systematic review and meta-analysis of the literature
TRANSCRIPT

CONFIDENTIAL
Work Package 1: Identification of
models of children’s primary care:
Systematic Review and Meta-analysis
of the Literature
February 2016
Commission Deliverable: Report on
systematic review and meta-analysis for
MOCHA WP1 (edition 1).

2
Systematic Review and Meta-analysis of the
Literature
Dr Nadia Minicuci, Dr Barbara Corso, Dr Ilaria Rocco - The CNR Institute of
Neuroscience (CNR-IN), Padova, Italy.
Status
MOCHA Commission Deliverable 2 (D1.1):
Report on systematic review and meta-analysis of the literature on models
for WP1. (1st Edition)
Origin Work Package 1: Identification of Models of Children’s Primary Care
Distribution
European Commission
Internal distributin to the MOCHA project
The project is funded by the European Commission through the Horizon 2020 Framework under the
grant agreement number: 634201. The sole responsibility for the content of this project lies with the
authors. It does not necessarily reflect the opinion of the European Union. The European Commission is
not responsible for any use that may be made of the information contained therein.

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
CONFIDENTIAL 3
Contents Introduction 5 Background 5 Autistic Spectrum Disorder 5
Autistic Spectrum Disorder diagnosis 6 Epidemiology of Autistic Spectrum Disorders 8
Immunisation 8 Materials and methods 17
Search Strategy 17 Eligibility Criteria 17 Data extraction 18 Summary of the study selection process 18
Meta Analysis 20 Type of care country classification 20
Results 23 Autistic Spectrum Disorder 23 Asperger’s syndrome 27 Autistic disorder 29 Pervasive developmental disorder, not otherwise specified 31 Immunisation 32 Measles, Mumps and Rubella (MMR) 33 Measles 36 Mumps 39 Rubella 40
Conclusions 41 Strengths and limitations 42 Appendix 1 43 Appendix 2 47 References 69
References for systematic review – appendix 1 71 References for systematic review – appendix 2 74
Table of Figures
Figure 1: Flow chart age at ASD diagnosis 18 Figure 2: Flow chart age at MMR coverage 19 Figure 3: Meta analysis for mean age at onset of ASD Paediatrician-led system 24 Figure 4: Meta analysis for mean age at onset of ASD GP-led system 25 Figure 5: Meta analysis for mean age at onset of ASD Mixed system 26 Figure 6: Meta analysis for mean age at onset of Asperger’s syndrome Paediatrician-led system
27
Figure 7: Meta analysis for mean age at onset of Asperger’s syndrome GP-led system 28 Figure 8: Meta analysis for mean age at onset of Autistic disorder Paediatrician-led system
29
Figure 9: Meta analysis for mean age at onset of Autistic disorder GP-led system 30 Figure 10: Meta analysis for mean age at onset of PDD-NOS Paediatrician-led system 31 Figure 11: Meta analysis for immunisation coverage for MMR Paediatrician-led system 33 Figure 12: Meta analysis for immunisation coverage for MMR GP-led system 34 Figure 13: Meta analysis for immunisation coverage for MMR Mixed system 35 Figure 14: Meta analysis for immunisation coverage for Measles Paediatrician-led system 36 Figure 15: Meta analysis for immunisation coverage for Measles GP-led system 37 Figure 16: Meta analysis for immunisation coverage for Measles Mixed system 38

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
CONFIDENTIAL 4
Figure 17: Meta analysis for immunisation coverage for Mumps Paediatrician-led system 39 Figure 18: Meta analysis for immunisation coverage for Measles GP-led system 40
Tables
Table 1: Recommended immunisations for Measles 11 Table 2: Recommended immunisations for Mumps 13 Table 3: Recommended immunisations for Rubella 15 Table 4: Type of primary care for each EU country 21 Table 5: Summary of the meta analysis findings 41
Note
This edition of the deliverable meets the purpose and objectioves as set out in the Description of
Activity of the MOCHA project. However, given the necessity to limit the number of conditions
studied, and the likelihood of new publications during the lifetime of the project, this deliverable
will be refreshed with later ediitons. Such further work is likely to reinforce and refine the
findings in this edition, rather than to change them fundamentally. Thus this edition forms a
sound building block for other MOCHA activities.

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
CONFIDENTIAL 5
Introduction
This deliverable addresses one of the aims of the WP1 “Identification of Models of Children’s
Primary Health Care”. In order to describe the different models of care provided in Member
States, Norway and Iceland we have conducted a systematic review of the literature and meta-
analysis of the evidence for different models by selecting two of three different aspects of
children’s primary care, each of which reflects a different perspective of the primary care health
system:
1. making an early diagnosis
2. prevention
3. how to deal with a chronic condition
This deliverable addresses the first two perspectives
The first focuses on the age of first diagnosis of Autistic Spectrum Disorder (ASD) (in
particular: Autism/ autistic disorder; Asperger’s syndrome; Pervasive developmental disorder
not otherwise specified; Childhood disintegrative disorder)
The second perspective concentrates on the coverage of immunisation of children (in
particular: measles, mumps and rubella).
The third perspective assesses the control of asthma in children aged over 5, with a particular
focus on unscheduled emergency care and the availability of spirometry at a primary care level-
a key quality indicator . This topic is of particular importance, and will be covered in a further
edition of this deliverable.
The systematic review of Autism spectrum disorders and immunisation produced an
unexpectedly high number of articles to be screened (more than 3000). The findings based on
ASD and Immunisation thus constitute a solid background for the validation of the subsequent
analyses on ADHD and asthma that will be reported in a future report.
Background
Autistic Spectrum Disorder Autism spectrum disorder (ASD) is a disorder of early brain development which affects social
interaction in terms of both verbal and nonverbal communication. Affected children display
restricted and/or repetitive behaviours and can be of varying intelligence.
The core autism behaviours are typically present in early childhood, but features are not always
apparent until the child or young person’s circumstances change, for example when the child
goes to nursery or primary school or moves to secondary school. Autism is strongly associated
with a number of coexisting conditions. Recent studies have shown that approximately 70% of
people with autism also meet diagnostic criteria for at least one other (often unrecognised)
psychiatric disorder that further impairs their psychosocial functioning. Intellectual disability
(intelligence quotient [IQ] below 70) occurs in approximately 50% of young people with autism
(NICE, 2011).All these factors can often make identification a challenge and lead to a delay in
diagnosis.

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
CONFIDENTIAL 6
Autism Spectrum Disorders: diagnosis
ASD is diagnosed by means of one of two classification of disease systems: the Diagnostic and
Statistical Manual of Mental Disorders (DSM), which is now in its fifth edition and is the
standard classification of ‘mental disorders’ used by mental health professionals in the United
States of America; and the International Statistical Classification of Diseases and Related Health
Problems (ICD), which is now on its 10th edition, updated in 2015, and is the standard diagnostic
tool for epidemiology, health management and clinical purposes devised by the World Health
Organisation.
Autism Spectrum Disorder was first described in 1943, by psychiatrist Leo Kanner, who
reported on a group of 11 children who had a preference for isolation and obsession for
sameness (Kanner, 1943). Independently of Kanner’s report, Hans Asperger, an Austrian
paediatrician published a paper in 1944 describing a similar group of children, but who had
higher verbal and cognitive skills (Asperger, 1944). By 1960, autism was viewed as a form of
childhood schizophrenia. However, as science gained a deeper understanding of brain process
and development the disorder was recognised as a product of differences in brain maturation
(Baker, 2013). In 1970s the concept that autism had a psychological origin, rather than a
physical one began to be disproved; and autism was understood as biological in origin and no
longer incompatible with impaired cognitive development.
In 1980, the Diagnostic and Statistical Manual of Mental Disorders third edition (DSM-III)
defined infantile autism as a pervasive developmental disorder (distinct from schizophrenia)
involving three domains: “lack of responsiveness to other people (autism), gross impairment in
communicative skills, and bizarre responses to various aspects of the environment, all
developing within the first 30 months of age” (American Psychiatric Association, 1980).
The DSM-III revision (American Psychiatric Association, 1987) provided a more complex
definition of autistic disorder that required a child to meet 8 of 16 criteria within the three
domains of social interaction, communication, and restricted interest or activities; this
definition dropped the requirement for early onset in life and provided a new category of
“Pervasive Developmental Disorder, Not Otherwise Specified” (PDD-NOS). This category was
used for children meeting some but not all diagnostic criteria for autistic disorder.
The later DSM editions, DSM-IV (1994) and DSM-IV-TR (2000) introduced further refinement
and increasingly complex criteria for autistic disorder and expanded the number of pervasive
developmental disorders to five, to include Asperger’s disorder and Rett’s syndrome (American
Psychiatric Association, 1994 and 2000).
Existing criteria were updated in DSM-V (2013) to give more precise descriptions and reflect
the scientific advances and clinical knowledge about Autism Spectrum Disorder gained in the
last two decades (American Psychiatric Association, 2013). An ASD diagnosis was given by
incorporating four disorders from the previous manual: autistic disorder, Asperger’s disorder,
childhood disintegrative disorder, and the catch-all diagnosis of pervasive developmental
disorder not otherwise specified. Concern grew that those four diagnoses were inconsistently
applied across clinics and treatment centres and, rather than distinct disorders, actually
represented symptoms and behaviours along a severity continuum. Describing ASD as a
continuum is a more accurate and medically and scientifically useful approach. People

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
CONFIDENTIAL 7
diagnosed with one of the separate DSM-IV disorders should still meet the criteria for autism
spectrum disorder or a different DSM-V diagnosis.
The World Health Organization International Statistical Classification of Diseases and Related
Health Problems (ICD)contains codes for diseases, signs and symptoms, abnormal findings,
complaints, social circumstances, and external causes of injury or diseases. The latest revision of
the ICD, ICD-10, was updated in 2015 (ICD-10 Version 2015). The ICD-10 classification of
pervasive developmental disorders, such as Autism Spectrum Disorders is schematically
organised as the following:
F84-Pervasive developmental disorders
A group of disorders characterized by qualitative abnormalities in reciprocal social interactions
and in patterns of communication, and by a restricted, stereotyped, repetitive repertoire of
interests and activities. These qualitative abnormalities are a pervasive feature of the
individual's functioning in all situations.
F84.0-Childhood autism
A type of pervasive developmental disorder that is defined by: (a) the presence of abnormal or
impaired development that is manifest before the age of three years, and (b) the characteristic
type of abnormal functioning in all the three areas of psychopathology: reciprocal social
interaction, communication, and restricted, stereotyped, repetitive behaviour. In addition to
these specific diagnostic features, a range of other nonspecific problems are common, such as
phobias, sleeping and eating disturbances, temper tantrums, and (self-directed) aggression.
F84.1-Atypical autism
A type of pervasive developmental disorder that differs from childhood autism either in age of
onset or in failing to fulfil all three sets of diagnostic criteria. This subcategory should be used
when there is abnormal and impaired development that is present only after age three years,
and a lack of sufficient demonstrable abnormalities in one or two of the three areas of
psychopathology required for the diagnosis of autism (namely, reciprocal social interactions,
communication, and restricted, stereotyped, repetitive behaviour) in spite of characteristic
abnormalities in the other area(s). Atypical autism arises most often in profoundly retarded
individuals and in individuals with a severe specific developmental disorder of receptive
language.
F84.2-Rett's syndrome
A condition, so far found only in girls, in which apparently normal early development is
followed by partial or complete loss of speech and of skills in locomotion and use of hands,
together with deceleration in head growth, usually with an onset between seven and 24 months
of age. Loss of purposive hand movements, hand-wringing stereotypes, and hyperventilation
are characteristic. Social and play development are arrested but social interest tends to be
maintained. Trunk ataxia and apraxia start to develop by age four years and choreoathetoid
movements frequently follow. Severe mental retardation almost invariably results.
F84.3-Other childhood disintegrative disorder
A type of pervasive developmental disorder that is defined by a period of entirely normal
development before the onset of the disorder, followed by a definite loss of previously acquired
skills in several areas of development over the course of a few months. Typically, this is
accompanied by a general loss of interest in the environment, by stereotyped, repetitive motor

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
CONFIDENTIAL 8
mannerisms, and by autistic-like abnormalities in social interaction and communication. In
some cases the disorder can be shown to be due to some associated encephalopathy but the
diagnosis should be made on the behavioural features.
F84.4-Overactive disorder associated with mental retardation and stereotyped movements
An ill-defined disorder of uncertain nosological validity. The category is designed to include a
group of children with severe mental retardation (IQ below 35) who show major problems in
hyperactivity and in attention, as well as stereotyped behaviours. They tend not to benefit from
stimulant drugs (unlike those with an IQ in the normal range) and may exhibit a severe
dysphoric reaction (sometimes with psychomotor retardation) when given stimulants. In
adolescence, the overactivity tends to be replaced by underactivity (a pattern that is not usual in
hyperkinetic children with normal intelligence). This syndrome is also often associated with a
variety of developmental delays, either specific or global. The extent to which the behavioural
pattern is a function of low IQ or of organic brain damage is not known.
F84.5-Asperger’s syndrome
A disorder of uncertain nosological validity, characterized by the same type of qualitative
abnormalities of reciprocal social interaction that typify autism, together with a restricted,
stereotyped, repetitive repertoire of interests and activities. It differs from autism primarily in
the fact that there is no general delay or retardation in language or in cognitive development.
This disorder is often associated with marked clumsiness. There is a strong tendency for the
abnormalities to persist into adolescence and adult life. Psychotic episodes occasionally occur in
early adult life.
F84.8-Other pervasive developmental disorders
F84.9-Pervasive developmental disorder. Unspecified
Epidemiology of Autistic Spectrum Disorders
Over the past 30 years, the number of reported cases of ASD has increased rapidly. The growth
in numbers of ASD cases has been partly explained by changes in diagnosis and classification
criteria, early diagnosis, better awareness and recognition of the condition, taking into account
the type of areas studied (e.g. rural vs urban areas) and also possible differences across
countries.
The lack of mechanisms to obtain consistent and reliable information about ASD trends at a
European level is an important obstacle for the development of better and more equitable
services. Sixteen studies conducted since the year 2000 in European countries by different
teams converge to estimates to a median of 19/10.000 for Autism Disorder (AD) and 62/10.000
for all Pervasive Developmental Disorders (PDDs) combined (Elsabbagh et al., 2012). The
estimate represents an average figure and there is substantial variability across studies;
however this is currently the best estimate for the prevalence of AD and PDDs available.
Immunisation In 1974, WHO established the Expanded Programme on Immunization to ensure that all
children have access to routinely recommended vaccines (Blend, 1998). Since then, global
coverage with the four core vaccines – Bacille Calmette-Guérin vaccine (BCG) for protection
against tuberculosis, diphtheria-tetanus-pertussis vaccine (DTP), polio vaccine, and measles

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
CONFIDENTIAL 9
vaccine – has increased from <5% to ≥85%, and additional vaccines have been added to the
recommended schedule.
The enhancement of immunization activities contributed to a considerable reduction in child in
the WHO European Region over the past few decades.
Coverage with the first dose of measles-containing vaccine (MCV1), the third dose of DTP
vaccine (DTP3) by age 12 months, and the third dose of polio vaccine (polio3) are some key
indicators of immunization programme performance because they reflect key steps or
completion of the basic infant immunization schedule.
In 2014 estimated global coverage for MCV1 was 85%; for the second routine dose of measles-
containing vaccine (MCV2) was 38% by the end of the second year of life and 56% when
including older age groups; for DTP3 was 86%; for BCG was 91% and for (polio3) was 86%
(WHO, 2015).
Vaccination coverage is calculated as the percentage of persons in a target age group who
received a vaccine dose. Countries report administrative coverage annually to the World Health
Organisation (WHO) and the United Nations Children’s Fund (UNICEF) (Administrative data
reported to WHO and UNICEF, 2015), so that national coverage estimates can be derived
through an annual country-by-country review of all available data.
Significant advances have been made in developing new vaccines, and by the end of 2014
supplementary vaccines were introduced into national routine immunization programmes in
some countries: MCV2 (154 countries, 79%), rubella (140 countries, 72%), hepatitis B (184
countries, 95%), 3 doses of Haemophilus influenzae type b (Hib) (192 countries, 99%), rotavirus
(74 countries, 38%), pneumococcal conjugate vaccine (PCV) (117 countries, 60%). Moreover,
immunization programmes have reached additional regional area leading to a greater coverage.
The Global Vaccine Action Plan (GVAP) calls on all countries to reach a target of 90% national
immunization coverage of all vaccines, and 80% coverage among all districts by 2015, with a
sustained coverage level for 3 years by 2020 (Global Vaccine Action Plan, 2014).
The GVAP highlights the importance of sustainable access to vaccines as 1 of its 6 strategic
objectives for achieving high coverage. Despite progress, weaknesses in vaccine stock
management at national and district level continue to hinder the achievement of this objective.
On 17 September 2014, the Member States of the WHO European Region unanimously adopted
the European Vaccine Action Plan 2015-2020 (Global Vaccine Action Plan, 2015). The aim of the
European Vaccine Action Plan is to complement, regionally interpret and adapt the Global
Vaccine Action Plan in harmony with Health 2020 and other key European regional health
strategies and polices by defining objectives, priority action areas and indicators and taking into
account specific needs and challenges of Member States in the WHO European Region.
Within the aspirational vision of European Vaccine Action Plan, six regional goals have been set,
aligned with the Decade of Vaccines and the Global Vaccine Action Plan and in the context of the
European Region:
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
CONFIDENTIAL 10
sustain polio-free status;
eliminate measles and rubella;
control hepatitis B infection;
meet regional vaccination coverage targets at all administrative levels throughout the
Region;
make evidence-based decisions on the introduction of new vaccines;
achieve financial sustainability of national immunization programme.
In general, vaccination coverage and time of administration varies greatly by WHO Region, but
despite the wide diversity of health systems in the European Region, national immunization
programmes are generally strong and routine national vaccination coverage is high.
Tables 1, 2, 3 show the immunization schedules for measles, mumps and rubella (MMR)
vaccines in the European countries (European centre for disease prevention, 2016). These
vaccines (generally given together as the MMR vaccine) were chosen because they are routinely
given to all children in Europe. In addition, the MMR vaccination has been the subject of
controversy in the past 20 years.
The first dose of MMR is given within 12 months of age in 10 countries (Belgium, Croatia,
Estonia, France, Ireland, Liechtenstein, Luxembourg, Portugal, Romania and Spain), within 16
months of age in 15 countries (Bulgaria, Cyprus, Czech Republic, Denmark, Germany, Greece,
Hungary, Italy, Latvia, Lithuania, Malta, Netherlands, Norway, Poland and United Kingdom) and
within the second year of age in the rest of the countries (Austria, Finland, Iceland, Slovakia,
Slovenia and Sweden). Almost all countries in the European Union have introduced the second
dose of MMR immunisation. In Austria, Czech Republic, France, Germany, Liechtenstein and
Luxembourg the second dose of MMR is given within the second year of life, while in Belgium,
Bulgaria, Hungary, Iceland, The Netherlands, Norway, Poland, and Slovakia is given after 9 years
old. In the remaining countries the second dose of MMR is administered between 3 and 8 years
old

11
Table 1. Nationally recommended immunisations for Measles (ME)
Months Years
6 11 12 13 14 15 16 17 18 21 23 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 35 45
Austria
ME1
ME2 Belgium
ME
ME
ME ME
Bulgaria
ME
ME Croatia
ME
ME
Cyprus
ME
ME Czech Republic
ME3
ME4
Denmark
ME5
ME
ME6 Estonia
ME
ME
Finland
ME7
ME France ME8 ME
ME
ME9 ME10
Germany
ME11 ME ME ME12
Greece
ME
ME13 Hungary
ME
ME
Iceland
ME
ME Ireland
ME
ME
Italy
ME
ME
ME14 Latvia
ME
ME
ME15
Liechtenstein
ME
ME Lithuania
ME
ME
Luxembourg
ME
ME Malta
ME
ME
Netherlands
ME
ME Norway
ME
ME
Poland
ME
ME ME16 Portugal
ME
ME
Romania
ME
ME17 Slovakia
ME
ME
Slovenia
ME
ME Spain
ME
ME
Sweden
ME
ME
ME18 United
Kingdom
ME
ME
ME19

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
12
1: Two doses at least 4 weeks apart 2: catch-up for children with no history of vaccination or disease or who received only one dose. Catch-up until 45 years of age 3: first doses given starting at the age of 15 months. second dose should be given 6-10 months after the first dose 4: Administered between 21st and 25th month of life 5: MMR vaccination possible from 9 months of age prior to visiting measles-endemic countries and areas where measles outbreaks are known to occur. The recommended two-dose vaccination schedule at 15 months and 4 years still need to be completed if first vaccination before 12 months 6: previously recommended age at second MMR that will last until 2016 for children who were older than 4 years by 1 April 2008 7: Vaccination can be given from 6 months of age in case of travel abroad. If vaccination starts before 12 months of age, 2 doses are recommended (14-18 months and 6 years) the temporary recommendation of giving measles at 12 months of age was made a permanent recommendation; i.e., now MMR should be given from 12-18 months except if travelling abroad to measles infected countries when it can be given from 6 months on. In case MMR is given at 6-11 months, the child needs a second and third dose to complete the series 8: Update 28 June 2013. For a full description of recommendations, please refer to: http://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=362. The vaccination from 9 months of age of children entering day care was suspended 9: 3 doses of MMR one month apart if no previous vaccination; 1 dose if only one dose previously 10: Two MMR doses in total among individuals born from 1980 11: Vaccination from 9 months in specific circumstances. In this case, the second dose should be given as early as possible in the second year of life 12: One dose of measles for those aged 18 years and over and born from 1970 with no or uncertain vaccination history, with no vaccination history or with only one dose received during childhood. Only an MMR-vaccine is available in Germany 13: Two doses recommended to people belonging to specific occupational categories, please refer to official recommendations. Women found to be seronegative during pregnancy should be vaccinated with 2 doses in the postpartum period 14: Only for those with no vaccination history 15: Catch-up for females not previously vaccinated, with no history of rubella vaccination or disease, 2-dose schedule recommended 16: Catch-up for children who did not receive MMR at 10 years of age (children born before 31 Dec 1996). An additional dose should be given by 19 years of age 17: school-based programme 18: Applicable to children born up to 2001 19: Catch-up programme children, born between 1997 and 2003, who are unvaccinated or only partially vaccinated against measles. For more information please refer to http://www.nhs.uk/news/2013/04April/Pages/New-MMR-catch-up-campaign-one-million-children-targeted.aspx
General recommendation Recommendation for specific groups only Catch-up (e.g. if previous dosed missed)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
13
Table 2. Nationally recommended immunisations for Mumps (MU)
Months Years
11 12 13 14 15 16 17 18 21 23 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 35
Austria MU1
MU2 Belgium
MU
MU
MU MU
Bulgaria
MU
MU Croatia
MU
MU
Cyprus
MU
MU Czech Republic
MU3
MU4
Denmark
MU5
MU
MU6 Estonia
MU
MU
Finland
MU7
MU France
MU
MU
MU8 MU9
Germany MU10 MU MU Greece
MU
MU11
Hungary
MU
MU Iceland
MU
MU
Ireland
MU
MU Italy
MU
MU
MU12
Latvia
MU
MU
MU13 Liechtenstein
MU
MU
Lithuania
MU
MU Luxembourg
MU
MU
Malta
MU
MU Netherlands
MU
MU
Norway
MU
MU Poland
MU
MU MU14
Portugal
MU
MU Romania
MU
MU15
Slovakia
MU
MU Slovenia
MU
MU
Spain
MU
MU Sweden
MU
MU
MU16
United Kingdom
MU
MU
MU17

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
14
1: Two doses at least 4 weeks apart 2: catch-up for children with no history of vaccination or disease or who received only one dose. Catch-up until 45 years of age 3: first doses given starting at the age of 15 months, second dose should be given 6-10 months after the first dose 4: Administered between 21st and 25th month of life 5: MMR vaccination possible from 9 months of age prior to visiting measles-endemic countries and areas where measles outbreaks are known to occur. The recommended two-dose vaccination schedule at 15 months and 4 years still need to be completed if first vaccination before 12 months 6: previously recommended age at second MMR that will last until 2016 for children who were older than 4 years by 1 April 2008 7: Vaccination can be given from 6 months of age in case of travel abroad. If vaccination starts before 12 months of age, 2 doses are recommended (14-18 months and 6 years). The temporary recommendation of giving measles at 12 months of age was made a permanent recommendation; i.e., now MMR should be given from 12-18 months except if travelling abroad to measles infected countries when it can be given from 6 months on. In case MMR is given at 6-11 months, the child needs a second and third dose to complete the series 8: 3 doses of MMR one month apart if no previous vaccination; 1 dose if only one dose previously 9: Two MMR doses in total among individuals born from 1980 10: Vaccination from 9 months in specific circumstances. In this case, the second dose should be given as early as possible in the second year of life 11: Two doses recommended to people belonging to specific occupational categories, please refer to official recommendations. Women found to be seronegative during pregnancy should be vaccinated with 2 doses in the postpartum period 12: Only for those with no vaccination history 13: Catch-up for females not previously vaccinated, with no history of rubella vaccination or disease, 2-dose schedule recommended 14: Catch-up for children who did not receive MMR at 10 years of age (children born before 31 Dec 1996). An additional dose should be given by 19 years of age 15: school-based programme 16: Applicable to children born up to 2001 17: Catch-up programme children, born between 1997 and 2003, who are unvaccinated or only partially vaccinated against measles. For more information please refer to http://www.nhs.uk/news/2013/04April/Pages/New-MMR-catch-up-campaign-one-million-children-targeted.aspx
General recommendation
Recommendation for specific groups only
Catch-up (e.g. if previous dosed missed)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
15
Table 3. Nationally recommended immunisations for Rubella (RU)
Months Years
11 12 13 14 15 16 17 18 21 23 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 45
Austria RU1
RU2 Belgium
RU
RU
RU RU
Bulgaria
RU
RU Croatia
RU
RU
Cyprus
RU
RU Czech Republic
RU3
RU4
Denmark
RU5
RU
RU6 Estonia
RU
RU
Finland
RU7
RU France
RU
RU
RU8 RU9
Germany RU10 RU RU Greece
RU
RU11
Hungary
RU
RU Iceland
RU
RU
Ireland
RU
RU Italy
RU
RU
RU12
Latvia
RU
RU
RU13 Liechtenstein
RU
RU
Lithuania
RU
RU Luxembourg
RU
RU
Malta
RU
RU Netherlands
RU
RU
Norway
RU
RU Poland
RU
RU RU14
Portugal
RU
RU Romania
RU
RU15
Slovakia
RU
RU Slovenia
RU
RU16
Spain
RU
RU Sweden
RU
RU
RU17
United Kingdom
RU
RU
RU18

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
16
1: Two doses at least 4 weeks apart 2: catch-up for children with no history of vaccination or disease or who received only one dose. Catch-up until 45 years of age 3: first doses given starting at the age of 15 months, second dose should be given 6-10 months after the first dose 4: Administered between 21st and 25th month of life 5: MMR vaccination possible from 9 months of age prior to visiting measles-endemic countries and areas where measles outbreaks are known to occur. The recommended two-dose vaccination schedule at 15 months and 4 years still need to be completed if first vaccination before 12 months 6: previously recommended age at second MMR that will last until 2016 for children who were older than 4 years by 1 April 2008 7: Vaccination can be given from 6 months of age in case of travel abroad. If vaccination starts before 12 months of age, 2 doses are recommended (14-18 months and 6 years) the temporary recommendation of giving measles at 12 months of age was made a permanent recommendation; i.e., now MMR should be given from 12-18 months except if travelling abroad to measles infected countries when it can be given from 6 months on. In case MMR is given at 6-11 months, the child needs a second and third dose to complete the series 8: 3 doses of MMR one month apart if no previous vaccination; 1 dose if only one dose previously 9: Two MMR doses in total among individuals born from 1980. For rubella, one dose of MMR among unvaccinated woman 10: Vaccination from 9 months in specific circumstances. In this case, the second dose should be given as early as possible in the second year of life 11: Two doses recommended to people belonging to specific occupational categories, please refer to official recommendations. Women found to be seronegative during pregnancy should be vaccinated with 2 doses in the postpartum period 12: Only for those with no vaccination history 13: Catch-up for females not previously vaccinated, with no history of rubella vaccination or disease, 2-dose schedule recommended 14: Catch-up for children who did not receive MMR at 10 years of age (children born before 31 Dec 1996). An additional dose should be given by 19 years of age 15: school-based programme 16: Recommended only. Not included in the national immunization schedule 17: Applicable to children born up to 2001 18: Catch-up programme children, born between 1997 and 2003, who are unvaccinated or only partially vaccinated against measles. For more information please refer to http://www.nhs.uk/news/2013/04April/Pages/New-MMR-catch-up-campaign-one-million-children-targeted.aspx
General recommendation Recommendation for specific groups only Catch-up (e.g. if previous dosed missed)
17
Materials and methods
Search strategy A comprehensive electronic search was performed using PubMed.
For Autism Spectrum Disorder (ASD) the following key words have been set for the search in
the title or in the abstract: (autism spectrum disorder OR autistic disorder OR Asperger OR
Asperger’s syndrome OR Asperger’s disorder OR pdd-nos OR pervasive developmental disorder
OR childhood disintegrative disorder OR cdd); moreover ((age) AND (diagnosis OR onset)) was
set for the search in the full-text. The filter child: birth <18 was set.
For immunisation the following key words have been set for the search in the title or in the
abstract: (vaccine* OR immuniz*) AND (measl* OR mump* OR rubell* OR mmr) AND (coverage),
using the filters child: birth <18 and humans.
All potentially eligible articles were screened at title, abstract, and full-text stages in order to
sequentially identify the study country and the availability of the investigated outcomes.
The PubMed search was supplemented with hand-searching of reference lists of all potentially
eligible full-text articles.
Eligibility criteria Types of study design: Any type of study design has been included in the search; however the
search identified mainly observational studies, either cross-sectional or longitudinal.
Reference year: all papers published in the range of years 2000-2016.
Language restriction: only papers published in English were considered
Outcomes investigated:
a) ASD focused on the age at onset of the following conditions:
a1) Autism/ autistic disorder;
a2) Asperger’s syndrome;
a3) Pervasive developmental disorder not otherwise specified;
a4) Childhood disintegrative disorder;
b) Immunisation investigated the coverage of the following conditions:
b1) Measles;
b2) Mumps;
b3) Rubella.

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
18
Data extraction The following data were extracted from all included papers: the first author’s last name,
publication year, country where the study was conducted, the study design, the outcome
measures investigated, the sample size, the age of reference, and gender.
Summary of the study selection process The following figures show the different steps of the selection process for ASD and
Immunisation, respectively.
The PubMed search retrieved 2122 articles on ASD from year 2000 to 2016 (Fig. 1). Sixty-nine
percent of these papers (1356/2122) have been excluded since the research was not carried out
in a European Country. Selecting the EU countries articles was particularly time-consuming as it
often required reading the full-text. Twenty-one articles were retrieved manually, leading to
787 articles read as a full text. Out of these, only 37 have been included in our systematic review
(4.7%).
Figure 1. Flow chart age at ASD diagnosis
The PubMed search retrieved 1008 articles on Immunisation from year 2000 to 2016 (Fig. 2).
Sixty-four percent of these papers (648/1008) have been excluded since the research was not
carried out in a European Country. The mere selection of the EU and EEA countries’ articles was
Identification of the studies by electronic search
(n=2122)
EU/EEA articles (n=787)
Finally included articles (n=37)
Articles excluded based on: - no full text or not in English
(n=192) - not pertinent or no information
(n=546) - duplication (n=12)
Articles excluded because not EU/EEA
(n=1356)
Articles identified by manual research (n=21)
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
19
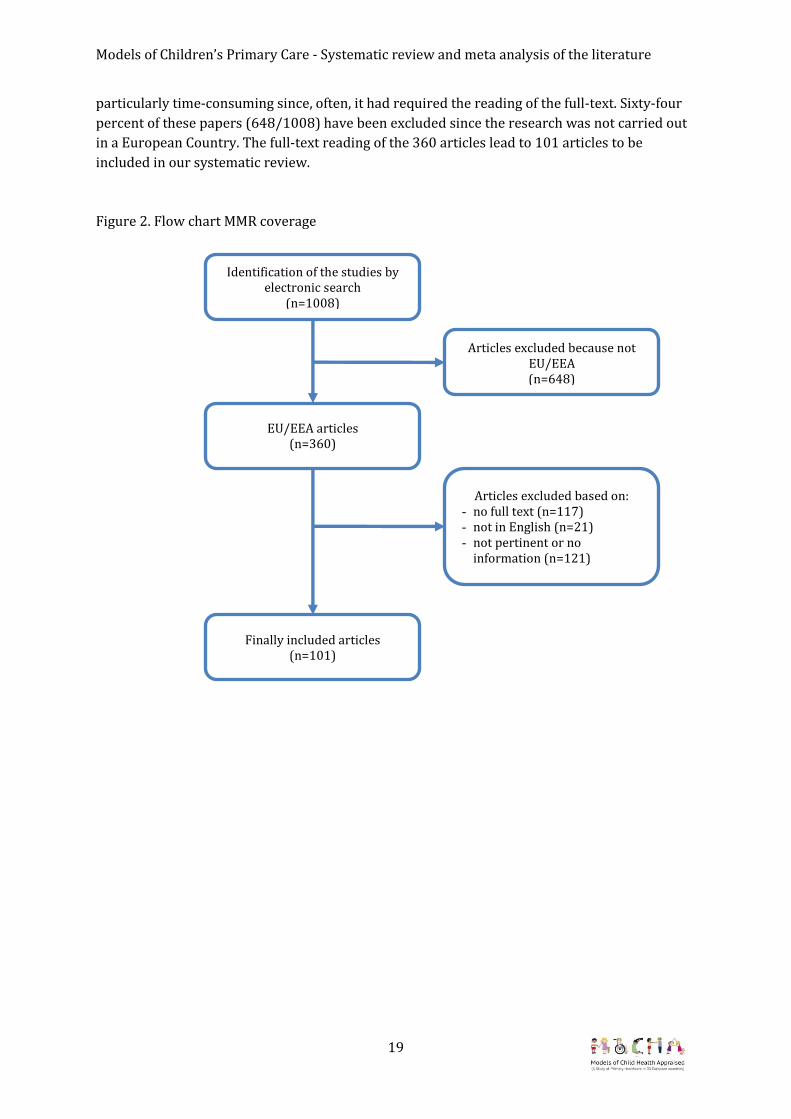
particularly time-consuming since, often, it had required the reading of the full-text. Sixty-four
percent of these papers (648/1008) have been excluded since the research was not carried out
in a European Country. The full-text reading of the 360 articles lead to 101 articles to be
included in our systematic review.
Figure 2. Flow chart MMR coverage
Identification of the studies by electronic search
(n=1008)
EU/EEA articles (n=360)
Finally included articles (n=101)
Articles excluded based on: - no full text (n=117) - not in English (n=21) - not pertinent or no
information (n=121)
Articles excluded because not EU/EEA (n=648)
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
20
Meta-analysis In our search the primary interest lies in the descriptive estimates, as opposed to comparative
estimates that arise naturally for Randomized Controlled Trial studies or cohort studies (where
exposed are compared with the unexposed) or case-control studies (where people with the
condition are compared with people without the condition).
Investigated outcomes have been combined in a pooled estimate, using the method of the
inverse of the variance, that is the weighting assigned to the different studies is related with the
inverse of the standard error and therefore indirectly to the sample size. This implies that
studies with smaller standard error and larger sample size are given more weight in the
calculation of the pooled estimates. Fixed effects or random effects model have been used,
according to the presence of heterogeneity which was tested by means of the Cochrane’s Q test
and the Higgins I2 statistic which was interpreted as follows: I2 of 25 % = low heterogeneity. I2 of
50 % = medium heterogeneity. I2 = 75 % = high heterogeneity. The results of the different
studies and the overall estimate with its 95% Confidence Interval (95%CI) are illustrated in a
"forest plot" graph.
Type of care: country classification The EU and EEA countries have been classified according to their primary care system defined
as: Paediatrician mainly oriented (Paed); General Practitioner mainly oriented (GP); Mixed. This
classification is the outcome of the MOCHA classification task group based on the Country Agent
investigations upon a specific request from the WP leaders on a case study.
Table 4 reports the description of the health system given by the Country Agents, the findings
from van Esso et al. (2010) ( who have used the term “combined”when referring to GP and
Paediatrician systems) and the MOCHA classification working group. The term mixed
incorporates other professionals involvement as first line contatcs e.g. nursing staff.

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
21
Table 4: Type of primary care for each EU country
Country Description of type of
primary care
From van Esso et al.
Arch Dis Child 2010;
95:791-5
MOCHA
Classification
Austria GP and paediatrician Combined Mixed
Belgium Family doctor or 1st line
paediatrician Combined Mixed
Bulgaria
GP for those with health
insurance. Pre 2000 was
mandatory to have a
community paediatrician for
children up to 18; this
generation now retiring and
GPs only have 9 weeks
paediatrics training.
GP GP
Croatia Primary care doctor /
paediatrician - Paed
Cyprus
Private paediatrician or
public funded GP who will
refer to hospital
Paediatrician if necessary
Paed Mixed
Czech Republic “registering paediatrician”
accessed via triage nurse Paed Paed
Denmark - GP GP
Estonia GP GP GP
Finland GP GP GP
France
Family physician or GP who
is either a Paediatrician or a
GP
GP Mixed
Germany Paediatrician GP Paed
Greece
GP or Paediatrician chosen
from insurance co list
Usually paediatrician up to
18 years old.
Paed Paed
Hungary - Combined Mixed
Iceland
One family doctor from a
health care centre or private
paediatrician
Combined Mixed
Ireland GP GP GP
Italy
0-14 have paediatrician or
GP if none locally. Max 800
children per paediatrician
Mixed Paed
Latvia GP / family doctor or a GP Mixed

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
22
paediatrician
Lithuania Family doctor or
paediatrician Combined Mixed
Luxembourg Family doctor. Paediatrician
up to the age of 2 years. Combined Mixed
Malta
Family doctor (private) or
walk in community health
centre
- GP
Netherlands GP (Triaged by nurse) GP GP
Norway GP GP GP
Poland GP or Paediatrician chosen
from insurance company list GP Mixed
Portugal GP (80%) or private
paediatrician GP GP
Romania Family doctor - GP
Slovakia - Paed Paed
Slovenia - Paed Paed
Spain Family doctor in health care
centre or a paediatrician Paed Mixed
Sweden
Child health care nurse up to
age 6; school health nurse
afterwards.
GP/Paediatricians in
hospital contacted by nurse
GP Mixed
United Kingdom GP as a named accountable
professional GP GP
The Paed/GP/Mixed MOCHA classification was used to perform the meta-analysis for each type
of primary care and allow some speculations on possible difference across types of primary care
systems.
Sweden reported a system based on a child health nurse and for our purposes was classified as
Mixed; Luxembourg reported a Paed if the child was under two years and a GP if was over 2
years and for our purposes was classified as Mixed.

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
23
Results
Autistic Spectrum Disorder Appendix 1 shows the main characteristics of the identified studies for ASD. A total of 37 studies
have been identified, of which 10 investigated ASD only. The age of reference reported in the
studies ranges from 0 to 65 years and the sample size from 6 to 10297 for ASD, from 11 to 4475
for Autism/ autistic disorder, from 3 to 4192 for Asperger’s syndrome, from 19 to 1796 for
Pervasive developmental disorder not otherwise specified, and 6 for Childhood disintegrative
disorder. The majority of the studies had been carried out in one country, with the exception of
Salomone E. (2015) that considered 18 EU countries and Pry R. (2005) that considered 4 EU
countries. Most of the studies (29.7%) have been carried out in UK, followed by Denmark
(13.5%), The Netherlands and Sweden (10.8%), Italy (8%), France (5.4%) and Finland, Greece,
Germany, Czech Republic and Belgium (3.7%).
For the meta-analysis 14 articles have been excluded because they did not provide the mean of
the age at diagnosis and/or the standard error.
The meta-analysis was performed by the MOCHA classification type of primary care in each
country. Paediatrician included 4 countries (Czech Republic, Germany, Greece and Italy), GP
included 8 countries (Denmark, Finland, Ireland, Netherland, Norway, Portugal, Romania and
UK), and Mixed included 7 countries (Belgium, Hungary, France, Iceland, Poland, Spain and
Sweden).

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
24
For the calculation of the pooled estimate of the mean age at onset for ASD, a random effect
model was used, due to the presence of heterogeneity in Paediatrician-led systems (Q=535.4; p-
value<0.0001; I2=99.44%), in GP-led systems (Q=9159.43; p-value<0.0001; I2=99.84%) and in
Mixed (Q=257.8; p-value<0.0001; I2=96.90%).
The pooled estimated of age at onset for ASD was 50.6 months with a 95% CI = (34.2-66.9) in a
Paediatrician-led primary care system, as presented in fig.3.
Figure 3. Meta-analysis for mean age at onset of ASD, Paediatrician-led primary care system.
Meta-analysis
30 40 50 60 70 80
Estimate
Salomone E., 2015 [Czech Rep.]
Salomone E., 2015 [Germany]
Salomone E., 2015 [Italy]
Ververi A., 2012 [Greece]
Total (fixed effects)
Total (random effects)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
25
The pooled estimated of age at onset for ASD was 57.5 months with a 95% CI= (39.8-75.2) in a
GP-led primary care system, as presented in fig.4.
Figure 4. Meta-analysis for mean age at onset of ASD, GP-led primary care system.
Meta-analysis
0 50 100 150 200 250
Estimate
Chakrabarti S., 2005 [UK(Midlands)]
Hathorn C., 2014 [UK (Scotland)]
Latif A.H.A., 2007 [UK(South Wales)]
Mouridsen S.E., 2014 [Denmark]
Oosterling I.J., 2010 [Netherlands (Gelderland)]
Salomone E., 2015 [Denmark]
Salomone E., 2015 [Finland]
Salomone E., 2015 [Ireland]
Salomone E., 2015 [Netherlands]
Salomone E., 2015 [Norway]
Salomone E., 2015 [Portugal]
Salomone E., 2015 [Romania]
Salomone E., 2015 [UK]
Stagg S.D., 2014 [UK (South London)]
van der Ven E., 2013 [Netherlands]
Visser J.C., 2013 [Netherlands]
Total (fixed effects)
Total (random effects)
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
26
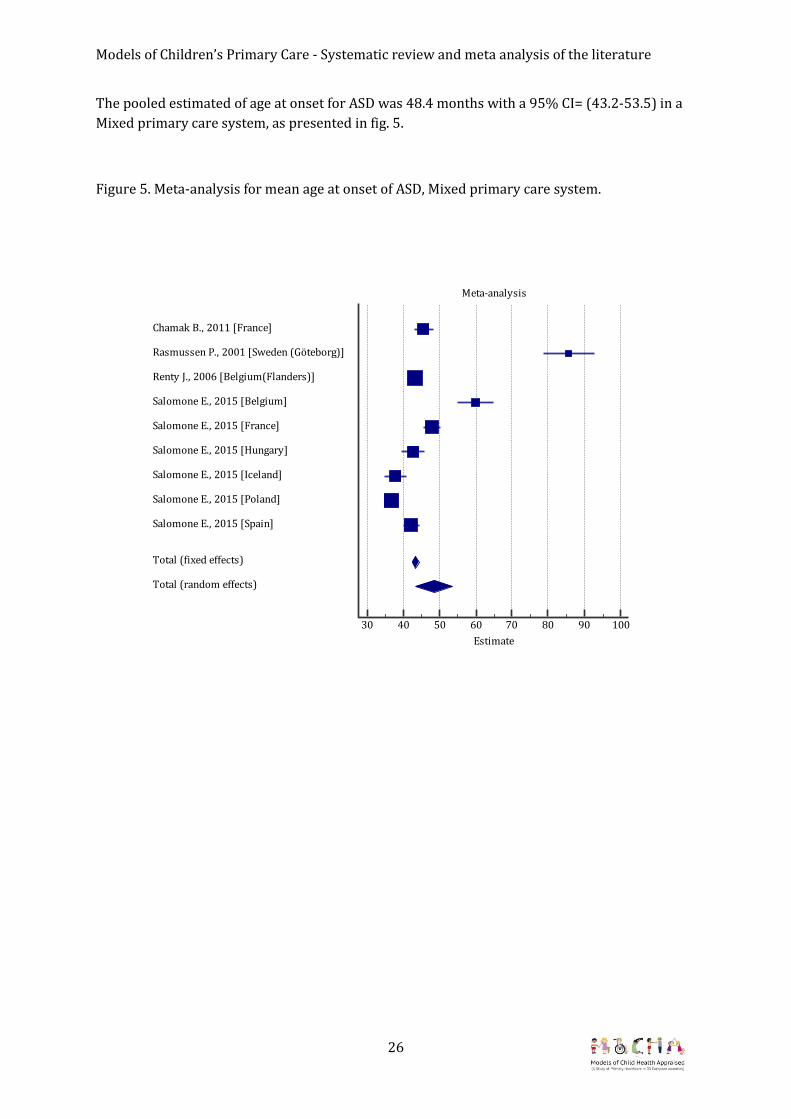
The pooled estimated of age at onset for ASD was 48.4 months with a 95% CI= (43.2-53.5) in a
Mixed primary care system, as presented in fig. 5.
Figure 5. Meta-analysis for mean age at onset of ASD, Mixed primary care system.
Meta-analysis
30 40 50 60 70 80 90 100
Estimate
Chamak B., 2011 [France]
Rasmussen P., 2001 [Sweden (Göteborg)]
Renty J., 2006 [Belgium(Flanders)]
Salomone E., 2015 [Belgium]
Salomone E., 2015 [France]
Salomone E., 2015 [Hungary]
Salomone E., 2015 [Iceland]
Salomone E., 2015 [Poland]
Salomone E., 2015 [Spain]
Total (fixed effects)
Total (random effects)
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
27
Asperger’s syndrome
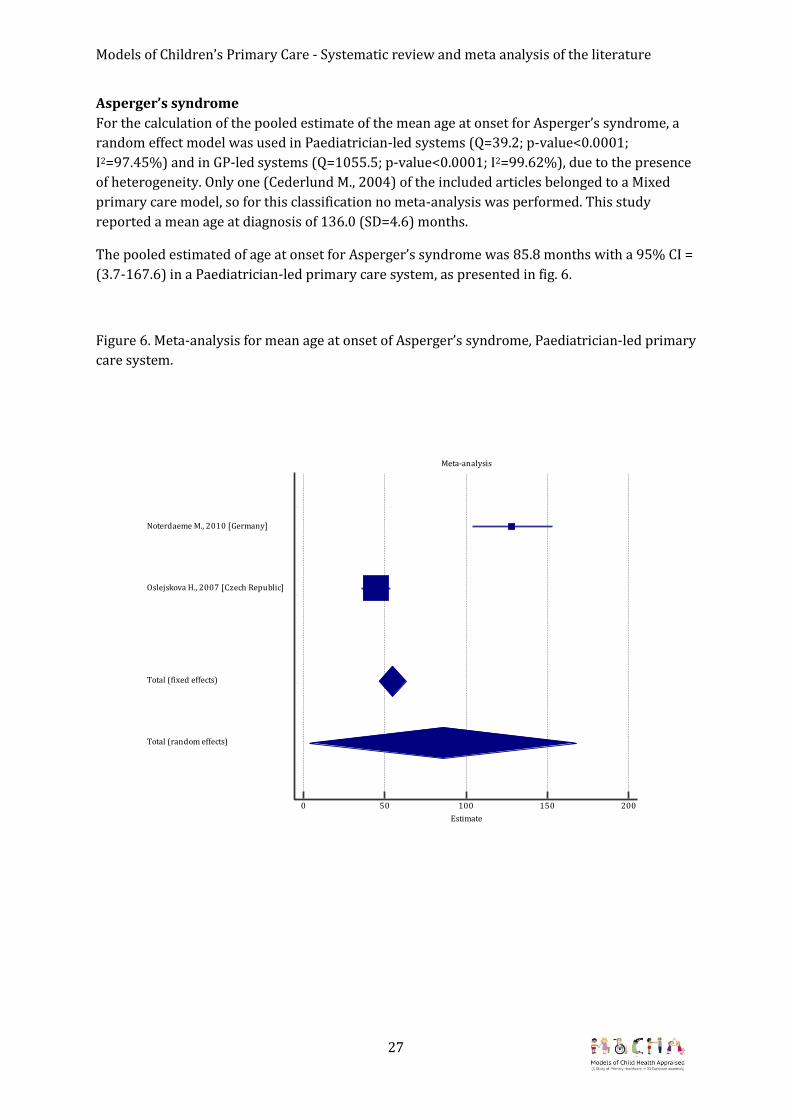
For the calculation of the pooled estimate of the mean age at onset for Asperger’s syndrome, a
random effect model was used in Paediatrician-led systems (Q=39.2; p-value<0.0001;
I2=97.45%) and in GP-led systems (Q=1055.5; p-value<0.0001; I2=99.62%), due to the presence
of heterogeneity. Only one (Cederlund M., 2004) of the included articles belonged to a Mixed
primary care model, so for this classification no meta-analysis was performed. This study
reported a mean age at diagnosis of 136.0 (SD=4.6) months.
The pooled estimated of age at onset for Asperger’s syndrome was 85.8 months with a 95% CI =
(3.7-167.6) in a Paediatrician-led primary care system, as presented in fig. 6.
Figure 6. Meta-analysis for mean age at onset of Asperger’s syndrome, Paediatrician-led primary
care system.
Meta-analysis
0 50 100 150 200
Estimate
Noterdaeme M., 2010 [Germany]
Oslejskova H., 2007 [Czech Republic]
Total (fixed effects)
Total (random effects)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
28
The pooled estimated of age at onset for Asperger’s syndrome was 111.2 months with a 95% CI
= (93.6-128.9) in a GP-led primary care system, as presented in fig. 7.
Figure 7. Meta-analysis for mean age at onset of Asperger’s syndrome, GP-led primary care
system.
Meta-analysis
70 80 90 100 110 120 130 140 150
Estimate
Begeer S., 2013 [Netherlands]
Begeer S., 2013 [Finland]
Chakrabarti S., 2005 [UK(Midlands)]
Mouridsen S.E., 2014 [Denmark]
van der Ven E., 2013 [Netherlands]
Total (fixed effects)
Total (random effects)
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
29
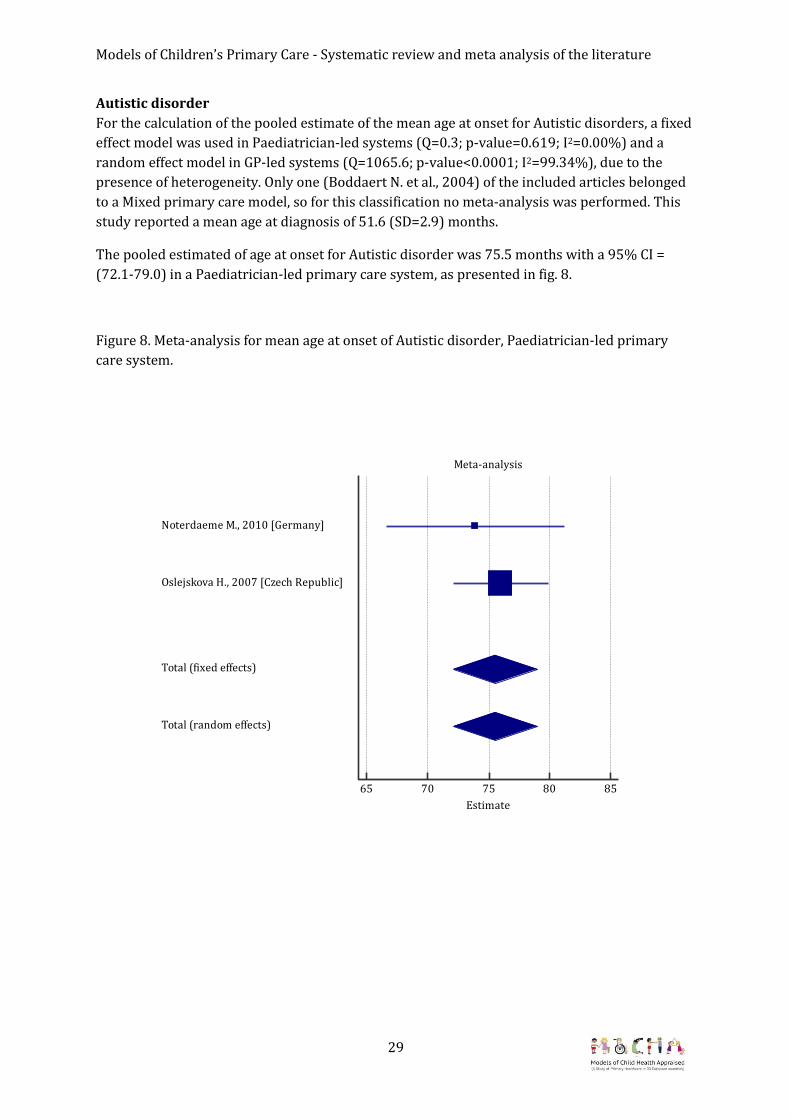
Autistic disorder
For the calculation of the pooled estimate of the mean age at onset for Autistic disorders, a fixed
effect model was used in Paediatrician-led systems (Q=0.3; p-value=0.619; I2=0.00%) and a
random effect model in GP-led systems (Q=1065.6; p-value<0.0001; I2=99.34%), due to the
presence of heterogeneity. Only one (Boddaert N. et al., 2004) of the included articles belonged
to a Mixed primary care model, so for this classification no meta-analysis was performed. This
study reported a mean age at diagnosis of 51.6 (SD=2.9) months.
The pooled estimated of age at onset for Autistic disorder was 75.5 months with a 95% CI =
(72.1-79.0) in a Paediatrician-led primary care system, as presented in fig. 8.
Figure 8. Meta-analysis for mean age at onset of Autistic disorder, Paediatrician-led primary
care system.
Meta-analysis
65 70 75 80 85
Estimate
Noterdaeme M., 2010 [Germany]
Oslejskova H., 2007 [Czech Republic]
Total (fixed effects)
Total (random effects)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
30
The pooled estimated of age at onset for Autistic disorder was 57.5 months with a 95% CI =
(45.1-69.9) in a GP-led primary care system, as presented in fig. 9.
Figure 9. Meta-analysis for mean age at onset of Autistic disorder, GP-led primary care system.
Meta-analysis
10 20 30 40 50 60 70 80 90
Estimate
Begeer S., 2013 [Netherlands]
Campbell M., 2013 [UK (Glasgow)]
Chakrabarti S., 2005 [UK(Midlands)]
Jokiranta E., 2013 [Finland]
Mouridsen S.E., 2007 [Denmark]
Mouridsen S.E., 2014 [Denmark]
Powell J.E., 2000 [UK (West Midlands)]
van der Ven E., 2013 [Netherlands]
Total (fixed effects)
Total (random effects)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
31
Pervasive Developmental Disorder, Not Otherwise Specified (PDD-NOS)
For the calculation of the pooled estimate of the mean age at onset for PDD-NOS, a random
effect model in GP-led systems (Q=583.2; p-value<0.0001; I2=99.49%) was used, due to the
presence of heterogeneity. None of the articles belonged to either Paediatrician-led or Mixed
primary care model classification.
The pooled estimated of age at onset for PDD-NOS was 72.9 months with a 95% CI = (54.9-90.8)
in a GP-led primary care system, as presented in fig. 10.
Figure 10. Meta-analysis for mean age at onset of PDD_NOS, GP-led primary care system.
Meta-analysis
30 40 50 60 70 80 90 100
Estimate
Begeer S., 2013 [Finland]
Begeer S., 2013 [Netherlands]
Chakrabarti S., 2005 [UK(Midlands)]
van der Ven E., 2013 [Netherlands]
Total (fixed effects)
Total (random effects)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
32
Immunisation Appendix 2 shows the main characteristics of the identified studies for Measles, Mumps and
Rubella vaccination. A total of 101 studies have been identified, of which the majority
investigated the MMR vaccination alone and Measles alone (56 papers and 23 papers,
respectively), 8 looked at all the three Measles, Mumps and Rubella conditions. Rubella alone
was studied in 6 studies, Mumps alone in 4 studies, and the combination Measles-Rubella,
Measles-MMR, Rubella-MMR and MMRV (MMR+Varicella) were analysed in one study each. In
four studies, immunisation coverage is presented as a comparison of more countries (one on
Measles alone, one on Rubella alone and two in MMR) whereas all the remaining regard only
one country. Germany, Italy, United Kingdom, Poland, Belgium and France are the most
investigated countries with at least 10 papers each (17, 15, 14, 11, 10 and 10, respectively),
whereas no papers were found from Estonia, Finland, Portugal and Iceland.
For the meta-analysis 53 studies have been excluded because neither the sample size nor the
95% CI for the stated percentage of coverage was reported in the paper. The meta-analysis was
performed by the MOCHA classification type of primary care in each country for the remaining
papers. Based on the information retrieved, for each type of primary care the following
countries were included for meta-analyses:
Paediatrician-led: 7 countries (Croatia, Czech Republic, Germany, Greece, Italy, Slovenia,
Slovakia);
GP-led: 6 countries (Bulgaria, Ireland, Malta, Netherlands, Romania, United Kingdom);
Mixed: 9 countries (Austria, Belgium, Cyprus, France, Latvia, Lithuania, Luxembourg,
Spain, Sweden).
There was no information received from 4 countries: Denmark, Hungary, Norway and
Poland.

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
33
Measles, Mumps and Rubella (MMR)
The pooled estimate of immunisation coverage for MMR was calculated by a random effect
model, due to the presence of heterogeneity in Paediatrician-led models (Q=73994.0; p-
value<0.0001; I2=99.99%), in GP-led models (Q=23375.9; p-value<0.0001; I2=99.96%) and in
Mixed models (Q=789.2; p-value<0.0001; I2=98.48%).
The pooled estimated of immunisation coverage for MMR was 73.1% with a 95% CI = (30.1-
99.0) in a Paediatrician-led primary care system, as presented in fig.11.
Figure 11. Meta-analysis for immunisation coverage for MMR, Paediatrician-led primary care
system.
Meta-analysis
0,0 0,2 0,4 0,6 0,8 1,0
Proportion
Kalies H, 2006 [Germany]
Khetsuriani N, 2011 [Croatia]
Mikolajczyk RT, 2008 [Germany (Bavaria)]
Pavlopoulou ID, 2013 [Greece (Athens)]
Restivo V, 2015 [Italy (Palermo)]
Reuss AM, 2010 [Germany]
Sakou II, 2011 [Greece (Athens)]
Takla A, 2014 [Italy (Friuli-Venezia-Giulia, Tuscany, Marche, Lazio, Calabria)]
Total (fixed effects)
Total (random effects)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
34
The pooled estimated of immunisation coverage for MMR was 73.7% with a 95% CI= (66.6-
80.2) in a GP-led primary care system, as presented in fig.12.
Figure 12. Meta-analysis for immunisation coverage for MMR, GP-led primary care system.
Meta-analysis
0,3 0,4 0,5 0,6 0,7 0,8 0,9 1,0
Proportion
Choi YH, 2008 [United Kingdom (England)]
Henderson R, 2004 [United Kingdom (Highland, Scotland)]
Khetsuriani N, 2011 [Ireland]
Lashkari HP, 2010 [United Kingdom (Haringey, London)]
Mixer RE, 2007 [United Kingdom (Brent, London)]
Sandford H, 2015 [United Kingdom (England)]
Simone B, 2014 [United Kingdom (England-LA)]
Simone B, 2014 [United Kingdom (England-LB)]
Stanescu A, 2011 [Romania]
van der Wal MF, 2005 [Netherlands (Amsterdam)]
Total (fixed effects)
Total (random effects)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
35
The pooled estimated of immunisation coverage for MMR was 93.9% with a 95% CI= (90.5-
96.6) in a Mixed primary care system, as presented in fig.13.
Figure 13. Meta-analysis for immunisation coverage for MMR, Mixed primary care system.
Meta-analysis
0,8 0,9 1,0
Proportion
Bystrom E, 2014 [Sweden (community near Stockholm)]
Lernout T, 2014 [Belgium (Flanders)]
Robert E, 2014 [Belgium (Wallonia)]
Robert E, 2014 [Belgium (Brussels)]
Barrabeig I, 2011 [Spain (Barcelona-South Health Region)]
Borràs E, 2009 [Spain (Catalonia, public health care)]
Borràs E, 2009 [Spain (Catalonia, private health care)]
Vandermeulen C, 2008 [Belgium (Flanders)]
Guagliardo V, 2007 [France (South-Eastern)]
Alfredsson R, 2004 [Sweden (Göteborg)]
Dannetun E, 2004 [Sweden (Ostergotland)]
Vandermeulen C, 2004 [Belgium (Bruges)]
Vellinga A, 2002 [Belgium (Flanders)]
Total (fixed effects)
Total (random effects)
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
36
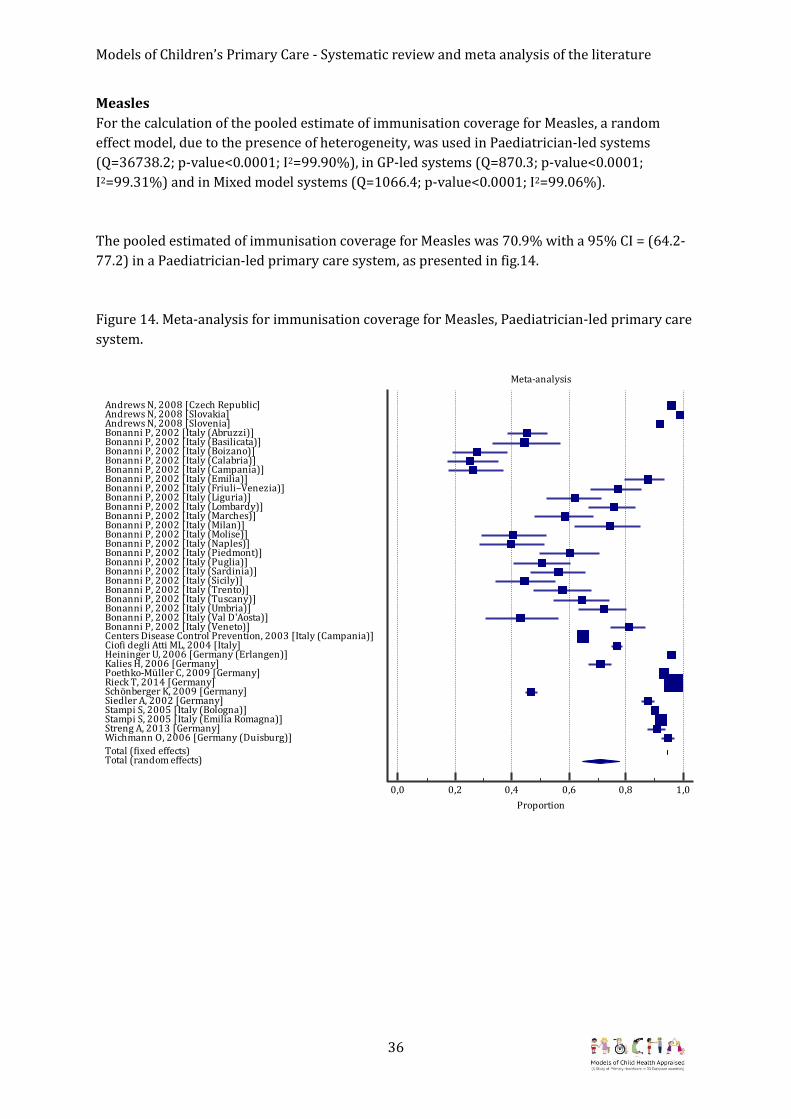
Measles
For the calculation of the pooled estimate of immunisation coverage for Measles, a random
effect model, due to the presence of heterogeneity, was used in Paediatrician-led systems
(Q=36738.2; p-value<0.0001; I2=99.90%), in GP-led systems (Q=870.3; p-value<0.0001;
I2=99.31%) and in Mixed model systems (Q=1066.4; p-value<0.0001; I2=99.06%).
The pooled estimated of immunisation coverage for Measles was 70.9% with a 95% CI = (64.2-
77.2) in a Paediatrician-led primary care system, as presented in fig.14.
Figure 14. Meta-analysis for immunisation coverage for Measles, Paediatrician-led primary care
system.
Meta-analysis
0,0 0,2 0,4 0,6 0,8 1,0
Proportion
Andrews N, 2008 [Czech Republic]Andrews N, 2008 [Slovakia]Andrews N, 2008 [Slovenia]Bonanni P, 2002 [Italy (Abruzzi)]Bonanni P, 2002 [Italy (Basilicata)]Bonanni P, 2002 [Italy (Boizano)]Bonanni P, 2002 [Italy (Calabria)]Bonanni P, 2002 [Italy (Campania)]Bonanni P, 2002 [Italy (Emilia)]Bonanni P, 2002 [Italy (Friuli–Venezia)]Bonanni P, 2002 [Italy (Liguria)]Bonanni P, 2002 [Italy (Lombardy)]Bonanni P, 2002 [Italy (Marches)]Bonanni P, 2002 [Italy (Milan)]Bonanni P, 2002 [Italy (Molise)]Bonanni P, 2002 [Italy (Naples)]Bonanni P, 2002 [Italy (Piedmont)]Bonanni P, 2002 [Italy (Puglia)]Bonanni P, 2002 [Italy (Sardinia)]Bonanni P, 2002 [Italy (Sicily)]Bonanni P, 2002 [Italy (Trento)]Bonanni P, 2002 [Italy (Tuscany)]Bonanni P, 2002 [Italy (Umbria)]Bonanni P, 2002 [Italy (Val D'Aosta)]Bonanni P, 2002 [Italy (Veneto)]Centers Disease Control Prevention, 2003 [Italy (Campania)]Ciofi degli Atti ML, 2004 [Italy]Heininger U, 2006 [Germany (Erlangen)]Kalies H, 2006 [Germany]Poethko-Müller C, 2009 [Germany]Rieck T, 2014 [Germany]Schönberger K, 2009 [Germany]Siedler A, 2002 [Germany]Stampi S, 2005 [Italy (Bologna)]Stampi S, 2005 [Italy (Emilia Romagna)]Streng A, 2013 [Germany]Wichmann O, 2006 [Germany (Duisburg)]
Total (fixed effects)Total (random effects)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
37
The pooled estimated of immunisation coverage for Measles was 91.0% with a 95% CI= (86.9-
94.4) in a GP-led primary care system, as presented in fig.15.
Figure 15. Meta-analysis for immunisation coverage for Measles, GP-led primary care system.
Meta-analysis
0,7 0,8 0,9 1,0
Proportion
Andrews N, 2008 [Bulgaria]
Andrews N, 2008 [England and Wales]
Andrews N, 2008 [Ireland]
Andrews N, 2008 [Malta]
Andrews N, 2008 [Romania]
Hanratty B, 2000 [United Kingdom]
Stanescu A, 2011 [Romania]
Total (fixed effects)
Total (random effects)
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
38
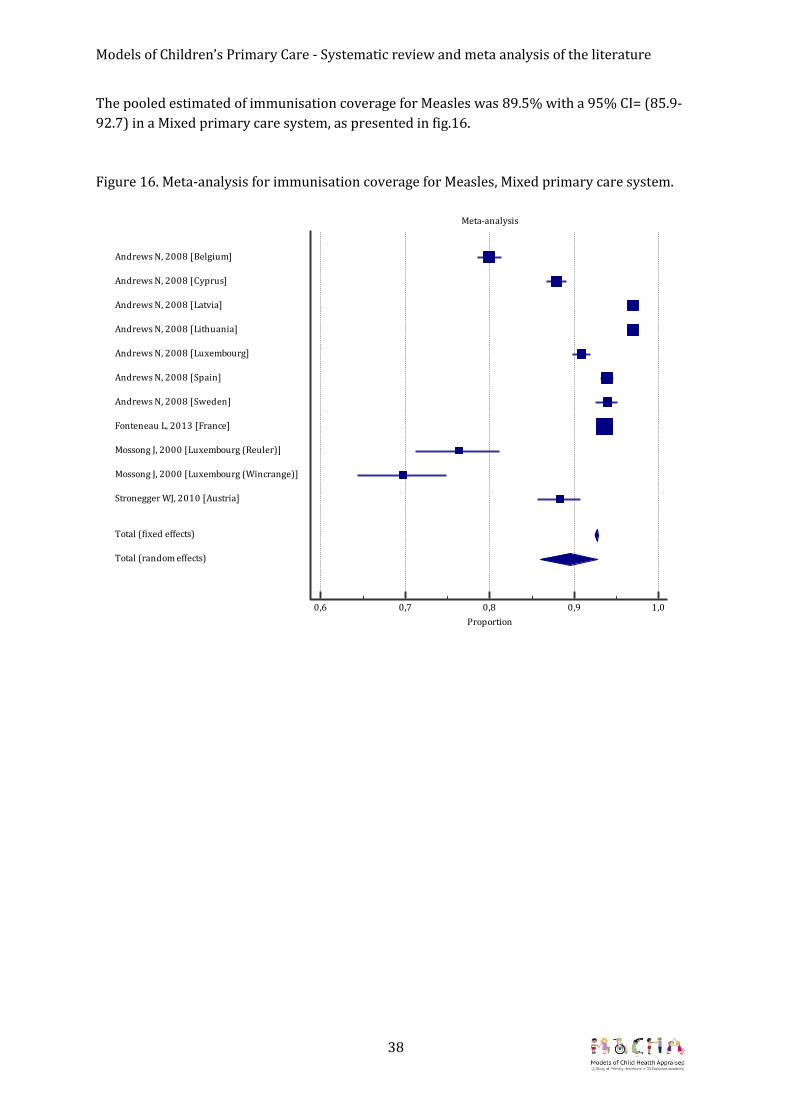
The pooled estimated of immunisation coverage for Measles was 89.5% with a 95% CI= (85.9-
92.7) in a Mixed primary care system, as presented in fig.16.
Figure 16. Meta-analysis for immunisation coverage for Measles, Mixed primary care system.
Meta-analysis
0,6 0,7 0,8 0,9 1,0
Proportion
Andrews N, 2008 [Belgium]
Andrews N, 2008 [Cyprus]
Andrews N, 2008 [Latvia]
Andrews N, 2008 [Lithuania]
Andrews N, 2008 [Luxembourg]
Andrews N, 2008 [Spain]
Andrews N, 2008 [Sweden]
Fonteneau L, 2013 [France]
Mossong J, 2000 [Luxembourg (Reuler)]
Mossong J, 2000 [Luxembourg (Wincrange)]
Stronegger WJ, 2010 [Austria]
Total (fixed effects)
Total (random effects)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
39
Mumps
For the calculation of the pooled estimate of immunisation coverage for Mumps, a random effect
model, due to the presence of heterogeneity, was used in Paediatrician-led systems (Q=2504.7;
p-value<0.0001; I2=99.80%). For the GP-led system no papers addressing Mumps were found,
whereas for Mixed primary care systems only one article was found.
The pooled estimated of immunisation coverage for Mumps was 80.2% with a 95% CI = (73.7-
85.9) in a Paediatrician-led primary care system, as presented in fig.17.
Figure 17. Meta-analysis for immunisation coverage for Mumps, Paediatrician-led primary care
system.
Only one study (Fonteneau L. et al., 2013) was found for Mumps in the Mixed primary care
system and the reported immunisation coverage was 91.4 (95%CI: 90.8-91.9).
Meta-analysis
0,0 0,2 0,4 0,6 0,8 1,0
Proportion
Heininger U, 2006 [Germany (Erlangen)]
Kalies H, 2006 [Germany]
Rieck T, 2014 [Germany]
Stampi S, 2005 [Italy (Bologna)]
Stampi S, 2005 [Italy (Emilia Romagna)]
Takla A, 2014 [Germany (Bavaria)]
Total (fixed effects)
Total (random effects)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
40
Rubella
For the calculation of the pooled estimate of immunisation coverage for Rubella, a random effect
model, due to the presence of heterogeneity, was used in the Paediatrician-led model
(Q=2079.0; p-value<0.0001; I2=99.81%). For GP-led models no articles that addressed Rubella
were found, whereas for Mixed primary care system models, only one article was found.
The pooled estimated of immunisation coverage for Rubella was 88.7% with a 95% CI = (83.5-
93.0) in a Paediatrician-led primary care system, as presented in fig.18.
Figure 18. Meta-analysis for immunisation coverage for Rubella, Paediatrician-led primary care
system.
Only one study (Fonteneau L. et al., 2013) was found for Rubella in the Mixed primary care
system and the reported immunisation coverage was 91.4 (95%CI: 90,8-91,9).
Meta-analysis
0,6 0,7 0,8 0,9 1,0
Proportion
Heininger U, 2006 [Germany (Erlangen)]
Kalies H, 2006 [Germany]
Rieck T, 2014 [Germany]
Stampi S, 2005 [Italy (Bologna)]
Stampi S, 2005 [Italy (Emilia Romagna)]
Total (fixed effects)
Total (random effects)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
41
Conclusions The meta–analysis performed according to the primary care classification revealed some
similarities and some differences in the investigated outcomes, which are shown in Table 5.
The ASD mean age at onset ranged from 48 to 57 months of age, with no statistical difference
across the three classifications. For Asperger’s syndrome the mean age at onset is higher at 86
months of age for the Paediatrician-led models of primary care and 111 months of age for the
GP-led models of primary care, but again with no statistical difference. As far as Autistic
disorder is concerned, the mean age of diagnosis at onset is statistically lower in the GP system
compared with the Paediatrician-led system (57 months versus 75 months, respectively).
The MMR immunisation coverage is statistically lower for the GP-led versus the Mixed system
(73.7% versus 93.9%), while no differences were found between each of these two
classifications and the Paediatrician system.
For Measles vaccination the findings are always in favour of the GP-led and the Mixed system.
The coverage of Measles vaccinations is lower among Paediatrician-led (70.9%) versus GP-led
(91.0%) and Mixed (89.5%) system.
Table 5. Summary of the meta-analysis findings.
Type of care primary care system Note Paed GP Mixed Mean age (in months) at onset of diagnosis and 95% CI ASD 50.6
(34.2-66.9) 57.5
(39.8-75.2) 48.4
(43.3-55.3) No difference
Asperger’s syndrome
85.8 (3.7-167.9)
111.2 (93.6-128.9)
No article found
No difference
Autistic disorder
75.5 (72.1-79.0)
57.5 (45.1-69.9)
Only one article found
In favour of GP
PDD-NOS No article found
72.9 (54.9-90.8)
No article found
-
Immunisation Coverage (%) and 95% CI MMR 73.1
(30.1-99.0) 73.7
(66.6-80.2) 93.9
(90.5-96.6) Difference between GP and
Mixed (favoured); Measles 70.9
(64.2-77.2) 91.0
(86.9-94.4) 89.5%
(85.9-92.7) Difference between
Paediatrician and GP (favoured);
Difference between Paediatrician and Mixed
(favoured) Mumps 80.2
(73.7-85.9) No article
found Only one
article found -
Rubella 88.7 (83.5-93.0)
No article found
Only one article found
-

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
42
Strength and limitations A meta-analysis is the statistical part of the systematic review process and has some
advantages. Meta-analysis includes more participants than a single constituent study, which
implies a reduction of random errors and an increase of the power. Moreover, a meta-analysis is
capable of exploring variations between studies. However, there are some limitations of both
the primary studies and the systematic review.
For ASD, depending on the age-range of the analysed sample, the age at diagnosis of ASD could
be subject to bias. For example, some studies considered adolescents as the reference
population while other studies included children under the age of 4 years. It is plausible that the
latter case would underestimate the mean age at diagnosis.
The systematic review for PDD-NOS was unable to retrieve studies for countries using the
Paediatrician-led and Mixed models, which made a true meta-analysis impossible. In terms of
autistic disorder, only one study (conducted in France) was found that referred to the countries
within the Mixed model, while for Asperger’s syndrome, there were no studies carried out in
countries using the Mixed model.
Regarding vaccination, different countries administer the first dose of MMR at different ages:
within 12 months of age in 10 countries, within 16 months of age in 15 countries and within the
second year of age in 6 countries. Almost all countries have introduced the second dose of MMR
vaccination within the second year of life, while in other countries it is administered between 3
and 9 years old.
Usually immunisation coverage is assessed, and reported, at 24, 36 months of age. However,
some of the retrieved studies take into account different age setting and retrospectively assess
the immunisation coverage through child’s personal vaccination card, so the coverage for these
studies could be overestimated if compared to other studies that took into considerations lower
ages.
No comparison was performed for Mumps and Rubella, since no studies were found for the
countries within the GP model and only one study (conducted in France) was found for the
Mixed model.
Finally, the MOCHA country classification of type of primary care is based on the actual health
system running in the country, whereas the retrieved articles for the systematic review refer to
precedent years during which the health system may have had a different legislation and
regulation. As the project progresses and different parameters of models of care are considered,
it is possible to carry out further re- analyses according to typologies of care provision other
than the predominant medical professional type.

43
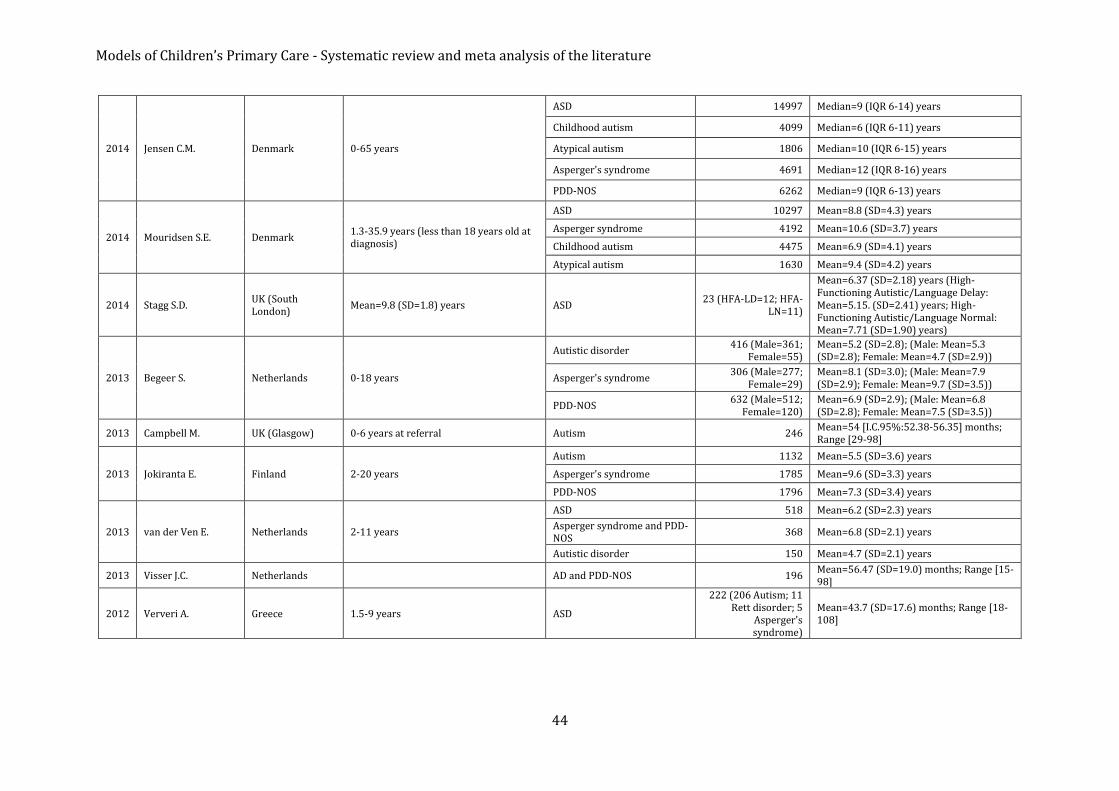
APPENDIX 1. Main characteristics of the identified studies. ASD; Autism/ autistic disorder; Asperger’s syndrome; Pervasive developmental disorder not otherwise specified; Childhood disintegrative disorder.
Year of publication
1st author Country Age of reference Disease Sample size Age at diagnosis
2015 Ferrante M. Italy (Catania) 0-17 years ASD 1122
Median= 4 years (IQR 3-8) in 2014
Median= 5 years (IQR 3-9) in 2004-2009 Median= 4 years (IQR 3-7) in 2010-2014
2015 Salomone E.
Portugal
>=4 years ASD
113 Mean=33.53 (SD=11.66) months
Italy 88 Mean=35.73 (SD=13.02) months
Spain 186 Mean=36.66 (SD=13.54) months
Romania 44 Mean=37.55 (SD=11.23) months
Poland 60 Mean=37.85 (SD=11.7) months
Macedonia 22 Mean=39.59 (SD=10.53) months
Czech Republic 81 Mean=42.21 (SD=10.26) months
Norway 24 Mean=42.5 (SD=14.37) months
Iceland 46 Mean=42.59 (SD=10.9) months
France 154 Mean=42.76 (SD=12.75) months
UK 92 Mean=43.28 (SD=12.42) months
Finland 41 Mean=44 (SD=11.55) months
Belgium 96 Mean=45.71 (SD=13.33) months
Ireland 22 Mean=46.59 (SD=13.45) months
Hungary 106 Mean=47.88 (SD=12.37) months
Germany 79 Mean=48.44 (SD=10.98) months
Netherlands 90 Mean=50.02 (SD=12.22) months
Denmark 66 Mean=50.17 (SD=14.4) months
Total 1410 Mean=42.16 (SD=13.4) months
2014 Hathorn C. UK (Scotland) Under 15 years (less than 7 years old at diagnosis)
ASD 90 Mean=44.6 (SD=12.9) months
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
44
2014 Jensen C.M. Denmark 0-65 years
ASD 14997 Median=9 (IQR 6-14) years
Childhood autism 4099 Median=6 (IQR 6-11) years
Atypical autism 1806 Median=10 (IQR 6-15) years
Asperger's syndrome 4691 Median=12 (IQR 8-16) years
PDD-NOS 6262 Median=9 (IQR 6-13) years
2014 Mouridsen S.E. Denmark 1.3-35.9 years (less than 18 years old at diagnosis)
ASD 10297 Mean=8.8 (SD=4.3) years
Asperger syndrome 4192 Mean=10.6 (SD=3.7) years
Childhood autism 4475 Mean=6.9 (SD=4.1) years
Atypical autism 1630 Mean=9.4 (SD=4.2) years
2014 Stagg S.D. UK (South London)
Mean=9.8 (SD=1.8) years ASD 23 (HFA-LD=12; HFA-
LN=11)
Mean=6.37 (SD=2.18) years (High-Functioning Autistic/Language Delay: Mean=5.15. (SD=2.41) years; High-Functioning Autistic/Language Normal: Mean=7.71 (SD=1.90) years)
2013 Begeer S. Netherlands 0-18 years
Autistic disorder 416 (Male=361;
Female=55) Mean=5.2 (SD=2.8); (Male: Mean=5.3 (SD=2.8); Female: Mean=4.7 (SD=2.9))
Asperger's syndrome 306 (Male=277;
Female=29) Mean=8.1 (SD=3.0); (Male: Mean=7.9 (SD=2.9); Female: Mean=9.7 (SD=3.5))
PDD-NOS 632 (Male=512;
Female=120) Mean=6.9 (SD=2.9); (Male: Mean=6.8 (SD=2.8); Female: Mean=7.5 (SD=3.5))
2013 Campbell M. UK (Glasgow) 0-6 years at referral Autism 246 Mean=54 [I.C.95%:52.38-56.35] months; Range [29-98]
2013 Jokiranta E. Finland 2-20 years
Autism 1132 Mean=5.5 (SD=3.6) years
Asperger's syndrome 1785 Mean=9.6 (SD=3.3) years
PDD-NOS 1796 Mean=7.3 (SD=3.4) years
2013 van der Ven E. Netherlands 2-11 years
ASD 518 Mean=6.2 (SD=2.3) years
Asperger syndrome and PDD-NOS
368 Mean=6.8 (SD=2.1) years
Autistic disorder 150 Mean=4.7 (SD=2.1) years
2013 Visser J.C. Netherlands AD and PDD-NOS 196 Mean=56.47 (SD=19.0) months; Range [15-98]
2012 Ververi A. Greece 1.5-9 years ASD
222 (206 Autism; 11 Rett disorder; 5
Asperger's syndrome)
Mean=43.7 (SD=17.6) months; Range [18-108]

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
45
2011 Chamak B. France
4-5 years
ASD
19 Mean=2.8 (SD=0.75) years
6-12 years 78 Mean=4.5 (SD=2) years
13-17 years 37 Mean=6.5 (SD=4) years
18-45 years 66 Mean=10 (SD=8) years
4-45 years 200 Mean=5 (SD=3) years
2010 Oosterling I.J. Netherlands (Gelderland)
0-11 years ASD 80 Mean=63.5 (SD=36.9) months
2010 Noterdaeme M. Germany 2-25.3 years at diagnosis
ASD (autism, atypical autism, Asperger’s syndrome) or other PDD
601 (579 ASD, 22 Other PDD)
Mean=6.3 years; Range [2-25.3]
Autism 464 Mean=76 (SD=43) months
Atypical autism 35 Mean=111 (SD=63) months
Asperger's syndrome 80 Mean=110 (SD=43) months
Rett's syndrome 6 Mean=49 (SD=12) months
Disintegrative disorder 6 Mean=60 (SD=25) months
Overactive disorder and stereotyped movements
10 Mean=86 (SD=23) months
2008 Williams E. UK (England) >=11 years
ASD 71 median=81.9 months (IQR 42.7-116.6)
Autism median=44.9 months (IQR 36.5-85.6)
Atypical autism median=75.5 months (IQR 42.7-117.9)
Asperger syndrome median=115.9 months (IQR 93.4-130.6)
2007 Latif A.H.A. UK(South Wales) 0-17 years
ASD
336
Mean=5.5 (SD=2.9) years
Asperger's syndrome Mean=6.6 (SD=2.8) years
Other forms Mean=4.3 (SD=2.3) years
2007 Mouridsen S.E. Denmark Mean=5.4 (SD=2.5) years Infantile autism 111 Mean=5 years 5 months (SD=2 years 6 months )
2007 Oslejskova H. Czech Republic 0-23 years
Childhood Autism 126 Mean=73.9 (SD=41.8) months
Atypical autism 57 Mean=81.1 (SD=37.0) months
Asperger's syndrome 21 Mean=128.5 (SD=57.6) months
2006 Renty J. Belgium(Flanders) 2.69-17.81 years ASD 139 Mean=7.15 (SD=3.55) years
2005 Chakrabarti S. UK(Midlands) 4-6 years olds in a 1996-1998 birth cohort
All PDDs 64 Mean=37.8 (SD=11.4) months
Autistic disorder 25 Mean=32.9 (SD=8.7) months
PDD-NOS 27 Mean=39.3 (SD=9.3) months
Asperger's disorder 12 Mean=44.7 (SD=16.0) months
2005 Larsson H.J. Denmark Infantile or atypical autism
698 ALL: Mean=7.7; Median=6.0; Range[1-24] years
154 DIAGNOSIS BEFORE 1994: Mean=6.2; Median=5.0; Range[1-20] years
554 DIAGNOSIS IN 1994-1999: Mean=8.1; Median=6.0; Range[1-24] years

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
46
2005 Maestro S. Italy (Pisa) AD 21 Mean=39.0 [36-58] months
PDD-NOS 19 Mean=38.4 [36-58] months
2005 Pry R.
France, Switzerland, Belgium and Luxembourg
Median=60 (IQR 48-72) months Infantile autism (F84.0) 222 Median=17 (IQR 8.4-24) months
2004 Boddaert N. France Mean=6.6 (SD=1.6) years [4-10] Autism 11 Mean=4.3 years (SD=0.8)
2004 Cederlund M. Sweden (Göteborg)
5 years 6 months to 24 years 6 months Asperger's syndrome 100 Mean=11 years 4 months (SD=3 years 10 months)
2004 Keen D. UK(Doncaster) 0–17 years ASD 261 Mean=6.3 years (Range: [3.8-15.8])
2004 Smeeth L. UK Birth year [1973-99] median age 5-9 years
Autism and other PDD 1294 Median=5.4 (IQR 3.6-9.7) years
2004 Sturm H. Sweden (Stockholm)
0-15 years Asperger syndrome. PDDNOS and high-functioning autism
101 Mean=9 years 8 months; [5-12]years
2004 Tebruegge M. UK (Maidstone district, Kent)
4 years in October 2000
Childhood autism
6
Mean=3.13 [2.75-3.50] years
Asperger's syndrome Mean=7.22 [5.75-9.25] years
Autistic spectrum disorder Mean=5.37 [3.33-9.42] years
2003 Lingam R. UK(five districts in north east London)
5-14 years
Childhood autism 266 Median=51 (IQR 40-78) months
Atypical autism 171 Median=40 (IQR 34-48) months
Asperger's syndrome 89 Median=97 (IQR 70-125) months
2002 Hultman C.M. Sweden Diagnosis of infantile autism before 10 years of age in the period 1987-1994
Infantile autism (excluding PDD-NOS)
408 Mean=4.4 years
2002 Madsen K.M. Denmark AD 316 Mean= 4 years 3 months
Other ASDs 422 Mean= 5 years 3 months
2001 Maestro S. Italy AD (excluding PDD-NOS) 15 Mean=4.5 years (4-5.2)
2001 Magnùsson P. Iceland Childhood Autism 37 Median=49 months (Range: [26-165])
Atypical autism 20 Median=52 months (Range: [33-170])
2001 Rasmussen P. Sweden (Göteborg)
4-33 years with Down syndrome ASD 25 Mean=14.4 (SD=7.4) years
2000 Powell J.E. UK (West Midlands)
1 years-4 years 11 months Childhood autism 42 Mean=36.2 (SD=59.1) months
Other ASDs 63 Mean=37.8 (SD=90.2) months

47
APPENDIX 2. Main characteristics of the identified studies. Immunisation. Measles, Mumps, Rubella.
Year of publication
1st author Country Years of study
Disease Sample size % Coverage 1st dose
% Coverage 2nd dose
% Coverage 1st+2nd doses
Age reference (years if not spec)
2015 Amendola A Italy (Lombardy) 2007 Measles 96.7 2
Rubella 96.6 2
2011 Measles 93.7 2
Rubella 93.5 2
Measles 90.1 (range: 72.4; 95.8)
2
2015 Cozza V Italy (Puglia) 2010 MMR 93.0 1 (cohort 2010)
2010 MMR 85.0 5-6 (cohort 2005)
2010 MMR 77.0 adolescents (cohort 1997)
2004-2006 MMR 70.9 49.8 7-15 (cohort 1991-1997)
2015 Giambi C Italy 2013 Rubella 88.0 1
Italy (18/21 Regions) 2008 Rubella 75.0 16
2015 Gross K Switzerland 2005 MMR 86.0 2
2015 Hens N Belgium (Brussels) 1995 MMR 68.1 adolescents
Belgium (Wallonia) 1999 MMR 82.4 adolescents
Belgium (Brussels) 2000 MMR 74.5 (95%CI: 70.1-78.9)
adolescents
Belgium (Wallonia) 2003 MMR 82.5 adolescents
Belgium (Flanders) 2005 MMR 94.0 (95%CI: 92.6-95.3)
83.6 (95%CI: 81.4-85.8)
adolescents
Belgium (Brussels) 2006 MMR 91.1 (95%CI: 88.7-93.6)
70.5 adolescents
Belgium (Wallonia) 2006 MMR 89.0 (95%CI: 86.3-91.8)
70.5 adolescents
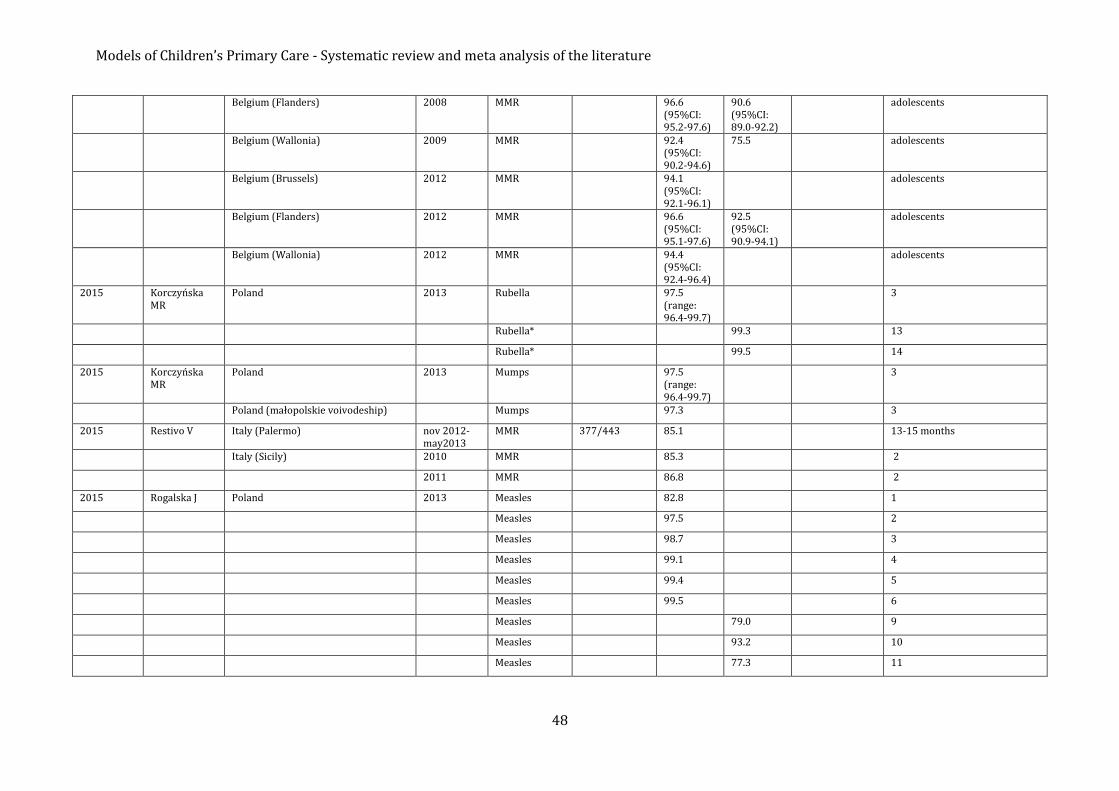
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
48
Belgium (Flanders) 2008 MMR 96.6 (95%CI: 95.2-97.6)
90.6 (95%CI: 89.0-92.2)
adolescents
Belgium (Wallonia) 2009 MMR 92.4 (95%CI: 90.2-94.6)
75.5 adolescents
Belgium (Brussels) 2012 MMR 94.1 (95%CI: 92.1-96.1)
adolescents
Belgium (Flanders) 2012 MMR 96.6 (95%CI: 95.1-97.6)
92.5 (95%CI: 90.9-94.1)
adolescents
Belgium (Wallonia) 2012 MMR 94.4 (95%CI: 92.4-96.4)
adolescents
2015 Korczyńska MR
Poland 2013 Rubella 97.5 (range: 96.4-99.7)
3
Rubella* 99.3 13
Rubella* 99.5 14
2015 Korczyńska MR
Poland 2013 Mumps 97.5 (range: 96.4-99.7)
3
Poland (małopolskie voivodeship) Mumps 97.3 3
2015 Restivo V Italy (Palermo) nov 2012-may2013
MMR 377/443 85.1 13-15 months
Italy (Sicily) 2010 MMR 85.3 2
2011 MMR 86.8 2
2015 Rogalska J Poland 2013 Measles 82.8 1
Measles 97.5 2
Measles 98.7 3
Measles 99.1 4
Measles 99.4 5
Measles 99.5 6
Measles 79.0 9
Measles 93.2 10
Measles 77.3 11

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
49
Measles 73.6 12
2015 Sandford H United Kingdom (England) 2007/08 MMR 2365400 mean: 75.1 (sd: 10.4; range: 39.0-89.0)
5
2008/09 MMR 2364700 mean: 78.0 (sd: 10.8; range: 32.0-91.5)
5
2009/10 MMR 2363700 mean: 82.7 (sd: 7.9; range: 49.3-93.8)
5
2010/11 MMR 2363800 mean: 84.2 (sd: 6.3; range: 61.0-95.1)
5
2014 Aasheim ET United Kingdom (England) 2012-2013 MMR 87.7 5
2014 Bystrom E Sweden (community near Stockholm) 2011 MMR 145 89.0 Not reported
2014 Lernout T Belgium 2012 MMR >=95.0 infants
Belgium (Flanders) 2005 MMR 62.0 13 months
Belgium (Flanders) 2005 MMR 94.0 (95%CI: 92.6-95.3)
18-24 months
Belgium (Flanders) 2008 MMR 69.0 13 months
Belgium (Flanders) 2008 MMR 96.6 (95%CI: 95.2-97.6)
18-24 months
Belgium (Flanders) 2012 MMR 72.0 13 months
Belgium (Flanders) 2012 MMR 96.6 (95%CI: 95.1-97.6)
18-24 months
2014 Rieck T Germany 2011 Measles 94.27 (95%CI: 94.19-94.35)
68.94 (95%CI: 68.78-69.09)
2
Germany 2011 Measles 96.65 (95%CI: 96.59-96.71)
82.34 (95%CI: 82.21-82.47)
3
Mumps 94.23 (95%CI: 94.15-94.31)
68.92 (95%CI: 68.76-69.07)
2

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
50
Mumps 96.61 (95%CI: 96.55-96.68)
82.32 (95%CI: 82.19-82.45)
3
Rubella 94.23 (95%CI: 94.15-94.31)
68.92 (95%CI: 68.77-69.07)
2
Rubella 96.61 (95%CI: 96.55-96.68)
82.32 (95%CI: 82.19-82.46)
3
2014 Robert E Belgium (Wallonia) May-July 2012
MMR 519 94.4 (95%CI: 92.4-96.4)
18-24 months
Belgium (Brussels) MMR 538 94.1 (95%CI: 92.1-96.1)
18-24 months
2014 Rogalska J Poland 2012 Rubella 97.9 (range: 96.4-99.7)
3
Rubella* 99.4 (range: 98.7-99.9)
13
Rubella* 99.4 (range: 98.6-100)
14
2014 Rogalska J Poland 2012 Mumps 97.9 (range: 96.4-99.7)
3
Poland (malopolskie voivodeship) Mumps 97.3 3
2014 Rogalska J Poland 2012 Measles 83.6 (range: 77.6-97.3)
1
Measles 97.9 2
Measles 98.9 3
Measles 99.3 4
Measles 99.5 5
Measles 99.6 6
Measles 76.6 9
Measles 94.7 10
Measles 96.7 11
2014 Simone B United Kingdom (England-London Borough (LB) and Local Authority outside London (LA))
01/04/2013 MMR 2407/6644 36.2 10-16
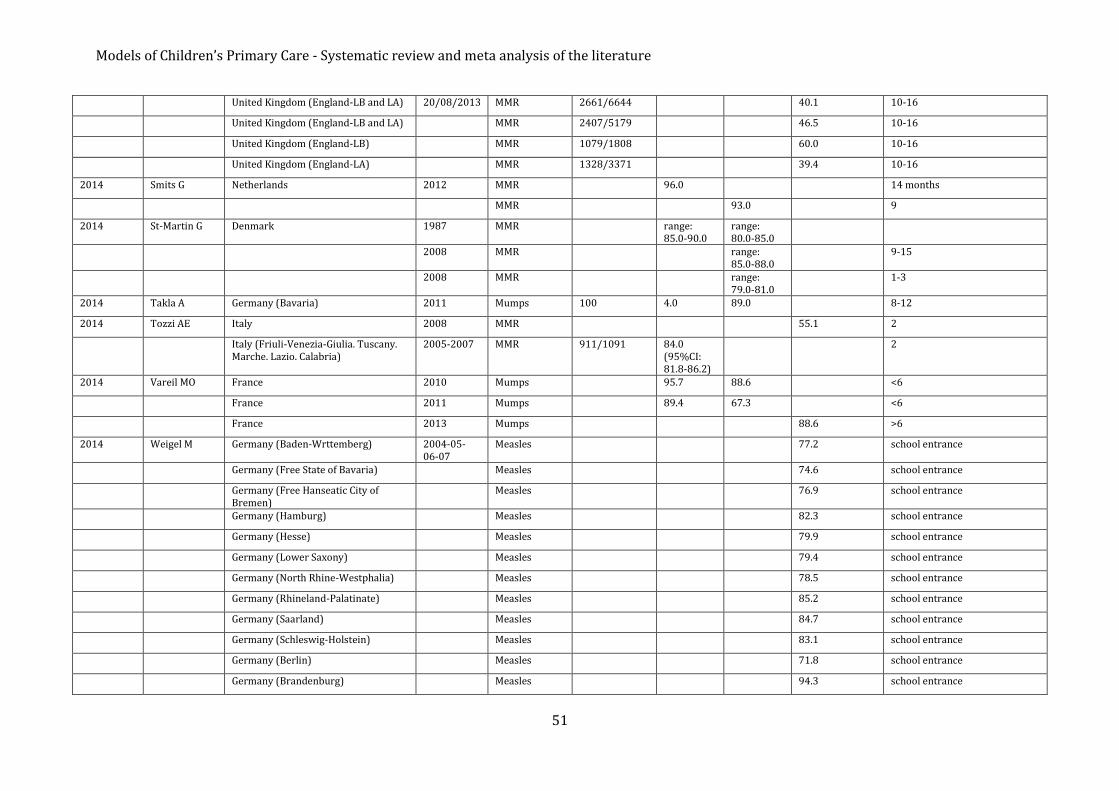
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
51
United Kingdom (England-LB and LA) 20/08/2013 MMR 2661/6644 40.1 10-16
United Kingdom (England-LB and LA) MMR 2407/5179 46.5 10-16
United Kingdom (England-LB) MMR 1079/1808 60.0 10-16
United Kingdom (England-LA) MMR 1328/3371 39.4 10-16
2014 Smits G Netherlands 2012 MMR 96.0 14 months
MMR 93.0 9
2014 St-Martin G Denmark 1987 MMR range: 85.0-90.0
range: 80.0-85.0
2008 MMR range: 85.0-88.0
9-15
2008 MMR range: 79.0-81.0
1-3
2014 Takla A Germany (Bavaria) 2011 Mumps 100 4.0 89.0 8-12
2014 Tozzi AE Italy 2008 MMR 55.1 2
Italy (Friuli-Venezia-Giulia. Tuscany. Marche. Lazio. Calabria)
2005-2007 MMR 911/1091 84.0 (95%CI: 81.8-86.2)
2
2014 Vareil MO France 2010 Mumps 95.7 88.6 <6
France 2011 Mumps 89.4 67.3 <6
France 2013 Mumps 88.6 >6
2014 Weigel M Germany (Baden-Wrttemberg) 2004-05-06-07
Measles 77.2 school entrance
Germany (Free State of Bavaria) Measles 74.6 school entrance
Germany (Free Hanseatic City of Bremen)
Measles 76.9 school entrance
Germany (Hamburg) Measles 82.3 school entrance
Germany (Hesse) Measles 79.9 school entrance
Germany (Lower Saxony) Measles 79.4 school entrance
Germany (North Rhine-Westphalia) Measles 78.5 school entrance
Germany (Rhineland-Palatinate) Measles 85.2 school entrance
Germany (Saarland) Measles 84.7 school entrance
Germany (Schleswig-Holstein) Measles 83.1 school entrance
Germany (Berlin) Measles 71.8 school entrance
Germany (Brandenburg) Measles 94.3 school entrance

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
52
Germany (Mecklenburg-Western Pomerania)
Measles 92.0 school entrance
Germany (Free State of Saxony) Measles not comparable (SIKO)
school entrance
Germany (Saxony-Anhalt) Measles 89.5 school entrance
Germany (Free State of Thuringia) Measles 93.3 school entrance
2013 Antona D France 1990s MMR range: 80.0-85.0
2
2002 MMR range: 93.0-96.0
school children
2008 MMR 96.6 11
2006 MMR 29.3 2
2010 MMR 60.9 2
2003 MMR 28.1 6
2006 MMR 45.1 6
2002 MMR 56.8 11
2005 MMR 74.2 11
2008 MMR 85.0 11
2004 MMR 65.7 15
2009 MMR 84.0 15
2010 MMR 89.1 60.9 2
2010 MMR 95.0 84.0 adolescents
2013 Fonteneau L France 2002-2003 Measles 4362 93.3 28.1 6
2002-2003 Mumps 4362 92.6 24.4 6
2002-2003 Rubella 4362 93.1 28.0 6
2005-2006 Measles 21346 93.7 (95%CI: 93.3-94.2)
45.1 (95%CI: 44.3-46.0)
6
2005-2006 Mumps 21346 91.4 (95%CI: 90.8-91.9)
43.2 (95%CI: 42.3-44.1)
6
2005-2006 Rubella 21346 91.4 (95%CI: 90.8-91.9)
43.3 (95%CI: 42.4-44.1)
6
2013 Karasek E Poland 2011 Rubella 98.1 (range:
3

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
53
96.7-99.8)
Rubella* 99.1 (range: 98.4-100)
12
2013 Knol M Netherlands 2012 MMR 96.0 2
2012 MMR 93.0 10
2013 Martinot A France 2008 MMR 60.3 24-35 month
2011 MMR 81.0 24-35 months
2013 Mayet A France 2008 MMR 89.1 40.6 2
2013 Pavlopoulou ID
Greece (Athens) Oct 2010-Nov 2011
MMR 660/704 (weighted)
90.5 2
MMR 20/56 (weighted)
35.9 60 months
MMR 462/731 (weighted)
63.7 5
2013 Poethko-Müller C
Germany 2010 Measles 91.5 (range: 87.6-95.3)
school entrance
2013 Smits G Netherlands 2011 MMR 96.0 93.0 Not reported
2013 Streng A Germany 2006 Measles 372 86.9 18-36 months
2011 Measles 302 91.1 18-36 months
2012 Bechini A Italy (Tuscany) 2003 MMR 87.0 2
2004 MMR 87.6 2
2006 MMR 91.2 2
2012 Bielicki JA Switzerland 2005-2007 Measles 62.6 (95%CI: 62.3-62.8)
13 months
2005-2007 Measles 84.5 (95%CI: 84.3-84.7)
59.4 (95%CI: 59.1-59.6)
25 months
2005-2007 Measles 85.7 (95%CI: 85.3-86.2)
66.7 (95%CI: 66.1-67.2)
24-35 months
2012 Bouhamam N France 2009-2010 MMR 375 77.0 9 months - 7years

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
54
2012 Delgado de Los Reyes J
Spain (Elche) 2011 MMR 96.4 1-2
MMR 90.4 3-7
2012 Fitzpatrick G Ireland 1999 MMR 77.0 2
2011 MMR 93.0 2
2012 Hug S Switzerland May 2009-Feb 2010
MMR 592 92.0 (95%CI: 90.0-94.0)
72.0 (95%CI: 69.0-76.0)
2
2012 Karasek E Poland 2010 Rubella* 99.2 13
2012 Karasek E Poland 2010 Measles 84.9 1
Measles 98.2 2
Measles 99.0 3
Measles 99.4 4
Measles 99.5 5
Measles 99.7 6
Measles 0.6 7
Measles 1.8 8
Measles 79.2 9
Measles 93.8 10
Measles 96.6 11
2012 Roggendorf H Germany 2007 Measles 95.0 88.0 5-6
Germany 2008 Measles 89.0 6
Germany (Essen) 2001 Measles 43.0 12
Germany (Essen) 2008 Measles 92.0 6
Germany (Essen) 2008 Measles 97.0 87.0 12
2012 Vainio K Norway 2011 MMR 93.0 2
2011 MMR 94.0 16
2011 Barrabeig I Spain (Barcelona-South Health Region)
01 Oct 2006-15 Jan 2007
MMR 1334 73.8 (range: 45.7-100)
27.3 months (median)
MMR 774/862 89.8 15 months - 4years
MMR 253/259 97.7 >=4

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
55
2011 Bassetti M Italy 2006 MMR 88.0 child
2011 Cockman P England 1992 MMR 92.0 2
2003 MMR 79.0 2
England (Tower Hamlets) 2011 MMR 94.0 2
2011 Khetsuriani N Croatia 2004 MMR 15042/18959 79.3 6
Ireland 2009 MMR 89034/125754 70.8 15-18
2011 Lang P Switzerland 2005-2007 Measles 8286 86.9 (95%CI: 85.9-87.9)
70.8 (95%CI: 69.3-72.2)
24-35 months
Mumps 8286 86.0 (95%CI: 85.0-87.0)
70.1 (95%CI: 68.6-71.5)
24-35 months
Rubella 8286 86.0 (95%CI: 85.0-87.0)
70.1 (95%CI: 68.7-71.6)
24-35 months
Measles 10314 89.9 (95%CI: 88.8-91.0)
75.2 (95%CI: 73.6-76.8)
8
Mumps 10314 88.8 (95%CI: 87.6-89.9)
74.2 (95%CI: 72.7-75.7)
8
Rubella 10314 88.7 (95%CI: 87.5-89.9)
73.8 (95%CI: 72.3-75.3)
8
Measles 9301 94.3 (95%CI: 93.6-95.0)
76.2 (95%CI: 74.9-77.6)
16
Mumps 9301 93.5 (95%CI: 92.7-94.2)
74.8 (95%CI: 73.5-76.2)
16
Rubella 9301 93.5 (95%CI: 92.7-94.2)
74.5 (95%CI: 73.1-75.8)
16
2011 Sabbe M Belgium (Brussels) 2000 MMR 74.5 18-24 months
Belgium (Wallonia) 2003 MMR 82.5 18-24 months
Belgium (Flanders) 2005 MMR 94.0 18-24 months
2005 MMR 83.6 14-16
Belgium (Brussels) 2006 MMR 91.1 18-24 months
2006 MMR 70.5 14-16

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
56
Belgium (Wallonia) 2006 MMR 89.0 18-24 months
2006 MMR 70.5 14-16
Belgium (Flanders) 2008 MMR 96.6 18-24 months
2008 MMR 90.6 14-16
Belgium (Wallonia) 2009 MMR 92.4 18-24 months
2009 MMR 75.5 18-24 months
2011 Sakou II Greece (Athens) 2009 MMR 911 93.1 (95%CI: 92.0-95.3)
11-19
MMR 381 95.7 11-14
MMR 529 91.5 14-19
2011 Siedler A Germany 2008 Measles 96.0 89.0 6
Germany (North Rhine–Westphalia) 2007-2008 Measles 88.4 10
Measles 87.2 11
Measles 85.2 12
Measles 83.2 13
Measles 82.0 14
Measles 82.1 15
Measles 79.7 16
Measles 77.1 17
Measles 73.3 18
2011 Stanescu A Romania 2000-2008 Measles range: 97.0-98.0
18-24 months
Measles range: 96.0-98.0
7
2009 MMR 85.1 (95%CI: 82.4-87.8)
1
MMR 95.0 (95%CI: 93.4-95.8)
18 months
2010 Measles 93.4 (95%CI: 90.7-95.0)
7

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
57
2011 Wadl M Germany 2008 Measles 89.0 (range: 85-94)
first graders
Germany (four Bavarian counties) 2006-2007 Measles 69.0 (range: 64-72)
first graders
2011 Zimmerman L Poland 2006 Rubella* 99.2 15
2005 MMR 91.0 3
2008 MMR 98.0 3
2010 Bätzing-Feigenbaum J
Germany 2001 MMR 91.4 25.9 school entrance
2002 MMR 91.3 33.1 school entrance
2003 MMR 92.5 50.9 school entrance
2004 MMR 93.3 65.7 school entrance
2005 MMR 94 76.6 school entrance
2006 MMR 94.5 83.2 school entrance
2007 MMR 95.4 88.4 school entrance
2008 MMR 95.9 91.3 school entrance
Germany (Berlin) 2001 MMR 91.2 24 school entrance
2004 MMR 93.4 71.7 school entrance
2005 MMR 93.5 78.8 school entrance
2006 MMR 93.8 83.6 school entrance
2007 MMR 94.5 86.8 school entrance
2008 MMR 95.2 88.2 school entrance
2010 Cova M Italy 2003 MMR 84.0 2
2006 MMR 90.0 2
Italy (Ferrara) 2008 MMR 96.7 2
2008 MMR 91.1 6
2010 Curtale F Italy 2003 MMR 82.0 2
2007 MMR 89.6 2
Italy (Lazio) 2003 MMR 83.9 2
2003 MMR 53.0 6-13

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
58
2003 MMR 14.0 15
2007 MMR 90.7 2
2007 MMR 67.0 6-13
2007 MMR 42.0 15
2010 Jeannot E Switzerland (Geneva) 2003 Measles 3542 65.4 5-6
Mumps 3542 63.2 5-6
Rubella 3542 63.9 5-6
2004 Measles 3679 75.4 5-6
Mumps 3679 73.4 5-6
Rubella 3679 73.6 5-6
2005 Measles 3425 85.2 5-6
Mumps 3425 82.7 5-6
Rubella 3425 83.6 5-6
2006 Measles 3374 87.3 5-6
Mumps 3374 84.9 5-6
Rubella 3374 86.2 5-6
2007 Measles 3164 89.4 5-6
Mumps 3164 87.9 5-6
Rubella 3164 88.5 5-6
2010 Lashkari HP United Kingdom (Haringey. London) 2006 MMR 373 36.0 (95%CI: 31.0-41.0)
55.0 (95%CI: 50.0-60.0)
14.7
2010 Parent du Châtelet I
France 2007 MMR 90.0 2
2004-2005 MMR 96.0 74.0 11
2005-2006 MMR 93.0 44.0 6
2010 Reuss AM Germany 2006 MMRV 281/415078 <1 2
2006 MMRV 95/415078 <1 2
2007 MMRV 16642/404988 4.0 2
2007 MMRV 21718/404988 5.0 2

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
59
2010 Stronegger WJ Austria Not reported
Measles 658 88.4 6.5
Measles 688 84.9 9.6
Measles 1040 76.8 13.1
Measles 2386 82.4 6-13
2009 Borràs E Spain (Catalonia. public health care) Oct 2003-Sept2004
MMR 428/431 99.3 (95%CI: 97.8-99.8)
15 month
Spain (Catalonia. private health care) MMR 192/196 98.0 (95%CI: 94.8-99.4)
15 month
2009 Poethko-Müller C
Germany May 2003-May2006
Measles 14826 93.6 (95%CI: 93.0-94.2)
2-17
2009 Richard JL Switzerland 2000 MMR 82.0 2
2005-2007 MMR 87.0 (range: 73.0-94.0)
2
2005-2007 MMR 90.0 71.0 8
2005-2007 MMR 94.0 76.0 16
2009 Schönberger K Germany 2116 46.8 (95%CI: 44.5-49.1)
15 month
2009 Theeten H Belgium (Flanders) 2005 MMR 792 88.0 (95%CI: 85.6-90.4)
7-8
2008 Andrews N Belgium 2001-2001 Measles 3374 80.0 2
Bulgaria 2001-2001 Measles 1666 93.0 2
Cyprus 2001-2001 Measles 2901 88.0 2
Czech Republic 2001-2001 Measles 3013 96.0 2
England and Wales 2001-2001 Measles 3570 88.0 2
Hungary 2001-2001 Measles 3490 100 2
Ireland 2001-2001 Measles 2590 77.0 2
Latvia 2001-2001 Measles 3026 97.0 2
Lithuania 2001-2001 Measles 3352 97.0 2
Luxembourg 2001-2001 Measles 2679 91.0 2

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
60
Malta 2001-2001 Measles 1867 90.0 2
Romania 2001-2001 Measles 3839 98.0 2
Slovakia 2001-2001 Measles 3640 99.0 2
Slovenia 2001-2001 Measles 3399 92.0 2
Spain 2001-2001 Measles 3605 94.0 2
Sweden 2001-2001 Measles 1392 94.0 2
2008 Choi YH England 2004 MMR 1663 n=1343 (80.8)
n=0 (0.0) 2-4
MMR 3582 n=627 (17.5)
n=2684 (74.9)
5-10
MMR 3656 n=826 (22.6)
n=2619 (71.6)
11-17
2008 Gagneur A France 2004 MMR 87.0 2
2008 Mikolajczyk RT
Germany (Bavaria) 2004-2005 MMR 1481 93.0 5-6
2008 Nardone A Belgium 1999 Rubella 82.0 infants
Bulgaria 1999-2003 Rubella 93.0 infants
Cyprus 1999-2003 Rubella 86.0 infants
Czech Republic 1999. 2001. 2003
Rubella 97.0 infants
England and Wales 1999-2003 Rubella 85.0 infants
Hungary 1999. 2001. 2003
Rubella 100 infants
Ireland 1999-2003 Rubella 76.0 infants
Latvia 1999-2003 Rubella 97.0 infants
Lithuania 1999-2003 Rubella 97.0 infants
Malta 1999-2003 Rubella 74.0 infants
Slovakia 1999-2003 Rubella 99.0 infants
Slovenia 1999-2003 Rubella 93.0 infants
Sweden 1999-2002 Rubella 92.0 infants
2008 Paulo AC Spain (La Rioja) 2005-2006 Measles 96.3 15 months

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
61
2008 Rota MC Italy 2004 MMR 85.1 2-4
MMR 78.3 5-9
MMR 59.2 10-14
2008 Vandermeulen C
Belgium (Flanders) 2005 MMR 1349 94.0 (95%CI: 92.6-95.3)
toddlers (mean age 1.67)
MMR 792 88.0 (95%CI: 85.6-90.4)
primary school children (mean age 7.8)
MMR 1344 80.6 (95%CI: 78.2-83.0)
83.6 (95%CI: 81.4-85.8)
adolescents (mean age 13.9)
2007 Guagliardo V France (South-Eastern) 2002-2003 MMR 2460 86.4 4
2007 Mixer RE United Kingdom (Brent. London) dic-03 MMR 6444 75.0 (95%CI: 74.0-75.1)
13 months - 3 years
2007 Sonnenberg P England 2004 MMR 81.0 2
2007 Tischer A Switzerland (Grabs) 2003 MMR 91 35.2 64.8 14.5
2004 MMR 75 21.3 78.7 14.5
2006 Heininger U Germany (Erlangen) 2002 Measles 1672 96.1 76.3 10-18
Mumps 1672 95.6 74.2 10-18
Rubella 1672 89.4 60.2 10-18
2006 Heininger U Switzerland 2001 Measles 449/505 88.9 7
Mumps 443/505 87.7 7
Rubella 440/505 87.1 7
Measles 135/269 50.2 7
Mumps 135/269 50.2 7
Rubella 135/269 50.2 7
Measles 75.0 2
Measles 82.0 3
Measles 86.0 4
Measles 88.0 19.0 7
Measles 505 33.0 10
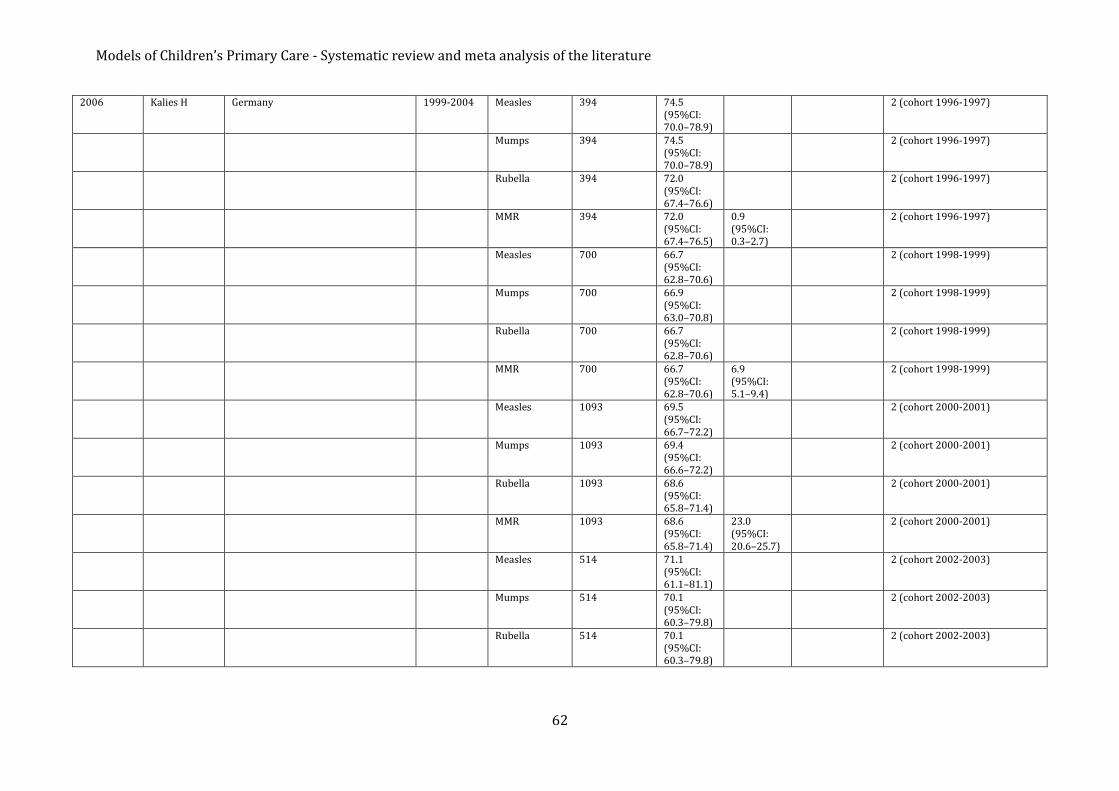
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
62
2006 Kalies H Germany 1999-2004 Measles 394 74.5 (95%CI: 70.0–78.9)
2 (cohort 1996-1997)
Mumps 394 74.5 (95%CI: 70.0–78.9)
2 (cohort 1996-1997)
Rubella 394 72.0 (95%CI: 67.4–76.6)
2 (cohort 1996-1997)
MMR 394 72.0 (95%CI: 67.4–76.5)
0.9 (95%CI: 0.3–2.7)
2 (cohort 1996-1997)
Measles 700 66.7 (95%CI: 62.8–70.6)
2 (cohort 1998-1999)
Mumps 700 66.9 (95%CI: 63.0–70.8)
2 (cohort 1998-1999)
Rubella 700 66.7 (95%CI: 62.8–70.6)
2 (cohort 1998-1999)
MMR 700 66.7 (95%CI: 62.8–70.6)
6.9 (95%CI: 5.1–9.4)
2 (cohort 1998-1999)
Measles 1093 69.5 (95%CI: 66.7–72.2)
2 (cohort 2000-2001)
Mumps 1093 69.4 (95%CI: 66.6–72.2)
2 (cohort 2000-2001)
Rubella 1093 68.6 (95%CI: 65.8–71.4)
2 (cohort 2000-2001)
MMR 1093 68.6 (95%CI: 65.8–71.4)
23.0 (95%CI: 20.6–25.7)
2 (cohort 2000-2001)
Measles 514 71.1 (95%CI: 61.1–81.1)
2 (cohort 2002-2003)
Mumps 514 70.1 (95%CI: 60.3–79.8)
2 (cohort 2002-2003)
Rubella 514 70.1 (95%CI: 60.3–79.8)
2 (cohort 2002-2003)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
63
MMR 514 70.1 (95%CI: 60.2–79.4)
20.2 (95%CI: 13.7–29.1)
2 (cohort 2002-2003)
2006 Rota MC Italy 2004 MMR 85.5 2
2005 MMR 88.3 2
2005 MMR 83.0 6-10
2006 Wichmann O Germany (Duisburg) 2002 Measles 90.0 29.0 school entrance
2004 Measles 92.0 70.0 school entrance
2006 Measles 431 95.0 74.0 10-12
2006 Measles 361 95.0 65.0 13-15
2006 Measles 67 94.0 58.0 16-18
2006 Measles 859 95.4 70.4 10-18
2005 Stampi S Italy (Emilia Romagna) 1998 Measles 29662 88.2 2
Rubella* 29662 85.2 2
Measles 83.8 13
Rubella* 85.2 13
1999 Measles 30916 89.1 2
Mumps 30916 84.2 2
Rubella 30916 88.0 2
Measles 89.1 13
Rubella 60.8 13
2000 Measles 31727 90.4 2
Mumps 31727 89.4 2
Rubella 31727 89.4 2
Measles 84.9 13
Rubella 66.3 13
2001 Measles 32866 90.7 2
Mumps 32866 90.1 2
Rubella 32866 90.1 2
Measles 87.4 13
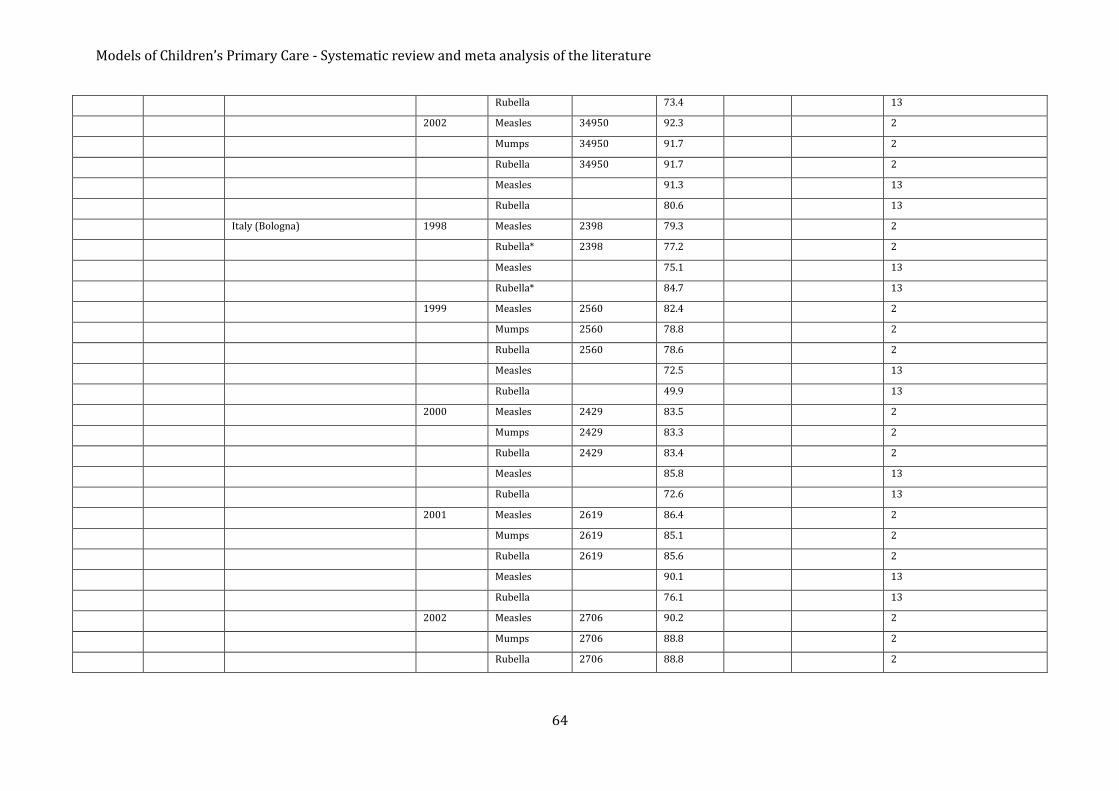
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
64
Rubella 73.4 13
2002 Measles 34950 92.3 2
Mumps 34950 91.7 2
Rubella 34950 91.7 2
Measles 91.3 13
Rubella 80.6 13
Italy (Bologna) 1998 Measles 2398 79.3 2
Rubella* 2398 77.2 2
Measles 75.1 13
Rubella* 84.7 13
1999 Measles 2560 82.4 2
Mumps 2560 78.8 2
Rubella 2560 78.6 2
Measles 72.5 13
Rubella 49.9 13
2000 Measles 2429 83.5 2
Mumps 2429 83.3 2
Rubella 2429 83.4 2
Measles 85.8 13
Rubella 72.6 13
2001 Measles 2619 86.4 2
Mumps 2619 85.1 2
Rubella 2619 85.6 2
Measles 90.1 13
Rubella 76.1 13
2002 Measles 2706 90.2 2
Mumps 2706 88.8 2
Rubella 2706 88.8 2

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
65
Measles 92.6 13
Rubella 84.2 13
2005 van der Wal MF
Netherlands (Amsterdam) 2003 MMR 57374 93.9 5-12
2004 Alfredsson R Sweden (Göteborg) 1999 MMR 9726 98.0 18 months
2004 Ciofi degli Atti ML
Italy 2003 Measles 76.9 (95%CI: 74.9–79.0)
2-3
2004 Dannetun E Sweden (Ostergotland) 2000 MMR 1171/1316 88.9 2
Sweden (Ostergotland) 2001 MMR 1012/1262 80.2 2
Sweden (Ostergotland) 2002 MMR 1076/1293 83.2 2
Sweden (Ostergotland) 2001 MMR 1232/1316 93.6 3
Sweden (Ostergotland) 2002 MMR 1137/1262 90.1 3
Sweden (Ostergotland) 2002 MMR 1249/1316 94.9 4
2004 Henderson R United Kingdom (Highland. Scotland) Oct 2001-Sept 2002
MMR 1700/2108 80.6 2
2004 Vandermeulen C
Belgium (Bruges) giu-96 MMR 1675/1825 91.8 3-12
2003 Centers Disease Control Prevention
Italy (Campania) 2001 Measles 41888 65.0 <=3
2003 Nardone A Denmark 1990 MMR 84.0 2
1991 MMR 86.0 2
1992 MMR 85.0 2
1993 MMR 81.0 2
1994 MMR 88.0 2
1995 MMR 88.0 2
1996 MMR 85.0 2
1997 MMR 84.0 2
1998 MMR 88.0 2
England and Wales 1990 MMR 86.0 2
1991 MMR 90.0 2
1992 MMR 92.0 2

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
66
1993 MMR 91.0 2
1994 MMR 91.0 2
1995 MMR 92.0 2
1996 MMR 92.0 2
1997 MMR 91.0 2
1998 MMR 88.0 2
France 1990 MMR 54.0 2
1991 MMR 52.0 2
1992 MMR 62.0 2
1993 MMR 80.0 3-4
1994 MMR 84.0 3-4
1995 MMR 85.0 3-4
1996 MMR 88.0 3-4
1997 MMR 89.0 3-4
1998 MMR 91.0 3-4
Netherlands 1990 MMR 95.0 2
1991 MMR 94.0 2
1992 MMR 94.0 2
1993 MMR 95.0 2
1994 MMR 94.0 2
1995 MMR 94.0 2
1996 MMR 94.0 2
1997 MMR 96.0 2
1998 MMR 96.0 2
2002 Bonanni P Italy 1998 Measles 56.0 12-24 months
Italy (Piedmont) 1998 Measles 60.4 (95%CI: 50.4–70.3)
12-24 months
Italy (Val D'Aosta) Measles 43.3 (95%CI: 31.2–56.0)
12-24 months
Italy (Lombardy) Measles 75.9 (95%CI: 68.1–83.7)
12-24 months

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
67
Italy (Milan) Measles 74.6 (95%CI: 62.5–84.1)
12-24 months
Italy (Boizano) Measles 28.1 (95%CI: 18.7–37.4)
12-24 months
Italy (Trento) Measles 58.0 (95%CI: 48.2–67.7)
12-24 months
Italy (Veneto) Measles 81.2 (95%CI: 75.4–87.0)
12-24 months
Italy (Friuli–Venezia) Measles 77.3 (95%CI: 68.9–85.7)
12-24 months
Italy (Liguria) Measles 62.1 (95%CI: 52.9–71.4)
12-24 months
Italy (Emilia) Measles 87.7 (95%CI: 81.1–94.3)
12-24 months
Italy (Tuscany) Measles 64.8 (95%CI: 55.5–74.2)
12-24 months
Italy (Umbria) Measles 72.3 (95%CI: 64.6–81.0)
12-24 months
Italy (Marches) Measles 58.7 (95%CI: 48.7–68.7)
12-24 months
Italy (Abruzzi) Measles 45.5 (95%CI: 38.5–51.9)
12-24 months
Italy (Molise) Measles 40.5 (95%CI: 29.6–51.4)
12-24 months
Italy (Campania) Measles 26.5 (95%CI: 17.3–35.7)
12-24 months
Italy (Naples) Measles 39.8 (95%CI: 29.2–51.1)
12-24 months
Italy (Puglia) Measles 50.6 (95%CI: 41.0–60.2)
12-24 months
Italy (Basilicata) Measles 44.7 (95%CI: 33.2–56.1)
12-24 months
Italy (Calabria) Measles 25.5 (95%CI: 17.0–33.9)
12-24 months
Italy (Sicily) Measles 44.6 (95%CI: 34.3–54.8)
12-24 months
Italy (Sardinia) Measles 56.3 (95%CI: 46.8–65.7)
12-24 months
2002 Siedler A Germany 1999 Measles 782 21.7 (95%CI: 18.0-25.3)
15 months
Measles 782 77.0 (95%CI: 72.7-81.4)
2
Measles 782 87.6 3

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
68
2002 Vellinga A Belgium (Flanders) 1999 MMR 1005 83.4 (95%CI: 80.3-86.5)
18-24 months
2000 Hanratty B United Kingdom 1994 Measles & Rubella (MR)
8 million 92 5-16
2000 Janaszek W Poland 1997 Measles 96.9 24-35 months
2000 Mossong J Luxembourg (Reuler) 1996 Measles 227/297 76.4 primary school (4-12)
Luxembourg (Wincrange) Measles 211/302 69.9 primary school (4-12)
* Girls only

69
References NICE, Autism in under 19s: recognition, referral and diagnosis, Clinical guideline, 2011.
Kanner L., Autistic disturbances of affective contact, Nerv. Child, 2: 217–250, 1943.
Asperger H., Die Autistischen psychopathen im kindesalter, Archives of Psychiatry and
Neurological Sciences, 117: 76–136, 1944.
Baker J.P., Autism at 70-redrawing the boundaries, The New England Journal of Medicine,
369(12): 1089–1091, 2013.
American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, third
ed. (DSM-III), American Psychiatric Association, Washington, DC, 1980.
American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, third
ed. revised (DSM-III-R), American Psychiatric Association, Washington, DC, 1987.
American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, forth
ed. (DSM-IV), American Psychiatric Association, Arlington, VA, 1994.
American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, forth
ed. text revised (DSM-IV-TR), American Psychiatric Association, Arlington, VA, 2000.
American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, fifth
ed. (DSM-V), American Psychiatric Association, Arlington, VA, 2013.
ICD-10 Version 2015 www.apps.who.int/classifications/icd10/browse/2015/en
Elsabbagh M. et al., Global Prevalence of Autism and Other Pervasive Developmental Disorders,
Autism Research, 5: 160–179, 2012.
Bland J. Clements J. Protecting the world’s children: the story of WHO’s immunization
programme, World Health Forum 1998;19: 162–172.
WHO Weekly epidemiological record, No.46, 2015, 90, 617-632.
Administrative data reported to WHO and UNICEF annually are available from:
http://www.who.int/immunization/monitoring_surveillance/data/administrative_
coverage.xls; accessed October 2015.
Global Vaccine Action Plan- Strategic Advisory Group of Experts on Immunization, 2014
Assessment Report of the Global Vaccine Action Plan. Available at
http://www.who.int/immunization/global_vaccine_action_plan/SAGE_DoV_GVAP_As-
sessment_report_2014_English.pdf?ua=1; accessed October 2015.
European Vaccine Action Plan 2015-2020 (EVAP). Available at
http://www.euro.who.int/__data/assets/pdf_file/0007/255679/WHO_EVAP_UK_v30_WEBx.pdf
?ua=1; accessed February 2016.

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
70
European Centre for Disease Prevention and Control available from:
http://ecdc.europa.eu/en/Pages/home.aspx; accessed 17 February 2016.

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
71
References for systematic review – appendix 1. Ferrante M. et al., Prevalence and age at diagnosis of Autism Spectrum Disorder in south Italy,
2004–2014 , The European Journal of Public Health, Vol. 25 Issue suppl 3, 2015.
Salomone E. et al., Child’s verbal ability and gender are associated with age at diagnosis in a
sample of young children with ASD in Europe, Child: care, health and development, 42(1): 141-
145, 2015.
Mouridsen S.E. et al., The Sex Ratio of Full and Half Siblings of People Diagnosed with an Autism
Spectrum Disorder: A Danish Nationwide Register Study, Child Psychiatry & Human
Development, 45:493-499, 2014.
Hathorn C. et al., Impact of Adherence to Best Practice Guidelines on the Diagnostic and
Assessment Services for Autism Spectrum Disorder, Journal of Autism and Developmental
Disorders, 44: 1859-1866, 2014.
Jensen C.M. et al., Time Trends Over 16 Years in Incidence-Rates of Autism Spectrum Disorders
Across the Lifespan Based on Nationwide Danish Register Data, Journal of Autism and
Developmental Disorders, 44: 1808-1818, 2014.
Stagg S.D. et al., Investigating eye movement patterns, language, and social ability in children
with autism spectrum disorder, Development and Psychopathology, 26:529–537, 2014.
Jokiranta E. et al., Parental psychiatric disorders and autism spectrum disorders, Psychiatry
Research, 207(3): 203-211, 2013.
van der Ven E. et al., An incidence study of diagnosed autism-spectrum disorders among
immigrants to the Netherlands, Acta Psychiatrica Scandinavica, 128:54-60, 2013.
Visser J.C. et al., Narrowly Versus Broadly Defined Autism Spectrum Disorders: Differences in
Pre- and Perinatal Risk Factors, Journal of Autism and Developmental Disorders, 43: 1505-1516,
2013.
Begeer S. et al., Sex Differences in the Timing of Identification Among Children and Adults with
Autism Spectrum Disorders, Journal of Autism and Developmental Disorders, 43: 1151-1156,
2013.
Campbell M. et al., Autism in Glasgow: cumulative incidence and the effects of referral age,
deprivation and geographical location, Child: care, health and development, 39(5): 688–694,
2013.
Ververi A. et al., Clinical and Laboratory Data in a Sample of Greek Children with Autism
Spectrum Disorders, Journal of Autism and Developmental Disorders, 42: 1470-1476, 2012.
Chamak B. et al., The autism diagnostic experiences of French parents, Autism, 15(1): 83-97,
2011.
Noterdaeme M. and Hutzelmeyer-Nickels A., Early symptoms and recognition of pervasive
developmental disorders in Germany, ASD and PDD, 14(6): 575-588, 2010.

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
72
Oosterling I.J. et al., Advancing early detection of autism spectrum disorder by applying an
integrated two-stage screening approach, Journal of Child Psychology and Psychiatry, 51(3):
250-258, 2010.
Williams E. et al., Prevalence and characteristics of autistic spectrum disorders in the ALSPAC
cohort, Dev Med Child Neurol., 50(9): 672-7, 2008.
Latif A.H.A. and Williams W.R., Diagnostic trends in autistic spectrum disorders in the South
Wales valleys, Autism, 11(6): 479-487, 2007.
Mouridsen S.E. et al., Autoimmune diseases in parents of children with infantile autism: a case–
control study, Developmental Medicine & Child Neurology, 49: 429-432, 2007.
Oslejskova H. et al., The course of diagnosis in autistic patients: the delay between recognition of
the first symptoms by parents and correct diagnosis, Neuroendocrinology Letters, 28(6): 895-
900, 2007.
Renty J. and Roeyers H., Satisfaction with formal support and education for children with autism
spectrum disorder: the voices of the parents, Child: Care, Health & Development, 32(3): 371-
358, 2006.
Maestro S. et al., Course of Autism Signs in the First Year of Life, Psychopathology, 38: 26-31,
2005.
Larsson H.J. et al., Risk Factors for Autism: Perinatal Factors, Parental Psychiatric History, and
Socioeconomic Status, American Journal of Epidemiology, 161(10): 916-925, 2005.
Chakrabarti S. and Fombonne E., Pervasive Developmental Disorders in Preschool Children:
Confirmation of High Prevalence, American Journal of Psychiatry, 162: 1133-1141, 2005.
Pry R. et al., The relationship between expressive language level and psychological development
in children with autism 5 years of age, Autism, 9(2): 179-189, 2005.
Sturm H. et al., Autism spectrum disorders in children with normal intellectual levels: associated
impairments and subgroups, Developmental Medicine & Child Neurology, 46: 444-447, 2004.
Smeeth L. et al., MMR vaccination and pervasive developmental disorders: a case-control study,
Lancet, 364: 963-69, 2004.
Tebruegge M. et al., Does routine child health surveillance contribute to the early detection of
children with pervasive developmental disorders? – An epidemiological study in Kent, U.K., BMC
Pediatrics, 4:4, 2004.
Boddaert N. et al., Perception of Complex Sounds in Autism: Abnormal Auditory Cortical
Processing in Children, American Journal of Psychiatry, 161: 2117-2120, 2004.
Cederlund M. and Gillberg C., One hundred males with Asperger syndrome: a clinical study of
background and associated factors, Developmental Medicine & Child Neurology, 46: 652-660,
2004.
Keen D. and Ward S., Autistic spectrum disorder-A child population profile, Autism, 8(1): 39-48,
2004.

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
73
Lingam R. et al., Prevalence of autism and parentally reported triggers in a north east London
population, Archives of Disease in Childhood, 88: 666-670, 2003.
Hultman C.M. et. al., Perinatal Risk Factors for Infantile Autism, Epidemiology, 13: 417-423,
2002.
Madsen K.M. et al., A Population-Based Study of Measles, Mumps, and Rubella Vaccination and
Autism, The New England Journal of Medicine, 347: 1477-1482, 2002.
Maestro S. et al., Early Behavioral Development in Autistic Children: The First 2 Years of Life
through Home Movies, Psychopathology, 34: 147–152, 2001.
Rasmussen P. et al., Autistic disorders in Down syndrome: background factors and clinical
correlates, Developmental Medicine & Child Neurology, 43: 750-754, 2001.
Magnùsson P. et al., Prevalence of Autism in Iceland, Journal of Autism and Developmental
Disorders, 31(2): 153-163, 2001.
Powell J.E. et al., Changes in the incidence of childhood autism and other autistic spectrum
disorders in preschool children from two areas of the West Midlands, UK, Developmental
Medicine & Child Neurology , 42: 624–628, 2000.

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
74
References for systematic review – appendix 2. Amendola A, Bubba L, Piralla A, Binda S, Zanetti A, Pariani E, Ranghiero A, Premoli M,
Pellegrinelli L, Coppola L, Gramegna M, Baldanti F, Zanetti A. Surveillance and vaccination
coverage of measles and rubella in Northern Italy. Hum Vaccin Immunother. 2015;11(1):206-13
Cozza V, Martinelli D, Cappelli MG, Tafuri S, Fortunato F, Prato R. Further efforts in the
achievement of congenital rubella syndrome/rubella elimination. Hum Vaccin Immunother.
2015;11(1):220-4
Giambi C, Filia A, Rota MC, Del Manso M, Declich S, Nacca G, Rizzuto E, Bella A; regional contact
points for rubella. Congenital rubella still a public health problem in Italy: analysis of national
surveillance data from 2005 to 2013. Euro Surveill. 2015 Apr 23;20(16)
Gross K, Hartmann K, Zemp E, Merten S. 'I know it has worked for millions of years': the role of
the 'natural' in parental reasoning against child immunization in a qualitative study in
Switzerland. BMC Public Health. 2015 Apr 12;15:373
Hens N, Abrams S, Santermans E, Theeten H, Goeyvaerts N, Lernout T, Leuridan E, Van
Kerckhove K, Goossens H, Van Damme P, Beutels P. Assessing the risk of measles resurgence in
a highly vaccinated population: Belgium anno 2013. Euro Surveill. 2015 Jan 8;20(1)
Korczyńska MR, Paradowska-Stankiewicz I. Rubella in Poland in 2013. Przegl Epidemiol.
2015;69(2):213-8, 341-3
Korczyńska MR, Rogalska J. Mumps in Poland in 2013. Przegl Epidemiol. 2015;69(2):209-12,
339-40
Restivo V, Napoli G, Marsala MG, Bonanno V, Sciuto V, Amodio E, Calamusa G, Vitale F, Firenze A.
Factors associated with poor adherence to MMR vaccination in parents who follow vaccination
schedule. Hum Vaccin Immunother. 2015;11(1):140-5
Rogalska J. Measles in Poland in 2013. Przegl Epidemiol. 2015;69(2):205-7, 335-8. English,
Polish. Erratum in: Przegl Epidemiol. 2015;69(3):452. Przegl Epidemiol. 2015;69(3):478
Sandford H, Tata LJ, Browne I, Pritchard C. Is there an association between the coverage of
immunisation boosters by the age of 5 and deprivation? An ecological study. Vaccine. 2015 Feb
25;33(9):1218-22
Aasheim ET, Inns T, Trindall A, Emmett L, Brown KE, Williams CJ, Reacher M. Outbreak of
mumps in a school setting, United Kingdom, 2013. Hum Vaccin Immunother. 2014;10(8):2446-9
Byström E, Lindstrand A, Likhite N, Butler R, Emmelin M. Parental attitudes and decision-
making regarding MMR vaccination in an anthroposophic community in Sweden--a qualitative
study. Vaccine. 2014 Nov 28;32(50):6752-7
Lernout T, Theeten H, Hens N, Braeckman T, Roelants M, Hoppenbrouwers K, Van Damme P.
Timeliness of infant vaccination and factors related with delay in Flanders, Belgium. Vaccine.
2014 Jan 3;32(2):284-9

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
75
Rieck T, Feig M, Eckmanns T, Benzler J, Siedler A, Wichmann O. Vaccination coverage among
children in Germany estimated by analysis of health insurance claims data. Hum Vaccin
Immunother. 2014;10(2):476-84
Robert E, Dramaix M, Swennen B. Vaccination coverage for infants: cross-sectional studies in
two regions of Belgium. Biomed Res Int. 2014;2014:838907
Rogalska J. Rubella in Poland in 2012. Przegl Epidemiol. 2014;68(2):195-9, 319-21
Rogalska J, Paradowska-Stankiewicz I. Mumps in Poland in 2012. Przegl Epidemiol.
2014;68(2):191-3, 317-8
Rogalska J, Karasek E, Paradowska-Stankiewicz I. Measles in Poland in 2012. Przegl Epidemiol.
2014;68(2):187-90, 313-6
Simone B, Balasegaram S, Gobin M, Anderson C, Charlett A, Coole L, Maguire H, Nichols T,
Rawlings C, Ramsay M, Oliver I. Evaluation of the measles, mumps and rubella vaccination
catch-up campaign in England in 2013. Vaccine. 2014 Aug 6;32(36):4681-8
Smits G, Mollema L, Hahné S, de Melker H, Tcherniaeva I, van der Klis F, Berbers G.
Seroprevalence of rubella antibodies in The Netherlands after 32 years of high vaccination
coverage. Vaccine. 2014 Apr 1;32(16):1890-5
St-Martin G, Knudsen LK, Engsig FN, Panum I, Andersen PH, Rønn J, Fonager J, Fischer TK.
Mumps resurgence in Denmark. J Clin Virol. 2014 Nov;61(3):435-8
Takla A, Böhmer MM, Klinc C, Kurz N, Schaffer A, Stich H, Stöcker P, Wichmann O, Koch J.
Outbreak-related mumps vaccine effectiveness among a cohort of children and of young adults
in Germany 2011. Hum Vaccin Immunother. 2014;10(1):140-5
Tozzi AE, Piga S, Corchia C, Di Lallo D, Carnielli V, Chiandotto V, Fertz MC, Miniaci S, Rusconi F,
Cuttini M. Timeliness of routine immunization in a population-based Italian cohort of very
preterm infants: results of the ACTION follow-up project. Vaccine. 2014 Feb 7;32(7):793-9
Vareil MO, Rouibi G, Kassab S, Soula V, Duffau P, Lafon ME, Neau D, Cazanave C. Epidemic of
complicated mumps in previously vaccinated young adults in the South-West of France. Med
Mal Infect. 2014 Dec;44(11-12):502-8
Weigel M, Weitmann K, Rautmann C, Schmidt J, Bruns R, Hoffmann W. Impact of physicians'
attitude to vaccination on local vaccination coverage for pertussis and measles in Germany. Eur
J Public Health. 2014 Dec;24(6):1009-16
Antona D, Lévy-Bruhl D, Baudon C, Freymuth F, Lamy M, Maine C, Floret D, Parent du Chatelet I.
Measles elimination efforts and 2008-2011 outbreak, France. Emerg Infect Dis. 2013
Mar;19(3):357-64
Fonteneau L, Urcun JM, Guthmann JP, Collet M, Neulat N, Bristol-Gauzy P, Guignon N, Lévy-Bruhl
D, Herbet JB. [Vaccination coverage in 6-year-old preschool children, France, 2005-2006]. Arch
Pediatr. 2013 Mar;20(3):241-7
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
76
Karasek E, Paradowska-Stankiewicz I. Rubella in Poland in 2011. Przegl Epidemiol.
2013;67(2):189-93, 313-5
Knol M, Urbanus A, Swart E, Mollema L, Ruijs W, van Binnendijk R, Te Wierik M, de Melker H,
Timen A, Hahne S. Large ongoing measles outbreak in a religious community in the Netherlands
since May 2013. Euro Surveill. 2013 Sep 5;18(36)
Martinot A, Cohen R, Denis F, Gaudelus J, Lery T, Le Danvic M, Stahl JP. [Annual trends (2008-
2011) in early childhood vaccination coverage for the French population: the Vaccinoscopie(®)
study]. Arch Pediatr. 2013 Aug;20(8):837-44
Mayet A, Genicon C, Duron S, Haus-Cheymol R, Ficko C, Bédubourg G, Laporal S, Trichereau J,
Meynard JB, Deparis X, Migliani R. The measles outbreak in the French military forces--2010-
2011: results of epidemiological surveillance. J Infect. 2013 Mar;66(3):271-7
Pavlopoulou ID, Michail KA, Samoli E, Tsiftis G, Tsoumakas K. Immunization coverage and
predictive factors for complete and age-appropriate vaccination among preschoolers in Athens,
Greece: a cross--sectional study. BMC Public Health. 2013 Oct 2;13:908
Poethko-Müller C, Mankertz A. [Vaccination coverage against measles and sero-epidemiology of
measles-specific IgG antibodies in German children and adolescents]. Bundesgesundheitsblatt
Gesundheitsforschung Gesundheitsschutz. 2013 Sep;56(9):1243-52
Smits G, Mollema L, Hahné S, de Melker H, Tcherniaeva I, Waaijenborg S, van Binnendijk R, van
der Klis F, Berbers G. Seroprevalence of mumps in The Netherlands: dynamics over a decade
with high vaccination coverage and recent outbreaks. PLoS One. 2013;8(3):e58234
Streng A, Grote V, Carr D, Hagemann C, Liese JG. Varicella routine vaccination and the effects on
varicella epidemiology - results from the Bavarian Varicella Surveillance Project (BaVariPro),
2006-2011. BMC Infect Dis. 2013 Jul 2;13:303
Bechini A, Boccalini S, Tiscione E, Pesavento G, Mannelli F, Peruzzi M, Rapi S, Mercurio S,
Bonanni P. Progress towards measles and rubella elimination in Tuscany, Italy: the role of
population seroepidemiological profile. Eur J Public Health. 2012 Feb;22(1):133-9
Bielicki JA, Achermann R, Berger C. Timing of measles immunization and effective population
vaccine coverage. Pediatrics. 2012 Sep;130(3):e600-6
Bouhamam N, Laporte R, Boutin A, Uters M, Bremond V, Noel G, Rodier P, Minodier P.
[Relationship between precariousness, social coverage, and vaccine coverage: survey among
children consulting in pediatric emergency departments in France]. Arch Pediatr. 2012
Mar;19(3):242-7
Delgado de Los Reyes J, Arencibia Jimenez M, Navarro Gracia J, Alonso Echabe E, Garcia Puente
P, Banqueri Guerrero E, Perez Torregrosa G, Calle Barreto J, Zurriaga Carda R. Ongoing measles
outbreak in Elche, Spain, 29 January to 9 March 2012. Euro Surveill. 2012 Mar 15;17(11)
Fitzpatrick G, Ward M, Ennis O, Johnson H, Cotter S, Carr MJ, O Riordan B, Waters A, Hassan J,
Connell J, Hall W, Clarke A, Murphy H, Fitzgerald M. Use of a geographic information system to
map cases of measles in real-time during an outbreak in Dublin, Ireland, 2011. Euro Surveill.
2012 Dec 6;17(49)
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
77
Hug S, Weibel D, Delaporte E, Gervaix A, Heininger U. Comparative coverage of supplementary
and universally recommended immunizations in children at 24 months of age. Pediatr Infect Dis
J. 2012 Mar;31(3):217-20
Karasek E, Paradowska-Stankiewicz I. [Rubella in Poland in 2010]. Przegl Epidemiol.
2012;66(2):197-203
Karasek E, Rogalska J, Paradowska-Stankiewicz I. [Measles in Poland in 2010]. Przegl Epidemiol.
2012;66(2):185-90
Roggendorf H, Santibanez S, Mankertz A, van Treeck U, Roggendorf M. Two consecutive measles
outbreaks with genotypes D8 and D4 in two mainly unvaccinated communities in Germany. Med
Microbiol Immunol. 2012 Aug;201(3):349-55
Vainio K, Steen TW, Arnesen TM, Rønning K, Ånestad G, Dudman S. Measles virus genotyping an
important tool in measles outbreak investigation in Norway, 2011. Euro Surveill. 2012 Dec
13;17(50)
Barrabeig I, Rovira A, Muñoz P, Batalla J, Rius C, Sánchez JA, Domínguez À. MMR vaccine
effectiveness in an outbreak that involved day-care and primary schools. Vaccine. 2011 Oct
19;29(45):8024-31
Bassetti M, Schenone E, Calzi A, Camera M, Valle L, Ansaldi F, Pagano G, Viscoli C. Measles
outbreak in adults in Italy. Infez Med. 2011 Mar;19(1):16-9
Cockman P, Dawson L, Mathur R, Hull S. Improving MMR vaccination rates: herd immunity is a
realistic goal. BMJ. 2011 Oct 4;343:d5703
Khetsuriani N, Deshevoi S, Goel A, Spika J, Martin R, Emiroglu N. Supplementary immunization
activities to achieve measles elimination: experience of the European Region. J Infect Dis. 2011
Jul;204 Suppl 1:S343-52
Lang P, Zimmermann H, Piller U, Steffen R, Hatz C. The Swiss National Vaccination Coverage
Survey, 2005-2007. Public Health Rep. 2011 Jul-Aug;126 Suppl 2:97-108
Sabbe M, Hue D, Hutse V, Goubau P. Measles resurgence in Belgium from January to mid-April
2011: a preliminary report. Euro Surveill. 2011 Apr 21;16(16
Sakou II, Tsitsika AK, Papaevangelou V, Tzavela EC, Greydanus DE, Tsolia MN. Vaccination
coverage among adolescents and risk factors associated with incomplete immunization. Eur J
Pediatr. 2011 Nov;170(11):1419-26
Siedler A, Mankertz A, Feil F, Ahlemeyer G, Hornig A, Kirchner M, Beyrer K, Dreesman J,
Scharkus S, Marcic A, Reiter S, Matysiak-Klose D, Santibanez S, Krause G, Wichmann O. Closer to
the goal: efforts in measles elimination in Germany 2010. J Infect Dis. 2011 Jul;204 Suppl
1:S373-80
Stanescu A, Janta D, Lupulescu E, Necula G, Lazar M, Molnar G, Pistol A. Ongoing measles
outbreak in Romania, 2011. Euro Surveill. 2011 Aug 4;16(31)

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
78
Wadl M, Siedler A, Krämer W, Haindl ME, Gebrande S, Krenn-Lanzl I, Mankertz A, Hautmann W.
Measles transmission from an anthroposophic community to the general population, Germany
2008. BMC Public Health. 2011 Jun 15;11:474
Zimmerman L, Rogalska J, Wannemuehler KA, Haponiuk M, Kosek A, Pauch E, Plonska E, Veltze
D, Czarkowski MP, Buddh N, Reef S, Stefanoff P. Toward rubella elimination in Poland: need for
supplemental immunization activities, enhanced surveillance, and further integration with
measles elimination efforts. J Infect Dis. 2011 Jul;204 Suppl 1:S389-95
Bätzing-Feigenbaum J, Pruckner U, Beyer A, Sinn G, Dinter A, Mankertz A, Siedler A, Schubert A,
Suckau M. Spotlight on measles 2010: preliminary report of an ongoing measles outbreak in a
subpopulation with low vaccination coverage in Berlin, Germany, January-March 2010. Euro
Surveill. 2010 Apr 1;15(13)
Cova M, Cucchi A, Turlà G, Codecà B, Buriani O, Gabutti G. Spotlight on measles 2010: Increased
measles transmission in Ferrara, Italy, despite high vaccination coverage, March to May 2010:
increased measles transmission in Ferrara, Italy, despite high vaccination coverage, March to
May 2010. Euro Surveill. 2010 Dec 16;15(50)
Curtale F, Perrelli F, Mantovani J, Ciofi degli Atti M, Filia A, Nicoletti L, Magurano F, Borgia P, Di
Lallo D. Description of two measles outbreaks in the Lazio Region, Italy (2006-2007).
Importance of pockets of low vaccine coverage in sustaining the infection. BMC Infect Dis. 2010
Mar 11;10:62
Jeannot E, Wyler Lazarevic CA, Duperrex O, Chastonay P. [Evolution of vaccine coverage from
school year 2003-2004 to 2006-2007, for 5 to 6-year-old children in Geneva]. Med Mal Infect.
2010 Jan;40(1):27-30
Lashkari HP, El Bashir H. Immunisations among school leavers: is there a place for measles-
mumps-rubella vaccine? Euro Surveill. 2010 Apr 29;15(17)
Parent du Châtelet I, Antona D, Freymuth F, Muscat M, Halftermeyer-Zhou F, Maine C, Floret D,
Lévy-Bruhl D. Spotlight on measles 2010: update on the ongoing measles outbreak in France,
2008-2010. Euro Surveill. 2010 Sep 9;15(36)
Reuss AM, Feig M, Kappelmayer L, Siedler A, Eckmanns T, Poggensee G. Varicella vaccination
coverage of children under two years of age in Germany. BMC Public Health. 2010 Aug
19;10:502
Stronegger WJ, Freidl W. A hierarchical analysis of social determinants of measles vaccination
coverage in Austrian schoolchildren. Eur J Public Health. 2010 Jun;20(3):354-9
Borràs E, Domínguez A, Oviedo M, Batalla J, Salleras L. The influence of public or private
paediatric health care on vaccination coverages in children in Catalonia (Spain). Eur J Public
Health. 2009 Jan;19(1):69-72
Poethko-Müller C, Ellert U, Kuhnert R, Neuhauser H, Schlaud M, Schenk L. Vaccination coverage
against measles in German-born and foreign-born children and identification of unvaccinated
subgroups in Germany. Vaccine. 2009 Apr 28;27(19):2563-9

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
79
Richard JL, Masserey Spicher V. Large measles epidemic in Switzerland from 2006 to 2009:
consequences for the elimination of measles in Europe. Euro Surveill. 2009 Dec 17;14(50)
Schönberger K, Grote V, von Kries R, Kalies H. [Risk factors for delayed or missed measles
vaccination in young children]. Bundesgesundheitsblatt Gesundheitsforschung
Gesundheitsschutz. 2009 Nov;52(11):1045-51
Theeten H, Vandermeulen C, Roelants M, Hoppenbrouwers K, Depoorter AM, Van Damme P.
Coverage of recommended vaccines in children at 7-8 years of age in Flanders, Belgium. Acta
Paediatr. 2009 Aug;98(8):1307-12
Andrews N, Tischer A, Siedler A, Pebody RG, Barbara C, Cotter S, Duks A, Gacheva N, Bohumir K,
Johansen K, Mossong J, Ory Fd, Prosenc K, Sláciková M, Theeten H, Zarvou M, Pistol A, Bartha K,
Cohen D, Backhouse J, Griskevicius A. Towards elimination: measles susceptibility in Australia
and 17 European countries. Bull World Health Organ. 2008 Mar;86(3):197-204
Choi YH, Gay N, Fraser G, Ramsay M. The potential for measles transmission in England. BMC
Public Health. 2008 Sep 26;8:338
Gagneur A, Pinquier D, Aubert M, Balu L, Brissaud O, De Pontual L, Gras Le Guen C, Hau-Rainsard
I, Mory O, Picherot G, Stephan JL, Cohen B, Caulin E, Soubeyrand B, Reinert P. Kinetics of decline
of maternal measles virus-neutralizing antibodies in sera of infants in France in 2006. Clin
Vaccine Immunol. 2008 Dec;15(12):1845-50
Mikolajczyk RT, Akmatov MK, Stich H, Krämer A, Kretzschmar M. Association between
acculturation and childhood vaccination coverage in migrant populations: a population based
study from a rural region in Bavaria, Germany. Int J Public Health. 2008;53(4):180-7
Nardone A, Tischer A, Andrews N, Backhouse J, Theeten H, Gatcheva N, Zarvou M, Kriz B, Pebody
RG, Bartha K, O'Flanagan D, Cohen D, Duks A, Griskevicius A, Mossong J, Barbara C, Pistol A,
Slaciková M, Prosenc K, Johansen K, Miller E. Comparison of rubella seroepidemiology in 17
countries: progress towards international disease control targets. Bull World Health Organ.
2008 Feb;86(2):118-25
Paulo AC, Gomes MC, Gomes MG. Dynamics and control of measles in Portugal: accessing the
impact of anticipating the age for the first dose of MMR from 15 to 12 months of age. Vaccine.
2008 May 2;26(19):2418-27
Rota MC, Massari M, Gabutti G, Guido M, De Donno A, Ciofi degli Atti ML. Measles serological
survey in the Italian population: interpretation of results using mixture model. Vaccine. 2008
Aug 12;26(34):4403-9
Vandermeulen C, Roelants M, Theeten H, Van Damme P, Hoppenbrouwers K. Vaccination
coverage and sociodemographic determinants of measles-mumps-rubella vaccination in three
different age groups. Eur J Pediatr. 2008 Oct;167(10):1161-8
Guagliardo V, Bouhnik AD, Verger P. [Evaluation of vaccine coverage in children from 2 to 4
years old in South-Eastern France]. Arch Pediatr. 2007 Apr;14(4):338-44
Mixer RE, Jamrozik K, Newsom D. Ethnicity as a correlate of the uptake of the first dose of
mumps, measles and rubella vaccine. J Epidemiol Community Health. 2007 Sep;61(9):797-801

Models of Children’s Primary Care - Systematic review and meta analysis of the literature
80
Sonnenberg P, Crowcroft NS, White JM, Ramsay ME. The contribution of single antigen measles,
mumps and rubella vaccines to immunity to these infections in England and Wales. Arch Dis
Child. 2007 Sep;92(9):786-9. Epub 2007 Apr 5
Tischer A, Gassner M, Richard JL, Suter-Riniker F, Mankertz A, Heininger U. Vaccinated students
with negative enzyme immunoassay results show positive measles virus-specific antibody
levels by immunofluorescence and plaque neutralisation tests. J Clin Virol. 2007 Mar;38(3):204-
9
Heininger U, Loos K, Lorenz I, Rascher W. Compliance with recommended immunizations in
adolescents. Eur J Pediatr. 2006 Oct;165(10):671-6. Epub 2006 May 18
Heininger U, Zuberbühler M. Immunization rates and timely administration in pre-school and
school-aged children. Eur J Pediatr. 2006 Feb;165(2):124-9. Epub 2005 Dec 3
Kalies H, Grote V, Schmitt HJ, von Kries R. Immunisation status of children in Germany: temporal
trends and regional differences. Eur J Pediatr. 2006Jan;165(1):30-6. Epub 2005 Sep 14
Rota MC, Bella A, Gabutti G, Giambi C, Filia A, Guido M, De Donno A, Crovari P, Ciofi Degli Atti
ML; Serological Study Group. Rubella seroprofile of the Italian population: an 8-year
comparison. Epidemiol Infect. 2007 May;135(4):555-62. Epub 2006 Nov 1
Wichmann O, Hellenbrand W, Sagebiel D, Santibanez S, Ahlemeyer G, Vogt G, Siedler A, van
Treeck U. Large measles outbreak at a German public school, 2006. Pediatr Infect Dis J. 2007
Sep;26(9):782-6
Stampi S, Ricci R, Ruffilli I, Zanetti F. Compulsory and recommended vaccination in Italy:
evaluation of coverage and non-compliance between 1998-2002 in Northern Italy. BMC Public
Health. 2005 Apr 21;5:42
van der Wal MF, Diepenmaat AC, Pel JM, Hirasing RA. Vaccination rates in a multicultural
population. Arch Dis Child. 2005 Jan;90(1):36-40
Alfredsson R, Svensson E, Trollfors B, Borres MP. Why do parents hesitate to vaccinate their
children against measles, mumps and rubella? Acta Paediatr. 2004 Sep;93(9):1232-7
Ciofi Degli Atti ML, Rota MC, Bella A, Salmaso S; ICONA Study Group. Do changes in policy affect
vaccine coverage levels? Results of a national study to evaluate childhood vaccination coverage
and reasons for missed vaccination in Italy. Vaccine. 2004 Oct 22;22(31-32):4351-7
Dannetun E, Tegnell A, Hermansson G, Törner A, Giesecke J. Timeliness of MMR vaccination--
influence on vaccination coverage. Vaccine. 2004 Oct 22;22(31-32):4228-32
Henderson R, Oates K, MacDonald H, Smith WC, Selvaraj S. Factors influencing the uptake of
childhood immunisation in rural areas. Br J Gen Pract. 2004 Feb;54(499):114-8
Vandermeulen C, Roelants M, Vermoere M, Roseeuw K, Goubau P, Hoppenbrouwers K. Outbreak
of mumps in a vaccinated child population: a question of vaccine failure? Vaccine. 2004 Jul
29;22(21-22):2713-6
Models of Children’s Primary Care - Systematic review and meta analysis of the literature
81
Centers for Disease Control and Prevention (CDC). Measles epidemic attributed to inadequate
vaccination coverage--Campania, Italy, 2002. MMWR Morb Mortal Wkly Rep. 2003 Oct
31;52(43):1044-7
Nardone A, Pebody RG, van den Hof S, Levy-Bruhl D, Plesner AM, Rota MC, Tischer A, Andrews
N, Berbers G, Crovari P, Edmunds WJ, Gabutti G, Saliou P, Miller E. Sero-epidemiology of mumps
in western Europe. Epidemiol Infect. 2003 Aug;131(1):691-701
Bonanni P, Bergamini M. Factors influencing vaccine uptake in Italy. Vaccine. 2001 Oct 15;20
Suppl 1:S8-12; discussion S1
Siedler A, Hermann M, Schmitt HJ, Von Kries R. Consequences of delayed measles vaccination in
Germany. Pediatr Infect Dis J. 2002 Sep;21(9):826-30
Vellinga A, Depoorter AM, Van Damme P. Vaccination coverage estimates by EPI cluster
sampling survey of children (18-24 months) in Flanders, Belgium. Acta Paediatr.
2002;91(5):599-603
Hanratty B, Holt T, Duffell E, Patterson W, Ramsay M, White JM, Jin L, Litton P. UK measles
outbreak in non-immune anthroposophic communities: the implications for the elimination of
measles from Europe. Epidemiol Infect. 2000 Oct;125(2):377-83
Janaszek W, Gut W, Gay NJ. The epidemiology of measles in Poland: prevalence of measles virus
antibodies in the population. Epidemiol Infect. 2000 Oct;125(2):385-92
Mossong J, Muller CP. Estimation of the basic reproduction number of measles during an
outbreak in a partially vaccinated population. Epidemiol Infect. 2000 Apr;124(2):273-8