tackling stigma associated with intellectual disability among the general public: a study of two...
TRANSCRIPT

Research in Developmental Disabilities 34 (2013) 2200–2210
Contents lists available at SciVerse ScienceDirect
Research in Developmental Disabilities
Tackling stigma associated with intellectual disability among
the general public: A study of two indirect contactinterventionsJessica Walker, Katrina Scior *
Department of Clinical Educational and Health Psychology, University College London, UK
A R T I C L E I N F O
Article history:
Received 17 December 2012
Received in revised form 26 March 2013
Accepted 26 March 2013
Available online 3 May 2013
Keywords:
Intellectual disabilities
Stigma
Attitude change
Interventions
Behavioral intentions
A B S T R A C T
Although evidence abounds that people with intellectual disabilities are exposed to stigma
and discrimination, few interventions have attempted to tackle stigma among the general
public. This study set out to assess the impact of two brief indirect contact interventions on
lay people’s inclusion attitudes, social distance and positive behavioral intentions, and to
explore emotional reactions towards the two interventions. 925 participants completed
the first online survey. Participants were randomized to watch either a 10 min film based
on intergroup contact theory, or a film based on a protest message. In total, 403
participants completed the follow-up survey at one month. Both interventions were
effective at changing inclusion attitudes and social distance in the short term and these
effects were partially maintained at one month. The protest based intervention had a
greater effect compared to the contact one on aspects of inclusion attitudes and evoked
stronger emotional reactions. Despite small effect sizes, brief indirect contact interven-
tions may have a potential role in tackling public stigma associated with intellectual
disability but their effects on behavioral intentions are questionable.
� 2013 Published by Elsevier Ltd.
1. Introduction
The International Classification of Functioning, Disability and Health (ICF) has suggested that ‘disability’ is definedaccording to environmental or contextual factors, and that negative societal attitudes are one of the most disabling factorsfor people with disabilities (World Health Organisation, 2001). Negative attitudes undoubtedly influence societal responsesand research in intellectual disabilities has tended to focus on prejudicial attitudes (Werner, Corrigan, Ditchman, & Sokol,2012). However, the concept of stigma can offer a broader perspective that does justice to the experiences of people withdisabilities. Stigma is an overarching term used to describe three elements: problems of knowledge (ignorance), attitudes(prejudice) and behavior (discrimination) (Thornicroft, Rose, Kassam, & Sartorius, 2007). The present study focused onstigma processes in the general population, referred to as ‘public stigma’ (Link et al., 1997).
While self-reported attitudes towards people with intellectual disabilities in recent research appear fairly positive (e.g.Ouellette-Kuntz, Burge, Brown, & Arsenault, 2010; Scior, Kan, McLoughlin, & Sheridan, 2010), discriminatory behaviortowards people with intellectual disability is an ongoing problem. There is ample evidence, for example, that people withintellectual disabilities continue to experience social exclusion, limited social relationships, very lower rates of employment,
* Corresponding author at: Department of Clinical Educational and Health Psychology, University College London, Gower Street, London WC1E 7HB, UK.
Tel.: +44 2076791897; fax: +44 20 7916 1989.
E-mail address: [email protected] (K. Scior).
0891-4222/$ – see front matter � 2013 Published by Elsevier Ltd.
http://dx.doi.org/10.1016/j.ridd.2013.03.024

J. Walker, K. Scior / Research in Developmental Disabilities 34 (2013) 2200–2210 2201
and a reduced likelihood of participating in community based activities (Verdonschot, de Witte, Reichrath, Buntinx, & Curfs,2009). In many cases, people with intellectual disabilities who participate in community activities are subject to hostilityfrom non-disabled peers and find this experience stressful (Cummins & Lau, 2003; Stalker & Lerpiniere, 2009). More recently,researchers and disability rights campaigners have drawn attention to hate crimes committed against people withintellectual disabilities, alongside frequent instances of bullying, abuse and harassment (Fyson & Kitson, 2010; Quarmby,2008; Sheikh et al., 2010; Sin et al., 2009). Hence it would seem that there remains a problem of societal attitudes which aresanctioning discriminatory behaviors in some way. Some have gone as far as proposing that ‘‘casual disablism permeates oursociety’’ (Quarmby, 2008, p. 32).
Finding effective ways of challenging negative attitudes and discriminatory behaviors should be a priority for researchersin intellectual disabilities. As recent theoretical evidence suggests that the constructs of prejudice and stigma overlap andcomplement each other (Phelan et al., 2008), interventions to challenge public stigma have drawn on theories of attitudechange. For example, intergroup contact theory hypothesis (Allport, 1954; Pettigrew, 1998) posits that direct interactionbetween members of the in-group and out-group can improve prejudicial attitudes. Allport (1954) originally named fourconditions necessary for positive attitude change, namely (a) equal status between members of different groups; (b) workingcooperatively; (c) working on a common goal; and (d) the perception that the interaction receives social sanction. However,there is now considerable evidence to suggest that these conditions are not needed and contact alone, or mere exposure, canbe an effective means of attitude change (Pettigrew, 1998; Pettigrew & Tropp, 2006; Zajonc, 2001). Several studies havefound a positive effect of direct contact on attitudes towards those with intellectual disabilities (McConkey et al., 1993;Rillotta & Nettelbeck, 2007; Roper, 1990). While direct contact is highly valuable, it can be difficult to secure on a large scaleand in positive way. Potentially more promising is the use of indirect contact via film footage which has the possibility ofreaching much larger audiences as part of anti-stigma interventions.
Several evaluations of indirect contact interventions show some promising results (Carsrud, Ahlgren, & Dood, 1986; Hall& Minnes, 1999; Smedema, Ebener, & Grist-Gordon, 2012). The effects of either a TV documentary or drama about a personwith Down’s syndrome on students’ willingness to volunteer with intellectual disability services was compared by Hall andMinnes (1999). The documentary was associated with greater feelings of comfort and increased willingness to volunteerintentions (Hall & Minnes, 1999). The authors explained these differences with reference to the perceived authority of thepresenter in the documentary and to differences in the way information was presented. Unfortunately, these results arelimited by a small sample size (N = 92 split across a control and two intervention groups) and lack of repeated measuresdesign. A study by Smedema et al. (2012) found that a humorous film resulted in more positive attitudes than a filmpromoting ideas of similarity and inclusion or a control film. The authors suggested that humor provides a non-threateningand less anxiety provoking means of communicating information about disability (Smedema et al., 2012). Their studyunfortunately did not assess emotional reactions, which are important to bear in mind in designing stigma changeinterventions. Social psychological research has suggested that dramatic portrayals (i.e. via film) promote persuasion bycreating an experiential learning situation, engendering an empathic emotional response, and encouraging inferentialprocesses in the viewer (Stern, 1994). Furthermore, there is evidence from social marketing campaigns that persuasionoccurs by creating an emotional response in the viewer (Joffe, 2008).
Existing indirect contact interventions (Carsrud et al., 1986; Hall & Minnes, 1999; Smedema et al., 2012) have providedpositive portrayals of people with intellectual disabilities integrated into their communities and closely match Allport’s(1954) conditions of contact. An alternative intervention is known as ‘protest’, which highlights the injustice of stigma andcreates a moral appeal for people to change their beliefs (Corrigan & Penn, 1999; Corrigan et al., 2001). At present, empiricalevidence does not support the application of protest interventions to influence mental illness stigma (Corrigan et al., 2001;Macrae, Bodenhausen, Milne, & Jetten, 1994; Thornton & Wahl, 1996). However, an experimental study found that protestcould influence attitudes (Penn & Corrigan, 2002), and as such, warrants further research. Therefore, this paper will considerthe potential of protest messages delivered via indirect contact, as a way of tackling stigma towards people with intellectualdisabilities.
Behavioral intentions are considered a precursor of actual behavior (Ajzen, 1991). Research has shown that behavioralintentions predict around 40% of the variance in actual behavior (Armitage & Conner, 2001). Thus assessing the impact of anyintervention on behavioral intentions is important, yet to date only one study in the intellectual disability field has expandedthe assessment of stigma change to include a measure of potential behavior (Hall & Minnes, 1999)
The present study aimed to explore the impact of indirect contact, that is exposure to individuals with intellectualdisabilities via the medium of film, on public stigma towards people with intellectual disabilities. In order to rectify gaps inthe evidence, the study used a measure of not only external stigma (inclusion attitudes) and social distance, but also positivebehavioral intentions. Data were collected at baseline, immediately post intervention and at one month follow-up to assesswhether a brief intervention can produce changes in attitudes and behavioral intentions, and importantly whether anychanges are maintained over time. Emotional reactions to the interventions were compared to enhance our understanding offactors that may affect the stigma change process.
Two interventions were compared; both consisted of 10 minute films that included an expert talking head outlining whatintellectual disabilities are and noting that many people with this condition are still not treated as equal citizens. One of theinterventions attempted to match Allport’s (1954) conditions of contact, the other one was designed to test the effects of aprotest approach, by focusing on injustices, harassment and discrimination experienced by people with intellectualdisabilities.
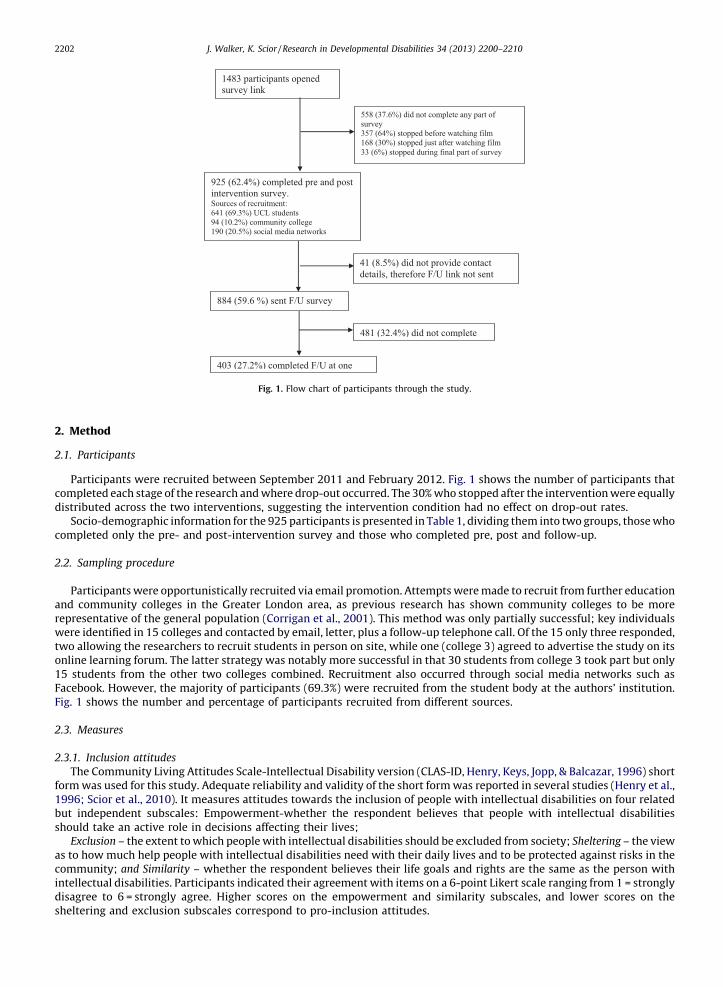
1483 pa rtic ipant s opened
survey link
925 (62.4 %) co mpl eted pr e and post
interv ention su rvey . Source s of rec rui tment:
641 (69.3%) UCL students
94 (10 .2% ) co mmunity coll ege
190 (20.5%) social media networks
558 (37. 6%) d id n ot complet e a ny pa rt of
survey
357 (64%) stopp ed b efore watching film
168 (30%) stopp ed just aft er wa tchi ng fi lm
33 (6%) st opp ed duri ng final pa rt of survey
884 (59.6 %) sen t F/U survey
41 (8.5 %) d id not p rovi de con tact
details, therefore F/U l ink not sent
403 (27.2 %) co mpl eted F/U at one
481 (32.4%) did not co mpl ete
Fig. 1. Flow chart of participants through the study.
J. Walker, K. Scior / Research in Developmental Disabilities 34 (2013) 2200–22102202
2. Method
2.1. Participants
Participants were recruited between September 2011 and February 2012. Fig. 1 shows the number of participants thatcompleted each stage of the research and where drop-out occurred. The 30% who stopped after the intervention were equallydistributed across the two interventions, suggesting the intervention condition had no effect on drop-out rates.
Socio-demographic information for the 925 participants is presented in Table 1, dividing them into two groups, those whocompleted only the pre- and post-intervention survey and those who completed pre, post and follow-up.
2.2. Sampling procedure
Participants were opportunistically recruited via email promotion. Attempts were made to recruit from further educationand community colleges in the Greater London area, as previous research has shown community colleges to be morerepresentative of the general population (Corrigan et al., 2001). This method was only partially successful; key individualswere identified in 15 colleges and contacted by email, letter, plus a follow-up telephone call. Of the 15 only three responded,two allowing the researchers to recruit students in person on site, while one (college 3) agreed to advertise the study on itsonline learning forum. The latter strategy was notably more successful in that 30 students from college 3 took part but only15 students from the other two colleges combined. Recruitment also occurred through social media networks such asFacebook. However, the majority of participants (69.3%) were recruited from the student body at the authors’ institution.Fig. 1 shows the number and percentage of participants recruited from different sources.
2.3. Measures
2.3.1. Inclusion attitudes
The Community Living Attitudes Scale-Intellectual Disability version (CLAS-ID, Henry, Keys, Jopp, & Balcazar, 1996) shortform was used for this study. Adequate reliability and validity of the short form was reported in several studies (Henry et al.,1996; Scior et al., 2010). It measures attitudes towards the inclusion of people with intellectual disabilities on four relatedbut independent subscales: Empowerment-whether the respondent believes that people with intellectual disabilitiesshould take an active role in decisions affecting their lives;
Exclusion – the extent to which people with intellectual disabilities should be excluded from society; Sheltering – the viewas to how much help people with intellectual disabilities need with their daily lives and to be protected against risks in thecommunity; and Similarity – whether the respondent believes their life goals and rights are the same as the person withintellectual disabilities. Participants indicated their agreement with items on a 6-point Likert scale ranging from 1 = stronglydisagree to 6 = strongly agree. Higher scores on the empowerment and similarity subscales, and lower scores on thesheltering and exclusion subscales correspond to pro-inclusion attitudes.

Table 1
Socio-demographic data and baseline scores for those who completed pre-post intervention only (n = 522) and those who completed pre-post intervention
and follow-up (n = 403).
Completed pre-post only Completed pre-post and follow-up
N % M (SD) N % M (SD)
Age (years) 26.3 (11.29) 25.8 (10.39)
Gender
Female 353 67.6 263 65.3
Male 169 32.4 140 35.7
Education
Up to 18 years 150 28.7 101 25
Degree 191 36.6 134 33.3
Post-graduate degree 181 34.7 168 41.7
Ethnicity
White British 209 40 152 37.7
Asian 129 24.7 87 21.1
Black African/Caribbean/British 28 5.4 11 2.7
Middle Eastern 47 9 36 8.9
White other 109 20.9 117 29.1
Previous contact
Know someone with ID 303 58.0 238 59.1
Work with someone with ID 178 34.1 143 35.1
Intervention completed
Intervention 1 267 51.1 210 52.2
Intervention 2 255 48.9 193 47.8
Baseline scores
Social desirability 5.61 (1.71) 5.38 (1.81)
Inclusion attitudes (CLAS-ID)
Empowerment 4.53 (0.78) 4.55 (0.80)
Exclusion 1.61 (0.74) 1.55 (0.71)
Sheltering 3.25 (0.91) 3.21 (0.86)
Similarity 5.37 (0.72) 5.42 (0.70)
Social distance 2.34 (1.25) 2.41 (1.24)
J. Walker, K. Scior / Research in Developmental Disabilities 34 (2013) 2200–2210 2203
2.3.2. Social distance
Desire for social contact was measured using items replicated from Link, Phelan, Bresnahan, Stueve and Pescosolido(1999). Respondents rated their agreement with five items of increasing intimacy using a 7-point Likert scale (1 = stronglydisagree to 7 = strongly agree). The total score is a mean of reversed items; higher scores indicate increased social distance.High internal consistency for this scale (a = .87) was reported by Scior and Furnham (2011).
2.3.3. Positive behavioral intentions
Two items were developed for this study to measure positive behavioral intentions relating closely tothe interventions: (1) ‘‘If I heard about a cultural event, such as a concert or play, featuring people with learningdisabilities I would attend’’; and (2) ‘‘If I saw an adult with learning disabilities being harassed in the streets byyoung people I would intervene’’. These were administered to all respondents, regardless of film condition. Bothitems had associated control items in order to control for general intentions to attend concerts or intervene whenwitnessing anyone being harassed in the street. Responses were measured on the same 7-point Likert scale as socialdistance.
2.3.4. Emotional reactions
The Emotional Reactions to Mental Illness Scale ERMIS (Angermeyer & Matschinger, 2003) was used to measureemotional responses to the stigma change interventions on three subscales: compassion/pity, fear and anger. In total, nineitems were rated using a 7-point Likert scale. The measure was previously used in an intellectual context by Connolly,Williams and Scior (in press). who reported good validity and reliability for the fear and anger subscales, and for the pitysubscale once the third item (desire to help) was removed.
2.3.5. Social desirability
The Marlowe–Crowne Social Desirability Scale 10-item version (Strahan & Gerbasi, 1972) was administered at baseline tomeasure the extent to which participants provide socially desirable responses.
2.3.6. Demographics
Participants reported their age, gender, ethnicity, religious affiliations, highest educational attainment and previouscontact with someone with intellectual disabilities, both in a personal and work context.

J. Walker, K. Scior / Research in Developmental Disabilities 34 (2013) 2200–22102204
2.4. Design
A 3 � 2 mixed design (three time points � two interventions) was employed. The outcome variables were scores on theCLAS-ID (Henry et al., 1996), social distance (Link et al., 1999) and positive behavioral intentions.
2.5. Stigma change conditions
The stigma change films were 10 min long and were in three parts: (1) an introduction delivered by an expert outlininghow intellectual disability is defined, inequalities faced by this population and a brief introduction to the themes relating toeach film clip; (2) film clips showing people with intellectual disabilities (see below); and (3) the same expert summarizingkey points made in each film.
2.5.1. Intervention 1
In addition to the elements outlined above, the 10 min film showed 8 min of clips from a documentary film on a rock bandthat includes people with and without intellectual disabilities. The excerpts selected aimed to meet conditions described byAllport (1954) as it showed people with and without disabilities working together on a common goal. It also promotedthemes used by disability advocacy groups by emphasizing shared hopes and values of people with and without disabilitiesand the benefits of integration.
2.5.2. Intervention 2
This included 8 min of clips from a documentary film about hate crime experienced by people with intellectualdisabilities and focused on a man with intellectual disabilities. As with the first intervention, the film focused on sharedgoals, in particular, a desire to work and contribute to society. However, the film also showed the man experiencingdiscrimination in seeking employment and being harassed and exploited by members of the public. As such the key messagein the second intervention was that harassment and victimization are common occurrences in the lives of people withintellectual disabilities.
2.6. Procedure
Potential participants were sent an email inviting them to take part in a survey on attitudes towards people with ‘learningdisabilities’, the most commonly used term in the UK. The invitation contained a link that took participants to a moredetailed information sheet and the survey.
Following completion of the baseline measures, participants were randomized to either stigma change condition.Following the intervention, participants’ emotional reactions to the material presented were assessed and measures ofinclusion attitudes, social distance and positive behavioral intentions were repeated. Socio-demographic variables wererecorded at this point. Participants were invited to provide their contact details to take part in a prize draw at this point andwere asked for their permission to be contacted again for the follow-up. Following a one month interval, all 884 participantswho provided their contact details and consented to being contacted again were sent a link to the follow-up survey. Inclusionattitudes, social distance, and positive behavioral intentions were measured for the third time. Participants who took part inthe follow-up were given a second opportunity to enter the prize draw, and were again asked for their contact details toallow matching of baseline and follow-up responses.
2.7. Statistical analysis
The data were analyzed using SPSS version 19. Independent sample t-tests were employed to test for significantdifferences between those who dropped out following the first survey (pre–post intervention) and those who completed theone month follow-up according to age, social desirability and baseline inclusion attitudes/social distance scores. Pairedsamples t-tests were used to assess the immediate impact of the intervention on inclusion attitudes and social distance. Thisprocedure was selected because it allowed the inclusion of all 925 participants who completed the pre- and post-intervention measures, rather than just the 403 who completed the measures at all three time points. This was followed by2 � 2 ANOVA to compare interventions on immediate changes in inclusion attitudes and social distance. A 3 � 2 mixeddesign ANOVA assessed changes over time, differences according to intervention condition, and potential interaction effectson inclusion attitudes and social distance. Changes in positive behavioral intentions while controlling for general behavioralintentions were examined using ANCOVA. Emotional reactions to the interventions were compared using independentsamples t-tests.
3. Results
In comparing those who only completed the first survey and those who completed all stages, including the follow-upsurvey, the only difference identified was for social desirability, see Table 1. Those who completed the follow-up scoredlower on social desirability (M = 5.38, SD = 1.81) compared to those who did not complete follow-up (M = 5.61, SD = 1.71), t
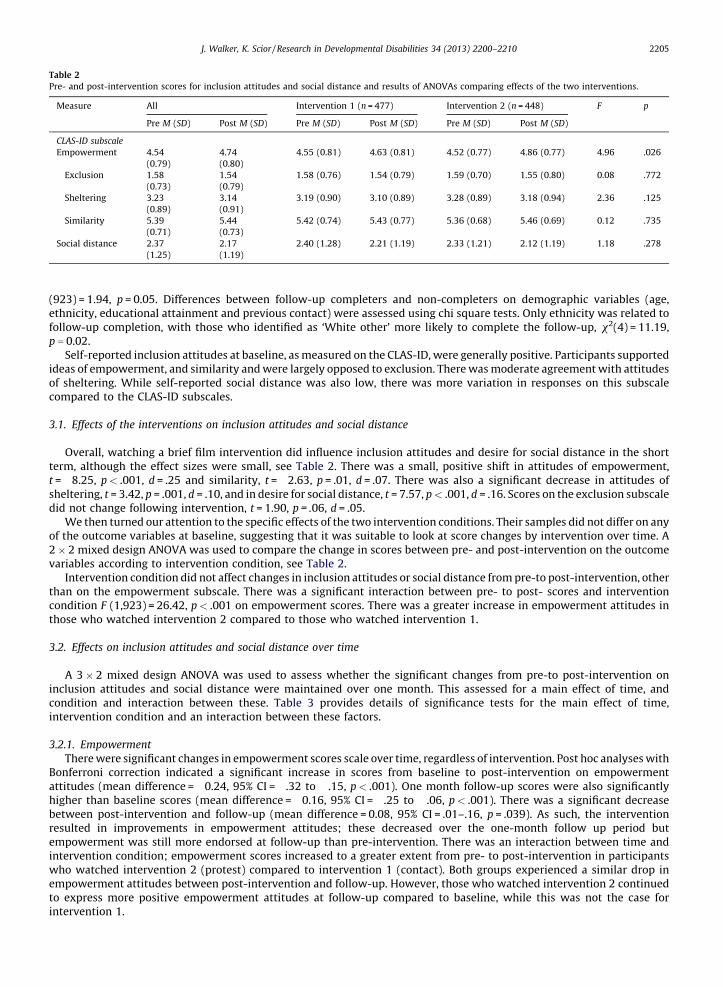
Table 2
Pre- and post-intervention scores for inclusion attitudes and social distance and results of ANOVAs comparing effects of the two interventions.
Measure All Intervention 1 (n = 477) Intervention 2 (n = 448) F p
Pre M (SD) Post M (SD) Pre M (SD) Post M (SD) Pre M (SD) Post M (SD)
CLAS-ID subscale
Empowerment 4.54 4.74 4.55 (0.81) 4.63 (0.81) 4.52 (0.77) 4.86 (0.77) 4.96 .026
(0.79) (0.80)
Exclusion 1.58 1.54 1.58 (0.76) 1.54 (0.79) 1.59 (0.70) 1.55 (0.80) 0.08 .772
(0.73) (0.79)
Sheltering 3.23 3.14 3.19 (0.90) 3.10 (0.89) 3.28 (0.89) 3.18 (0.94) 2.36 .125
(0.89) (0.91)
Similarity 5.39 5.44 5.42 (0.74) 5.43 (0.77) 5.36 (0.68) 5.46 (0.69) 0.12 .735
(0.71) (0.73)
Social distance 2.37 2.17 2.40 (1.28) 2.21 (1.19) 2.33 (1.21) 2.12 (1.19) 1.18 .278
(1.25) (1.19)
J. Walker, K. Scior / Research in Developmental Disabilities 34 (2013) 2200–2210 2205
(923) = 1.94, p = 0.05. Differences between follow-up completers and non-completers on demographic variables (age,ethnicity, educational attainment and previous contact) were assessed using chi square tests. Only ethnicity was related tofollow-up completion, with those who identified as ‘White other’ more likely to complete the follow-up, x2(4) = 11.19,p = 0.02.
Self-reported inclusion attitudes at baseline, as measured on the CLAS-ID, were generally positive. Participants supportedideas of empowerment, and similarity and were largely opposed to exclusion. There was moderate agreement with attitudesof sheltering. While self-reported social distance was also low, there was more variation in responses on this subscalecompared to the CLAS-ID subscales.
3.1. Effects of the interventions on inclusion attitudes and social distance
Overall, watching a brief film intervention did influence inclusion attitudes and desire for social distance in the shortterm, although the effect sizes were small, see Table 2. There was a small, positive shift in attitudes of empowerment,t = �8.25, p < .001, d = .25 and similarity, t = �2.63, p = .01, d = .07. There was also a significant decrease in attitudes ofsheltering, t = 3.42, p = .001, d = .10, and in desire for social distance, t = 7.57, p < .001, d = .16. Scores on the exclusion subscaledid not change following intervention, t = 1.90, p = .06, d = .05.
We then turned our attention to the specific effects of the two intervention conditions. Their samples did not differ on anyof the outcome variables at baseline, suggesting that it was suitable to look at score changes by intervention over time. A2 � 2 mixed design ANOVA was used to compare the change in scores between pre- and post-intervention on the outcomevariables according to intervention condition, see Table 2.
Intervention condition did not affect changes in inclusion attitudes or social distance from pre-to post-intervention, otherthan on the empowerment subscale. There was a significant interaction between pre- to post- scores and interventioncondition F (1,923) = 26.42, p < .001 on empowerment scores. There was a greater increase in empowerment attitudes inthose who watched intervention 2 compared to those who watched intervention 1.
3.2. Effects on inclusion attitudes and social distance over time
A 3 � 2 mixed design ANOVA was used to assess whether the significant changes from pre-to post-intervention oninclusion attitudes and social distance were maintained over one month. This assessed for a main effect of time, andcondition and interaction between these. Table 3 provides details of significance tests for the main effect of time,intervention condition and an interaction between these factors.
3.2.1. Empowerment
There were significant changes in empowerment scores scale over time, regardless of intervention. Post hoc analyses withBonferroni correction indicated a significant increase in scores from baseline to post-intervention on empowermentattitudes (mean difference = �0.24, 95% CI = �.32 to �.15, p < .001). One month follow-up scores were also significantlyhigher than baseline scores (mean difference = �0.16, 95% CI = �.25 to �.06, p < .001). There was a significant decreasebetween post-intervention and follow-up (mean difference = 0.08, 95% CI = .01–.16, p = .039). As such, the interventionresulted in improvements in empowerment attitudes; these decreased over the one-month follow up period butempowerment was still more endorsed at follow-up than pre-intervention. There was an interaction between time andintervention condition; empowerment scores increased to a greater extent from pre- to post-intervention in participantswho watched intervention 2 (protest) compared to intervention 1 (contact). Both groups experienced a similar drop inempowerment attitudes between post-intervention and follow-up. However, those who watched intervention 2 continuedto express more positive empowerment attitudes at follow-up compared to baseline, while this was not the case forintervention 1.

Table 3
Pre-post and follow-up scores for inclusion attitudes and social distance according to overall group and split by intervention 1 (n = 210) and intervention 2
(n = 193).
Measure Time point Overall scores Intervention 1 Intervention 2 Main effect time Main effect
film
Interaction
M (SD) M (SD) M (SD) F p F p F p
CLAS-ID subscale
Empowerment Pre 4.55 (0.78) 4.59 (0.76) 4.50 (0.84) 22.37 <.001 2.79 .095 11.56 <.001
Post 4.76 (0.78) 4.67 (0.76) 4.89 (0.78) (2, 802) (1.401) (2802)
Follow-up 4.72 (0.74) 4.61 (0.80) 4.80 (0.73)
Exclusion Pre 1.54 (0.65) 1.55 (0.75) 1.55 (0.66) 2.89 .056 0.07 .786 0.67 .51
Post 1.51 (0.75) 1.48 (0.71) 1.50 (0.76) (2, 802) (1.401) (2802)
Follow-up 1.48 (0.67) 1.49 (0.75) 1.55 (0.78)
Sheltering Pre 3.23 (0.89) 3.17 (0.85) 3.26 (0.87) 3.23 .04 0.02 .888 2.33 .098
Post 3.13 (0.90) 3.12 (0.88) 3.14 (0.92) (2, 802) (1.401) (2802)
Follow-up 3.11 (0.82) 3.16 (0.86) 3.09 (0.78)
Similarity Pre 5.40 (0.70) 5.46 (0.70) 5.36 (0.69) 8.98 <.001 0.62 .431 1.43 .241
Post 5.46 (0.72) 5.50 (0.70) 5.50 (0.66) (2, 802) (1.401) (2802)
Follow-up 5.56 (0.58) 5.55 (0.59) 5.52 (0.62)
Social distance Pre 2.34 (1.22) 2.41 (1.24) 2.41 (1.25) 15.07 <.001 0.36 .551 0.99 .368
Post 2.13 (1.15) 2.23 (1.17) 2.14 (1.23) (2, 802) (1.401) (2802)
Follow-up 2.21 (1.18) 2.31 (1.23) 2.20 (1.18)
Table 4
Pre-, post and follow-up positive behavioral intentions for intervention 1 (n = 210) and intervention 2 (n = 193).
Intention by intervention condition Time point Behavioral intentions Main effect time Time * intervention
condition
M (SD) F p F p
See concert
Intervention 1 Pre 4.61 (1.63)
Post 4.77 (1.69) 5.48 .004 0.31 .74
Follow-up 4.63 (1.71) (2,400) (2,400)
Intervention 2 Pre 4.62 (1.61)
Post 4.80 (1.70)
Follow-up 4.57 (1.69)
Stop harassment
Intervention 1 Pre 5.65 (1.35)
Post 5.80 (1.34) 6.87 .001 0.93 .39
Follow-up 5.73 (1.40) (2,400) (2,400)
Intervention 2 Pre 5.75 (1.29)
Post 5.91 (1.25)
Follow-up 5.73 (1.35)
J. Walker, K. Scior / Research in Developmental Disabilities 34 (2013) 2200–22102206
3.2.2. Exclusion
There was no significant main effect for time, or intervention condition on this subscale.
3.2.3. Sheltering
There was a significant main effect for time on the sheltering subscale. Post hoc analyses with Bonferroni correctionindicated that there was no significant change in sheltering attitudes from pre- to post-intervention (mean difference = 0.09,95% CI = �.01 to .18, p = .11) and no significant difference between pre-intervention and follow-up (mean difference = 0.09,95% CI = �.01 to .18, p = .08). Thus, when using a 5% significance level, the differences between sheltering scores according totime were not meaningful. However, planned linear contrasts with a less conservative alpha value found a significantdifference pre- to post-intervention (F(1,401) = 4.38, p = .04) and pre-intervention to follow-up (F(1,401) = 4.87, p = .03). Thisindicates that the intervention did affect sheltering attitudes and these effects were maintained at one-month, althoughthese results should be interpreted with caution as a less conservation alpha value was applied. Overall, there was no maineffect of intervention condition, and no significant interaction between time and intervention. However, planned contraststhat considered the interaction between pre-intervention and follow-up according to intervention condition found asignificant effect (F(1,401) = 4.48, p = .04). Sheltering scores decreased over time in those who watched intervention 2, butremained constant in intervention 1 viewers.

J. Walker, K. Scior / Research in Developmental Disabilities 34 (2013) 2200–2210 2207
3.2.4. Similarity
There was a significant main effect of time on the similarity scale. Post hoc analyses with Bonferroni correction indicatedthat pre-intervention scores were significantly lower than post-intervention (mean difference = �0.09, 95% CI = �.16 to �.02,p = .01) and follow-up scores (mean difference = �0.13, 95% CI = �.2 to �.05, p < .001). There was no significant differencebetween post-intervention and follow-up (mean difference = �0.04, 95% CI = �.12 to .03, p = .55). As such, followingintervention, endorsement of similarity items had increased and the increase was maintained at one month. There was nomain effect of intervention condition, and no interaction between time and intervention condition.
3.2.5. Social distance
There was a significant effect of time on social distance scores. Post hoc analyses with Bonferroni correction revealed thatsocial distance scores decreased significantly from pre- to post-intervention (mean difference = 0.22, 95% CI = .13–.31,p < .001) and pre-intervention to follow-up (mean difference = 0.16, 95% CI = .05–.27, p < .001). Social distance scores did notchange significantly from post-intervention to follow-up (mean difference = �0.06, 95% CI = �.15 to .04, p = .43). Thus socialdistance decreased and this effect was maintained over time. There was no significant effect of intervention condition, andno interaction between time and intervention condition.
3.3. Effects on positive behavioral intentions
To assess whether the two groups differed in their general behavioral intentions, initially responses to the control itemswere compared at baseline. Participants presented with intervention 1 (contact) were as likely as those presented withintervention 2 (protest) to attend concerts, t = 0.64, p = .52, or to say they would intervene if they saw anyone being harassedin public, t = �0.96, p = .34. Therefore general behavioral intentions were not controlled for in subsequent analyses.
For both interventions there was a significant effect of time, see Table 4. Post hoc analyses with Bonferroni correctionrevealed a significant positive shift in behavioral intentions from pre- to post-intervention for intervention 1 (meandifference = �.17, 95% CI = �.27 to �.08, p = .001) and intervention 2 (mean difference = �.16, 95% CI = �.22 to �.09, p < .001).However, for both interventions intention scores at follow-up had reverted to baseline levels (mean difference pre- tofollow-up for intervention 1 = .01, 95% CI = �.13 to .15, p = .87; for intervention 2 = �.03, 95% CI = �.13 to .07, p = .54).Therefore both interventions had only short term positive effects on behavioral intentions, and these effects were not specificto the intervention.
3.4. Emotional reactions to the interventions
Self-reported emotional reactions to the two interventions are presented in Table 5. Intervention 2 resulted in strongerreactions on all emotion items, both in terms of negative and positive emotions.
4. Discussion
The present study investigated the impact of two indirect contact interventions on inclusion attitudes, social distance andpositive behavioral intentions both in the short term and after one month. It also explored emotional reactions towards theinterventions. The main findings can be summarized as follows: (1) indirect contact interventions had a small but significantshort term impact on inclusion attitudes and social distance; (2) the intervention effects were maintained at one month onsocial distance and two of the CLAS-ID subscales, empowerment and similarity; (3) the ‘protest’ intervention resulted in agreater increase in empowerment attitudes and a greater decrease in sheltering attitudes; (4) it also provoked strongeremotional responses than the contact intervention; and (5) while there was a short term positive shift in behavioral intentionsin response to both interventions, this was not maintained over time nor was it specific to the intervention delivered.
Table 5
Emotional reactions to watching intervention 1 (n = 477) and intervention 2 (n = 448).
Emotional reaction Intervention 1 Intervention 2 t
M (SD) M (SD)
Scared 1.79 (1.38) 3.21 (1.80) �13.38**
Sympathetic 5.32 (1.56) 6.16 (1.15) �9.36**
Angry 2.57 (1.69) 5.65 (1.42) �30.07**
Uncomfortable 2.34 (1.66) 4.42 (1.92) �17.59**
Insecure 2.00 (1.38) 2.96 (1.69) �9.41**
Irritated 2.04 (1.50) 4.63 (1.95) �22.48**
Empathic 5.08 (1.69) 5.54 (1.51) �4.32**
Annoyed 2.19 (1.58) 4.78 (1.90) �22.42**
Helpful and giving 4.99 (1.50) 5.25 (1.44) �2.68*
* p < .01.
** p < .001

J. Walker, K. Scior / Research in Developmental Disabilities 34 (2013) 2200–22102208
Overall, the results would seem to hold some promise for efforts to reduce stigma and negative attitudes towards peoplewith intellectual disabilities on a much larger scale than has been attempted by most interventions to date. Although effectsizes were small, watching a ten minute intervention resulted in greater support for the view that people with intellectualdisabilities should play an active role in making decisions about their own lives and that they have similar life goals andrights as those without disabilities. The interventions also resulted in greater disagreement with the notion that people withintellectual disabilities need to be protected against the risks of community living, and a short term reduction in desire forsocial distance. The findings are in line with other research supporting the short term effects of indirect contact onstigmatizing attitudes towards people with intellectual disabilities (Hall & Minnes, 1999; Smedema et al., 2012). As such, thecurrent findings suggest that mere exposure is sufficient to have a positive effect on attitudes (Pettigrew & Tropp, 2006;Pettigrew, 1998; Zajonc, 2001) and that interventions designed in line with Allport’s (1954) conditions of contact are perhapsnot most effective in tackling negative lay responses.
While most previous attitude change evaluations in the intellectual disability field have not included follow-up data, thecurrent study tested the effects of the two interventions at one-month. Changes in a desirable direction on two of the fourCLAS-ID subscales and on social distance were maintained at follow-up. While there are no previous findings in theintellectual disabilities field to compare the present results to, a comparison to efforts aimed at tackling mental illness stigmaseems appropriate. A study of filmed contact by Corrigan et al., 2007, for example, found positive changes on measures ofpity, avoidance and segregation that were maintained over a one week period. A study which included a one month follow-up and used the Community Attitudes to Mental Illness scale (CAMI, Taylor & Dear, 1981), from which the CLAS-ID is derived,found reductions in authoritarianism and social restrictiveness and an increase in benevolence at one month (Faigin & Stein,2008). These findings contrast somewhat with the current study, as exclusion, the outcome most similar to the CAMI’s socialrestrictiveness subscale, did not change in response to the interventions.
An important consideration is whether these changes observed are meaningful in the real world. Are they likely, forexample, to indicate any real change in terms of how members of the general public think about and behave towards thosewith intellectual disabilities? While the reader may well feel that the changes reported are too small to be meaningful, thequestion of what magnitude change can realistically be achieved in any interventions targeting the general public is animportant question that has not been addressed in the intellectual disability field to date. We found a 6% increase inempowerment attitudes in those who received the protest intervention at one month follow-up, and a 3% increase insimilarity attitudes and 2% reduction in social distance, regardless of intervention. Other short term effects were notmaintained. The largest mental illness anti-stigma campaign ever to run in the UK, Time to Change, is far more comprehensivethan the fairly minimal intervention reported in this article. It includes a media and mass marketing campaign aimed atreaching 29 million adults and aims to result in a five per cent shift in attitudes (Department of Health, 2012). We cite thisfigure as a possible benchmark for debate, rather than a figure against which our findings should be compared given thatTime to Change targets a general population audience with more varied educational backgrounds than our sample.
With regards to the question what type of intervention may be most effective at improving lay responses, the findingsindicate that protest interventions may have more scope than the existing literature would suggest. Alternatively, theapparent effectiveness of the protest intervention may be directly attributable to the background of the studied populationand their already favorable baseline attitudes. Certainly it would seem that the potential benefits of bringing individual casestories and the real life effects of discrimination and harassment of people with intellectual disabilities to the attention of thepublic merit further consideration. It has been suggested that protest interventions are less helpful because they create‘psychological reactance’ (Brehm, 1996), meaning that people are less likely to develop a new way of thinking if they havebeen instructed to do so. Furthermore, the rebound hypothesis (Macrae et al., 1994), which states that being instructed tosuppress prejudicial thoughts actually results in an increase in these thoughts, would argue against such interventions.However, empirical investigations of the influence of suppression in tackling mental illness stigma have shown that it doesnot necessarily result in rebound (Penn & Corrigan, 2002). What appears fundamental in the present study is that the protestintervention merely highlighted injustices, without telling the viewer how they should respond cognitively, emotionally orindeed behaviorally, but as noted a more representative audience may be less receptive to such an approach.
The finding that protest may be helpful for stigma change is valuable because frequent bullying, abuse and hate crimetargeting people with intellectual disabilities has only fairly recently been fully recognized by the government and deemedin need of addressing (Equality & Human Rights Commission, 2011). It has been suggested that the public need to becomeaware of the scope of the problem (Quarmby, 2008). The current findings support this argument, but also suggest that reallife case studies without instructing the viewer on how to respond may be most helpful.
It is possible that the protest intervention resulted in a greater change in attitudes due to the stronger positive andnegative emotional reactions it elicited. Other intellectual disability research has hypothesized that emotional processesplay a role in stigma change (Smedema et al., 2012) but to date these have only rarely been formally tested. In contrast,literature on persuasion and attitude change highlights the importance of emotional engagement in order to facilitatememory of the material and influence attitude change (Joffe, 2008). Furthermore, Stern (1994) emphasized that an empathicemotional response towards a film will increase persuasion.
The current study included measures of behavioral intentions as, admittedly limited, predictors of behavior (Ajzen, 1991).While both intention items shifted in a positive direction immediately after the intervention, by the time of follow-up theyhad reverted to baseline levels. As positive behavioral intentions were measured using a single item for each intervention, itis possible that poor measurement explains these findings. Alternatively, brief interventions such as the ones reported here

J. Walker, K. Scior / Research in Developmental Disabilities 34 (2013) 2200–2210 2209
are perhaps unlikely to have a sustained impact on behavioral intentions; instead it is likely that more comprehensive andtargeted strategies would need to be incorporated into stigma change efforts. Furthermore future research should considerthe feasibility of measuring changes in actual behavior over the course of the follow-up period.
The external validity of the present findings is limited due to the sample characteristics and problems with the studydesign. One serious limitation of the design was the lack of control group. The changes in inclusion attitudes and socialdistance found in the present study could be due to measurement effects. It has been suggested that ‘respondentsensitization’ occurs following the mere process of completing attitude questionnaires, and that this creates a small buttransient positive shift in attitudes, which could be erroneously attributed to the intervention (Antonak & Livneh, 1995;Triandis, 1971). Certainly the finding that behavioral intentions shifted in the short term, regardless whether they weredirectly related to the material presented, could be seen to support this notion. Future studies testing stigma changeinterventions would be well advised to include a control condition to account for the effect of measurement.
In terms of sample characteristics, participants were highly educated, young and reported a lot of previous contact withpeople with intellectual disabilities. Attempts were made to recruit from community colleges, which provide access to amore representative population (Corrigan et al., 2001). As noted, this proved time consuming and ultimately relativelyunproductive. In considering reasons for our difficulties in this regard, we note that Corrigan et al. (2001) recruited throughonly one community college, an approach which may allow researchers to establish closer relationships. However, it maylimit sample size – Corrigan et al.’s study had only 152 participants. Future researchers attempting to recruit a morerepresentative sample may need to consider engaging the services of opinion research companies, with obvious costimplications though.
The fact that data were collected through an electronic survey also merits consideration. In the UK 77% of people haveaccess to the Internet at home (Office for National Statistics, 2010), indicating that the Internet offers great potential forresearch. However, there is evidence that people who participate in Internet based research are younger and of higher socio-economic status than the population at large (Robinson et al., 2002). As such, although there are benefits to conductingonline research (Kraut et al., 2004), this study should be repeated with a more representative sample.
In line with other recent studies (Ouellette-Kuntz et al., 2010; Scior et al., 2010), participants in the present study reportedpositive baseline attitudes that were pro-inclusion and low on stigma. This is likely to reflect the sample but is problematic asit means that there were potential ceiling effects.
The CLAS-ID (Henry et al., 1996) alongside other attitude measures used in intellectual disabilities research, has beencriticized as it does not include all three elements of attitudes, namely affect, behavior and cognition (Werner et al., 2012).Yet there is correlation between CLAS-ID scores and measures of discriminatory behavior (Horner-Johnson et al., 2002).Nevertheless, other researchers suggest that implicit attitude measures may offer a useful alternative to explicit measures(Zsambok et al., 1999).
Previous research has examined emotional reactions towards the referent group (Angermeyer et al., 2010; Connolly et al.,in press), but not in relation to emotions evoked by anti-stigma interventions. The present study is the first to measureemotional reactions towards the intervention. The measure used did not create one overall score of emotional reactions, thusit was not possible to perform a mediator analysis, which would have increased the validity of the findings. In terms ofemotional reactions, this is a pilot study that begins to join up stigma change research and research in social psychologyabout the process of persuasion. Future research assessing stigma interventions should include all the psychologicalprocesses underlying persuasion (Petty & Brinol, 2008).
5. Conclusions & implications
This study has assessed the impact of two indirect contact interventions on inclusion attitudes, social distance andpositive behavioral intentions towards people with intellectual disabilities. While the findings partly support the use ofindirect contact to challenge stigma towards this population and suggest that protest approaches may be more effective infacilitating stigma change, their validity with a more representative general population sample needs to be tested in furtherresearch.
References
Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50, 179–211.Allport, G. W. (1954). The nature of prejudice. Cambridge MA: Addison Wesley.Angermeyer, M. C., Holzinger, A., & Matschinger, H. (2010). Emotional reactions towards people with mental illness. Epidemiologia e Psichiatria Sociale, 19, 26–32.Angermeyer, M. C., & Matschinger, H. (2003). The stigma of mental illness: Effects of labelling on public attitudes towards people with mental disorder. Acta
Psychiatrica Scandinavica, 108, 304–309.Antonak, R. F., & Livneh, H. (1995). Direct and indirect methods to measure attitudes toward persons with disabilities with an exegesis of the error-choice test
method. Rehabilitation Psychology, 4, 3–24.Armitage, C. J., & Conner, M. (2001). Efficacy of the theory of planned behaviour: A meta-analytic review. British Journal of Social Psychology, 40, 471–499.Brehm, J. W. (1996). A theory of psychological reactance. New York: Academic Press.Carsrud, A. L., Ahlgren, R. D., & Dood, B. G. (1986). Evaluating the effects of a community awareness programme on attitudes toward sheltered work and living
projects. British Journal of Mental Subnormality, 32, 12–41.Connolly, T., Williams, J., & Scior, K. The effects of symptom recognition and diagnostic labels on public beliefs, emotional reactions and stigma associated with
intellectual disability. American Journal of Intellectual and Developmental Disabilities, in press.

J. Walker, K. Scior / Research in Developmental Disabilities 34 (2013) 2200–22102210
Corrigan, P. W., Larson, J., Sells, M., Niessen, N., & Watson, A. C. (2007). Will filmed presentations of education and contact diminish mental illness stigma?Community Mental Health Journal, 43, 171–181.
Corrigan, P. W., & Penn, D. L. (1999). Lessons from social psychology on discrediting psychiatric stigma. American Psychologist, 54, 765–776.Corrigan, P. W., River, L. P., Lundin, R. K., Penn, D. L., Uphoff-Wasowski, K., Campion, J., et al. (2001). Three strategies for changing attributions about severe mental
illness. Schizophrenia Bulletin, 27, 187–195.Cummins, R. A., & Lau, A. L. D. (2003). Community integration or community exposure? A review and discussion in relation to people with an intellectual
disability. Journal of Applied Research in Intellectual Disabilities, 16, 145–157.Department of Health (2012). Time to change. Department of Health [On-line]. Available at www.time-to-change.org.uk.Equality and Human Rights Commission. (2011). Hidden in plain sight. Inquiry into disability related harassment. Manchester: Equality and Human Rights
Commission.Faigin, D. A., & Stein, C. H. (2008). Comparing the effects of live and video-taped theatrical performance in decreasing stigmatization of people with serious mental
illness. Journal of Mental Health, 17, 594–606.Fyson, R., & Kitson, D. (2010). Human rights and social wrong doings. Issues in safeguarding adults with learning disabilities. Practice: Social Work in Action, 22,
309–320.Hall, H., & Minnes, P. (1999). Attitudes toward persons with Down Syndrome: The impact of television. Journal of Developmental and Physical Disabilities, 11, 61–76.Henry, D., Keys, C., Jopp, D., & Balcazar, F. (1996). The community living attitudes scale mental retardation form: Development and psychometric properties.
Mental Retardation, 34, 149–158.Horner-Johnson, W., Keys, C., Henry, D., Yamaki, K., Oi, F., Watanabe, K., et al. (2002). Attitudes of Japanese students towards peole with intellectual disability.
Journal of Intellectual Disability Research, 46, 365–378.Joffe, H. (2008). The power of visual material: Persuasion, emotion and identification. Diogenes, 55, 84-+.Kraut, R., Olson, J., Banaji, M., Bruckman, A., Cohen, J., & couper, M. (2004). Psychological research online. American Psychologist, 59, 105–117.Link, B. G., Phelan, J. C., Bresnahan, M., Stueve, A., & Pescosolido, B. A. (1999). Public conceptions of mental illness: Labels, causes, dangerousness and social
distance. American Journal of Public Health, 89, 1328–1333.Link, B. G., Struening, E. L., Rahav, M., Phelan, J. C., & Nuttbrock, L. (1997). On stigma and its consequences: Evidence from a longitudinal study of men with dual
diagnoses of mental illness and substance abuse. Journal of Health and Social Behavior, 38, 177–190.Macrae, C. N., Bodenhausen, G. V., Milne, A. B., & Jetten, J. (1994). Out of mind but back in sight—Stereotypes on the rebound. Journal of Personality and Social
Psychology, 67, 808–817.McConkey, R., Walsh, P. N., & Conneally, S. (1993). Neighbours’ reactions to community services: Contrasts before and after services open in their locality. Mental
Handicap Research, 6, 131–141.Office for National Statistics (2010). Internet access 2010: Households and individuals. http://www.ons.gov.uk/ons/guide-method/census/2011/census-data/
index.html [On-line]. Available at http://www.ons.gov.uk/ons/guide-method/census/2011/census-data/index.html.Ouellette-Kuntz, H., Burge, P., Brown, H. K., & Arsenault, E. (2010). Public attitudes towards individuals with intellectual disabilities as measured by the concept of
social distance. Journal of Applied Research in Intellectual Disabilities, 23, 132–142.Penn, D. L., & Corrigan, P. W. (2002). The effects of stereotype suppression on psychiatric stigma. Schizophrenia Research, 55, 269–276.Pettigrew, T. F. (1998). Intergroup contact theory. Annual Review of Psychology, 49, 65–85.Pettigrew, T. F., & Tropp, L. R. (2006). A meta-analytic test of intergroup contact theory. Journal of Personality and Social Psychology, 90, 751–783.Petty, R. E., & Brinol, P. (2008). Psychological processes underlying persuasion—A social psychological approach. Diogenes, 55, 52-+.Phelan, J. C., Link, B. G., & Dovidio, J. F. (2008). Stigma and prejudice: One animal or two? Social Science & Medicine, 67, 358–367.Quarmby, K. (2008). Getting away with murder: Disabled people’s experiences of hate crime in the UK. London: Scope.Rillotta, F., & Nettelbeck, T. (2007). Effects of an awareness program on attitudes of students without an intellectual disability towards persons with an intellectual
disability. Journal of Intellectual and Developmental Disability, 32, 19–27.Robinson, J. P., Neustadtl, A., & Kestenbaum, M. (2002). Why public opinion polls are inherently biased: Public opinion differences between Internet users and
non-users, Paper presented at the annual meeting of the American Association for Public Opinion Research, St. Petersburg Beach, FL.Roper, P. (1990). Changing perceptions through contact. Disability Handicap & Society, 5, 243–255.Scior, K., & Furnham, A. (2011). Development and validation of the Intellectual Disability Literacy Scale for assessment of knowledge beliefs and attitudes to
intellectual disability. Research in Developmental Disabilities, 32, 1530–1541.Scior, K., Kan, K. Y., McLoughlin, A., & Sheridan, J. (2010). Public attitudes toward people with intellectual disabilities: A cross-cultural study. Intellectual and
Developmental Disabilities, 48, 278–289.Sheikh, S., Pralat, R., Reed, C., & Sin, C. H. (2010). Hate Crime Report for Mencap Don’t Stand By Campaign Mencap.Sin, C. H., Hedges, A., Cook, C., Mguni, N., & Comber, N. (2009). Disabled people’s experiences of targeted violence and hostility. Research report 21 (Rep. No. 21).
Manchester: Equality and Human Rights Commission.Smedema, S. M., Ebener, D., & Grist-Gordon, V. (2012). The impact of humorous media on attitudes toward persons with disabilities. Disability and Rehabilitation.Stalker, K., & Lerpiniere, J. (2009). ‘It’s against our law never mind anyone else’s’: The Disability Discrimination Act 1995 and adults with learning disabilities.
Disability & Society, 24, 829–843.Stern, B. (1994). Authenticity and the textual persona: Postmodern paradoxes in advertsing narrative. International Journal of Research Marketing, 11, 387–400.Strahan, R., & Gerbasi, K. C. (1972). Short homogeneous versions of the Marlowe–Crowne Social Desirability Scale. Journal of Clinical Psychology, 28, 191–193.Taylor, S. M., & Dear, M. J. (1981). Scaling community attitudes towards the mentally ill. Schizophrenia Bulletin, 7, 225–240.Thornicroft, G., Rose, D., Kassam, A., & Sartorius, N. (2007). Stigma: Ignorance, prejudice or discrimination? British Journal of Psychiatry, 190, 192–193.Thornton, J. A., & Wahl, O. F. (1996). Impact of a newspaper article on attitudes toward mental illness. Journal of Community Psychology, 24, 17–25.Triandis, H. C. (1971). Attitude and attitude change. New York: John Wiley & Sons.Verdonschot, M. M. L., de Witte, L. P., Reichrath, E., Buntinx, W. H. E., & Curfs, L. M. G. (2009). Community participation of people with an intellectual disability: A
review of empirical findings. Journal of Intellectual Disability Research, 53, 303–318.Werner, S., Corrigan, P., Ditchman, N., & Sokol, K. (2012). Stigma and intellectual disability: A review of related measures and future directions. Research in
Developmental Disabilities, 33, 748–765.World Health Organisation. (2001). International classification of functioning, disability and health. Geneva: World Health Organisation.Zajonc, R. B. (2001). Mere exposure: A gateway to the subliminal. Current Directions in Psychological Science, 10, 224–228.Zsambok, J., Hammer, D., & Rojahn, J. (1999). Put your money where your mouth is: Direct and indirect measures of attitude towards community integration.
American Journal of Mental Retardation, 104, 88–92.