systemic biomarkers in exacerbations of copd: the evolving ... ex.pdf · of copd: the evolving...
TRANSCRIPT

DOI 10.1378/chest.11-0495; Prepublished online August 11, 2011;Chest
Angela Koutsokera, Daiana Stolz, Stelios Loukides and Konstantinos Kostikas CHALLENGEOF COPD: THE EVOLVING CLINICAL SYSTEMIC BIOMARKERS IN EXACERBATIONS
http://chestjournal.chestpubs.org/content/early/2011/08/10/chest.11-0495
can be found online on the World Wide Web at: The online version of this article, along with updated information and services
) ISSN:0012-3692http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(without the prior written permission of the copyright holder.reserved. No part of this article or PDF may be reproduced or distributedChest Physicians, 3300 Dundee Road, Northbrook, IL 60062. All rights
ofbeen published monthly since 1935. Copyright2011by the American College is the official journal of the American College of Chest Physicians. It hasChest
Department at (847) 498-1400 or [email protected]. appear online. For inquriires, please contact the AACP Media Relations
Papers in Press are not under media or public embargo once theCHEST (DOI) and date of in-press publication. references to an in-press article must include the digital object identifiernonsubstantive changes. These articles are indexed by PubMed, but any edited or typeset. The final version may contain substantive ornot yet been published in an issue of the journal and have not yet been
Papers in Press are peer-reviewed, accepted articles that haveCHEST
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from
1
Word Count: 3,666
Abstract Word Count: 248
SYSTEMIC BIOMARKERS IN EXACERBATIONS OF COPD: THE
EVOLVING CLINICAL CHALLENGE
Angela Koutsokera, MD1, [email protected]
Daiana Stolz, MD, FCCP2, [email protected]
Stelios Loukides, MD, FCCP3, [email protected]
Konstantinos Kostikas, MD, FCCP3, [email protected]
From the 1Service de Pneumologie et Rehabilitation Respiratoire, Hôpital de Rolle,
Switzerland; 2Clinic for Pulmonary Medicine and Respiratory Cell Research,
University Hospital Basel, Switzerland; 32
nd Respiratory Medicine Department,
University of Athens Medical School, Athens, Greece
Correspondence to:
Dr. Konstantinos Kostikas
Stamouli 3, Karditsa 43100, Greece
Tel + 30-6944780616, Fax +30-2441022370, e-mail [email protected]
Short Title: Systemic Biomarkers in COPD Exacerbations
Conflict of Interest: Dr. Stolz has received speakers’ honoraria from BRAHMS AG
(the manufacturer of pro-adrenomedullin, copeptin, pro-endothelin, and procalcitonin
assays) and was sponsored by BRAHMS AG for speaking engagements and research
(unrestricted grant). None of the other authors has any conflict of interest related to
the present manuscript.
Page 1 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

2
ABSTRACT
Word Count: 248
Background: Exacerbations of chronic obstructive pulmonary disease (ECOPD)
remain a major cause of mortality and morbidity of COPD patients. Despite advances
in the understanding of their pathophysiology, their assessment relies primarily on
clinical presentation which can be variable and difficult to predict. A large number of
biomarkers have already been assessed in this context and some appear to be
promising.
Methods: An online search for articles published until December 2010 was conducted
using 3 terms for ECOPD, 5 terms for biomarkers and 5 terms regarding the sampling
method. Biomarkers were evaluated for their potential role in the establishment and/or
confirmation of the diagnosis of ECOPD, the evaluation of etiology and severity, the
prediction of prognosis and the guidance of treatment decisions.
Results: Several systemic biomarkers have been measured in the context of ECOPD
and most of them have been found to increase at ECOPD onset and to subside during
the course of exacerbations. Correlations have been reported among these biomarkers
but direct associations with clinical variables have been more difficult to establish.
Although there are several limitations yet to be addressed, some of the biomarkers,
and most notably C-reactive protein for the identification of a COPD exacerbation and
procalcitonin for antibiotic guidance, may provide clinically relevant information.
Conclusions: So far no single biomarker has been able to gain wide acceptance, but
some provide clinically useful information. The evaluation of such biomarkers in
large decision-making studies is expected to become an area of intense investigation
in the near future.
Page 2 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

3
KEYWORDS
COPD
Exacerbation
Biomarkers
Antibiotics
Page 3 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from
4
ABBREVIATIONS
ATS/ERS: American Thoracic Society / European Respiratory Society
AUC: area under the curve
BNP: brain natriuretic peptide
COPD: chronic obstructive pulmonary disease
CRP: C-reactive protein
ECOPD: exacerbations of COPD
ECP: eosinophil cationic protein
HRV: human rhinovirus
ICU: intensive care unit
IL-6: interleukin 6
IP-10: IFN-γ induced protein 10
MMP-9: matrix metalloproteinase 9
MPIF-1: myeloid progenitor inhibitory factor-1
NIV: non invasive ventilation
PCT: procalcitonin
ProADM: pro-adrenomedullin
ProET1: proendothelin 1
SAA: serum amyloid A
sIL-5Rα: soluble interleukin 5 receptor α
sTNFR: soluble tumor necrosis factor receptor
sTREM-1: Soluble form of the triggering receptor expressed on myeloid cells
TEAC: Trolox equivalent antioxidant capacity
TNF-α: tumor necrosis factor α
Page 4 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

5
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) patients are susceptible to periodic
deteriorations of their illness that are mainly triggered by bacterial and viral
pathogens, called exacerbations of COPD (ECOPD). Frequent ECOPD accelerate
lung function decline and have major implications on the quality of life, morbidity
and mortality of COPD patients1. Currently ECOPD are diagnosed on clinical
grounds, when specific symptoms deteriorate beyond day-to-day variability, and their
severity is rated according to healthcare resource utilization1,2
. The identification of
ECOPD etiology often remains unclear and treatment decisions are usually empirical.
Biomarkers are biological molecules that can be used as indicators of normal
biologic processes, pathogenic processes or responses to therapeutic interventions.
While their use is not intended as a substitute for clinical judgment, biomarkers may
be valuable tools for describing the natural history of the disease as well as in helping
management, clinical decision making and predicting outcomes. Several systemic
biomarkers of inflammation and oxidative stress have been studied in ECOPD but
none has gained wide acceptance so far. The aim of this review is to provide an
overview of the systemic biomarkers studied in the context of ECOPD and to
highlight the most promising molecules, by dissecting their relative contribution to
clinical decision making and prediction of outcomes.
METHODOLOGY AND DEFINITIONS
A search for articles published in the English language until December 2010 was
conducted using Medline and Highwire databases as well as the reference lists of
reviews and retrieved articles. We combined 3 terms for ECOPD (COPD
exacerbation, COPD deterioration, acute COPD) with 5 terms related to biomarkers
Page 5 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

6
(biomarkers, acute phase proteins, cytokines, oxidative stress) and 5 terms regarding
the sampling method (serum, plasma, systemic, circulating levels, peripheral blood).
Abstracts or unpublished reports were not included in this review. Data obtained from
mixed populations (e.g. subjects with lower respiratory tract infection, patients with
respiratory failure or exacerbations of obstructive pulmonary disease in general) were
not included in the analysis. The methodology used was in accordance with the
suggestions of the MOOSE guidelines3. Figure 1 provides a flow chart diagram of
search strategy and study selection.
The current literature is characterized by an evident lack of consensus regarding
the definition of baseline, ECOPD onset and disease stability as well as by a vast
heterogeneity in study designs. The diversity of accumulating evidence renders result
interpretation difficult. In order to resolve the observed discrepancies of extracted
data, the following terminology was applied invariably in the current review:
• The term baseline describes a time point before the development of ECOPD,
i.e. during a phase of clinical stability, and this term has been used only for
longitudinal studies (paired samples).
• The term ECOPD onset has been used to describe the first time-point that the
patients suffering from an exacerbation were assessed by the investigators.
• The terms stability or recovery after an exacerbation were avoided and we have
used instead the specific time point of the measurement, e.g. Day 35 or Month
1.
• Finally, the term stable COPD was used only for cross-sectional studies that
compared ECOPD patients with another group of stable COPD patients (not
referring to paired samples).
Page 6 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

7
SYSTEMIC BIOMARKERS AND THE NATURAL HISTORY OF ECOPD
Several studies have measured numerous systemic biomarkers at ECOPD onset or
during recovery. Although not invariably demonstrated, most of the studied
inflammatory biomarkers increase at ECOPD onset and subside during the course of
exacerbations. This is especially true for C-reactive protein (CRP), the most widely
studied molecule in literature to-date, as well as for other acute phase proteins and
pro-inflammatory biomarkers. The presence of an anti-oxidant imbalance is also
considered to play an important role during the course of an ECOPD4-6
. These events
are associated with modifications of the levels of other metabolically active
molecules, such as copeptin7, leptin
8 or erythropoietin
9, as well as with modifications
of molecules expressed on circulating cells10,11
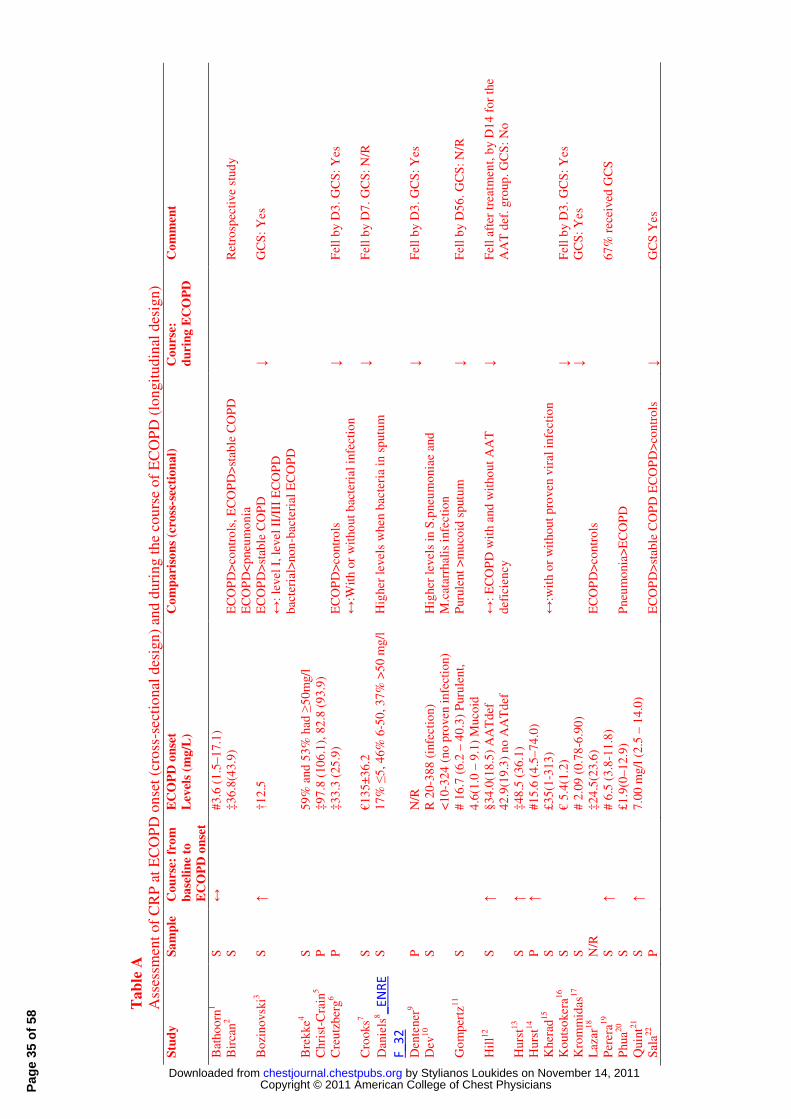
. The Tables A to D of the online
supplement provide a detailed overview of the biomarkers measured in ECOPD,
whereas Tables 1 and 2 specifically focus on the major finding concerning CRP and
procalcitonin (PCT). Although many of these biomarkers correlate with each other,
direct associations with clinically important variables have been more difficult to
establish (Table C of the online supplement).
The ultimate goal for clinicians is to draw clinically relevant conclusions from
research data in order to improve patient outcomes. This can be a very challenging
task as there is currently a large pool of candidate biomarkers studied in ECOPD. In
the following paragraphs we will focus on the clinical relevance of these biomarkers,
by discussing their potential role in the establishment and/or confirmation of the
diagnosis, the evaluation of etiology and severity, the prediction of prognosis and the
guidance of treatment decisions. Table 3 summarizes the biomarkers that have been
assessed in these directions.
Page 7 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from
8
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS OF ECOPD
Currently, and in the absence of specific biomarkers, ECOPD are diagnosed on
clinical grounds2. Biomarkers contributing to a prompt diagnosis of an imminent or
established ECOPD may modify treatment decisions and patient outcomes. In the
largest study to-date, Hurst et al. investigated the ability of 36 biomarkers to identify
ECOPD, and suggested that the three best performing molecules were CRP,
interleukin 6 (IL-6) and myeloid progenitor inhibitory factor-1 (MPIF-1)12
. The most
selective biomarker was CRP, presenting a moderate diagnostic performance with an
area under the curve (AUC) of 0.73, that provided 40% sensitivity and a 90%
specificity for a cut-off point of 27.6 mg/l12
. None of those biomarkers in isolation
could provide a better diagnostic performance compared to the presence of any major
ECOPD symptoms (dyspnea, sputum volume, or sputum purulence). The best
combination of three biomarkers [CRP, matrix metalloproteinase 9 (MMP-9), and
MPIF-1] resulted in an AUC which was not significantly better than CRP alone12
, but
the addition of CRP to any major symptom significantly increased the AUC to 0.88.
Several other studies have supported a possible role for CRP in the identification of an
ECOPD, however with modest diagnostic accuracy.
Data on the use of biomarkers for the differential diagnosis of ECOPD are
limited. In patients with mild exacerbation of bronchospastic symptoms, the values of
IL-1ra, IL-4 and IL-6 were lower in asthma than in ECOPD13
. In another study
involving 150 patients with acute respiratory infections, patients with pneumonia
presented the highest levels of the soluble form of the triggering receptor expressed on
myeloid cells-1 (sTREM-1), followed by ECOPD, asthma exacerbations and
controls14
. In a recent retrospective study of 319 patients hospitalized for pneumonia,
asthma exacerbation or ECOPD, CRP values greater than 48mg/L providing a
Page 8 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

9
sensitivity of 91% and a specificity of 93% for identifying patients with pneumonia15
.
However, prospective studies are needed for the evaluation of these biomarkers in the
differential diagnosis of ECOPD from other conditions with similar clinical
presentation.
ETIOLOGY OF ECOPD
ECOPD can be precipitated by pollutants, bacterial and viral causes, but in the
majority of cases the exact cause is not recognized. The identification of biomarkers
that may help in the identification of ECOPD etiology has possible treatment
implications. CRP has been invariably associated with increased sputum purulence16-
19, but studies that provide a bacteriological analysis do not reach common
conclusions, as some investigators describe increased CRP levels in bacterial
ECOPD20,21
and others don’t22,23
. Bircan et al. reported that a CRP cut-off point of
more than 10mg/l has 84% sensitivity but with 38.4% specificity for detecting
bacterial infections24
. When analyzed as the percentage change from stable state to
ECOPD, CRP shows a significantly larger increase in bacterial exacerbations25
,
whereas a study showed that the odds of a bacterial ECOPD increases by 57% per 1-
unit increase in logeCRP22
. Interestingly, the predictive value of CRP to distinguish an
ECOPD due to a new bacterial strain improves when it is combined with sputum
tumor necrosis factor α (TNF-α) and sputum neutrophil elastase26
. In the same
context, IL-625
and serum amyloid A (SAA)22
levels have been found significantly
elevated in bacterial ECOPD, whereas glucose23
, insulin23
, leptin23
, brain natriuretic
peptide (BNP)27
, PCT21,28
, pro-adrenomedullin (ProADM)29
, proendothelin 1 (ProET-
1)29
and soluble tumor necrosis factor receptors R55 and R7523
(sTNF-R55,
Page 9 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

10
sTNF/R75) failed to differentiate between patients with positive and negative sputum
cultures for bacteria.
Viral ECOPD have been associated with increased eosinophil cationic protein
(ECP)30
, soluble interleukin 5 receptor α (sIL5Rα)30
, fibrinogen31
and interferon-γ
induced protein 10 (IP-10)32
. Fibrinogen levels were elevated in viral ECOPD31
,
whereas Quint et al. have shown that IP-10 was increased in human rhinovirus
(HRV)-positive ECOPD, presenting a significant correlation to viral load32
.
According to this study, a cut-off point of 260pg/ml of IP-10 in the presence of cold
symptoms would be 80% specific and 67% sensitive for a HRV ECOPD32
. On the
other hand, CRP32,33
and PCT28,33
could not discriminate virus-associated ECOPD
from others, whereas the role of IL-6 has not yet been elucidated. Seemungal et al.
showed that serum IL-6 were higher in viral than in non-viral ECOPD, with the
difference not reaching statistical significance31
. Although one study showed that
ECOPD with both rhinovirus and Haemophilus influenza are associated with higher
serum IL-6 than ECOPD without both pathogens34
, other studies have shown that IL-
6 is not associated with either the detection of respiratory syncytial virus31
or the viral
load in sputum32
.
EVALUATION OF ECOPD SEVERITY
Stratification of ECOPD severity is usually made with the use of the ATS/ERS
criteria, focusing on health care resource utilization1,2
or with Anthonisen’s criteria
which stratify patients according to the presence of symptoms and sputum
purulence35
. Both classifications are based on the subjective evaluation of clinical
presentation and biomarkers are needed for a more objective evaluation of severity.
Page 10 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

11
Patients with severe ECOPD requiring admission to the intensive care unit
(ICU) present higher levels of BNP27
, copeptin36
, ProADM29
and PCT36
on admission.
In the same context, peak levels of troponin have been associated with the need for
noninvasive ventilation37
. On the other hand, CRP36
and ProET-129
levels did not
differ between patients admitted to the ICU and those receiving ward care.
CRP levels were significantly higher in patients with Anthonisen’s type I
ECOPD36
and correlated with the clinical severity assessed by a clinical score26
.
However, no difference was found in CRP between ATS/ERS level I and II/III
ECOPD and this biomarker performed no better than dyspnea or Anthonisen's criteria
in predicting severe episodes36
. When using the ratio of ECOPD onset to stable state
value to predict severe episodes, a cutoff point of a twofold change of CRP was 80%
sensitive and 54% specific with a positive and a negative likelihood ratio of 1.73 and
0.37 respectively22
.
SAA, another acute phase protein, was significantly elevated in ERS/ATS
level II/III events versus level I ECOPD and a fourfold or greater increase above basal
levels was associated with a severe ECOPD. Specifically, at a cut-off of 12.5 mg/L,
SAA had a 87% sensitivity for severe ECOPD with a negative predictive value of
92%. In contrast to CRP, SAA was better than dyspnea or Anthonisen’s criteria in
predicting severe episodes, whereas the combination of CRP or SAA with a major
symptom did not improve the prediction of a severe ECOPD over SAA alone22
.
Regarding other biomarkers, sTREM-1 levels were higher in Anthonisen type
1 ECOPD14
, whereas PCT maximal levels (assessed with 3 samplings within the first
24 hours of admission) of more than 0.25µg/l were present in more critically ill
patients28
. In the case of PCT a cut-off of point of 12.5µg/l had 54% sensitivity and
79% negative predictive value for severe ECOPD22
. On the contrary, BNP27
,
Page 11 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

12
ProADM29
or ProET-129
could not discriminate ECOPD type according to
Anthonisen’s criteria, whereas the study of Hurst et al. found no statistically
significant role in the evaluation of ECOPD severity for its 36 investigated
biomarkers12
.
GUIDANCE OF ANTIBIOTIC USE
Only a subgroup of patients suffering from ECOPD benefit from a treatment with
antibiotics, and biomarkers that can aid in the identification of such subjects may help
in limiting antibiotic use and microbiological resistance. PCT has been studied the
most for its potential to define the need for antibiotic use in patients with ECOPD.
The study of Stolz et al. discouraged the use of antibiotics for procalcitonin levels
<0.1 µg/L and recommended their administration for levels >0.25 µg/L, whereas for
levels between 0.1-0.25 µg/L antibiotic use was based on clinical judgment38
. This
study showed that procalcitonin guidance offered a sustained advantage over standard
therapy in reducing antibiotic use for up to 6 months with a number-needed-to treat of
3, whereas clinical outcomes, including exacerbation rate and time to next
exacerbation, were not compromised38
. These results were in line with studies
focusing on populations with lower respiratory tract infections that assessed ECOPD
patients in subgroup analyses (even if procalcitonin cut-off points and
recommendations are not common between those studies)39,40
.
In contrast, the study of Daniels et al. suggested that PCT levels did not differ
in the presence or absence of bacteria and patients with low PCT levels did benefit
from antibiotics21
. In this study data were obtained from a randomized placebo
controlled trial on doxycycline in addition to systemic corticosteroids for ECOPD and
treatment success was defined as a complete resolution or reduction of the symptoms
Page 12 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

13
and signs in the absence of the occurrence of a new infection. The discrepancy of the
results was attributed to different study designs, especially as far as population
characteristics and studied outcomes were concerned. Moreover, in the study by Stolz
et al. patients were randomized to either management based on PCT values or
standard care, further supporting a possible role for PCT. It is also worth mentioning,
that in the study by Daniels et al. most patients with low PCT levels had a high CRP.
Although clinicians had knowledge of the CRP values and this might have influenced
treatment decisions, a gradually increasing treatment effect of doxycycline was
observed for increasing levels of CRP21
.
CLINICAL EVOLUTION OF ECOPD
(a) Duration of hospitalization
A positive correlation with the length of hospital stay has been described for
copeptin36
, ProADM29
, ProET129
, albumin41
, troponin37,42
, BNP27
levels and for
ECOPD associated with eosinopenia43
. Interestingly, copeptin levels less than
40pmol/l on admission were associated with a mean length of hospital stay of 9 days
as compared to 14 days in subjects with more than 40pmol/l36
. In the case of troponin,
patients with raised levels had longer hospitalizations42
, but only peak levels could
predict the length of hospitalization37
. A trend for a shorter duration of hospitalization
was also observed in patients with low procalcitonin levels, but this difference did not
reach statistical significance36
. In ICU patients, BNP27
and copeptin36
levels on
admission correlated with the length of ICU stay, whereas no significant correlations
were reported for PCT28,36
, ProADM29
, CRP36
or ProET-129
.
(b) Duration of symptomatic recovery and development of complications
Page 13 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

14
Only a few papers have focused on the subject and most studies investigated the
predictive role of CRP on the duration of symptomatic recovery. One study described
similar CRP levels on admission between the subgroup of patients who subsequently
reported persistent symptoms by Day 10 as compared to those who reported symptom
resolution6. In another study, patients who had not recovered from ECOPD by day 35
had persistently higher serum CRP levels during the recovery period44
. Several other
biomarkers such as fibrinogen6, TNF-α
6, SAA
6 and IL-6
6,44 were not related to
symptom recovery time.
Regarding the development of complications, data on CRP are contradictory,
as some investigators report no correlation with long term clinical failure36
, whereas
others have showed that overall complications are correlated with CRP levels on
admission and with peak CRP levels37
. In the area of investigation, copeptin appears
to be a promising biomarker, as its levels on admission were associated with long
term clinical failure, especially when they were combined with a history of ECOPD
hospitalization during the previous year36
. This was not demonstrated for PCT36
.
(c) ECOPD frequency and recurrence
Several biomarkers have been assessed as indicators of an impending ECOPD. Some
have been measured during clinical stability and have been associated with the
frequency of exacerbations or the incidence of hospitalization of COPD patients
(Table 4). However only a limited number of studies focused on biomarkers sampled
at or after the onset of an exacerbation on ECOPD and attempted to predict ECOPD
frequency or recurrence. Perera et al. showed a significantly different evolution of
serum IL-6 and CRP between frequent and infrequent exacerbators44
. More
specifically, a higher concentration of CRP 14 days after the onset of an exacerbation
Page 14 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from
15
was associated with a shorter time to the next ECOPD, whereas elevated CRP levels
at Day 14 were related to ECOPD recurrence within 50 days, independent of disease
severity, ECOPD frequency or treatment with oral steroids44
. On the other hand, PCT
had no predictive value on ECOPD recurrence28
and albumin levels did not differ in
patients readmitted with ECOPD41
.
(d) Prediction of mortality
ProADM has been shown to be independently associated with 2 year survival, as
higher admission levels were found in hospital non-survivors and in long-term non-
survivors29
. The best diagnostic cut-off value was 0.77 nmol/l with a sensitivity of
0.81 and a specificity of 0.53 to predict death at two years. Moreover, as compared to
patients with proADM levels <0.84 nmol/l, the odds ratio for mortality within 2 years
in patients presenting with proADM ≥0.84 nmol/l at hospital admission was 3.12
(95% confidence interval 1.35 to 7.58)29
.
ProET-1, copeptin and PCT have also been studied in this context. ProET-1
levels did not differ in those who survived and deceased during hospitalization but
higher admission levels were observed in long-term non-survivors29
. Copeptin tended
to be higher in non-survivors as far as in hospital mortality was concerned with an
area under the curve for survival at 0.75 (higher than CRP and similar to PCT). A cut-
off point of 53 pmol/l had a sensitivity of 58% and a specificity of 80% to predict
mortality until follow-up and this biomarker was found to be an independent predictor
of outcome7. PCT was also associated with 2 year mortality with a hazard ratio of
1.517(95% CI, 1.144-2.010)29
, whereas PCT levels at admission of more than
0.25µg/l were associated with ICU mortality28
.
Page 15 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

16
CRP7,29,36,45
and BNP27
failed to predict mortality, whereas data concerning the
prognostic value of troponin on hospital mortality are contradictory, with some
investigators describing no difference37,42
and others reporting elevated levels as a
strong predictor of in-hospital death46
. However, most of the studies conclude that
elevated troponin during ECOPD is associated with increased risk of death after
discharge45
.
Finally, a retrospective study, reported that eosinopenia was associated with
increased mortality independent of age, white blood count and blood pH. Although
prospective studies are lacking, this observation is rather interesting as it might be
associated with the airway eosinophilia observed in some cases of ECOPD43,47
.
PROMISING BIOMARKERS AND FUTURE CHALLENGES
The evolution of a candidate biomarker to a clinical assay should conceptually
involve the following steps: (1) demonstrated association with the diagnosis or
outcome of interest; (2) prospective validation in independent cohorts of patients
representative of the intended target populations; (3) documentation of significant
incremental information when added to existing clinical information; (4) assessment
of effects on patient management and outcomes; and (5) cost effectiveness. It is
noteworthy that in this long pathway of biomarker validation, statistical factors are
not the only parameter to consider, as availability, ease of interpretation and cost play
also a major role48,49
. Although, most of the candidate biomarkers or their
combinations have not gone beyond the first steps of this pathway current literature is
rapidly evolving. Despite of the several limitations that hamper wide application and
acceptance, clinically useful information can be extracted for the biomarkers that have
been studied the most. For example, CRP has a modest diagnostic performance in the
Page 16 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

17
identification of ECOPD (40% sensitivity and a 90% specificity for a cut-off point of
27.6 mg/l) which does not transcend the diagnostic performance of any major ECOPD
symptom but it has been demonstrated that the addition of CRP to any major
symptom increases significantly the diagnostic performance of the latter12
. Moreover,
when analyzed as the percentage change from stable state to ECOPD, CRP shows a
significantly larger increase in bacterial exacerbations22,25
and may predict severe
episodes, although it does not perform better than dyspnea or Anthonisen’s
criteria25,36
. PCT has also been associated with the severity stratification of ECOPD
and it has been shown that PCT-guided treatment leads to a reduction of antibiotic use
without compromising clinical outcomes38
. Finally, SAA could also be a promising
marker, as a fourfold increase above basal levels was associated with severe ECOPD
episodes, performing better than dyspnea or Anthonisen’s criteria in predicting
severity22
.
For the immediate future, the combination of multiple, complementary and
independent, biomarkers measured in the same or different samples holds great
promise and is apt to become an area of intense investigation. Moreover,
combinations of systemic and local biomarkers could provide useful information.
Additionally, genomics and more specifically proteomics, a method of studying the
entire protein complement of the genome, are in the frontier of medical research. This
technique has the potential to provide an insight in the various interactions among
different pathways, but in the absence of a thoughtful approach it runs the risk of
merely increasing complexity without significantly improving clinical
outcomes48,50,51
. Statistical methods, such as the decision curve analysis, are
increasingly implemented in this context in order to improve the clinical relevance of
the statistical analysis52
.
Page 17 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

18
CONCLUSIONS
In this review we summarized the majority of studies that evaluated candidate
systemic biomarkers for the diagnosis and classification of ECOPD, the facilitation of
management decisions and the prognosis of COPD patients on exacerbation. Despite
the promising results of many studies, the contradictory findings suggest that no
single biomarker is likely to accomplish all the above targets. Taking into
consideration the several limitations yet to be addressed, some of the biomarkers, and
most notably CRP for the identification of a COPD exacerbation and PCT for
antibiotic guidance, may provide clinically relevant information. Therefore, the way
ahead possibly leads through the validation of existing biomarkers in large clinical
trials, the combination of biomarkers with important clinical information in decision-
making studies and the evolution of novel disease-specific systemic biomarkers.
ACKNOWLEDGEMENTS
KK and SL were involved in the conception of the present review. AK, DS, and KK
prepared the manuscript. KK and SL were involved in revising the manuscript for
important intellectual content. All authors read and approved the final manuscript.
Page 18 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

19
REFERENCES
1. Celli BR, MacNee W. Standards for the diagnosis and treatment of patients
with COPD: a summary of the ATS/ERS position paper. Eur Respir J 2004;23:932-
46.
2. Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis,
management, and prevention of chronic obstructive pulmonary disease: GOLD
executive summary. Am J Respir Crit Care Med 2007;176:532-55.
3. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies
in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in
Epidemiology (MOOSE) group. Jama 2000;283:2008-12.
4. Rahman I, Skwarska E, MacNee W. Attenuation of oxidant/antioxidant
imbalance during treatment of exacerbations of chronic obstructive pulmonary
disease. Thorax 1997;52:565-8.
5. Rahman I, Morrison D, Donaldson K, MacNee W. Systemic oxidative stress in
asthma, COPD, and smokers. Am J Respir Crit Care Med 1996;154:1055-60.
6. Koutsokera A, Kiropoulos TS, Nikoulis DJ, et al. Clinical, functional and
biochemical changes during recovery from COPD exacerbations. Respir Med
2009;103:919-26.
7. Muller B, Morgenthaler N, Stolz D, et al. Circulating levels of copeptin, a
novel biomarker, in lower respiratory tract infections. Eur J Clin Invest 2007;37:145-
52.
8. Kythreotis P, Kokkini A, Avgeropoulou S, et al. Plasma leptin and insulin-like
growth factor I levels during acute exacerbations of chronic obstructive pulmonary
disease. BMC Pulm Med 2009;9:11.
Page 19 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from
20
9. Sala E, Balaguer C, Villena C, et al. Low Erythropoietin Plasma Levels during
Exacerbations of COPD. Respiration 2010;80:190-7.
10. Noguera A, Busquets X, Sauleda J, Villaverde JM, MacNee W, Agusti AG.
Expression of adhesion molecules and G proteins in circulating neutrophils in chronic
obstructive pulmonary disease. Am J Respir Crit Care Med 1998;158:1664-8.
11. Tkacova R, Kluchova Z, Joppa P, Petrasova D, Molcanyiova A. Systemic
inflammation and systemic oxidative stress in patients with acute exacerbations of
COPD. Respir Med 2007;101:1670-6.
12. Hurst JR, Donaldson GC, Perera WR, et al. Use of plasma biomarkers at
exacerbation of chronic obstructive pulmonary disease. Am J Respir Crit Care Med
2006;174:867-74.
13. Stankiewicz W, Dabrowski MP, Chcialowski A, Plusa T. Cellular and
cytokine immunoregulation in patients with chronic obstructive pulmonary disease
and bronchial asthma. Mediators Inflamm 2002;11:307-12.
14. Phua J, Koay ES, Zhang D, et al. Soluble triggering receptor expressed on
myeloid cells-1 in acute respiratory infections. Eur Respir J 2006;28:695-702.
15. Bafadhel M, Clark TW, Reid C, et al. Procalcitonin and C reactive protein in
hospitalised adult patients with community acquired pneumonia, exacerbation of
asthma and chronic obstructive pulmonary disease. Chest 2010 Oct 28. [Epub ahead
of print].
16. Gompertz S, O'Brien C, Bayley DL, Hill SL, Stockley RA. Changes in
bronchial inflammation during acute exacerbations of chronic bronchitis. Eur Respir J
2001;17:1112-9.
Page 20 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

21
17. Stockley RA, O'Brien C, Pye A, Hill SL. Relationship of sputum color to
nature and outpatient management of acute exacerbations of COPD. Chest
2000;117:1638-45.
18. Weis N, Almdal T. C-reactive protein--can it be used as a marker of infection
in patients with exacerbation of chronic obstructive pulmonary disease? Eur J Intern
Med 2006;17:88-91.
19. Brusse-Keizer MG, Grotenhuis AJ, Kerstjens HA, et al. Relation of sputum
colour to bacterial load in acute exacerbations of COPD. Respir Med 2009;103:601-6.
20. Dev D, Wallace E, Sankaran R, et al. Value of C-reactive protein
measurements in exacerbations of chronic obstructive pulmonary disease. Respir Med
1998;92:664-7.
21. Daniels JM, Schoorl M, Snijders D, et al. Procalcitonin vs C-reactive protein
as predictive markers of response to antibiotic therapy in acute exacerbations of
COPD. Chest 2010;138:1108-15.
22. Bozinovski S, Hutchinson A, Thompson M, et al. Serum amyloid a is a
biomarker of acute exacerbations of chronic obstructive pulmonary disease. Am J
Respir Crit Care Med 2008;177:269-78.
23. Creutzberg EC, Wouters EF, Vanderhoven-Augustin IM, Dentener MA,
Schols AM. Disturbances in leptin metabolism are related to energy imbalance during
acute exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care
Med 2000;162:1239-45.
24. Bircan A, Gokirmak M, Kilic O, Ozturk O, Akkaya A. C-reactive protein
levels in patients with chronic obstructive pulmonary disease: role of infection. Med
Princ Pract 2008;17:202-8.
Page 21 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

22
25. Bathoorn E, Liesker JJ, Postma DS, et al. Change in inflammation in out-
patient COPD patients from stable phase to a subsequent exacerbation. Int J Chron
Obstruct Pulmon Dis 2009;4:101-9.
26. Sethi S, Wrona C, Eschberger K, Lobbins P, Cai X, Murphy TF. Inflammatory
profile of new bacterial strain exacerbations of chronic obstructive pulmonary disease.
Am J Respir Crit Care Med 2008;177:491-7.
27. Stolz D, Breidthardt T, Christ-Crain M, et al. Use of B-Type Natriuretic
Peptide in the Risk Stratification of Acute Exacerbations of COPD. Chest
2008;133:1088-94.
28. Daubin C, Parienti JJ, Vabret A, et al. Procalcitonin levels in acute
exacerbation of COPD admitted in ICU: a prospective cohort study. BMC Infect Dis
2008;8:145.
29. Stolz D, Christ-Crain M, Morgenthaler NG, et al. Plasma pro-adrenomedullin
but not plasma pro-endothelin predicts survival in exacerbations of COPD. Chest
2008;134:263-72.
30. Rohde G, Gevaert P, Holtappels G, et al. Soluble interleukin-5 receptor alpha
is increased in acute exacerbation of chronic obstructive pulmonary disease. Int Arch
Allergy Immunol 2004;135:54-61.
31. Seemungal T, Harper-Owen R, Bhowmik A, et al. Respiratory viruses,
symptoms, and inflammatory markers in acute exacerbations and stable chronic
obstructive pulmonary disease. Am J Respir Crit Care Med 2001;164:1618-23.
32. Quint JK, Donaldson GC, Goldring JJ, Baghai-Ravary R, Hurst JR, Wedzicha
JA. Serum IP-10 as a biomarker of human rhinovirus infection at exacerbation of
COPD. Chest 2010;137:812-22.
Page 22 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from
23
33. Kherad O, Kaiser L, Bridevaux PO, et al. Upper viral respiratory infection,
biomarkers and chronic obstructive pulmonary disease (COPD) exacerbations. Chest
2010;138:896-904.
34. Wilkinson TM, Hurst JR, Perera WR, Wilks M, Donaldson GC, Wedzicha JA.
Effect of interactions between lower airway bacterial and rhinoviral infection in
exacerbations of COPD. Chest 2006;129:317-24.
35. Anthonisen NR, Manfreda J, Warren CP, Hershfield ES, Harding GK, Nelson
NA. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease.
Ann Intern Med 1987;106:196-204.
36. Stolz D, Christ-Crain M, Morgenthaler NG, et al. Copeptin, C-reactive
protein, and procalcitonin as prognostic biomarkers in acute exacerbation of COPD.
Chest 2007;131:1058-67.
37. Martins CS, Rodrigues MJ, Miranda VP, Nunes JP. Prognostic value of
cardiac troponin I in patients with COPD acute exacerbation. Neth J Med
2009;67:341-9.
38. Stolz D, Christ-Crain M, Bingisser R, et al. Antibiotic treatment of
exacerbations of COPD: a randomized, controlled trial comparing procalcitonin-
guidance with standard therapy. Chest 2007;131:9-19.
39. Christ-Crain M, Jaccard-Stolz D, Bingisser R, et al. Effect of procalcitonin-
guided treatment on antibiotic use and outcome in lower respiratory tract infections:
cluster-randomised, single-blinded intervention trial. Lancet 2004;363:600-7.
40. Schuetz P, Christ-Crain M, Thomann R, et al. Effect of procalcitonin-based
guidelines vs standard guidelines on antibiotic use in lower respiratory tract
infections: the ProHOSP randomized controlled trial. Jama 2009;302:1059-66.
Page 23 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

24
41. Giron R, Matesanz C, Garcia-Rio F, et al. Nutritional state during COPD
exacerbation: clinical and prognostic implications. Ann Nutr Metab 2009;54:52-8.
42. Harvey MG, Hancox RJ. Elevation of cardiac troponins in exacerbation of
chronic obstructive pulmonary disease. Emerg Med Australas 2004;16:212-5.
43. Holland M, Alkhalil M, Chandromouli S, Janjua A, Babores M. Eosinopenia
as a marker of mortality and length of stay in patients admitted with exacerbations of
chronic obstructive pulmonary disease. Respirology 2010;15:165-7.
44. Perera WR, Hurst JR, Wilkinson TM, et al. Inflammatory changes, recovery
and recurrence at COPD exacerbation. Eur Respir J 2007;29:527-34.
45. Brekke PH, Omland T, Holmedal SH, Smith P, Soyseth V. Troponin T
elevation and long-term mortality after chronic obstructive pulmonary disease
exacerbation. Eur Respir J 2008;31:563-70.
46. Baillard C, Boussarsar M, Fosse JP, et al. Cardiac troponin I in patients with
severe exacerbation of chronic obstructive pulmonary disease. Intensive Care Med
2003;29:584-9.
47. Saetta M, Di Stefano A, Maestrelli P, et al. Airway eosinophilia in chronic
bronchitis during exacerbations. Am J Respir Crit Care Med 1994;150:1646-52.
48. Allen LA. Use of multiple biomarkers in heart failure. Curr Cardiol Rep
2010;12:230-6.
49. Shariat SF, Lotan Y, Vickers A, et al. Statistical consideration for clinical
biomarker research in bladder cancer. Urol Oncol;28:389-400.
50. Bowler RP, Ellison MC, Reisdorph N. Proteomics in pulmonary medicine.
Chest 2006;130:567-74.
Page 24 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

25
51. Hirsch J, Hansen KC, Burlingame AL, Matthay MA. Proteomics: current
techniques and potential applications to lung disease. Am J Physiol Lung Cell Mol
Physiol 2004;287:L1-23.
52. Vickers AJ, Cronin AM, Elkin EB, Gonen M. Extensions to decision curve
analysis, a novel method for evaluating diagnostic tests, prediction models and
molecular markers. BMC Med Inform Decis Mak 2008;8:53.
53. Crooks SW, Bayley DL, Hill SL, Stockley RA. Bronchial inflammation in
acute bacterial exacerbations of chronic bronchitis: the role of leukotriene B4. Eur
Respir J 2000;15:274-80.
54. Dentener MA, Creutzberg EC, Schols AM, et al. Systemic anti-inflammatory
mediators in COPD: increase in soluble interleukin 1 receptor II during treatment of
exacerbations. Thorax 2001;56:721-6.
55. Hill AT, Campbell EJ, Bayley DL, Hill SL, Stockley RA. Evidence for
excessive bronchial inflammation during an acute exacerbation of chronic obstructive
pulmonary disease in patients with alpha(1)-antitrypsin deficiency (PiZ). Am J Respir
Crit Care Med 1999;160:1968-75.
56. Hurst JR, Perera WR, Wilkinson TM, Donaldson GC, Wedzicha JA. Systemic
and upper and lower airway inflammation at exacerbation of chronic obstructive
pulmonary disease. Am J Respir Crit Care Med 2006;173:71-8.
57. Krommidas G, Kostikas K, Papatheodorou G, et al. Plasma leptin and
adiponectin in COPD exacerbations: Associations with inflammatory biomarkers.
Respir Med 2010;104:40-6.
58. Lazar Z, Huszar E, Kullmann T, et al. Adenosine triphosphate in exhaled
breath condensate of healthy subjects and patients with chronic obstructive pulmonary
disease. Inflamm Res 2008;57:367-73.
Page 25 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

26
59. Spruit MA, Gosselink R, Troosters T, et al. Muscle force during an acute
exacerbation in hospitalised patients with COPD and its relationship with CXCL8 and
IGF-I. Thorax 2003;58:752-6.
60. Shakoori TA, Sin DD, Ghafoor F, Bashir S, Bokhari SN. Serum surfactant
protein D during acute exacerbations of chronic obstructive pulmonary disease. Dis
Markers 2009;27:287-94.
61. Daniels JM, Schoorl M, Snijders D, et al. Procalcitonin versus C-reactive
protein as predictive markers of response to antibiotic therapy in acute exacerbations
of COPD. Chest.
62. Wedzicha JA, Seemungal TA, MacCallum PK, et al. Acute exacerbations of
chronic obstructive pulmonary disease are accompanied by elevations of plasma
fibrinogen and serum IL-6 levels. Thromb Haemost 2000;84:210-5.
63. Chakrabarti B, Angus RM, Agarwal S, Lane S, Calverley PM.
Hyperglycaemia as a predictor of outcome during non-invasive ventilation in
decompensated COPD. Thorax 2009;64:857-62.
64. Engstrom G, Segelstorm N, Ekberg-Aronsson M, Nilsson PM, Lindgarde F,
Lofdahl CG. Plasma markers of inflammation and incidence of hospitalisations for
COPD: results from a population-based cohort study. Thorax 2009;64:211-5.
65. Dahl M, Vestbo J, Lange P, Bojesen SE, Tybjaerg-Hansen A, Nordestgaard
BG. C-reactive protein as a predictor of prognosis in chronic obstructive pulmonary
disease. Am J Respir Crit Care Med 2007;175:250-5.
66. Gompertz S, Bayley DL, Hill SL, Stockley RA. Relationship between airway
inflammation and the frequency of exacerbations in patients with smoking related
COPD. Thorax 2001;56:36-41.
Page 26 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

27
67. Eagan TM, Ueland T, Wagner PD, et al. Systemic inflammatory markers in
COPD: results from the Bergen COPD Cohort Study. Eur Respir J;35:540-8.
68. Roland M, Bhowmik A, Sapsford RJ, et al. Sputum and plasma endothelin-1
levels in exacerbations of chronic obstructive pulmonary disease. Thorax 2001;56:30-
5.
69. Donaldson GC, Seemungal TA, Patel IS, et al. Airway and systemic
inflammation and decline in lung function in patients with COPD. Chest
2005;128:1995-2004.
70. Groenewegen KH, Postma DS, Hop WC, Wielders PL, Schlosser NJ, Wouters
EF. Increased systemic inflammation is a risk factor for COPD exacerbations. Chest
2008;133:350-7.
71. Eagan TM, Aukrust P, Bakke PS, et al. Systemic mannose-binding lectin is
not associated with Chronic Obstructive Pulmonary Disease. Respir Med;104:283-90.
72. Eagan TM, Damas JK, Ueland T, et al. Neutrophil Gelatinase Associated
Lipocalin - a biomarker in Chronic Obstructive Pulmonary Disease. Chest.
73. Lomas DA, Silverman EK, Edwards LD, et al. Serum surfactant protein D is
steroid sensitive and associated with exacerbations of COPD. Eur Respir J 2009.
Page 27 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

28
Table 1
Assessment of CRP at ECOPD onset (cross-sectional design) and during the course of
ECOPD (longitudinal design). An extended version of this Table is included in the
Online Supplement of this paper.
Reference Course: from
baseline to
ECOPD onset
Comparisons at ECOPD onset Course:
during
ECOPD
Bathoorn25
↔
Bircan24
ECOPD>controls, ECOPD>stable COPD,
ECOPD<pneumonia
Bozinovski22
↑ ECOPD>stable COPD ↓
↔: level I, level II/III ECOPD
bacterial>non-bacterial ECOPD
Brekke45
59% and 53% had ≥50mg/l
Creutzberg23
ECOPD>controls, ↔:With or without bacterial
infection
↓
Crooks53
↓
Daniels21
Higher levels when bacteria in sputum
Dentener54
↓
Dev20
Higher levels in S. pneumoniae and M. catarrhalis
infection
Gompertz16
Purulent >mucoid sputum ↓
Hill55
↑ ↔: ECOPD with and without α1-antitrypsindeficiency ↓
Hurst56
↑
Hurst12
↑
Kherad33
↔:with or without proven viral infection
Koutsokera6 ↓
Krommidas57
↓
Lazar58
ECOPD>controls
Perera44
↑
Phua14
Pneumonia>ECOPD
Quint32
↑
Sala9 ECOPD>stable COPD, ECOPD>controls ↓
Sethi26
↑ ↓
Spruit59
ECOPD>stable COPD, ECOPD>controls ↓
Stockley17
Purulent>mucoid sputum
Stolz36
Higher levels in type I ECOPD
Higher levels in mild to moderate COPD
↓
Tkacova11
ECOPD patients GOLD II<III<IV
Weis18
↔: ECOPD with increased sputum purulence,
pneumonia
Symbols: ↔: no difference, ↑: increase, ↓: decrease
Page 28 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

29
Tab
le 2
Ass
essm
ent
of
Pro
calc
itonin
at
EC
OP
D o
nse
t (c
ross
-sect
ional
des
ign)
and d
uri
ng t
he
cours
e of
EC
OP
D (
longit
udin
al d
esi
gn).
An e
xte
nded
ver
sion o
f th
is T
able
is
incl
uded
in t
he
Onli
ne
Supple
ment
of
this
pap
er.
Refe
ren
ce
Cou
rse
: fr
om
base
lin
e to
EC
OP
D o
nse
t
Co
mp
aris
on
s at
EC
OP
D o
nse
t C
ou
rse
: d
urin
g
EC
OP
D
Bozi
novsk
i22
↔
Chri
st-
Cra
in39
44.8
% h
ad>
0.1
µg/L
, 17.2
% h
ad >
0.2
5 µ
g/L
Dan
iels
21
↔
: P
rese
nce
or
abse
nce
of
sputu
m b
acte
ria
Dau
bin
28
↔
: E
CO
PD
bac
teri
olo
gic
ally
confi
rmed
or
not
Kher
ad3
3
↔
: E
CO
PD
ass
oci
ate
d o
r not
wit
h a
vir
us
Phua1
4
E
CO
PD
<pneum
onia
Sto
lz3
8
51%
had
<0.1
µg/L
, 29%
had
0.1
-0.2
5,
20%
had >
0.2
5
Sto
lz3
6
↔
: G
OL
D s
tages
↓
Sy
mb
ols
: ↔
: no d
iffe
rence
, ↓:
dec
reas
e
Pag
e 29
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

30
Tab
le 3
Stu
die
s in
vest
igat
ing t
he
pro
gnost
ic v
alue
of
syst
emic
bio
mar
ker
s fo
r cli
nic
al o
utc
om
es
Param
ete
r
Stu
die
d B
iom
ark
ers
Dia
gnosi
s C
RP
12,2
4,
IL-6
12,
MP
IF1
2,
SP
-D6
0 (
36 b
iom
arker
s as
sess
ed b
y H
urs
t et
al.
12*)
Eti
olo
gy
BN
P2
7,
CR
P16
-20,2
2-2
6,3
2,3
3,6
1,
EC
P3
0,
Fib
rinogen
31
,62,
Glu
cose
23,
IL-6
25
,31
,32
,34,
Insu
lin
23,
IP-1
03
2,
Lep
tin
23,
Pro
AD
M2
9,
Pro
ET
-12
9,
Pro
cal
cit
onin
21
,28
,29,
SA
A22,
s IL
5R
α3
0, sT
NF
-R55
23, sT
NF
-R75
23
Sev
erit
y
BN
P2
7,
Copep
tin
7,3
6, C
RP
22
,26,3
6,
Pro
AD
M2
9,
Pro
ET
-12
9,
PC
T 2
2,2
8,3
6,
SA
A2
2,
s T
RE
M-1
14 (
36
bio
mar
kers
ass
esse
d b
y H
urs
t et
al.
12*)
Guid
ance
of
anti
bio
tic
use
C
RP
21,
PC
T2
1,3
8-4
0,
s T
RE
M-1
14
Dura
tion o
f hosp
ital
izati
on
Alb
um
in41,
BN
P27,
Copep
tin
36,
CR
P36,
PC
T28
,36,
Pro
AD
M2
9,
Pro
ET
-12
9,
s T
RE
M-1
14, T
roponin
37,4
2
Dura
tion o
f re
covery
/Com
pli
cati
ons
Copepti
n36,
CR
P6,3
6,3
7,4
4, F
ibri
no
gen
6,
Glu
cose
63,
IL-6
6,4
4,
PC
T28
,36,
SA
A6,
s T
RE
M-1
14,
TN
Fα
6
EC
OP
D f
requen
cy/r
ecurr
ence
A
lbum
in41,
CR
P4
4,
IL-6
44,
PC
T28
Mort
alit
y/S
urv
ival
B
NP
27,
CR
P7,2
9,3
6,4
5,
PC
T2
8,2
9,
Pro
AD
M2
9,
Pro
ET
-12
9,
s T
RE
M-1
14,
Tro
ponin
37
,42,4
5,4
6
*N
ote
: th
e st
udy o
f H
urs
t et
al.
12 i
nves
tigat
ed t
he
role
of
36
pla
sma
bio
mar
ker
s (C
RP
, IL
6,
MP
IF-1
, P
AR
C, ad
iponec
tin
, sI
CA
M-1
, β
DN
F,
EN
A-7
8, E
ota
xin
-
2,
Erb
-B2,
fibro
nec
tin,
IFN
-γ, IL
-1β
, IL
-1R
a, I
L-8
, IL
-12p40,
IL-1
5,
IP-1
0,
ITA
C,
MC
P-1
, M
IP-1
β, M
MP
-9,
MP
O, P
rola
ctin
, R
AN
TE
S,
L-s
elec
tin,
TG
F-α
,
TIM
P-1
, T
NF
-α, T
NF
R1, T
NF
R2,
VE
GF
) in
the
confi
rmat
ion o
f E
CO
PD
dia
gnosi
s an
d i
n t
he
det
erm
inat
ion o
f it
s se
ver
ity. In
the
pre
sent
table
th
e bes
t per
form
ing m
ark
ers
of
this
stu
dy w
ere
incl
uded
.
Ab
bre
via
tion
s: B
NP
: bra
in n
atri
ure
tic
pep
tide,
βD
NF
: bra
in-d
eriv
ed n
euro
trophic
fac
tor,
CR
P:
C-r
eact
ive
pro
tein
, E
CP
: eo
sinop
hil
cat
ionic
pro
tein
, E
rb-B
2;
eryth
robla
stic
leu
kem
ia v
iral
onco
gen
e ho
molo
g 2
, IL
: in
terl
eukin
, IP
-10
: IF
N-γ
induce
d p
rote
in 1
0, IT
AC
: IF
N γ
indu
cible
T c
ell
α c
hem
oat
trac
tant,
MP
IF-1
:
Myel
oid
pro
gen
itor
inhib
ito
ry f
acto
r-1,
PA
RC
: pulm
onar
y a
nd a
ctiv
atio
n-r
egula
ted c
hem
ok
ine,
Pro
AD
M: p
ro-a
dre
nom
edull
in, P
roE
T1:
pro
endoth
elin
1,
PC
T:
pro
calc
itonin
, S
AA
: se
rum
am
ylo
id A
, sI
L-5
Rα
: so
luble
inte
rleu
kin
5 r
ecep
tor
α, sT
RE
M-1
: S
olu
ble
form
of
the
trig
ger
ing r
ecep
tor
expre
ssed
on
myel
oid
cel
ls, T
NF
α:
tum
or
nec
rosi
s fa
cto
r a,
TN
T:
tro
ponin
, V
EG
F:
vas
cula
r en
do
thel
ial
gro
wth
fac
tor
Pag
e 30
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

31
Tab
le 4
Syst
emic
bio
mar
ker
s m
easu
red d
uri
ng c
linic
ally
sta
ble
CO
PD
as
pre
dic
tors
of
EC
OP
D-r
ela
ted o
utc
om
es
Bio
mark
er
Ref
. E
nd
poin
t C
om
men
t
α1-a
nti
tryp
sin
P
64
CO
PD
hosp
ital
izat
ions
In
crea
sed l
evel
s w
ere
asso
ciat
ed w
ith
the
inci
den
ce o
f C
OP
D h
osp
ital
izat
ion
Ceru
lop
lasm
inP
64
CO
PD
hosp
ital
izat
ions
Incr
ease
d l
evel
s w
ere
asso
ciat
ed w
ith
the
inci
den
ce o
f C
OP
D h
osp
ital
izat
ion
CR
PS
65
CO
PD
hosp
ital
izat
ion, d
eath
In
crea
sed l
evel
s is
a s
tron
g l
ong-t
erm
pre
dic
tor
of
CO
PD
ho
spit
aliz
atio
n a
nd d
eath
6
6
EC
OP
D f
requ
ency
N
o d
iffe
ren
ce b
etw
een f
requen
t (≥
3/y
ear)
or
infr
equen
t (≤
2/y
ear)
exac
erbat
ors
CR
PP
67
EC
OP
D f
requ
ency
E
levat
ed i
n f
requen
t ex
acer
bat
ors
C
XC
L-1
6P
67
EC
OP
D f
requ
ency
N
o a
sso
ciat
ion
rep
ort
ed
ET
-1P
68
EC
OP
D f
requ
ency
N
o a
sso
ciat
ion
rep
ort
ed
Fib
rin
og
enP
69
EC
OP
D f
requ
ency
F
requ
ent
exac
erbat
ors
(≥
2.5
2/y
) had
a f
aste
r ri
se o
ver
tim
e in
pla
sma
fibri
nogen
6
4
CO
PD
hosp
ital
izat
ions
Incr
ease
d l
evel
s w
ere
asso
ciat
ed w
ith
the
inci
den
ce o
f C
OP
D h
osp
ital
izat
ion
7
0
EC
OP
D f
requ
ency
, se
ver
ity
Incr
ease
d l
evel
s w
ere
asso
ciat
ed w
ith
EC
OP
D f
requen
cy a
nd
the
dev
elo
pm
ent
of
sever
e E
CO
PD
Hap
tog
lob
inP
64
CO
PD
hosp
ital
izat
ions
Incr
ease
d l
evel
s as
soci
ated
wit
h i
nci
den
ce o
f C
OP
D h
osp
ital
izat
ion
IL
-6S
44
EC
OP
D r
ecu
rren
ce
No a
sso
ciat
ion
rep
ort
ed
LB
PP
70
EC
OP
D f
requ
ency
N
o r
elat
ion w
ith t
he
occ
urr
ence
of
sever
e or
moder
ate
EC
OP
D. N
o a
sso
ciat
ion
wit
h t
ime
to f
irst
EC
OP
D.
MB
LP
71
EC
OP
D f
requ
ency
N
o a
sso
ciat
ion
rep
ort
ed
MC
P 4
P
67
EC
OP
D f
requ
ency
N
o a
sso
ciat
ion
rep
ort
ed
NA
P 2
P
67
EC
OP
D f
requ
ency
N
o a
sso
ciat
ion
rep
ort
ed
NG
AL
P
72
EC
OP
D f
requ
ency
H
igher
lev
els
wer
e as
soci
ated
wit
h f
requ
ent
exac
erbat
ions
O
roso
mu
coid
P
64
CO
PD
hosp
ital
izat
ions
Incr
ease
d l
evel
s w
ere
asso
ciat
ed w
ith
the
inci
den
ce o
f C
OP
D h
osp
ital
izat
ion
Ost
eop
rote
gri
nP
67
EC
OP
D f
requ
ency
In
crea
sed l
evel
s w
ere
asso
ciat
ed w
ith
fre
qu
ent
EC
OP
D
SP
-DS
73
EC
OP
D f
requ
ency
In
crea
sed r
isk o
f E
CO
PD
wit
h v
alues
> 9
5th p
erce
nti
le (
for
non-s
moker
s)
sTN
F-R
1P
67
EC
OP
D f
requ
ency
In
crea
sed l
evel
s w
ere
asso
ciat
ed w
ith
fre
qu
ent
EC
OP
D
sTN
F-R
55
P
70
EC
OP
D f
requ
ency
N
o r
elat
ion w
ith t
he
occ
urr
ence
of
sever
e or
moder
ate
EC
OP
D. N
o a
sso
ciat
ion
wit
h t
ime
to f
irst
EC
OP
D.
sTN
F-R
75
P
70
EC
OP
D f
requ
ency
N
o r
elat
ion w
ith t
he
occ
urr
ence
of
sever
e or
moder
ate
EC
OP
D. N
o a
sso
ciat
ion
wit
h t
ime
to f
irst
EC
OP
D.
Ab
bre
via
tion
s: C
RP
: C
rea
ctiv
e p
rote
in, E
T-1
: E
ndoth
elin
-1,
LB
P:
lipopoly
sacc
har
ide
bin
din
g p
rote
in, M
BL
: m
anno
se b
indin
g l
ecti
n, M
CP
: M
onocy
te
chem
oat
trac
tant
pro
tein
, N
AP
: N
eutr
ophil
act
ivat
ing p
epti
de
NA
P,
NG
AL
: N
eutr
oph
il g
elat
inas
e as
soci
ated
lip
oca
lin
, S
P-D
: su
rfac
tant
pro
tein
D, s-
TN
F-R
:
solu
ble
rec
epto
r o
f tu
mor
nec
rosi
s fa
cto
r S
ym
bols
: S
: se
rum
, P
: pla
sma
Pag
e 31
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

254x190mm (96 x 96 DPI)
Page 32 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

ONLINE SUPPLEMENT
SYSTEMIC BIOMARKERS IN EXACERBATIONS OF COPD: THE
EVOLVING CLINICAL CHALLENGE
Angela Koutsokera, MD1, [email protected]
Daiana Stolz, MD, FCCP2, [email protected]
Stelios Loukides, MD, FCCP3, [email protected]
Konstantinos Kostikas, MD, FCCP3, [email protected]
From the 1Service de Pneumologie et Rehabilitation Respiratoire, Hôpital de Rolle,
Switzerland; 2Clinic for Pulmonary Medicine and Respiratory Cell Research,
University Hospital Basel, Switzerland; 32
nd Respiratory Medicine Department,
University of Athens Medical School, Athens, Greece
Correspondence to:
Dr. Konstantinos Kostikas
Stamouli 3, Karditsa 43100, Greece
Tel + 30-6944780616, Fax +30-2441022370, e-mail [email protected]
Short Title: Systemic Biomarkers in COPD Exacerbations
Conflict of Interest: Dr. Stolz has received speakers’ honoraria from BRAHMS AG
(the manufacturer of pro-adrenomedullin, copeptin, pro-endothelin, and procalcitonin
assays) and was sponsored by BRAHMS AG for speaking engagements and research
(unrestricted grant). None of the other authors has any conflict of interest related to
the present manuscript.
Page 33 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from
Ta
ble
A
Ass
essm
ent
of
CR
P a
t E
CO
PD
on
set
(cro
ss-s
ecti
on
al d
esig
n)
and
du
rin
g t
he
cou
rse
of
EC
OP
D (
longit
ud
inal
des
ign)
Stu
dy
S
am
ple
C
ou
rse:
fro
m
ba
seli
ne
to
EC
OP
D o
nse
t
EC
OP
D o
nse
t
Lev
els
(mg
/L)
Co
mp
ari
son
s (c
ross
-sec
tio
na
l)
Co
urs
e:
du
rin
g E
CO
PD
Co
mm
ent
Bat
ho
orn
1
S
↔
#3
.6 (
1.5
–1
7.1
)
Bir
can
2
S
‡
36
.8(4
3.9
) E
CO
PD
>co
ntr
ols
, E
CO
PD
>st
able
CO
PD
EC
OP
D<
pneu
mo
nia
R
etro
spec
tive
stud
y
Bo
zino
vsk
i3
S
↑
†1
2.5
E
CO
PD
>st
able
CO
PD
↓
GC
S:
Yes
↔:
level
I,
level
II/I
II E
CO
PD
bac
teri
al>
no
n-b
acte
rial
EC
OP
D
Bre
kke4
S
59
% a
nd
53
% h
ad ≥
50
mg/l
Chri
st-C
rain
5
P
‡
97
.8 (
10
6.1
), 8
2.8
(9
3.9
)
Cre
utz
ber
g6
P
‡
33
.3 (
25
.9)
EC
OP
D>
contr
ols
↓
Fel
l b
y D
3.
GC
S:
Yes
↔:W
ith o
r w
itho
ut
bac
teri
al i
nfe
cti
on
Cro
oks7
S
€1
35±
36
.2
↓
Fel
l b
y D
7.
GC
S:
N/R
Dan
iels
8_ENRE
F_32
S
1
7%
≤5
, 4
6%
6-5
0, 3
7%
>5
0 m
g/l
H
igher
lev
els
when b
acte
ria
in s
putu
m
Den
tener
9
P
N
/R
↓
Fel
l b
y D
3.
GC
S:
Yes
Dev
10
S
R
20
-38
8 (
infe
ctio
n)
<1
0-3
24
(no
pro
ven
in
fect
ion)
Hig
her
lev
els
in S
.pneu
mo
nia
e an
d
M.c
atar
rhal
is i
nfe
cti
on
Go
mp
ertz
11
S
#
16
.7 (
6.2
– 4
0.3
) P
uru
lent,
4.6
(1.0
– 9
.1)
Muco
id
Puru
lent
>m
uco
id s
putu
m
↓
Fel
l b
y D
56
. G
CS
: N
/R
Hil
l12
S
↑
§3
4.0
(18.5
) A
AT
def
42
.9(1
9.3
) no
AA
Td
ef
↔:
EC
OP
D w
ith a
nd
wit
ho
ut
AA
T
def
icie
ncy
↓
Fel
l af
ter
trea
tmen
t, b
y D
14
fo
r th
e
AA
T d
ef.
gro
up
. G
CS
: N
o
Hurs
t13
S
↑
‡4
8.5
(36
.1)
Hurs
t14
P
↑
#1
5.6
(4
.5–
74
.0)
Kher
ad1
5
S
£3
5(1
-31
3)
↔:w
ith o
r w
itho
ut
pro
ven v
iral
infe
ctio
n
Ko
uts
oker
a16
S
€
5.4
(1.2
)
↓
Fel
l b
y D
3.
GC
S:
Yes
Kro
mm
idas1
7
S
#
2.0
9 (
0.7
8-6
.90
)
↓
GC
S:
Yes
Laz
ar1
8
N/R
‡2
4.5
(23.6
)
EC
OP
D>
contr
ols
Per
era1
9
S
↑
# 6
.5 (
3.8
-11
.8)
67
% r
ecei
ved
GC
S
Phua2
0
S
£1
.9(0
–12
.9)
Pneu
mo
nia
>E
CO
PD
Quin
t21
S
↑
7.0
0 m
g/l
(2
.5 –
14
.0)
Sal
a22
P
EC
OP
D>
stab
le C
OP
D E
CO
PD
>co
ntr
ols
↓
GC
S Y
es
Pag
e 35
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

Set
hi2
3
S
↑
¥2
.12 (
1.7
–2.6
5)
↓
GC
S N
/R
Sp
ruit
24
S
#
28
(1
1–
86
) E
CO
PD
>st
able
CO
PD
EC
OP
D>
contr
ols
↓
Fel
l b
y D
3.
GC
S Y
es
Sto
ckle
y2
5
S
#
4.9
(1.0
-10
.2)
muco
id
14
.5(6
.2-3
5.8
) p
uru
lent
Puru
lent>
mu
coid
sp
utu
m
Sto
lz2
6
N/R
#1
6 (
5–
53
), 2
2(7
–62
)
Sto
lz2
7
N/R
#1
7.1
(5
.2–
55
.9)
Sto
lz2
8
P
#
26
.5 (
7.4
-60
.1)
Hig
her
lev
els
in t
yp
e I
EC
OP
D
Hig
her
lev
els
in m
ild
to
mo
dera
te C
OP
D
↓
Fel
l b
y D
14
. G
CS
Yes
Tkac
ova2
9
S
£1
7.9
(0.1
-28
2.8
) E
CO
PD
pat
ients
GO
LD
II<
III<
IV
Wei
s30
S
4
6%
had
0-1
0m
g/L
↔
: E
CO
PD
wit
h i
ncr
ease
d s
putu
m
puru
lence
, p
neu
mo
nia
Ab
bre
via
tio
ns:
AA
T d
ef.:
A1
anti
tryp
sin d
efi
ciency,
GC
S:
syst
em
ic g
luco
cort
ico
ster
oid
s, P
: p
lasm
a, S
: se
rum
, N
/R:
no
t re
po
rted
Sy
mb
ols
:↔:
no
dif
fere
nce
, ↑:
incr
ease
, ↓:
dec
reas
e, #
Med
ian (
inte
rquar
tile
ran
ge)
, †
med
ian,
‡m
ean (
SD
), €
mea
n±
SE
M,
§ a
ver
age(
SE
), ¥
geo
metr
ic m
ean (
95
% C
I),
£
med
ian (
ran
ge)
Pag
e 36
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from
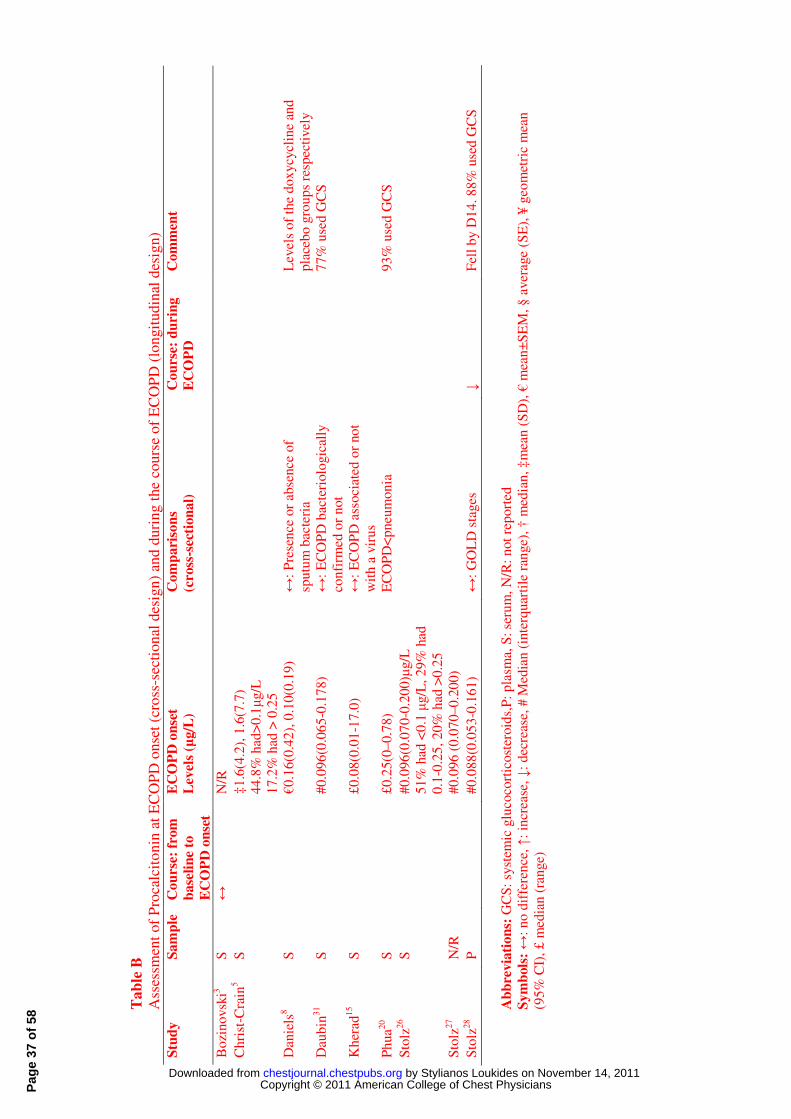
Ta
ble
B
Ass
essm
ent
of
Pro
calc
ito
nin
at
EC
OP
D o
nse
t (c
ross
-sec
tio
nal
des
ign
) an
d d
uri
ng t
he
cou
rse
of
EC
OP
D (
longit
udin
al d
esig
n)
Stu
dy
Sa
mp
le
Co
urs
e: f
rom
ba
seli
ne
to
EC
OP
D o
nse
t
EC
OP
D o
nse
t
Lev
els
(µg/L
) C
om
pa
riso
ns
(cro
ss-s
ecti
on
al)
C
ou
rse:
du
rin
g
EC
OP
D
Co
mm
ent
Bo
zin
ovsk
i3
S
↔
N/R
Ch
rist
-Cra
in5
S
‡
1.6
(4.2
), 1
.6(7
.7)
4
4.8
% h
ad>
0.1µ
g/L
1
7.2
% h
ad >
0.2
5
Dan
iels
8
S
€
0.1
6(0
.42
), 0
.10
(0.1
9)
↔:
Pre
sen
ce o
r ab
sence
of
spu
tum
bac
teri
a
Lev
els
of
the
do
xycy
clin
e an
d
pla
ceb
o g
rou
ps
resp
ecti
vel
y
Dau
bin
31
S
#
0.0
96
(0.0
65
-0.1
78
) ↔
: E
CO
PD
bac
teri
olo
gic
ally
con
firm
ed o
r n
ot
7
7%
use
d G
CS
Kh
erad
15
S
£
0.0
8(0
.01
-17
.0)
↔:
EC
OP
D a
sso
ciat
ed o
r no
t
wit
h a
vir
us
Ph
ua2
0
S
£
0.2
5(0
–0
.78)
EC
OP
D<
pn
eum
on
ia
9
3%
use
d G
CS
Sto
lz26
S
#
0.0
96
(0.0
70
-0.2
00
)µg/L
5
1%
had
<0
.1 µ
g/L
, 2
9%
had
0
.1-0
.25
, 2
0%
had
>0
.25
Sto
lz27
N/R
#0
.09
6 (
0.0
70
–0
.20
0)
S
tolz
28
P
#
0.0
88
(0.0
53
-0.1
61
) ↔
: G
OL
D s
tages
↓
Fel
l b
y D
14
. 8
8%
use
d G
CS
Ab
bre
via
tio
ns:
GC
S:
syst
emic
glu
coco
rtic
ost
eroid
s,P
: p
lasm
a, S
: se
rum
, N
/R:
not
rep
ort
ed
Sy
mb
ols
: ↔
: n
o d
iffe
ren
ce, ↑
: in
crea
se, ↓:
dec
reas
e, #
Med
ian
(in
terq
uar
tile
ran
ge)
, †
med
ian
, ‡
mea
n (
SD
), €
mea
n±
SE
M,
§ a
ver
age
(SE
), ¥
geo
met
ric
mea
n
(95
% C
I),
£ m
edia
n (
ran
ge)
Pag
e 37
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

Table C
Assessment of systemic biomarkers* at ECOPD onset (cross-sectional design)
Biomarker Ref. Comparisons at ECOPD onset
A1 antitrypsinS
12 ECOPD without deficiency>ECOPD with deficiency
BNPP
27 ↔:ECOPD with and without cardiomyopathy
27
↔: ECOPD with steady state PAH, without PAH
27
↔: ECOPD with positive or negative bacterial sputum cultures
CopeptinS
32 ECOPD>controls
CopeptinP
28 ↔: COPD stages
ECPS
33,34
ECOPD>controls (Controls
33: patients with pulmonary oedema,
pulmonary embolism, interventricular communication)
34
↔:ECOPD, healthy smokers
34
Higher levels when respiratory viruses were detected
33
ECOPD>stable COPD
ErythropoietinP
22 ECOPD<stable COPD
22
ECOPD<never smokers
22
ECOPD<smokers
E-selectinS
35 ECOPD>controls
FibrinogenP
36 Higher levels: purulent sputum, increased cough and presence of
a cold
GlucoseP
6 ECOPD>controls
6 ↔: ECOPD with and without bacterial infection
GM-CSFS
37 ECOPD>stable COPD
IgES
33 ECOPD>controls (Controls: patients with pulmonary oedema,
pulmonary embolism, interventricular communication)
IGF-IS
24 ↔: ECOPD, controls
IGF-IP
38 ECOPD<controls
38
ECOPD emphysema<chronic bronchitis
IL-1βS
38 ECOPD>controls
39
↔:ECOPD, asthma exacerbations
IL-1RaS
39 ECOPD>asthma exacerbations
IL-4S
39 ECOPD>asthma exacerbations
IL-6S
38,40 ECOPD>controls
24
↔: ECOPD, controls
19,36,38
ECOPD>stable COPD
24
↔:ECOPD, stable COPD
29
↔: ECOPD GOLD stages (Not specified at which time point
lung functions used for GOLD characterization were done)
39
↔:ECOPD, asthma exacerbations
41
ECOPD with both rhinovirus and H. influenzae> ECOPD
without both pathogens
IL-8S
24,35,38 ECOPD>controls
24
ECOPD>stable COPD
39
ECOPD>asthma exacerbations
IL-10S
24 ↔: ECOPD, stable COPD
InsulinS
6 ECOPD>controls
6
↔: ECOPD with and without bacterial infection
LeptinS
38,42 ECOPD>controls
38,42
ECOPD>stable COPD
LeptinP
6 ECOPD>controls
6 ↔: ECOPD with and without bacterial infection
LFA-1∞ adhesion molecule, PMN
43
ECOPD<Stable COPD, ECOPD<controls
Page 38 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

L-selectin∞ adhesion molecule, PMN
43
↔: ECOPD, stable COPD, controls
Mac-1∞ adhesion molecule, PMN
43
ECOPD<Stable COPD, ↔: ECOPD, controls
MPOS
33 ECOPD>controls (Controls: patients with pulmonary oedema,
embolism, interventricular communication)
33
ECOPD>stable COPD
33
↔: ECOPD smokers, ECOPD non smokers
Nitrite/nitrateS
40 ECOPD>controls
40
ECOPD>stable COPD
ProADMP
44 Elevated in 87.4% of ECOPD patients
44
No correlation with ECOPD stage
ProET-1P
44 Elevated in 87.4% of ECOPD patients
Protein thiolsP
45 ECOPD<controls
45
↔:ECOPD current<ex-smokers
SAA 3
ECOPD>stable COPD (Mean time from ECOPD onset to
obtaining serum 6.2 days)
3
ECOPD level II/III>level I
3
Bacteria-associated ECOPD>nonbacterial ECOPD
sICAMS
35 ECOPD>controls
sICAM-1P
43 ↔: ECOPD, stable COPD, ECOPD<controls
sIL-5RαS
34 ECOPD>controls
34
↔: ECOPD, healthy smokers
SP-DS
46 ECOPD> stable COPD> controls
sTNF R55P
6 ↔: ECOPD, controls
47
ECOPD>controls
6 ↔: patients with and without bacterial infection
sTNF R75P
6 ↔: ECOPD, controls
47
ECOPD>controls
6 ↔: patients with and without bacterial infection
TBA-MDA ad.P
45 ECOPD>controls
TEACP
45,48 ECOPD<controls
45
ECOPD smokers<ex-smokers
45
↔:ECOPD on or without GCS
TNFαS
38,40,42 ECOPD>controls
42
ECOPD>stable COPD
40
↔:ECOPD, stable COPD
24
Undetectable levels
39
↔:ECOPD, asthma exacerbations
TNFαP
47 ECOPD>controls (smokers, non smokers)
sTREM-1S
20 ECOPD>controls
20
ECOPD type I> type II/III
20
ECOPD type I>asthma exacerbations
20
↔: ECOPD type II+III, asthma exacerbations
20
ECOPD type II+III<pneumonia
20
↔: ECOPD type I, pneumonia
*CRP and PCT are discussed in Tables 1 and 2 respectively Abbreviations: BNP: B natriuretic peptide, ECP: Eosinophil cationic protein, GCS:
glucocorticosteroids, GSHPx: Glutathione peroxidase, GM-CSF: granulocyte macrophage
colony-stimulating factor, ICU: intensive care unit, IgE: immunoglobulin E, IGF-I: insulin-
like growth factor, IL: interleukin, IL-1Ra: interleukin 1 receptor antagonist, LFA-1:
lymphocyte function-associated antigen-1, Mac-1: MPO: myeloperoxidase, PAH: pulmonary
arterial hypertension, PMN: polymorphonuclear neutrophils, proADM: pro-adrenomedullin,
proET-1: proendothelin 1, Ref.: references, SAA: serum amyloid A, sICAM: soluble
intercellular adhesion molecule-, sIL-5Rα: soluble interleukin 5 receptor α, sTNF R: soluble
tumor necrosis factor receptor, TBA-MDA ad.: Thiobarbituric acid, malondialdehydeadducts,
Page 39 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

TEAC: Trolox equivalent antioxidant capacity, TNFα: tumor necrosis factor α, SP-D:
surfactant protein D, sTREM-1: Soluble form of the triggering receptor expressed on myeloid
cells. Symbols: ↔: no difference, P: plasma, S: serum, ∞: biomarkers of circulating cells
Page 40 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

Ta
ble
D
Ass
essm
ent
of
syst
emic
bio
mar
ker
s* f
rom
bas
elin
e to
war
ds
EC
OP
D o
nse
t an
d d
uri
ng E
CO
PD
(lo
ngit
udin
al d
esig
n)
Bio
mark
er
Ref
. C
ou
rse:
Ba
seli
ne-
On
set
Co
urs
e: d
uri
ng
EC
OP
D
Sy
stem
ic G
CS
du
rin
g E
CO
PD
Co
mm
ents
A1
-AC
PS
7
↓
N
/R
Fel
l b
y D
14
Ad
ipo
nec
tin
P
14
↑
17
↓
Y
es
Fel
l b
y t
reat
men
t co
mp
leti
on
an
d s
ym
pto
m r
eso
luti
on
A1
an
titr
yp
sin
S
12
P
eak:
D3
, fa
llin
g t
her
eaft
er
Yes
S
ubje
cts
wit
h A
1 a
nti
tryp
sin
def
icie
ncy
Am
ph
ireg
uli
nP
14
↔
A1
-PIS
7
↓
N
/R
Fel
l b
y D
14
BD
NF
P
14
↔
β-N
GF
P
14
↔
BN
PP
27
↓
N
/R
Fel
l b
y D
14
-18
Cat
alas
eP
49
↔
N
/R
Tim
e p
oin
ts:
D0
, per
iod
aft
er t
reat
men
t
Co
pep
tin
P
28
↓
8
8%
F
ell
by D
14
EC
PS
34
↔
U
sual
ly
Tim
e p
oin
ts:
D1
, ho
spit
al d
isch
arge
EN
A-7
8P
14
↔
Pag
e 41
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

Eo
taxin
-2P
14
↓
Ery
thro
poie
tin
P
22
Yes
C
han
ge
of
level
s b
y M
3 a
fter
dis
char
ge
Erb
-B2
P
14
↔
E s
elec
tin
S
35
↔
Y
es
Tim
e p
oin
ts:
D1
,3,7
ET
-1P
50
↑
Fib
rin
ogen
P
36,5
1
↑
16
↓
Y
es
Fel
l b
y D
40
Fib
ron
ecti
nP
14
↔
Glu
cose
P
6
↓
Y
es
Fel
l b
y D
7
GS
HP
xP
49
↓
N
/R
Fel
l af
ter
trea
tmen
t
GR
dP
49
↓
N
/R
Fel
l af
ter
trea
tmen
t
IFN
-γP
14
↔
IGF
-IS
24
↑
Y
es
Sig
nif
ican
t ↑
bet
wee
n D
8-D
90
, b
ut
12
of
34
pat
ien
ts d
rop
ped
out
IGF
-IP
38
↓
Y
es
Fel
l b
y D
15
IL-1β
S
38
↓
Y
es
Fel
l b
y D
15
IL-1β
P
14
↔
Pag
e 42
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

IL-1
RaP
14
↑
IL-2
RγP
14
↔
IL-6
S
1,3
,13,1
9,2
1
↑
41
↔
19
N
o c
om
par
iso
n w
ith D
0
67
%
D7
<b
asel
ine
(bef
ore
EC
OP
D),
D1
4=
Bas
elin
e, D
35=
Bas
elin
e
16,1
7,3
8,5
1
↓
Y
es16,1
7,3
8,Y
som
e51
16:
fell
by D
3
24,4
0
↔
Y
es
Tim
e p
oin
ts:2
4:
D3
,8,9
0,
40:
D0
,D1
4,W
6
IL-6
P
14
↑
52
↓
Y
es
Fel
l b
y D
2
IL-8
S
24
↔
Y
es
Tim
e p
oin
ts:
D3
,8,9
0 (
12
of
34
pat
ien
ts d
rop
ped
ou
t)
35,3
8
↓
Y
es
35:
fell
by D
7
IL-8
P
14
↔
52
↓
Y
es
Fel
l b
y D
2
IL-1
0S
24
↔
Y
es
Tim
e p
oin
ts:
D3
,8,9
0
IL-1
2p
40
P
14
↔
IL-1
5P
14
↔
Pag
e 43
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

IL-1
7P
14
↔
Insu
lin
S
6
↔
Y
es
Gra
du
al d
rop
by D
7,
bu
t n
o s
tati
stic
ally
sig
nif
ican
t
IP-1
0S
21
↑
IP-1
0P
14
↑
ITA
CP
14
↔
LB
PP
9
↓
Y
es
Fel
l b
y D
7
Lep
tin
S
38
↓
Y
es
Fel
l b
y D
15
Lep
tin
P
6
↓
Y
es
Dec
reas
ed g
radu
ally
th
rou
gh
ou
t E
CO
PD
17
↓
Y
es
Fel
l b
y t
reat
men
t co
mp
leti
on
an
d s
ym
pto
m r
eso
luti
on
L-s
elec
tin
P
14
↔
LT
B4
P
52
↓
Y
es
Rem
ain
ed s
tab
le u
nti
l D
2 a
nd
fel
l b
y 8
W
MC
P-1
P
14
↔
MD
AP
49
↑
N
/R
Incr
ease
d a
fter
tre
atm
ent
Mel
ato
nin
S
49
↑
N
/R
Incr
ease
d a
fter
tre
atm
ent
(wit
hin
10
day
s)
MIP
-1β
P
14
↔
MM
P-9
P
14
↔
Pag
e 44
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

MP
IF-1
P
14
↑
MP
OP
14
↔
Nit
rite
/nit
rate
S
40
↔
Y
es
Tim
e p
oin
ts:
D0
, D
14
, W
6
Ox
idat
ive
stre
ssS
16
↔
Y
es
Tim
e p
oin
ts:
D0
,3,1
0,4
0
PA
RC
P
14
↑
Pro
ET
1P
44
↓
Y
es s
om
e F
ell
by D
14
-18
Pro
lact
inP
14
↔
Pro
AD
MP
44
↓
Y
es s
om
e F
ell
by D
14
-18
RA
NT
ES
P
14
↔
SA
AS
3
↑
Mea
n t
ime
fro
m E
CO
PD
on
set
to s
eru
m s
amp
lin
g:
6.2
day
s
3,1
6
↓
Y
es
16F
ell
by D
10
sIC
AM
S
1
↔
35
↓
Y
es
Fel
l b
y D
7.
On
ad
mis
sio
n 6
pat
ients
wer
e al
read
y o
n o
ral
GC
S
sIC
AM
-1P
14
↑
sIL
1 R
IIP
9
↑
Y
es
Incr
ease
d b
y D
5 a
nd
rem
ain
ed s
table
bet
wee
n D
5-7
sIL
5 Rα
S
34
↓
Y
es u
sual
ly
Fel
l b
y h
osp
ital
dis
char
ge
Pag
e 45
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

SL
PIP
52
↔
Y
es
Tim
e p
oin
ts:
D0
, D
2, 8
W a
fter
dis
char
ge
SO
DP
49
↓
N
/R
Dec
reas
ed a
fter
tre
atm
ent
TB
A-M
DA
ad.P
45
↓
6
of
13
F
ell
wit
hin
12
h,
no
ch
ange
bet
wee
n 1
2h
an
d 4
8h
sTN
F R
55
P
6,9
in
itia
l↑, ↓
Y
es
Ris
e bet
wee
n D
1-3
, d
ecre
ase
ther
eaft
er b
ut
D1=
D7
47
↔
A
vo
ided
T
ime
po
ints
: ad
mis
sio
n, p
ost
tre
atm
ent
sTN
F R
75
P
47
↔
Y
es
Tim
e p
oin
ts:
6 :
D1
,3,5
,7,
47:a
dm
issi
on
, p
ost
tre
atm
ent
6
in
itia
l↑, ↓
Y
es
Sta
tist
ical
sig
nif
ican
ce n
ot
rep
ort
ed
9
in
itia
l↑, ↓
Y
es
Ris
e bet
wee
n D
1-3
, d
ecre
ase
ther
eaft
er b
ut
D1=
D7
TE
AC
P
45
↑
6
of
13
N
o c
han
ge
un
til
D2
, in
crea
sed
D5
-10
lat
er
TIM
P-1
P
14
↔
TG
F-α
P
14
↔
TN
Fα
S
1
↔
16
In
itia
l ↓
, tr
end
of ↑
ther
eaft
er
Yes
R
edu
ced
by D
3 a
nd
10
, n
o d
iffe
ren
ce b
etw
een
D0
an
d D
40
17,3
8
↓
Y
es
38R
edu
ced
by D
15
40
↔
Y
es
Tim
e p
oin
ts:
D0
,D1
4,W
6
Pag
e 46
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

TN
F-α
P
14
↔
52
↔
Y
es
Tim
e p
oin
ts:
D0
, D
2, 8
W a
fter
dis
char
ge
47
↓
A
vo
ided
F
ell
afte
r tr
eatm
ent
TN
FR
1P
14
↑
TN
FR
2P
14
↔
VE
GF
P
14
↔
*C
RP
an
d P
CT
are
dis
cuss
ed i
n T
ab
les
1 a
nd
2 r
esp
ecti
vel
y
Ab
bre
via
tio
ns:
A1
-AC
P:
A1
an
tich
ym
otr
yp
sin
, A
1-P
I: A
1 p
rote
ase
inh
ibit
or,
BD
NF
: B
rain
-der
ived
neu
rotr
op
hic
fac
tor,
β-N
GF
: N
erv
e gro
wth
fac
tor β
,
BN
P:
B n
atri
ure
tic
pep
tide,
D:
day
aft
er E
CO
PD
onse
t, E
CP
: E
osi
no
phil
cat
ionic
pro
tein
, E
NA
-78
: E
pit
hel
ial-
der
ived
neu
tro
phil
act
ivat
ing p
rote
in-7
8,
ET
-1:
end
oth
elin
1,
GC
S:
glu
coco
rtic
ost
ero
ids,
GS
HP
x:
Glu
tath
ion
e per
ox
idas
e, G
Rd:
Glu
tath
ion
e re
du
ctas
e, I
FN
- γ:
inte
rfer
on
γ,
IGF
-I:
Insu
lin
-lik
e gro
wth
fac
tor,
IL:
inte
rleu
kin
, IL
-2Rγ:
in
terl
eukin
2 r
ecep
tor γ,
IP
-10
: IF
Nγ
ind
uce
d p
rote
in 1
0,
ITA
C :
IF
Nγ
ind
uci
ble
T c
ell α
ch
emo
attr
acte
inas
e, L
BP
: li
po
poly
sacc
har
ide
bin
din
g p
rote
in,
LT
B4:
leuco
trie
ne
B4
, M
CP
-1 :
Mo
no
cyte
ch
emo
attr
acta
nt
pro
tein
1, M
DA
: m
alo
nd
iald
ehyd
e, M
IP-1β
: m
acro
ph
age
infl
amm
ato
ry p
rote
in-
1,
MM
P-9
: m
atri
x m
etal
lop
rote
inas
e 9
, M
PIF
-1 :
Myel
oid
pro
gen
itor
inh
ibit
ory
fac
tor-
1,
MP
O:
myel
op
erox
idas
e, ,
N/R
: no
t re
port
ed,
PA
RC
: P
ulm
on
ary a
nd
acti
vat
ion
-reg
ula
ted
ch
emo
kin
e, P
roA
DM
: p
road
ren
om
edu
lin
, R
AN
TE
S:
Reg
ula
ted
on
act
ivat
ion
norm
al T
-cel
l ex
pre
ssed
an
d s
ecre
ted
, R
ef.:
refe
ren
ces,
SA
A:
seru
m a
mylo
id A
, sI
CA
M:
solu
ble
inte
rcel
lula
r ad
hes
ion
mo
lecu
le-1
, S
LP
I: s
ecre
tory
leu
ko
cyte
pro
teas
e in
hib
ito
r, S
OD
: su
per
oxid
e
dis
mu
tase
, T
BA
-MD
A a
d.:
Thio
bar
bit
uri
c ac
id,
mal
ond
iald
ehyd
e ad
du
cts,
sT
NF
R:
solu
ble
tu
mo
r n
ecro
sis
fact
or
rece
pto
r, T
EA
C:
Tro
lox
eq
uiv
alen
t
anti
ox
idan
t ca
pac
ity,
TIM
P-1
: T
issu
e in
hib
ito
r of
met
allo
pro
tein
ase,
TG
F α
: tr
ansf
orm
ing g
row
th f
acto
r α
, T
NFα
: tu
mo
r n
ecro
sis
fact
or α
, V
EG
F:
vas
cula
r
end
oth
elia
l gro
wth
fac
tor,
W:
wee
ks
afte
r E
CO
PD
onse
t
Sy
mb
ols
: ↔
: n
o d
iffe
ren
ce, ↑
: in
crea
se, ↓:
dec
reas
e, S
: se
rum
, P
: pla
sma
Pag
e 47
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

Ta
ble
E
Co
rrel
atio
ns
of
syst
emic
bio
mar
ker
s at
EC
OP
D o
nse
t an
d d
uri
ng t
hei
r co
urs
e
Bio
mark
er
Sa
mp
le
Co
r.
Wit
h o
ther
bio
mark
ers
Wit
h c
lin
ica
l v
ari
ab
les
log
adip
onec
tin
P
-
CR
PS
17,
IL-6
S1
7,
TN
Fα
S17
BN
P
P
+
CR
PN
/R27,
PC
TN
/R27
Age2
7
Co
pep
tin
P
+
L
euco
cyte
co
unts
(w
eak c
orr
elat
ion)2
8
S
+
leu
cocy
te c
ou
nt2
,10, lo
g n
eutr
op
hil
co
unt2
9,
log l
epti
n P
17,
IL-
6S
13,
IL-8
SP
13,
PC
TS
8_ENREF_32
Cli
nic
al s
core
23
P
+
BN
P27,
EP
OP
22,
IL-6
P14,
PC
TN
/R26,
pro
AD
MP
44,
pro
ET
1P
44,
leu
cocy
te c
ou
nt
(wea
k c
orr
elat
ion
)28
N/R
+
B
NP
P27,
PC
TN
/R26
Un
ivar
iate
ass
oci
atio
n w
ith s
pu
tum
co
lou
r53
CR
P
S
- lo
g a
dip
onec
tin
P17
log
CR
P
S
- lo
g E
ryth
rocy
ticG
SH
Px
act
ivit
y29
∆ (
b-D
0)
CR
P
P
+
∆(b
-D0
) IL
-6P
14
EC
P
S
+
MP
OS
33
∆ (
b-D
0)E
T-1
P
-
∆ΕΤ
1S
P50
∆S
atO
250
EP
O
P
+
CR
PP
22,
circ
ula
tin
g n
eutr
oph
ils2
2
Pag
e 48
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

∆(b
-D0
)fib
rino
gen
P
+
∆
(b-D
0)
IL-6
P36
Glu
cose
P
+
s
TN
F R
55 (
on
Day
7 )
6
%F
M (
on
Day
7 )
6
Lep
tin
S
+
T
NFα
S38,4
2
∆le
pti
n
S
+
∆T
NFα
S38
P
+
CR
PS
17,
IL-6
S1
7,
TN
Fα
S17
lo
gle
pti
n
P
-
Die
tary
in
take/
RE
E r
atio
(on
Day
7)6
IgE
S
+
M
PO
S33
IGF
-I
S
+
Q
uad
rice
ps
pea
k t
orq
ue2
4
∆(b
-D0
)IL
-1R
a P
+
∆
(b-D
0)
IL-6
P14
S
+
CR
PS
13,
IL8
SP
13,
logle
pti
nP
17
P
+
CR
PP
14,
MP
IF-1
P14,
a n
etw
ork
of
seven
in
terr
elat
ed p
rote
ins
(co
mp
risi
ng I
L-1
Ra,
IL
-8,
IL-1
2,
IL-1
5,
IL-2
R,
NG
F,
and
amp
hir
egu
lin)P
14
IL-6
S
- L
og a
dip
on
ecti
n P
17
log
IL
-6
S
-
Qu
adri
ceps
pea
k t
orq
ue2
4
P
+
∆
Dysp
nea
52
∆IL
-6
P
-
∆
FE
V1
52
Pag
e 49
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

S
+
∆ (
b-D
0)
fib
rin
ogen
P36, ∆
(b
-D0
) IL
6S
P41
∆ i
n b
acte
rial
lo
ad21
P
+
∆ (
b-D
0)
CR
PP
14, ∆
(b-D
0)
fibri
no
gen
P36,∆
(b-D
0)
IL-1
RaP
14,
∆(b
-D0
) M
PIF
-1P
14
∆(b
-D0
)IL
-6
S
-
Bas
elin
e F
EV
141
log
IL
-8
S
-
Qu
adri
ceps
pea
k t
orq
ue2
4
∆ I
L-8
P
+
∆ D
ysp
nea
52
IP-1
0
S
+
V
iral
load
21
MP
IF-1
P
+
IL
-6P
14
∆(b
-D0
)MP
IF-1
P
+
∆
(b-D
0)
IL-6
P14
MP
O
S
+
EC
PS
S
+
BN
P27,
CR
PS
8,2
6_ENREF_51
, le
uco
cyte
co
un
ts26,
pro
AD
MP
44,
pro
ET
1P
44
P
CT
N/R
+
B
NP
27,
CR
PN
/R26,
Pro
AD
MP
44
P
or
S
-
Sy
mp
tom
sco
re (
at a
dm
issi
on
)28
Pro
AD
M
P
+
CR
PP
44,
PC
TN
/R44,
pro
ET
1P
44
Age,
Ch
arls
on’s
co
mo
rbid
ity s
core
, le
ft v
entr
icu
lar
ejec
tio
n
frac
tio
n44
Pro
ET
1
P
+
CR
PP
44,
PC
TN
/R44,P
roA
DM
P44
Age,
Ch
arls
on’s
co
mo
rbid
ity s
core
44
sIL
-1 R
II
P
+
∆le
uco
cyte
cou
nt9
Pag
e 50
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

SP
-D
S
-
Lu
ng f
un
ctio
n p
aram
eter
s46
sTN
F R
55
P
+
G
luco
seP (
on
Day
7)6
D
ieta
ry i
nta
ke/
RE
E r
atio
(on
Day
7)
P
+
Pro
tein
su
lfh
yd
ryl
con
cen
trat
ion
P45
T
EA
C
P
- S
up
ero
xid
e an
ion
rel
ease
by s
tim
ula
ted
neu
tro
ph
ils4
5
Co
mm
ents
:
a)T
he
stu
dy o
f H
urs
t et
al.
14co
mp
ared
36
pla
sma
bio
mar
ker
s at
EC
OP
D o
nse
t usi
ng a
mat
rix o
f 63
0 c
orr
elat
ion
s. I
n t
he
curr
ent
table
th
e m
ost
pro
min
ent
corr
elat
ion
s ar
e re
po
rted
.
b)
As
far
as p
red
icto
rs a
re c
on
cern
ed, in
a s
tep
wis
e m
ult
iple
lin
ear
regre
ssio
n m
od
el t
he
mo
st s
ign
ific
ant
pre
dic
tor
of
log l
epti
n a
nd
of
log a
dip
onec
tin
on
adm
issi
on
was
IL
6 w
her
eas
the
mo
st s
ign
ific
ant
pre
dic
tors
of
log L
/A r
atio
on
ad
mis
sio
n w
ere
TN
Fa
and
IL
617.
PC
T w
as a
pre
dic
tor
for
pro
AD
M44,
pro
ET
144
and
co
pep
tin
28 l
evel
s o
n a
dm
issi
on
. C
RP
lev
els
on
adm
issi
on
wer
e si
gn
ific
ant
pre
dic
tors
of
copep
tin
lev
els2
8.
Ab
bre
via
tio
ns:
BN
P:
bra
in n
atri
ure
tic
pep
tid
e, C
or.
: co
rrel
atio
n,
CR
P:
C-r
eact
ive
pro
tein
, E
CP
: eo
sin
op
hil
cat
ionic
pro
tein
, E
T-1
: en
do
thel
in 1
, E
PO
:
eryth
ropo
ieti
n,
FM
%:
fat
mas
s ex
pre
ssed
as
per
centa
ge
of
bo
dy w
eigh
t, F
EV
1:
forc
ed e
xp
irat
ory
vo
lum
e in
1se
c, G
SH
Px
: G
luta
thio
ne
per
ox
idas
e, I
gE
:
imm
un
oglo
bu
lin
E,
IGF
-I:
insu
lin
-lik
e gro
wth
fac
tor
I, I
L:
inte
rleu
kin
, IL
-1R
a: i
nte
rleu
kin
1 r
ecep
tor
anta
go
nis
t, I
P-1
0:
IFNγ
ind
uce
d p
rote
in 1
0, lo
g:
logar
ith
m,
MP
IF-1
: M
yel
oid
pro
gen
ito
r in
hib
itory
fac
tor-
1,
MP
O:
myel
op
erox
idas
e, P
:pla
sma,
PC
T:
pro
calc
ito
nin
, P
roA
DM
: pro
-ad
reno
med
ull
in,
Pro
ET
1:
pro
endo
thel
in 1
, R
EE
: re
stin
g e
ner
gy e
xp
end
iture
, S
: se
rum
, ,
SP
: sp
utu
m,
s T
NF
R:
solu
ble
tu
mo
r n
ecro
sis
fact
or
rece
pto
r, S
P-D
: su
rfac
tant
pro
tein
D,
TE
AC
: T
rolo
x e
quiv
alen
t an
tiox
idan
t ca
pac
ity,
TN
Fα
: tu
mo
r n
ecro
sis
fact
or α
, T
NT
: tr
op
onin
Sy
mb
ols
: +
: po
siti
ve
corr
elat
ion
, -:
neg
ativ
e co
rrel
atio
n, ∆
: ch
ange
du
rin
g t
he
cours
e of
EC
OP
D, ∆
(b-D
0):
chan
ge
bet
wee
n b
asel
ine
and
EC
OP
D o
nse
t, N
/R:
no
t re
port
ed
Pag
e 51
of
58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

REFERENCES
1. Bathoorn E, Liesker JJ, Postma DS, et al. Change in inflammation in out-
patient COPD patients from stable phase to a subsequent exacerbation. Int J Chron
Obstruct Pulmon Dis 2009;4:101-9.
2. Bircan A, Gokirmak M, Kilic O, Ozturk O, Akkaya A. C-reactive protein
levels in patients with chronic obstructive pulmonary disease: role of infection. Med
Princ Pract 2008;17:202-8.
3. Bozinovski S, Hutchinson A, Thompson M, et al. Serum amyloid a is a
biomarker of acute exacerbations of chronic obstructive pulmonary disease. Am J
Respir Crit Care Med 2008;177:269-78.
4. Brekke PH, Omland T, Holmedal SH, Smith P, Soyseth V. Troponin T
elevation and long-term mortality after chronic obstructive pulmonary disease
exacerbation. Eur Respir J 2008;31:563-70.
5. Christ-Crain M, Jaccard-Stolz D, Bingisser R, et al. Effect of procalcitonin-
guided treatment on antibiotic use and outcome in lower respiratory tract infections:
cluster-randomised, single-blinded intervention trial. Lancet 2004;363:600-7.
6. Creutzberg EC, Wouters EF, Vanderhoven-Augustin IM, Dentener MA,
Schols AM. Disturbances in leptin metabolism are related to energy imbalance during
acute exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care
Med 2000;162:1239-45.
7. Crooks SW, Bayley DL, Hill SL, Stockley RA. Bronchial inflammation in
acute bacterial exacerbations of chronic bronchitis: the role of leukotriene B4. Eur
Respir J 2000;15:274-80.
Page 52 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

8. Daniels JM, Schoorl M, Snijders D, et al. Procalcitonin vs C-reactive protein
as predictive markers of response to antibiotic therapy in acute exacerbations of
COPD. Chest 2010;138:1108-15.
9. Dentener MA, Creutzberg EC, Schols AM, et al. Systemic anti-inflammatory
mediators in COPD: increase in soluble interleukin 1 receptor II during treatment of
exacerbations. Thorax 2001;56:721-6.
10. Dev D, Wallace E, Sankaran R, et al. Value of C-reactive protein
measurements in exacerbations of chronic obstructive pulmonary disease. Respir Med
1998;92:664-7.
11. Gompertz S, O'Brien C, Bayley DL, Hill SL, Stockley RA. Changes in
bronchial inflammation during acute exacerbations of chronic bronchitis. Eur Respir J
2001;17:1112-9.
12. Hill AT, Campbell EJ, Bayley DL, Hill SL, Stockley RA. Evidence for
excessive bronchial inflammation during an acute exacerbation of chronic obstructive
pulmonary disease in patients with alpha(1)-antitrypsin deficiency (PiZ). Am J Respir
Crit Care Med 1999;160:1968-75.
13. Hurst JR, Perera WR, Wilkinson TM, Donaldson GC, Wedzicha JA. Systemic
and upper and lower airway inflammation at exacerbation of chronic obstructive
pulmonary disease. Am J Respir Crit Care Med 2006;173:71-8.
14. Hurst JR, Donaldson GC, Perera WR, et al. Use of plasma biomarkers at
exacerbation of chronic obstructive pulmonary disease. Am J Respir Crit Care Med
2006;174:867-74.
15. Kherad O, Kaiser L, Bridevaux PO, et al. Upper viral respiratory infection,
biomarkers and chronic obstructive pulmonary disease (COPD) exacerbations. Chest
2010;138:896-904.
Page 53 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

16. Koutsokera A, Kiropoulos TS, Nikoulis DJ, et al. Clinical, functional and
biochemical changes during recovery from COPD exacerbations. Respir Med
2009;103:919-26.
17. Krommidas G, Kostikas K, Papatheodorou G, et al. Plasma leptin and
adiponectin in COPD exacerbations: Associations with inflammatory biomarkers.
Respir Med 2010;104:40-6.
18. Lazar Z, Huszar E, Kullmann T, et al. Adenosine triphosphate in exhaled
breath condensate of healthy subjects and patients with chronic obstructive pulmonary
disease. Inflamm Res 2008;57:367-73.
19. Perera WR, Hurst JR, Wilkinson TM, et al. Inflammatory changes, recovery
and recurrence at COPD exacerbation. Eur Respir J 2007;29:527-34.
20. Phua J, Koay ES, Zhang D, et al. Soluble triggering receptor expressed on
myeloid cells-1 in acute respiratory infections. Eur Respir J 2006;28:695-702.
21. Quint JK, Donaldson GC, Goldring JJ, Baghai-Ravary R, Hurst JR, Wedzicha
JA. Serum IP-10 as a biomarker of human rhinovirus infection at exacerbation of
COPD. Chest 2010;137:812-22.
22. Sala E, Balaguer C, Villena C, et al. Low Erythropoietin Plasma Levels during
Exacerbations of COPD. Respiration 2010;80:190-7.
23. Sethi S, Wrona C, Eschberger K, Lobbins P, Cai X, Murphy TF. Inflammatory
profile of new bacterial strain exacerbations of chronic obstructive pulmonary disease.
Am J Respir Crit Care Med 2008;177:491-7.
24. Spruit MA, Gosselink R, Troosters T, et al. Muscle force during an acute
exacerbation in hospitalised patients with COPD and its relationship with CXCL8 and
IGF-I. Thorax 2003;58:752-6.
Page 54 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

25. Stockley RA, O'Brien C, Pye A, Hill SL. Relationship of sputum color to
nature and outpatient management of acute exacerbations of COPD. Chest
2000;117:1638-45.
26. Stolz D, Christ-Crain M, Bingisser R, et al. Antibiotic treatment of
exacerbations of COPD: a randomized, controlled trial comparing procalcitonin-
guidance with standard therapy. Chest 2007;131:9-19.
27. Stolz D, Breidthardt T, Christ-Crain M, et al. Use of B-Type Natriuretic
Peptide in the Risk Stratification of Acute Exacerbations of COPD. Chest
2008;133:1088-94.
28. Stolz D, Christ-Crain M, Morgenthaler NG, et al. Copeptin, C-reactive
protein, and procalcitonin as prognostic biomarkers in acute exacerbation of COPD.
Chest 2007;131:1058-67.
29. Tkacova R, Kluchova Z, Joppa P, Petrasova D, Molcanyiova A. Systemic
inflammation and systemic oxidative stress in patients with acute exacerbations of
COPD. Respir Med 2007;101:1670-6.
30. Weis N, Almdal T. C-reactive protein--can it be used as a marker of infection
in patients with exacerbation of chronic obstructive pulmonary disease? Eur J Intern
Med 2006;17:88-91.
31. Daubin C, Parienti JJ, Vabret A, et al. Procalcitonin levels in acute
exacerbation of COPD admitted in ICU: a prospective cohort study. BMC Infect Dis
2008;8:145.
32. Muller B, Morgenthaler N, Stolz D, et al. Circulating levels of copeptin, a
novel biomarker, in lower respiratory tract infections. Eur J Clin Invest 2007;37:145-
52.
Page 55 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

33. Fiorini G, Crespi S, Rinaldi M, Oberti E, Vigorelli R, Palmieri G. Serum ECP
and MPO are increased during exacerbations of chronic bronchitis with airway
obstruction. Biomed Pharmacother 2000;54:274-8.
34. Rohde G, Gevaert P, Holtappels G, et al. Soluble interleukin-5 receptor alpha
is increased in acute exacerbation of chronic obstructive pulmonary disease. Int Arch
Allergy Immunol 2004;135:54-61.
35. Gerritsen WB, Asin J, Zanen P, van den Bosch JM, Haas FJ. Markers of
inflammation and oxidative stress in exacerbated chronic obstructive pulmonary
disease patients. Respir Med 2005;99:84-90.
36. Wedzicha JA, Seemungal TA, MacCallum PK, et al. Acute exacerbations of
chronic obstructive pulmonary disease are accompanied by elevations of plasma
fibrinogen and serum IL-6 levels. Thromb Haemost 2000;84:210-5.
37. Balbi B, Bason C, Balleari E, et al. Increased bronchoalveolar granulocytes
and granulocyte/macrophage colony-stimulating factor during exacerbations of
chronic bronchitis. Eur Respir J 1997;10:846-50.
38. Kythreotis P, Kokkini A, Avgeropoulou S, et al. Plasma leptin and insulin-like
growth factor I levels during acute exacerbations of chronic obstructive pulmonary
disease. BMC Pulm Med 2009;9:11.
39. Stankiewicz W, Dabrowski MP, Chcialowski A, Plusa T. Cellular and
cytokine immunoregulation in patients with chronic obstructive pulmonary disease
and bronchial asthma. Mediators Inflamm 2002;11:307-12.
40. Karadag F, Karul AB, Cildag O, Yilmaz M, Ozcan H. Biomarkers of systemic
inflammation in stable and exacerbation phases of COPD. Lung 2008;186:403-9.
Page 56 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from
41. Wilkinson TM, Hurst JR, Perera WR, Wilks M, Donaldson GC, Wedzicha JA.
Effect of interactions between lower airway bacterial and rhinoviral infection in
exacerbations of COPD. Chest 2006;129:317-24.
42. Calikoglu M, Sahin G, Unlu A, et al. Leptin and TNF-alpha levels in patients
with chronic obstructive pulmonary disease and their relationship to nutritional
parameters. Respiration 2004;71:45-50.
43. Noguera A, Busquets X, Sauleda J, Villaverde JM, MacNee W, Agusti AG.
Expression of adhesion molecules and G proteins in circulating neutrophils in chronic
obstructive pulmonary disease. Am J Respir Crit Care Med 1998;158:1664-8.
44. Stolz D, Christ-Crain M, Morgenthaler NG, et al. Plasma pro-adrenomedullin
but not plasma pro-endothelin predicts survival in exacerbations of COPD. Chest
2008;134:263-72.
45. Rahman I, Skwarska E, MacNee W. Attenuation of oxidant/antioxidant
imbalance during treatment of exacerbations of chronic obstructive pulmonary
disease. Thorax 1997;52:565-8.
46. Shakoori TA, Sin DD, Ghafoor F, Bashir S, Bokhari SN. Serum surfactant
protein D during acute exacerbations of chronic obstructive pulmonary disease. Dis
Markers 2009;27:287-94.
47. Zeng M, Wen Y, Liu LY, Wang H, Guan KP, Huang X. Role of TNF-alpha,
sTNF-R55 and sTNF-R75 in Inflammation of Acute Exacerbations of Chronic
Obstructive Pulmonary Disease. Respiration 2009;78:399-403.
48. Rahman I, Morrison D, Donaldson K, MacNee W. Systemic oxidative stress in
asthma, COPD, and smokers. Am J Respir Crit Care Med 1996;154:1055-60.
Page 57 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

49. Gumral N, Naziroglu M, Ongel K, et al. Antioxidant enzymes and melatonin
levels in patients with bronchial asthma and chronic obstructive pulmonary disease
during stable and exacerbation periods. Cell Biochem Funct 2009;27:276-83.
50. Roland M, Bhowmik A, Sapsford RJ, et al. Sputum and plasma endothelin-1
levels in exacerbations of chronic obstructive pulmonary disease. Thorax 2001;56:30-
5.
51. Seemungal T, Harper-Owen R, Bhowmik A, et al. Respiratory viruses,
symptoms, and inflammatory markers in acute exacerbations and stable chronic
obstructive pulmonary disease. Am J Respir Crit Care Med 2001;164:1618-23.
52. Pinto-Plata VM, Livnat G, Girish M, et al. Systemic cytokines, clinical and
physiological changes in patients hospitalized for exacerbation of COPD. Chest
2007;131:37-43.
53. Brusse-Keizer MG, Grotenhuis AJ, Kerstjens HA, et al. Relation of sputum
colour to bacterial load in acute exacerbations of COPD. Respir Med 2009;103:601-6.
Page 58 of 58
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from

DOI 10.1378/chest.11-0495; Prepublished online August 11, 2011;Chest
Angela Koutsokera, Daiana Stolz, Stelios Loukides and Konstantinos KostikasCLINICAL CHALLENGE
SYSTEMIC BIOMARKERS IN EXACERBATIONS OF COPD: THE EVOLVING
November 14, 2011This information is current as of
http://chestjournal.chestpubs.org/content/early/2011/08/10/chest.11-0495Updated Information and services can be found at:
Updated Information & Services
http://www.chestpubs.org/site/misc/reprints.xhtmlonline at: Information about reproducing this article in parts (figures, tables) or in its entirety can be foundPermissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
Reprints
the right of the online article.Receive free e-mail alerts when new articles cite this article. To sign up, select the "Services" link to
Citation Alerts
slide format. See any online figure for directions. articles can be downloaded for teaching purposes in PowerPointCHESTFigures that appear in Images in PowerPoint format
[email protected]. For inquriires, please contact the AACP Media Relations Department at (847) 498-1400 or
Papers in Press are not under media or public embargo once the appear online.CHEST (DOI) and date of in-press publication. PubMed, but any references to an in-press article must include the digital object identifier version may contain substantive or nonsubstantive changes. These articles are indexed bypublished in an issue of the journal and have not yet been edited or typeset. The final
Papers in Press are peer-reviewed, accepted articles that have not yet beenCHEST
Copyright © 2011 American College of Chest Physicians by Stylianos Loukides on November 14, 2011chestjournal.chestpubs.orgDownloaded from