sustained hemodynamic and antianginal effect
TRANSCRIPT

ISOSORBIDE DINITRATE IN ANGINA/Danahy et al.
3. Beregovich J, Bianchi C, D'Angelo R, Diaz R, Rubler S: Hemodynamicstudies with dobutamine, a new inotropic agent. Circulation 47 (supplIV): IV-144, 1973
4. Goldberg LI, McDonald RH Jr, Zimmerman AM: Sodium diuresisproduced by dopamine in patients with congestive heart failure. N EngI JMed 269: 1060, 1963
5. Talley RC, Goldberg LI, Johnson CE, McNay JL: A hemodynamic com-parison of dopamine and isoproterenol in patients in shock. Circulation39: 361, 1969
6. Holzer J, Karliner JS, O'Rourke RA, Pitt W, Ross J Jr: Effectiveness ofdopamine in patients with cardiogenic shock. Am J Cardiol 31: 139, 1973
7. McNay JL, McDonald RH Jr, Goldberg LI: Direct renal vasodilatationproduced by dopamine in the dog. Circ Res 16: 510, 1965
8. Mark AL, lizuka T, Wending MG, Eckstein JW: Response of saphenousand mesenteric veins to administration of dopamine. J Clin Invest 49:259, 1970
9. Tuttle RR, Mills J: Dobutamine: Development of a new catecholamine toselectively increase cardiac contractility. Circ Res 36: 185, 1975
10. Robie NW, Nutter DO, Moody C, McNay JL: In vivo analysis ofadrenergic receptor activity of dobutamine. Circ Res 34: 663, 1974
11. Vatner SF, McRitchie RJ, Braunwald E: Effects of dobutamine on leftventricular performance, coronary dynamics, and distribution of cardiacoutput in conscious dogs. J Clin Invest 53: 1265, 1974
12. Loeb HS, Khan M, Saudye A, Gunnar RM: Acute hemodynamic effectsof dobutamine and isoproterenol in patients with low output cardiacfailure. Circulatory Shock 3: 55, 1976
13. Loeb HS, Sinno MZ, Saudye A, Towne WD, Gunnar RM: Elec-trophysiologic properties of dobutamine. Circulatory Shock 1: 217, 1974
14. Hinds JE, Hawthorne EW: Comparative cardiac dynamic effects ofdobutamine and isoproterenol in conscious instrumented dogs. Am JCardiol 36: 894, 1975
15. Loeb HS, Winslow EBJ, Rahimtoola SH, Rosen KM, Gunnar RM:Acute hemodynamic effects of dopamine in patients with shock. Circula-tion 44: 163, 1971
16. Winslow EJ, Loeb HS, Rahimtoola SH, Kamath S, Gunnar RM:Hemodynamic studies and results of therapy in 50 patients withbacteremic shock. Am J Med 54: 421, 1973
17. Robinson JA, Klodnycky ML, Loeb HS, Racic MR, Gunnar RM: En-dotoxin, prekallikrein, complement and systemic vascular resistance. AmJ Med 59: 61, 1975
18. Chidsey CA, Braunwald E, Morrow AG, Mason DT: Myocardialnorepinephrine concentration in man: Effects of reserpine and of con-gestive heart failure. N Engl J Med 269: 653, 1963
19. Mason DT, Braunwald E: Studies on digitalis. X. Effects of ouabain onforearm vascular resistance and venous tone in normal subjects and in pa-tients in heart failure. J Clin Invest 43: 532, 1964
20. Tuttle RR, Pollock GD, Todd G, Tust R: Dobutamine: Containment ofmyocardial infarction size by a new inotropic agent. Circulation 47 (supplIV): IV-521, 1973
21. Gillespie TA, Roberts R, Ambos HD, Sobel BE: Salutary effects ofdobutamine on hemodynamics without exacerbation of arrhythmia ormyocardial injury. Circulation 51 (suppl II) 11-294, 1975
22. Willerson JT, Hutton I, Watson JT, Platt MR, Templeton GH: Influenceof dobutamine on regional myocardial blood flow and ventricular perfor-mance during acute and chronic myocardial ischemia in dogs. Circulation53: 828, 1976
23. Luz P, Forrester JS, Wyatt HL, Waters D, Swan HJC: Divergent effectof dopamine upon ischemic myocardium with partial and total coronaryocclusion. Am J Cardiol 37: 130, 1976
24. Wilkes SB, Murthy VS, Laffan RJ: Effect of intravenous infusion ofdopamine on coronary circulation and oxygen transport to myocardiumin anesthetized dogs. (abstr) Clin Res 24: 514A, 1976
Sustained Hemodynamic and Antianginal Effectof High Dose Oral Isosorbide Dinitrate
DANIEL T. DANAHY, M.D., DOUGLAS T. BURWELL, M.D.,
WILBERT S. ARONOW, M.D., AND RAVI PRAKASH, M.D.
SUMMARY Twenty-one patients with documented coronary
atherosclerotic heart disease were studied to determine the effect ofhigh dose oral isosorbide dinitrate (ISDN) on heart rate, bloodpressure, and exercise time until angina pectoris. Patients were testedin two phases, initially with 0.4 mg of sublingual nitroglycerin andwith sublingual placebo, and then with oral ISDN, mean dose 29 mg,and oral placebo. Both phases of the study were conducted in a ran-
domized, double-blind, crossover manner. After ISDN was comparedto oral placebo, heart rate increased at 30 to 300 min (P < 0.01)
SUBLINGUAL NITROGLYCERIN has enjoyed long-standing and almost universal acceptance as an antianginalagent. The remarkable efficacy of this drug has led to its usenot only as a therapeutic agent but also as a standard forevaluating other antianginal agents' and even as a diagnostictool.2 Many attempts have been made to prolong the briefaction of sublingual nitroglycerin by altering both molecularstructure and method of administration. These attempts
From the Cardiology Section, Long Beach Veterans AdministrationHospital, and the University of California College of Medicine, Irvine,California.
Supported by VA Project Number 0366-02.Address for reprints: Daniel T. Danahy, M.D., Cardiology Section,
Veterans Administration Hospital, Long Beach, California 90822.Received June 17, 1976; revision accepted September 2, 1976.
(peak increase 18 beats/min at 60 min), and systolic blood pressuredecreased from 45 to 300 min (P < 0.005) (peak decrease 18 mm Hgat 60 min). Exercise time at 2 min after sublingual nitroglycerin in-creased 51% as compared to sublingual placebo (P < 0.001). AfterISDN was compared to oral placebo, exercise time increased 54% at1 hr (P < 0.005), 37% at 3 hr (P < 0.01), and 12% at 5 hr (NS).Twelve of 21 patients (57%) improved their exercise time until angina2 25% at I hr after oral ISDN. The exercise response to sublingualnitroglycerin was a good predictor of this response to oral ISDN.
have generated a long history of controversy, still un-resolved.3 16 Orally administered nitrates in particular havebeen subject to attack.'7- ' Needleman and associates,20working with rats, reported rapid and nearly completedegradation by the liver of orally administered nitrates.Thus it has been argued that there is no rational basis for theuse of orally administered nitrates.More recent hemodynamic studies, however, have caused
us to reexamine this issue. Decreases in arterial bloodpressure and left ventricular filling pressure following oralisosorbide dinitrate (ISDN) have been demonstrated inseveral carefully conducted studies in cardiac patients.20-24These hemodynamic effects suggested that an antianginaleffect might also be present. Careful review of previousstudies on the antianginal effect of oral isosorbide dinitrate
381
by guest on March 21, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 55, No 2, FEBRUARY 1977
suggested that inadequate dosage may have prevented thedemonstration of antianginal efficacy."7 58
Our study was designed to answer the following questions.Can hemodynamic effects from large, individually deter-mined doses of oral ISDN be demonstrated in patients withangina pectoris due to coronary heart disease but withoutcongestive heart failure? Can antianginal efficacy be dem-onstrated? What is the relationship between the response tosublingual nitroglycerin and the response to oral ISDN?
Methods
Twenty-one men between 42 and 64 years of age withdocumented coronary atherosclerotic heart disease andtypical effort angina pectoris were studied. Twenty patientshad either a history of a clearly documented myocardial in-farction and/or coronary angiographic demonstration ofgreater than 70% luminal narrowing in at least one majorcoronary artery. One patient (patient 12) gave a history ofmyocardial infarction which was not documented. One mmflat ST-segment depression developed with typical anginalpain during exercise electrocardiography in this patient. Allpatients signed consent forms approved by the hospitalHuman Studies Subcommittee.
All patients reported benefit from sublingual nitro-glycerin for relief or prevention of angina pectoris. Thepresence of any of the following excluded patients from thestudy: myocardial infarction or onset or significant changein angina pectoris within the previous 6 months; history,physical findings, or a liver function abnormality (serumglutamic oxaloacetic transaminase, bilirubin, albumin, or
total protein) consistent with liver disease; a blood pressure_ 150/100 mm Hg; or history, physical findings, or chestroentgenographic evidence of congestive heart failure. Noc-turnal angina without evidence of congestive heart failurewas not an excluding factor.A history of nocturnal angina on at least one occasion
could be elicited from eight study patients. Two of theseeight patients were receiving digoxin therapy, initiatedbecause of nocturnal angina. The digoxin therapy hadproduced no change in symptoms when it had been initiatedand no change occurred when the digoxin was stopped one
week prior to the study.Propranolol therapy was gradually tapered prior to the
study. No patient received propranolol, digitalis, or diureticsduring or for 72 hours prior to the study period. Nitrateswere given only as prescribed by the study protocol, and no
other vasodilators were received during or for 72 hours priorto the study period.
Patients were hospitalized for five days for this study.Practice exercise tests were performed on the first twohospital days. All patients had at least two practice exercisetests prior to definitive testing. Exercise testing was per-
formed in a sitting position on a Collins* constant load bicy-cle ergometer. The workload was increased by 25 watt in-crements every 3 min. The initial workload was chosen so
that angina pectoris developed between 3 and 6 min duringcontrol testing. Four patients had control exercise times of
less than 3 min despite an initial workload of only 25 watts.Patients were exercised to the onset of angina pectoris or, ifangina did not occur, to exhaustion. Exercise times weremeasured to the onset of angina but patients continued toexercise until blood pressure could be measured and an elec-trocardiographic strip recorded.
Simultaneous electrocardiographic leads II and V5 were
recorded via telemetry in the supine and sitting positionsbefore exercise and in the sitting position during exercise, atthe end of exercise, 30 sec after exercise, I min after exer-cise, and at min intervals for at least 1 to 6 min after exer-
cise. Heart rates were measured from the electrocardio-grams. Blood pressures were recorded using a mercurysphygmomanometer with the patient in the supine and sit-ting positions before exercise and in the sitting position atthe end of exercise.
Test doses of oral ISDN were administered on hospitaldays to 3, but none were given for at least 16 hours prior toexercise testing. Isosorbide dinitrate dosage was individuallydetermined by side effects and by the response of heart rateand blood pressure in the sitting position from I to 3 hoursafter administration. An attempt was made to maximizeISDN dosage while avoiding significant headache or a
precipitous fall in blood pressure. All patients had at least a
10 mm fall in systolic blood pressure and/or a 10 beat/minincrease in heart rate following the chosen dose of ISDNduring this dose selection phase.On the third through fifth hospital days, definitive exercise
testing was performed. On each of these three days, patientswere brought to the exercise laboratory in a fasting state at 8A.M. Fasting was continued for the duration of each day'stesting. No smoking was allowed during or for eight hoursprior to each day's testing.On the third hospital day, patients received two exercise
tests with two hour separations between the tests. Sublingualnitroglycerin 0.4 mg and sublingual placebo of identicalappearance were given 2 min prior to the beginning of exer-
cise in a double-blind, randomized, crossover manner. Bloodpressure and heart rate were determined in the sitting posi-tion immediately prior to drug administration and 2 minlater, immediately prior to exercise. Patients 1 through 4were tested with sublingual nitroglycerin and with sublingualplacebo approximately 2 to 3 months after they were testedwith oral ISDN.On the fourth and fifth hospital days, patients received a
control exercise test followed in 15 min by oral drug ad-ministration and then exercise tests at 1, 3, and 5 hours afterdrug administration. Patients received oral ISDN and oralplacebo of identical appearance in a randomized, double-blind, crossover manner.t In addition to blood pressure andheart rate determinations prior to and during each exercisetest, blood pressures and heart rates were measured in a sit-ting position at 15, 30, 45, 90, 120, 150, 240, and 270 minafter oral drug administration.The data were analyzed by our biostatistician with a com-
puter using Student's t-test for correlated means to deter-mine significance levels. Correlation coefficients were cal-culated using P-earson's product moment method.
*Warren E. Collins, Inc.tOral ISDN and oral placebo of identical appearance were supplied
through Dr. Clarence Denton, Ives Laboratories, New York, New York.
CIRCULATION382
by guest on March 21, 2018
http://circ.ahajournals.org/D
ownloaded from
ISOSORBIDE DINITRATE IN ANGINA/Danahy et al.
TABLE 1. Clinical DataISDN ISDN Initial
Prev Previous dose dose work1Pt. MI Noct ang CABG On P On N (mg) (mg/kg) (wv
1 yes yes no yes yes 50 .582 yes no yes n10 yes 25 .343 yes no yes yes yes 20 .244 no yes no yes yes 25 .375 yes yes yes no no 30 .386 yes no no no no 25 .327 yes no no yes no 30 .418 yes yes no yes no 25 .379 no no no yes no 25 .3710 no no no yes no 35 .5311 no yes yes yes no 25 .2412 no no no yes no 30 .4413 yes no no yes yes 40 .4914 yes no no no no 25 .3115 no no no yes no 20 .2016 yes yes no yes no 20 .2417 no no yes yes no 30 .3818 yes no no yes yes 35 .2719 yes yes no yes yes 40 .5120 yes yes yes yes no 20 .2421 yes no no yes no 30 .51Mean 29 .37
25i25
25
25
25
25
50
25
25
2525255025a2550
50
100
252525
Abbreviations: Prev MI = previous myocardial infarction; P = propra-nolol; Noct ang = nocturnal angina; CABG = coronary artery bypassgraft surgery; N = any nitrate other than sublingual nitroglycerin in themonth prior to study; ISDN = oral isosorbi(le dinitrate.
Results
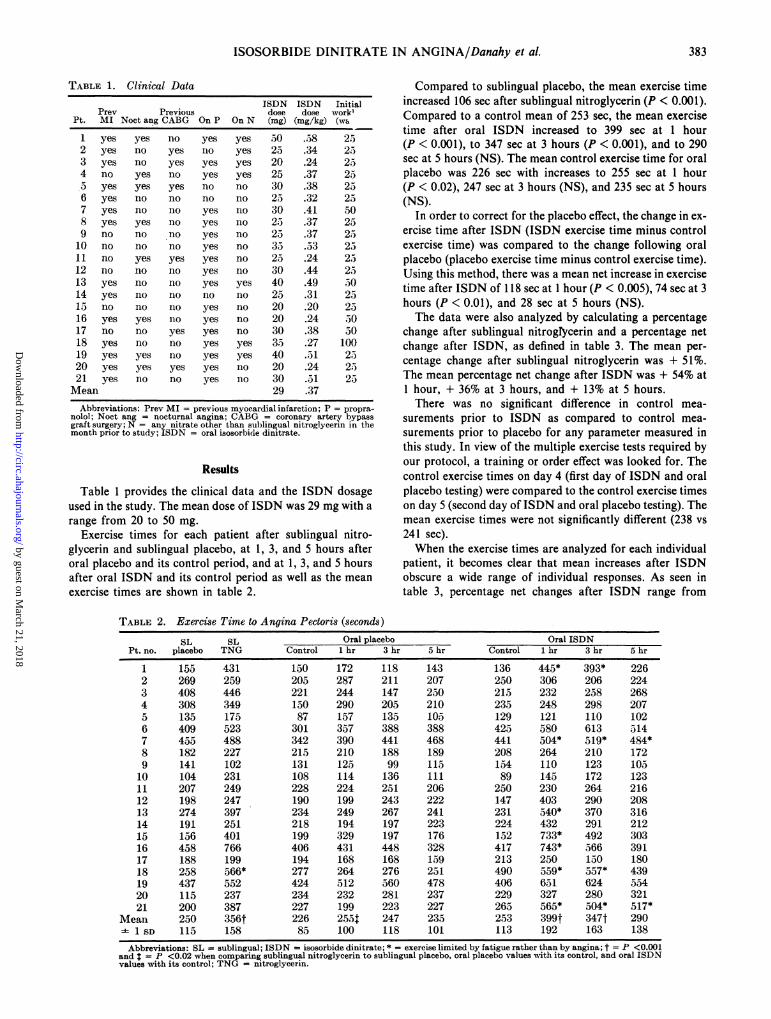
Table 1 provides the clinical data and the ISDN dosageused in the study. The mean dose of ISDN was 29 mg with arange from 20 to 50 mg.
Exercise times for each patient after sublingual nitro-glycerin and sublingual placebo, at 1, 3, and 5 hours afteroral placebo and its control period, and at 1, 3, and 5 hoursafter oral ISDN and its control period as well as the meanexercise times are shown in table 2.
Compared to sublingual placebo, the mean exercise timeincreased 106 sec after sublingual nitroglycerin (P < 0.001).Compared to a control mean of 253 sec, the mean exercisetime after oral ISDN increased to 399 sec at 1 hour(P < 0.001), to 347 sec at 3 hours (P < 0.001), and to 290sec at 5 hours (NS). The mean control exercise time for oralplacebo was 226 sec with increases to 255 sec at 1 hour(P < 0.02), 247 sec at 3 hours (NS), and 235 sec at 5 hours(NS).
In order to correct for the placebo effect, the change in ex-
ercise time after ISDN (ISDN exercise time minus controlexercise time) was compared to the change following oralplacebo (placebo exercise time minus control exercise time).Using this method, there was a mean net increase in exercisetime after ISDN of 118 sec at 1 hour (P < 0.005), 74 sec at 3hours (P < 0.01), and 28 sec at 5 hours (NS).The data were also analyzed by calculating a percentage
change after sublingual nitrogNcerin and a percentage netchange after ISDN, as defined in table 3. The mean per-centage change after sublingual nitroglycerin was + 51%.The mean percentage net change after ISDN was + 54% at1 hour, + 36% at 3 hours, and + 13% at 5 hours.There was no significant difference in control mea-
surements prior to ISDN as compared to control mea-surements prior to placebo for any parameter measured inthis study. In view of the multiple exercise tests required byour protocol, a training or order effect was looked for. Thecontrol exercise times on day 4 (first day of ISDN and oralplacebo testing) were compared to the control exercise timeson day 5 (second day of ISDN and oral placebo testing). Themean exercise times were not significantly different (238 vs
241 sec).When the exercise times are analyzed for each individual
patient, it becomes clear that mean increases after ISDNobscure a wide range of individual responses. As seen intable 3, percentage net changes after ISDN range from
TABLE 2. Exercise Time to Angina Pectoris (seconds)
SL SL Oral placebo Oral ISDNPt. no. placebo TNG Control 1 hr 3 hr 5 hr Control 1 hr 3 hr 5 hr
1 155 431 150 172 118 143 136 445* 393* 2262 269 259 205 287 211 207 250 306 206 2243 408 446 221 244 147 250 215 232 258 2684 308 349 150 290 205 210 235 248 298 2075 135 175 87 157 135 105 129 121 110 1026 409 523 301 357 388 388 425 580 613 5147 455 488 342 390 441 468 441 504* 519* 484*8 182 227 215 210 188 189 208 264 210 1729 141 102 131 125 99 115 154 110 123 10510 104 231 108 114 136 111 89 145 172 12311 207 249 228 224 251 206 250 230 264 21612 198 247 190 199 243 222 147 403 290 20813 274 397 234 249 267 241 231 540* 370 31614 191 251 218 194 197 223 224 432 291 21215 156 401 199 329 197 176 152 733* 492 30316 458 766 406 431 448 328 417 743* 566 39117 188 199 194 168 168 159 213 250 150 18018 258 566* 277 264 276 251 490 559* 557* 43919 437 552 424 512 560 478 406 651 624 55420 115 237 234 232 281 237 229 327 280 32121 200 387 227 199 223 227 26a 565* 504* 517*
Mean 250 356t 226 255t 247 235 253 399t 347t 290- 1 SD 115 158 85 100 118 101 113 192 163 138Abbreviations: SL = sublingual; ISDN = isosorbide dinitrate; * = exercise limited by fatigue rather than by angina; t = P <0.001
and t = P <0.02 when comparing sublingual nitroglycerin to sublingual placebo, oral placebo values with its control, and oral ISDNvalues with its control; TNG = nitroglycerin.
383
by guest on March 21, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 55, No 2, FEBRUARY 1977
TABLE 3. Percentage Change in Exercise Time after Sub-lingual Nitroglycerin and Percentage Net Change in ExerciseTime after Oral Isosorbide Dinitrate
% net change % net change % net change% change 1 hr after 3 hr after 5 hr after
Pt. after TNG* ISDNt ISDNt ISDNt
1 +178 +212 +210 + 732 - 4 - 18 - 21 - 113 + 9 - 1 + 53 + 124 + 13 - 87 -10 - 52. + 30 - 86 -70 - 416 + 28 + 17 + 15 - 87 + 7 0 - 11 - 278 + 25 + 29 + 14 - t9 - 28 - 24 + 4 - 2010 +122 + 57 + 67 + 3511 + 20 - 6 - 4 - 412 + 25 +169 + 69 + 2413 + 45 +128 + 46 + 3414 + 31 +104 + 39 - 715 +157 +317 +225 +11116 + 67 + 72 + 26 + 1317 + 6 + 30 - 17 -18 +119 + 19 + 14 - 319 + 26 + 39 + 22 + 2320 +106 + 44 + 2 + 3921 + 94 +125 + 92 + 95
Mean + 51 + 54 + 36 + 13
Abbreviations: TNG sublingual nitroglycerin; ISDN = oral isosorhidedinitrate; ET = exercise time.*% change after TNG (TNG ET minus placeho ET) X 100changeafer TNG placeho ET
(ISDN ET minus control ET) X 100t% net change after ISDN control ET ......
(placebo ET minus control ET) X 100control ET
+ 317% to - 87%. Comparison of the 12 patients whoshowed a 25% or greater net improvement in exercise time at1 hour after ISDN with the other nine patients revealed nosignificant difference in age, prevalence of previous myocar-dial infarction, medications used prior to the study, ISDNdose used during the study, control exercise time, or controlexercise time times initial workload.
Eleven of 21 patients (52%) increased their exercise time_ 25% after both sublingual nitroglycerin and oral ISDN.Six of 21 patients (29%) failed to increase their exercise time_ 25% after both sublingual nitroglycerin and oral ISDN.
C,,f +14-a 2-
1- 8cc 6
4
w 2Io
- 2
- 4z< - 6u - 8
Three of 21 patients (14%) increased their exercise time_ 25% after sublingual nitroglycerin but not after oralISDN. One of 21 patients (5%) increased his exercise timeby 25% or more after oral ISDN but not after sublingualnitroglycerin. The change in exercise time after sublingualnitroglycerin correlated with the net change in exercise timeat 1 hour after oral ISDN (r = 0.65), and at 3 hours afteroral ISDN (r = 0.69).
Seven patients were able to exercise to exhaustion withoutdeveloping angina pectoris after ISDN (table 2). All of thecontrol exercise tests and all of the exercise tests after oraland sublingual placebo ended with angina. One patient exer-
cised to exhaustion without developing angina afternitroglycerin. When patients exercised to angina, the inten-sity and duration of their anginal discomfort was essentiallyconstant for each patient for all tests.The depth of the ST-segment response to exercise and the
duration of ST-segment depression after exercise were alsoconstant for the majority of patients, regardless of changesin the exercise time required to reach an anginal endpoint.None of 21 patients showed a worsening of the ST-segmentresponse after either ISDN or nitroglycerin. Five of 21patients (24%) (7, 9, 12, 18, and 19) had 2 1 mm less ST-segment depression after exercise following sublingual nitro-glycerin. Five of 21 patients (24%) (7, 9, 12, 16, and 18) had_ mm less ST-segment depression in response to exerciseat 1 hour after ISDN. In four of these five patients, the im-provement in ST-segment depression after ISDN persistedthrough 3 hours, and in two of these five patients, the im-provement persisted through 5 hours. Three of the fivepatients who showed less ST-segment depression afterISDN were patients who exercised to exhaustion withoutdeveloping angina.The mean changes in resting heart rate and systolic blood
pressure in the sitting position and their statisticalsignificance are graphically displayed in figures 1 and 2. Theheart rate increased significantly from 15 min through 300min with a peak net increase ([ISDN heart rate minus con-
trol heart rate] minus [placebo heart rate minus controlheart rate]) of 18 beats/min at 60 min after drug administra-
I
E
E
a.
CzY,I0 2 3 4 5
HOURS AFTER DRUG
FIGURE 1. Mean changes in resting heart rate in the sitting posi-tion after oral isosorbide dinitrate and after oral placebo ± I SEM.
The difference between isosorbide dinitrate and placebo is signifi-cant at all plotted points; at 15 min, P < 0.02; at 45 min, P < 0.01;at the other points, indicated by triangles, P < 0.005.
0 2 3 4 5HOURS AFTER DRUG
FIGURE 2. Mean changes in resting systolic blood pressure in thesitting position after isosorbide dinitrate and after oral placebo ± ISEM. The difference between isosorbide dinitrate and placebo wasnot significant at 15 min; at 30 min, P < 0.05; at the other points,indicated by triangles, P < 0.005.
384 CIRCULATION
by guest on March 21, 2018
http://circ.ahajournals.org/D
ownloaded from

ISOSORBIDE DINITRATE IN ANGINA/Danahy et al.
tion. Systolic blood pressure decreased significantly from 30min through 300 min with a peak net decrease of 18 mm Hgat 60 min. Diastolic blood pressure decreased significantlyfrom 90 min through 270 min with a peak net decrease of 8mm Hg at 180 min. Heart rate and blood pressure recordedin the supine position showed similar changes but were ofless magnitude than those found in the sitting position.The mean net increase in resting heart rate, measured 2
min after nitroglycerin, was 11 beats/min (P < 0.001). Themean net decrease in systolic blood pressure after nitro-glycerin was 11 mm Hg (P < 0.001).
Table 4 shows the mean values for heart rate, systolic anddiastolic blood pressure, and product of systolic bloodpressure times heart rate at the end of exercise after sub-lingual placebo and sublingual nitroglycerin, at 1, 3, and 5hours after oral placebo and its control period, and 1, 3, and5 hours after oral ISDN and its control period.The mean heart rate at the end of exercise was 13
beats/min greater after sublingual nitroglycerin than aftersublingual placebo (P < 0.001). The mean heart rate at theend of exercise had a net increase of 12 beats/min at 1 hourafter ISDN (P < 0.001), a net increase of 5 beats/min at 3hours after ISDN (P < 0.001), and a net increase of 5beats/min at 5 hours after ISDN (P < 0.005). Neither oralISDN nor sublingual nitroglycerin produced a significantchange in the mean systolic blood pressure at the end of ex-
ercise.The mean product of systolic blood pressure times heart
rate/100 at the end of exercise increased by 21 after sub-lingual nitroglycerin compared to after sublingual placebo(P < 0.001). The mean product of systolic blood pressuretimes heart rate/100 at the end of exercise had a net increaseof 23.5 at 1 hour after ISDN (P < 0.005), a net increase of10 at 3 hours after ISDN (P < 0.05), and a net increase of6.9 at 5 hours after ISDN (NS).Comparison of the subgroups of patients with and without
nocturnal angina revealed no significant difference in exer-
cise times or in heart rate and blood pressure data.Analysis of the heart rate and blood pressure data for the
subgroup of patients with a good response to ISDN (2 25%net increase in exercise time at 1 hour) and the subgroupwith a poor response to ISDN (< 25% net increase in exer-
cise time at 1 hour) showed significant changes in both sub-groups.
DiscussionFigures 1 and 2 illustrate that a consistent and prolonged
hemodynamic response to large oral doses of ISDN was
demonstrated in this study. The peak effect on both heartrate and systolic blood pressure occurred at 1 hour afterISDN but significant changes were noted from 15 minthrough the termination of the study at 5 hours. Franciosaand associates have recently established that hemodynamiceffects occur after oral ISDN in patients with congestiveheart failure.2' The question has been raised whether a
similar hemodynamic effect will also occur in patientswithout heart failure, patients in whom the hepaticmetabolism of orally administered nitrates may be more
efficient. Recent reports by Willis and associates,2' Kaspar-ian and co-workers,2' and Poliner and associates24 indicatethat hemodynamic effects do occur following oral ISDN inpatients with normal hepatic function and without heartfailure. The results reported here further confirm this fact.The studies of Needleman and associates have frequently
been quoted as proving the futility of administering nitratesorally.2e Needleman's studies were performed in rats and theconclusions were based on an inability to demonstrate a
vasodepressor response to nitrates administered orally or
directly into the portal vein. Since an unequivocal hemo-dynamic response to oral ISDN has now been demonstratedin patients both with and without congestive heart failure,Needleman's data would no longer appear relevant to con-
siderations regarding patients. Needleman's studies as wellas other studies25 do suggest that the active vasodilatingcompound or compounds must be a metabolite of ISDNrather than ISDN itself.The heart rate and product of systolic blood pressure
times heart rate at the end of exercise increased both afternitroglycerin and after ISDN. These findings followingnitroglycerin are consistent with the reports of Goldsteinand associates,7 Detry and Bruce,'I and Robinson.27 Clausenand Trap-Jensen'8 also showed an increase in product ofsystolic blood pressure times heart rate at angina after nitro-glycerin but the increase was not statistically significant.
The product of systolic blood pressure times heart ratehas been used as an index of myocardial oxygen demand butit is both an indirect and incomplete index. Nitrates are
known to alter both left ventricular ejection time7' 8 and leftventricular volume,29> 30 both of which influence myocardial
TABLE 4. Mean Heart Rate, Systolic and Diastolic Blood Pressure, and Product of Systolic Blood PressureTimes Heart Rate at End of Exercise after Sublingual Placebo, Sublingital Nitroglycerin, Oral Placebo and ItsControl, and Isosorbide Dinitrate and Its Control
SL SL Oral placebo Oral isosorbide dinitrateplacebo TNG Control 1 hr 3 hr 5 hr Control 1 hr 3 hr 5 hr
HR (beats/min) 118 131* 117 117 115 116 116 128* 121T 121t1 SD 14 15 15 16 16 17 14 17 20 19
SBP (mm Hg) 169 168 159 158 156 158 161 163 157 1561 SD 28 31 28 28 29 28 29 32 30 29
DBP (mm Hg) 93 94 92 92 94 92 92 90 88t 89t1SD 10 12 11 11 11 10 10 12 9 10
SBP X HR 199 220* 185 184 179 181 187 210t 191 1911 SD 41 47 3a 37 38 36 43 53 50 48
*P <0.001.tP <0.01.tP <0.05.Sublingual nitroglycerin is compared to sublingual placebo; oral placebo values and oral isosorbide dinitrate values are compared to
their respective controls.Abbreviations: SL = sublingual; TNG = nitroglycerin; HR = heart rate; SBP = systolic blood pressure; DBP = distolic blood
pressure; SBP X HR = product of systolic blood pressure times heart rate/100.
385
by guest on March 21, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 55, No 2, FEBRUARY 1977
oxygen consumption. Since neither of these parameters, normany others, were measured in this study, no conclusionscan be drawn about how nitrates are changing the myo-cardial oxygen supply and demand equation.The exercise times in this study clearly establish the acute
antianginal efficacy of oral ISDN when used in high doses.The peak effect occurred at 1 hour with a significant im-provement in exercise time persisting through 3 hours inmost patients who responded, and, persisting through 5hours in some patients. A number of previous studies usingoral ISDN as an antianginal agent'7 18 failed to show abeneficial effect. The large, individualized doses of ISDNemployed in this study are likely a major factor accountingfor the differences in results although there are some reportsof antianginal effect at lower doses.1 31
The duration of antianginal effect demonstrated in thisstudy is probably also a dose-related phenomenon with theprolonged efficacy reflecting, in part, the high doses used.Reichek and associates,9 using nitroglycerin ointment, Win-sor and Berger,' using oral controlled release nitroglycerin,and Lee and associates,32 using ISDN capsules, havereported antianginal efficacy for 3 hours or longer. Glancyand associates33 also reported improved exercise time toangina at 2 hours after oral ISDN. In contrast, thehemodynamic and antianginal effects of sublingualnitroglycerin have generally been found to be less than 1hour in duration.4 6, 7, 22
Consideration solely of mean data obscures some verypertinent information about individual patient response. It isclear that there was a very wide range of response in exercisetimes to ISDN. Some patients showed dramatic improve-ment while in others, ISDN may have had a detrimentaleffect. Attempts to classify patients as good responders arenecessarily arbitrary, particularly in the absence of multipleretests to limit random scatter of exercise times in individualpatients. Thus, figures for the number of patients who weregood responders or poor responders are only rough ap-proximations. It is quite clear from the data that the exerciseresponse to ISDN was not uniform.
Additional light is shed on this problem when the responseto sublingual nitroglycerin is considered. The exerciseresponse to sublingual nitroglycerin is a good predictor ofthe response to oral ISDN. Six of 21 patients (29%) failed torespond (less than 25% net increase in exercise time) toeither drug. These patients might thus be termed nitratenonresponders rather than oral ISDN nonresponders. Thatsome patients with angina pectoris will not have a beneficialresponse to nitrates, including sublingual nitroglycerin, haslong been recognized2' 34 but curiously overlooked in manystudies evaluating long-acting nitrates.35A number of factors need to be considered as explanations
for these therapeutic failures. It is important to give anadequate dose of nitrate. Although we used only a singlestandard dose of sublingual nitroglycerin, we deliberatelymaximized ISDN doses in an attempt to eliminatetherapeutic failures due to insufficient dosage of ISDN.Significant heart rate and blood pressure changes occurredin the subgroup of patients who showed a poor exerciseresponse (< 25% improvement) after oral ISDN. Significantheart rate and blood pressure changes also occurred in the
patients who showed a poor exercise response after sub-lingual nitroglycerin. These hemodynamic changes suggestthat inadequate dosage is not the explanation for thetherapeutic failure of nitrates in these particular patients.An overdose of nitrates might also prevent the beneficial
effect on exercise performance, but the pattern of responsewas not suggestive of a nitrate overdose in any patient. Aplausible but untested hypothesis for the therapeutic failureof nitrates in some patients is that the net effect of the com-plex nitrate-induced hemodynamic alterations does notchange or influences adversely the balance of myocardialoxygen supply and demand.A consideration of untoward effects is in order when using
ISDN doses of the magnitude employed in this study.Marked changes in resting blood pressure and heart raterecorded in the sitting position occurred at its peak effect. Inonly one instance did any adverse effect occur as a result ofthese hemodynamic changes. Patient' 13 complained oflightheadedness while sitting on the bicycle immediatelyprior to his exercise test 1 hour after ISDN administration.His blood pressure at this time was 84/74 mm Hg as com-pared to a control blood pressure of 114/89 mm Hg. Thepatient was allowed to lie supine for several minutes beforeproceeding with the exercise test. His exercise time increasedby 134% compared to the control value.
Headaches occurred in seven of 21 patients (33%) follow-ing sublingual nitroglycerin and in 10 of 21 patients (48%)following ISDN. In several of these patients, headaches oc-curred only while exercising. The headaches following ISDNwere most frequent and of greatest intensity approximately1 hour after the ISDN dose. However, six of the 10 patientswho experienced headache had at least a mild headache dur-ing the exercise test 5 hours after ISDN. In no instance didheadache interfere with the testing protocol or require cessa-tion of exercise.Some caution is advised about conclusions to be drawn
from these data. The demonstration of improved exercisetolerance following a single dose of a nitrate drug does notestablish its long-term efficacy. Indeed, there is need for cau-tion regarding the use of drugs which produce chronicvasodilatation. The industrial medicine literature is repletewith descriptions of withdrawal syndromes in workerschronically exposed to nitrate powder and vapor.36 38
In addition to this problem of dependence, there isevidence of tolerance developing to nitrate effects,39' 4 in-cluding the common observation of rapid tolerance tonitrate-induced headaches. Until more information isavailable regarding the long-term effects of high doses ofnitrates, we feel that caution is advised for continuousnitrate prophylaxis, particularly in patients with only mildangina pectoris.
Evaluation of nitrates as antianginal agents is difficult.Variations in study protocol, doses utilized, and the popula-tion of patients studied have probably all contributed to thelong-standing controversy regarding nitrates. This study, aswell as other recent studies, establishes that orally ad-ministered ISDN has a prolonged hemodynamic effect aswell as a prolonged antianginal effect. However, not allpatients with angina pectoris benefit from oral ISDN.Further work is needed to predict which patients will have a
386 CIRCULATION
by guest on March 21, 2018
http://circ.ahajournals.org/D
ownloaded from

ISOSORBIDE DINITRATE IN ANGINA/Danahy et al.
good antianginal response. Further work is also required toestablish the efficacy and safety of the long-term use ofISDN when given in effective doses.
Acknowledgment
The authors wish to express their appreciation to Louis Raggio fortechnical assistance and to Clifford Risk, Ph.D., for biostatistical analysis ofthe data.
References1. Russek HI: The therapeutic role of coronary vasodilators: Glyceryl
trinitrate, isosorbide dinitrate, and pentaerythritol tetranitrate. Am JMed Sci 252: 9, 1966
2. Horwitz LD, Herman MV, Gorlin R: Clinical response to nitroglycerinas a diagnostic test for coronary artery disease. Am J Cardiol 29: 149,1972
3. Aronow WS, Chesluk HM: Sublingual isosorbide dinitrate therapy ver-sus sublingual placebo in angina pectoris. Circulation 41: 869, 1970
4. Klaus AP, Zaret BL, Pitt BL, Ross RS: Comparative evaluation of sub-lingual long-acting nitrates. Circulation 48: 519, 1973
5. Winsor T, Berger HJ: Oral nitroglycerin as a prophylactic antianginaldrug: Clinical, physiologic, and statistical evidence of efficacy based on a
three-phase experimental design. Am Heart J 90: 611, 19756. Sweatman T, Strauss G, Selzer A, Cohn KE: The long-acting hemo-
dynamic effects of isosorbide dinitrate. Am J Cardiol 29: 475, 19727. Goldstein RE, Rosing DR, Redwood DR, Beiser GD, Epstein SE:
Clinical and circulatory effects of isosorbide dinitrate. Circulation 43:629, 1971
8. Hurwitz L, Naughton J, Gorman PA, Miller A: Isosorbide dinitrate andcardiovascular adaptation to exercise. Chest 69: 10, 1976
9. Reichek N, Goldstein RE, Redwood DR, Epstein SE: Sustained effectsof nitroglycerin ointment in patients with angina pectoris. Circulation 50:348, 1974
10. Battock DJ, Alvarez H, Chidsey CA: Effects of propranolol and isosor-bide dinitrate on exercise performance and adrenergic activity in patientswith angina pectoris. Circulation 39: 157, 1969
11. Freis ED, Gaffney TE, Kirkendall W, Marcus Fl, Nickerson M, PearceML: Report of the panels on cardiovascular drugs from the drug efficacystudy. Circulation 41: 149, 1970
12. Aronow WS: The medical treatment of angina pectoris. V. Long-actingnitrites as antianginal drugs. Am Heart J 84: 567, 1972
13. Aronow WS: Management of stable angina. N Engl J Med 289: 516,1973
14. Winsor T: Oral nitrates: Efficacious? Ann Intern Med 78: 457, 197315. Goldstein RE, Epstein SE: Nitrates in the prophylactic treatment of
angina pectoris. Circulation 48: 917, 197316. Krantz JC Jr, Leake CD: The gastrointestinal absorption of organic
nitrates. Am J Cardiol 36: 407, 197517. Aronow WS, Kaplan MA: Evaluation of propranolol and of isosorbide
dinitrate in angina pectoris. Curr Ther Res 11: 80, 196918. Goldbarg AN, Moran JF, Butterfield TK, Nemickas R, Bermudez GA:
Therapy of angina pectoris with propranolol and long-acting nitrates.Circulation 40: 847, 1969
19. Livesley B, Catley PF, Campbell RC, Oram S: Double-blind evaluation
of verapamil, propranolol, and isosorbide dinitrate against a placebo inthe treatment of angina pectoris. Br Med J 1: 375, 1973
20. Needleman P, Lang S, Johnson EM Jr: Organic nitrates: Relationshipbetween biotransformation and rational angina pectoris therapy. J Phar-macol Exp Therap 181: 489, 1972
21. Franciosa JA, Mikulic E, Cohn JN, Jose E, Fabie A: Hemodynamiceffects of orally administered isosorbide dinitrate in patients with con-gestive heart failure. Circulation 50: 1020, 1974
22. Willis WH Jr, Russell RO Jr, Mantle JA, Ratshin RA, Rackley CE:Hemodynamic effects of isosorbide dinitrate vs nitroglycerin in patientswith unstable angina. Chest 69: 15, 1976
23. Kasparian H, Wiener L, Duca PR, Gottlieb RS, Brest AN: Comparativehemodynamic effects of placebo and oral isosorbide dinitrate in patientswith significant coronary artery disease. Am Heart J 90: 68, 1975
24. Poliner L, Ritter W, Wohl A, Nixon JV, Willerson JT: The comparativehemodynamic effects of oral and sublingual isosorbide dinitrate inpatients with coronary insufficiency. (abstr) Clin Res 24: 5A, 1976
25. Sisenwine SF, Ruelius HW: Plasma concentrations and urinary excretionof isosorbide dinitrate and its metabolites in the dog. J Pharmacol ExpTher 176: 296, 1971
26. Detry JMR, Bruce RA: Effects of nitroglycerin on "maximal" oxygen in-take and exercise electrocardiogram in coronary heart disease. Circula-tion 43: 155, 1971
27. Robinson BF: Mode of action of nitroglycerin in angina pectoris.Correlation between haemodynamic effects during exercise and preven-tion of pain. Br Heart J 30: 295, 1968
28. Clausen JP, Trap-Jensen J: Heart rate and arterial blood pressure duringexercise in patients with angina pectoris. Effects of training and of nitro-glycerin. Circulation 53: 436, 1976
29. Dove JT, Shah PM, Schreiner BF: Effects of nitroglycerin on left ventric-ular wall motion in coronary artery disease. Circulation 49: 682, 1974
30. Burggraf GW, Parker JO: Left ventricular volume changes after amylnitrite and nitroglycerin in man as measured by ultrasound. Circulation49: 136, 1974
31. Zetterquist S, Furberg C, Ringqvist I, Soderholm B: Separate and com-bined effects of pindolol and isosorbide dinitrate in standardized exercisetests of patients with angina pectoris. Curr Ther Res 17: 139, 1975
32. Lee G, Mason DT, Amsterdam EA, DeMaria A: Improved exercisetolerance for six hours following isosorbide dinitrate capsules in patientswith ischemic heart disease. (abstr) Am J Cardiol 37: 150, 1976
33. Glancy DL, Richter MA, Ellis EV: Effects of swallowed isosorbidedinitrate on blood pressure, heart rate and exercise tolerance in patientswith coronary artery disease. (abstr) Circulation 52 (suppl II): II-189,1975
34. Riseman JEF: The treatment of angina pectoris. N Engl J Med 261:1017, 1959
35. Tremblay G, Biron P, Proulx A: Quantification pitfalls in comparativestudies of antianginal therapies. Am Heart J 89: 521, 1975
36. Lange RL, Reid MS, Tresch DD, Keelan MH, Bernhard VM, CoolidgeG: Nonatheromatous ischemic heart disease following withdrawal fromchronic industrial nitroglycerin exposure. Circulation 46: 666, 1972
37. Klock JC: Nonocclusive coronary disease following withdrawal fromchronic industrial nitroglycerin exposure. Am Heart J 89: 510, 1975
38. Lund RP, Haggendal J, Johnsson G: Withdrawal symptoms in workersexposed to nitroglycerine. Br J Industr Med 25: 136, 1968
39. Schelling JL, Lasagna L: A study of cross-tolerance to circulatory effectsof organic nitrates. Clin Pharmacol Ther 8: 256, 1967
40. Zelis R, Mason DT: Isosorbide dinitrate. Effect on the vasodilatorresponse to nitroglycerin. JAMA 234: 166, 1975
387
by guest on March 21, 2018
http://circ.ahajournals.org/D
ownloaded from

D T Danahy, D T Burwell, W S Aronow and R PrakashSustained hemodynamic and antianginal effect of high dose oral isosorbide dinitrate.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1977 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.55.2.381
1977;55:381-387Circulation.
http://circ.ahajournals.org/content/55/2/381the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on March 21, 2018
http://circ.ahajournals.org/D
ownloaded from