telomeres and telomerase in mature b-cell disorders (aging of immune system) ... (hiyama k j immunol...
TRANSCRIPT

Telomeres and telomerase
in mature B-cell disorders
Elisa Genuardi PhD, Torino, Italy, EU

What is my
destiny?

Somatic cell destiny
replicative senescence
MORTAL
mitosis
somatic cells
MORTAL
NECROSIS
APOPTOSIS

TELOMERE
effective sensor of genetic fitness from a dangerous open end
Telomeric DNA and telomere-specific binding
proteins have an essential role in stabilizing
chromosome ends by forming a cap structure that
protects chromosome ends from degradation and
terminal fusions.

Telomeres and Cell Senescence
Adapted from Shay JW and Wright WE, Journal of pathology 2007
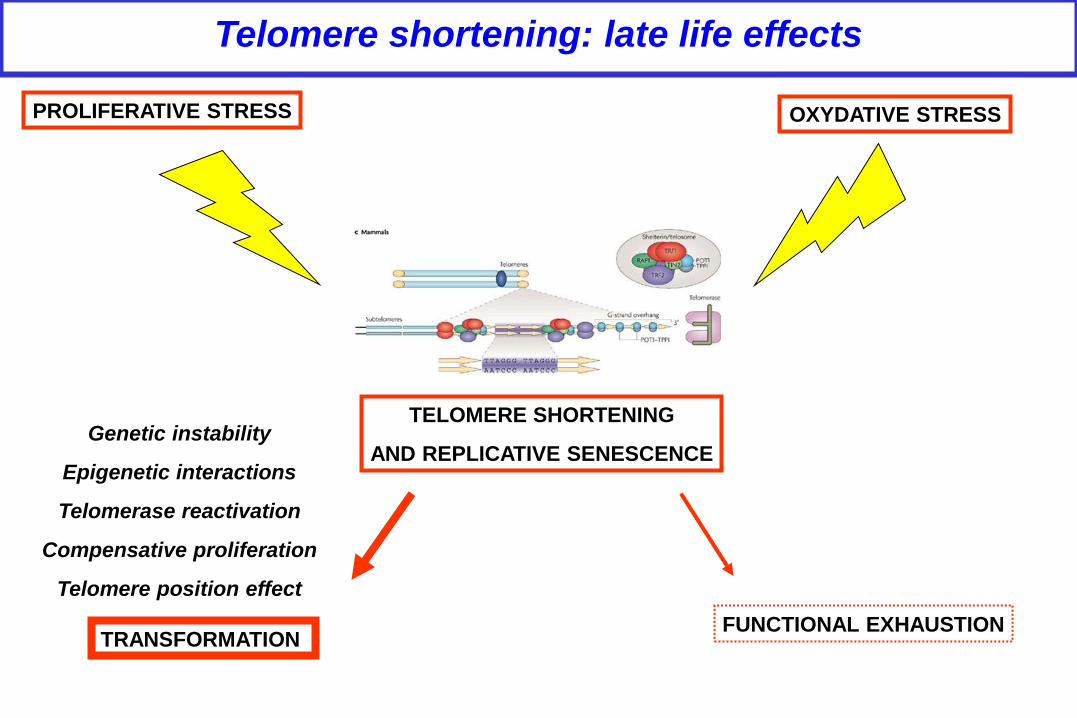
Telomere shortening: late life effects
PROLIFERATIVE STRESS OXYDATIVE STRESS
TELOMERE SHORTENING
AND REPLICATIVE SENESCENCE
FUNCTIONAL EXHAUSTION
Genetic instability
Epigenetic interactions
Telomerase reactivation
Compensative proliferation
Telomere position effect
TRANSFORMATION

Tumor-suppressing function of replicative senescence
replicative senescence
GENETIC INSTABILITY
crisis
MORTAL
mitosis
somatic cells
telomere length Hayflick’s limit
tumor cells
Rb1
p53
IMMORTAL
Telomere stabilization
TELOMERASE ACTIVATION
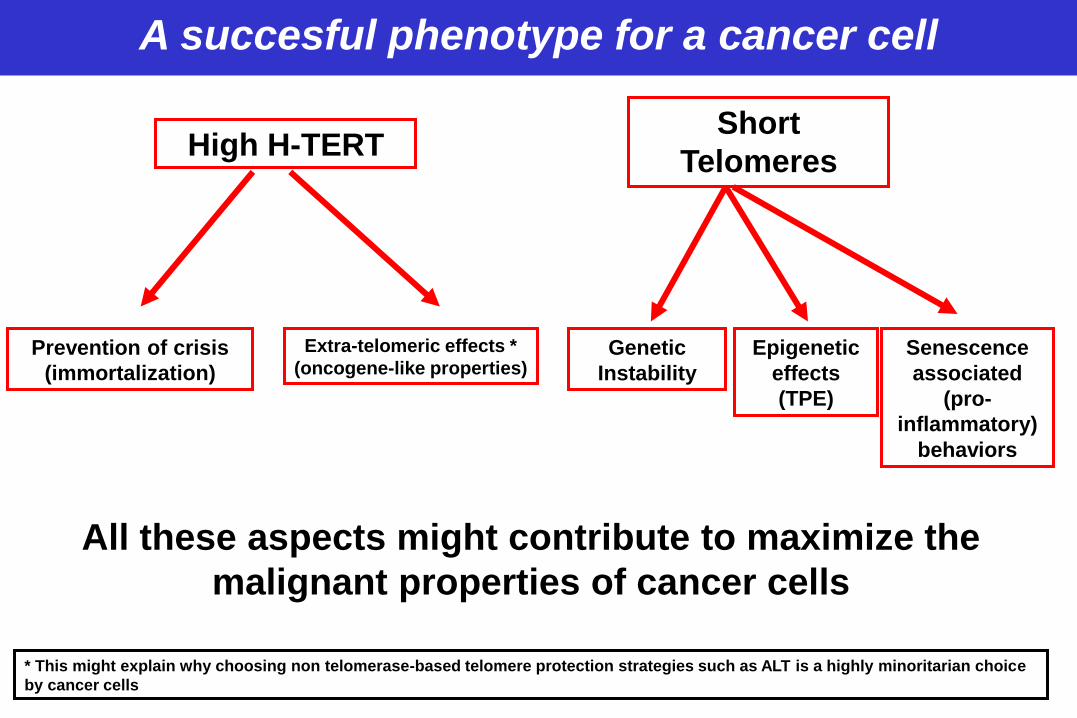
A succesful phenotype for a cancer cell
Short
Telomeres High H-TERT
Prevention of crisis
(immortalization)
Extra-telomeric effects *
(oncogene-like properties) Genetic
Instability
Epigenetic
effects
(TPE)
Senescence
associated
(pro-
inflammatory)
behaviors
* This might explain why choosing non telomerase-based telomere protection strategies such as ALT is a highly minoritarian choice
by cancer cells
All these aspects might contribute to maximize the
malignant properties of cancer cells

Telomerase and escape to cell senescence
SOME TISSUES MUST ESCAPE CELL SENESCENCE TO PERFORM THEIR FUNCTIONS
Germinal cells
Some embryonic tissues
lymphoid cells
Other adult tissues (to a lesser extent)
These “ESCAPE” Mechanisms can (or must) be exploited by tumor cells
Low level of TA
Skvortzov D.A. Acta Naturae 2009

Telomere and telomerase in normal lymphoid compartment
Telomere in B-cell tumours: ALL, MCL, MM
The example of CLL
Telomere and telomerase in lymphoid tumors

Telomere and Telomerase in normal lymphoid compartment
(Aubert G. Physiol Rev. 2008)
telomerase
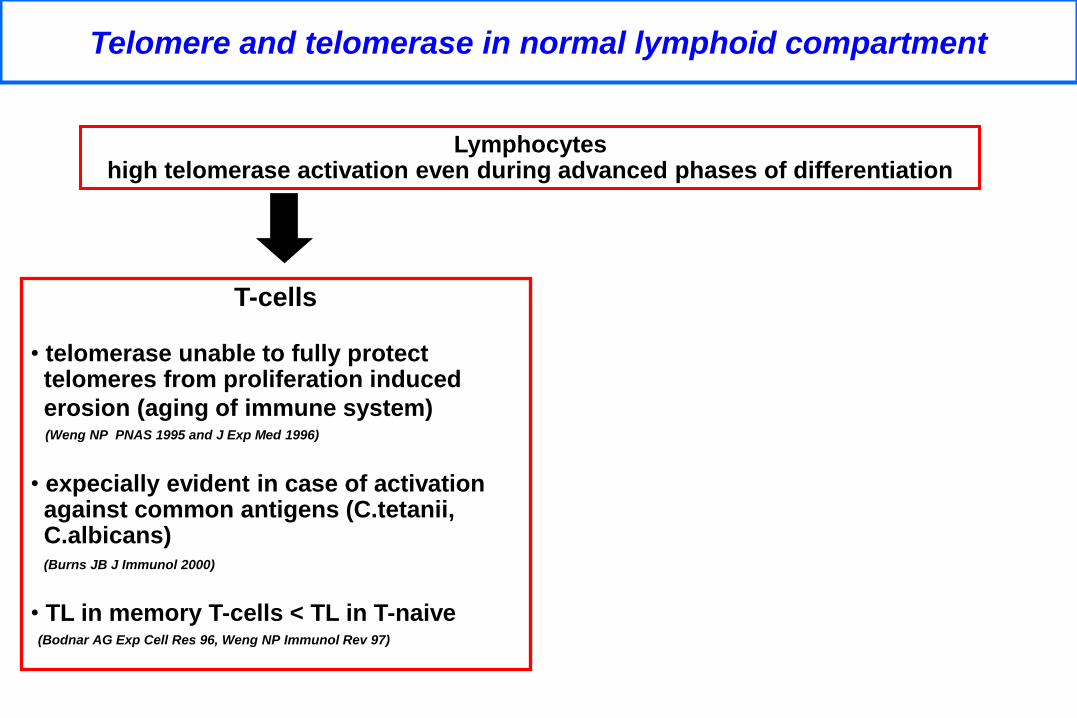
Telomere and telomerase in normal lymphoid compartment
Lymphocytes high telomerase activation even during advanced phases of differentiation
T-cells
• telomerase unable to fully protect telomeres from proliferation induced
erosion (aging of immune system) (Weng NP PNAS 1995 and J Exp Med 1996)
• expecially evident in case of activation against common antigens (C.tetanii, C.albicans) (Burns JB J Immunol 2000)
• TL in memory T-cells < TL in T-naive (Bodnar AG Exp Cell Res 96, Weng NP Immunol Rev 97)

Telomerase and B-cell development
B-cell precursor TA +
naive B-cell TA +/-
memory B-cell TA +/-
extra GC activation TA ++
GC maturation TA +++++
high proliferation
no TL erosion

Telomere and telomerase in normal lymphoid compartment
Lymphocytes high telomerase activation even during advanced phases of differentiation
B-cells
• physiologic age-related shortening lower compared to T-cells (Son NH J Immunol 2000)
• absence of telomere erosion during GC differentiation process (only somatic district where extensive cell prolife- ration occurs without telomeric attrition) (Weng NP PNAS 1997 and Immunity 1998, Hu BT J Immunol 1997)
• TL in memory B-cells≤TLinB-naive (Son NH Mech Ageing Dev 2003)

...However...
TELOMERIC EROSION OCCURS IN LYMPHOCYTES
extra-physiological stressors
• extensive proliferation
• inflammation
• viral infections (i.e. CMV)
• sex hormones
• ROS
• genetic polymporphisms of
telomere related proteins
• mechanisms occurring in
hematopoietic stem cells ageing
• mechanisms associated with
lymphocytes specific functions
physiological mechanisms

Two pathways to cancer
Cancer
Critical telomere shortening
Loose regulation of the senescence checkpoint

Telomere and telomerase in normal lymphoid compartment
Telomere in B-cell tumours
Telomere in mature B-cell disorders: MCL and MM
The example of CLL

TELOMERE in B-CELL TUMOURS
high proliferative and differentiative potential of GC lymphocytes
high TA and TL conservation in GC
telomeric
checkpoint
released
increased risk of neoplastic transformation in GC
B-cell tumours arise frequently in phases with physiological telomerase activation
TELOMERE in B-CELL TUMOURS Telomere in B-cell tumours
(Hiyama K J Immunol 1995, Hodes RJ Immunology 2002)

TL heterogeneity in lymphoproliderative diseases is not related to
patient age
TRF (
bp)
0
2000
4000
6000
8000
10000
12000A B
FL
age (years)
20 30 40 50 60 70 80 90
TRF (
bp)
2000
4000
6000
8000
10000
12000
MZL
age (years)
20 30 40 50 60 70 80 90
TRF (
bp)
2000
4000
6000
8000
10000
12000
r ² = 0.0267
r ² = 0.0103
age (years)
20 30 40 50 60 70 80 90
TRF (
bp)
2000
4000
6000
8000
10000
12000
r ² = 0.2205
MCL
age (years)20 30 40 50 60 70 80 90
TRF (
bp)
2000
4000
6000
8000
10000
12000
BL
MM
age (years)
20 30 40 50 60 70 80 90
TRF (
bp)
2000
4000
6000
8000
10000
12000
MM
age (years)
20 30 40 50 60 70 80 90
TRF (
bp)
2000
4000
6000
8000
10000
12000
DLCL
r ² =0.3949
r ² = 0.0005
r ² = 0.0121
2D Graph 9
age (years)
20 30 40 50 60 70 80 90
TRF (
bp)
2000
4000
6000
8000
10000
12000
all
r ² = 0.0783
CLL
age (years)
20 30 40 50 60 70 80 90
TRF (
bp)
2000
4000
6000
8000
10000
12000
r ² = 0.0891
90th percentile
75th percentile
25th percentile
10th percentile
mean
median
St.Dev.
(Lansdorp P Blood 2008;
Ladetto M Blood 2004)

TL in mature B-cell lymphoproliferative disorders

GC unexp NHL
n° of cell divisions
telomere
shortening
GC-derived NHL GC-lymphomagenesis
pre-GC-lymphomagenesis
Telomere in B-cell tumours
GC unexperienced GC experienced
Healthy B naive 8300 bp 9000bp
Tumor B-cells 3900 bp 7500bp
TL shortening -4400 bp -1500 bp

TL is not a mere histopathogenetic marker
MULTIPLE FACTORS MIGHT INFLUENCE THE TELOMERE STATUS OF LYMPHOID TUMOURS
prolipherative history (number of replication cycles)
histopathogenesis (GC vs non GC experience)
oxidative stress
oncogenes (c-myc)
tumour suppressor genes (ATM)
disease progression (MGUS vs MM)

Telomere and telomerase in normal lymphoid compartment
Telomere in B-cell tumours
Telomere in mature B-cell disorders: MCL and MM
The example of CLL

MCL patients show significantly shorter TL indicating the occurrence of telomere dysfuction
TL and MCL
(Cottliar A. Eur J Haeatol 2009)
(Jebaraj BM, Blood 2013)

In MCL patients TL was not associated with any of clinical or biologic factor rilevant for pathogenesis or prognostication and disease
outcome
(Jebaraj BM, Blood 2013)
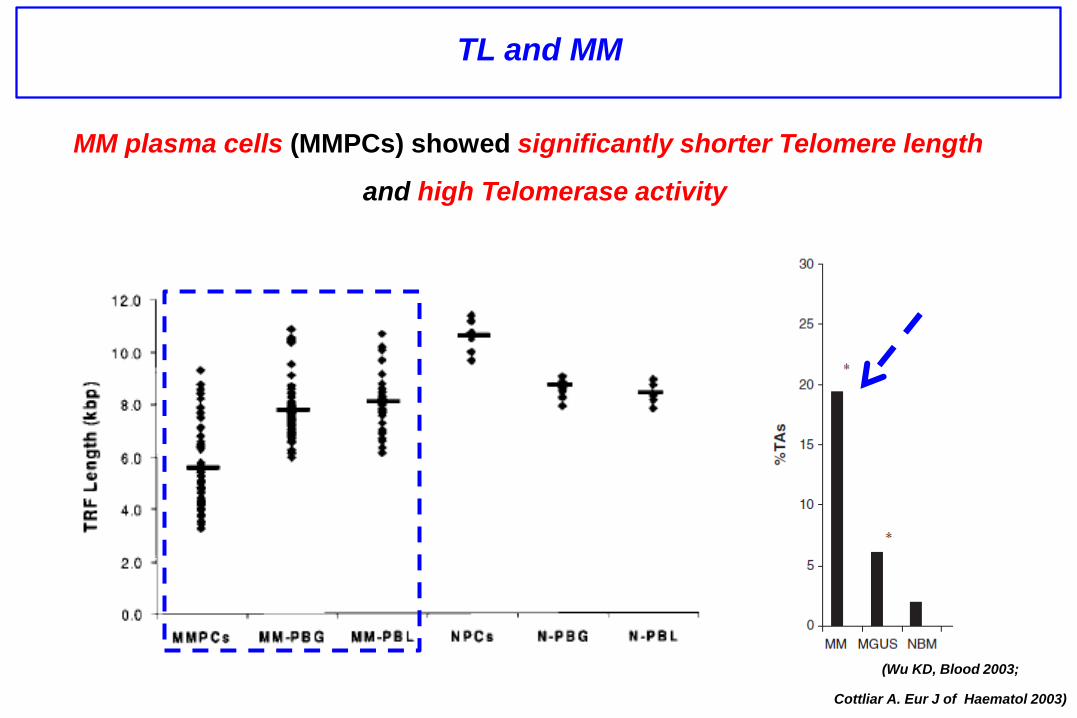
TL and MM
MM plasma cells (MMPCs) showed significantly shorter Telomere length
and high Telomerase activity
(Wu KD, Blood 2003;
Cottliar A. Eur J of Haematol 2003)

Telomere and telomerase in normal lymphoid compartment
Telomere in B-cell tumours
The example of CLL
...Telomere shortening is a crucial event in tumorigenesis but it
isn’tadiseasepredictor....
…INCONTRASTTO….

The example of CLL
PROGNOSTIC BIOMARKERS
Binet status
Genetic abnormalities
IGVH mutational status
p53, CD38, ZAP-70, CD49d
Stratification according to these parameters does not fully explain the
heterogeneity of CLL.
HAS TELOMERE LENGTH A POTENTIAL ROLE IN THE BIOLOGY AND
CLINICAL OUTCOME OF CLL?

Prognostic role of TL in CLL
(Bechter OE Cancer Res 1998)
SHORT TELOMERES ARE ASSOCIATED WITH A WORSE OUTCOME
58 B-CLL pts
median TL 6.0 kb
TL < 6.0 kb associates to inferior OS and Binet
B-C
high TA (TRAP) associates to poor
outcome
TL and TRAP are inversely correlated

Correlation between TL and IGHV-MS
LONG TELOMERES ARE ASSOCIATED TO A VH MUTATED STATUS...
(Hultdin M Br J Cancer 03) (Damle RN Blood 2004)
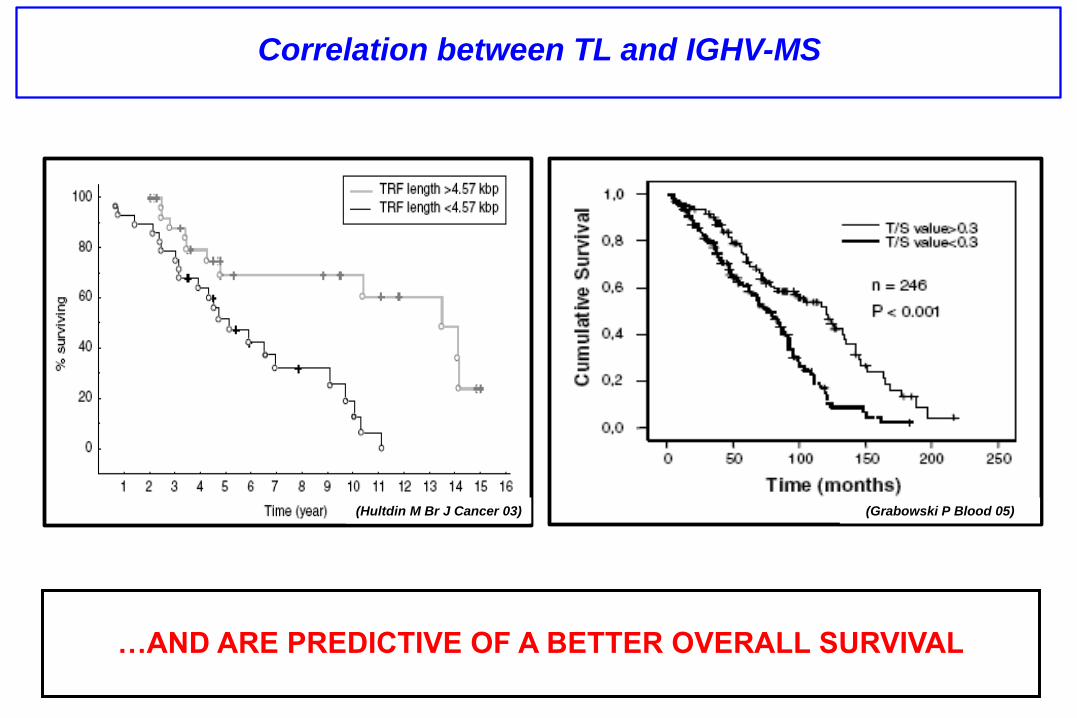
Correlation between TL and IGHV-MS
…ANDAREPREDICTIVEOFABETTEROVERALLSURVIVAL
(Hultdin M Br J Cancer 03) (Grabowski P Blood 05)
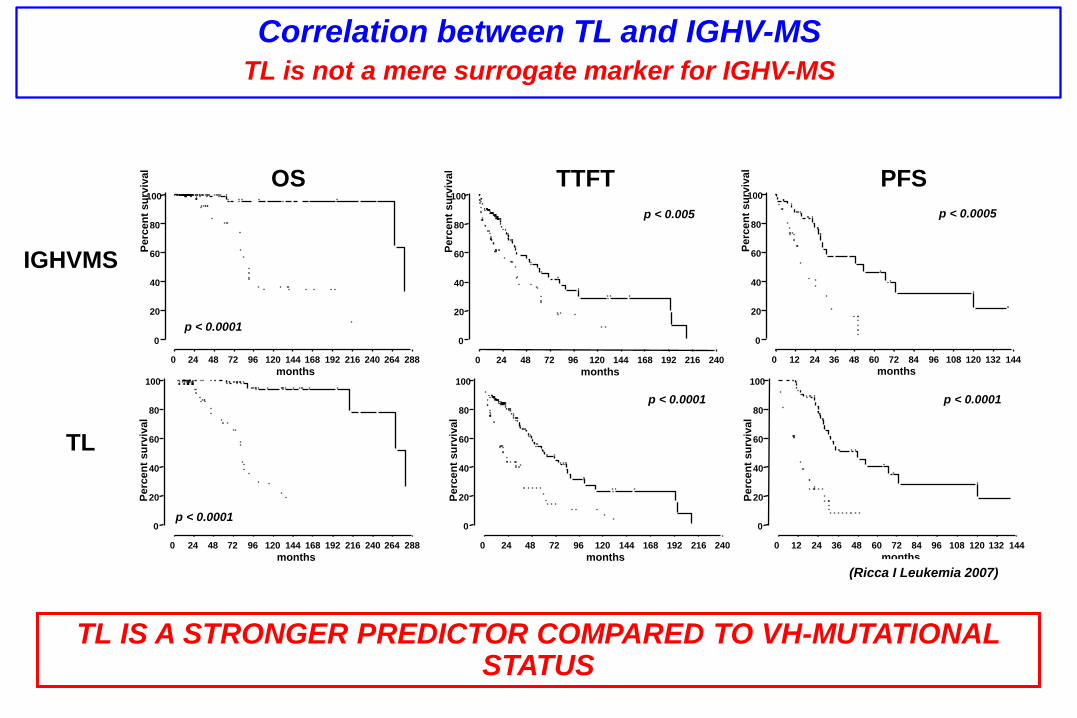
Correlation between TL and IGHV-MS TL is not a mere surrogate marker for IGHV-MS
TL IS A STRONGER PREDICTOR COMPARED TO VH-MUTATIONAL STATUS
0 24 48 72 96 120 144 168 192 216 240 264 288
0
20
40
60
80
100
p < 0.0001
months
Perc
en
t su
rviv
al
0 24 48 72 96 120 144 168 192 216 240
0
20
40
60
80
100
p < 0.0001
months
Perc
en
t su
rviv
al
0 12 24 36 48 60 72 84 96 108 120 132 144
0
20
40
60
80
100
p < 0.0001
months
Perc
en
t su
rviv
al
0 24 48 72 96 120 144 168 192 216 240 264 288
0
20
40
60
80
100
p < 0.0001
months
Perc
en
t su
rviv
al
0 24 48 72 96 120 144 168 192 216 240
0
20
40
60
80
100
p < 0.005
months
Perc
en
t su
rviv
al
0 12 24 36 48 60 72 84 96 108 120 132 144
0
20
40
60
80
100
p < 0.0005
months
Perc
en
t su
rviv
al
IGHVMS
TL
OS TTFT PFS
(Ricca I Leukemia 2007)
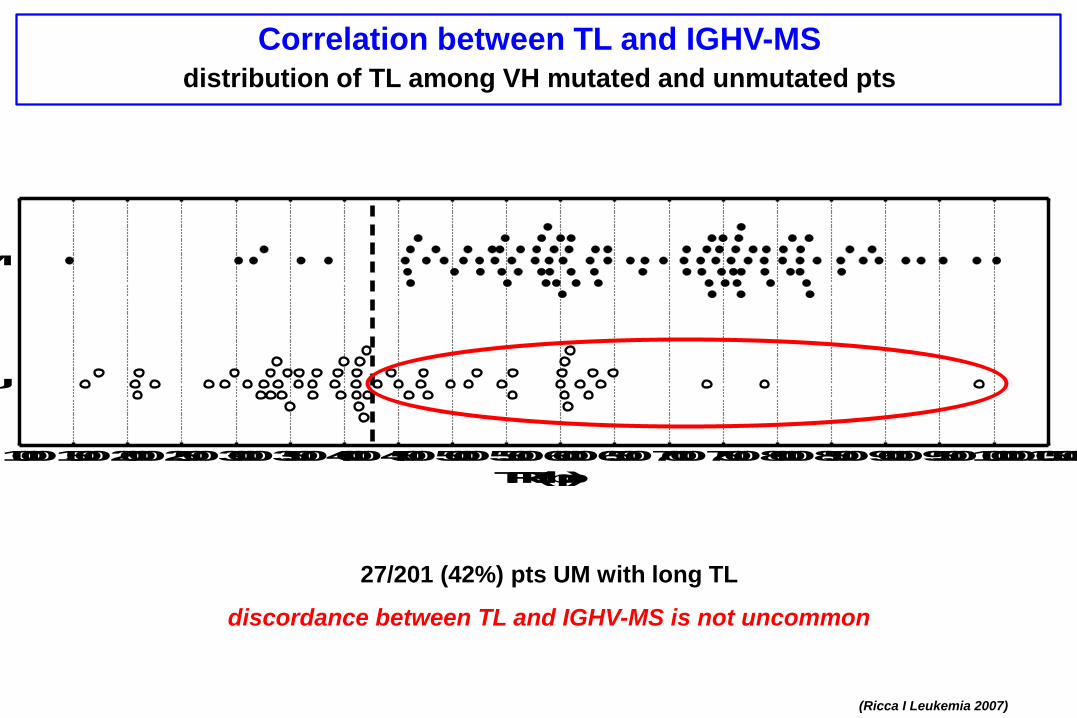
Correlation between TL and IGHV-MS distribution of TL among VH mutated and unmutated pts
1000150020002500300035004000450050005500600065007000750080008500900095001000010500
U
M
TRF (bp)
(Ricca I Leukemia 2007)
27/201 (42%) pts UM with long TL
discordance between TL and IGHV-MS is not uncommon

Correlation between TL and IGHV-MS survival analysis in UM pts according to TL
In discordant cases TL IS A STRONGER PREDICTOR than IGHV-MS
OS PFS
(Ricca I Leukemia 2007)

Shortly telomeres are associated with NOTCH 1 and SF3B1 gene mutations
(Mansouri L, Am J Hematol 2013)

validation on a series of 401 pts
blinded analysis of results
191 pts Turin University
LEARNING SERIES
210 pts Novara Amedeo Avogadro
University
BLINDED
VALIDATION
SERIES
(Rossi D Leukemia 2009)
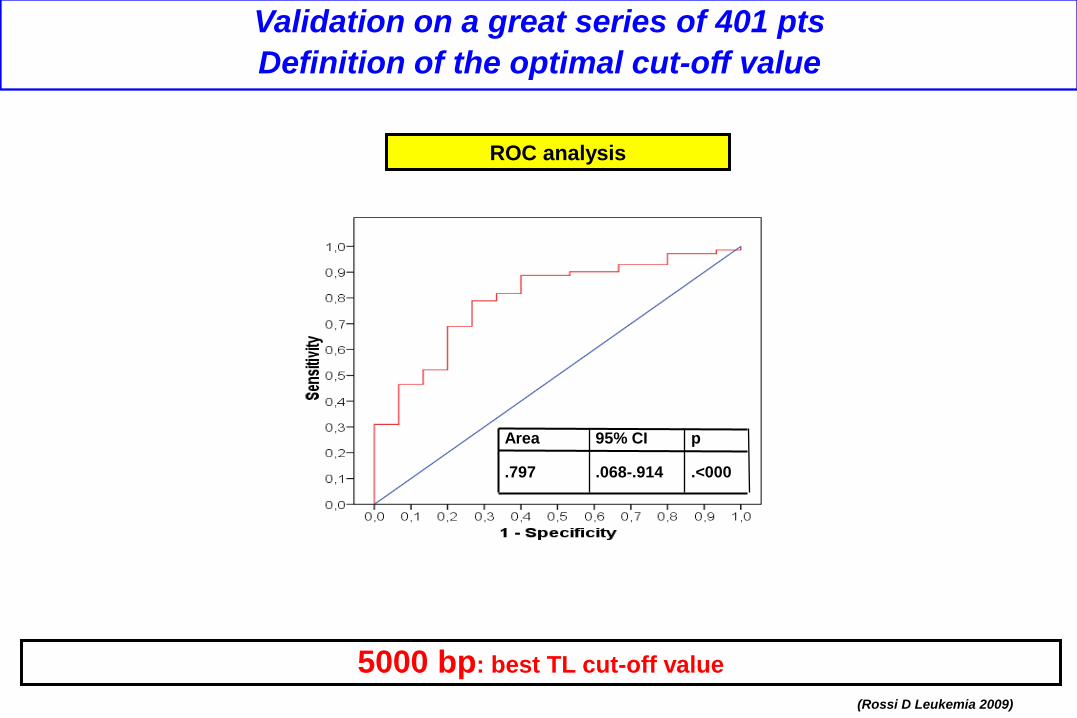
Validation on a great series of 401 pts
Definition of the optimal cut-off value
ROC analysis
5000 bp: best TL cut-off value
(Rossi D Leukemia 2009)
Area 95% CI p
.797 .068-.914 .<000

Confirm the prognostic value of TL in terms of clinical outcome
TFS OS
TL is an independent predictor of TFS and OS
(Rossi D Leukemia 2009)

Prediction of additional outcome events
(Richter Syndrome transformation)
TL is an independent predictor of risk of Richter transformation
(Rossi D Leukemia 2009)

...however data on TL dynamics over time are scant and anedoctal...
study of telomere dynamics during the natural history of CLL

(Sellmann L. Int J Hematol 2011
Mansouri L, Am J Hematol 2013)
Telomere length can predict OS at diagnosis and when measured at the time of follow up

median time between
TL determinations:
42 months
1° TL determination: 88 pts at diagnosis
2° TL determination:
63 pts in WW phase
2° TL determination:
25 pts at relapse
median time between
TL determinations:
56 months
TFS analysis descriptive evaluation of telomere dynamics
over time
(Bernocco E. ASH 2011)
PROGRESSIVE TELOMERE SHORTENING IS PART OF THE NATURAL HISTORY
OF CHRONIC LYMPHOCYTIC LEUKEMIA (CLL) AND IMPACTS CLINICAL
OUTCOME

TL shorten over time compared to baseline
(Bernocco E. ASH 2011)
telomere loss is greater in cases with higher baseline TL (only modest additional erosion in pts with short TL at diagnosis)

MUTATED UNMUTATED
-2000
-1000
0
1000 IgH status p<0.05
YL
(bp
(
whole population
no correlation with available
clinical and biological
parameters except IGHV-MS
MUTATED UNMUTATED
-2000
-1000
0
1000 IgH status p=0.02
YL
(bp
(
WW patients
rapid telomere erosion associates
with IGHV-mutated status and
unfavourable cytogenetics
(Bernocco E. ASH 2011)
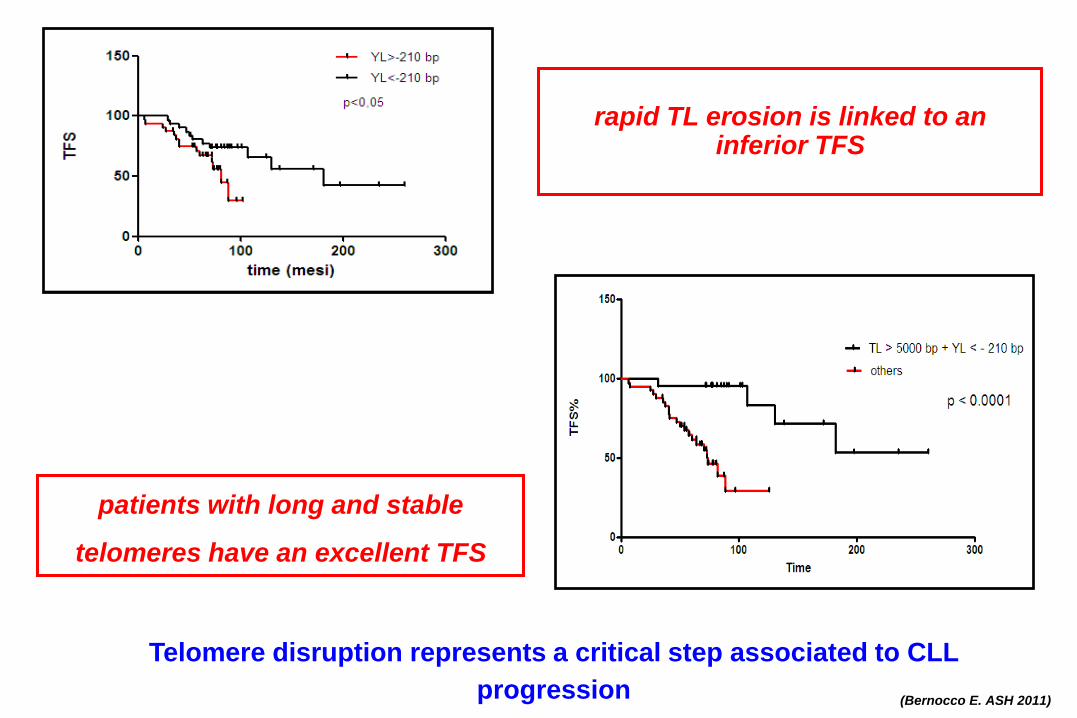
rapid TL erosion is linked to an
inferior TFS
(Bernocco E. ASH 2011)
patients with long and stable
telomeres have an excellent TFS
Telomere disruption represents a critical step associated to CLL
progression
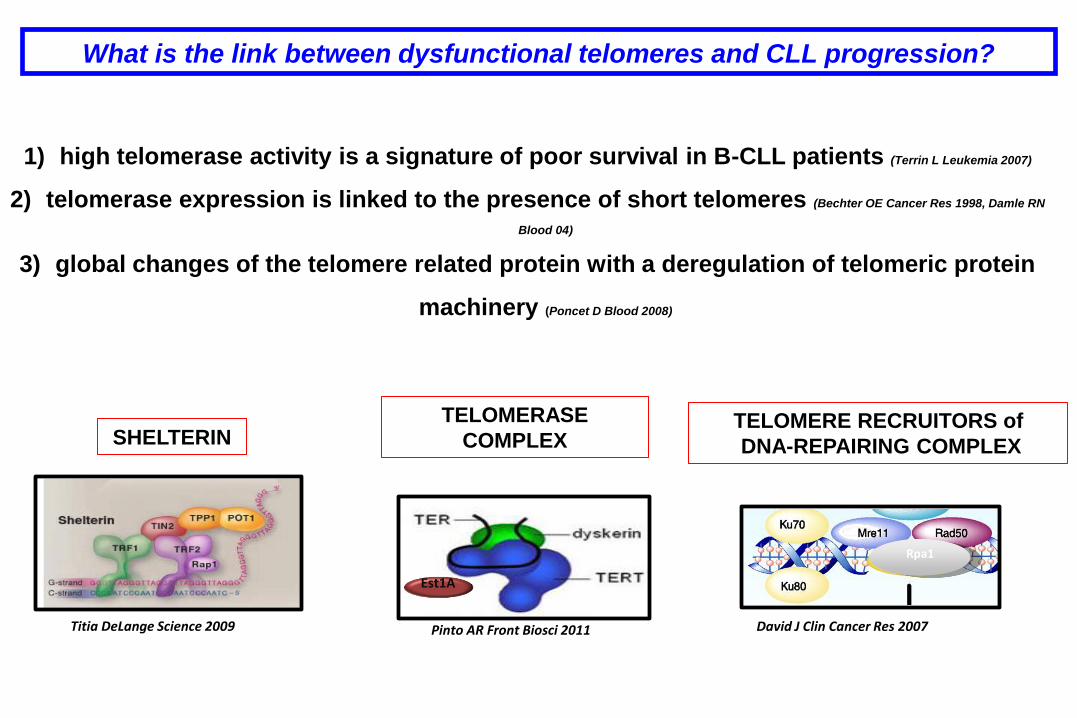
What is the link between dysfunctional telomeres and CLL progression?
1) high telomerase activity is a signature of poor survival in B-CLL patients (Terrin L Leukemia 2007)
2) telomerase expression is linked to the presence of short telomeres (Bechter OE Cancer Res 1998, Damle RN
Blood 04)
3) global changes of the telomere related protein with a deregulation of telomeric protein
machinery (Poncet D Blood 2008)
Titia DeLange Science 2009
Est1A
Pinto AR Front Biosci 2011 David J Clin Cancer Res 2007
Rpa1
SHELTERIN TELOMERASE
COMPLEX TELOMERE RECRUITORS of
DNA-REPAIRING COMPLEX

POT1 mutations cause telomere disfunctions in CLL
POT1 somatic mutation emerged
as the second most frequently
mutated gene
POT1 is exclusively mutated in
IgHV unmutated patients
Telomerase complex dysfunctions
genomic instability and
progression to crisis phase
(Ramsay AJ Nat Genet 2013)

crisis-like phenomena associated with
dysfunctional telomeres play a role in
CLL progression
(Lin TT Blood 2011)

(Lin TT Blood 2011)
Single-molecule Telomere Length Analysis (STELA) revealed:
presence of critically short telomeres was associated with severe genomic instability
(complete telomeric loss events, fusion events and genomic rearrangements in telomeric
regions)

(Lin TT Blood 2011)
DNA sequencing in pts with dysfunctional telomeres telomere fusion shows a characteristic mutational profile
reduced number of TTAGGG repeats subtelomeric deletions
microhomology
...moreover the presence of dysfunctional telomeres was more common BUT NOT EXCLUSIVELY found in
patients with poor prognostic features...
TELOMERIC DYSFUNCTIONS MIGHT BE INVOLVED AT EARLY STAGE OF CLL PROGRESSION


Telomere distrupt, CLL progresses
(Ladetto M, Blood 2010)


Thanksto…
LYMPHOMA unit
Simone Ferrero
Barbara Mantoan
Daniela Barbero
Luigia Monitillo
Daniela Drandi
Roberta Benedetto
Giulia Verardo
Federica Cavallo
Paola Ghione
and the clinical team
Haematology division
UNIVERSITÀ DI TORINO - Prof. Mario Boccadoro
Dott.ssa Paola Omedè
FISH-Cytofluorimetric
Staff
Dott. Roberto Passera
Dott.Marco Ladetto
Dott.ssa Elisa Bernocco