susan k. laird, msn, rn clinical director/content lead cdc-info presentation to airs conference...
TRANSCRIPT
Susan K. Laird, MSN, RNClinical Director/Content Lead
CDC-INFO
Presentation to AIRS CONFERENCE
Reno, Nevada, June 1, 2009
Objectives
• The purpose of this workshop is to…
– Share CDC-INFO background, successes and challenges, and lessons learned.
– Identify CDC and CDC-INFO resources that are available for use every day and in emergency response.
Agenda
• Welcome and Introductions
• What is CDC-INFO?
• Background and Scope
• Role in Emergency Response
• Impact – Internal and External
• Questions/Discussion

What Is CDC-INFO?
CDC-INFO Vision
To be a trusted source that partners, providers, and the public come to for accurate, timely and consistent information.
What is CDC-INFO?
– Launched in 2005– CDC-INFO employs 94 staff at its National Contact
Center– Delivers health information 24/7/365 – Audience: Consumers, healthcare providers and
professionals – English and Spanish service
CDC-INFO workload:– More than 2.1 million telephone inquiries answered
since 2005– Over 200,000 e-mails answered since 2005– Distributes 9M publications annually
6
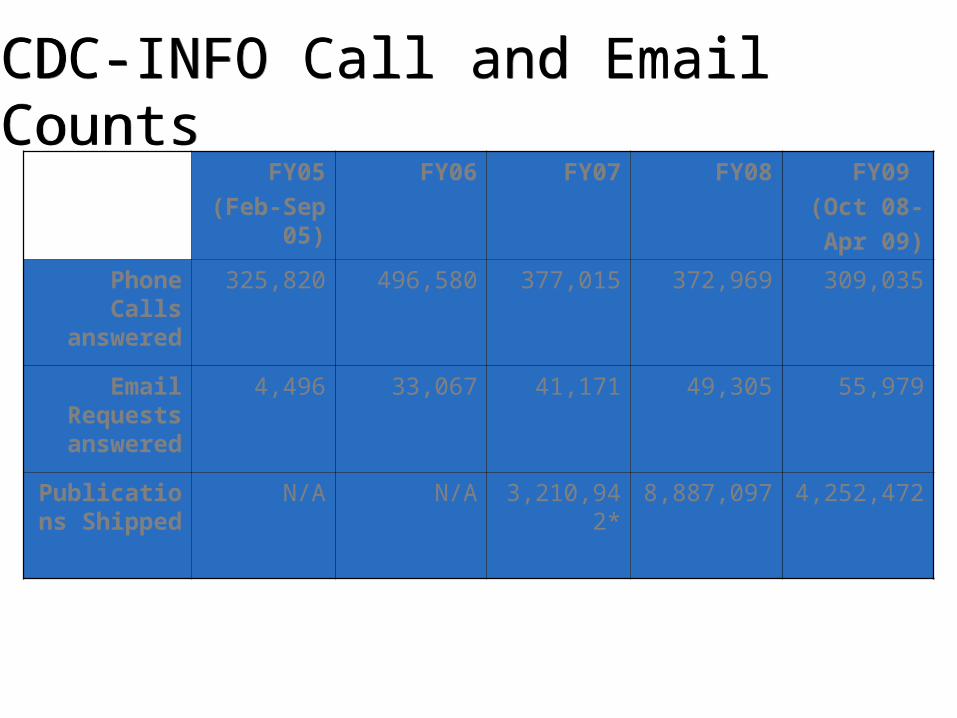
FY05
(Feb-Sep 05)
FY06 FY07 FY08 FY09
(Oct 08-
Apr 09)
Phone Calls answered
325,820 496,580 377,015 372,969 309,035
Email Requests answered
4,496 33,067 41,171 49,305 55,979
Publications Shipped
N/A N/A 3,210,942* 8,887,097 4,252,472
CDC-INFO Call and Email CountsCDC-INFO Call and Email Counts

CDC-INFO’s Role in Public Health and Communication
• Best Practices in eHealth Science and Research• Health Communication and Marketing
– Multi-channel modalities to address differing information-seeking needs, preferences and behaviors
– Audience Research: analyzing inquirers and demographics to inform CDC programs
• Public Health – Accurate, credible health information to positively impact health
behavior• “call to action”• Measure inquirers’ reported behavior change
– Health Disparities and Health Equity– Emergency Response
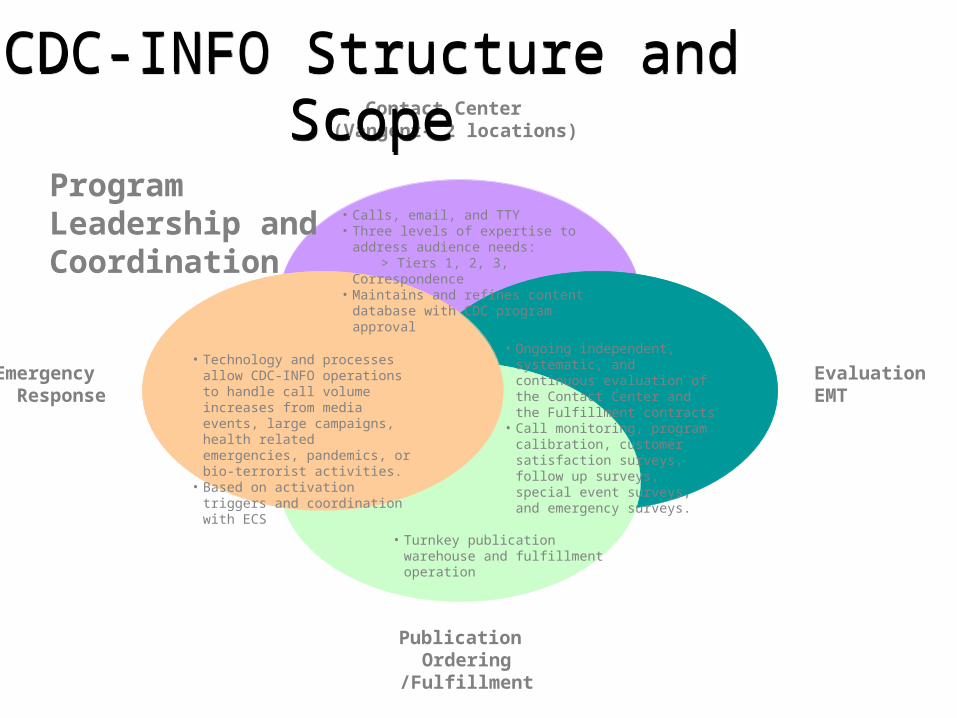
Contact Center (Vangent– 2 locations)
EvaluationEMT
Publication Ordering
/Fulfillment
Emergency Response
• Calls, email, and TTY• Three levels of expertise to address
audience needs: > Tiers 1, 2, 3, Correspondence• Maintains and refines content database with
CDC program approval
CDC-INFO Structure and Scope
CDC-INFO Structure and Scope
• Ongoing independent, systematic, and continuous evaluation of the Contact Center and the Fulfillment contracts
• Call monitoring, program calibration, customer satisfaction surveys, follow up surveys, special event surveys, and emergency surveys.
• Technology and processes allow CDC-INFO operations to handle call volume increases from media events, large campaigns, health related emergencies, pandemics, or bio-terrorist activities.
• Based on activation triggers and coordination with ECS
• Turnkey publication warehouse and fulfillment operation
Program Leadership and Coordination

Vangent Staffing (Dec. 2008)• Contact Center Operations
Management and Support - 8• Phoenix and Rockville CSRs – 60• Email Support- 13• Content Development (SRA)- 9• Training – 3 • Quality Assurance - 1
Everything we do should help the contact center staff better meet the needs of consumers, providers and CDC partners
Contact Center OperationsContact Center OperationsPhoenix, AZSupervisionTiers 1, 2, 3
Correspondence
RockvilleTier 3 Only
Location 2Tier 3 Only
TrainingContinuous:
Group &Self-paced
Quality AssuranceAll calls recorded1 in 25 calls per
Operator 3 rd party evaluation
Location 1SupervisionTiers 1, 2, 3,
Correspondence
Phone & EmailContact Center
Operations
Location 2Tier 3 Only
TrainingContinuous:
Group &Self-paced
Quality AssuranceAll calls recorded1 in 25 calls per
Operator 3 rd party evaluation
Location 1SupervisionTiers 1, 2, 3,
Correspondence
Phone & EmailContact Center
Operations
Contact Center Management 2 Locations
Some remote staff

Contact Center TiersContact Center Tiers
Tier 1 (general): Prepared responses, clinic referrals, and publication ordersTier 2 (research): Requests requiring web and database research Tier 3 (provider): Calls requiring medical/public health expertise and escalate inquiries to CDC Correspondence (email)Emails from physicians, public health partners, and general public
Tier 1 – 20,819 calls
Tier 2 – 7,436 calls
Tier 3 –4,092 calls
Interactive Voice Response (IVR) system
Call Counts are for calls answered by Tier, December, 2008

Content DevelopmentContent Development
• Prepared Responses are program cleared content written in a question and answer format for contact center reps to consistently and accurately answer inquiries
• Over 8,000 Prepared Responses (PRs) in database• Developed and cleared in collaboration with CDC
SMEs• Plain language and scientific accuracy focus• Focus on most frequently requested questions from
public and professional audiences • Leverage existing CDC website content
• Maintains scientific integrity• Meets Health Literacy and Plain Language goals
Content Development
What the public wants to know…
• What is it?• What are the signs/symptoms? (What does it look like/feel
like?)• How will it hurt me – will I die? How sick, etc.• How can I catch it/prevent myself (and my family, loved
ones, etc.) from catching it?• If I get it what should I do? Do I stay home and drink fluids?
See a doctor? Go to the ER? Call 911?
Content Development
• What does CDC-INFO need to know to best represent CDC Programs?
– What types of questions can we anticipate from healthcare providers/hospitals?
– What types of questions can we anticipate from state and local health departments?
Content Development
• What do you consider to be sentinel topics?– Best to develop individual Prepared Responses for all potential
sentinel topics
• What constitutes an “event?”– Do you have pre-defined “talking points” for events?
• Do you have “tipping points” defined?– Is there a specific number of inquiries that could indicate an
event of some kind?– When and how do you decide to ramp up?

Prepared Response ExamplePrepared Response Example
[Partial example – there are publications and background materials on the full PR
1053 - What is a healthcare provider's risk of HIV infection after occupational exposure?
The risk of a healthcare provider getting HIV after coming into contact with HIV-infected blood, through a needlestick or cut, is very low (0.3 percent or about 3 chances out of 1,000). In fact, most injuries from needlesticks or cuts (99.7 percent) do not lead to infection. The risk of a healthcare provider getting HIV after his or her: * eye, * nose, or * mouth comes into contact with HIV-infected blood is also very low (0.1 percent). The risk is also very low for a healthcare provider whose non-intact skin, such as a cut or scrape, comes into contact with HIV-infected blood (less than 0.1 percent). If you are a healthcare provider managing occupational exposures to blood/body fluids and have questions about appropriate medical treatment after an exposure at work, you can call the National Clinicians' Post -Exposure Prophylaxis Hotline (PEPline) at 1-888-448-4911 for guidance. Call to Action
If you are a healthcare provider, and are concerned about contact you have had with blood or other body fluids, report it to your supervisor right away. It is important to report the exposure to the right people in your workplace right away, because you may need post-exposure treatment. If you do, it must be started as soon as possible.
PROBE:
Would you like to know what you should do if you are exposed to the blood of a patient? See prepared response ID 1052, What should I do if I am exposed to the blood of a patient?
PROBE:
Would you like to know how effective postexposure prophylaxis (PEP) is in preventing percutaneous transmission in healthcare personnel? See prepared response ID 1408, Is postexposure prophylaxis (PEP) effective in preventing percutaneous transmission in healthcare personnel?

EvaluationEvaluation– Impact and Process Evaluation
• Quality Assurance• Customer Satisfaction
– Audience Research• User profiles• Health disparities and health equity
– Methodology• Approved OMB package for evaluation surveys, including
emergency response • CSR monitoring (audio and video)• Scorecards for phone and email• IVR post-call survey• Email survey• Call-back survey• Mystery shopper and calibration/call review
– Results• Overall CDC-INFO customer satisfaction consistently meets or
exceeds industry standard (75%)• 50% of survey respondents indicate a behavior change was
made because of CDC-INFO health information they received
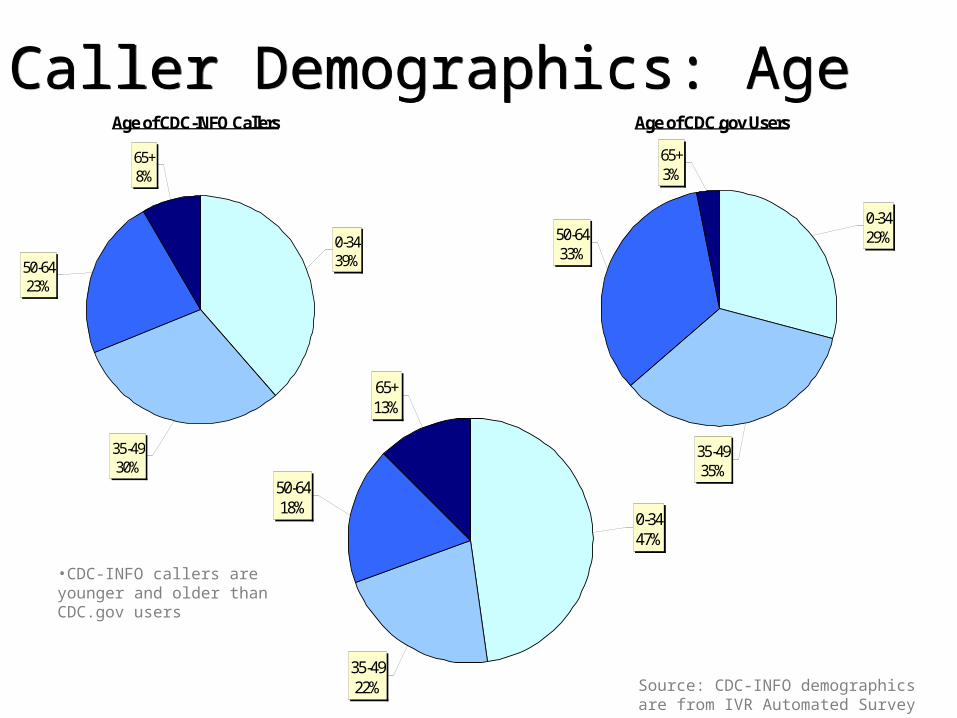
Caller Demographics: AgeCaller Demographics: AgeAge of CDC-INFO Callers
50-6423%
65+8%
0-3439%
35-4930% Sample Size: 77,624
Age of CDC.gov Users
0-3429%
35-4935%
50-6433%
65+3%
Sample Size: 1,297
35-4922%
65+13%
50-6418%
0-3447%
Age of U.S. Population
•CDC-INFO callers are younger and older than CDC.gov users
Source: CDC-INFO demographics are from IVR Automated Survey

Caller Demographics: GenderCaller Demographics: GenderGender of CDC-INFO Callers
Female66%
Male34%
Sample Size: 78,092
Male49%
Female51%
Gender of U.S. Population
•CDC-INFO callers are disproportionately female
Gender of CDC.gov Users
Female72%
Male28%
Source: ACSI Survey, 2006
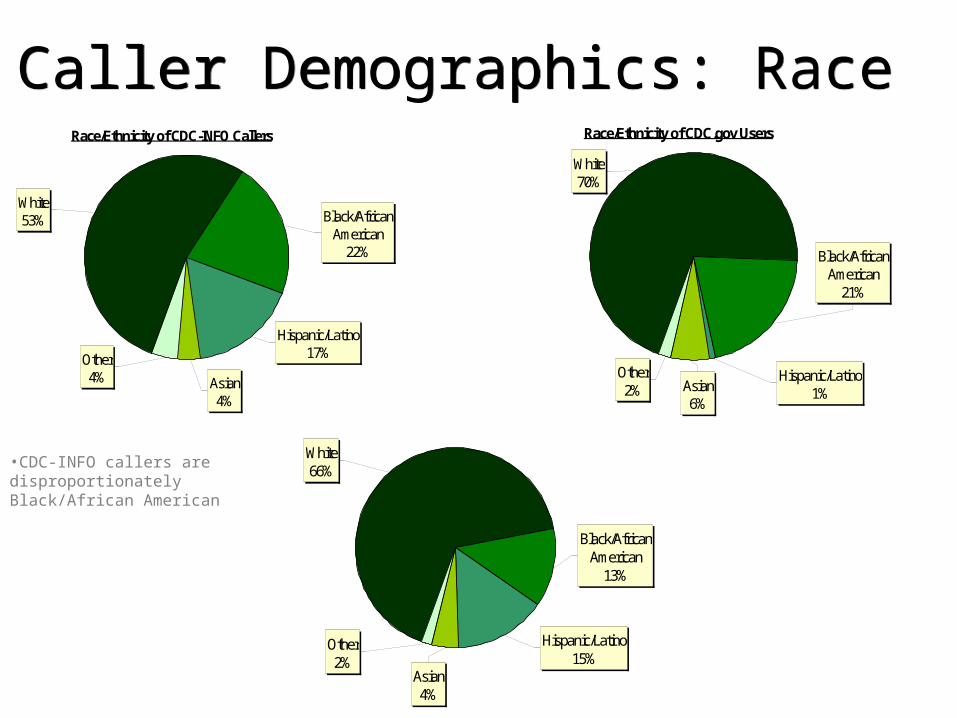
Caller Demographics: RaceCaller Demographics: RaceRace/Ethnicity of CDC-INFO Callers
Asian4%
Other4%
Hispanic/Latino17%
Black/African American
22%
White53%
Sample Size: 76,715
Asian4%
Other2%
Hispanic/Latino15%
Black/African American
13%
White66%
Race/Ethnicity of U.S. Population
•CDC-INFO callers are disproportionately Black/African American
Race/Ethnicity of CDC.gov Users
Asian6%
Other2%
Hispanic/Latino1%
Black/African American
21%
White70%
Source: ACSI Survey, 2006

Customer SatisfactionCustomer Satisfaction
Source: EMT, Dec. 2008
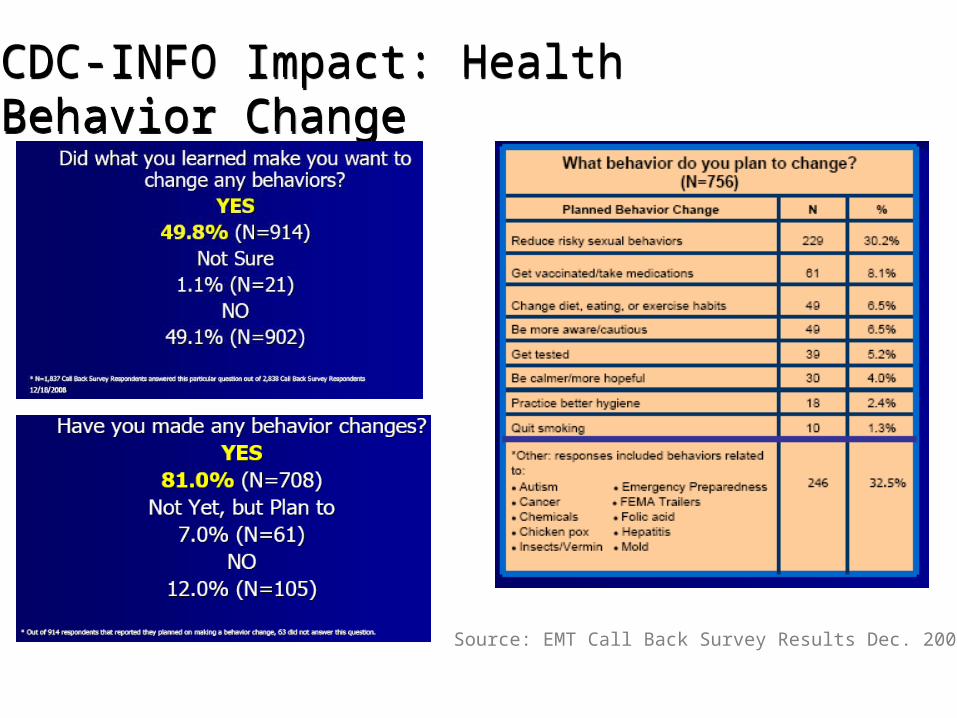
CDC-INFO Impact: Health Behavior ChangeCDC-INFO Impact: Health Behavior Change
Source: EMT Call Back Survey Results Dec. 2008

CDC-INFO Impact: PartnersCDC-INFO Impact: Partners• 19% of incoming calls are from partners*
– State and local governments– Health professionals– Technical “peer-to-peer” call handling needed
• State and Federal coordination during emergency response– Provide assistance with call and email handling
• Iowa – statewide mumps outbreak• Rhode Island – meningitis in schools• FEMA – Hurricane Katrina during and after, formaldehyde in trailers• FDA – Various food outbreaks• DoD – Camp LeJeune• New Jersey – Hepatitis outbreak• New York – H1N1
• Partner Engagement Opportunities– Tailor content specific to partners for emergencies and other events– Cross-promotion across other CDC channels (www.cdc.gov/partners, Partnership
Matters, etc.)– Resource to partners on public health trends to inform communication and
response strategies
* 13.8% English and 4.9% Spanish selected the Medical Professional picks on the IVR. Includes Physicians with patients and health departments
CDC-INFO’S ROLE INEMERGENCY RESPONSE
CDC-INFO & Emergency ResponseCDC-INFO & Emergency ResponseCDC-INFO Surge Response
• CDC-INFO serves as the contact center for HHS resources in the event of pandemic flu or other disease outbreaks
• CDC-INFO implemented a state-of-the-art system that provides critical surge capacity to respond to 98,000 to 273,000 calls per day – with an average call time of 3 minutes – based on the American Red Cross experience during Hurricane Katrina
• CDC-INFO increases response capacity for public and healthcare provider inquiries in emergency and natural disaster events, disease outbreaks and media events
• CDC-INFO extends state and local responder capacity during high volume and after hours inquiries
Agency Impact• The IVR (call menu system) allows for
pre-recorded or on-the-fly messages about events or campaigns
• OMB approved surveillance questions that CSRs will ask during events
• 17 questions for Health Professionals
• 12 questions for General Public
• Federal Coordinator brings together other Federal agencies to ensure resource sharing, standard protocol adherence, and inter-connectivity before, during and after an event.

How CDC-INFO Responds During EmergenciesHow CDC-INFO Responds During Emergencies
Multi-Stage Scalability Process
Stage 1Notification and
Activation
• Triggers• Inquiry volume
assessment• Selection of contact
center staffing option• Requirements Gathering• Cost/Partner
Assessment
Stage 2Mobilization
• Staffing ramp up• Event Training• Content updates• IVR set up and
routing
Stage 3Operations
• Inquiry volume tracking
• FAQ/Content Tracking• Reporting• CSR Communication• Quality Monitoring• Technology enabled
Stage 4Demobilization
• Staffing ramp down• Inquiry volume
tracking• Deactivation of surge
SOP, IVR and call routing
Stage 5Recovery/ Lessons
Learned
• Steady state staffing• Lessons learned
analysis

CDC-INFO & Salmonella

CDC-INFO & H1N1

Timeline• MMWR Dispatch• Vol. 58 / April 21, 2009
• Swine Influenza A (H1N1) Infection in Two Children — Southern California, March–April 2009
• On April 17, 2009, CDC determined that two cases of febrile respiratory illness occurring in children who resided in adjacent counties in southern California were caused by infection with a swine influenza A (H1N1) virus. The viruses from the two cases are closely related genetically, resistant to amantadine and rimantadine, and contain a unique combination of gene segments that previously has not been reported among swine or human influenza viruses in the United States or elsewhere. Neither child had contact with pigs; the source of the infection is unknown. Investigations to identify the source of infection and to determine whether additional persons have been ill from infection with similar swine influenza viruses are ongoing.
Timeline – 4/21/2009
• 4:17 PM - Influenza Coordination Unit sends “heads up” to CDC-INFO Leadership
• 4:18 PM – Content Team asked to develop Log Call. Contact Center management team notified of potential surge
• 5:30 PM – Log Call process initiated at CDC-INFO Contact Center