tachyarrhythmias in the icu - mc.vanderbilt.edu · ib lidocaine, mexilitine, phenytoin ... qrs)...
TRANSCRIPT

Tachyarrhythmias in the ICU
ACNP/PA Critical Care Boot CampVanderbilt University Medical Center
September 21, 2015
Ariel KappaRN, MSN, ACNP-BC

• “Acute Arrhythmias are the gremlins of the ICU because they pop up unexpectedly, create some havoc, and are often gone in a flash…”
-Paul Marino
(The ICU Book, 2007)

Objectives
• Review
– EKG characteristics
– Initial Considerations
– Pharmacology
• Interactive Case Studies
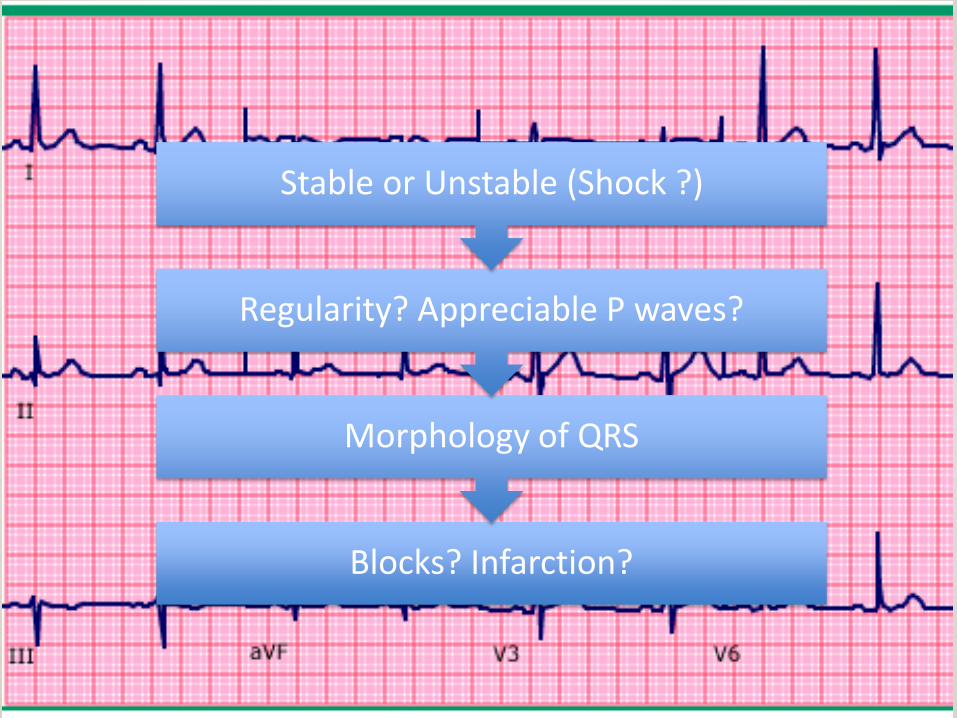
Blocks? Infarction?
Morphology of QRS
Regularity? Appreciable P waves?
Stable or Unstable (Shock ?)

Tachycardia
Regular
Narrow
Sinus Tachycardia,
Atrial Tachycardia,
AVNRT/AVRT, Atrial flutter
Wide
Monomorphic VT,
SVT with aberrancy/blo
ck/pacing-mediated
Irregular
Narrow
Atrial fibrillation,
MAT
Wide
Polymorphic VT/VF/
Torsades, Irregular SVT
with aberrancy/blo
ck

Initial considerations
• Stable?
– Hypotension, AMS, signs of shock, CP
– 12-lead EKG
• Pharmacological management
• Non-Pharmacological management
– Synchronized cardioversion (50-200 J)
• Oxygen, airway, monitor, sedation

Pharmacology
Class Common Examples Mechanism Clinical Use
Ia QuinidineProcainamide
Na+ Channel blocker; Fast (effects QRS)
Pre-excited afib, Stable monomorphic VT
Ib Lidocaine, Mexilitine, Phenytoin
Na+ Channel blocker; No effect on conduction; may prolong APD
VT
Ic Fleicanide, Propafenone
Na+ Channel blocker; (no effect on QRS)
SVT, PVCs, WPW
II Metoprolol, Esmolol, Propranalol
Block beta-adrenergic receptors Afib rate control, Narrow Stable SVT
III Amiodarone*, Sotalol*, Ibitulide
K+ channel blocker SVT (Regular and Irregular)
IV Verapamil, Diltiazem Non-dihydropyridine Calciumchannel blocker, vasodilate, negative inotrope
Rate control SVT*Avoid in CHF/VT Pre-exited Afib
Misc. Digoxin, AdenosineMagnesium
Dig- parasympathetic AV, + InotropeAdenosine- AVMag- effect Na/K transport
Dig- SVT, Afib in HF,Adenosine- SVT, stable WCTMg- Polymorphic VT/Torsades

Case 1
• 73 yo female with history of HTN, Aortic Stenosis, DMII, COPD
• POD 1 s/p AVRt with EF of 60% c/o SOB.
• Vitals: HR: 162, SBP: 131/71, RR: 26

Case 1
• What does this EKG show?
• 1. Atrial tachycardia
• 2. AV nodal reentrant tachycardia
• 3. Atrial fibrillation
• 4. Atrial flutter

What is the best next step?
• 1. Prepare for synchronized cardioversion of atrial fibrillation.
• 2. Initiate IV amiodarone bolus and infusion.
• 3. Assess timing, electrolytes and consider IV diltiazem bolus and infusion.
• 4. Administer 5mg IV metoprolol.

Rate vs. Rhythm control
• AFFIRM TRIAL
• True or False:
• Rhythm control is more important than rate control
• 1. True
• 2. False
• RACE II
• True or False:
• HR less than 110 is non-inferior to HR less than 80 in morbidity/mortality outcomes
• 1. True
• 2. False
(AFFIRM, NEJM, 2002), (VanGelder et al., NEJM, 2010)

Atrial Fibrillation
EKG Characteristics: Irregularly Irregular.
Etiology: Numerous waves of depolarization spreading throughout the atria, leading to an absence of coordinated atrial contraction.
Treatment: Class II, Class IV, Class III, Digoxin: HF (inotropic support). Unstable: Low voltage DCCV
AFFIRM trial (NEJM, 2000): Rate control not rhythm control
Race II Trial: (NEJM, 2010): Lenient rate control
Case 2
• 68 yo male with COPD exacerbation admitted to MICU.
• HR: 151, SBP: 121/73, RR: 28

Case 2
• What does this EKG show?
• 1. Atrial tachycardia
• 2. Sinus tachycardia
• 3. Atrial fibrillation
• 4. Atrial flutter
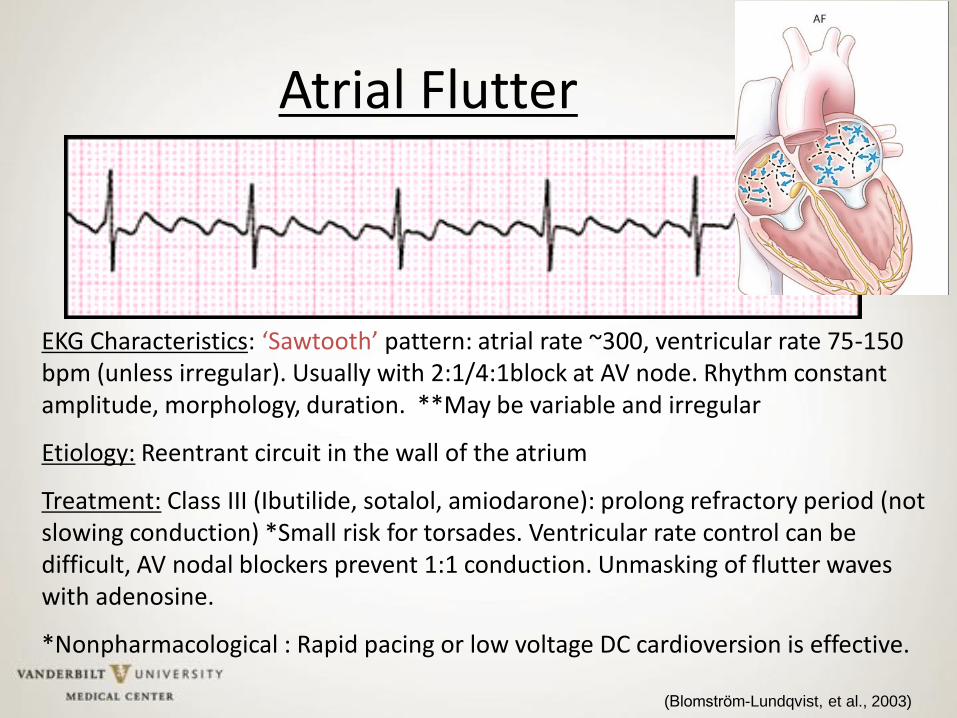
Atrial Flutter
EKG Characteristics: ‘Sawtooth’ pattern: atrial rate ~300, ventricular rate 75-150 bpm (unless irregular). Usually with 2:1/4:1block at AV node. Rhythm constant amplitude, morphology, duration. **May be variable and irregular
Etiology: Reentrant circuit in the wall of the atrium
Treatment: Class III (Ibutilide, sotalol, amiodarone): prolong refractory period (not slowing conduction) *Small risk for torsades. Ventricular rate control can be difficult, AV nodal blockers prevent 1:1 conduction. Unmasking of flutter waves with adenosine.
*Nonpharmacological : Rapid pacing or low voltage DC cardioversion is effective.
(Blomstrom-Lundqvist, et al., 2003)

Case 3
• 24 yo female admitted to Trauma ICU with pelvic fracture s/p MVC complaining of palpitations.
• Vitals: HR: 148, SBP 118/58, RR: 22
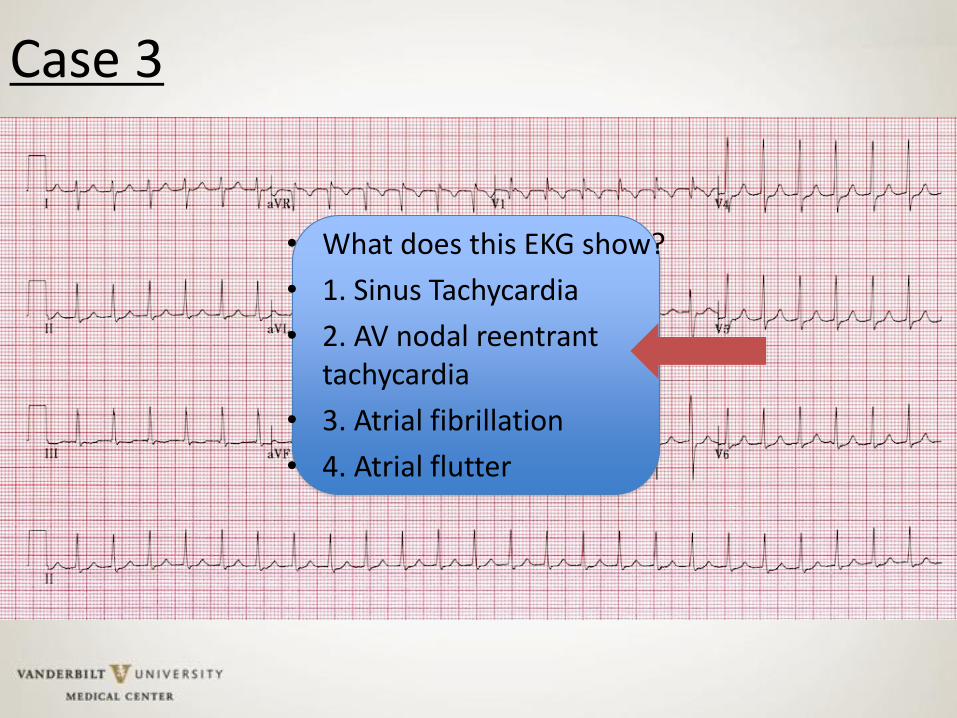
Case 3
• What does this EKG show?
• 1. Sinus Tachycardia
• 2. AV nodal reentrant tachycardia
• 3. Atrial fibrillation
• 4. Atrial flutter

AV Nodal Reentrant Tachycardia (AVNRT)
• EKG characteristics: Rate 140-280, P wave undetected (activation atria/ventricle simultaneously),
• Etiology: Triggered by PACs, “Micro” Reentry at AV node (atrial stretch, inflammation, irritability- catecholamines)
• Treatment: Vagal maneuvers, Adenosine 6-12 mg IV push,
Ca++ channel blockers, Digoxin, Beta blockers
(Blomstrom-Lundqvist, et al., 2003)

Multifocal Atrial Tachycardia (MAT)
• EKG characteristics: at least 3 P wave morphologies, variable intervals P-P, R-R, P-R, look for isoelectric baseline
• Etiology: No single dominant pacemaker, multiple atrial foci fire independently. COPD/CHF
• Treatment: Treat underlying cause (electrolyte derangement, hypoxemia). Rate control- Class IV- CCBs, Class II- Beta-blockers
ST • PACs

Atrioventricular Reentrant Tachycardia (AVRT)
• Etiology: Macrorentry through normal conduction system with accessory AV pathway; Delayed activation of atria = visible P wave
• Treatment: Similar to treatment of AVNRT, AV nodal blockers, eventual ablation

Sinus Tachycardia Atrial Tachycardia
EKG characteristics:
Constant PR interval
Varies with stimulation/respiration
Normal Rate 220 bpm –age (yrs)
Etiology: Physiologic
Treatment: Fix underlying
physiologic insult
(Fever, anxiety, thyrotoxicosis,
exogenous catecholamines,
anticholinergic, LV dysfunction- MI
etc.
EKG characteristics:
Atrial rate 150-250
Distinct P wave morphology
Etiology: CHF, HTN,
electrolyte abnormalities
Treatment: Adenosine, Class
II, Class III, *Dig toxicity?
Case 4
• 38 yo male with PMH: Appendectomy
• Presented to ED with SBO s/t incarcerated groin hernia now POD 3 s/p SBO repair.
• Vitals: HR 148, SBP 100/58, RR: 20
• BMP:
148 19 41
2.1 21 1.6

Case 4

What is your next course of action?
• 1. Correct hypokalemia and prepare amiodarone for administration.
• 2. Grab the crash cart and prepare for emergent cardioversion.
• 3. Correct hypokalemia and prepare lidocaine for bolus/infusion.
• 4. Grab the crash cart and ask the nurse to give sotalol.

Monomorphic VT
EKG characteristics: 3 consecutive beats >100 bpm, QRS >120ms
Brugada criteria: Precordial leads- No RS complex or RS >100ms, AV dissociation, QRS morphology- Fusion beats
Etiology: CAD, CM, Ischemia
Treatment: Correct aggravating conditions (hypokalemia, ischemia)
Class I: Wide QRS presumed VT if unclear ( LOE: C). *DCCV unstable ( LOE: C). Class II: Procainamide- careful in LV dysfunction, CHF, hypotension-prolong QT. Class III- Sotalol, Amiodarone (benefit IV to PO). Class IIb- IV lidocaine initial treatment associated with MI (LOE: C).
(Zipes et al., 2006)

Wide Complex SVT
•EKG characteristics: Regular, Wide complex, Fails Brugada’s Criteria (from previous slide)
•Etiology: BBB/IVCD, Pre-excitation, Presence of PPM/ICD
•Treatment: WPW- Procainamide (*Avoid AV nodal blockers)
•Vagal maneuvers, Adenosine, Class III, Cardioversion
Delta wave
WPW Pacemaker-Mediated

Which of these below is not a treatment option?
• 1. DC Cardioversion
• 2. Metoprolol
• 3. Amiodarone
• 4. Procainamide

Case 5
• Lets go back to the 38 yo. male with VT
• Unfortunately you look up at the monitor and see this…

Case 5
1. Give magnesium
2. Defibrillate
3. Stop all QT prolonging
medications
4. All of the above.
What do you do next?

Irregular, Wide Complex
• Polymorphic VT– Etiology: Ischemia, Catecholamines
– Treatment: Defibrillation
• Ventricular fibrillation, Torsades de pointes– Etiology- QT prolongation, Class I, III- prolong refractory period

General Tips
• Narrow complex tachyarrhythmias can be diagnosed or possibly terminated in most cases with IV adenosine.
• If the origin of arrhythmia is unclear on a symptomatic patient, it is generally consider safe to treat as ventricular in origin.
References• The Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) Investigators . A comparison of
rate control and rhythm control in patients with atrial fibrillation. New England Journal of Medicine. 2002, 347, 1825-1833.
• Carina Blomstrom-Lundqvist, Melvin M. Scheinman, Etienne M. Aliot, Joseph S. Alpert, Hugh Calkins, A. John Camm…Hans-Joachim Trappe. CC/AHA/ESC Guidelines for the Management of Patients With Supraventricular Arrhythmias−−Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Supraventricular Arrhythmias). Circulation, 2003, 108:1871-1909. doi: 10.1161/01.CIR.0000091380.04100.84.
• Delle Karth G, Geppert A, Neunteufl T , et al. Amiodarone versus diltiazem for rate control in critically ill patients with atrial tachyarrhythmias. Critical Care Medicine. 2001, 29, 1149-1153.
• Douglas P. Zipes, A. John Camm, Martin Borggrefe, Alfred E. Buxton, Bernard Chaitman, Martin Fromer…Cynthia Tracy. CC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart
Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): Developed in Collaboration With the European Heart Rhythm Association and the Heart Rhythm Society. Circulation, 2006, 114, e385-e484. doi: 10.1161/CIRCULATIONAHA.106.178233.
• Dubin, Dale. (2000). Rapid Interpretation of EKGs: Dr. Dubin’s classic simplified methodology for understanding EKGs, 6th Ed. Location. C.o.v.e.r.

• ECC Guidelines. Part 6: Advanced Cardiovascular Life Support: Section 5: Pharmacology I: Agents for Arrhythmias. Circulation. 2000, 102, I-112-I-128. doi: 10.1161/01.CIR.102.suppl_1.I-112.
• Fuster V, Ryden LE, Cannom DS, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/ American Heart Association Task Force on Practice Guidelines. Circulation. 2011, 123, e269-e367.
• Goodman S, Shiov T, Weissman C. Supraventricular arrhythmias in intensive care unit patients: short and long-term consequences. Anesth Analg. 2007, 104:880-886.
• January CT, Wann LS, Alpert JS, Calkins H, Cleveland JC, Cigarroa JE, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation. 2014, 129, 1-
56. DOI: 10.1161/CIR.0000000000000040.
• Marino, P.L. Tachyarrhythmias. The ICU Book. 2007, 343-361.
• Robert W. Neumar, Chair; Charles W. Otto; Mark S. Link; Steven L. Kronick; Michael Shuster; Clifton W. Callaway…Laurie J. Morrison. Part 8: Adult Advanced Cardiovascular Life Support 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010, 122, S729-S767. DOI: 10.1161/CIR.0b013e31820ff511.
• Trohman, G. Richard. Supraventricular tachycardia: Implications for the intensivist. Critical Care Medicine. 2000, 28, N129-N135.
• Van Gelder IC et al. Lenient versus strict rate control in patients with atrial fibrillation. The New England Journal of Medicine. 2010. 362 (15): 1363-73.