teach educational rounds - microsoft...teach educational rounds an update on cannabis and mental...
TRANSCRIPT
#TEACHwebinar
Educational Rounds 2018 1
TEACH Educational Rounds
An Update on Cannabis and Mental Health in an Age of
Legalization Date: August 15, 2018
Dr. Peter Selby, MBBS, CCFP, FCFP, MHSc, dipABAM, DFASAM Chief – Medicine in Psychiatry Division, Deputy Physician-in-Chief of Education and Clinical Scientist – Addictions, CAMH Professor, DFCM, Psychiatry, and the Dalla Lana School of Public Health, University of Toronto @drpselby www.nicotinedependenceclinic.com
#TEACHwebinar
Educational Rounds 2018 2
Requirements:
1. Registered for the webinar & complete Pre- Learning Assessment
2. Sign-in to view/participant in the live webinar session using your FIRST and LAST name.
3. Complete Evaluation and Post- Learning Assessment
Interested in Obtaining a Letter of Completion for this TEACH Educational Rounds?

#TEACHwebinar
Educational Rounds 2018 3
• These webinars are being live tweeted on Twitter
• Follow the CAMH Nicotine Dependence Service on Twitter: @PSQuitSmoking
• To follow the live tweeting or to post your questions or comments using Twitter follow:
#TEACHwebinar
4 #teachproject
Presenter Dr. Peter Selby MBBS, CCFP, FCFP, MHSc, DipABAM, DFASAM [email protected] Peter Selby is the Chief of Primary Care, Deputy Physician-in-Chief-Education, and a Clinician Scientist at the Centre for Addiction and Mental Health (CAMH). He is a Professor in the Departments of Family and Community Medicine, Psychiatry, and the Dalla Lana School of Public Health at the University of Toronto. He is also a Clinician Scientist in the Department of Family and Community Medicine. Dr. Selby is the Executive Director and creator of the TEACH project - a continuing education certificate program in Applied Counselling for Health with a focus on smoking cessation, through the University of Toronto. Dr. Selby’s research, as a Principal Investigator at the Ontario Tobacco Research Unit, includes smoking cessation especially in smokers with co morbid conditions. As the Principal Investigator of the STOP Study, he investigates the effectiveness of NRT and counselling in different types of intervention settings. He is also the PI of CANADAPTT- a unique Canadian Smoking Cessation Guideline development and dissemination project. Dr. Selby also continues his clinical research with pregnant women who use substances and is the PI of a knowledge translation program (PREGNETS) to increase the adoption of evidence-based interventions with pregnant smokers.
He has received grant funding totaling over 85 million dollars from CIHR, NIH, and Ministry of Health and has published 135 peer reviewed publications. He has published 5 books (including 4 edited), is the author of 30 book chapters, and 32 research reports prepared for the government. He is the Chair of the Canadian Centre on Substance Abuse National Task Force on Treatment for Prescription Drug Misuse and the Chair of the Medical Education Council for the American Society of Addiction Medicine. Dr. Selby mentors Fellows in Addiction Medicine and Addiction Psychiatry, junior investigators and medical students. The use of innovative methods to communicate messages makes Dr. Selby a sought after speaker for various topics including addictive disorders, motivational interviewing, and health behavior change.

#TEACHwebinar
Educational Rounds 2018 5
Disclosures (5 year) Grants/Research Support: • CAMH, Health Canada, OMOH, CIHR, CCSA, PHAC, Pfizer Inc./Canada, OLA, • Medical Psychiatry Alliance, ECHO, CCSRI, CCO, OICR, Ontario Brain Institute, • McLaughlin Centre, AHSC/AFP, WSIB, NIH, AFMC, Shoppers Drug Mart, • Bhasin Consulting Fund Inc., Patient-Centered Outcomes Research Institute
Speaking Engagements (Content not subject to sponsors approval)/Honoraria: • Pfizer Canada Inc., ABBVie, Bristol-Myers Squibb
Consulting Fees: • Pfizer Inc./Canada, Evidera Inc., Johnson & Johnson Group of Companies, • Medcan Clinic, Inflexxion Inc., V-CC Systems Inc., MedPlan Communications, • Kataka Medical Communications, Miller Medical Communications, • NVision Insight Group, Sun Life Financial, Myelin & Associates
Other: (Received drugs free/discounted for study through open tender process) • Johnson & Johnson, Novartis, Pfizer Inc.
NO TOBACCO or ALCOHOL or FOOD INDUSTRY FUNDING

#TEACHwebinar
Educational Rounds 2018 6
Potential sources of bias outlined on the following slide have been mitigated by making this information accessible and available to all participants at the time of registration and the presentation date.
Disclosures

#TEACHwebinar
Educational Rounds 2018 7
Content of the TEACH Curriculum slides are primarily based on evidence based guidelines
including:
• CAN-ADAPTT Canadian Practice Guidelines Initiative – developed in collaboration with national
experts in tobacco cessation and health behaviour change (www.can-adaptt.net)
• US Guidelines Treating Tobacco Use and Dependence: Clinical Practice Guideline 2008 Update. US
Department of Health and Human Services, Public Health Service
• Rethinking Stop-Smoking Medications: Treatment Myths and Medical Realities OMA Position Paper,
January 2008.
The development and delivery of the TEACH curriculum is not influenced or funded in any part
by tobacco industry. TEACH has not received funding from the tobacco industry. The
development of the TEACH curriculum has not been influenced by pharmaceutical industry.
Information presented on pharmacotherapy refers to generic products only, and
recommendations are based on existing research, including the CAN-ADAPTT and US guidelines.
TEACH Curriculum Development
#TEACHwebinar
Educational Rounds 2018 8
These materials (and any other materials provided in connection with this
presentation) as well as the verbal presentation and any discussions, set out only
general principles and approaches to assessment and treatment pertaining to
tobacco cessation interventions, but do not constitute clinical or other advice as to
any particular situations and do not replace the need for individualized clinical
assessment and treatment plans by health care professionals with knowledge of
the specific circumstances.
Disclaimer
#TEACHwebinar
Educational Rounds 2018 9
Copyright
Copying or distribution of these materials is
permitted providing the following is noted on
all electronic or print versions:
© CAMH/TEACH
No modification of these materials can be
made without prior written permission of
CAMH/TEACH.
#TEACHwebinar
Educational Rounds 2018 10
Learning Objectives
1. Identify the risks and benefits of cannabis use in patients with mental illnesses and addiction
2. Explain the risks and benefits of cannabis use in patients with mental illnesses and addiction
3. Discuss treatment approaches to cannabis use in clinical populations

#TEACHwebinar
Educational Rounds 2018 11
Agenda 1. Case
2. Brief overview of Cannabis
3. Why legalize?
4. Psychological effects of Cannabis
5. How to intervene with patients
– Pharmacotherapy interventions
– Psychosocial interventions
6. Summary
#TEACHwebinar
Educational Rounds 2018 12
Case
• 25 year old female
• ED- 3x visit
• Vomiting, abdo pain cramping, no diarrhea
• IV fluids both visits
• This visit reports that after a hot shower, noticed improvement
• Then vomiting began again
• Pregnancy test negative
What’s going on?

#TEACHwebinar
Educational Rounds 2018 13
Brief
Overview of Cannabis
13

#TEACHwebinar
Educational Rounds 2018 14
Brief Overview of Cannabis
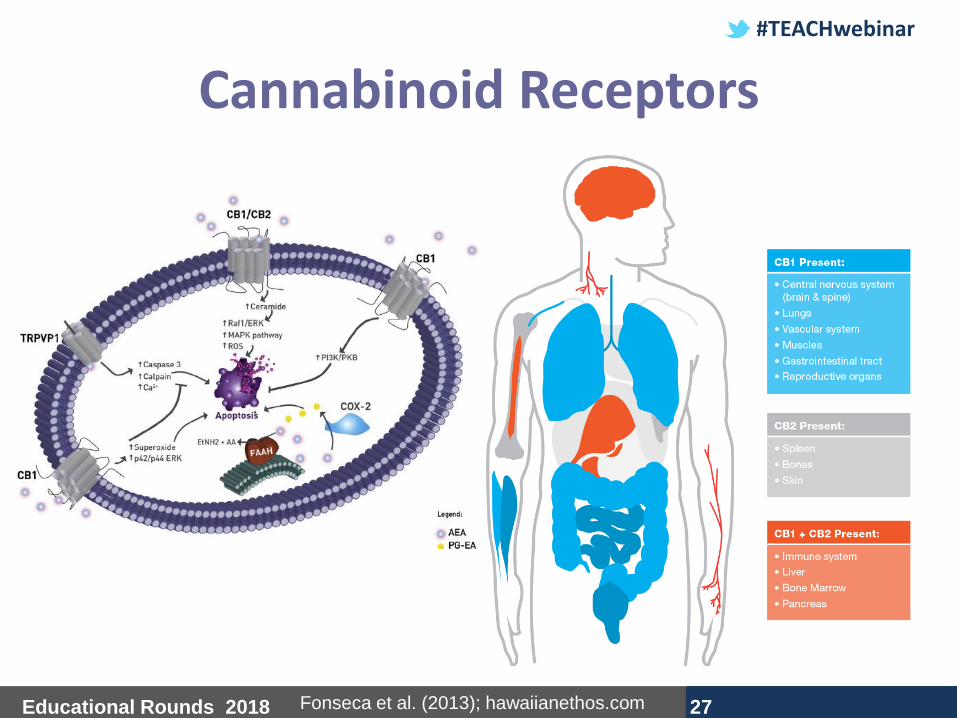
• Flowering plant (male and female)
• Alkaloids- Cannabinoids, terpenoids (smell)
– THC (tetrahydrocannibinol)
– Psychoactive constituent
– Binds to CB1 receptors
– Cannabidiol – Non-psychoactive compound
• Dried flowering buds= Marijuana
• Resin= hash
www.leafy.com
#TEACHwebinar
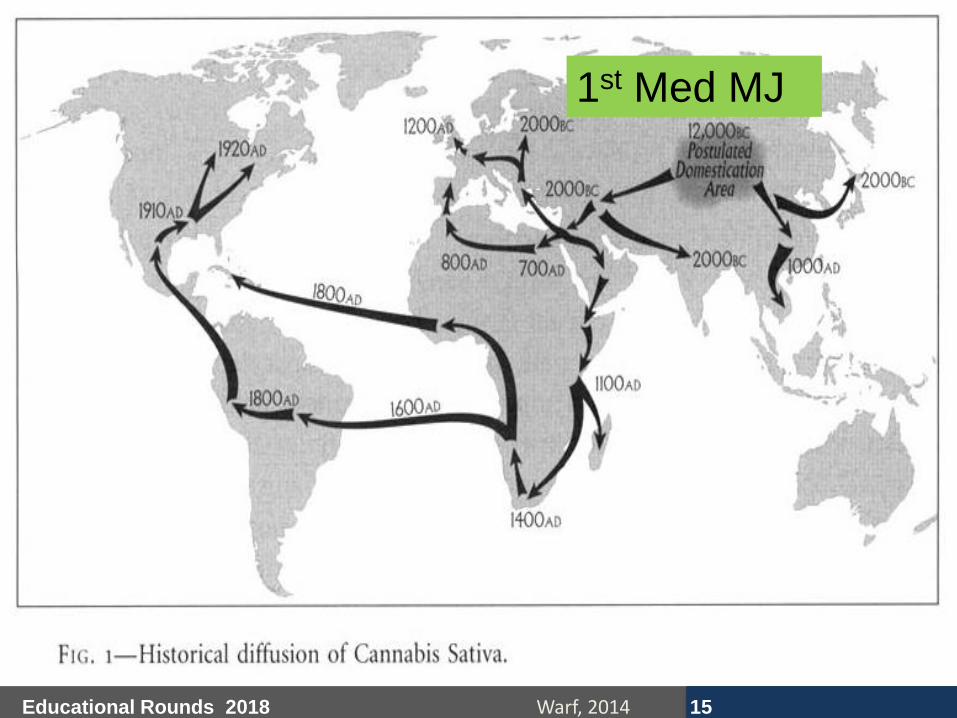
Educational Rounds 2018 15 Warf, 2014
1st Med MJ
#TEACHwebinar
Educational Rounds 2018 16
Historical Overview – Cannabis
#TEACHwebinar
Educational Rounds 2018 17
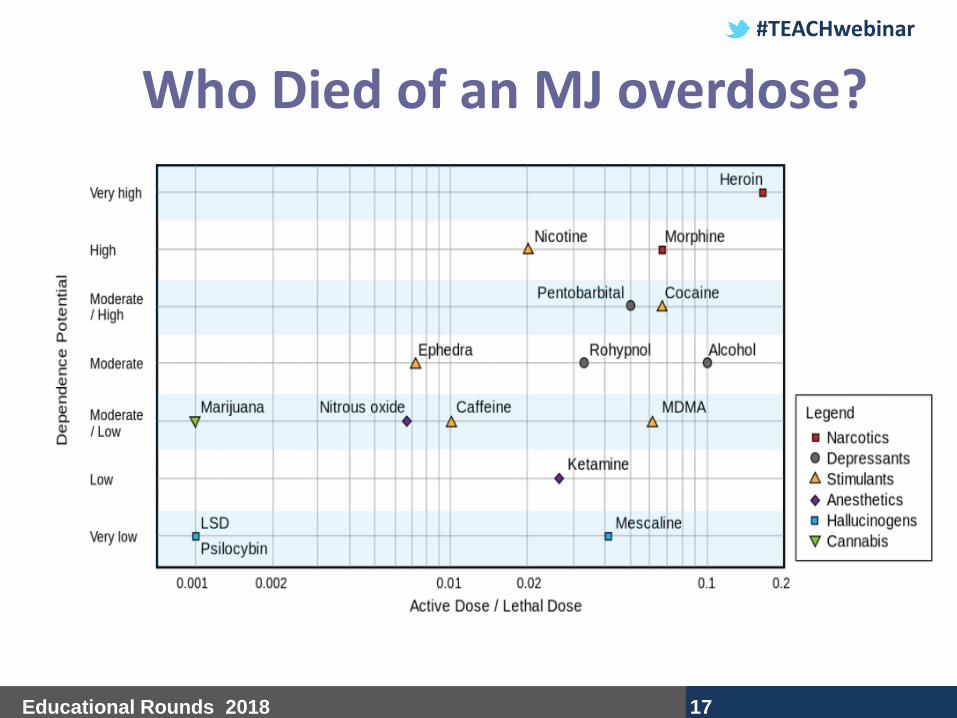
Who Died of an MJ overdose?

#TEACHwebinar
Educational Rounds 2018 18
...And During Prohibition
Medical Alcohol- who knew?

#TEACHwebinar
Educational Rounds 2018 19
Key Issues: Canadian Cannabis Use
Cannabis
not used for
recreational purposes.
25 convictions
for cannabis
possession in Canada.
Increase in cannabis use.
Canada signs the UN’s
Single Convention on Narcotic Drugs.
Le Dain Commission
concludes Canada’s
prohibition laws create
little respect for law
enforcement, congestion
of judicial system, and
strengthening organized crime.
Marihuana Medical
Access Regulations –
Canada 1st to legalize
marijuana for terminal
illness and chronic conditions.
Ontario Superior
Court sought to prohibit the
possession and production of
marijuana. Medical marijuana is now legalized.
Cannabis Act will
legalize and regulate
recreational cannabis
by Oct 17, 2018. Policy
focuses on health
impacts and public safety.
1930s
1930- 1946
1960- 1970s
Early 1970s
1987
Canada’s Drug
Strategy, the most
severe in the world,
addresses supply
and demand
reduction.
2001
2011
2018
Maistro et al., 2013; Health Reform Monitor 2018

#TEACHwebinar
Educational Rounds 2018 20 CTADS, 2013
10.6
0.9 0.2 0.6 0.4 0.1
0
2
4
6
8
10
12
Perc
en
tag
e
Illicit Drugs
Illicit Drug Use Within the Past 12 Months, Canada (2013)
Cannabis is the most widely used illicit drug
76% reported alcohol
consumption
15% smoking
prevalence

#TEACHwebinar
Educational Rounds 2018 21
Why Legalize?
#TEACHwebinar
Educational Rounds 2018 22
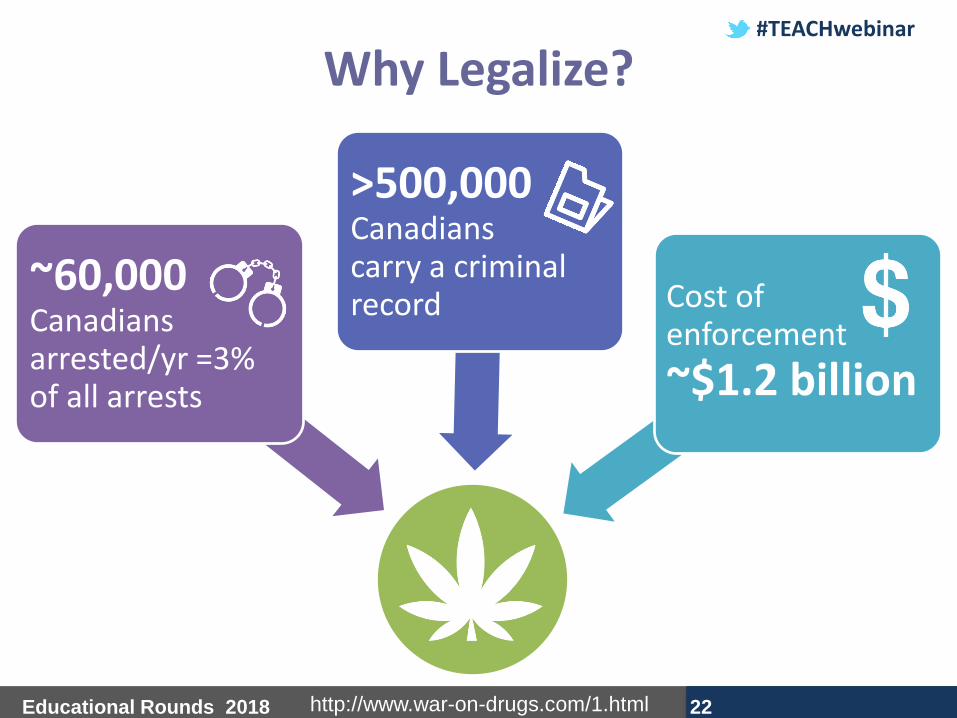
Why Legalize?
~60,000 Canadians arrested/yr =3% of all arrests
>500,000 Canadians carry a criminal record Cost of
enforcement
~$1.2 billion
http://www.war-on-drugs.com/1.html
#TEACHwebinar
Educational Rounds 2018 23
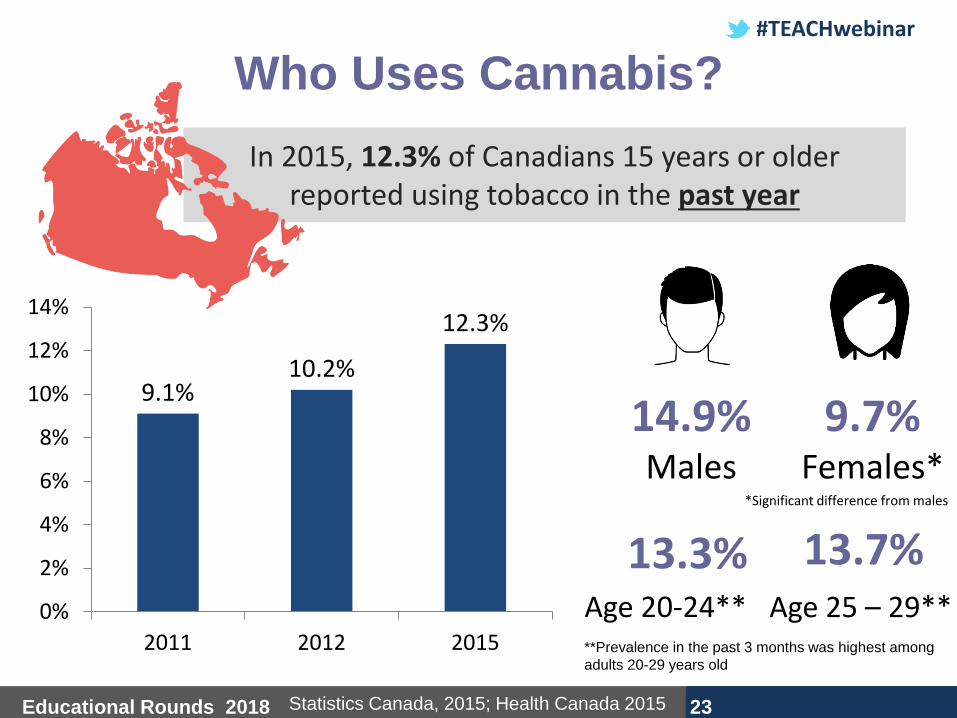
Who Uses Cannabis?
In 2015, 12.3% of Canadians 15 years or older reported using tobacco in the past year
14.9%
Males
9.7% Females*
Statistics Canada, 2015; Health Canada 2015
**Prevalence in the past 3 months was highest among
adults 20-29 years old
13.3% Age 20-24**
13.7% Age 25 – 29**
9.1% 10.2%
12.3%
0%
2%
4%
6%
8%
10%
12%
14%
2011 2012 2015
*Significant difference from males

#TEACHwebinar
Educational Rounds 2018 24
Prevalence of Past Year Cannabis
Use, by Province, Canada (2012)
12.3%
12.2%
10.8%
15.7%*
11.6%
11.9%
12.0%
11.1%
9.9%*
11.1%
14.3%*
Ontario 12.0%
Nova Scotia 15.7% (highest); Saskatchewan 9.9% (lowest)
Statistics Canada; 2012
#TEACHwebinar
Educational Rounds 2018 25
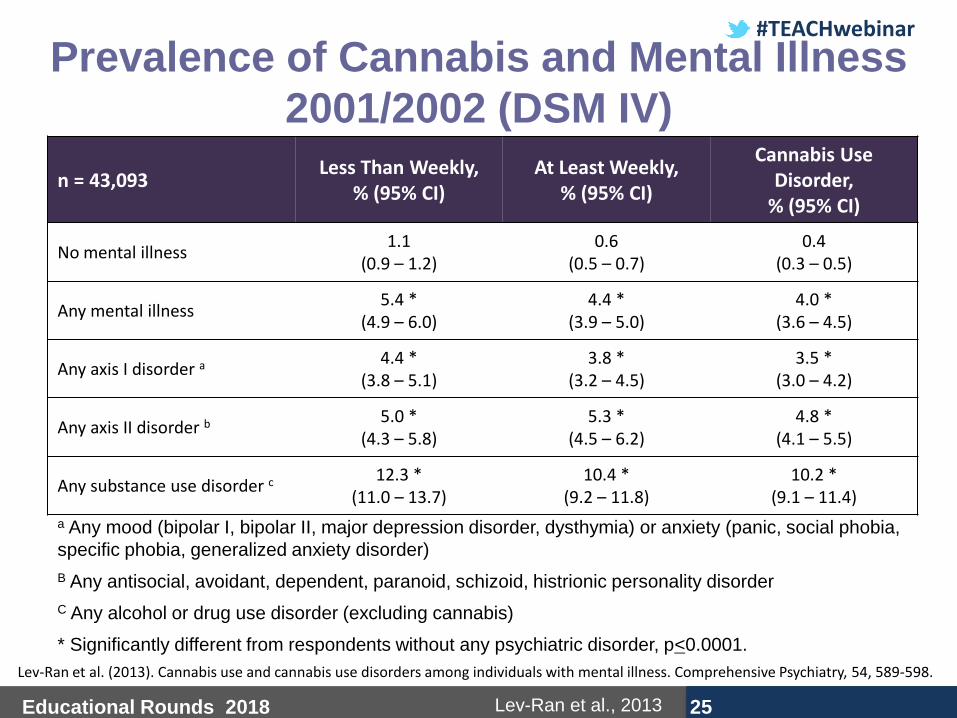
Prevalence of Cannabis and Mental Illness
2001/2002 (DSM IV)
n = 43,093 Less Than Weekly,
% (95% CI) At Least Weekly,
% (95% CI)
Cannabis Use Disorder,
% (95% CI)
No mental illness 1.1
(0.9 – 1.2) 0.6
(0.5 – 0.7) 0.4
(0.3 – 0.5)
Any mental illness 5.4 *
(4.9 – 6.0) 4.4 *
(3.9 – 5.0) 4.0 *
(3.6 – 4.5)
Any axis I disorder a 4.4 * (3.8 – 5.1)
3.8 * (3.2 – 4.5)
3.5 * (3.0 – 4.2)
Any axis II disorder b 5.0 * (4.3 – 5.8)
5.3 * (4.5 – 6.2)
4.8 * (4.1 – 5.5)
Any substance use disorder c 12.3 * (11.0 – 13.7)
10.4 * (9.2 – 11.8)
10.2 * (9.1 – 11.4)
a Any mood (bipolar I, bipolar II, major depression disorder, dysthymia) or anxiety (panic, social phobia,
specific phobia, generalized anxiety disorder)
B Any antisocial, avoidant, dependent, paranoid, schizoid, histrionic personality disorder
C Any alcohol or drug use disorder (excluding cannabis)
* Significantly different from respondents without any psychiatric disorder, p<0.0001.
Lev-Ran et al., 2013
Lev-Ran et al. (2013). Cannabis use and cannabis use disorders among individuals with mental illness. Comprehensive Psychiatry, 54, 589-598.
#TEACHwebinar
Educational Rounds 2018 26
Physiological Effects of Cannabis
#TEACHwebinar
Educational Rounds 2018 27
Cannabinoid Receptors
Fonseca et al. (2013); hawaiianethos.com

#TEACHwebinar
Educational Rounds 2018 28
Physiological Effects of Cannabis
Maistro et al., 2013; Volkow et al., 2014
Acute Effects
Long-term Effects
1. Increased risk of respiratory
infections and pneumonia
2. Increased in heart and pulse
rates
3. Increased risk of lung cancer,
myocardial infarction, stroke,
and transient ischemic attacks
1. Bloodshot eyes
2. Increase in heart and pulse
rates
3. Decrease in general motor
activity
4. Hunger
#TEACHwebinar
Educational Rounds 2018 29
Effect of Cannabis on Brain Development
During this time, brain is more vulnerable
to THC
Earlier age of cannabis onset = greater
neuropsychological impairment
Volkow et al., 2014
Brain is in a state of development from prenatal period until 21 years of age
#TEACHwebinar
Educational Rounds 2018 30
Effect of Cannabis on Brain
Development
Volkow et al., 2014
• Regular cannabis use during adolescence impairs
neural connectivity, thereby:
– Reducing alertness and self-conscious awareness
– Memory and learning impairments
– Reduced inhibitory control
– Down regulation of CB1/CB2 receptors
– Decline in IQ
– Impaired school performance
• Increased risk of dropping
out of school

#TEACHwebinar
Educational Rounds 2018 31
Effect of Cannabis on Brain Development
Scholastic Inc. 2016

#TEACHwebinar
Educational Rounds 2018 32
Brain Effects of Cannabis
Maistro et al., 2013; Hoch et al., 2015
Behavioral effects:
• Decrease in psychomotor activity (relaxation,
motivation) and motor performance (coordination,
signal detection)
Cognitive effects:
• Impaired short-term memory, cognitive functioning
• Perception of time (time moves slowly)
• Attention
• Retentiveness
Emotional effects:
• Mood changes (happy, euphoric, excited)
• Laughter

#TEACHwebinar
Educational Rounds 2018 33
Additional Effects of Cannabis
Volkow et al., 2014
• Persons testing +ve for THC are 3-
7x more likely to be responsible for
a motor vehicle accident
• Possible role as a gateway
behaviour
• Increased risk of ED visits
– Possibly due to an increase in the
potency of THC content

#TEACHwebinar
Educational Rounds 2018 34
Evidence

#TEACHwebinar
Educational Rounds 2018 35
Cannabinoids for Medical Use
Condition
Number of Trials and Patients
Odds Ratio (95% CI)
What does this mean
Nausea and vomiting due to chemotherapy
3 Trials (n = 102)
3.82 * (1.55 – 9.42)
The use of dronabinol or nabiximols were associated with a 3.82 greater odds of
complete remission of nausea and vomiting compared to patients treated with placebo
Chronic pain (minimum 30% reduction)
8 Trials (n = 1,370)
1.41 (0.99 – 2.00)
Use of Smoked THC and nabixmols was not associated with a 30% reduction in chronic
pain compared to patents treated with placebo
Neuropathic pain
6 Trials 1.38
(0.93 – 2.03)
Use of cannabinoids were not associated with a reduction in neuropathic pain
compared to patents treated with placebo
Cancer pain 2 Trials 1.41
(0.99 – 2.00)
Use of cannabinoids were not associated with a reduction in cancer pain compared to
patents treated with placebo
Whiting et al., 2015 * Significant at p < 0.05

#TEACHwebinar
Educational Rounds 2018 36
Marijuana used alone = significant increase of 100% in the number of ED visits during 2004 to 2011
Marijuana used in combination with other drugs = significant increase of 62% in the number of ED visits during 2004 to 2011
Volkow et al., 2014
#TEACHwebinar
Educational Rounds 2018 37
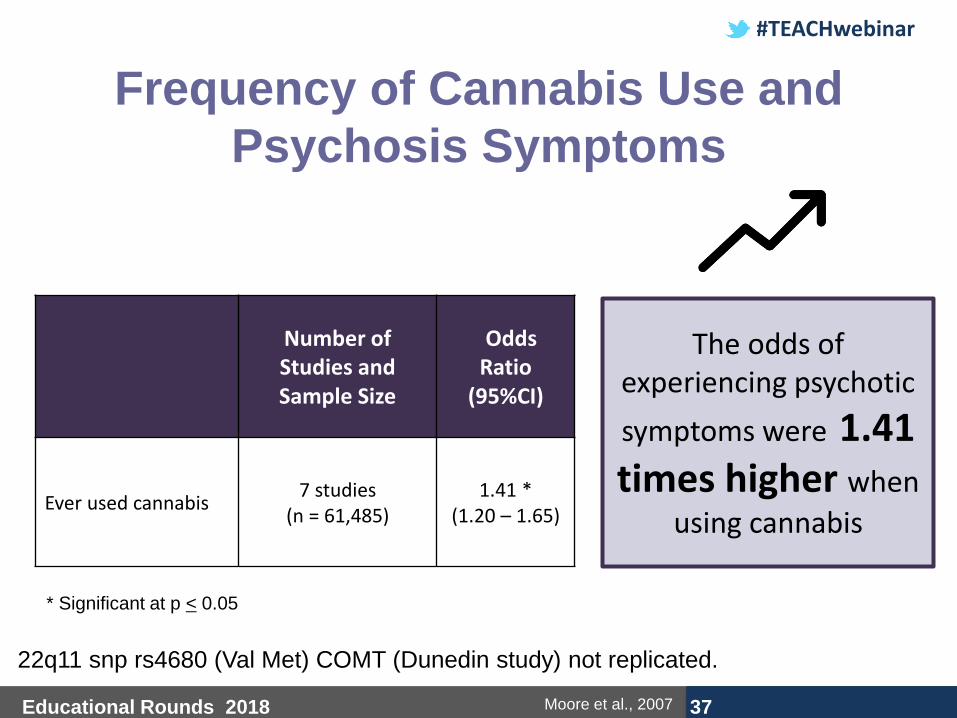
Frequency of Cannabis Use and
Psychosis Symptoms
Number of Studies and Sample Size
Odds Ratio
(95%CI)
Ever used cannabis 7 studies
(n = 61,485) 1.41 *
(1.20 – 1.65)
* Significant at p < 0.05
Moore et al., 2007
22q11 snp rs4680 (Val Met) COMT (Dunedin study) not replicated.
The odds of experiencing psychotic
symptoms were 1.41 times higher when
using cannabis
#TEACHwebinar
Educational Rounds 2018 38
Cannabis Use and Psychosis: Patient
views
Large et al., 2014; Gomez Perez et al., 2014; Gill et al., 2015; Mane et al., 2015; Bruins et al., 2016
Benefits:
• Mood enhancement
• Social motives
• Belonging to a group, avoid isolation
• Self-medicate
• Relax
• Decrease hallucinations and suspiciousness
Risks:
• Increase in psychotic symptoms (positive and general symptoms)
• Increase in episodes of violence and convictions for non-violent offences
#TEACHwebinar
Educational Rounds 2018 39
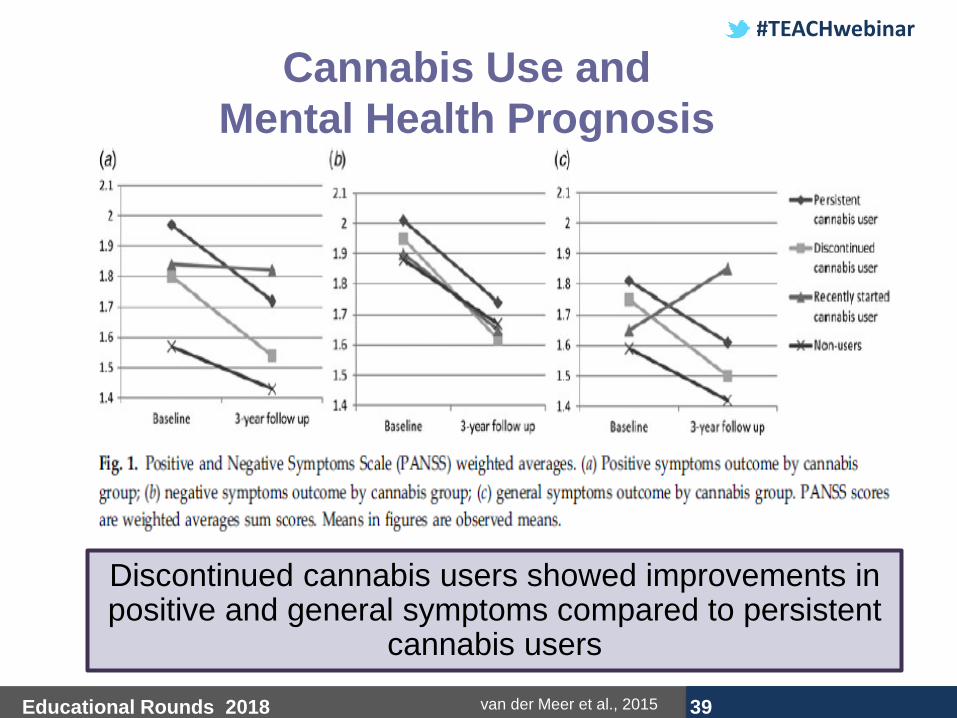
Cannabis Use and
Mental Health Prognosis
van der Meer et al., 2015
Discontinued cannabis users showed improvements in positive and general symptoms compared to persistent
cannabis users

#TEACHwebinar
Educational Rounds 2018 40
Cannabis Use and Mental Health
Prognosis
• 3 year follow up study was part of a multi-center study in the Netherlands and Belgium, 678 participants
• There is no association between timing
of cannabis cessation and clinical outcomes
• Furthermore, the impact of cannabis on
severity of symptoms is reversible
van der Meer et al., 2015

#TEACHwebinar
Educational Rounds 2018 41
Cannabis Use and Mental Health Prognosis
van der Meer et al., 2015
Early Discontinuation (n = 47)
Mean (SD)
Late Discontinuation (n = 210)
Mean (SD) P-value
Positive Symptoms Scale (PANSS)
1.44 (0.55)
1.57 (0.60)
0.179
Negative Symptoms Scale (PANSS)
1.60 (0.66)
1.64 (0.78)
0.777
General Symptoms (PANSS) 1.43
(0.41) 1.52
(0.46) 0.195
Global Assessment of Functioning Scale Symptoms
64.28 (16.68)
59.40 (16.42)
0.163
Global Assessment of Functioning Scale Disability
65.00 (15.96)
61.75 (16.12)
0.371
Psychotic Relapse 0.28
(0.58) 0.34
(0.80) 0.629
Early discontinuation: Patients stopped using cannabis within 3 years of psychosis onset
Late discontinuation: Patients stopped using cannabis after 3 years of psychosis onset

#TEACHwebinar
Educational Rounds 2018 42
Dose-Response Relationship with
Psychosis
Toftdahl et al., 2016
• Purpose:
– Evaluate impact that cannabis has on individuals with
established psychotic disorder
• Longitudinal study:
– Post-treatment (6 months)
– Follow-up (10 months)
• Individuals: N=60
– Diagnosed with cannabis use disorder
– Diagnosed with either schizophrenia,
schizotypal, and delusional disorders

#TEACHwebinar
Educational Rounds 2018 43
Dose-Response Relationship with
Psychosis
Toftdahl et al., 2016
Severe use was associated with
more severe symptoms
Reducing use had greatest
improvement in symptoms for every
symptom scale
#TEACHwebinar
Educational Rounds 2018 44
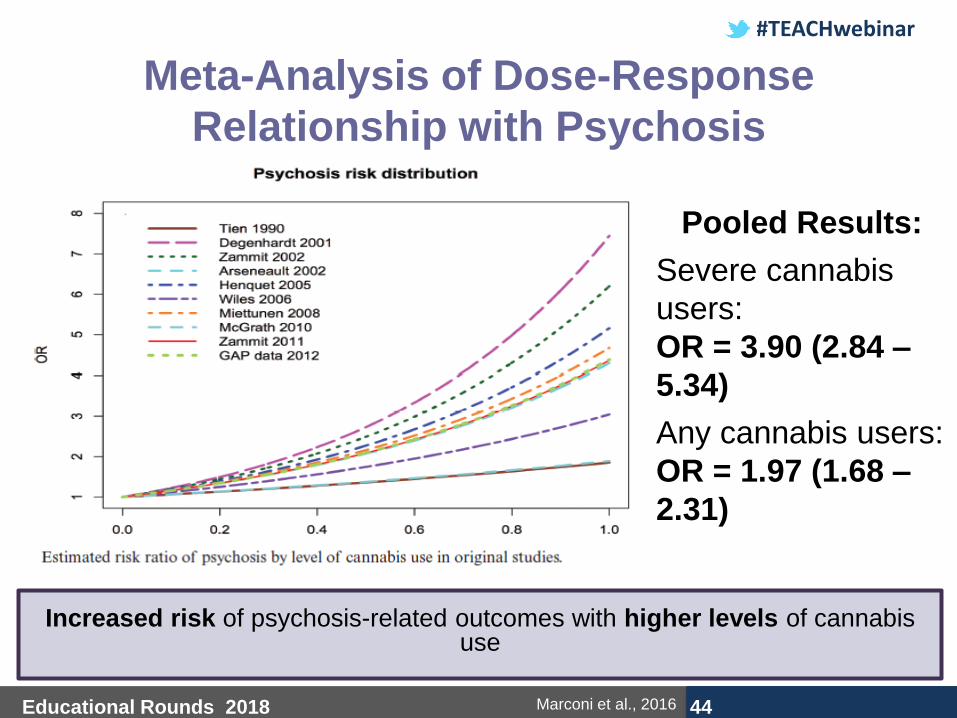
Meta-Analysis of Dose-Response
Relationship with Psychosis
Marconi et al., 2016
Pooled Results:
Severe cannabis
users:
OR = 3.90 (2.84 –
5.34)
Any cannabis users:
OR = 1.97 (1.68 –
2.31)
Increased risk of psychosis-related outcomes with higher levels of cannabis
use
#TEACHwebinar
Educational Rounds 2018 45
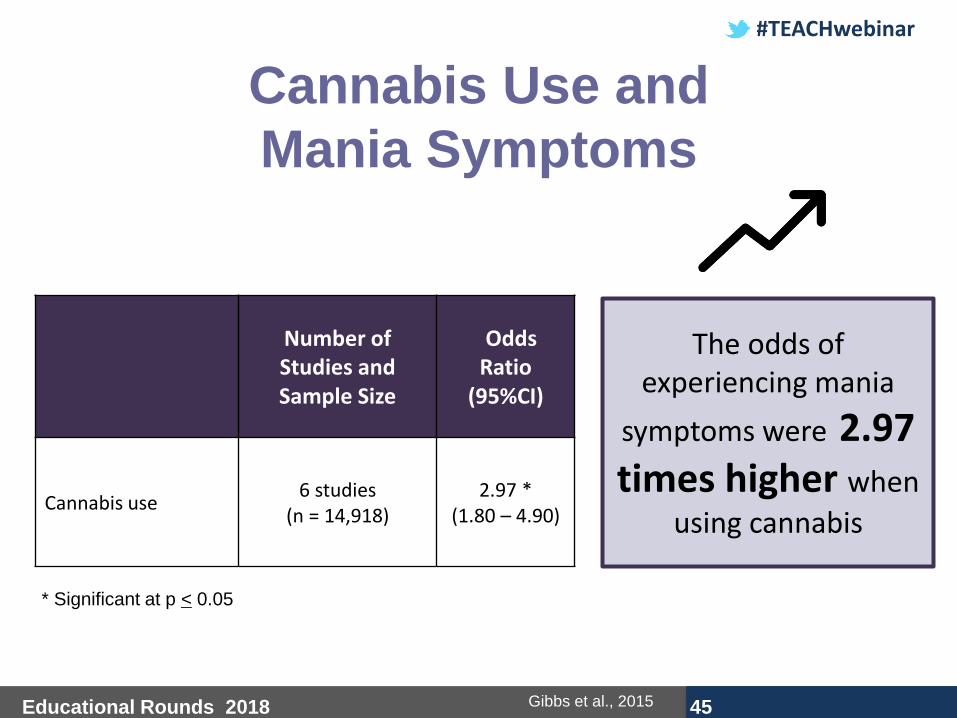
Cannabis Use and
Mania Symptoms
* Significant at p < 0.05
Gibbs et al., 2015
Number of Studies and Sample Size
Odds Ratio
(95%CI)
Cannabis use 6 studies
(n = 14,918) 2.97 *
(1.80 – 4.90)
The odds of experiencing mania
symptoms were 2.97 times higher when
using cannabis

#TEACHwebinar
Educational Rounds 2018 46
Cannabis Use and Anxiety
Number of Studies
Odds Ratio (95%CI)
What Does This Mean?
Anxiety and cannabis use 15 studies 1.24 *
(1.06 – 1.45)
The odds of anxiety is 1.24 times higher when using
cannabis
Anxiety and cannabis use disorder
13 studies 1.68 *
(1.23 – 2.31)
The odds of anxiety is 1.68 times higher when diagnosed
with a cannabis use disorder
Anxiety + depression and cannabis use
5 studies 1.68 *
(1.17 – 2.40)
The odds of anxiety and
depression is 1.68 times higher when using cannabis
* Significant at p < 0.05
Moore et al., 2007

#TEACHwebinar
Educational Rounds 2018 47
Temporal Association
Cannabis Use Anxiety
Symptoms
Anxiety
Symptoms Cannabis Use
Baseline Follow-up
5 studies
1 study
OR = 1.28 *
(95% CI: 1.06 – 1.54)
OR = 0.94
(95% CI: 0.86 – 1.03)
* Significant at p < 0.01
Kedzior et al., 2014
Baseline cannabis positively associated with anxiety
symptoms at follow-up
#TEACHwebinar
Educational Rounds 2018 48
Cannabis Use and Depression
Degenhardt et al., 2003
The US National Longitudinal Alcohol Epidemiologic Survey found that individuals meeting criteria for DSM-IV major depression within the past 12 months had 6.4 times the odds of meeting criteria for DSM-IV cannabis abuse/dependence as those without major depression (6% vs 1%)

#TEACHwebinar
Educational Rounds 2018 49
Plausibility for Causation
• Depression:
– Cannabis may impact serotonin, dopamine, or
other neurotransmitters and thus regulating
emotional experiences symptoms
– Cannabis use could exacerbate events,
circumstances, or environments that increase
the likelihood of the depression
– An unknown factors, social, biological,
physiological, mediate the relationship
between cannabis use and depression
Degenhardt et al., 2003
#TEACHwebinar
Educational Rounds 2018 50
Confounders
Caron et al, 2010; Large et al., 2014; Gill et al., 2015; van der Meer et al. 2015
Cannabis use is more likely among:
Males Less
educated
Young
individuals Earlier age of
psychosis onset
Other substance
users (e.g., alcohol)
High symptom
score
Don’t control for
tobacco use

#TEACHwebinar
Educational Rounds 2018 51
How to
Intervene
with
Patients?

#TEACHwebinar
Educational Rounds 2018 52
Interventions for Cannabis Use
Disorders • Pharmacotherapy interventions
– THC preparations
– SSRI antidepressants
– Mixed action antidepressants
– Anticonvulsants or mood stabilizers
• Psychosocial interventions
– Cognitive-behavioural therapies
– Motivational interviewing

#TEACHwebinar
Educational Rounds 2018 53
Pharmacotherapy
Interventions

#TEACHwebinar
Educational Rounds 2018 54
Completion of Treatment Number of Studies and Sample Size
Risk Ratio (95%CI)
What Does This Mean?
Preparations containing THC vs placebo
2 studies (n = 207)
1.29 * (1.08 – 1.55)
Using preparations containing THC
increases the likelihood of completing
treatment by 29% compared to placebo
SSRI antidepressants vs placebo
2 studies (n = 122)
0.82 (0.44 – 1.53)
Using SSRI antidepressants does not increase the likelihood of completing
treatment compared to placebo
Mixed action antidepressants vs placebo
2 studies (n = 169)
0.93 (0.71 – 1.21)
Using mixed action antidepressants
does not increase the likelihood of
completing treatment compared to placebo
Anticonvulsants and mood stabilizers vs placebo
2 studies (n = 75)
0.78 (0.42 – 1.46)
Using anticonvulsants and mood
stabilizers does not increase the
likelihood of completing treatment compared to placebo
* Significant at p < 0.05
Marshall et al., 2014

#TEACHwebinar
Educational Rounds 2018 55
Abstinence Number of Studies and Sample Size
Risk Ratio (95%CI)
What Does This Mean?
Preparations containing THC vs placebo
1 study (n = 156)
1.14 (0.56 – 2.30)
Using preparations containing THC
does not increase abstinence rates compared to placebo
SSRI antidepressants vs placebo
1 study (n = 52)
2.33 (0.68 – 8.05)
Using SSRI antidepressants does not increase abstinence rates
compared to placebo
Mixed action antidepressants vs placebo
2 studies (n = 179)
0.82 (0.12 – 5.41)
Using mixed action
antidepressants does not increase abstinence rates
compared to placebo
Anticonvulsants and mood stabilizers vs placebo
1 study (n = 19)
1.08 (0.50 – 2.34)
Using anticonvulsants and mood
stabilizers does not increase abstinence rates compared to
placebo
Marshall et al., 2014
#TEACHwebinar
Educational Rounds 2018 56
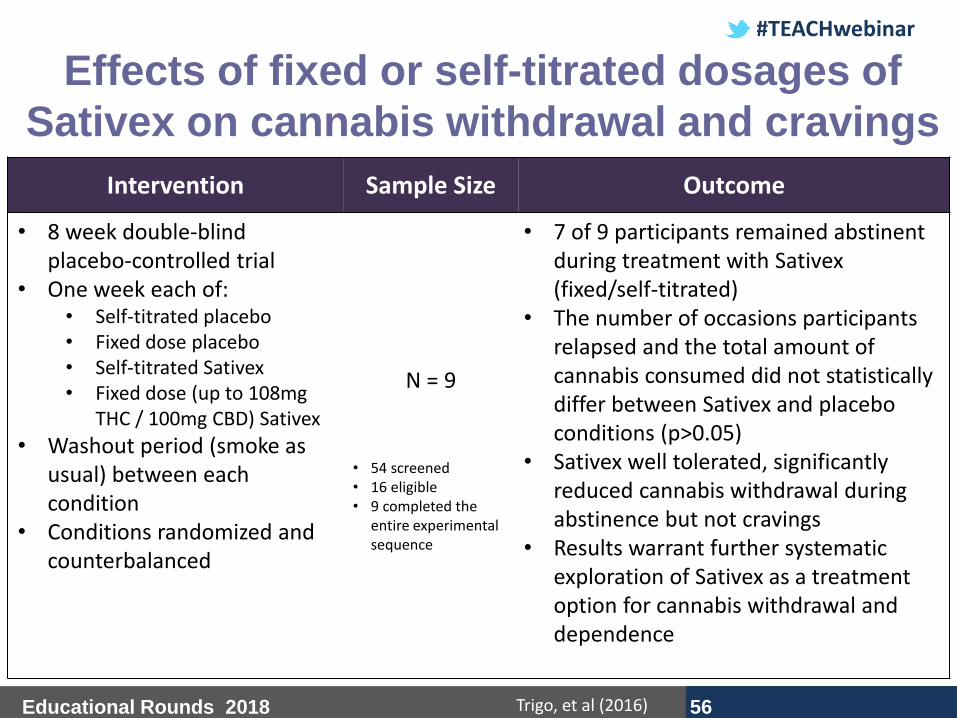
Effects of fixed or self-titrated dosages of
Sativex on cannabis withdrawal and cravings
Intervention Sample Size Outcome
• 8 week double-blind placebo-controlled trial
• One week each of: • Self-titrated placebo • Fixed dose placebo • Self-titrated Sativex • Fixed dose (up to 108mg
THC / 100mg CBD) Sativex
• Washout period (smoke as usual) between each condition
• Conditions randomized and counterbalanced
N = 9
• 54 screened • 16 eligible • 9 completed the
entire experimental sequence
• 7 of 9 participants remained abstinent during treatment with Sativex (fixed/self-titrated)
• The number of occasions participants relapsed and the total amount of cannabis consumed did not statistically differ between Sativex and placebo conditions (p>0.05)
• Sativex well tolerated, significantly reduced cannabis withdrawal during abstinence but not cravings
• Results warrant further systematic exploration of Sativex as a treatment option for cannabis withdrawal and dependence
Trigo, et al (2016)
#TEACHwebinar
Educational Rounds 2018 57
Psychosocial
Interventions

#TEACHwebinar
Educational Rounds 2018 58
Harm Reduction: Frequency of
Use
Number of Studies and Sample Size
Mean Difference
(95%CI) What Does This Mean?
CBT vs inactive control 1 study
(n = 134) 10.94 *
(7.44 – 14.44)
Individuals receiving CBT used cannabis on
11 fewer days in the last month compared with the inactive control
MET vs inactive control 4 studies (n = 612)
4.45 * (1.90 – 7.00)
Individuals receiving MET used cannabis on
4 fewer days in the last month compared with the inactive control
CBT + MET vs inactive control
4 studies (n = 612)
7.38 * (3.18 – 11.57)
Individuals receiving CBT + MET used
cannabis on 7 fewer days in the last month compared with the inactive control
Gates et al., 2016
Cognitive-behavioural therapy (CBT); Motivational interviewing/motivational enhancement therapy
(MET)
* Significant at p < 0.05

#TEACHwebinar
Educational Rounds 2018 59
Harm Reduction: Quantity of Use
Number of Studies and Sample Size
Standardized Mean
Difference (95%CI)
What Does This Mean?
CBT vs inactive control 2 studies (n = 306)
4.60 * (2.21 – 7.00)
Individuals receiving CBT used
fewer joints per day compared with the inactive control
MET vs inactive control 4 studies (n = 611)
3.14 * (2.66 – 3.61)
Individuals receiving MET used
fewer joints per day compared
with the inactive control
CBT + MET vs inactive control 4 studies (n = 683)
4.91 * (3.29 – 6.54)
Individuals receiving CBT + MET
used fewer joints per day compared with the inactive control
Gates et al., 2016
Cognitive-behavioural therapy (CBT); Motivational interviewing/motivational enhancement therapy (MET)
* Significant at p < 0.05
#TEACHwebinar
Educational Rounds 2018 60
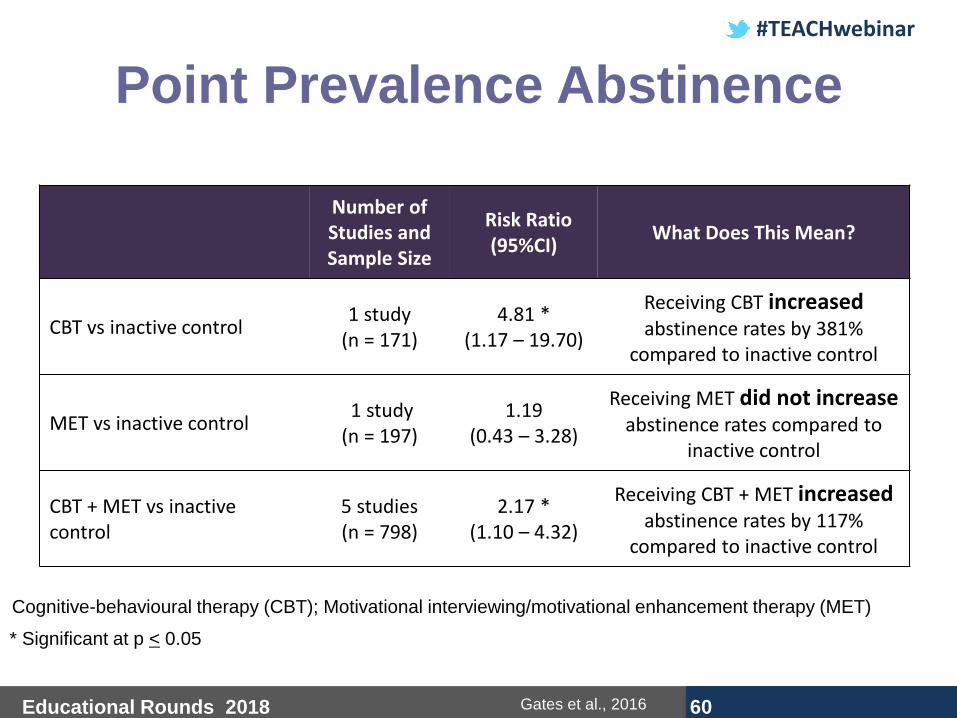
Point Prevalence Abstinence
Number of Studies and Sample Size
Risk Ratio (95%CI)
What Does This Mean?
CBT vs inactive control 1 study
(n = 171) 4.81 *
(1.17 – 19.70)
Receiving CBT increased abstinence rates by 381%
compared to inactive control
MET vs inactive control 1 study (n = 197)
1.19 (0.43 – 3.28)
Receiving MET did not increase abstinence rates compared to
inactive control
CBT + MET vs inactive control
5 studies (n = 798)
2.17 * (1.10 – 4.32)
Receiving CBT + MET increased abstinence rates by 117%
compared to inactive control
Gates et al., 2016
Cognitive-behavioural therapy (CBT); Motivational interviewing/motivational enhancement therapy (MET)
* Significant at p < 0.05

#TEACHwebinar
Educational Rounds 2018 61
Intervention Sample Size Outcome
• Double blind randomized clinical trial
• As-needed nabiximols up to 113.4mg THC/ 105 mg CBD OR placebo daily, concurrently with MET/CBT for 12 weeks
N = 27
• 68 screened • 50 eligible • 40 dosed • 27 completed the
entire experimental sequence
• Nabiximols in combination with MET/CBT was well tolerated and allowed for reduction of cannabis use.
• Nabiximols may help to decrease cannabis use, with no increase in craving or withdrawal
• Results suggest that the combination of doses above 20 sprays per day of nabiximols + MET/CBT should be explored further for its potential as treatment for cannabis use disorder (CUD)
Trigo, et al (2016)
Nabiximols combined with motivational
enhancement/cognitive behavioral therapy for the
treatment of cannabis dependence: A pilot
randomized clinical trial
#TEACHwebinar
Educational Rounds 2018 62
Lower Risk Guidelines • Use is delayed until early adulthood
• Frequent (daily or near‐daily) use is avoided
• Users shift away from smoking cannabis towards less harmful (smokeless) delivery systems such as vaporizers
• Less potent products are used, or THC dose is titrated
• Driving is avoided for 3 to 4 hours after use, or longer if needed
• People with higher risk of cannabis‐related problems (e.g. people with a personal or family history of psychosis, people with cardiovascular problems, and pregnant women) abstain altogether
Fischer et al
#TEACHwebinar
Educational Rounds 2018 63
• Cannabis use is common in Canada
• Cannabis use has some benefits, however persistent use can be harmful
• Cannabis use has demonstrated a significant association with mental illness
• The severity of symptoms associated with cannabis use are reversible
• Psychosocial interventions are the foundation for treatment of cannabis use disorders/dependence
Summary
#TEACHwebinar
Educational Rounds 2018 64
Resources
• Canadian Centre on Substance Abuse
www.ccsa.ca
• Substance Abuse and Mental Health
Services Administration
http://www.samhsa.gov/
• Centre for Addiction and Mental Health
www.camh.ca

#TEACHwebinar
Educational Rounds 2018 65
Questions or Comments?
#TEACHwebinar
Educational Rounds 2018 66
References • Bruins et al. (2016). Cannabis use in people with severe mental illness: The association with
physical and mental health – a cohort study. A pharmacotherapy Monitoring and Outcome
Survey study. Journal of Psychopharmacology, 30(4), 354-362.
• Canadian Mental Health Association. (2016). Fast facts about mental illness.
http://www.cmha.ca/media/fast-facts-about-mental-illness/#.WA4dIMlgmb0
• Caron & Liu. (2010). A descriptive study of the prevalence of psychological distress and
mental disorders in the Canadian population: Comparison between low-income and non-
low-populations. Chronic Diseases in Canada, 30(3), 84-94.
• Degenhardt et al. (2003). Exploring the association between cannabis use and depression.
Addiction, 98(11), 1493-1504.
• Fonseca et al. (2013). Endogenous cannabinoids revisted: a biochemistry perspective.
Prostaglandins & Other Lipid Mediators, 102, 13-30.
• Gates et al. (2016). Psychosocial interventions for cannabis use disorder. Cochrane Review
of Systematic Reviews. Issue 5. Art. No.: CD005336
• Gibbs et al. (2015). Cannabis use and mania symptoms: A systematic review and meta-
analysis. Journal of Affective Disorders, 171, 39-47.
• Gill et al. (2015). Reasons for cannabis use among youths at ultra high risk for psychosis.
Early Intervention Psychiatry, 9(3), 207-210.

#TEACHwebinar
Educational Rounds 2018 67
References • Gomez Perez et al. (2014). Reasons and subjective effects of cannabis use among people
with psychotic disorders: a systematic review. Actas españolas de psiquiatría, 42(2), 83-90.
• Government of Canada. (2013). Canadian Tobacco, Alcohol, and Drugs Survey (CTADS).
http://healthycanadians.gc.ca/science-research-sciences-recherches/data-donnees/ctads-
ectad/tables-tableaux-2013-eng.php#t8
• Health Canada. (2012). Canadian Alcohol and Drug Use Monitoring Survey. http://www.hc-
sc.gc.ca/hc-ps/drugs-drogues/stat/_2012/summary-sommaire-eng.php
• Health Reform Monitor. (2018). The Canadian Cannabis Act legalizes and regulates
recreational cannabis use in 2018. Health Policy. 122, 3. 205-209
• Hoch, E., et al. (2015). Risks associated with the non-medicinal use of cannabis. Deutsches
Arzteblatt International, 112, 271-278.
• Kedzior et al. (2014). A positive association between anxiety disorders and cannabis use or
cannabis use disorders in the general population – a meta-analysis of 31 studies. BMC
Psychiatry, 14, 136.
• Large et al. (2014). Systematic meta-analysis of outcomes associated with psychosis and
co-morbid substance use. Australian & New Zealand Journal of Psychiatry, 48(5), 418-432.
• Lev-Ran et al. (2013). Cannabis use and cannabis use disorders among individuals with
mental illness. Comprehensive Psychiatry, 54, 589-598.

#TEACHwebinar
Educational Rounds 2018 68
References • Marconi et al. (2016). Meta-analysis of the association between the level of cannabis use
and risk of psychosis. Schizophrenia Bulletin, 42(5), 1262-1269.
• Maistro et al. (2013). Drug use and abuse. 1st ed. Nelson Education Ltd. Toronto, ON.
• Mane et al. (2015). Relationship between cannabis and psychosis: Reasons for use and
associated clinical variables. Psychiatry Research, 229, 70-74.
• Marshall et al. (2014). Pharmacotherapies for cannabis dependence. Cochrane Database of
Systematic Reviews. Issue 12. Art. No.: CD008940.
• Moore et al. (2007). Cannabis use and risk of psychotic or affective mental health outcomes:
A systematic review. Lancet, 370(9584), 319-28.
• Scholastic Inc. (2016). The Science of the Endocannabinoid System: How THC Affects the
Brain and the Body. http://headsup.scholastic.com/students/endocannabinoid
• Statistics Canada. (2012). Prevalence and correlates of marijuana use in Canada, 2012.
http://www.statcan.gc.ca/pub/82-003-x/2015004/article/14158-eng.htm
• Statistics Canada. (2015). Canadian Tobacco, Alcohol and Drugs Survey, 2015
https://www150.statcan.gc.ca/n1/pub/75-006-x/2018001/article/54968-eng.htm
• Toftdahl et al. (2016). The effect of changes in cannabis exposure on psychotic symptoms in
patients with comorbid cannabis use disorder. Journal of Dual Diagnosis, 12(2), 129-136.
#TEACHwebinar
Educational Rounds 2018 69
References
• Trigo JM, Lagzdins D, Rehm J, Selby P, et al. (2016). Effects of fixed or self-titrated dosages of Sativex on cannabis withdrawal and cravings. Drug and Alcohol Dependence 161, 298-306.
• Trigo JM, Soliman A, Quilty LC, Fischer B, Rehm J, Selby P, et al. (2018) Nabiximols combined with motivational enhancement/cognitive behavioral therapy for the treatment of cannabis dependence: A pilot randomized clinical trial. PLoS ONE 13(1): e0190768. https://doi.org/10.1371/journal.pone.0190768van der Meer et al. (2015). Course of cannabis use and clinical outcome in patients with non-affective psychosis: A 3-year follow-up study. Psychological Medicine, 45(9), 1977-1988.
• Volkow et al. (2014). Adverse health effects of marijuana use. New England Journal of Medicine, 370, 2219-2227.
• Warf. (2014). High points: An historical geography of cannabis. Geographical Review,
104(4), 414-438.
• Whiting, P. F., et al. (2015). Cannabinoids for medical use: A systematic review and meta-
analysis. Journal of the American Medical Association, 313(24), 2456-2473.

#TEACHwebinar
Educational Rounds 2018 70
Thank you!
Dr. Peter Selby
#TEACHwebinar
Educational Rounds 2018 71
Remember …
• A link to the Evaluation and Post- Learning Assessment will be sent by e-mail by this afternoon. You will have one week to complete this Post-Learning Assessment in order to receive your Letter of Completion.
• If you participated as a group, make sure to email [email protected] with a complete list of participants by 2:00 PM EST today.

#TEACHwebinar
Educational Rounds 2018 72
Remember …
Next Educational Rounds Webinar:
Trauma Informed Care Presenter: Dr. Inbal Gafni, MSc, MD
Date: Wednesday, September 26, 2018 | 12:00-1:00pm EST
**Registration Open Soon**
#TEACHwebinar
Educational Rounds 2018 73
TEACH Educational Rounds Archives:
Missed the beginning of today’s presentation?
Want to view it again?
Interested in seeing previous TEACH webinars?
No problem! View the archived webinar links on our website! How do you access the archives?
The TEACH Project records all Educational Rounds webinars for later viewing, in case you are not able to attend the live session.
In order to access the archived webinars please visit our website
www.teachproject.ca “TEACH Educational Rounds” “Archive and Self Study” (here).

#TEACHwebinar
Educational Rounds 2018 74