surgical teamwork and communication
TRANSCRIPT

SURGICAL TEAMWORK
AND COMMUNICATION
Clifford Y. Ko, MD, MS, MSHS, FACS, FASCRS
Director, Division of Research and Optimal Patient Care, ACS
Professor of Surgery, UCLA
Dedicated to improving the care of the surgical patient and to safeguarding standards of care in an optimal and
ethical practice environment

1913 1922 1950
1951
1998
2004
2005
2011
Trauma
2015
TQIP
ACS Quality Programs
Cancer Improvement program;
1500+ hospitals
Trauma; 500+
hospitals
Multispecialty (surgery)
600+ hospitals
Bariatric; 800+
hospitals
Peds Surg
Standards/
Verification Breast Centers; 500+

Four Guiding Principles of Continuous Quality Improvement:
1. Infrastructure • Staffing
level/Specialists/Culture
• Committees (care,
quality, peer review)
• Equipment
2. Standardization • Standards
• Protocols, pathways
• Quality Processes
• Innovation
3. Data • From EHR, Patients
• Financial, Registries
• Post-discharge tracking
• Continuously updated
4. Verification • External peer-review
• Creates public
assurance

THE NATIONAL STUDY ON
COSTS AND OUTCOMES
OF TRAUMA CENTER CARE
25% Mortality Reduction in age<55

Results- Change in O/E
Change 2006 to 2007
Complication Mortality
Mean Change in O/E -0.1137 -0.1740
P-value (mean not zero) <0.000001 <0.0001
Volume weighted mean -0.1126 -0.1631
% Institutions Improved 82% 66%

UTI
Pneumonia
SSI
Continuous improvement occurs when data are
fed back, and acted upon…
Mortality

Some hospitals took more time to get better. Why?
Good Improved Improved Bad Improved Improved Good Improved Improved Bad Improved Improved
Outliers in in Outliers in in Outliers in in Outliers in in
2005 2006 2007 2005 2006 2007 2005 2006 2007 2005 2006 2007 x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x
Complication Mortality

Standardize how
we do things
Observation 1: Some took longer to incorporate standardized evidence-based practice.
17.9%
10.6%
0%2%4%6%8%10%12%14%16%18%20%
0
10
20
30
40
50
60
70
80
90
Quarter 3 (2012) Quarter 4 (2012)
Re
adm
issi
on
Rat
e (
%)
Nu
mb
er
of
Pat
ien
ts
Discharges Readmissions Readmission Rate
Readmission Rate Decreased 41%

Standardization was essential, but something more was needed
“…we tried something new...”
“…we changed…”
“…innovated…”
Co
nti
nu
ou
s Q
ua
lity
Imp
rove
me
nt
Obs 2.
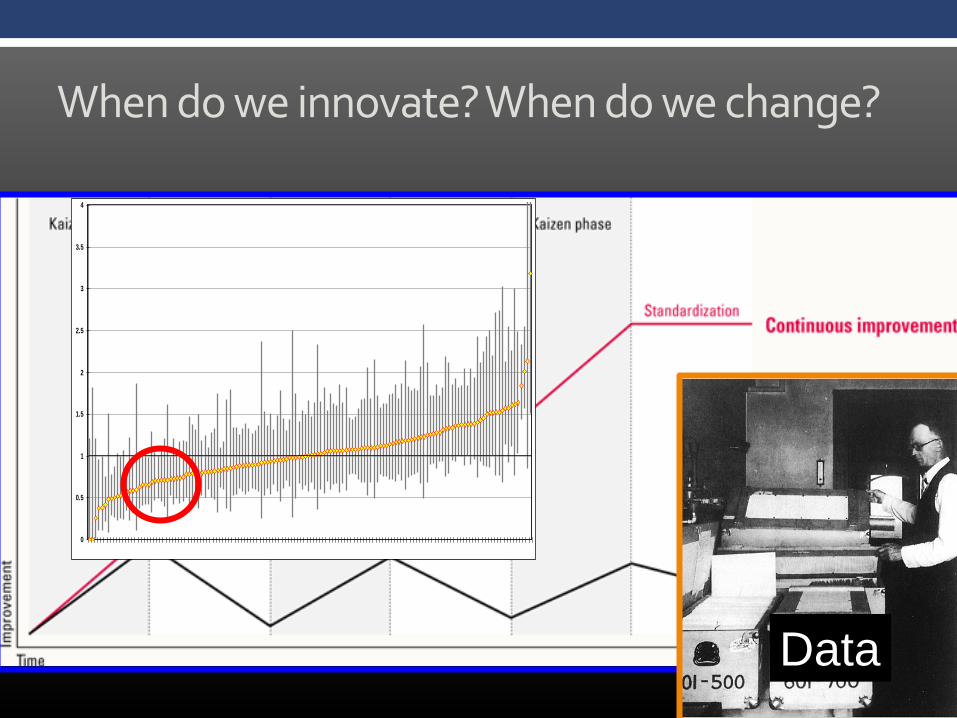
When do we innovate? When do we change?
Data
0
0.5
1
1.5
2
2.5
3
3.5
4
109
114
143
29
13
132
118
113
123
50
54
34
102
69
64
148
45
44
53
76
25
19
62
127
135
39
85
98
88
20
117
65
51
136
12
84 8
43
41
70
31
37
52
81
138
147
104
126
38
57
67
55
36
40
94
108
110 5
134
14
90
15
107
78
56
140
99
101
97
68
128
105
83
58
66
33
96
116
115
74
47
61
26
46
100 2
89
71
120
112
129
91
119
11
60
93
131
48
77
92
144
142
95
73
86
87
122
16
80
30 9
10
35 4
124
130
72
82
21
111
103
49
28
32
146
106
139
27
79
75
152
141
137
23
63
22
145 3
42
59
24
121

“I skate to where the puck is going to be, not where it has been.“
“You miss 100% of the shots you don’t take.“

When data told them something, “achieving” providers took more shots…
• Employed new ways to learn what they didn’t know how to do…
• Often required accelerating the failure cycle…not avoiding failure.
• Failed strategically.
• Lived like the “Hurt, didn’t it” parent
• Smart people haven't had as many opportunities to consider alternatives that failure affords
• So when they do fail, instead of critically examining inward, they tend to cast elsewhere…
• Accepted the notion that they didn’t always know…

Learn from failures. Fail cheap.

Observation 3 : Consider (and embrace) equifinality: There can be more than one solution to a problem (we often need to discover the answer)
“All roads lead to Rome…”
Many
Solution A
Solution B
Solution C

#4: Communication and teamwork (culture) is
routinely associated with sustained quality and
safety improvement
• Culture: a set of shared mental assumptions that guide interpretation and action in organizations by defining appropriate behavior for various situations.
• The way things get done around here
• It is THE most difficult organizational attribute to change, it can outlast organizational products, services, founders and leadership and all other physical attributes of the organization.

The type of strategy and success of implementation locally will depend on levels of evidence and culture
Less Rare; fix
culture
Ideal
Situation;
(easiest strategy)
Too common;
(most
challenging
strategy)
Rare; work on
evidence
Ev
ide
nce
Weak
Str
on
g
Culture
Weak Strong
Un
it P
RE
Un
it P
OS
T
--U
nit
Tim
e 3
0
10
20
30
40
50
60
70
80
90
100
WICU PRE CUSP
WICU POST CUSP
--SICU POST CUSP
Com
mun
icat
ion/
Team
wor
k
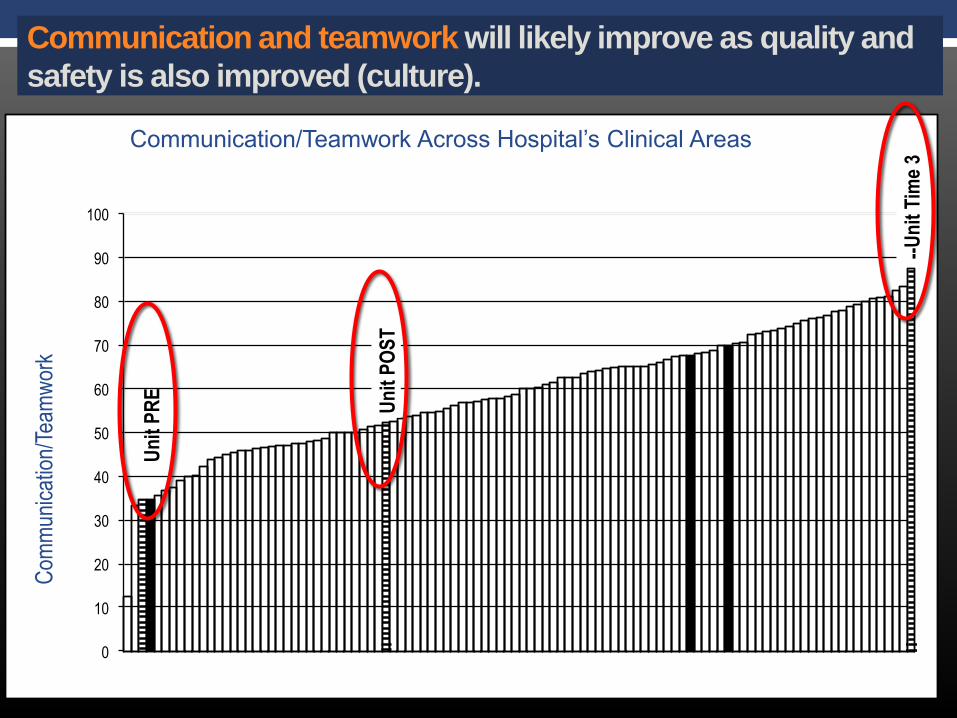
Communication/Teamwork Across Hospital’s Clinical Areas
Communication and teamwork will likely improve as quality and
safety is also improved (culture).

88%
68%
48%
99%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Surgeon Nursing Anesthesia AnesResident
Do you think: “Surgeons and Anesthesiologists
work together as a well-coordinated team”
“We have great culture/teamwork/leadership”

1:1
3:1
6:1
The Positivity Ratio for Achieving Communication and Teamwork

Being Positive…
“Yes, but…”

“Yes and…”
• What you get …
• Start with unexpected/unknown
• Co-creating something out of nothing
• Listening (follow a follower)
• Enhances positivity
Try This:

Team Brainstorming…Figuring out how to fix the problem (new ideas)
• Look for lots of ideas
• Accept all ideas; even if you think (to yourself) it’s stupid
• Make yourself “stretch”
• Take time to “simmer”
• Seek combinations of ideas, connect the dots - be a “hitchhiker”
• Defer judgment, no dominant logic

The Team Member “Portfolio” for CQI

Need to Harmonize The Team

Cycle of Implementing New Ideas

The Beatles
• British rock band 1960-1970
• Most #1 hits (20)
• Academy award; Grammy award (10)
• Best selling band in history
• 12 albums; 207 songs

The Beatles: Authorship and Collaboration

The Beatles: Authorship and Collaboration
Collaborative Writing:
Love Me Do
She Loves You
Can’t Buy Me Love
~68%

The Beatles: Authorship and Collaboration
Magical Mystery Tour
With a Little Help from my Friends
Yellow Submarine

The Beatles: Authorship and Collaboration
Let it Be: Paul
Octopus Garden: Ringo
Here Comes the Sun: George
Come Together: John
8% I’ve Got a Feeling
Dig it
Piggies
Birthday
Hey Bulldog

Seeds of our undoing are sewn at the
pinnacle of our success
-Joseph Schumpeter

Observations from the team that achieved better outcomes while also developing the best
culture…
1. Team-based approach with each having a key role
(not necessarily top-down leadership)
2. Empowering the front line people to provide and test
solutions
3. Biggest difference vs. the past: Everyone
participated in the process, was valued, and
believed they were helping the patient. Dedication.
Engagement. Teamwork/Collaboration.

Even if you increase your communication 4-fold,
you’re probably still not communicating enough
Thank you!