suture materials and tendon junctures
TRANSCRIPT
Suture Materials and Tendon Junctures
R. GuY PULVERTAFT, F.R.C.S., Derby, England
From the Orthopaedic and Accident Service, Derbyshire Royal Infirmary, Derby, England.
I N 1938 Mayer [1] said, "Reconstruction of severed tendons constitutes one of the
most delicate problems in surgery, a challenge to the ingenuity and dexterity of the operator."
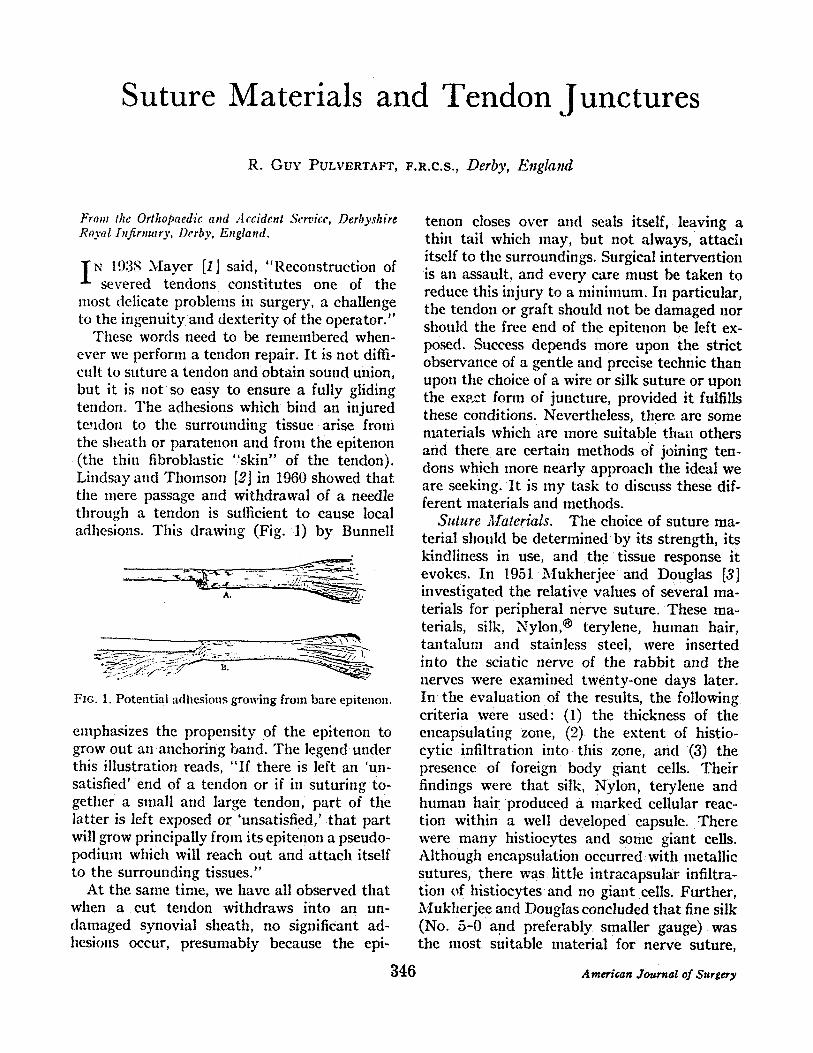
These words need to be remembered when- ever we perform a tendon repair. It is not diffi- cult to suture a tendon and obtain sound union, but it is not so easy to ensure a fully gliding tendon. The adhesions which bind an injured tendon to the surrounding tissue arise from the sheath or paratenon and from the epitenon (the thin fibroblastic "skin" of the tendon). Lindsay and Thomson [2] in 1960 showed that the mere passage and withdrawal of a needle through a tendon is sufficient to cause local adhesions. This drawing (Fig. 1) by Bunnell
FIG. 1. Potential adhesions growing from bare epitenon.
emphasizes the propensity of the epitenon to grow out an anchoring band. The legend under this illustration reads, "If there is left an 'un- satisfied' end of a tendon or if in suturing to- gether a small and large tendon, part of the latter is left exposed or 'unsatisfied,' that part will grow principally from its epitenon a pseudo- podimn which will reach out and attach itself to the surrounding tissues."
At the same time, we have all observed that when a cut tendon withdraws into an un- damaged synovial sheath, no significant ad- hesions occur, presumably because the epi-
tenon closes over and seals itself, leaving a thin tail which may, but not always, attacii itself to the surroundings. Surgical intervention is an assault, and every care must be taken to reduce this injury to a minimum. In particular, the tendon or ~ a f t should not be damaged nor should the free end of the epitenon be left ex- posed. Success depends more upon the strict observance of a gentle and precise technic than upon the choice of a wire or silk suture or upon the exact form of juncture, provided it fulfills these conditions. Nevertheless, there are some materials which are more suitable than others and there are certain methods of joining ten- dons which more nearly approach the ideal we are seeking. It is my task to discuss these dif- ferent materials and methods.
Suture Materials. The choice of suture ma- terial should be determined by its strength, its kindliness in use, and the tissue response it evokes. In 1951 Mukherjee and Douglas [3] investigated the relative values of several ma- terials for peripheral nerve suture. These ma- terials, silk, Nylon, @ terylene, human hair, tantalum and stainless steel, were inserted into the sciatic nerve of the rabbit and the nerves were exanfined twenty-one days later. In the evaluation of the results, the following criteria were used: (1) the thickness of the encapsulating zone, (2) the extent of histio- eytic infiltration into this zone, and (3) the presence of foreign body giant cells. Their findings were that silk. Nylon, terylene and human hair produced a marked cellular reac- tion within a well developed capsule. There were many histiocytes and some giaut cells. Although encapsulation occurred with metallic sutures, there was little intracapsular infiltra- tion of histiocytes and no giant cells. Further, Mukherjee and Douglas concluded that fine silk (No. 5-0 and preferably smaller gauge) was the most suitable material for nerve suture,
~46 A merir~n Journal of Surgery
S u t u r e M a t e r i a l a n d
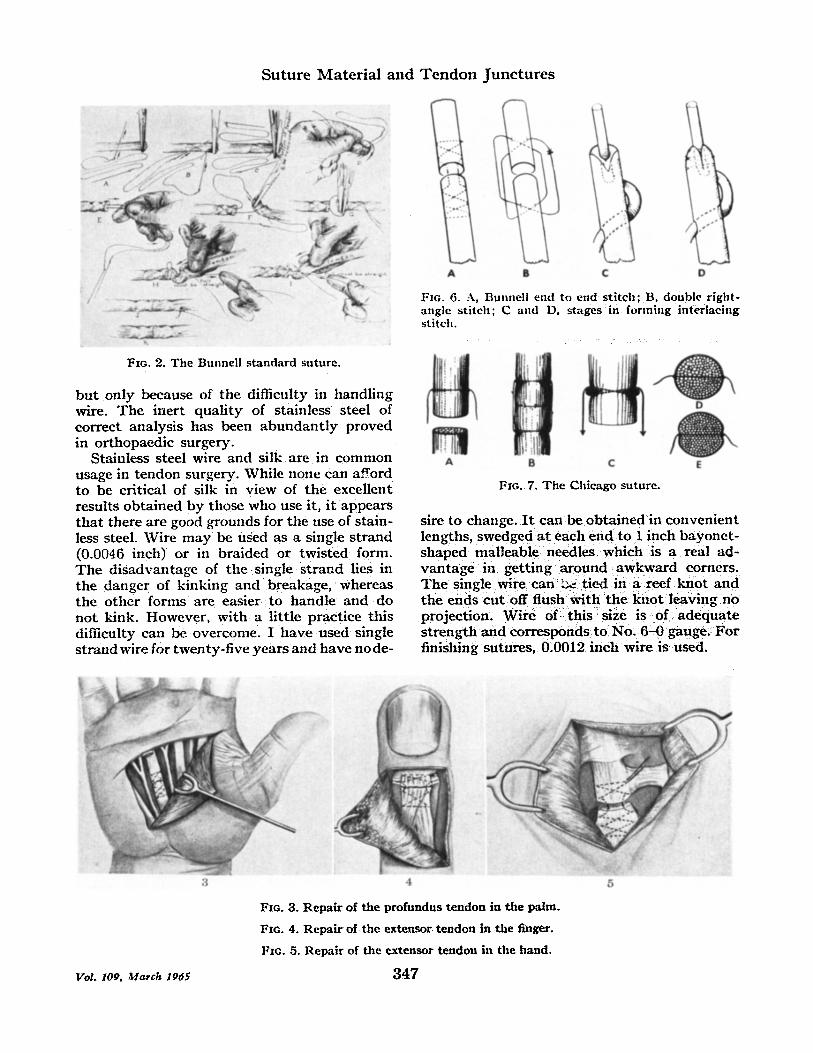
Fie. 2. The Bunnell standard suture.
b u t on ly because of the di f f icul ty in hand l ing wire. T h e iner t qua l i t y of s ta inless s teel of cor rec t ana lys i s has been a b u n d a n t l y p r o v e d in o r t hopaed i c surgery .
Sta inless s teel wire and silk are in c o m m o n usage in t endon surgery . Whi le none can afford to be cr i t ica l of silk in v i ew of t h e excel lent resul ts ob t a ined b y those who use it , i t appea r s t h a t there are good g rounds for the use of s ta in- less steel. Wi re m a y be used as a single s t r a n d (0.0046 inch) or in b ra ided or t w i s t e d form. T h e d i s a d v a n t a g e of t he single s t r a n d lies in the danger of k ink ing and breakage , whereas t he o the r fo rms are easier to hand le and do n o t kink. H o w e v e r , wi th a l i t t le p rac t i ce th is diff icul ty can be ove rcome . I h a v e u sed single s t r a n d wire for twen ty - f i ve y e a r s a n d h a v e no de-
T e n d o n J u n c t u r e s
A 6 ¢ D
Fie. 6. A, Bunnell end to end stitch; B, double right- angle stitch; C and D0 stages in forming interlacing stitch.
A 8 C
FIG. 7. The Chicago suture.
sire to change. I t can be o b t a i n e d in c o n v e n i e n t lengths, swedged a t each e n d t o 1 inch b a y o n e t - s h a p e d mal leab le n e e d l e s wh ich is a real ad- v a n t a g e in ge t t ing a r o u n d a w k w a r d corners . T h e single wire c a n ~ t i ed in a reef k n o t a n d t he ends c u t off f lush w i t h t h e k n o t l eav ing no pro jec t ion . W i r e o f this size is o f a d e q u a t e s t r e n g t h a n d co r r e sponds to No. 6 - 0 gauge . F o r f inishing s u t u r e s , 0.0012 i n c h wire is used.
Vol. 109, ~Iarch 1965
4
F*G. 3. Repair of the profundus tendon in the palm.
F,o. 4. Repair of the extensor tendon in the finger.
Fx~. 5. Repair of the extensor tendon in the hand.
3 4 7

P u l v e r t a f t
A - . ~
B
FIG, S, Tubiana 's modification of the interlace suture.
A
.% .; ,~ . j -
J " ~ " l B .
0 ; . r
Fio, 10. The Rober tson suture. Deta i ls of anastomosis of tendon gra f t .
t
¢-.
FIO. 9, Diagrams of "wrap-around" method of tendon suture for uniting slim tendon grafts to stout motor tendon (Brand).
Tendon Junctures. N u m e r o u s me thods of joining t endons have been devised and it would be tedious if I a t t e m p t e d to discuss t hem all. I propose ins tead to describe those which come within m y experience and give brief men t ion to the others.
Tendons of equal size: T h e Mayer -Bunne l l criss-cross s t i tch is excellent. (Fig. 2.) I t se- cures a firm grip and accura te apposi t ion. The only possible crit icism is t ha t the epi tenon is pene t r a t ed several t imes. I t is sui table for round and flat tendons, for jo in ing t endon to
FIG. I1. The Bunnell pull-out suture for distal fixation. Method of attaching a tendon to the distal phalanx in a finger utilizing the top of the old tendon and using re- movable stainless-steel wire.
graft when of equal size and for dis tal fixation of a graft. Figures 3, 4 and 5 show this technic in use for var ious s i tuat ions.
T h e second c o m m o n l y used m e t h o d is the Bunnel l double angle st i tch. (Fig. 6B.) Th i s is an ex t remely useful su ture when jo in ing m a n y tendons, for ins tance in multil)le divi- sions of flexor tendons at the wrist. I t is quickly inser ted and adequa te for this s i tuat ion.
T h e Mason or Chicago s t i tch (Fig. 7) is ano the r excellent me thod . I do not use it, bu t it is widely favored.
Tendons of unequal size: Grafts , par t icular ly plantaris , are usual ly considerably smaller
3 4 8 american Journal of Surgery

S u t u r e M a t e r i a l a n d T e n d o n J u n c t u r e s
FIG. 12. E y r e - B r o o k ' s m o d i f i c a t i o n for d i s t a l f i xa t ion . M e t h o d of d i s t a l a t t a c h m e n t of g r a f t . T h e i n s e r t i o n is p l a c e d d i s t a l to t h e j o i n t , a n d t h e w i r e s u t u r e t i ed o v e r a b u t t o n Oil t l le d o r s u l n of t h e f inger .
FIG. 13. T u b i a n a ' s m o d i f i c a t i o n for d i s t a l f ixa t ion .
16
17
FIG. 16. A n e w m e t h o d of d i s t a l f ixa t ion .
FIG. 17. T h e n e w m e t h o d in use.
FIG. 14. T h e u se of ho lh )w n e e d l e s d u r i n g d i s t a l f ixa t ion .
F ro . 15. I ) i s t a l f i xa t ion t h r o u g h a t u n n e l .
t han the mo to r t endon and require a different type of junc ture . For m a n y years I have used a s imple modif icat ion of the welt known inter- lacing technic. The larger t endon is slit wi th a t e n o t o m e near its end and the graf t is th readed into the slit. I t is th readed back again th rough a second slit placed in the opposi te p lane; finally, the end of the t endon is split, and the fish tail t hus formed embraces the graft. (Fig- ure 6C and D.) T h e i l lustrat ion by T u b i a n a (Fig. S) shows his modif icat ion of this me thod . I t is cus tomary , and I believe sound practice, to cover the junc t ion with the lumbricalis muscles, if the p rofundus t endon end is used. Care needs to be taken to ensure t h a t the ]um- bricalis t endon is no t t igh tened with contrac- t ion of the p rofundus muscle instead of the
graft. This error causes extension at the l)roximal in terphalangeal jo int and produces the "extensor hab i tus" as described by Will iam White.
If plantar is t endon is used as a , , r a ¢~ a(t- van tage can be t aken of its peculiar p rope r ty of spreading when drawn ou t gent ly from the sides. Brand has emphasized the advan tages of the plantar is t endon for a mult i - ta i l graft . (Fig. 9.) It tnay equal ly well be appl ied to a single graft.
Rober t son described this me thod (Ft~. 10) which is nea t and appa ren t ly very effective in joining small t endons to large tendons.
F I X A T I O N OF T E N D O N G R A F T TO T t I E
T E R M I N A L P I I A L A N X
The distal a t t a c h m e n t of a t endon graft m a y be ei ther to bone or to tendon. Frankly , I do not believe it ma t t e r s which me thod is used provided the junc tu re is sound, nea t and be- yond the in terphalangeal joint. Bunnel l ' s i l lustration (Fig. 11) shows the a t t a c h m e n t to the distal t endon by the "pu l l -ou t" technic. One slight modif icat ion is by Kyle and Eyre- Brook of Bristol (Fig. 12) and ano the r is by T u b i a n a of Paris. (Fig. 13.)
Vol. 109, Alarch 1965 3 4 9

P u l v e r t a f t
FIG. 18, The owreet tension of a t e n d , n graft.
A B FIG. 21. A and B, late repair of flexor tendon divi- sions of all fingers in the palm. Result after bridge graft ing.
19
2(1
. J
t""
: A f2
FIG. 19. The Bunnel l bridge graft,
Fro. 20. The bridge graft in use.
I have used three me thods for the fixation of a graf t to the te rmina l phalanx. T h e first is the Btmnell "pu l l -ou t " st i tch. T h e graf t is at- tached to the distal t endon s t m n p or tucked into the angle between the bone and the ten- don s tump . To achiEvE this easily, hollow needles are passed th rough the pulp to emerge a t the angle and the wire is pushed th rough the needlE. (Fig. 14.) Th is t idy m e t h o d of fixa- tion has one significant d i sadvantage , t h a t is, i t is difficult to judge the correct l ength of graf t unt i l t he s t i tch has been comple ted .
T h e SEcond m e t h o d is to pass the graft th rough a t ransverse tunne l in the phalanx and su tu re it back to itself. (Fig. 15.) This me thod is sound and SECURE; it permi ts accura te ad jus tme t l t of the tension. However , I advise
its use only when the graft is thin and I would no t employ it in chi ldren because of the risk of in jur ing the epiphyseal plate, Special .in- s t rumen t s are used to bore the tunne l precisely in the correct place. Dur ing the period when I was especially enthus ias t ic abou t encouraging early m o v e m e n t in pa t ien ts wi th flexor t endon grafts, I used this fixation cons tant ly ,
Dur ing the pas t few years I have employed a different technic which has been devised for a special purpose. The Bunnel l "pull-otW' su ture for terminal fixation is a nea t and Excellent m e t h o d except for the difficulty in judg ing the tension. The tension, which mus t be per- fect, canno t bE es t imated accura te ly unt i l the suti lre has been comple ted . If it is found to be too t ight, correct ion is difficult. If it is a little too slack, one is tEmptEd to accept i t r a the r t h a n s tar t again. Dur ing the pas t few years I have EmployEd a different technic. T h e graft is d rawn th rough the finger pulp wi th a Reverden ' s needle and tile ex tending pa r t clasped by a fine a r t e ry forcep or special clip. (Fig. 16.) The tension is ad jus t ed with precision, e i ther by allowing the graf t to slip back or by wi thd -awing it a little fu r the r as tile case m a y require. T h e graft is s t i tched to the p ro fundus tag t h rough which it has passed before en ter ing the pulp. We have no compla in t s with this m e t h o d and it has bECOmE s tandard practice, Figures 17 and lS show the clip in place and the ideal tension. T im finger is a little more flexed t h a n the posi t ion i t would normal ly assume in relation to the o the r fingers.
SPECIAL TECtINICS
"_l'he BrMge Graft. This me thod , described by Bunnell , is ideal when insert ing a shor t
3 5 0 American Journal of Surgery

S u t u r e M a t e r i a l a n d T e n d o n J u n c t u r e s
A B C
FIe;. "22. A, 13 and Q, l a te r epa i r of f lexor t e n d o n d i v i s i o n s of al l f ingers a n d t h u m b in t h e wr is t . R e s u l t a f t e r b r i d g e g ra f t i ng ,
graft of equal size to make up a deficiency in length. I t is especially apl)licable to the see- ondary repair of tendons in the pahn and wrist. Originally, Bunnell used silk (Fig, 19) but later he used wire. The wire passes through the graft itself. Figure 2~1 shows how the teelmic is used to restore tendon length during a see- ondary repair; the muscles have shortened and
i"mes~- ~, " ' i }Aood vee~p. 1
~ i l k ~ "i " | '! i ~ , l - - - - - ._- ' t ! : ! ( x
I :
~ u t l l o u t x , ~ r , e
Fro . 23. B u n n e l l " p u l l o u t " t e c l m i e for i m m e d i a t e re- pa i r of f lexor t e n d o n s in t he d ig i t a l t heea .
l'ol. 109, ~llarch 1965 351
a bridge graft taken from the sublimis is used to close the gap in the profundus. Tim pat ient shown in Figure 21 had division of all the finger flexor tendons in the pahn. T h e y were recon- s t ructed by 1 inch sublimis grafts used in this i l l a t l n e r .
One young man (Fig. 22A, B and C) had division of all s t ructures on the volar surface of the wrist. The resident who examined him did not believe any tendons should be sutured primari ly and so the skin alone was st i tched. He came to us like this and was t rea ted by bridge grafts to all the profundus {endons and flexor pollicis longus. The median and ulnar nerves were also repaired.
S P E C I A L S U T U R E S
I,Vithdrawal Suture. Bunnell, in his con- s tan t striving for perfection, said tha t the
FIG. 24. V e r d a n ' s t e c h n i c for i m m e d i a t e r e p a i r of f lexor t e n d o n s in t h e d i g i t a l t heea .

P u l v e r t a f t
FIG. 25. The Bunnell figure eight suture. For pr imary or secondary repair of the extensor tendons, a simple figure eight stitch with No. 35 stainless-stcel wire is used. One loop unites the tendon ends and the other the skin edges. The stitch is without strength and is merely for approximation of tendon ends. Splinting as shown pre- vents tendon ends from being pulled apart.
•
" : ; 5 1 , ,
FiG. 26. The s tandard technic used for tendon trans- ference.
best suture is the one that is not present at all. For tha t reason lie introduced the withdrawal suture. The only time I use this is for distal fixa- tion of the graft, where it is very useful. Bun- nell also used his withdrawal suture as a means of relieving tension from the true suture line in cases of pr inmry tendon repair within the digital theca. (Fig. 23.) Verdan uses the same principle, but tie relieves tension by small transfi.~ing wires. (Fig. 24.)
Figure Eight Suture. This is a simple figure eight for repair of extensor tendons and skin at the same time. (Fig. 25.) This is a perfectly good suture, but I consider tha t extensor divi- sions in the finger, if seen immediately, can be treated successfully by splinting alone.
Gig Suture. Bunnell worked out the gig suture technic to simplify and expedite ex- tensive pr imary repair.
Running Suture. This teclmic, also sug- gested by Bunnell, is useful in the finger for at- taching a transferred tendon to the intrinsic tendon.
Temton Transfer. The s tandard method for sutur ing tendon transfers was well illus- t ra ted by Donal Brooks. (Fig. 26.) I t is sintple and effective. The transferred tendon is passed through slits in the accepting tendon and fastened by mattress stitches.
CONCLUSION
It should be emphasized that each surgeon will approvc his particular form of suture ma- terial and juncture, for this he has learned to trust. However, it is the delicacy and precision with which the whole operation is performed tha t determines the result.
Acknowledgment: The following illustrations appear with the permission of the publishers: Figures 2, 1l, 19, 23 and 25 from "Surgery of the Hand ," 3rd edition, ]. B. Lippincott , Co. ; Figures 3, 4, 5, 20 and 26 from "Operat ive Surgery," But te rwor th & Co., Ltd. ; Figure 6 from "Brit ish Surgical Practice," But te rwor th & Co., Ltd. ; Figure 7 from Surgery, Gynecology amt Obstetrics, vol. 72; Figure 8, 13 and 24 from Revue de Chirurgie Orthop~dique, vols. 46 and 47; Figure 9 from "Leprosy in Theory and Practice," John Wright & Sons, Ltd. ; Figure 10 from "Clinical Orthopaedics," vol. 15, ]. B. Lippincot t Co. ;Figure 1 and 15 from the Journal of Bone and Joint Surgery, vol. 14 and 38B; Fig- ure 12 from The British Journal of Surgery, vol. 41.
REFERENCES
1. MAYER, L. Repair of severed tendons. Am..7. Surg., 12: 714, 1938.
2. LINDSAY, ~V. K. and TttOMSON', H. G. Digital flexor tendons: an experimental study. Par t I. Brit. J. Plast. Surg., 12: 289, 1960.
3. MUKHERJEE, S. R, and DOUGLAS, D. M. An investi- gation into the value of nylon and terylene as nerve sutures. Brit. J. Surg., 39: 271, 1951.
352 A merican Journal of Surgery