tarceva ( erlotinib )
TRANSCRIPT

Tarceva® ( erlotinib )
By
Sirinoot Jantharangkul

Tarceva• Generic name: Erlotinib
• Brand name: Tarceva® • FDA Approval Date: November 18,
2004

Tarceva• Indicated for :the treatment of locally
advanced or metastatic non-small cell lung cancer that has failed prior chemotherapy
• Human Epidermal Growth Factor Receptor Type 1/Epidermal Growth Factor Receptor (HER1/EGFR) tyrosine kinase inhibitor
• Inhibits intracellular phosphorylation of tyrosine kinase associated with EGFR
Introduction

Introduction• Lung Cancer
– Non-Small Cell Lung Cancer
– Stage of Non-Small Cell Lung Cancer
• Tarceva in action – Cancer cell proliferation
– HER family of receptors and the role of
HER1/EGFR– Dysregulation of HER1/EGFR– Tarceva mechanism of inhibition
Introduction

Lung Cancer
• Two general types of lung cancer exist:
– Non-small cell lung cancer (NSCLC) – Small cell lung cancer
• The most common type of lung cancer is NSCLC. Approximately 147,000 new cases of NSCLC were reported in the United States in 2004.
Introduction

Main types of NSCLC• There are three main
types of NSCLC: – Adenocarcinoma (including
bronchioloalveolar carcinoma)
– Squamous cell carcinoma
– Large cell undifferentiated carcinoma
Introduction

Stage of Non-Small Cell Lung Cancer (NSCLC)
Introduction

Stage of Non-Small Cell Lung Cancer (NSCLC)
Introduction

Tarceva in action
• Cancer cell proliferation
• The Human Epidermal Receptor (HER) family of receptors
and the role of HER1/Epidermal Growth Factor Receptor (EGFR)
• Dysregulation of HER1/EGFR
• Tarceva mechanism of inhibition
Introduction
Cancer cell proliferationCancer cell proliferation Introduction

HER family of receptorsHER family of receptors Introduction

The role of EGFR
The role of EGFRThe role of EGFR
Introduction

HER1/EGFR dysregulationHER1/EGFR dysregulation
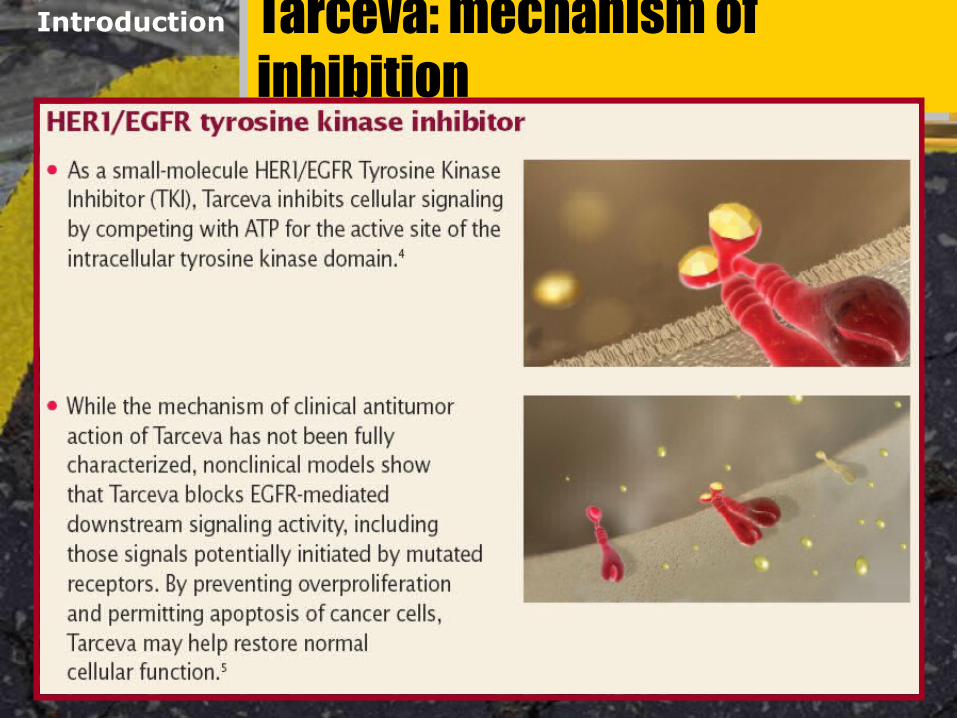
Tarceva: mechanism of inhibitionTarceva: mechanism of inhibition
Introduction


Tarceva
O
O
H3C
H3CO
O
NH
N
N
Tarceva (erlotinib)
• Small-molecule inhibitor of HER1/EGFR• Molecular wight 429.90• Orally available

Pharmacokinetics
• A: bioavailability ≈ 60%; food ↑ bioavailability to almost 100%
• D: ≈ 93% protein bound to albumin and alpha-1 acid glycoprotein
• M: primarily by CYP3A4 and to a lesser extent by CYP1A2
• E: mainly fecal (> 80%); t½= 36h
Introduction

Drug Interactions
• CYP3A4 inhibitors expected to increase exposure to erlotinib: ketoconazole increased AUC by 67%
• CYP3A4 inducers expected to decrease exposure to erlotinib: rifampicin increased clearance by 3-fold and reduced AUC by 67%

Adverse Effects
• Common adverse effects– Rash (75) [17]– Diarrhea (54) [18]– Anorexia (52) [38]– Dyspnea (41) [35]– Infection (24) [15]– Stomatitis (17) [3]– Pruritus (13) [5]
*(treatment) [placebo]

Monitoring
• Monitor for acute onset of new or progressive pulmonary symptoms such as dyspnea, cough, or fever
• If interstitial lung disease is diagnosed, discontinue erlotinib
• Consider dose adjustment with severe LFT changes (AST,ALT, Bili, Alk Phos)

Prescription Information
• Standard dose is 150 mg po daily taken at least one hour before or two hours after the ingestion of food
• Cost: #30 150 mg tablets $2125.02

Clinical studies :Tarceva: BR.21Tarceva: BR.21
Target enrolment
700 patients; stage IIIB or IV NSCLC
Prior therapy 1 or 2 chemotherapy regimensDesign Randomised 2:1
Tarceva 150mg/day plus BSC vs Placebo plus BSC
Primary endpoint
Overall survival
Secondary endpoints
Progression-free survivalSymptom deteriorationResponse rateTolerabilityTissue HER1/EGFR vs outcome/safety

BR.21 Progression Free Survival
SUMMARY STATISTICS:Log-Rank test for equality of groups: p=0.0000Wilcoxon test for equality of groups: p=0.0000Survival rate at 12 months for OSI-774: 8% - % C.I. ( 5%, 10%)Survival rate at 12 months for Placebo: 2% - % C.I. ( 0%, 4%)Hazard Ratio of Placebo/OSI-774: 1.572 - 95 % C.I. (1.337, 1.848)
OSI-774 Placebo
Perc
enta
ge
0
20
40
60
80
100
Time (months) # At Risk(OSI-774) # At Risk(Placebo)
0.0488243
5.015334
10.0526
15.081
20.010
Months
___ Erlotinib: 2.2 m
___ Placebo: 1.8 m
*HR 0.61, p <0.0001

BR.21 Overall Survival
SUMMARY STATISTICS:Log-Rank test for equality of groups: p=0.0018Wilcoxon test for equality of groups: p=0.0143Survival rate at 12 months for OSI-774: 31% - % C.I. ( 27%, 35%)Survival rate at 12 months for Placebo: 22% - % C.I. ( 16%, 27%)Hazard Ratio of Placebo/OSI-774: 1.309 - 95 % C.I. (1.105, 1.551)
OSI-774 Placebo
Perc
enta
ge
0
20
40
60
80
100
Time (months) # At Risk(OSI-774) # At Risk(Placebo)
0.0488243
10.018859
20.0124
30.000
___ Erlotinib: 6.7 m
___ Placebo: 4.7 m
*HR 0.71, p <0.0001
Months

BR.21 Survival by Smoking History
SUMMARY STATISTICS:Log-Rank test for equality of groups: p=0.0000
Smoked/OSI-774 Smoked/PlaceboNever Smoked/OSI-774 Never Smoked/Placebo
Perc
enta
ge
0
20
40
60
80
100
Time (months) # At Risk(Smoked/OSI-774) # At Risk(Smoked/Placebo)
# At Risk(Never Smoked/OSI-774) # At Risk(Never Smoked/Placebo)
0.035818710442
10.011646639
20.07340
30.00000
_____ Erlotinib Never Smoked
_____ Erlotinib Current/past Smoker
_____ Placebo Never Smoked
_____ Placebo Current/past smoker
Months

Selected BR.21 Adverse Events
76
17
55
19
4034
19
30
10
20
30
40
50
60
70
80
All G
rade
s, %
Rash Diarrhea Nausea St omat it is
erlot inibplacebo

Prolonged Time to Deterioration of QoL Symptoms
SUMMARY STATISTICS:Log-Rank test for equality of groups: p=0.0386
OSI-774 Placebo
Perc
enta
ge
0
20
40
60
80
100
Time (months) # At Risk(OSI-774) # At Risk(Placebo)
0.0298153
5.05920
10.0206
15.060
20.000
SUMMARY STATISTICS:Log-Rank test for equality of groups: p=0.0181
OSI-774 Placebo
Perc
enta
ge
0
20
40
60
80
100
Time (months) # At Risk(OSI-774) # At Risk(Placebo)
0.0348179
5.06516
10.0265
15.030
SUMMARY STATISTICS:Log-Rank test for equality of groups: p=0.0098
OSI-774 PlaceboPe
rcen
tage
0
20
40
60
80
100
Time (months) # At Risk(OSI-774) # At Risk(Placebo)
0.0353179
5.07820
10.0285
15.050
___ Erlotinib
___ Placebo
Cough : p=0.04
Dyspnea : p=0.01
Pain : p=0.02

BR.21 Summary• In patients who have failed standard
chemotherapy for NSCLC, erlotinib significantly improves– Response rates and progression free
survival– Overall survival– Disease related QoL and overall QoL
• Prolongation of survival was seen in most subsets of patients

Summary
• Tarceva™, erlotinib, is a Human Epidermal Growth Receptor Type 1/ Epidermal growth Factor Receptor (HER1/EGFR) tyrosine kinase inhibitor.
• Tarceva™ is indicated for the treatment of patients with locally advanced or metastatic nonsmall cell lung cancer (NSCLC) after failure of at least one prior chemotherapy regimen.

Summary
• Dermatologic and GI side effects are common.
• The incidence of Interstitial Lung Disease was the same as the placebo group (0.8%) in one trial.

References
1. http://www.tarceva,com. Accessed on 2/27/05
2. Tarceva™ package insert. Genentech. 2004 Downloaded from www.tarceva.com 2/27/05
3. http://www.drugstore.com. Accessed on 3/6/05

Common Approaches to Targeting HER1/EGFR
Introduction
Anti-HER1/EGFR-blocking antibodies
Anti-ligand-blocking
antibodies
TKinhibitors
Ligand–toxin
conjugates
Antibody–toxin
conjugates


Mechanism