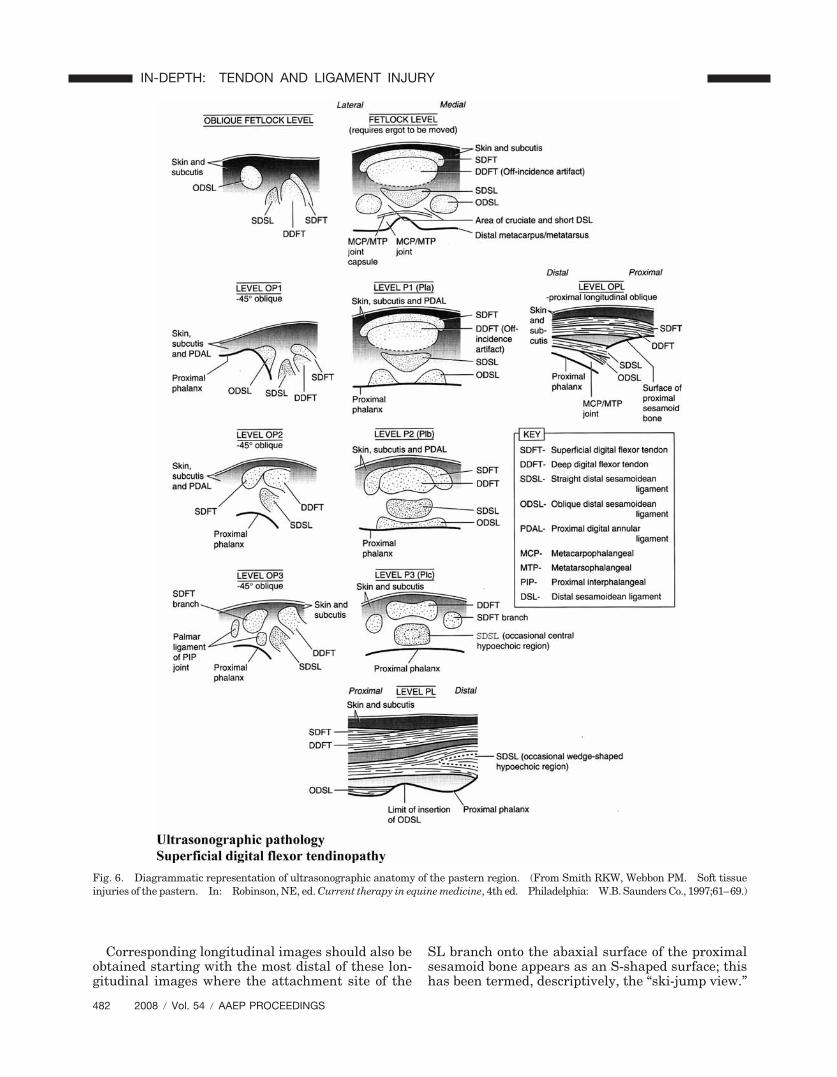
Fig. 6. Diagrammatic representation of ultrasonographic anatomy of the pastern region. (From Smith RKW, Webbon PM. Soft tissueinjuries of the pastern. In: Robinson, NE, ed. Current therapy in equine medicine, 4th ed. Philadelphia: W.B. Saunders Co., 1997;61–69.)
482 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY
The branches show similar fiber alignment to flexortendons at this level.
Digital Sheath
The digital sheath extends from the distal metacar-pal/metatarsal region to the foot on the palmar/plan-tar aspect of the limb. Therefore, abnormalities ofthis structure should include evaluation of this en-tire region. The digital sheath is commonly associ-ated with pathology in the pastern region, althoughits involvement is more frequently secondary. Innormal horses, the digital sheath contains onlysmall amounts of synovial fluid, and its intrathecalarchitecture is often obscure. However, with effu-sion, more structures become visible. Outpouch-ings of the digital sheath can be seen proximallyabaxial to the flexor tendons, immediately distal tothe proximal sesamoid bones abaxially, and in thedistal pastern region in the midline superficial to theDDFT. This is the best site to aspirate synovialfluid from the sheath.
In the distal metacarpal region within the proxi-mal pouch of the digital sheath, abaxial synovialplicae connect the DDFT to the digital sheath wallboth medially and laterally. Although not nor-mally visible in the non-distended sheath, they areeasily identified with the improved contrast associ-ated with sheath distension. The plicae should notbe confused with adhesions, but they are usefulstructures with which to assess the status of thesynovial membrane.
In the distal pastern region, a normal thin meso-tenon is sometimes visible in the midline betweenthe DDFT and the digital sheath.
Palmar/Plantar Annular Ligament of the Fetlock
Identification of the palmar/plantar annular liga-ment of the fetlock (PAL) in normal horses is diffi-cult because of its size (1–2 mm in thickness).4–6
However, moving the probe medially or laterallyaway from the midline (where the annular ligamentis joined to the SDFT by the vinculum) will improvedefinition of the ligament by the relatively hypo-echogenic synovial lining (� synovial fluid) betweenit and the SDFT. If it still cannot be identified withconfidence, the probe should be moved further me-dially or laterally to visualize its attachment to thevery palmar/plantar border of the proximal sesam-oid bones.
Some veterinarians prefer to assess the PAL bymeasuring the distance between the palmar/plantarsurface of the SDFT and the skin surface, althoughthis distance will include the skin, SC tissues, PAL,and synovial membrane. All of these can be af-fected to a variable degree in the condition of annu-lar ligament syndrome (see below). A normalmeasurement of 3.6 � 0.7 mm has been quoted;therefore, anything �5 mm should be consideredsignificant.4
Digital Annular Ligaments
The digital annular ligaments (proximal and distal)cannot be easily visualized in the normal horse,because they are usually �1 mm in thickness.However, they can be seen when enlarged. Theycan be identified proximal to the distal out-pouchingof the digital sheath, especially medially and later-ally where they are more discrete structures grossly.
Distal Sesamoidean Ligaments
Both the oblique distal sesamoidean ligament(ODSL) and straight distal sesamoidean ligament(SDSL) can be identified ultrasonographically.The SDSLs are the most echogenic structures withinthis region and are often more easily assessed in thelongitudinal images. The ODSLs require obliqueviews for adequate imaging. The short and cruci-ate distal sesamoidean ligaments (DSLs) cannot bedistinguished but can sometimes be identified adja-cent to the joint capsule in oblique views of thepalmar/plantar aspect of the fetlock joint.
The insertion of the SDSLs onto the middlescutum on the palmar/plantar aspect of the proximalinterphalangeal (PIP) joint frequently contains a hy-poechoic “core” or “sandwich” in the transverseviews (P3 only) and a hypoechoic “wedge” with itsapex directly proximally in the longitudinal view.The hypoechoic region does not usually extend far-ther proximally than the distal limit of insertion ofthe ODSL. These are normal anatomical varia-tions and should not be mistaken for pathology.
Differences in the Hindlimb
The ultrasonographic anatomy of the metatarsal re-gion is similar to the metacarpal region, but thereare a few differences:
● The SDFT is positioned laterally and theDDFT is positioned medially in the proximalmetatarsal region.
● The subtarsal check ligament (ALDDFT) is avery thin structure lying on the dorsal surfaceof the distal tarsal sheath wall.
● The medial head of the DDFT, in its own ten-don sheath, joins the DDFT on its medial bor-der in the very proximal metatarsal region.
● The SL arises as a triangular structure adja-cent to the third and fourth metatarsal bones(the latter is particularly prominent proxi-mally).
● Proximal to the tarsometatarsal joint, threestructures are visualized—the SDFT superfi-cially, the DDFT deep to the SDFT and medi-ally positioned, and the plantar ligament deepto the SDFT and laterally positioned.
AAEP PROCEEDINGS � Vol. 54 � 2008 483
IN-DEPTH: TENDON AND LIGAMENT INJURY

6. Ultrasonographic Pathology
Superficial Digital Flexor Tendinopathy
A common manifestation of acute injury to this ten-don is a concentric hypoechoic/anechoic lesion visi-ble in the center of the tendon (thus, the usual term“core lesion”), usually centered in the mid-metacar-pal region. It is accompanied by enlargement andSC edema in the acute stage. Lesions can also belocalized eccentrically to the borders of the tendon—medially, laterally, dorsally, or palmarly. Often,dorsal lesions are thought to be associated withmore lameness, presumably because of the directpressure exerted by the DDFT onto the lesion underweight-bearing load.
In very subtle cases, often the only finding can beenlargement and/or change in shape of the tendon.This can be accompanied by peritendinous edema,which is not specific for tendonitis and can alsoresult from local trauma. Providing that there isno evidence of tendon injury and the edema disap-pears, work can be recommenced after only a shortperiod of rest. However, persistent edema suggeststhe presence of tendonitis.
Not all lesions involved local abnormalities, andanother common manifestation is a generalized hy-poechogenic tendon. This may represent either atendon that is healing in which the core lesion hasdisappeared or, if the injury is recent, more diffusedamage to the tendon and/or intratendinous edema.
Injury can also occur to the SDFT in the fetlock(low bow) and pastern regions where it is associatedwith variable amounts of digital sheath effusion.Damage to the SDFT in the region of the fetlockcanal appears ultrasonographically as a hypoechoictendon with minimal enlargement because of theconstraints of the palmar annular ligament. As aresult, these injuries are often associated with sec-ondary thickening of the palmar annular ligament.Injury to the branches of the SDFT is best identifiedby enlargement and hypoechogenicity of individualbranches that is usually observed with the trans-ducer positioned palmarolaterally or palmaromedi-ally. There is usually secondary SC fibrosis withthese injuries in contrast with those affecting theSDFT more proximally. If the injury is localized tothe region of the MCP joint or distally, then theremay be evidence of previous injury to the mid-meta-carpal region.
Complete rupture of the SDFT is the most severeextreme of an overstrain injury, and it often resultsin an almost totally anechoic region of the SDFTsurrounded by a thin echogenic line called theparatenon; this usually remains intact unless theinjury has been caused by percutaneous trauma.Evidence of damage will also be apparent proximaland distal to the rupture. If the tendon ends haveretracted, the outline of the paratenon at the site ofthe rupture may not be particularly enlarged butbunched up, retracted fibers will be identifiableproximal and distal to the rupture site. The SDFT
also becomes medially displaced because of length-ening of the tendon.
Semi-Objective Assessment of Injury to the SDFT
Objective measurements potentially allow a betterdetermination of prognosis and assessment of heal-ing. The following measurements have been sug-gested: (1) the CSA (transverse image), (2) thepercentage of damaged tendon (transverse image)for focal lesions, (3) the type of lesion, and (4) theFAS (longitudinal image).
1. There is a large interindividual variation inthe CSA in normal horses—80–130 mm2 forThoroughbreds.3,7 A �20% difference be-tween limbs is considered a significant en-largement, although this may not be the caseif both limbs are affected.7
2. The CSAs for both the size of the focal lesionand the total tendon CSA at each individuallevel can be summed for all seven levels orzones to give an approximation of the “vol-ume” of the lesion over the volume of the ten-don. This has been used to give what isthought to be the optimal assessment of sever-ity: 0–15% of the tendon affected is a mildinjury, 16–25% of the tendon affected is amoderate injury, and �25% of the tendon af-fected is a severe injury.8 An alternativemethod is to consider the maximum injuryzone only. A mild injury involves �10% ofthe CSA, a moderate injury involves 10–40%of the CSA, and a severe injury involves �40%of the CSA. However, this obviously does nottake into account the length of the lesion.
3. There are four types of lesions or degrees ofechogenicity. Type 1 is a hypoechoic lesionwith more white than black. Type 2 is a hy-poechoic lesion with the same amounts ofwhite and black. Type 3 is a hypoechoic le-sion with more black than white. Type 4 isan anechoic lesion with all black and no white.
4. The FAS (longitudinal image) is assessed sub-jectively on a scale from 0 (76%–100% parallelfibers; normal) to 3 (0–25% of parallel fibers).
Assessment of Healing
All tendon injuries should ideally be monitored ul-trasonographically at 3-mo intervals or before andafter a change in the exercise level. At each exam-ination, the following indicates good progress:
1. A stable or decreasing CSA. Sequential CSAmeasurements provide the most sensitive in-dicator of exercise to tendon healing mismatchduring the rehabilitation phase. If the CSAat any level increases by �10%, it is advisableto maintain or lower the exercise level.
2. An increase in the lesion echogenicity and ahomogeneous texture.
484 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY
3. An improvement in the striated pattern seenlongitudinally (fiber alignment).
4. An absence of peritendinous fibrosis and ad-hesions.8
More recently, the blood flow within healing digitalflexor tendons can be assessed with the limb raisedusing Doppler (Fig. 4).9 Normal digital flexor ten-dons usually have minimal discernible blood flow,whereas, after injury, a pronounced vascular pat-tern is usually visible. Hypervascularity is normalin the healing process. However, it should subsideas healing progresses (normally between 3 and 6 moafter injury), and its reappearance can be an indica-tion of reinjury.
Horses suffering from tendonitis are constantly atrisk of reinjury. Healing, determined histologi-cally, takes at least 15–18 mo.10 The mean intervalbetween injury and return to training in racehorsesis dependent on the severity of the initial injury andvaries between 9 and 18 mo.10 Sports horses maybe able to return to full work in a shorter time, buteven the mildest ultrasonographically detectable in-juries should have at least 6 mo to heal. Occasion-ally, horses are returned to full work before fullresolution of the ultrasonographic lesion; however,this success may be caused by the horse being capa-ble of sustaining work despite the presence of atendon injury.
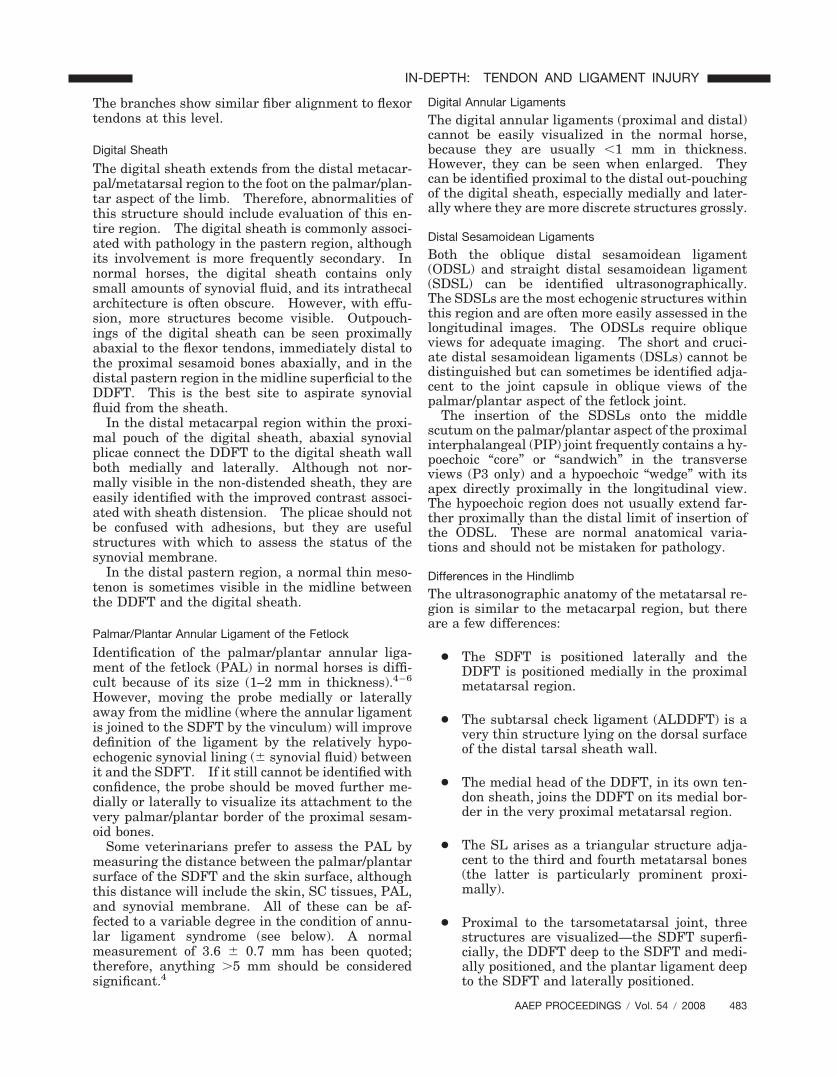
Chronic TendinopathyThe ultrasound characteristics of chronic tendinopa-thy are more variable and can be subtle. The ten-don is often enlarged, but its echogenicity variesfrom hypoechogenic through normoechogenic to hy-
perechogenic if the injury is severe and substantialfibrosis has occurred. The intratendinous patternis usually more coarse and lacks striations in thelongitudinal images (Fig. 7). In some cases, theoutline of the original core lesion can still be seen.Mineralization may occur, which causes acousticshadowing. However, if the calcification is florid,previous intratendinous injection of depot corticoste-roids should be suspected. Off-incidence trans-ducer orientation can help to define areas ofdisorganized scar tissue in chronic injury, because itretains its echogenicity at greater transducer anglesthan normal tendon (Fig. 1).
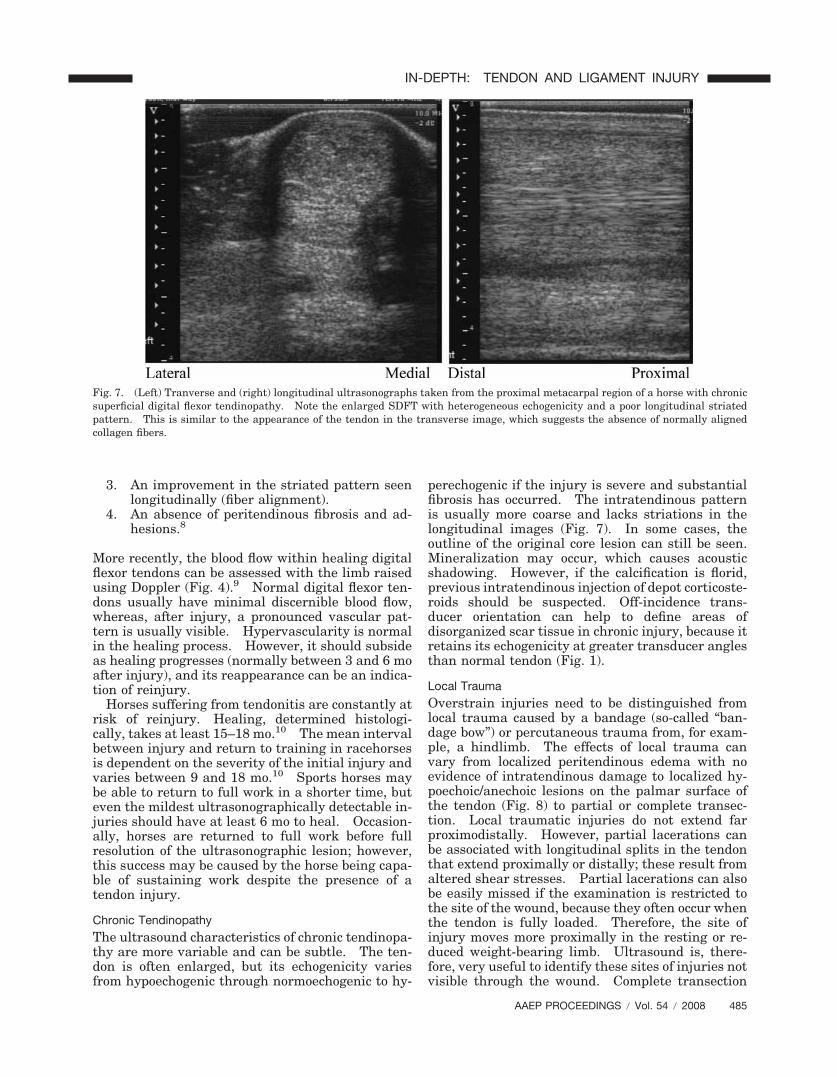
Local TraumaOverstrain injuries need to be distinguished fromlocal trauma caused by a bandage (so-called “ban-dage bow”) or percutaneous trauma from, for exam-ple, a hindlimb. The effects of local trauma canvary from localized peritendinous edema with noevidence of intratendinous damage to localized hy-poechoic/anechoic lesions on the palmar surface ofthe tendon (Fig. 8) to partial or complete transec-tion. Local traumatic injuries do not extend farproximodistally. However, partial lacerations canbe associated with longitudinal splits in the tendonthat extend proximally or distally; these result fromaltered shear stresses. Partial lacerations can alsobe easily missed if the examination is restricted tothe site of the wound, because they often occur whenthe tendon is fully loaded. Therefore, the site ofinjury moves more proximally in the resting or re-duced weight-bearing limb. Ultrasound is, there-fore, very useful to identify these sites of injuries notvisible through the wound. Complete transection
Fig. 7. (Left) Tranverse and (right) longitudinal ultrasonographs taken from the proximal metacarpal region of a horse with chronicsuperficial digital flexor tendinopathy. Note the enlarged SDFT with heterogeneous echogenicity and a poor longitudinal striatedpattern. This is similar to the appearance of the tendon in the transverse image, which suggests the absence of normally alignedcollagen fibers.
AAEP PROCEEDINGS � Vol. 54 � 2008 485
IN-DEPTH: TENDON AND LIGAMENT INJURY

of one branch of the SDFT in the pastern regionresults in a shift in position of the SDFT toward theside of the intact branch more proximally.
Sepsis after a penetrating injury (or occasionally,hematogenous spread) of the SDFT is rare. It usu-ally gives an anechoic lesion, often with a communi-cating tract to the periphery of thetendon. Aspiration of the lesion will yield a samplecontaining large numbers of degenerate neutrophils.These lesions do not usually cause gross enlarge-ment of the affected tendon and change rapidly intime compared with the core lesion in a tendonstrain. If the lesion is present within a tendonsheath, there will usually be an accompanying septictenosynovitis.
Manica Flexoria TearsThis is a common cause of digital sheath tenosyno-vitis, especially in hindlimbs.11 Ultrasonographicdiagnosis is difficult, but an altered position of themanica flexoria seen in a longitudinal scan in themidline immediately proximal to the metacarpo/
metatarsophalangeal joint is probably the best indi-cator (Fig. 9). Tenoscopic assessment provides thedefinitive diagnosis.
Deep Digital Flexor Tendinopathy
DDFT injuries are extremely rare in the metacarpalregion, but they do occur within the confines of thedigital sheath. Of the strain-induced DDFT inju-ries, there are two forms—the intratendinous injuryand surface tears.
Intratendinous Injury
Intratendinous injuries are frequently centered atthe level of the MCP joint. They result from asudden overextension of the distal interphalangealjoint when the MCP joint is fully extended and thelimb is weight bearing. These injuries are fre-quently associated with considerable disruption ofthe tendon resulting in marked and persistent lame-ness. There is usually concurrent tenosynovitisand as with most soft tissue injuries in the phalan-geal region, SC fibrosis. Other lesions are manifestby focal hypoechogenic lesions proximal12 or distalto the MCP joint. Many central defects may extendto the surface of the tendon without penetrating theepitenon and therefore, may not be visible tenoscopi-cally (Fig. 10).
Because of the location of the injuries within thedigital sheath, healing is, at best, problematic.In the chronic stage, the lesions often persist ashypoechoic lesions with or without areas of calcifi-cation. Lameness usually persists, arising from te-nalgia and/or adhesion formation within the sheath.Such adhesions can distort the tendon shape.
Border Tears
Damage to the surface of the DDFT can occur as avariant of overextension injury to the tendon.13
This frequently occurs at the lateral and less com-monly, medial borders of the DDFT in the region ofthe MCP joint. It occurs most commonly in the
Fig. 8. Transverse ultrasonograph from the proximal metatar-sal region in a horse that has suffered percutaneous trauma tothe SDFT. Note the plantar surface defect (labeled).
Fig. 9. The best method of diagnosing a manica flexoria tear ultrasonographically involves the identification of instability of themanica in midline longitudinal views in the distal metatarsal region. (A) The normal contralateral limb is on the left, and the tornmanica flexoria is on the right. Note the wavy form to the manica (arrows). (B) Tenoscopic appearance. The arrow indicates tornmanica.
486 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY

forelimbs, presumably because of excessive forcesduring overextension that compress the tendon andcause a pressure-induced rupture.11 Because oftheir intrasynovial location that is surrounded bysynovial fluid, healing does not occur. These le-sions often persist, being responsible for persistentdigital sheath tenosynovitis and lameness.
Confident diagnosis of these tears using ultra-sonography is difficult. Greater sensitivity in theirdetection can be made by using an oblique trans-ducer positioned to assess the lateral and medialborders (Fig. 3). However, a negative finding onultrasound does not rule out the presence of a tear.Tenoscopy is recommended to identify occult tearsand should certainly be considered in those cases oftenosynovitis that have failed to respond or recurredafter intrathecal medication.
Local TraumaLocal trauma to the palmar/plantar aspect of thepastern is common during overextension of themetacarpo/metatarsophalangeal joint at maximalexercise. Because of the close proximity to theskin, such injuries frequently damage the digitalsheath and DDFT. Such combination injuries canresult in digital sheath (and rarely, DDFT) sepsis ifopen, which gives rise to effusion and synovial thick-ening that is evident ultrasonographically. Thissynovial thickening also usually involves the ep-itenon surrounding the DDFT, which gives a “halo”appearance to the tendon. Such signs, althoughnot pathognomic for sepsis, are strongly suggestiveof it, and they should indicate synoviocentesis toconfirm or refute the presence of sepsis. Localtrauma will cause variably sized hypoechogenic le-sions within the DDFT and enlargement, and it is
often associated with adhesion formation betweenthe damaged areas of the DDFT and sheath wall.Individual adhesions can sometimes be visualizedultrasonographically when surrounded by fluid (nor-mal mesotenon/synovial plicae). Poor tendon bor-der definition has been suggested as a sign ofadhesions, but it can lead to overestimation of ad-hesions. When percutaneous trauma does not pen-etrate the skin, damage can still be induced in theunderlying DDFT (blunt contusion), which may onlybecome visible as a hypoechoic lesion over time.Therefore, if clinical signs persist, a repeat ultra-sonographic examination is indicated after 2–4 wk.
7. Suspensory Ligament—UltrasonographicAppearance and Pathology
Proximal Suspensory Desmitis
Proximal suspensory desmitis is also called highsuspensory disease or proximal metacarpal syn-drome. The ultrasonographic appearance of thisinjury has considerable overlap with the normal ap-pearance. The presence of hypoechoic areas in theproximal SL is common in normal horses, and there-fore, the significance of such findings must be inter-preted in the light of clinical findings (swelling andpain on palpation) and diagnostic local analgesia.Those considered to be true lesions of SL desmitiswill vary in time, and therefore, repeat examina-tions are useful to confirm their significance.
Ultrasonographic features of injury include en-largement of the SL, poor definition to the margins(especially dorsally), single or multiple poorly definedfocal areas of hypoechoicity, diffuse hypoechoicity, andirregularity of the palmar surface of the proximalmetacarpus/metatarsus, which is indicative of enthe-
Fig. 10. The image on the left is a transverse ultrasonograph from the region of the proximal digital sheath in a horse suffering fromdeep digital flexor tendinopathy. Note the hypoechoic region on the palmar surface of the DDFT. Tenoscopic examination of thiscase (right) proved that the lesion did not communicate with the digital sheath, which has important consequences for managementand healing.
AAEP PROCEEDINGS � Vol. 54 � 2008 487
IN-DEPTH: TENDON AND LIGAMENT INJURY

siophytosis. In addition to the ultrasonographic ab-normalities, radiographic changes, such as sclerosisand altered trabecular pattern at the origin of the SL,may also be present. They may occur with or withoutconcurrent increased radionuclide uptake on gammascintigraphy in the proximal metacarpal/metatarsalregions. Differential diagnoses include palmar corti-cal fractures, which usually have no abnormalitieswithin the proximal SL and higher uptake on gammascintigraphy, and avulsion fractures of the head of theSL, where abnormalities in the SL are often confinedto an area immediately adjacent to the site of theavulsion fracture.
Desmitis of the Body of the SL
If this area is injured, there is usually generalizedhypoechogenicity and enlargement to the ligament.In competition/sports horses, the injury often ex-tends into the branches of the SL.
There is some controversy over the link betweensuspensory desmitis and splints. Some aggressiveexostoses on the second or fourth metacarpal/meta-tarsal bones may impinge on the body of the SL andcause a localized suspensory desmitis, but this prob-ably occurs in only the minority of cases. Manyexostoses grow around rather than into the SL.Careful assessment by oblique positioning of theultrasound transducer is necessary, because the ul-trasound “window,” when the transducer is placedon the palmar/plantar aspect, does not usually ex-tend sufficiently abaxially to image these areas ad-jacent to the splint bones.
Desmitis of the SL Branches
This is the most common of the SL injuries in sportshorses. In the forelimbs, biaxial desmitis has thehighest incidence, whereas lateral branch desmitisis the most common manifestation in the hindlimbs.A core lesion or generalized involvement of thebranch, together with enlargement, is seen ultra-sonographically. The longitudinal image from theabaxial aspect gives an excellent assessment of theabaxial surface of the proximal sesamoid boneswhere any associated enthesiopathy is seen by stepsin the S-shaped surface of the bone. The size of theSL branches should be compared with both contra-axial and contralateral branches at the same level,because the branches increase in size in a proximo-distal direction. One of the most sensitive indica-tors of suspensory branch desmitis is periligamentarfibrosis, which is extremely common in this condi-tion. It has the effect of “moving” the SL branchaway from the skin (Fig. 11).
Clinical and radiographic examination of themetacarpo/metatarsophalangeal joint is also recom-mended in cases of SL desmitis. Concurrent painand pathology in this joint is frequently presentbecause of the nature of the injury (hyperextension).Furthermore, radiography will reveal bony pathol-ogy that is frequently associated with the SL bodyand branch desmitis, such as enthesiopathy of the
proximal sesamoid bones (“sesamoiditis”) and distalsplint bone fractures.
8. Other Diagnostic Techniques for DiagnosingTendon and Ligament Injuries
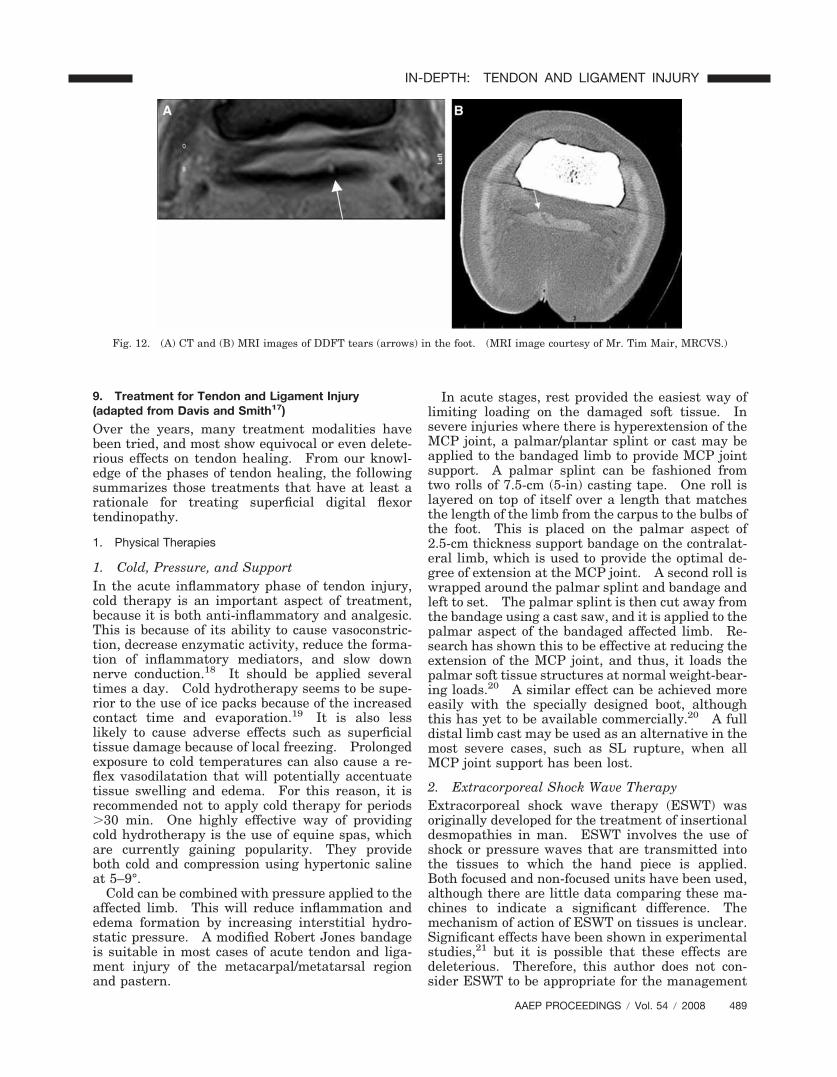
In the ultrasonographic descriptions of pathologyoutlined above, other imaging techniques have beenmentioned including radiography (for the identifica-tion of mineralization and/or enthesiopathy inchronic disease) and the pool phase of gamma scin-tigraphy. More recently, the advent of magneticresonance imaging (MRI)14 and computed tomogra-phy (CT), including contrast-enhanced CT,15 forhorses has enabled us to identify pathology in thoseareas where ultrasonography is limited. This hasbeen particularly true for the foot—most commonlyfor injuries of the DDFT (Fig. 12) and the collateralligaments of the distal interphalangeal joint. How-ever, it is also beginning to help us differentiatepathologies in other areas where ultrasonographyhas frequently not provided sufficient evidence ofpathology, such as the proximal suspensory region.
Finally, although not available clinically as yet, itis hoped that the use of molecular markers, assayedin blood or synovial fluid (for intrasynovial tendonand ligament injuries), may allow us to diagnose andmonitor tendon injuries. This would provide an ob-jective assessment of the efficacy of different treat-ments. One such marker is cartilage oligomericmatrix protein (COMP), which has shown good dif-ferentiation of digital sheaths containing injuredtendons (e.g., tendon tears that are poorly identifiedby other means other than tenoscopy) compared withthose without tendon pathology.16
Fig. 11. Transverse ultrasonograph taken from the lateral as-pect of the forelimb of a horse suffering from suspensory branchdesmitis. Note the collar of periligamentar fibrosis (arrows) thatis characteristic of this condition.
488 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY
9. Treatment for Tendon and Ligament Injury(adapted from Davis and Smith17)
Over the years, many treatment modalities havebeen tried, and most show equivocal or even delete-rious effects on tendon healing. From our knowl-edge of the phases of tendon healing, the followingsummarizes those treatments that have at least arationale for treating superficial digital flexortendinopathy.
1. Physical Therapies
1. Cold, Pressure, and SupportIn the acute inflammatory phase of tendon injury,cold therapy is an important aspect of treatment,because it is both anti-inflammatory and analgesic.This is because of its ability to cause vasoconstric-tion, decrease enzymatic activity, reduce the forma-tion of inflammatory mediators, and slow downnerve conduction.18 It should be applied severaltimes a day. Cold hydrotherapy seems to be supe-rior to the use of ice packs because of the increasedcontact time and evaporation.19 It is also lesslikely to cause adverse effects such as superficialtissue damage because of local freezing. Prolongedexposure to cold temperatures can also cause a re-flex vasodilatation that will potentially accentuatetissue swelling and edema. For this reason, it isrecommended not to apply cold therapy for periods�30 min. One highly effective way of providingcold hydrotherapy is the use of equine spas, whichare currently gaining popularity. They provideboth cold and compression using hypertonic salineat 5–9°.
Cold can be combined with pressure applied to theaffected limb. This will reduce inflammation andedema formation by increasing interstitial hydro-static pressure. A modified Robert Jones bandageis suitable in most cases of acute tendon and liga-ment injury of the metacarpal/metatarsal regionand pastern.
In acute stages, rest provided the easiest way oflimiting loading on the damaged soft tissue. Insevere injuries where there is hyperextension of theMCP joint, a palmar/plantar splint or cast may beapplied to the bandaged limb to provide MCP jointsupport. A palmar splint can be fashioned fromtwo rolls of 7.5-cm (5-in) casting tape. One roll islayered on top of itself over a length that matchesthe length of the limb from the carpus to the bulbs ofthe foot. This is placed on the palmar aspect of2.5-cm thickness support bandage on the contralat-eral limb, which is used to provide the optimal de-gree of extension at the MCP joint. A second roll iswrapped around the palmar splint and bandage andleft to set. The palmar splint is then cut away fromthe bandage using a cast saw, and it is applied to thepalmar aspect of the bandaged affected limb. Re-search has shown this to be effective at reducing theextension of the MCP joint, and thus, it loads thepalmar soft tissue structures at normal weight-bear-ing loads.20 A similar effect can be achieved moreeasily with the specially designed boot, althoughthis has yet to be available commercially.20 A fulldistal limb cast may be used as an alternative in themost severe cases, such as SL rupture, when allMCP joint support has been lost.
2. Extracorporeal Shock Wave TherapyExtracorporeal shock wave therapy (ESWT) wasoriginally developed for the treatment of insertionaldesmopathies in man. ESWT involves the use ofshock or pressure waves that are transmitted intothe tissues to which the hand piece is applied.Both focused and non-focused units have been used,although there are little data comparing these ma-chines to indicate a significant difference. Themechanism of action of ESWT on tissues is unclear.Significant effects have been shown in experimentalstudies,21 but it is possible that these effects aredeleterious. Therefore, this author does not con-sider ESWT to be appropriate for the management
Fig. 12. (A) CT and (B) MRI images of DDFT tears (arrows) in the foot. (MRI image courtesy of Mr. Tim Mair, MRCVS.)
AAEP PROCEEDINGS � Vol. 54 � 2008 489
IN-DEPTH: TENDON AND LIGAMENT INJURY

of acute tendinopathy. One of the most convincingexplanations for its effectiveness clinically is theinduction of analgesia by an effect of sensorynerves.22 The most frequently reported use ofESWT in horses has been for the treatment of prox-imal SL desmitis (PSLD) where it has shown a signif-icant improvement in prognosis over conservativetreatment for chronic hindlimb PSLD. Forty-one per-cent of hindlimb cases returned to full work within 6mo of diagnosis23 compared with the previously re-ported 13% for conservatively managed cases.24
3. Rehabilitation—The Use of Physical Forces toInfluence HealingImmediate controlled passive mobilization of thelimb has been advocated in the acute phase of ten-don and ligament injury in man to reduce inflam-mation and improve healing.25 To be successful,the degree or frequency of mobilization must remainbelow the patient’s pain threshold. This can beadministered by a 15-min session of gentle physicaltherapy. The session should involve a series of10–30 passive carpal and MCP joint flexions as longas they are tolerated by the horse.
Controlled exercise is an intrinsic part of the reha-bilitation of tendon and ligament injuries, and it alsohelps to resolve residual inflammation, maintain glid-ing function, and promote optimal collagen remodel-ing.26 Most SDFT injuries require at least 8–9 mo ofrehabilitation before resuming full athletic function,although some may require up to 18 mo. It is rarelynecessary to prolong rehabilitation longer than this,because healing seems complete by this stage.
A suitable exercise rehabilitation program shouldbe created based on the severity of the ultrasono-graphic appearance of the lesion. The aim of theprogram is to provide a controlled and ascendingexercise regimen that optimizes scar tissue functionwithout causing further injury. This is difficult topredict because of the variability between animals.Therefore, the program should be adapted based onserial ultrasonographic monitoring and clinicalsigns such as lameness, heat, and swelling.
Ultrasonographic monitoring of the tendon/liga-ment should include measurements of tendon CSA.An increase in the CSA of �10% between examina-tions would suggest a degree of reinjury, and in suchcases, the level of exercise should be reduced.27
Because there is a sudden increase in strain levels inthe SDFT and SL with an upward transition in gaitfrom walk to trot, trot to canter, and canter to gallop,ultrasonographic examinations before and afterthese transitions can help to determine if the injuredtendon/ligament can withstand the increased strainlevels.
2. Pharmacological Management
1. Anti-Inflammatory Systemic MedicationBoth systemic corticosteroids and non-steroidal an-ti-inflammatory drugs can be considered for the
management of tendon/ligament inflammation inthe acute stages. Phenylbutazone is commonlyused at a dose of 2.2 mg/kg, q 12 h; however, theclinical effects of this drug seem to be more analgesicthan anti-inflammatory.28 Systemic steroids canbe administered early in the acute inflammatorystage of the injury (usually within the first 24–48 hpost-injury), and they are very effective. Theyshould be avoided during the healing phase, becausethey also inhibit fibroplasia and therefore, repair ofthe tendon.29,30 The induction of laminitis withsystemic steroids represents a small, but neverthe-less real, risk. In the author’s opinion, this is lesslikely in Thoroughbreds compared with Warm-bloods. Topical or IV dimeythl sulphoxide (DMSO)may reduce the inflammation, but a study hasshown that 40–90% topical medical grade DMSOmay weaken normal tendon tissue.31
Polysulphated glycosaminoglycans (PSGAGs)have been shown to inhibit collagenases and meta-loproteinases as well as inhibit macrophage activa-tion, but they were shown to have no effect onfibroblasts.32 Thus, this drug can be viewed as a softtissue anti-inflammatory agent. PSGAGs have beenwidely used for the treatment of tendinopathy anddesmopathy. They are most commonly administeredsystemically through intramuscular injection, al-though they can also be given by intralesional injec-tion.33 Evidence for efficacy is limited; however,improved echogenicity of collagenase-induced superfi-cial digital flexor tendinitis and faster resolution ofcore lesions treated with intralesional PSGAGs wasdemonstrated.34 No significant difference in reinjuryrates between horses treated with PSGAGs comparedwith controlled exercise alone has been shown.35
2. Intralesional Medication
Intralesional tendon and ligament treatment can beperformed under standing sedation and local anal-gesia or under general anesthesia. It is preferredthat it be performed with the leg bearing weight.Although the technique is frequently performedblindly by injecting where least resistance withinthe tendon is detected, accurate placement of theneedle in the center of the lesion is best achievedusing ultrasonographic guidance. The skin overly-ing the tendon or ligament to be injected should beclipped and aseptically prepared, and if ultrasono-graphic guidance is used, a sterile sleeve should beplaced over the probe. A 2.5-cm, 23-g hypodermicneedle can be used for most intratendinous treat-ments, but it varies with the viscosity of the agent.Intralesional treatment should not be administereduntil 3 days after the injury, because there is poten-tial to increase hemorrhage. The volume injectedinto the tendon or ligament will depend on the ex-tent of the lesion. Large volumes can be potentiallydamaging to the healing tendon.36 In addition toPSGAGs, the other agents most frequently used forintralesional medication are hyaluronic acid (HA),
490 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY

corticosteroids, and beta-aminoproprionitrile fuma-rate (BAPN).
HA is a component of tendon matrix and has beenadministered peritendinously, intralesionally, andsystemically to treat tendinitis. In a study of collag-enase-induced digital flexor tendinitis, HA was foundto minimize tendon enlargement compared with con-trols; however, histopathological examination of thetendons failed to show a significant difference in thedegree of inflammation.37 Peritendinous HA hasbeen shown to have no effect on ultrasonographic orhistological appearance, biomechanical properties, ormolecular composition of tendons in collagenase-in-duced tendinitis compared with controls, although itdid appear to reduce lameness.38 A review of theeffectiveness of various medications has failed to showa significant difference between the reinjury rates ofhorses with SDFT tendinitis treated with intralesionalHA compared with conservative treatment.35 Thedrug is probably most appropriately used in the reduc-tion of severity of adhesions after intrathecal injury.39
Corticosteroids, at least the depot preparationssuch as methylprednisolone, should not be injecteddirectly into tendons or ligaments, because theyhave been shown to cause dystrophic tissue miner-alization and tissue necrosis, most likely a conse-quence of the carrier.40 Peritendinous or systemicuse in the early stages are appropriate and can beused judiciously.
BAPN, a lathyrogen that inhibits the enzyme lysyloxidase that normally forms cross-links between col-lagen fibers, has been used to treat tendinopathy.The rationale for its use is to allow exercise to pro-mote alignment of newly formed collagen fibrilswhile preventing them being fixed in a haphazardfashion by cross-linking. BAPN does not hastenthe resolution of the tendinitis, but it aims to im-prove the structure of the repaired tendon. Earlyexperimental studies in collagenase-induced modelsof tendonitis appeared to show improvement in boththe ultrasonographic appearance41 and the histolog-ical collagen alignment.42 However, more recently,concerns have been raised over its efficacy based onobservations that BAPN reduces collagen synthe-sis43 and showed no improvement over controls in arabbit model of tendinitis.44 Clinical studies havesuggested that the reinjury rate of limbs treatedwith BAPN was reduced, although the rate for bothlimbs was no different from other treatments. Thisis caused by the fact that both limbs should betreated, because unilateral treatment increases theloading/reinjury risk on the contralateral limb.However, the drug has been withdrawn from themarket and therefore, is now rarely used.
3. Surgery
1. Tendon SplittingTendon splitting was initially advocated as a treat-ment for chronic tendinitis to improve blood flow todamaged tendon tissue. The technique fell out of
favor when subsequent research showed extensivegranulation tissue formation, increased trauma tothe tendon tissue, and persistent lameness post-treatment.45 Tendon splitting is, therefore, nolonger recommended for the treatment of chronictendonitis. However, it is now thought to be morerelevant for the management of acute cases wherethere is an anechoic core lesion evident on ultrasono-graphic examination that indicates the presence of aseroma or hematoma. It has been hypothesizedthat the presence of a core lesion within a tendonproduces a “compartment syndrome,” which resultsin decreased perfusion and ischemia of the region.The aim of tendon splitting in acute cases is todecompress the core lesion by evacuating the serum/hemorrhage and to facilitate vascular ingrowth.Removal of the fluid within the core lesion may alsoreduce proximodistal propagation of the lesion.In a collagenase-induced model of tendinitis in sixhorses, tendon splitting using the knife techniqueresulted in a faster resolution of the core lesion, aquicker revascularization of the lesion, and an in-creased collagen deposition relative to controls.46
Tendon splitting may be performed under stand-ing sedation or under general anesthesia. It can bedone blindly or using ultrasonographic guidance,which minimizes damage to normal tendon tissue byenabling the needle or knife to be inserted at a pointwhere the core lesion is closest to the periphery ofthe tendon. A #11 scalpel blade or double-edgedblade is inserted into the tendon and “fanned” prox-imally and distally. Alternatively, the procedurecan be achieved with multiple insertions of a 23-gneedle. This may cause less damage to the remain-ing, relatively intact tendon tissue. Furthermore,needle splitting may be combined with various in-tralesional treatments, although multiple needle in-jections may provoke leakage of the drug/agent outof the tendon.
After tendon splitting has been performed, a mod-ified Robert Jones bandage should be applied. Thehorse should be rested in a box stall for 10–14 days,subsequent to which a controlled exercise programshould be initiated.
2. Desmotomy of the Accessory Ligament of theSDFTThe aim of desmotomy of the accessory ligament ofthe superficial digital flexor tendon (or superiorcheck ligament desmotomy (SCLD)) is to produce afunctionally longer musculotendinous unit to reducestrain on the SDFT.47 However, it has been shownin equine cadaver models that SCLD actually in-creases the strain on the SDFT and SL during load-ing because of increased extension of the MCPjoint.48 The biomechanical alterations of SCLD arecomplex, and it is recognized that studies using ca-daver limbs may not represent the biomechanicalevents in a fatigued galloping racehorse. However,increased risk of injury of the SL after the SCLD hasbeen performed has also been shown in vivo.49
AAEP PROCEEDINGS � Vol. 54 � 2008 491
IN-DEPTH: TENDON AND LIGAMENT INJURY

SCLD can be performed using a percutaneous ap-proach50 with the horse in lateral or dorsal recum-bency. More recently, however, this procedure hasbeen carried out tenoscopically through the carpalsheath.51 With the affected limb uppermost andpartially flexed, an arthroscopic portal is createdinto the carpal sheath 2 cm proximal to the distalradial physis on the lateral side of the limb. Aninstrument portal is made immediately proximal tothe distal radial physis. With the limb in 90° flex-ion, the accessory ligament is visualized on the me-dial aspect of the sheath and cut using a #10 scalpelblade on a long handle or meniscectomy knife.The very proximal portion of the ligament cannot bevisualized directly, but it is transected by carefuldissection using punch biopsy forceps. Care mustbe taken to avoid perforating the blood vessel at theproximal limit of the accessory ligament.
3. TenoscopyThe increasingly widespread use of tenoscopy hasshown a high frequency of intrathecal tendon tearsthat are associated with tenosynovitis and lame-ness. Thus, horses presenting with tenosynovitiswith pain on palpation of the proximal digital sheathand lameness should always be considered candi-dates for tenoscopic evaluation. Based on a recentsurvey of cases, tears in the DDFT (Fig. 13) are morecommonly found in forelimb digital sheaths,whereas tears to the manica flexoria are more com-monly found in hindlimbs. Ultrasonographic eval-uation usually reveals non-specific changes ofsynovial hypertrophy, and it is frequently not possi-ble to identify tears on ultrasonographic examina-tion with confidence. In addition, tears can also befound and debrided tenoscopically in the SDFT andDSL within the digital sheath. Tears of other ten-dons and ligaments communicating with a synovialcavity have been seen associated with synovial dis-tension and lameness (e.g., in the SL branches intothe metacarpal/metatarsal joint).
Tenoscopy of the digital sheath requires generalanesthesia and can be performed in lateral or dorsalrecumbency. However, dorsal recumbency allowseasier access to both sides of the digital sheath andis recommended. Arthroscopic portals are createdimmediately distal to the proximal sesamoid and1–2 cm palmar/plantar to the neurovascular bun-dle.52 This allows evaluation of the proximal anddistal parts of the digital sheath, although distalvisualization can sometimes be easier with the ar-throscope inserted through a portal in the proximaldigital sheath (e.g., as for a proximal instrumentportal). Instrument portals are created where ap-propriate to allow debridement of any tendon tearswith a mechanical resector, arthroscopic scissors, orsuction punch biopsy forceps (Fig. 13). This mayrequire the instrument portals to be extendedthrough the synovial reflection that attaches to theproximal border of the manica flexoria to allow ac-cess to DDFT tears located within or proximal to themanica. Although manica tears can also be de-brided in a similar fashion to the DDFT tears, in theauthor’s opinion, this has resulted in a poorer out-come than with complete removal. Because no ad-verse effects have been observed with completeremoval, this is recommended for all except for themost minor manica tears. Removal requires trans-action of both medial and lateral attachments to theSDFT as well as the synovial attachment to theproximal border of the manica. This is facilitatedby an assistant maintaining tension on the manicawith rongeurs through the contra-axial proximal in-strument portal. Transection can be achieved witharthroscopic scissors or a hook knife.
Adhesions can also be resected during tenoscopicevaluation, and the palmar or plantar annular liga-ment can be transected if it is believed to be involvedin the pathology. Post-operatively, the horseshould be strictly rested for at least 2 wk. Afterthat period, hand walking can be started and grad-ually increased over a minimum period of 6 wk.
Fig. 13. Tenoscopic appearance of a tear in the lateral border of the DDFT. The torn fibers are debrided using a (A) mechanicalsynovial resector, arthroscopic scissors, or (B) suction punch biopsy forceps.
492 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY

Thereafter, the duration of rehabilitation will de-pend on the severity of the injury. The prognosisfor DDFT tears (�20%) is worse than for manicatears (�80%).11
4. Annular Ligament DesmotomyAnnular ligament desmotomy has been most fre-quently advocated as a treatment of annular liga-ment syndrome where there is a relativeconstriction of the tendons within the fetlock canal.This constriction can be either primary or secondaryto other pathology within the digital sheath.53–55
Consequently, desmotomy has been advocated forthe management of DDFT and SDFT lesions in theregion of the metacarpal/metatarsal joint. Usually,the procedure is indicated if the annular ligament isimpeding the normal gliding function of the flexortendons. It is probably rarely necessary, becausethe prognosis is closely related to the primary pa-thology. Desmotomy is, therefore, best performedtenoscopically using a hook knife rather thanthrough closed or open techniques, because it is lesstraumatic, ensures accurate transection of only thePAL, and allows evaluation of the tendons to iden-tify any surface defects.
5. Fasciotomy and Neurectomy of the DeepBranch of the Lateral Plantar Nerve for theTreatment of PSLDSurgery has been advocated in cases of PSLD of thehindlimb that are unresponsive to conservativemanagement. It has been reported that horseshave returned to high-level competition after tibialneurectomy to treat PSLD.34 However, a more spe-cific neurectomy of the deep branch of the plantarnerve has been recently described.56 This was per-formed under general anesthesia with the horse indorsal recumbency. An incision 4–6 cm wide,which originates proximally from the level of thechestnut, is made adjacent to the lateral border ofthe SDFT. The plantar metatarsal fascia is in-cised, and the incision is extended deep to the SDFTby blunt dissection, which is facilitated by retractionof the SDFT. The lateral plantar nerve is located inconnective tissue, and the deep branch is identified.It is then transected using a scalpel, and a 3-cmsection is removed. The connective tissue fasciacovering the SL is subsequently cut (fasciotomy)adjacent to the lateral splint bone to “decompress”the origin of the SL, because hindlimb PSLD is be-lieved to be associated with a compressive “compart-ment” syndrome involving the plantar metatarsalnerves.
Post-operatively, only a short period of strict restis needed (�2 wk) to allow the surgical incisions toheal. Thereafter, the horse can gradually begin acontrolled, ascending exercise program.
Unpublished reports have suggested that thistechnique is associated with a high level of success(79%) in returning affected animals to full work withminimum risk of exacerbating the desmitis.
4. Alternatives
The effect of ultrasound, laser, and magnetic fieldson tissues is not completely understood. It isthought that the main effect of ultrasound is theconversion of sound energy into thermal energy.Although there is a paucity of scientifically convinc-ing research into the effects of ultrasound for thetreatment of equine musculoskeletal disorders, astudy by Morcos and Aswad57 showed that the use oftherapeutic ultrasound resulted in increased vascular-ization and fibroblastic proliferation compared withcontrols in experimentally split equine tendons.
Low-level laser therapy has been shown to stimu-late cellular metabolism and enhance fibroblast prolif-eration and collagen synthesis in vitro.58 There are,however, no clinical trials showing a significant differ-ence between laser-treated and control cases of tendi-nopathy or desmopathy.
Despite its widespread use by horse owners andanecdotal reports of its efficacy, magnetic therapyhas not been shown to enhance tendon or ligamenthealing in any clinical trials.
Counter irritation (“firing”) has long been used inequine practice for the treatment of tendon and lig-ament injuries in the form of chemical or thermalcauterization. Topical iodine and mercurial-basedcompounds have been used for chemical cauteriza-tion or “blistering” of tendon injuries. Thermalcauterization or “firing” is performed under generalanesthesia or standing sedation with local analgesiausing heated bars or pins that are applied to theskin over the injured tendon or ligament. In somecases, the tendon is penetrated with the heated pins.Studies have shown that there is no histologicaldifference between the collagen arrangement withinthe scar in cases of tendinopathy treated with firingcompared with controls.59 It has been postulatedthat any benefits from firing result from the en-forced rest, local release of inflammatory cytokines,and/or a protective “bandage” of fibrous tissue/skinthat will support the tendon. The limited con-trolled studies that have been performed on firinghave concluded that it is not an effective treatmentfor tendon and ligament injuries.59
5. Tendon Lacerations
1. Emergency Treatment of Tendon Lacerations
The limb should be stabilized using a splint and asupport bandage before the horse is moved to anappropriate place for treatment. It is importantthat the limb is supported to ensure the comfort ofthe horse. This may help to restore some biome-chanical function of the limb and prevent furthertissue damage. It is particularly important toavoid further trauma to the neurovascular struc-tures of the distal limb. For flexor tendon lacera-tions, a palmar or dorsal splint or a commercialsplint should be applied.
AAEP PROCEEDINGS � Vol. 54 � 2008 493
IN-DEPTH: TENDON AND LIGAMENT INJURY

2. Surgical Repair
Surgical repair of flexor tendon lacerations involvesdebridement, with or without suturing of the ten-don, and closure of the wound, usually performedunder general anesthesia in lateral or dorsal recum-bency. The aim of tenorraphy is to restore tendongliding function, minimize gap formation betweenthe tendon ends, minimize adhesion formation, andpreserve functional vasculature. If the lacerationis complete, the tendon may have recoiled, requiringproximal and distal extension of the skin wound inan elongated “S” to locate both tendon ends. Flex-ing of the metacarpal/metatarsal joint may facilitatelocating of the distal tendon end. The wound andtendon ends should be debrided and lavaged. If thetendon ends can be apposed, tenorraphy can be per-formed using a monofilament absorbable suture(e.g., polydioxanone or polyglyconate). Non-ab-sorbable materials should be avoided, because thiscan result in shearing between the healed tissue andthe suture material. It may be responsible for per-sistent lameness. Two suture patterns have beencommonly used—the three-loop pulley and the in-terlocking loop.60 The three-loop pulley is stron-gest, and it prevents distraction of the ends of thetendon under loading (“gapping”). The interlockingloop has little suture material outside the tendon,and it is, therefore, the recommended technique forrepair of intrathecal lacerations.
Frequently, however, the injury is associated withsignificant blunt trauma to the tendon ends, whichprecludes direct apposition of the tendon ends.In this situation, the tendon ends are left after de-bridement, the wound is closed, and the limb is cast,or an implant can be used to maintain the alignmentof the tendon ends. The ideal tendon implant ma-terial would have similar biomechanical propertiesto normal tendon. Various implant materials havebeen used to repair lacerated flexor tendons includ-ing carbon fiber, terylene (polyester), autologous ex-tensor tendon grafts, absorbable tendon splints, andpoly-L-lactic acid (PLLA).61 Carbon fiber implantswere associated with persistent lameness postoper-atively. This may have been caused by tenalgiathat results from shear forces between inelastic car-bon fibers and the healed tendon tissue. Autolo-gous grafts with extensor tendons can be used tobridge the deficit between two ends of a laceratedtendon, but this technique has never gained popu-larity. PLLA has an advantage in that it supportsfibroblast growth on its surface and loses itsstrength over several months. Therefore, it is ableto match its mechanical properties with the tendon.Implants are anchored in each end of the laceratedtendon by fixing the ends in V incisions created inthe tendon ends with sutures of monofilament ab-sorbable sutures. The tendon splints have a semi-circular cross-section and can be sutured to thetendon ends through holes in the splints. Implants
are not recommended as a treatment for strain-induced tendinopathies.62
Partial lacerations involving �50% of the tendonmay need only local debridement. Lacerations in-volving �50% of the tendon are probably best su-tured, because this can prevent the generation oflongitudinal splits between loaded and unloadedparts of the tendon or the failure of the remainder ofthe tendon under weight-bearing load.
Flexor tendon lacerations require a protracted re-habilitation period. A distal limb cast should beplaced with forelimb lacerations post-operatively.In the hindlimb, a full limb cast is ideally requiredafter flexor tendon laceration to immobilize theforces of the reciprocal apparatus. Distal limbcasts can be used in the hindlimb to avoid the in-creased risk of complications with full limb casts.However, if an implant has been placed, this usuallyresults in one end being pulled out of the tendon.Casting is required for a minimum of 6–8 wk and nomore than 10–12 wk, because studies have shownthat the breaking strength of the tendon repair at 6wk approximates the body weight of the horse.63
This means that usually at least one cast changeunder general anesthesia is needed.
Support of the metacarpal/metatarsal joint usinga palmar/plantar splint with a modified RobertJones bandage and caudal shoe extensions (forDDFT lacerations) can help protect the repair aftercast removal. Continued box-stall rest is necessaryfor an additional 2–3 mo after which walking exer-cise followed by an ascending exercise regimen can beinitiated. Ultrasonographic monitoring of tendonhealing is useful to assess the integrity of the tendonrepair. A minimum of 8–12 mo is usually requiredbefore full athletic function can be resumed.
The prognosis for flexor tendon injuries isguarded. In one study, �45% returned to athleticfunction,63 whereas in another study, the prognosiswas 59% for flexor tendon lacerations.64 In the sec-ond study, the prognosis for return to soundness wasnot increased if the DDFT and SDFT were simulta-neously lacerated compared with if only a singlestructure was lacerated. Short-term complicationsinclude necrotic tendonitis, which occurs as a resultof infection or damage to the vascular supply, con-current synovial sepsis, cast complications, and ex-uberant granulation tissue formation. Long-termcomplications include adhesions, which result incontinued pain and lameness, and occasionally, flex-ural deformity.
In contrast to the flexor tendons, extensor tendonsheal remarkably successfully without tenorraphy,and they respond well to conservative management.The wound should be debrided, and the primarywound should be closed, if appropriate. If the ex-tensor tendon has been lacerated within the confinesof a tendon sheath (e.g., for extensor lacerations overthe dorsal aspect of the carpus), lavage and elimina-tion of sepsis from the tendon sheath also needs tobe addressed. The prognosis for extensor tendon
494 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY

lacerations is good with �72% of horses returning toathletic function.65 Other sources report an 80%good prognosis,64 because the extensor tendon bearsconsiderably less load. Additionally, it has a mini-mal effect on the gait, because most protraction ofthe limb and digit arises from the upper limb andmomentum of the foot. Indeed, a recent publicationreported the successful management of septic com-mon digital extensor tenosynovitis by complete re-section of the tendon.66 Stumbling may be evidentat the walk until the tendon has healed, but it can bereduced by shortening the toe of the hoof and rollingthe toe of the shoe or by fitting a “Natural Balance”type shoe.
6. New Advances—the Evolution of BiologicsSo far, none of the accepted treatment methodsseems to be consistently more efficacious than anyother for long-term return to racing without rein-jury. After injury, tendon heals (repairs) well, butthe scar tissue that replaces the damaged tendon isless functional than normal tendon tissue. This re-sults in reduced performance and a substantial riskof reinjury. To avoid these adverse consequences,an ideal treatment should, therefore, aim to avoidthe formation of excessive fibrous tissue and be ableto regenerate normal tendon matrix. Spontaneousregeneration of tendon post-injury does not seem tooccur. This is most likely because the endogenousstem cell response is inadequate: cells recoveredfrom tendon show poorer differentiation capacitythan bone-marrow cells.67 In addition, the cellularinfiltration, although initially dominated by blood-born cells derived from the bone marrow that arelikely to be white blood cells involved in local de-bridement of damaged tissue, is later substituted bymore long-lasting cellular infiltration, which is prob-ably derived from local surrounding tissues like theparatenon.68 This provides further support for atechnique of exogenous administration of bone mar-row-derived stem cells.
The aim of regenerating tendon tissue involves atissue engineering approach that has been proposedto depend on four separate components: an appro-priate mechanical environment, a scaffold, an ana-bolic stimulus, and a cell source.69 Each of thesecomponents can be used individually, although themaximum effect is believed to occur with a combi-nation of all four.
1. ScaffoldsScaffolds can have a variety of potential beneficialeffects. They can be used to carry or attract cells,help align reparative tissue by their structure, andprotect the cells immediately after implantation andbefore new matrix has been synthesized. However,their influence can be both positive and negative.
ACell Vet is a novel intralesional treatment fortendinopathy/desmopathy using acellular tissuecomponents derived from porcine urinary bladdersubmucosa. This preparation has been suggested
to deliver appropriate growth factors to the injuredtissue as well as attract mesenchymal stem cells.It is injected in liquid form as a reconstituted pow-der. However, it has been associated with signifi-cant inflammatory reaction after injection. It isrecommended that horses are premedicated withanti-inflammatories and that cold is applied locallyafter treatment. It has mostly been used to treatchronic SL disease where there are anecdotal re-ports of benefit, although no objective data has yetbeen published of its efficacy.
2. Growth FactorsInsulin-like growth factor-1 (IGF-1) has been inves-tigated to assess its effect on tendon healing both invitro and in collagenase-induced models of tendini-tis.70 IGF-1 stimulates extracellular tendon ma-trix synthesis and is also a potent mitogen.70 Incollagenase-induced models of tendinitis, initialswelling was decreased after intralesional injectionsof IGF-1 compared with controls. However, no dif-ferences were found at later time points, and therewas no difference between the quantities of type Iand type III collagen synthesized.70 Currently,there is no published long-term follow-up data re-garding reinjury rates of tendinitis treated withIGF-1.
Equine recombinant growth hormone (rEGH) ad-ministered intramuscularly has shown a negativeeffect on the biomechanical properties (decreasedyield point and ultimate tensile strength) of theSDFT during the early phases of healing in collage-nase-induced tendinitis.71 These properties were,however, assessed at 6 wk after treatment, whichmay have been too soon to detect any beneficialeffects of the rEGH.
Transforming growth factor-beta (TGF-�) hasbeen considered as another appropriate growth-fac-tor treatment, although clinical experience has beenlimited. Treated horses showed significant en-largement of the tendon. Reinjury rates were sim-ilar to conservatively managed horses, but thesereinjuries were all on contralateral, untreatedlimbs.c
Platelet-rich plasma (PRP) is becoming more com-monly used for the treatment of tendon and liga-ment injuries. It is usually defined as having �4times the platelet count of normal blood, and it canbe prepared by either centrifugation or filtration(Fig. 14). PRP contains high levels of those growthfactors sequestered in platelets like TGF-�1, IGF-1,and platelet-derived growth factor (PDGF). It isnot known if these growth factors are optimum fortendon and ligament healing, but they do have an-abolic effects72,73 and are, therefore, logical factorsto use. However, it may be that PRP will serve topromote an exaggerated fibrotic reaction ratherthan regeneration. Given this concern, PRP isprobably most suited to the treatment of SL lesions.Evidence of efficacy is still lacking, but small clinicalstudies have been positive.74
AAEP PROCEEDINGS � Vol. 54 � 2008 495
IN-DEPTH: TENDON AND LIGAMENT INJURY

3. Mesenchymal Stem CellsStem cells have the potential of differentiating into anumber of tissues.75–79 Embryonic stem cells aretruly pluripotential but have the disadvantages ofbeing allogenic (although with greater immunologi-cal tolerance) and being associated with a risk ofteratoma formation. Postnatally derived stem cellsare thought to be multipotential or have a restrictednumber of cell lineages into which they can differ-entiate. They are subdivided into hemopoietic(blood-cell lines) and mesenchymal stem cells(MSCs), which can give rise to osteoblasts (bone),chondrocytes (cartilage), tenocytes (tendon and lig-ament), fibroblasts (scar tissue), adipocytes (fat),and myofibroblasts (myotubes). Furthermore,these stem cells can be recovered from adult tissue,
and thus, there is the possibility of autologous reim-plantation. This also has the added benefit thatthey do not incite an immune response from thehost. Such stem cells are most easily recoveredfrom bone marrow, although other workers are con-sidering the use of fat-derived stem cells. Thesepreparations are, however, less well characterizedat present.
The differentiation of the MSCs into tenocytes isbelieved to be induced by a combination of mechan-ical (tension) cues, growth factors, and contact with“like” cells and matrix, most, if not all, of which areprovided by implantation within the tissue.
There is currently much interest in the use ofstem cells to “engineer” new tissue. Clinically,MSCs are currently being used for the treatment ofischemic heart disease in man with encouraging re-sults of survival and increased cardiac output.The transplantation of MSCs into injured skeletaltissues has been shown to promote healing in amultitude of studies in experimental animals. Intendon, studies have used surgically created defectsin tendons and ligaments of laboratory animals andhave all shown significantly improved outcomeswith the implantation of bone marrow(BM)-MSCs.53–55
The equine SDFT injury has a different etiopatho-genesis. However, it is ideal for the implantation ofMSCs, because there is usually an enclosed defectwithin the tendon that can retain implanted MSCswithout the need for a scaffold.
There are several techniques currently employedclinically: direct administration of bone marrow,use of fat-derived stem cells, and autologous implan-tation of MSCs.
1. The direct intraligamentous (or intratendi-nous) administration of bone marrow hasbeen reported to show promising results inthe treatment of SL disease.80 However,there are very few MSCs present in a bone-marrow aspirate (�1 MSC per 105 nucleatedcells), which has led some to suggest thatthis treatment more resembles a growth-factor treatment than a true cell-based ther-apy. Certainly, the supernatant of bonemarrow has been shown to contain a richmix of anabolic factors.81 Furthermore, theinjection of large volumes (20–30 ml) cannotbe fully retained in the structure, and to-gether with the presence of other cell typesand tissues (e.g., bone spicules), it can po-tentially be damaging to the healing tendonor ligament, especially by inducing ectopiccalcification.
2. The above technique using BM-MSCs hasreceived the most basic science research andaims to provide a pure source; however, Vet-Stemb in the United States has used anothersource of stem cells from fat (Fig. 15). Thistechnique involves collecting fat from the
Fig. 14. fPRPa system for preparing plasma rich in platelets.This system uses a filtration system for concentrating the plate-lets rather than centrifugation, and it is a closed system that canbe used “horse side.”
496 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY
tail head, digesting the tissue, and removingthe fat cells. This leaves a mixture of cellsthat includes the adipose-derived stem cells(�2%), which are shipped back to the veter-
inarian without further purification for in-tratendinous injections.
3. In contrast, we have been developing analternative approach involving the implan-
Fig. 16. The VetCell technique for the treatment of tendon and ligament injuries with autologous BM-MSCs.
Fig. 15. The Vet-Stemb system for the treatment of tendon and ligament injuries with fat-derived cells.
AAEP PROCEEDINGS � Vol. 54 � 2008 497
IN-DEPTH: TENDON AND LIGAMENT INJURY

tation of large numbers of autologous MSCsderived from bone marrow and expanded inthe laboratory (Fig. 16). We hypothesizedthat the implantation of marrow-derivedstromal stem cells (BM-MSCs) directly intothe central cavity of an injured SDFT wouldprovide all four of the requirements for ef-fective tissue engineering.
● The cells within the tendon would experiencethe tensional load placed on the tendon.
● They would be injected into a scaffold of gran-ulation tissue that is highly vascular-ized. This provides maximal chance of cellsurvival, even with large lesions.
● The cells are implanted with the supernatantof the bone marrow from which they were de-rived. This has a pronounced anabolic effecton equine ligament cells that is greater thanthat of other biological fluids, including plate-let-rich plasma.81
● The use of BM-MSCs would have the potentialof synthesizing a matrix that more closely re-sembles tendon matrix than scar tis-sue. Thus, this would improve functionaloutcome because of the increased capacity for asuccessful return to performance without rein-jury.
Our technique (developed in conjunction with Vet-Cell Bioscience Ltd.) involves the collection of bonemarrow from the sternum in the standing sedated
horse followed by isolation and expansion of thenucleated adherent cell population (containing theMSCs) in the laboratory.77 After �3 wk, in excessof 10 106 cells are available for implantation.The cells are suspended in bone-marrow superna-tant, because this has been found to have a benefi-cial mix of growth factors. Then, they areimplanted under ultrasonographic guidance into thecore lesion of the tendon or ligament under standingsedation.
The horses then enter an ascending exercise reg-imen aimed at providing a controlled, mechanicallyappropriate (tension) environment for the cells.This consists of initial rest for 7 days (for the cells toestablish themselves) and is followed by walkingexercise for 3 mo. Thereafter, trotting is intro-duced after 3 mo and is followed by cantering after 9mo and full work at 12 mo. Regular ultrasono-graphic monitoring is advised at 1, 3, 6, 9, and 12 mopost-implantation.
Initially, a Phase I trial was performed to ensuresafety. This consisted of six horses with large corelesions in their SDFTs that were followed for up to12 mo. Results indicated that the technique did notcause any worsening of the injury, and there was noreaction or enlargement of the tendon post-implan-tation. Furthermore, no bone or cartilage wasformed based on gamma scintigraphy and ultra-sonography after 3 mo. Core lesions filled inquickly when a hypoechoic lesion was still visible atthe time of implantation. The longitudinal pattern,
Table 1. Typical Exercise Program After Tendon Injury (NB This program should be shortened or lengthened depending on the severity and progressof the case)
ExerciseLevel Weeks Duration and nature of exercise
0 0–2 Box rest1 3 10 minutes walking1 4 15 minutes walking1 5 20 minutes walking1 6 25 minutes walking1 7 30 minutes walking1 8 35 minutes walking1 9 40 minutes walking1 10–12 45 minutes walking daily
Week 12 Repeat ultrasound examination.2 13–16 40 minutes walking and 5 minutes trotting daily2 17–20 35 minutes walking and 10 minutes trotting daily2 21–24 30 minutes walking and 15 minutes trotting daily
Week 24 Repeat ultrasound examination2 25–28 25 minutes walking and 20 minutes trotting daily2 29–32 20 minutes walking and 25 minutes trotting daily
Week 32 Repeat ultrasound examination3 33–36 45 minutes exercise daily with slow canter3 37–40 45 minutes exercise daily with slow canter3 41–44 45 minutes exercise daily with fast work three times a week3 45–48 45 minutes exercise daily with fast work three times a week
Week 48 Repeat ultrasound examination4 From 48 wks Return to full competition/race training
498 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY

however, remained inferior to normal tendon butimproved with exercise.
Since the initial trial, in excess of 500 horses havebeen treated with this technique. At the most re-cent evaluation of clinical outcome (September2007), 172 racehorses had been treated with �1 yrfollow-up. For National Hunt racehorses (n � 145),the reinjury rate was 18% (23% when injuries to un-treated contralateral limbs were included). Whenonly those horses that had entered full training wereincluded, the reinjury rate rose slightly to 24% (33%with contralateral reinjuries). These percentageshave remained relatively constant for up to 3 yr aftertreatment, although numbers are small for the longestfollow-up. However, these data compare favorablywith previous analyses for the same category of horse(56% reinjury rate for National Hunt horses14) foranalysis of horses used for the same discipline followedfor 2 yr after a return to full work. In further supportfor this improvement in outcome, reinjury rates forsports horses (all disciplines combined; n � 109 with�1 yr follow-up) was improved by a similar degree(13% compared with 23–43% reported for differentsport-horse disciplines35).
We proposed that the optimum time to implantthe cells is after the initial inflammatory phase butbefore fibrous tissue formation. It was hypothe-sized that the presence of mature fibrous tissuewithin the tendon would (1) make implantationmore difficult and (2) reduce the benefits of the stem-cell therapy because of its persistence. Both havebeen supported by clinical experience of delayed im-plantation of BM-MSCs and outcome. Successeshad an average interval between injury and implan-tation of 44 days, whereas horses suffering reinjuryhad an average interval of 83 days (p � 0.0035).Current recommendations are that bone marrow isaspirated within 1 mo of injury. For the same rea-son, known recurrent injuries are not consideredideal cases, because significant fibrosis would al-ready be present. The time of implantation may befurther optimized by pre-injury storage of cells.
Five cases that died through unrelated causeshave been analyzed histologically and showed excel-lent healing with minimal inflammatory cells andcrimped organized collagen fibers. In contrast, acontralateral untreated SL injury in one of thesehorses, which was clinically silent at the time ofimplantation, showed persistent inflammatory cellsand poorly organized collagen fibers.
A more limited number of cases have been treatedwith injuries to other tendons and ligaments. Forlesions present within a tendon sheath, the implan-tation is done after tenoscopic evaluation to ensurethat there are no surface defects through which thecells could leak.
10. Conclusions
The extensive number of treatments available forthe treatment of tendon and ligament injuries pro-vides strong evidence that none are universally ef-
fective. Because of the natural variability of thedisease, careful and objective assessment of largenumbers of cases is essential to prove efficacy of atreatment. Treatment should be selected by stageand severity of disease, use of horse (racing is stillthe most severe test for an effective treatment), andfollow-up time (reinjuries tend to occur when thehorse is back racing but not before). This meansthat strong evidence-based treatments cannot beprovided. The two most important aspects are to(1) obtain an accurate diagnosis of which structureis injured, including the stage and severity, and (2)apply treatments based on a strong scientific ratio-nale with respect to the pathophysiology. Cur-rently, combinations of treatments may offer thebest approach (e.g., stem-cell treatment and SCLD).However, in many cases, cost implications may alsoinfluence the choice of combination treatments.
References and Footnotes1. Genovese RL, Rantanen NW, Simpson BS, et al. Clinical
experience with quantitative analysis of superficial digitalflexor tendon injuries in Thoroughbred and Standardbredracehorses. Vet Clin North Am [Equine Pract] 1990;6:129–145.
2. Smith RKW, Webbon PM. Diagnostic imaging—musculo-skeletal ultrasonography. In: Hodgson DR, Rose R, eds.The athletic horse. 1992.
3. Avella CS, Ely ER, Verheyen KLP, et al. Ultrasonographicassessment of the superficial digital flexor tendon of NationalHunt racehorses in training over two racing seasons. EquineVet J 2008. In press.
4. Dik KJ, Dyson SJ, Vail TB. Aseptic tenosynovitis of thedigital flexor tendon sheath, fetlock and pastern annularligament constriction. Vet Clin North Am [Equine Pract]1995;11:151–162.
5. Dik KJ, van den Belt AJ, and Keg PR. Ultrasonographicevaluation of fetlock annular ligament constriction in thehorse. Equine Vet J 1991;23:285–288.
6. Smith RKW, Webbon PM. Soft tissue injuries of the pas-tern. In: Robinson, NE, ed. Current therapy in equine med-icine, 4th ed. Philadelphia: W.B. Saunders Co., 1997;61–69.
7. Smith RK, Jones R, Webbon PM. The cross-sectional areasof normal equine digital flexor tendons determined ultrasono-graphically. Equine Vet J 1994;26:460–465.
8. Reef VB. Superficial digital flexor tendon healing: ultra-sonographic evaluation of therapies. Vet Clin North Am[Equine Pract] 2001;17:159–178.
9. Kristoffersen M, Ohberg L, Johnston C, et al. Neovasculari-sation in chronic tendon injuries detected with colour Dopplerultrasound in horse and man: implications for research andtreatment. Knee Surg Sports Traumatol Arthrosc 2005;13:505–508.
10. Marr CM, McMillan I, Boyd JS, et al. Ultrasonographic andhistopathological findings in equine superficial digital flexortendon injury. Equine Vet J 1993;25:23–29.
11. Smith MR, Wright IM. Noninfected tenosynovitis of thedigital flexor tendon sheath: a retrospective analysis of 76cases. Equine Vet J 2006;38:134–141.
12. Barr AR, Dyson SJ, Barr FJ, et al. Tendonitis of the deepdigital flexor tendon in the distal metacarpal/metatarsal re-gion associated with tenosynovitis of the digital sheath in thehorse. Equine Vet J 1995;27:348–355.
13. Wright IM, McMahon PJ. Tenosynovitis associated withlongitudinal tears of the digital flexor tendons in horses: areport of 20 cases. Equine Vet J 1999;31:12–18.
14. Dyson S, Murray R. Magnetic resonance imaging evalua-tion of 264 horses with foot pain: the podotrochlear appara-
AAEP PROCEEDINGS � Vol. 54 � 2008 499
IN-DEPTH: TENDON AND LIGAMENT INJURY

tus, deep digital flexor tendon and collateral ligaments of thedistal interphalangeal joint. Equine Vet J 2007;39:340–343.
15. Puchalski SM, Galuppo LD, Hornof WJ, et al. Intraarterialcontrast-enhanced computed tomography of the equine distalextremity. Vet Radiol Ultrasound 2007;48:21–29.
16. Smith RK, Heinegard D. Cartilage oligomeric matrix pro-tein (COMP) levels in digital sheath synovial fluid and serumwith tendon injury. Equine Vet J 2000;32:52–58.
17. Davis CS, Smith RKW. Diseases of tendon and ligament.In: Auer J, ed. Equine surgery. 2006.
18. Petrov R, MacDonald HH, Tesch AM, et al. Influence oftopically applied cold treatment on core temperature and cellviability in equine superficial digital flexor tendons. Am JVet Res 2003;64:835–844.
19. Kasashima Y, Eto D, Kusano K. Comparison of the methodof cold therapy to equine limbs after training, with the aim ofpreventing tendonitis. Jpn J Equine Sci 2001;12:96.
20. Smith RK, McGuigan MP, Hyde JT, et al. In vitro evalua-tion of nonrigid support systems for the equine metacarpo-phalangeal joint. Equine Vet J 2002;34:726–731.
21. Kersh KD, McClure SR, Van Sickle D, et al. The evaluationof extracorporeal shock wave therapy on collagenase inducedsuperficial digital flexor tendonitis. Vet Comp Orthop Trau-matol 2006;19:99–105.
22. Bolt DM, Burba DJ, Hubert JD, et al. Evaluation of cuta-neous analgesia after non-focused extracorporeal shock waveapplication over the 3rd metacarpal bone in horses. Can JVet Res 2004;68:288–292.
23. Crowe OM, Dyson SJ, Wright IM, et al. Treatment ofchronic or recurrent proximal suspensory desmitis using ra-dial pressure wave therapy in the horse. Equine Vet J 2004;36:313–316.
24. Dyson S. Proximal suspensory desmitis in the hindlimb:42 cases. Br Vet J 1994;150:279–291.
25. Buckwalter JA. Effects of early motion on healing of mus-culoskeletal tissues. Hand Clin 1996;12:13–24.
26. Gillis CL. Rehabilitation of tendon and ligament injuries, inProceedings. 43rd Annual American Association of EquinePractitioners Convention 1997;306–309.
27. Reef VB. Equine diagnostic ultrasound. Philadelphia:W.B. Saunders Co., 1998.
28. May SA, Lees P. Non-steroidal anti-inflammatory drugs.In: McIlwraith CW, Trotter GW, eds. Joint disease in thehorse. Philadelphia: W.B. Saunders Co., 1997.
29. Scutt N, Rolf CG, Scutt A. Glucocorticoids inhibit tenocyteproliferation and tendon progenitor cell recruitment. J Or-thop Res 2006;24:173–182.
30. Shrier I, Matheson GO, Kohl HW III. Achilles tendonitis:are corticosteroid injections useful or harmful? Clin J SportMed 1996;6:245–250.
31. Albrechtsen SJ, Harvey JS Jr. Dimethyl sulfoxide. Biome-chanical effects on tendons. Am J Sports Med 1982;10:177–179.
32. Dahlgren LA, Rosenbusch RF, Booth LC. The effect of poly-sulphated glycosaminoglycan on the production of proteogly-can by equine tendon fibroblasts in monolayer culture. VetComp Orthop Traumatol 1998;11:136.
33. Smith RKW. A case of superficial digital flexor tendinitis:ultrasonographic examination and treatment with intrale-sional polysulphated glycosaminoglycans. Equine Vet Edu1992;4:280–285.
34. Redding WR, Booth LC, Pool RR. Effects of polysulphatedglycosaminoglycans on the healing of collagenase-inducedtendonitis of the equine superficial digital flexor tendon. VetSurg 1992;21:403.
35. Dyson SJ. Medical management of superficial digital flexortendonitis: a comparative study in 219 horses (1992–2000).Equine Vet J 2004;36:415–419.
36. Van den Belt AJ, Keg PR, Dik KJ. The correlation betweenthe dose distribution of intratendinous fluid injections in theflexor tendons of the horse; a pilot study. Vet Radiol Ultra-sound 1992;33:120.
37. Gift LJ, Gaughan EM, DeBowes RM. The influence of in-tratendinous sodium hyaluronate on tendon healing inhorses. Vet Comp Orthop Traumatol 1992;5:151.
38. Foland JW, Trotter GW, Powers BE, et al. Effect of sodiumhyaluronate in collagenase-induced superficial digital flexortendinitis in horses. Am J Vet Res 1992;53:2371–2376.
39. Gaughan EM, Nixon AJ, Krook LP, et al. Effects of sodiumhyaluronate on tendon healing and adhesion formation inhorses. Am J Vet Res 1991;52:764–773.
40. Pool RR, Wheat JD, Ferraro GL. Corticosteroid therapy incommon joint and tendon injuries of the horse. Part I and II:the effects on tendons, in Proceedings. 26th Annual Ameri-can Association of Equine Practitioners Convention 1980.
41. Reef VB, Genovese RL, Byrd JW. Treatment of superficialdigital flexor tendon injuries with beta-aminoproprionitrilefumarate (BAPN-F): sonographic evaluation of early tendonhealing and remodeling, in Proceedings. First Dubai Inter-national Equine Symposium 1996.
42. Alves ALG, Rodrigues MAM, Aguiar AJA. Effects of beta-aminoproprionitrile fumarate and exercise on equine tendonhealing: gross and histological aspects. J Equine Vet Sci2001;21:335.
43. Dahlgren LA, Nixon AJ, Brower-Toland BD. Effects of beta-aminopropionitrile on equine tendon metabolism in vitro andon effects of insulin-like growth factor-I on matrix productionby equine tenocytes. Am J Vet Res 2001;62:1557–1562.
44. Yamamoto E, Hata D, Kobayashi A, et al. Effect of beta-aminopropionitrile and hyaluronic acid on repair of collage-nase-induced injury of the rabbit Achilles tendon. J CompPathol 2002;126:161–170.
45. Stromberg B, Tufvesson G, Nilsson G. Effect of surgicalsplitting on vascular reactions in the superficial flexor tendonof the horse. J Am Vet Med Assoc 1974;164:57–60.
46. Henninger RW, Bramlage LR, Bailey M. Effects of tendonsplitting on experimentally-induced acute equine tendonitis.Vet Comp Orthop Traumatol 1992;5:1.
47. Bramlage LR. Superior check ligament desmotomy as atreatment for superficial digital flexor tendonitis: initial re-port, in Proceedings. 32nd Annual Amercian Association ofEquine Practitioners Convention 1986;365–369.
48. Shoemaker RS, Bertone AL, Mohammad LN, et al. Desmo-tomy of the accessory ligament of the superficial digital flexormuscle in equine cadaver limbs. Vet Surg 1991;20:245–252.
49. Gibson KT, Burbidge HM, Pfeiffer DU. Superficial digitalflexor tendonitis in thoroughbred race horses: outcome fol-lowing non-surgical treatment and superior check desmot-omy. Aust Vet J 1997;75:631–635.
50. McIlwraith CW, Robertson JT. Superior check ligament des-motomy (after Bramlage). In: Equine surgery advanced tech-niques. Baltimore: Williams and Wilkins, 1998.
51. Southwood LL, Stashak TS, Kainer RA, et al. Desmotomy ofthe accessory ligament of the superficial digital flexor tendonin the horse with use of a tenoscopic approach to the carpalsheath. Vet Surg 1999;28:99–105.
52. Nixon AJ. Endoscopy of the digital flexor tendon sheath inhorses. Vet Surg 1990;19:266–271.
53. Gerring EL, Webbon PM. Fetlock annular ligament desmo-tomy: a report of 24 cases. Equine Vet J 1984;16:113–116.
54. McGhee JD, White NA, Goodrich LR. Primary desmitis ofthe palmar and plantar annular ligaments in horses: 25cases (1990–2003). J Am Vet Med Assoc 2005;226:83–86.
55. Owen KR, Dyson SJ, Parkin TDH, et al. Retrospectivestudy of palmar/plantar annular ligament injury in 71 hors-es: 2001–2006. Equine Vet J 2008;40:237–244.
56. Bathe AP. Plantar metatarsal neurectomy and fasciotomyfor the treatment of hindlimb proximal suspensory desmitis.Vet Surg 2003;32:480.
57. Morcos MB, Aswad A. Histological studies of the effects ofultrasonic therapy on surgically split flexor tendons. EquineVet J 1978;10:267–268.
58. Henninger R. Treatment of superficial digital flexor tendi-nitis. Vet Clin North Am [Equine Pract] 1994;10:409–424.
500 2008 � Vol. 54 � AAEP PROCEEDINGS
IN-DEPTH: TENDON AND LIGAMENT INJURY

59. Silver IA, Brown PN, Goodship AE, et al. A clinical andexperimental study of tendon injury, healing and treatmentin the horse. Equine Vet J 1983;1(Suppl):1–43.
60. Jann HW, Stein LE, Good JK. Strength characteristics andfailure modes of locking-loop and three-loop pulley suturepatterns in equine tendons. Vet Surg 1990;19:28–33.
61. Eliashar E, Schramme MC, Schumacher J, et al. Use of abioabsorbable implant for the repair of severed digital flexortendons in four horses. Vet Rec 2001;148:506–509.
62. Gibson KT, Burbidge HM, Robertson ID. The effects of poly-ester (terylene) fibre implants on normal equine superficialdigital flexor tendon. New Zeal Vet J 2002;50:186–194.
63. Bertone AL. Tendon lacerations. Vet Clin North Am[Equine Pract] 1995;11:293–314.
64. Foland JW, Trotter GW, Stashak TS, et al. Traumatic inju-ries involving tendons of the distal limbs in horses: a retro-spective study of 55 cases. Equine Vet J 1991;23:422–425.
65. Belknap JK, Baxter GM, Nickels FA. Extensor tendon lac-erations in horses: 50 cases (1982–1988). J Am Vet MedAssoc 1993;203:428–431.
66. Booth TM, Abbot J, Clements A, et al. Treatment of septiccommon digital extensor tenosynovitis by complete resectionin seven horses. Vet Surg 2004;33:107–111.
67. Strassburg S, Smith RK, Goodship AE, et al. Adult and latefoetal equine tendon contain cell populations with weak progen-itor properties in comparison to bone marrow derived mesen-chymal stem cells, in Proceedings. 52nd Orthopaedic ResearchSociety 2006;1113.
68. Kajikawa Y, Morihara T, Watanabe N, et al. GFP chimericmodels exhibited a biphasic pattern of mesenchymal cell in-vasion in tendon healing. J Cell Physiol 2007;210:684–691.
69. Juncosa-Melvin N, Matlin KS, Holdcraft RW, et al. Me-chanical stimulation increases collagen type I and collagentype III gene expression of stem cell-collagen sponge con-structs for patellar tendon repair. Tissue Eng 2007;13:1219–1226.
70. Dahlgren LA, et al. Insulin-like growth factor-I improvescellular and molecular aspects of healing in a collagenase-induced model of flexor tendinitis. J Orthop Res 2002;20:910–919.
71. Dowling BA, Dart AJ, Hodgson DR, et al. The effect ofrecombinant equine growth hormone on the biomechanical
properties of healing superficial digital flexor tendons inhorses. Vet Surg 2002;31:320–324.
72. Schnabel LV, Mohammed HO, Miller BJ, et al. Platelet richplasma (PRP) enhances anabolic gene expression patterns inflexor digitorum superficialis tendons. J Orthop Res 2007;25:230–240.
73. Schnabel LV, Mohammad HJ, Jacobson MS, et al. Effects ofplatelet rich plasma and acellular bone marrow on gene expres-sion patterns and DNA content of equine suspensory ligamentexplant cultures. Equine Vet J 2008;40:260–265.
74. Waselau M, et al. Intralesional injection of platelet-richplasma followed by controlled exercise for treatment of mid-body suspensory ligament desmitis in Standardbred race-horses. J Am Vet Med Assoc 2008;232:1515–1520.
75. Richardson LE, Dudhia J, Clegg P, et al. Stem cells inveterinary medicine—attempts at regenerating equine tendonafter injury. Trends Biotechnol 2007;25:409–416.
76. Smith RK. Mesenchymal stem cell therapy for equine ten-dinopathy. Disabil Rehabil 2008:1–7. [Epub ahead ofprint].
77. Smith RK, Korda M, Blunn GW, et al. Isolation and implan-tation of autologous equine mesenchymal stem cells frombone marrow into the superficial digital flexor tendon as apotential novel treatment. Equine Vet J 2003;35:99–102.
78. Smith RK, Webbon PM. Harnessing the stem cell for thetreatment of tendon injuries: heralding a new dawn? Br JSports Med 2005;39:582–584.
79. Taylor SE, Smith RK, Clegg PD. Mesenchymal stem celltherapy in equine musculoskeletal disease: scientific fact orclinical fiction? Equine Vet J 2007;39:172–180.
80. Herthel DJ. Enhanced suspensory ligament healing in 100horses by stem cells and other bone marrow components, inProceedings. 47th Annual American Association of EquinePractitioners Convention 2001;319–321.
81. Smith JJ, Ross MW, Smith RK. Anabolic affects of acellularbone marrow, platelet rich plasma, and serum on equinesuspensory ligament fibroblasts in vitro. Vet Comp OrthopTraumatol 2006;19:43–47.
afPRP, VetCell Bioscience, Cambridge CB22 3AT, United King-dom.
bVet-Stem, Poway, CA 92064.cBath AP, Unpublished data, 2003.
AAEP PROCEEDINGS � Vol. 54 � 2008 501
IN-DEPTH: TENDON AND LIGAMENT INJURY