surrogate endpoints. the surrogates story 3 drug trials 2 fda policy issues 1. cast trial –cardiac...
TRANSCRIPT

Surrogate Endpoints

The Surrogates Story 3 Drug Trials
2 FDA Policy Issues
• 1. CAST Trial –Cardiac Arrhythmias • 2. Concorde – AZT for AIDS• 3. Erythropoietin for Dialysis Pts
• 1. Accelerated Approval (AA)• 2. Patient-Reported Outcomes (PRO)

PVCs




Managing the “Wild Card” of Cardiovascular Disease-
Sudden Cardiac Death
• Up to half of the ½ million cardiovascular deaths are “sudden” deaths
• Known risk factors for sudden death– Cardiac ischemia (esp recent) – Poor ejection fraction fraction– Ventricular arrhythmias



Rigorous testing of new anti-arrhythmics

Antiarrthymics in the late 80’s
• Antiarrthymics for PVCs & V-Tach widely prescribed– Between ¼ - ½ million patients/yr were taking
• “New” antiarrthymic drugs more effective in suppression arrthymias
• Scientific EPS selection of best therapies– Encainide Flecainide Moricizine
• Placebo controlled trials considered unethical – Even tho no trails showing reduction of arrhythmias led to
reduction of sudden death

Cardiac Arrhythmia Suppression Trial
CAST-ing doubt on the
dominant pradigms

High Risk Patients Require Treatment
• “Unethical” not to treat such high risk patients
• Have to do something• How would you feel if one of these
patients you “ignored” suffered sudden death– Plus legal ramifications

Cardiac Arrhythmia Suppression Trial
CAST-ing doubt on the
dominant pradigms

CAST trial 1987
• Randomized, Double-Blind, Placebo Control • 27 clinical centers, 4,400 patients
– Open-label titration to select drug-responsive patients:
• 1,727 randomized to Encainide, Flecainide or Moricizine
• Trial is discontinued early – Encainide and Flecainide 1989– Moricizine 1991
http://clinicaltrials.gov/ct/show/NCT00000526

CAST Results
Sudden Death Total Death
Drug 43 63
Placebo 9 23

Cardiac Arrhythmia Suppression Trial
CAST-ing doubt on the
dominant pradigms

Surrogate Endpoints• Change in a clinical variable
not experienced directly by the patient – Blood pressure – Serum cholesterol – Serum Glucose – PVC’s
• Not itself a direct measure of clinical harm or benefit– Patient does not necessarily feel better or worse

Clinically Relevant Endpoints
• Mortality or survival benefit• Clinically important change experienced
directly by the patient– Reduced pain – Improved functional status – Improved quality of life
• Directly measures clinical benefit or harm

Hierarchy of endpoints
Level 1: True clinical-efficacy measure
Level 2: Validated surrogate endpoint
Level 3: Non-validated surrogate endpoints reasonably likely to predict clinical benefit
Level 4: A correlate that measures biological activity but whose clinical relevance is not well established
Fleming, T. Surrogate endpoints and FDA’s accelerated approval process: the challenges are greater than they seem. Health Affairs (2005) 24(1) 67-78

Why Use Surrogate Endpoints?
• Reduction in sample size, duration of trial and cost– Easier to show benefits: weeks to mos vs. years
• Assess benefits of drug where measurement of clinical outcomes would be unethical/invasive
• Because death and other “harder” outcomes are uncommon or delayed well into future

Surrogate Reductio ad absurdum
• Elevated WBC count – surrogate for severity of pneumonia
• So, why not give cytotoxic agents to reduce the white count?!

Limitations of Surrogate Endpoints
• Surrogates may not be valid predictors of actual clinical outcomes
• Rests upon physiologic assumptions– Persuasiveness of biologic plausibility
• May be statistically significant but not clinically significant
• Provide only partial picture of totality of drug’s effect
• Lend themselves to manipulation by PhARMA• Many turn out to be misleading “red herrings”

Fleming, T. R. et. al. Ann Intern Med 1996;125:605-613
Reasons for failure of surrogate end points
Surrogate is not involved in disease pathway
Disease has multiple pathways and intervention effects only one pathway mediated through surrogate
Surrogate is not affected by/ insensitive to intervention’s effect
Intervention has mechanisms of action independent of disease process
Prostate Biopsy Finasteride Trials
Ventricular ArrythmiasEncainide and Flecainide Trials
CD4 levelsHIV drugs
Ventricular ArrythmiasEncainide and Flecainide Trials

Effective antimicrobial treatment or Useless surrogate?
• 4,000 surgical patients • Treated patients for nasal staph carriage • Treated pts 4.6% vs. 21.3% control (p<.001)
• No difference in surgical infections: 2.3% in treated vs. 2.4% in controls
Perl NEJM 2003

Zidovudine -- AZT
• Thymidine Analogue• Synthesized 1964• Drug in the public domain• 1984 scientists approach
drug companies to expedite R&D
• Got Burroughs Wellcome to patent (w/ difficulty)
Mitsuya, H. et al., 3'-Azido-3'-deoxythymidine (BW A509U): An antiviral agent that inhibits the infectivity and cytopathic effect of human T-lymphotropic virus
type III/lymphadenopathy associated virus in vitro, Proc. Natl. Acad. Sci USA (82) 1985

Pathophysiology of HIV
http://research.bidmc.harvard.edu/vptutorials/HIV/home.htm
AZT

The Evidence it “Works”
AZT uM
Tot
al v
iab
le c
ells
x 1
0 -5
Mitsuya, H. et al., 3'-Azido-3'-deoxythymidine (BW A509U): An antiviral agent that inhibits the infectivity and cytopathic effect of human T-lymphotropic virus
type III/lymphadenopathy associated virus in vitro, Proc. Natl. Acad. Sci USA (82) 1985
HIV positive T cells
HIV negative T cells

AZT surrogate endpoints: the context
• No treatments for AIDS desperation– Bribery to enter trials– Difficulties of obtaining accurate results– Drug smuggling rings
• Cook County: 100’s of deaths per quarter• Regan administration largely ignores HIV

AZT- The Hopes
• New public private partnership • Burroughs Wellcome submits AZT application
in 3 stages over 7 months
• Drug companies, scientists and regulatory agency working together for good of the public– Sets stage for accelerated approval of other drugs

AZT: The Doubts
• The myth of public health altruism– Burroughs Wellcome charges $10,000/year– Largely assumes credit for innovation
• Despite doing relatively little of R & D
• Clinical trials on limited population– White, gay males
• Difficult to adhere to regimen – Initially 6x/day
• Controversies and questions about role of the drug

1994 CONCORDE Study


Kaplan-Meier Plot for all causes of death

Kaplan-Meier Plot for time to AIDS or Death

Kaplan-Meier for time to ARC AIDS or death

Kaplan-Meier for time to reduction in CD4 count less than half of baseline, AIDS or death

The small but highly significant and persistent difference in CD4 count between the groups was not translated into a significant clinical benefit. Thus, analyses of the time until certain concentrations of CD4 were reached revealed significantly shorter times in the Deferred AZT treatment group. Had such analyses been regarded as fundamental, the trial might have been stopped early with a false-positive result.
CONCORDE Conclusions

The small but highly significant and persistent difference in CD4 count between the groups was not translated into a significant clinical benefit. Thus, analyses of the time until certain concentrations of CD4 were reached revealed significantly shorter times in the Deferred AZT treatment group. Had such analyses been regarded as fundamental, the trial might have been stopped early with a false-positive result.
CONCORDE Conclusions

This discrepancy in the differences between Immediate and Deferred AZT treatment groups in terms of changes in CD4 count and of long-term clinical response casts doubt on the uncritical use of CD4 counts as "surrogate endpoints" in trials, although their value as a prognostic marker for disease progression in cohorts and trials is beyond dispute. The reason for this discrepancy is unclear.
CONCORDE Conclusions II

This discrepancy in the differences between Immediate and Deferred AZT treatment groups in terms of changes in CD4 count and of long-term clinical response casts doubt on the uncritical use of CD4 counts as "surrogate endpoints" in trials, although their value as a prognostic marker for disease progression in cohorts and trials is beyond dispute. The reason for this discrepancy is unclear.
Conclusions Continued



History of Erythropoietin
• U of C scientist Eugene Goldwasser starts research on erythropoietin 1960s
• Purified in 1970s

Erythropoietin and Biotech Revolution
• Amgen works with Goldwasser to sequence and clone erythropoietin
• 1985 Amgen files patent• Orphan Drug • 1989 approved for marketing• Decade later $5b in profits

Erythropoietin
Blood’s Life-Blood


Policy Context: Not that simple
• Natl Kidney Foundation guidelines– Progressively raised Hb level w/out clinical
evidence of benefit– Strong conflicts of interest
• 10/18 panel members w/significant financial interest
• 57% of NKF funding from industry
• Medicare reimbursements source of profit for dialysis centers

CHOIR and CREATE Studies
• Researchers in US and France simultaneously conduct erythropoietin studies w/ clinical endpoints
• Funded by Amgen’s competitors– Roche Johnson & Johnson
• To get their “me-too” drugs to market

Singh A et al. N Engl J Med 2006;355:2085-2098
CHOIR: Enrollment and Outcomes

Mean Monthly Hemoglobin Levels
Singh A et al. N Engl J Med 2006;355:2085-2098

Kaplan-Meier Estimates of the Probability of the Primary Composite End Point
Singh A et al. N Engl J Med 2006;355:2085-2098

Kaplan-Meier Estimates of Secondary Endpoint of Death
Singh A et al. N Engl J Med 2006;355:2085-2098
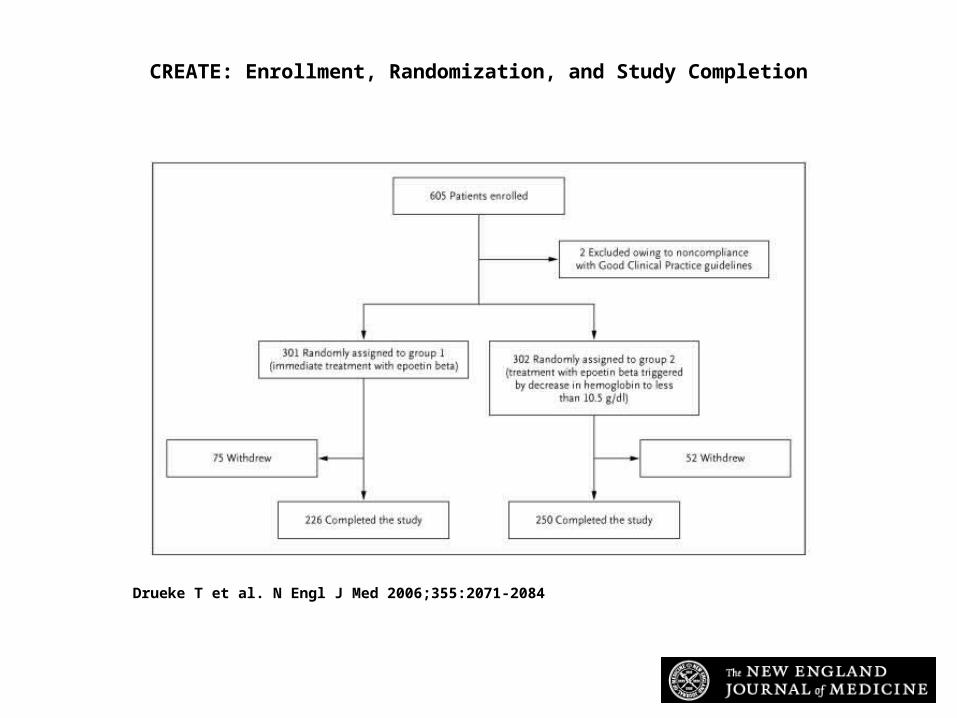
Drueke T et al. N Engl J Med 2006;355:2071-2084
CREATE: Enrollment, Randomization, and Study Completion

Drueke T et al. N Engl J Med 2006;355:2071-2084
Median Hemoglobin Levels in the Intention-to-Treat Population during the Study

Drueke T et al. N Engl J Med 2006;355:2071-2084
Changes from Baseline to Year 1 in SF-36 Quality-of-Life Scores

Changes from baseline to Year 1 in Time to Dialysis during the Study
Drueke T et al. N Engl J Med 2006;355:2071-2084
Lower Hb Group remains off dialysis longer

Current FDA issues with Regulation of Surrogate Endpoints
• Accelerated approval (1992)– Formal acceptance of surrogates– Endpoints “reasonably likely to predict clinical
benefit”– Early marketing approval contingent upon post-
marketing studies confirming clinical benefit
• Patient-Centered Outcomes– Lancet commentary, controversies


Pressures for Accelerated Approval (AA)
• 1962 Kefauver-Harris Amendments require demonstration of efficacy
• Alleged “drug lag” – Drug industry and free market economists
want less regulation– Patient groups demand more available
treatments for AIDS and cancer

ACT UP Demonstrations
http://aidshistory.nih.gov/search_for_treatments/demonstration.html
http://www.actupny.org/documents/FDAhandbook1.html
1988 FDA Headquarters
1990 NIH Headquarters

Accelerated Approval --Issues
• More lenient criteria-slipping into surrogates
• Lack of urgency to complete post-marketing study commitments
• No “teeth”– Unwillingness and lack of power to pull
drugs off the market

Oncology Drug Advisory Committee Report
• Review 8 products approved under AA in first five years AA available for oncology rx (3/03)
• Average time for completion of post-approval studies = 10 years
• Marketing of interventions shown to have little benefit, continued

Accelerated Approval, Animal Efficacy Rule and Pediatric Research Equity Act

Open Post-Marketing Commitments
Behind Schedule
On schedule
Submitted
Concluded
64%13%
10%
13%

• How to handle cases where validation studies don’t conclusively support the drug?
• What to do if no tangible benefit in face of well documented toxicities or safety risks

CAST-ing about for
better pradigms

Patient-Reported Outcomes (PRO)
• Attempt to weigh patient-centered quality of life outcomes
• Step forward: care about more than just death – Want to value and measure quality of life (QOL) – Respect and weight for how patients are feeling
• True valued outcomes ……….or “back door” surrogates?
• Susceptible to manipulation• How to achieve validated measures/scales?
Revicki, Lancet 2/17/2007


Policy analysis found this study & related promotional activities resulted in increase sales worth $375-450 million

Take Home Points
• Misconception that if an outcome is a “correlate” it is a valid surrogate end point – “A correlate does not a surrogate make”
• Lowering risk marker: ? masking or killing the messenger
• Multiple other “unintended” effects to drugs besides putative “neat” mechanisms of action
• Even best surrogates, risk misleading in various ways

2 Criteria for Valid Surrogate
• Biologic marker must be correlated with the clinical endpoint
• Marker must fully capture the net effect of the intervention on the clinical-efficacy endpoint
Fleming, Health Affairs 2005


Searching for Surrogates in JAMA Ads
• How many drug ads (denominator)?• How many ads have efficacy outcome data
of any sort (numerator 1)?• How many of the outcomes are actual clinical
outcomes; how many are surrogates?• Pick out 1 or 2 and analyze them
– As a pharmaceutical researcher design surrogate tools and studies to show how well the drug “works”
– As an FDA reviewer critique/discuss real or implied surrogate issues related to the drug and the ad .