system chief of cardiovascular president, … bleeding both received mv repair, no mr at d/c...
TRANSCRIPT
William A. Gray MD
System Chief of Cardiovascular
Services, Main Line Health
President, Lankenau Heart Institute
Wynnewood, Pennsylvania
USA

Main Line Health Lankenau Heart Institute
Mitral Valve Disease Today…
Nkomo VT et al. Lancet. 2006; 368:1005-1011
AHA Heart Disease and Stroke Statistics – 2017 Update, Circulation 2017
Mitral regurgitation is the most common type of heart valve insufficiency in the US
Prevalence increases with increasing age, from 0.5% for 18-44 yr old rising to 9.3% for ≥75 yo
Main Line Health Lankenau Heart Institute
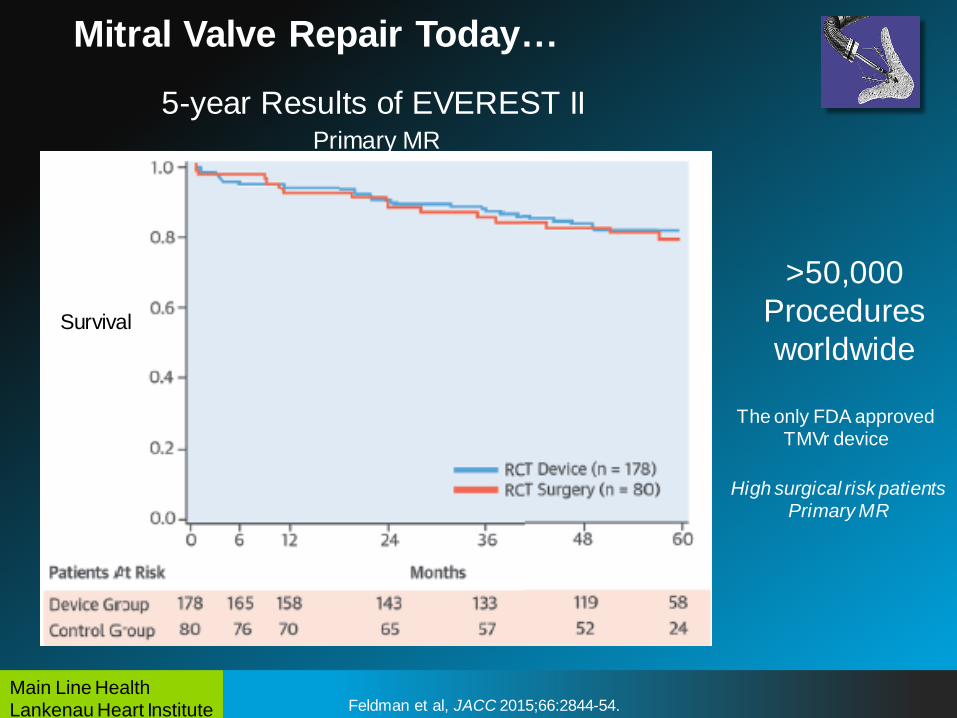
Mitral Valve Repair Today…
Feldman et al, JACC 2015;66:2844-54.
5-year Results of EVEREST II Primary MR
Survival
>50,000
Procedures
worldwide
The only FDA approved TMVr device
High surgical risk patients Primary MR
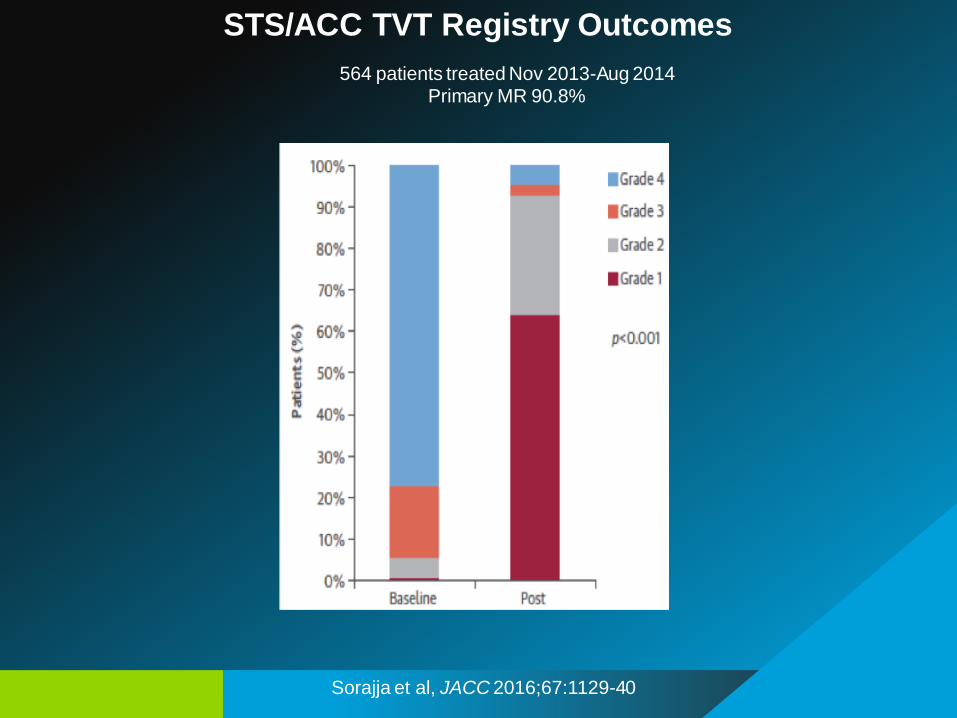
Evanston Hospital Sorajja et al, JACC 2016;67:1129-40
Feldman et al, JACC 2015;66:2844-54.
STS/ACC TVT Registry Outcomes
564 patients treated Nov 2013-Aug 2014 Primary MR 90.8%

Evanston Hospital Sorajja et al, JACC 2017;70:2315-27
Feldman et al, JACC 2015;66:2844-54.
STS/ACC TVT Registry Outcomes
2,952 patients treated Nov 2013-Sep 2015 Primary MR 85.9%
Presented at TCT
10-31-17

Evanston Hospital
Functional MR, unmet need with unmet evidence base…
Enrollment complete
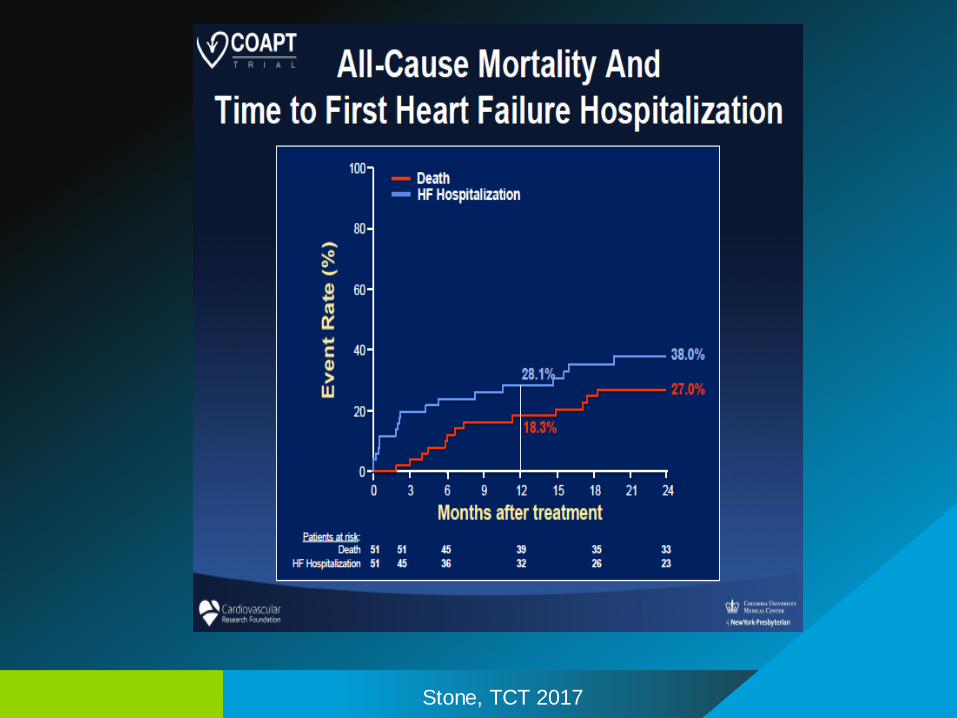
Stone, TCT 2017

Evanston Hospital

Evanston Hospital Stone, TCT 2017

Evanston Hospital Stone, TCT 2017
Evanston Hospital Stone, TCT 2017

Evanston Hospital Stone, TCT 2017
Evanston Hospital Stone, TCT 2017

Evanston Hospital
Many New Technologies

Evanston Hospital Worthley et al, TCT 2017
New TMVs devices today…
ARTO-MVRx System

Main Line Health Lankenau Heart Institute
Characteristic All Patients (N=45)
Device Technical Success (MVARC)*% 100
Compression of LCX or other coronary
artery n (%) 0(0)
New Onset Atrial Fibrillation, n (%) 0 (0)
ARTO procedure time (mins) 88.0 ± 28.7
Fluoro Time (mins) 43.5 ± 16.2
Total Contrast Vol (ml) 96.0 ± 82.0
Days in Hospital (median)
(IQR)
2.0
(1-5)
Device Technical success defined as: At exit from cath lab, alive, with: 1) Successful access, delivery and retrieval of the
device delivery system, and 2)Deployment and correct positioning (including repositioning/recapture if needed) of the
single intended device, and 3)No need for additional unplanned or emergency surgery or re-intervention related to the
device or access procedure
Procedural Outcomes (Phase I/II)

Effective MR Reduction at 30 days (Phase I/II)

30 day Safety Outcomes (Phase I/II)

Main Line Health Lankenau Heart Institute
MR Grade Reduction Maintained to 3 years
(Phase I)

Main Line Health Lankenau Heart Institute
Reduced Heart Failure Hospitalization (Phase I)
The post ARTO number includes a hospitalization for a patient who died but was not hospitalized
P=0.01

Main Line Health Lankenau Heart Institute
NYHA Class Reduction
Maintained to 3 years (Phase I)
*

Evanston Hospital Gammie et al, TCT 2017
New TMVs devices today…
HARPOON System

Harpoon: Technology
21-gauge needle with pre-wound
ePTFE suture in preformed knot
configuration
Hemostatic introducer to
reduce blood loss
Delivered to the valve via a low profile
3mm delivery system
Double helix anchor with ePTFE
suture as the only implant


Harpoon Procedure

Real-Time Titration of ePTFE
Cordal Length

Early Feasibility Study
First 13 Patients
Feb 2015 – Feb 2016
-Safe
-Effective MR Reduction
Circulation. 2016;134:189–197

Technical success rate:
95 % (41/43)
Two intraoperative conversions to conventional surgery
-Patient #14 poor imaging, insufficient MR reduction
-Patient #23 poor imaging prolonged proc, access
site bleeding
Both received MV repair, No MR at D/C
Procedural success at 30 days:
93% (40/43)
One repaired valve MSSA infective endocarditis POD #27
Preop elevated WBC, dental disease unrecognized: successful MVR
Results

Excludes 3 conversions to conventional surgery
100% 100%
87.5%
12.5%
100%
0%
20%
40%
60%
80%
100%
Baseline(43)
Procedure(41)
Discharge(38)
30-Day(40)
Mass General Core Lab Adjudicated
Harpoon Patients MR Grades
Severe
Moderate
Mild or Less
Results: MR Grades

P2
Pr
e
Post
5 mm
Harpoon Annuloplasty Effect
Evanston Hospital Praz et al, Lancet 2017;390:773-80
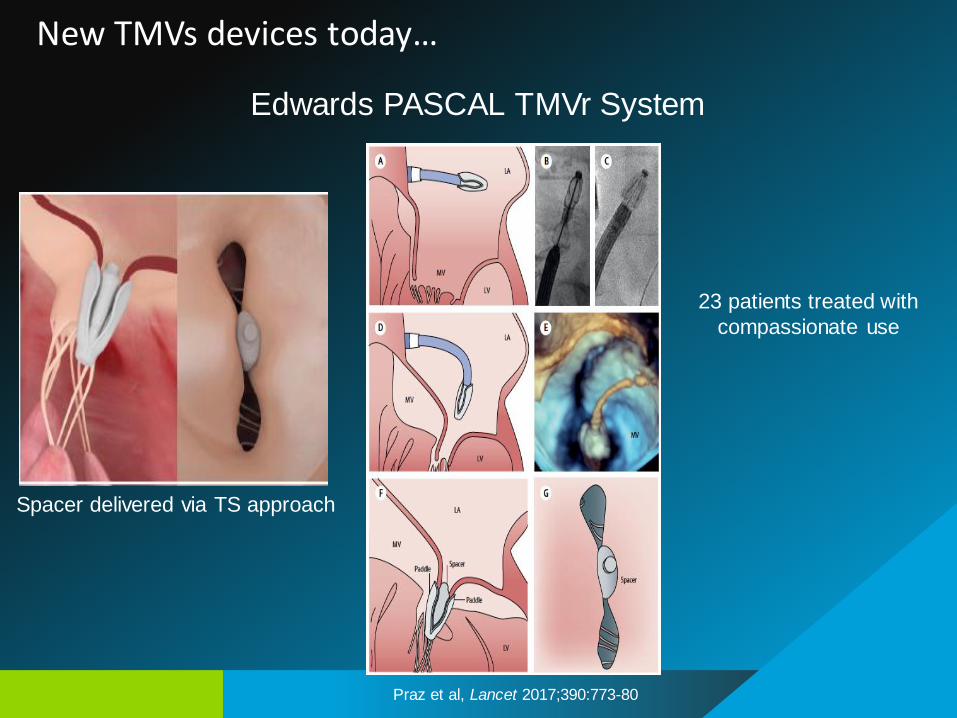
New TMVs devices today…
Edwards PASCAL TMVr System
23 patients treated with
compassionate use
Spacer delivered via TS approach

Evanston Hospital Praz et al, Lancet 2017;390:773-80
Edwards PASCAL TMVr System
New TMVs devices today…

Evanston Hospital
Ongoing Clinical Trials today…
Edwards PASCAL TrAnScatheter Mitral Valve RePair System Study
Multicenter, multi-national, prospective, single arm, early feasibility
60 patients, 20 sites
3 (+) to 4 (+) MR (FMR or DMR)
NYHA II or greater
Candidate for surgery but surgery considered not the best option

Evanston Hospital
Ongoing Clinical Trials today…
Cardioband The Carrillon Trial (FDA IDE)
400 patients, 50 sites US, Canada, EU, Australia
EF <50%
At least 2+ MR and EORA ≥0.2 cm2
NYHA II, III or IV
2:1 Device vs GDMT
Blinded sham-controlled
400 patients
Ischemic or non-ischemic CMP
2:1 Device vs GDMT

Evanston Hospital
Combo therapy today…
+ =
“Tool Box” Concept

Evanston Hospital
CardiaQ Tendyne Tiara Twelve
SAPIEN 3 MAC-ViR-ViV
SAPIEN XT MAC-ViR-ViV
TMVR Early Feasibility Study Trials today…
Caison

Evanston Hospital

Evanston Hospital
TMVR EFS Trials today…
Tendyne Feasibility Trial
30 high risk surgical patients
Muller et al, J Am Coll Cardiol Dec 2016;S0735-1097(16)37122-4.

Evanston Hospital
Tendyne 30-Day Outcomes
Device Success at 30 Days
Success 80% (60/75)
Failure* 20% (15/75)
Mortality 6.7% (5/75)
Implant not Successful 4.0% (3/75)
LVOT Obstruction 1.3% (1/75)
Valve did not seat properly 1.3% (1/75)
Patient became hemodynamically unstable,
procedure not completed, unplanned circulatory support
1.3% (1/75)
Re-intervention 2.6% (2/75)
Reposition Device- resolve PVL 1.3% (1/75)
Bleeding with re-operation 1.3% (1/75)
Device-related performance or Adverse Events* 5.3% (6/75)
Mitral valve gradient > 6 mmHg 5.3% (4/75)
Paravalvular Leak 1.3% (1/75)
Device Malpositioning 1.3% (1/75)
Device Thrombosis 1.3% (1/75) Muller, London Valves 2017

Kaplan-Meier survival curve (n=30)
•
1.0
0.8
0.6
0.4
0.2
0.0 0 100 200 300
Days
All-cause mortality
0.83

Main Line Health Lankenau Heart Institute
Tendyne TMVR: 1yr outcomes
Outcome N=30
Death (all cause) 5 (16.7%)
Cardiac 4 (13.3%)
Non-cardiac 1 (3.3%)
CVA/TIA 0 (0%)
Re-hospitalisation
Heart failure 3 (10.0%)
MV surgery 0 (0%)
Valve performance (n=28)
Malposition/PVL/hemolysis 1 (3.6%)
Leaflet thrombosis 1 (3.6%)

•
MR severity 1 year post-TMVR Paired data
N: 19 19 19
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Baseline 1mth 12mths
Grade 4
Grade 3
Grade 2
Grade 1
Grade 0
89.5
10.5
94.7
5.3
94.7
5.3

LVEF post-TMVR Paired analysis
p=NS
N: 18 18 18
0
5
10
15
20
25
30
35
40
45
50
Baseline 1mth 12mths
46.7
38.4 42.0
p<0.01 vs baseline p=NS
LVEF (%)
Main Line Health Lankenau Heart Institute
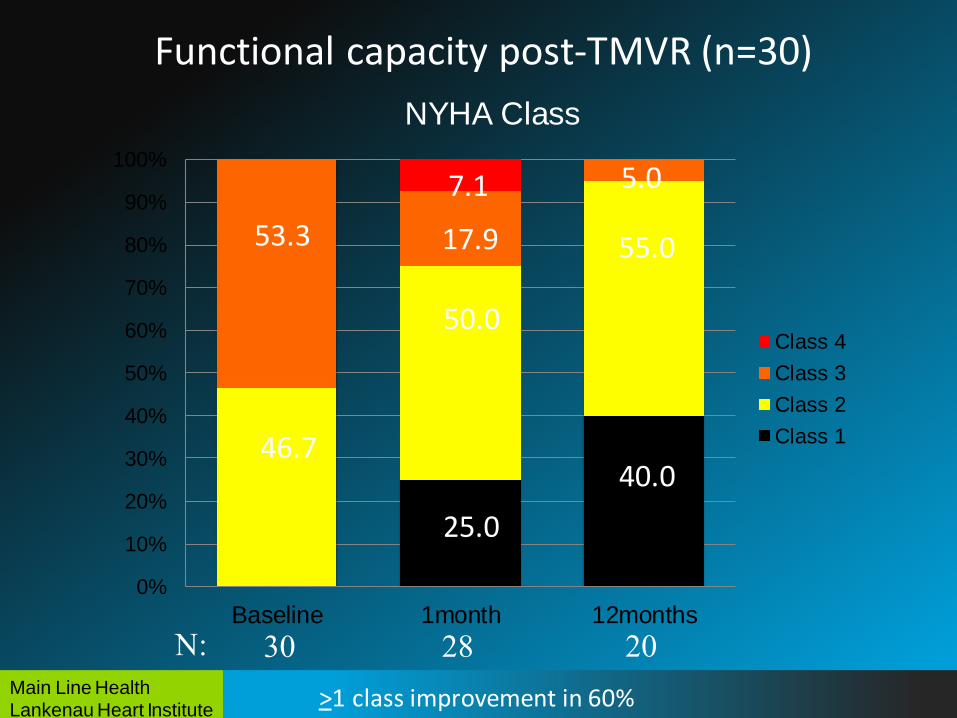
Functional capacity post-TMVR (n=30)
>1 class improvement in 60%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Baseline 1month 12months
NYHA Class
Class 4
Class 3
Class 2
Class 146.7
53.3 55.0
40.0
5.0 7.1
25.0
50.0
17.9
N: 30 28 20

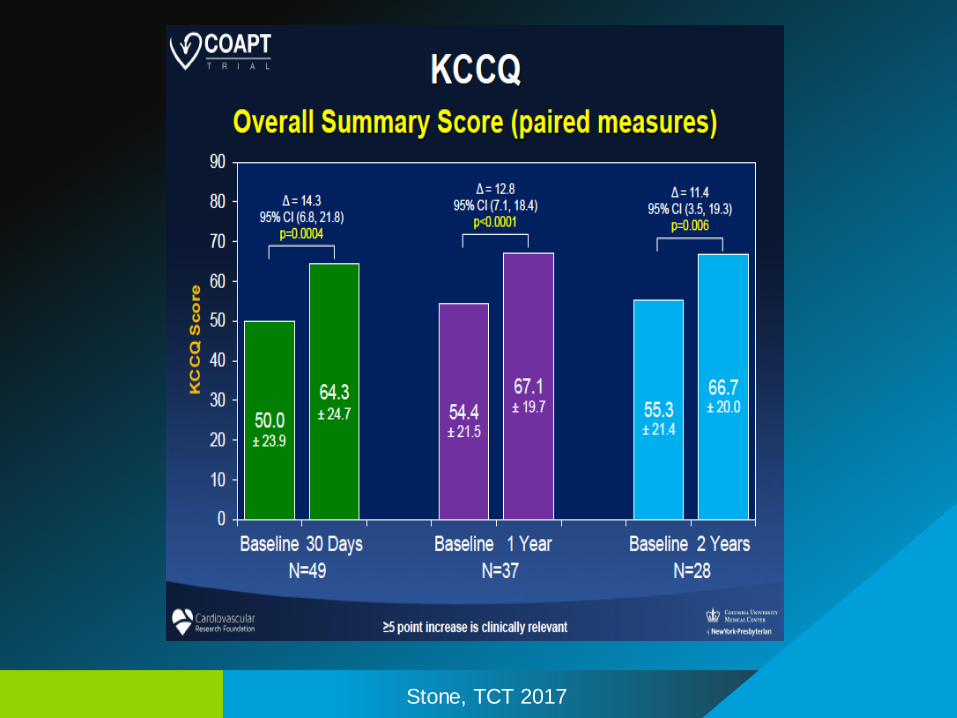
Quality of Life: KCCQ
•
0
20
40
60
80
100
120
baseline 30 day 12 months
KC
CQ
KCCQ in subjects with complete data at three timepoints (n=22)
* *
p<0.001 p<0.001
* vs baseline

Evanston Hospital
Intrepid Pilot study
Sorajja, TCT 2017

Evanston Hospital
APOLLO Pivotal Trial
650 patients, 60 sites
2 cohorts:
1 randomized to surgery to demonstrate non-inferiority
1 single arm for high surgical patients
Press release 10-23-17

Evanston Hospital
Conclusions
Large number of patients need MV intervention
The era of TMVr and TMVR has begun
The is an explosion of new devices and clinical trials
TMVR is developing at a lower pace than TAVR
With aging population, more patients will need MV intervention
Outcomes of TMVr & TMVR will be superior than surgical outcomes
Most MV patients will be treated with transcatheter therapies
Most procedures will be performed with a transseptal approach
Today…
Tomorrow…

Evanston Hospital
Tissue engineered THV’s ?
Bioabsorbable valve stent frames ?
The day after tomorrow…