susanne)hernes,)ph.d,)cand.med.) haraldsplass)diakonale...
TRANSCRIPT

Pneumonier hos eldre
Susanne Hernes, Ph.d, Cand.med. Haraldsplass Diakonale Sykehus Sørlandet Sykehus Arendal

Dødelighet pneumoni
0
2000
4000
6000
8000
10000
12000
14000
16000
Alder <10 10-‐19 20-‐29 30-‐39 40-‐49 50-‐59 60-‐69 70-‐79 >80
KummulaJvt antall døde av pneumoni i Norge 2004-‐2013
Antall døde
www.ssb.no



InterrelaJonship of risk factors, acute illness and outcomes in CAP
Sligl. Curr Opin Infect Dis. 2011 Apr;24(2):142-‐7

InterrelaJonship of risk factors, acute illness and outcomes in CAP
Sligl. Curr Opin Infect Dis. 2011 Apr;24(2):142-‐7

FIT INTERMEDIATE
FRAIL
FYSISK
FUNKSJON
KOMORBIDITET
ERNÆRINGS-‐
STATUS
KOGNITIV FUNKSJON
MEDIKAMENTER
Kristjansson. Crit Rev Oncol Hematol. 2010;76: 208-‐217.

Andre faktorer
AnJpsykoJka
Protonpumpe inhibitorer ?
KorJkosteroider (tabl/inhalasjon)
ACE-‐ hemmere
StaJner
Myles.Pharmacoepidem Drug Safety 2009 Vol 18 (4) 269–275 Knop. JAGS 2008 56 (4) 661–666

Munnhulen
• Plakk • Periodontale lommer.
• Tannproteser under søvn.
Intervensjon!
www.mouthville.com
Pace. Dysphagia 2010, 25 (4) 307-‐322 Linuma. JDR October 7, 2014 (epub)
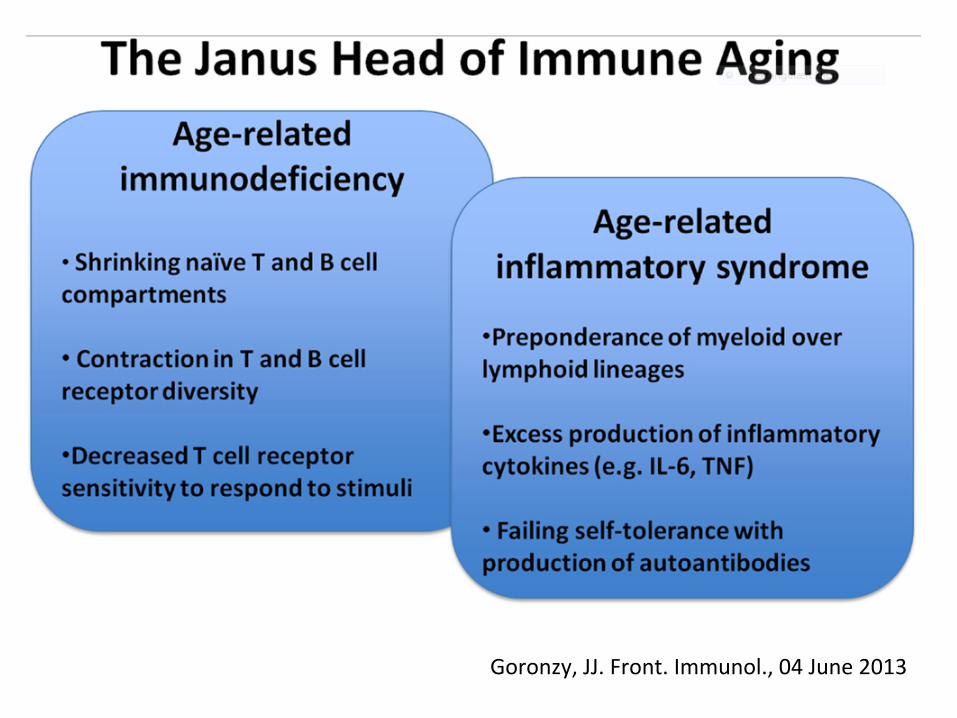
Goronzy, JJ. Front. Immunol., 04 June 2013


‘in old age, pneumonia may be latent, coming on without chill, the cough and expectoraJon are slight, the physical signs ill-‐defined and changeable, and the consJtuJonal symptoms out of all proporJon. Importantly, fever may be absent’
Sir W. Osler, The Principles and PracJce of Medicine. 1893.

Radiologisk diagnosJkk av pneumoni hos eldre
– Forsinket infiltrat? Ingen skikkelige studier.
– Tilbakegang av infiltrat oppJl 2-‐4 ganger senere enn hos yngre.
El Solh. JAGS 2004. 52 (2), 224–229

Mikrobiologiske agens
• Pneumokokker • Hemophilus Influenzae • Staphylococcus Aureus • Virus
• Gram negaJve species • Atypiske mikrober • Tuberculose
RuJnediagnosJkk ved pneumoni gir eJologisk agens hos 20 % av sykehusinnlagte pasienter.
File TM2011 Clin Chest Med 32 (3):417-‐430

Mikrobiologiske prøver fra lumveiene
• Øvre respirasjonstraktus – Penselprøver fra nese – Penselprøver fra hals – Aspirasjon fra nese
• Nedre respirasjonstraktus – Bronchoalveolar lavage – Protected brush – Sputum

• Urin anJgen test • Blodkultur • Parret serumprøver
• HurJgtester for influenza og RS kan ikke brukes hos eldre!

Gullstandard ved eJologisk diagnosJkk av pneumoni?

Gullstandard ved eJologisk diagnosJkk av pneumoni?

Kan vi seqe likhetstegn?
David, Michelangelo

Transthorakal finnålsaspirasjon
• Aspirasjon av prøvemateriale direkte fra lungebetennelsen.
• Røntgengjennomlysning ved prøvetagning.
• EJologisk diagnose hos 70 % av de inkluderte.

Patient Blood culture
Sputum culture
Urinary antigen
Paired sera Oropharynx PCR
TFNA
1 - S.aur, H.inf
- M.pneumonia - S.aureus
2 S.pneumoniae Not repr S.pneumoniae - - S.pneumoniae 3 - No sample - M.pneumonia - - 4 - - - - - S.pneumoniae 5 - No sample - - - S.pneumoniae 6 - - - M.pneumonia M.pneumonia M.pneumonia
PI4 9 - M.cat - - - - 11 - Not repr S.pneumoniae - CorOC43 - 12 - - - - Rhinov - 13 - Not repr - - - S.pneumoniae
H.influenzae 15 - - - InflA1 - H.influenzae 16 - No sample S.pneumoniae - - S.pneumoniae 17 - - - M.pneumonia M.pneumonia M.pn.
H.inf 18 - - S.pneumoniae - - S.pn,
H.inf 20 - No sample - - - H.inf
Transthorakal finnålaspirasjon
Hernes, SS. Clin Microbiol Infect 2010

Patient Blood culture
Sputum culture
Urinary antigen
Paired sera Oropharynx PCR
TFNA
1 - S.aur, H.inf
- M.pneumonia - S.aureus
2 S.pneumoniae Not repr S.pneumoniae - - S.pneumoniae 3 - No sample - M.pneumonia - - 4 - - - - - S.pneumoniae 5 - No sample - - - S.pneumoniae 6 - - - M.pneumonia M.pneumonia M.pneumonia
PI4 9 - M.cat - - - - 11 - Not repr S.pneumoniae - CorOC43 - 12 - - - - Rhinov - 13 - Not repr - - - S.pneumoniae
H.influenzae 15 - - - InflA1 - H.influenzae 16 - No sample S.pneumoniae - - S.pneumoniae 17 - - - M.pneumonia M.pneumonia M.pn.
H.inf 18 - - S.pneumoniae - - S.pn,
H.inf 20 - No sample - - - H.inf
Transthorakal finnålaspirasjon
Hernes, SS. Clin Microbiol Infect 2010

The Human Microbiome
Nature, June 14. 2012

• KonJnuerlig flora i hele respirasjonstraktus? Charlson ES Am. J. Respir. Crit. Care Med. 2011;184(8):957-‐63
• Dynamisk utveksling mellom patogener og kolonister, ubalanse gir infeksjon?
Dickson. Lancet 2014;384(9944):691–702
• Nye angrepspunkter for behandling i fremJden?

Virus

Dødelighet
• Barn: – RS virus 1.2-‐5% – Influensa: <1%-‐5%
• Eldre: – Influensa 2-‐20 % – RS virus 2-‐9 % (50%?)
Falsey AR, Walsh EE (2000) Clin Microbiol Rev 13 (3):371-384
Lee N et al. (2013) Clin Infect Dis 57 (8):1069-1077 Ellis SE et al JAGS 51(6), 761-767
Szabo SM et al(2013) Paediatric respiratory reviews 13 Suppl 2:S1-8

RS-‐virus vs influensa Variable RSV
(N=607) Influenza (N=547)
p-value
Age, y, mean (SD) 75.1 (16.4) 74.7 (16.6) .650
Major systemic comorbidity 74.0 65.8 .003
Chronic lung disease 35.6 24.1 <.001
Pneumonia 42.3 36.7 0.006
Lower respiratory tract complications
71.9 55.6 <.001
Supplimentary oxygen therapy 67.9 59.0 .002
Ventilation, noninvasive/invasive 11.1 6.2 .003
30 day mortality 9.1 8.0 .538
Omarbeidet fra Lee N et al. (2013) Clin Infect Dis 57 (8):1069-1077
Sykehusinnlagte pasienter i Kina. Immunofluorescence analyser. 91.2% av influensapasientene fikk oseltamivir.

Lee N et al. (2013) Clin Infect Dis 57 (8):1069-1077
Kaplan-Meier survival curves of 607 adults hospitalized for respiratory syncytial virus (RSV) infection.
Overlevelse RS virus

Hvem bør testes for lumveisvirus?
• Betydelig lumveisinfeksjon hos små barn, eldre og personer med nedsaq immunforsvar.
• Ved pneumoni i alle aldre. • Ved spørsmål om epidemi.
• Ved akuq funksjonssvikt hos eldre i RS/influensa-‐sesongen.
Samdal (2004) Virale luftveisinfeksjoner, anbefalinger og sammendrag av forelesninger

Det meste i livet dreier seg om timing

Hvor skal prøven tas?
Gjennomsniqlig CT verdier for penselprøver fra hals og nese. En høy gjennomsniqlig CT verdi Jl svarer en lavere relaJv virusmenge i prøven. CT= Cycle treshold.
Hernes SS et al.(2011). Eur J Clin Microbiol Infect Dis 30 (2):159-165

Påvises virus lengre i nedre lumveier?
Mulrennan S. et al. PLoSONE 5 (9):e12849
Nedre lumveier
Øvre lumveier

PreanalyJske kjede
LAB
PRØVE-TAKING
HVEM ER SYK ?
FUNN AV VIRUS???

Sputum fremfor swabs??
Jeong, J Med Virol, epub May 6. 2014

Mixed infecJons
• Bakterie-‐bakterie
• Bakterie-‐virus
• Vanlig?? Avhengig av hvilke kriterier som legges Jl grunn…..
©Velica

Gir virusdiagnosen noen konsekvenser?
• Kortere liggeJd?
• Mindre bruk av anJbioJka?

• 583 pasienter fordelt i enten intervensjon eller kontrollgruppe.
• Real Jme PCR for 17 lumveispatogener.
• Informasjon Jl behandler i intervensjonsgruppen i løpet av 36 Jmer, i kontrollgruppen eqer 4 uker.
• Virus funnet hos 82% av pasientene. Wishaupt JO et (2011) Pediatrics 128 (5):e1113-1120
Liggetid og antibiotikabruk hos barn

LiggeJd og anJbioJkabruk hos barn
Wishaupt JO et (2011) Pediatrics 128 (5):e1113-1120
Intervention Group (N=298)
Control Group (N=285)
P
Hospital admissions, n (%) 223 (74.8) 211 (74) .825a
Time in hospital, mean ± SD(range), d
3.68 ± 2.68 (1-18)
3.96 ± 2.67 (1-15)
.170b
Antibiotic therapy initiated, n (%)
124 (41.6) 78 (27.4) .000a
Duration of antibiotic therapy if inititated, mean ± SD (range), d
6.52 ± 2.15 (1-14)
6.97 ± 2.86 (2-21)
.490b

Behovet for sykehusinnleggelse skyldes kliniske parametre som sykdommens alvorlighetsgrad, behov for oksygen og forstøverbehandling og ikke om pasienten har fåq påvist eq virus eller ikke.
LiggeJd og anJbioJkabruk hos barn
Wishaupt JO et (2011) Pediatrics 128 (5):e1113-1120

Kostnader ved sykehusinnleggelse og diagnosJkk hos voksne
• 107 voksne pasienter randomisert Jl en intervensjons-‐ eller kontrollgruppe
• Begge gruppene analysert med real Jme PCR, men kun i intervensjonsgruppen ble resultatet opplyst.
• Pasienter på intensivavdeling utelaq fra analysen.
• ”Treatment as usual”.
Oosterheert J J et al. Clin Infect Dis. 2005;41:1438-1444

• EJologisk diagnosJkk økte fra 21% Jl 43 %
• AnJbioJsk behandling avsluqet hos 6 (11%) av pasientene.
• Ingen forskjell i medisinsk behandling mellom de to gruppene
Oosterheert J J et al. Clin Infect Dis. 2005;41:1438-1444

Kostnader ved sykehusinnleggelse og diagnostikk
Oosterheert J J et al. Clin Infect Dis. 2005;41:1438-1444

Intervensjon ved CAP
• Tidlig mobilisering : 1.1 dager redusert liggeJd.
Mundy. Chest. 2003;124(3):883-‐889.
• Blåseflaske? Bjorqvist.Scand J Infect dis. 1997; 29 1):77-‐82
• Ernæring? Lindhardt. Danish Medical Journal [2013, 60(2):A4572]

• IdenJfikasjon av sykt individ kan være vanskelig.
• OpJmalisering av behandling også hos eldre.
• Tidlig mobilisering!

Takk for meg