telegroup program bloomfield hospital
TRANSCRIPT
Telegroup Program
Bloomfield Hospital
Evidence Based Practice for Carer Support
Presented by
Bronwyn Hyde (Senior Social Worker)
1
Bronwyn Hyde (Senior Social Worker)
Gill Leonard (Social Worker Rehabilitation)
Outline of Outline of
PresentationPresentation�� Description of the Mental Health Inpatient Description of the Mental Health Inpatient
Rehab UnitsRehab Units
��The Use of Telephone Support GroupsThe Use of Telephone Support Groups
2
��The Use of Telephone Support GroupsThe Use of Telephone Support Groups
�� Carer NeedsCarer Needs
�� Literature Search on Telephone Support GroupsLiterature Search on Telephone Support Groups
�� Social Work and the Mutual Aid Groupwork Social Work and the Mutual Aid Groupwork
ModelModel
�� Evaluation Methodology & Collation of Data Evaluation Methodology & Collation of Data
�� Challenges and Future DirectionsChallenges and Future Directions
Overview of the TGC Overview of the TGC
Program for Program for CarersCarers
•• TGC (TeleGroup Counselling Program) has TGC (TeleGroup Counselling Program) has been part of the inpatient rehabilitation been part of the inpatient rehabilitation service since 2004service since 2004
3
service since 2004service since 2004
•• Carers NSW Carers NSW –– provide TGC programs to all provide TGC programs to all carers and training to staffcarers and training to staff
•• Link up of 6 carers/family members with 2 Link up of 6 carers/family members with 2 facilitators for 1 hour/week over 8 weeksfacilitators for 1 hour/week over 8 weeks
•• Two programs run each year Two programs run each year

Aims of the TGC ProgramAims of the TGC Program
For Carers toFor Carers to
•• Share experiencesShare experiences
•• Reduce feelings of isolationReduce feelings of isolation
•• Create social contactsCreate social contacts•• Create social contactsCreate social contacts
•• Have lived experience acknowledgedHave lived experience acknowledged
•• Gain information and understanding of MH System Gain information and understanding of MH System and mental illnessand mental illness
•• Increase understanding of self in caring roleIncrease understanding of self in caring role
4

Rehabilitation UnitsRehabilitation Units
Bloomfield HospitalBloomfield Hospital
Provide medium to long termProvide medium to long term
rehabilitation to people with anrehabilitation to people with an
5
rehabilitation to people with anrehabilitation to people with an
enduring mental illnessenduring mental illness
ManaraManara ClinicClinic16 Bed Mental Health Inpatient Rehabilitation Unit 16 Bed Mental Health Inpatient Rehabilitation Unit
Bloomfield Hospital (Male)Bloomfield Hospital (Male)

Turon HouseTuron House16 Bed Mental Health Inpatient Rehabilitation Unit 16 Bed Mental Health Inpatient Rehabilitation Unit
Bloomfield Hospital (Female)Bloomfield Hospital (Female)

Carer NeedsCarer Needs
All people who provide care for someoneAll people who provide care for someone
with a chronic physical or mental illnesswith a chronic physical or mental illness
face potentially enormous emotional, face potentially enormous emotional,
8
face potentially enormous emotional, face potentially enormous emotional,
physical and financial consequences.physical and financial consequences.
Carers often report chronic physical andCarers often report chronic physical and
emotional exhaustion, decreased income, emotional exhaustion, decreased income,
stress, isolation and feelings of grief and stress, isolation and feelings of grief and
loss as a result of their role.loss as a result of their role.

Needs of Needs of CarersCarers of People with a of People with a
Mental Illness Mental Illness -- Specific StressorsSpecific Stressors
•• Sometimes dealing with antiSometimes dealing with anti--social, frightening social, frightening behavioursbehaviours
•• Diagnosis is difficult to determine, changeable Diagnosis is difficult to determine, changeable
9
•• Diagnosis is difficult to determine, changeable Diagnosis is difficult to determine, changeable and can take years to formulateand can take years to formulate
•• Treatment options are many but often require Treatment options are many but often require trial and error trial and error –– this and the side effects of this and the side effects of medication often contribute to non compliancemedication often contribute to non compliance
•• Course of the illness is unpredictableCourse of the illness is unpredictable

Needs of Carers of People with a Needs of Carers of People with a
Mental Illness Mental Illness –– Specific stressorsSpecific stressors
•• Person with the illness may not participate in Person with the illness may not participate in treatmenttreatment
•• Carers are often the focus of conflict when relative Carers are often the focus of conflict when relative •• Carers are often the focus of conflict when relative Carers are often the focus of conflict when relative
is unwell is unwell -- increased feelings of guilt, self blame, increased feelings of guilt, self blame,
poor parentingpoor parenting
•• Often feel ostracized from the MH system, not Often feel ostracized from the MH system, not
included in treatment decisionsincluded in treatment decisions
•• Stigma of MI increases sense of isolationStigma of MI increases sense of isolation
10

Needs of Carers of People with a Needs of Carers of People with a
Mental Illness Mental Illness –– Unique stressorsUnique stressors
Carers of people with a mental illness have Carers of people with a mental illness have many unmet needs formany unmet needs for
-- InformationInformation
11
-- InformationInformation
-- Coping strategiesCoping strategies
-- General support General support
(Pagnini 2005, Carer Life Course Framework)(Pagnini 2005, Carer Life Course Framework)

Challenges in Providing Support for Challenges in Providing Support for
Carers Manara/TuronCarers Manara/Turon
•• Catchment area is wide Catchment area is wide –– carers are carers are geographically dispersedgeographically dispersed
12

Challenges in Providing Support for Challenges in Providing Support for
Carers Manara/TuronCarers Manara/Turon
•• FaceFace--toto--face contact is limitedface contact is limited
•• Little or no information about rehab unitLittle or no information about rehab unit
•• Residents may have had little recent contact Residents may have had little recent contact •• Residents may have had little recent contact Residents may have had little recent contact with family members/carerswith family members/carers
•• Relationships with family members may be Relationships with family members may be hostilehostile

Challenges in Delivering Carer Challenges in Delivering Carer
SupportSupportHow to provide for carer needs forHow to provide for carer needs for
-- InformationInformation
-- Coping strategiesCoping strategies
-- General supportGeneral support-- General supportGeneral support
to this carer populationto this carer population
Are telephone support groups providingAre telephone support groups providing
for these needs? for these needs?
14
Literature SearchLiterature Search
Teleconferencing format has been used for theTeleconferencing format has been used for thefollowing populationsfollowing populations
•• Persons living with HIV/AIDS in rural areas and Persons living with HIV/AIDS in rural areas and their carerstheir carers
15
their carerstheir carers
•• Carers of people living with dementia, ofCarers of people living with dementia, ofstroke survivors, of Alzheimer sufferers, of adults stroke survivors, of Alzheimer sufferers, of adults with brain injurywith brain injury

Literature Search cont'Literature Search cont'
•• WomenWomen with breast cancerwith breast cancer
•• Women with spinal cord injury in rural & Women with spinal cord injury in rural & remote areas remote areas
16
remote areas remote areas
•• Parents of children with chronic conditions Parents of children with chronic conditions
•• Caregivers of adults with brain injuryCaregivers of adults with brain injury

Literature SearchLiterature Search
These and other studies also cite use of These and other studies also cite use of telephone groups for the following telephone groups for the following populationspopulations
17
populationspopulations
-- Persons with diabetes, multiple sclerosis, Persons with diabetes, multiple sclerosis, hemophilia, cardiac conditions hemophilia, cardiac conditions
-- People who are housebound such as the People who are housebound such as the elderly, blind and severely disabledelderly, blind and severely disabled
Literature SearchLiterature Search
•• The literature indicates that telephone support groups The literature indicates that telephone support groups are an effective way of providing support and are an effective way of providing support and information to carers of people with a chronic illness information to carers of people with a chronic illness AND to the sufferers of a chronic illness.AND to the sufferers of a chronic illness.
•• Telephone groups are an effective way of linking people Telephone groups are an effective way of linking people who are geographically isolated and those who are who are geographically isolated and those who are socially isolated or housebound due to illness, old age socially isolated or housebound due to illness, old age or caring responsibilitiesor caring responsibilities
18

Literature SearchLiterature Search
•• Several studies have confirmed that nothing is Several studies have confirmed that nothing is lost therapeutically when a telephone group is lost therapeutically when a telephone group is used in preference to a faceused in preference to a face--toto--face group.face group.
(Rosswurm, Larrabee & Zhang 2002; Hartke & King 2003; Martindale(Rosswurm, Larrabee & Zhang 2002; Hartke & King 2003; Martindale--Adams, Adams, Nichols, Burns & Malone 2002)Nichols, Burns & Malone 2002)

Literature SearchLiterature Search
•• There was only one study found outlining the There was only one study found outlining the use of telephone groups specifically for carers use of telephone groups specifically for carers of people with a chronic mental illness of people with a chronic mental illness
20
of people with a chronic mental illness of people with a chronic mental illness (Pagnini 2005)(Pagnini 2005)
•• The subject of this paper The subject of this paper -- the evaluation of the evaluation of TGC program for carers of residents of a TGC program for carers of residents of a rural mental health inpatient facility is adding rural mental health inpatient facility is adding to best practice knowledgeto best practice knowledge

Models of telephone Models of telephone
group workgroup work
21
group workgroup work

For carers, groups provide For carers, groups provide
(Shanley 2008)(Shanley 2008)
Problem solving Problem solving Emotion Emotion
coping Support coping Support focussed focussed coping Support coping Support focussed focussed
copingcoping
22

Theme centred interactional modelTheme centred interactional model(Reagan 1997)(Reagan 1997)
•• This modelThis model’’s proponents see as one of its major s proponents see as one of its major
contribution the explicit attention given to both the contribution the explicit attention given to both the
emotionalemotional--experientialexperiential--interactional aspects on the one interactional aspects on the one
hand (the hand (the ‘‘II’’ and the and the ‘‘WeWe’’), and to the group), and to the group’’s cognitive s cognitive
23
hand (the hand (the ‘‘II’’ and the and the ‘‘WeWe’’), and to the group), and to the group’’s cognitive s cognitive
tasktask--learning function on the other (the learning function on the other (the ‘‘ItIt’’))
Mutual Aid Model (Schulman)Mutual Aid Model (Schulman)
““this is a helping system in which clients need each other as this is a helping system in which clients need each other as
well as the worker. This need to use each other, to create well as the worker. This need to use each other, to create
not one but many helping relationships, is a vital not one but many helping relationships, is a vital
ingredient of the group process and constitutes a need ingredient of the group process and constitutes a need
24
ingredient of the group process and constitutes a need ingredient of the group process and constitutes a need
over and above the specific tasks for which the group was over and above the specific tasks for which the group was
formedformed”” (Schwartz 1961)(Schwartz 1961)
““what I got from this was a sense of belonging, being able to what I got from this was a sense of belonging, being able to
share experiences with people who have gone through the share experiences with people who have gone through the
same type of problemsame type of problem””..

Mutual AidMutual Aid
AntiAnti--oppressive practiceoppressive practice
•• EmpowermentEmpowerment
•• Relinquishing of powerRelinquishing of power•• Relinquishing of powerRelinquishing of power
•• Power vs time restraintsPower vs time restraints
25

Mutual Aid model central to Mutual Aid model central to
Social WorkSocial Work•• Steinberg (2010) believes concept of mutual aid Steinberg (2010) believes concept of mutual aid is unique to Social Work group practiceis unique to Social Work group practice
•• Argues that mutual aid Argues that mutual aid is is groupworkgroupwork
•• Mutual aid is holistic, strengthsMutual aid is holistic, strengths--driven and has driven and has •• Mutual aid is holistic, strengthsMutual aid is holistic, strengths--driven and has driven and has exceptional goodness of fit with antiexceptional goodness of fit with anti--oppressive oppressive practice and with the recovery model of mental practice and with the recovery model of mental health practicehealth practice

Social Workers as group Social Workers as group
facilitatorsfacilitatorsSupporting Carers Through Telephone Mediated Group Programs: Supporting Carers Through Telephone Mediated Group Programs:
Opportunities for Gerontological Social Workers (Shanley 2008Opportunities for Gerontological Social Workers (Shanley 2008))
•• Social Workers are part of the multi Social Workers are part of the multi disciplinary team and disciplinary team and
27
disciplinary team and disciplinary team and
•• providing support to carers is part of the providing support to carers is part of the Social work role within that team andSocial work role within that team and
•• Group facilitation is a core skill for Social Group facilitation is a core skill for Social WorkersWorkers
Why TeleGroups for carers of people Why TeleGroups for carers of people
with a Mental Illness?with a Mental Illness?
The purpose as identified in the literature is to The purpose as identified in the literature is to provide carers withprovide carers with
EducationEducation
28
EducationEducation
Support Support
Therapy Therapy
Education Support Therapy Education Support Therapy

Use of the telephone to run groupsUse of the telephone to run groups
•• The telephone is accessible to a wide range of The telephone is accessible to a wide range of peoplepeople
•• Enables people to participate who would not Enables people to participate who would not
29
•• Enables people to participate who would not Enables people to participate who would not otherwise be able to attend a groupotherwise be able to attend a group

Advantages of Telephone group Advantages of Telephone group
counselling (Shanley, 2008)counselling (Shanley, 2008)
1.1. Ease of accessEase of access
2.2. Reduces isolationReduces isolation
3.3. AnonymityAnonymity
30
3.3. AnonymityAnonymity
4.4. Time management Time management
5.5. Ease of useEase of use
6.6. Change of locationChange of location

Disadvantages of tele group Disadvantages of tele group
counselling (Shanley 2004)counselling (Shanley 2004)
1.1. Skilled facilitators neededSkilled facilitators needed
2.2. IntenseIntense
3.3. Challenge to Keep people interestedChallenge to Keep people interested
31
3.3. Challenge to Keep people interestedChallenge to Keep people interested
4.4. Lack of Non verbal cuesLack of Non verbal cues
5.5. Size of group needs to be limitedSize of group needs to be limited
6.6. Care recipient needsCare recipient needs

The Carer Life Course The Carer Life Course
FrameworkFramework
•• An EvidenceAn Evidence--Based Approach to Effective Based Approach to Effective Carer Education and Support (Pagnini 2005) Carer Education and Support (Pagnini 2005) noted definable phases within the caring rolenoted definable phases within the caring rolenoted definable phases within the caring rolenoted definable phases within the caring role
•• We found these stages significant in our We found these stages significant in our facilitation of the TGC program in the facilitation of the TGC program in the rehabilitation unitsrehabilitation units
32
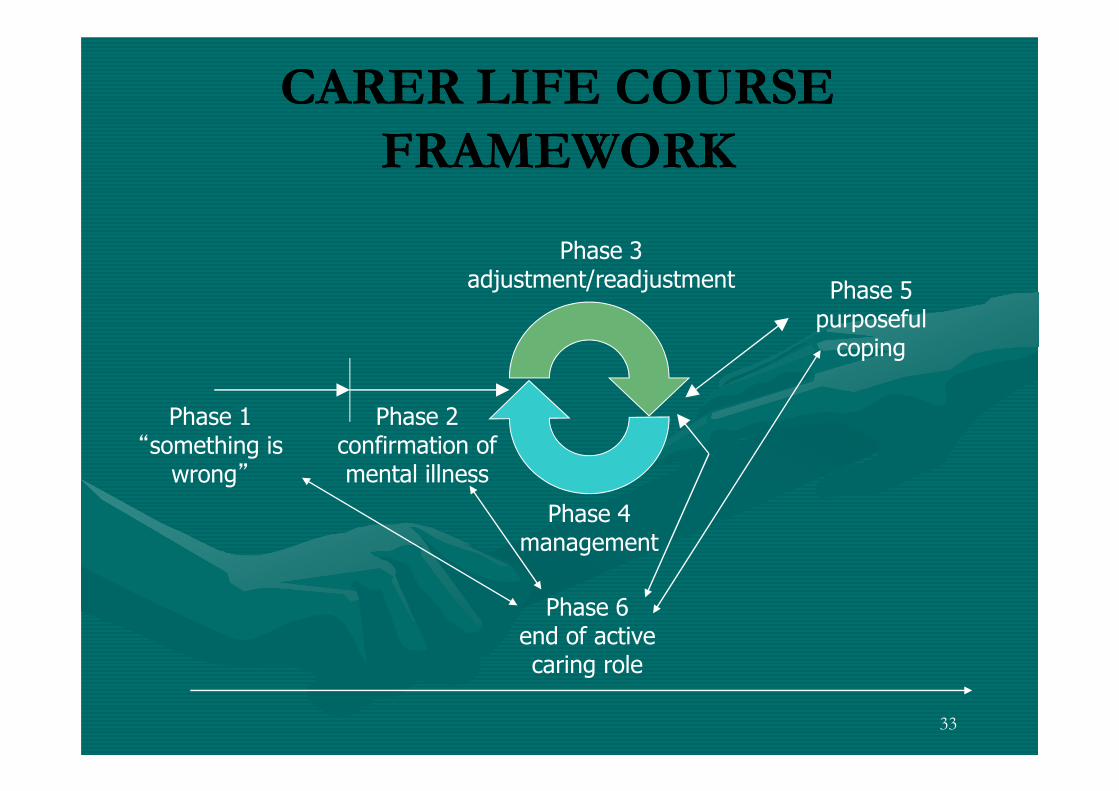
CARER LIFE COURSE CARER LIFE COURSE
FRAMEWORKFRAMEWORK
Phase 3 adjustment/readjustment Phase 5
purposeful coping
33
Phase 1“something is wrong”
Phase 2confirmation of mental illness
Phase 4 management
Phase 6end of active caring role

Collation of Data from Collation of Data from
Evaluations 2004Evaluations 2004--20102010

Number of TGC ProgramsNumber of TGC Programs
YearYear No. of ParticipantsNo. of Participants2004 (1x session)2004 (1x session) 66
2005 (2x sessions)2005 (2x sessions) 1111
2006 (2x sessions)2006 (2x sessions) 1212
2007 (2x sessions) 2007 (2x sessions) 1111
2008 (2x sessions)2008 (2x sessions) 1010
2010 (1x session)2010 (1x session) 66
TOTALTOTAL 5656
35
Evaluation MethodEvaluation Method
•• Registration form serves as a pre program surveyRegistration form serves as a pre program survey
•• Post program evaluation form completed at the Post program evaluation form completed at the end of the 8 weeksend of the 8 weeks
•• Overall evaluation consists of a combination of Overall evaluation consists of a combination of •• Overall evaluation consists of a combination of Overall evaluation consists of a combination of qualitative and quantitative data with majority of qualitative and quantitative data with majority of questions relying on subjective self reporting questions relying on subjective self reporting and measures of caregiver burdenand measures of caregiver burden
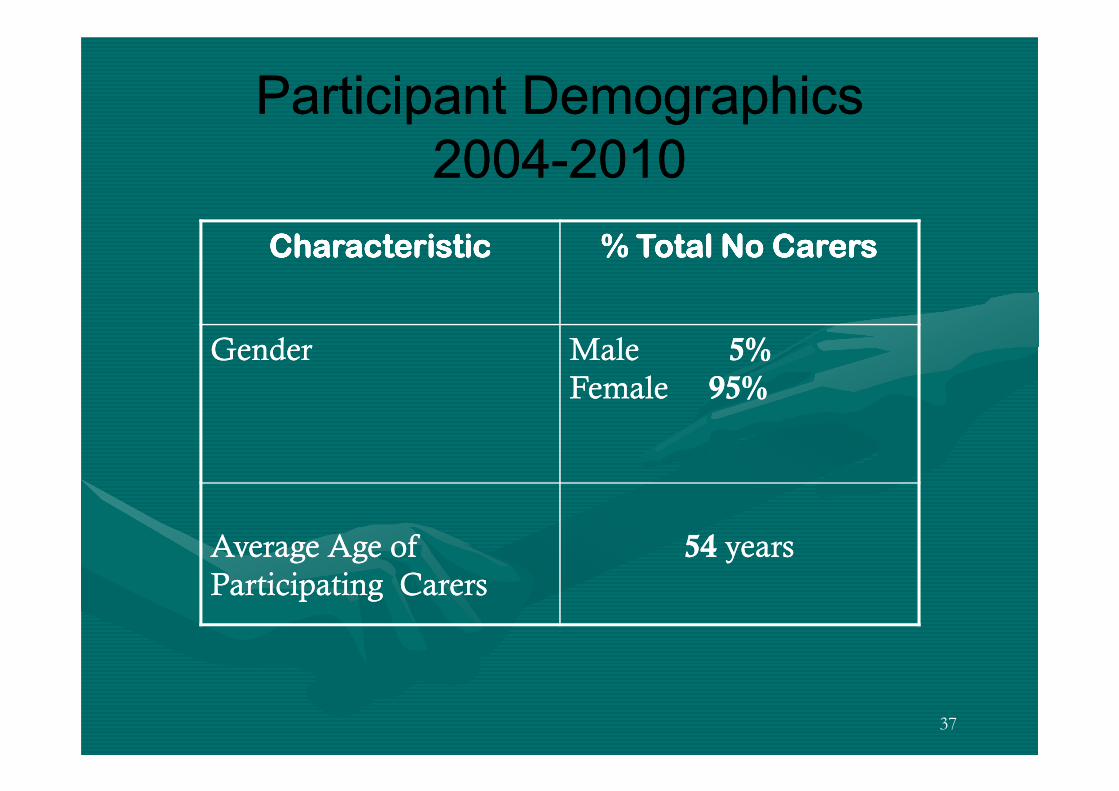
Participant DemographicsParticipant Demographics
20042004--20102010
CharacteristicCharacteristicCharacteristicCharacteristicCharacteristicCharacteristicCharacteristicCharacteristic % Total No Carers% Total No Carers% Total No Carers% Total No Carers% Total No Carers% Total No Carers% Total No Carers% Total No Carers
GenderGender Male Male 5%5%
Female Female 95%95%
37
Female Female 95%95%
Average Age of Average Age of
Participating CarersParticipating Carers
5454 yearsyears

Participant DemographicsParticipant Demographics
20042004--20102010To whom assistance isTo whom assistance is
being providedbeing provided
DaughterDaughter 47%47%
SonSon 42%42%
SiblingSibling 5%5%
Ages of those beingAges of those being
cared forcared for
<18<18 8%8%
1818--2525 28%28%
2626--4545 56%56%SiblingSibling 5%5%
NieceNiece 2%2%
StepmotherStepmother 2%2%
GranddaughterGranddaughter 2%2%
2626--4545 56%56%
4646--6464 8%8%
38
DiagnosisDiagnosis
•• Overwhelming majority had been diagnosed Overwhelming majority had been diagnosed with schizophreniawith schizophrenia
•• Anxiety and depression were next most Anxiety and depression were next most common diagnoses (often in conjunction with common diagnoses (often in conjunction with common diagnoses (often in conjunction with common diagnoses (often in conjunction with schizophrenia)schizophrenia)
•• Other diagnoses included schizoaffective, Other diagnoses included schizoaffective, PTSD, Bipolar Disorder and Borderline PTSD, Bipolar Disorder and Borderline Personality DisorderPersonality Disorder
39

Participant DemographicsParticipant Demographics
Place of ResidencePlace of Residence
20042004--20102010
SydneySydney 40%40% GWAHS GWAHS –– local health local health
areaarea
38%38%
South CoastSouth Coast 6%6% North CoastNorth Coast 3%3%South CoastSouth Coast 6%6% North CoastNorth Coast 3%3%
GSAHS GSAHS –– Greater Greater
Southern AHSSouthern AHS
3%3% NewcastleNewcastle 2%2%
Blue MtnsBlue Mtns 2%2% QueenslandQueensland 2%2%
TasmaniaTasmania 2%2% ACTACT 2%2%
40

Structure of TGC ProgramStructure of TGC Program
•• Each session is structured and time limitedEach session is structured and time limited
•• Carers select topicsCarers select topics
•• Two facilitators and one Two facilitators and one ‘‘observerobserver’’
•• Newsletter sent out after each sessionNewsletter sent out after each session•• Newsletter sent out after each sessionNewsletter sent out after each session
41

Reasons for participating in TGC Reasons for participating in TGC -- Pre Pre
Program Program (Registrations 2004 (Registrations 2004 –– 2010 as % total responses)2010 as % total responses)
42
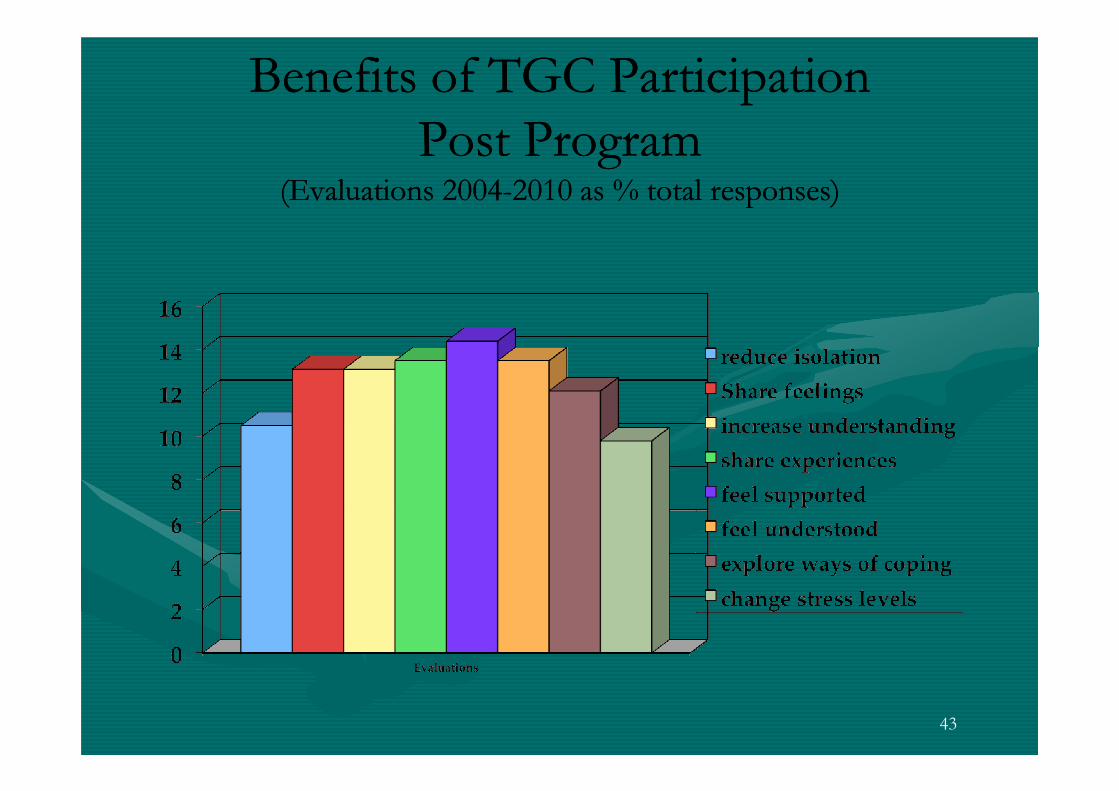
Benefits of TGC ParticipationBenefits of TGC Participation
Post ProgramPost Program(Evaluations 2004(Evaluations 2004--2010 as % total responses)2010 as % total responses)
43

Comparison Comparison ––reasons for participation and reasons for participation and
perceived benefitsperceived benefits(Pre and Post comments as % total responses)(Pre and Post comments as % total responses)
44

Comparison of Pre & Post Comparison of Pre & Post
Program DataProgram Data•• Comparisons of reasons for participating in the Comparisons of reasons for participating in the program [as identified in the registration form] program [as identified in the registration form] with the perceived benefits [as noted in the post with the perceived benefits [as noted in the post program evaluation] reflected a shift away from program evaluation] reflected a shift away from program evaluation] reflected a shift away from program evaluation] reflected a shift away from a psychoeducational focus to a mutual aid focusa psychoeducational focus to a mutual aid focus

Carer Statement of own health & Carer Statement of own health &
wellbeing (2004wellbeing (2004--2010)2010)
ExcellentExcellent Very Very
GoodGood
GoodGood FairFair PoorPoor
Pre Pre
ParticipationParticipation
9.8%9.8% 7.8%7.8% 29.6%29.6% 47%47% 5.8%5.8%
ParticipationParticipation(% completed(% completed
Registrations N=51)Registrations N=51)
Post Post
ParticipationParticipation(% completed evaluations (% completed evaluations
N=45)N=45)
13.3%13.3% 20%20% 40%40% 20%20% 6.7%6.7%
46

Carer Statement of own health & Carer Statement of own health &
wellbeing (2004wellbeing (2004--2010)2010)•• Over the six years of the TGC carers have consistently Over the six years of the TGC carers have consistently rated a significant improvement in their health and rated a significant improvement in their health and wellbeing from pre program ratings to post program wellbeing from pre program ratings to post program ratingsratings
•• Strongly suggests that programs like the TGC based on Strongly suggests that programs like the TGC based on •• Strongly suggests that programs like the TGC based on Strongly suggests that programs like the TGC based on a mutual aid model can significantly contribute to a mutual aid model can significantly contribute to lessening the degree of carer burdenlessening the degree of carer burden
47

Qualitative DataQualitative Data
What did you like most about the TGC?What did you like most about the TGC?
ThemesThemes
•• Sharing of experiences & knowledgeSharing of experiences & knowledge
•• Break down isolationBreak down isolation•• Break down isolationBreak down isolation
•• Listening to othersListening to others
•• Anonymous Anonymous -- easier to talk over the phone, high easier to talk over the phone, high level of trust, can be honest without being level of trust, can be honest without being judged or embarrassedjudged or embarrassed
48

Qualitative DataQualitative Data
•• ““Good to have opportunity to share Good to have opportunity to share experiences…also helped to break the isolation experiences…also helped to break the isolation for people living in small communitiesfor people living in small communities””
•• ““Made it easier to talk when not face to faceMade it easier to talk when not face to face””•• ““Made it easier to talk when not face to faceMade it easier to talk when not face to face””
•• ““All anonymous. Nobody can judge (also All anonymous. Nobody can judge (also physically)physically)””
49
Qualitative DataQualitative Data
What did you like least about the TGC?What did you like least about the TGC?
ThemesThemes
•• Not long enough (each session and the program)Not long enough (each session and the program)
•• Would like less structure and more opportunities to Would like less structure and more opportunities to talk, more problem solvingtalk, more problem solvingWould like less structure and more opportunities to Would like less structure and more opportunities to talk, more problem solvingtalk, more problem solving
•• High emotional content (but easier over the phone, High emotional content (but easier over the phone, beneficial), difficult to hear othersbeneficial), difficult to hear others’’ storiesstories
•• FaceFace--toto--face meetingface meeting
50

Qualitative DataQualitative Data
•• ““Shortness of it. Just get used to it/barriers Shortness of it. Just get used to it/barriers
down/comfortable,OK and now itdown/comfortable,OK and now it’’s overs over””
•• ““…having to hear from others that children are not …having to hear from others that children are not
getting better getting better –– made me very upset because I like to made me very upset because I like to getting better getting better –– made me very upset because I like to made me very upset because I like to
think things will get betterthink things will get better””
•• ““Hearing other peopleHearing other people’’s stories and the length of time s stories and the length of time
they had been caring made me realise this will be the they had been caring made me realise this will be the
rest of my liferest of my life””
51

Qualitative DataQualitative Data
The theme regarding high emotional content thatThe theme regarding high emotional content that
emerged appears to be unique to telephoneemerged appears to be unique to telephone
support groups with carers of people with asupport groups with carers of people with a
mental illnessmental illnessmental illnessmental illness
•• Difficulty hearing otherDifficulty hearing other’’s stories about length s stories about length of time caringof time caring
•• Difficulty retaining hope when hearing of Difficulty retaining hope when hearing of
othersothers’’ relatives not getting betterrelatives not getting better
52

Living GriefLiving Grief
These findings seem to reinforce theThese findings seem to reinforce the
notion of notion of ‘‘living griefliving grief’’ that carers ofthat carers of
people with a mental illness experience.people with a mental illness experience.
The episodic nature of mental illnessThe episodic nature of mental illness
creates difficulties for carers in retainingcreates difficulties for carers in retaining
hope. Raises issue of what is meant byhope. Raises issue of what is meant by
‘‘recoveryrecovery’’
53
Implications for TGCs with Implications for TGCs with
Carers of People with MICarers of People with MI•• Need for awareness about stages of caring for Need for awareness about stages of caring for each participanteach participant
•• Need for sensitivity about the impact of the Need for sensitivity about the impact of the sharing of experiencessharing of experiencessharing of experiencessharing of experiences
•• Inclusion of discussion about hope and recoveryInclusion of discussion about hope and recovery
54

Continuing challenges and shortcomingsContinuing challenges and shortcomings
•• ChallengesChallenges
–– Completion of paperworkCompletion of paperwork
–– Carers at different stages in their journeyCarers at different stages in their journey
–– Maintaining hopeMaintaining hope
55
–– High emotional content in a strict time limited sessionHigh emotional content in a strict time limited session
•• Short comingsShort comings
–– Not long enoughNot long enough
–– Ending is too abruptEnding is too abrupt
–– Recruitment of carersRecruitment of carers
–– Including other disciplinesIncluding other disciplines

Estimated Costs of TGCEstimated Costs of TGC(Pagnini 2006. Carers Mental Health Project Final Evaluation Report August 2001(Pagnini 2006. Carers Mental Health Project Final Evaluation Report August 2001--
June 2004)June 2004)
ItemItem CostCost•• Recruitment of participants, telephone calls, other prep Recruitment of participants, telephone calls, other prep
(15hrs @ $25.00)(15hrs @ $25.00)
•• 2 facilitators 2 facilitators –– prepre--session prep, post course debriefing session prep, post course debriefing
$375.00$375.00
560.00560.00•• 2 facilitators 2 facilitators –– prepre--session prep, post course debriefing session prep, post course debriefing after each session ($35.00 x 1 hour x 8 x 2 facilitators)after each session ($35.00 x 1 hour x 8 x 2 facilitators)
•• Facilitation time Facilitation time -- $35.00 x 1 hour session x 8 sessions x 2 $35.00 x 1 hour session x 8 sessions x 2 facilitatorsfacilitators
•• Telstra telelink charges Telstra telelink charges –– average $80 per session x 8 average $80 per session x 8 sessionssessions
560.00560.00
560.00560.00
640.00640.00
TOTAL all costsTOTAL all costs $2,135.00$2,135.00
Unit cost per participant (based on 8 participants)Unit cost per participant (based on 8 participants) $267.00$267.0056

SummarySummary
•• Challenges in the provision of structured Challenges in the provision of structured support for family members of residents of a support for family members of residents of a rural inpatient rehabilitation facilityrural inpatient rehabilitation facility
•• Evidence based practice supports the use of Evidence based practice supports the use of telephone mediated support groupstelephone mediated support groups
•• TGC initiated in response to these challenges TGC initiated in response to these challenges and run over six yearsand run over six years
•• Mutual aid model of groupwork on which the Mutual aid model of groupwork on which the TGC is based fits well with antiTGC is based fits well with anti--oppressive oppressive practice and recovery principlespractice and recovery principles

SummarySummary
•• Data from evaluations indicate a possible Data from evaluations indicate a possible correlation between participation in TGC correlation between participation in TGC program and an increase in program and an increase in carercarer perception of perception of improved health and well beingimproved health and well beingimproved health and well beingimproved health and well being
•• The data confirmed findings from other studies The data confirmed findings from other studies that the therapeutic elements of facethat the therapeutic elements of face--toto--face face groupworkgroupwork are not lost in telephone mediated are not lost in telephone mediated groupsgroups

SummarySummary
•• In mental health more than in other areas of In mental health more than in other areas of health care delivery the sharing of experiences health care delivery the sharing of experiences alone does not alone equate to mutual aid. alone does not alone equate to mutual aid. Facilitators need to be mindful of notion of Facilitators need to be mindful of notion of Facilitators need to be mindful of notion of Facilitators need to be mindful of notion of ‘‘living griefliving grief’’
•• Social workers have the required skills to Social workers have the required skills to manage this aspect in the facilitation of a mutual manage this aspect in the facilitation of a mutual aid model using telephone mediated groupsaid model using telephone mediated groups

Future researchFuture research
•• Is there a causal link between participation in Is there a causal link between participation in the TGC and improved carer health & well the TGC and improved carer health & well being?being?
60
•• Are there sustained changes in carer well Are there sustained changes in carer well being after participation in a TGC?being after participation in a TGC?
•• Follow up Follow up –– would this assist in maintaining would this assist in maintaining decreased carer stress?decreased carer stress?
•• Does support for carers result in reduced Does support for carers result in reduced hospitalizations for person with MI?hospitalizations for person with MI?

Questions/Comments?Questions/Comments?Questions/Comments?Questions/Comments?
61