surgical anatomy of the aortic valve and root · surgical anatomy of the . aortic valve and root....
TRANSCRIPT
Joseph S. Coselli, M.D.?
Surgical Anatomy of the Aortic Valve and Root
AATS International Cardiovascular Symposium 2017Session 6: Basic Principles of Aortic Valve Disease
Sao Paulo, Brazil • Friday, December 8, 2017
Vice-Chair, Department of SurgeryProfessor, Chief, and Cullen Foundation Endowed Chair
Division of Cardiothoracic SurgeryBaylor College of Medicine
DisclosureMedtronic, Inc PI Clinical Trials
ConsultantVascutekTerumo
ConsultantPI Clinical TrialsRoyalties Coselli branched graft
WL Gore & Associates
PI Clinical Trials Consultant
Bolton Medical PI Clinical Trials

Thubrikar, M.J. . The aortic valve. CRC Press (1990) pp. 11–20
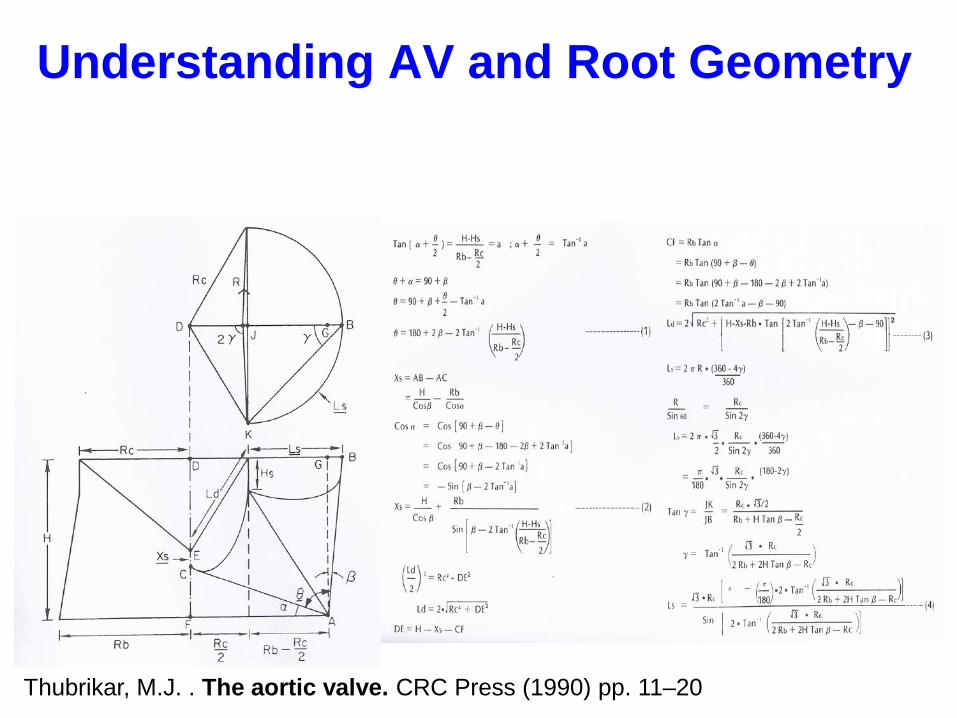
Understanding AV and Root Geometry

Thubrikar, M.J. . The aortic valve. CRC Press (1990) pp. 11–20
Understanding AV and Root GeometryRIDICULOUS
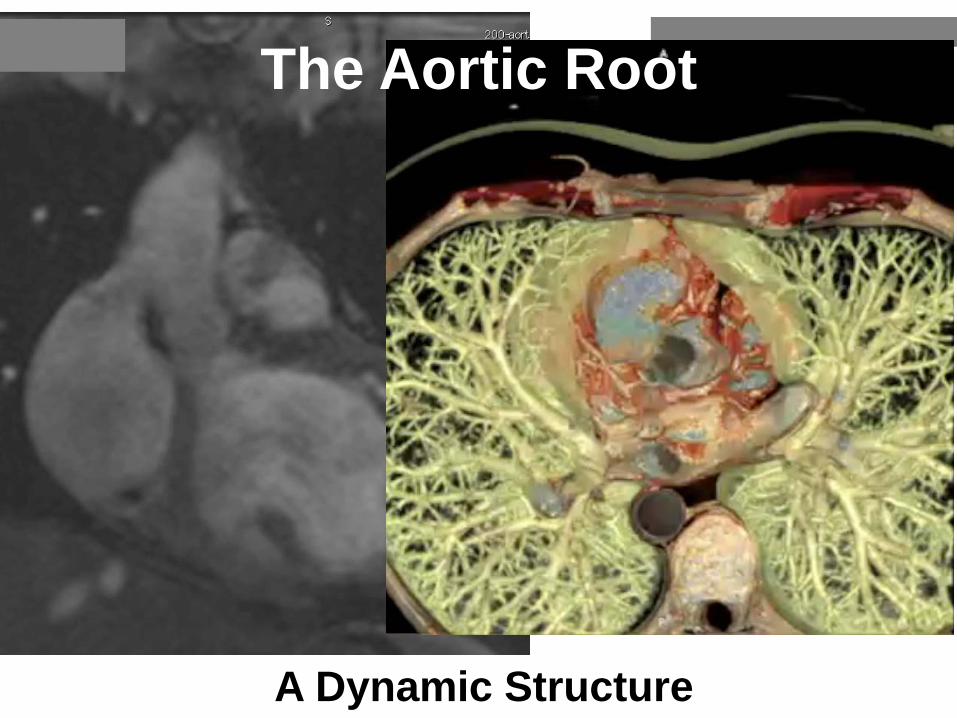
The Aortic Root
A Dynamic Structure

5 Key Components:
• Sino-Tubular Junction• Sinuses of Valsalva• Annulus• Sub Aortic Segment• Aortic Leaflets

8
What is the definition of aortic root?
Basal attachment of aortic valve leaflets
Sinutubular junction
Parasternal Long Axis
Left ventricle
Aorta
Root extends from the basal attachments of the aortic valve leaflets (green line) to the sinutubular junction (blue line)
Slide courtesy of Nicolo Piazza, MDAnderson MMCTS 2006
Aorticsinus

Surgical Anatomy• Aortic root is
anchored between the pulmonary root anteriorly and mitral and tricuspid posteriorly
• Fibrous skeleton of the heart
Pulmonaryvalve/root
Aorticvalve/root
Posteromedial trigone (right)
Carpentier’s Reconstructive Valve Surgery Ch 5, 2010
Diastole shown

10
1: Sinutubular Junction
“Crown” formed by attachment of semilunar valve leaflets
2: Anatomic ventriculo-aortic junction
3: Virtual basal ring“echo” annulus
Membranousseptum
Aorta
Slide courtesy of Nicolo Piazza, MDAnderson MMCTS 2006
Aortic Root: Crown and 3 “Rings”
1
3
2

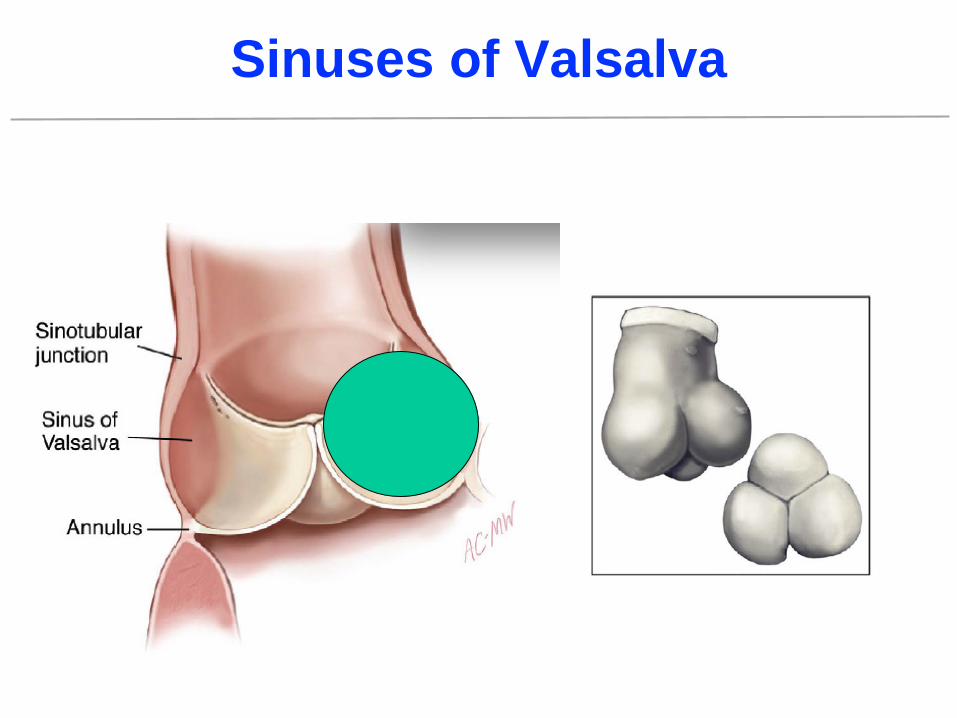
Sinuses of Valsalva
Anterolateral trigone
Aorto-mitral curtainMitral valve
Posteromedial trigone
Membranous septum
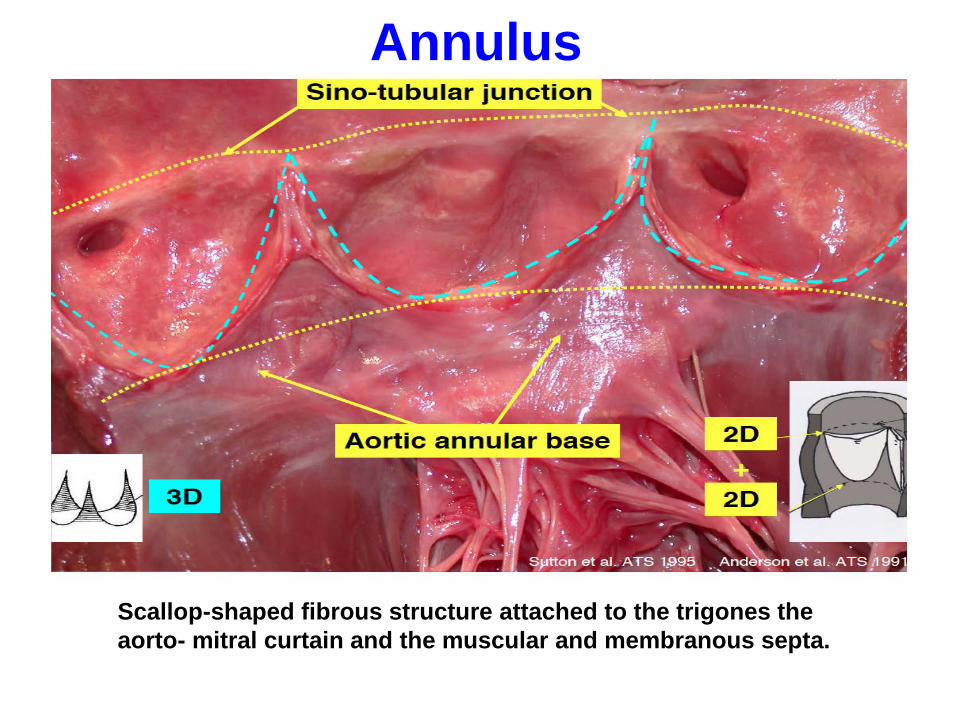
Annulus
Scallop-shaped fibrous structure attached to the trigones the aorto- mitral curtain and the muscular and membranous septa.

Aortic Root Function
Early systole Late systole Diastole

Sinuses of Valsalva
Collagen → Elastin• More collagen at base• Progressive increase in elastic lamellae superiorly as approach sinutubular junction
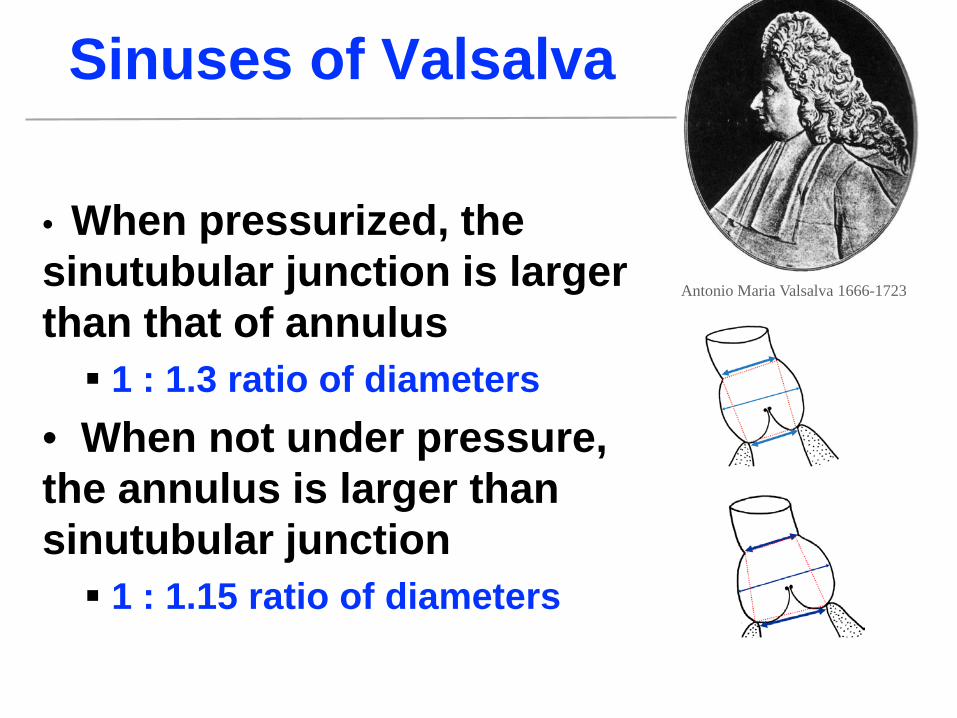
Antonio Maria Valsalva 1666-1723
Sinuses of Valsalva
• When pressurized, the sinutubular junction is larger than that of annulus 1 : 1.3 ratio of diameters
• When not under pressure, the annulus is larger than sinutubular junction 1 : 1.15 ratio of diameters
Antonio Maria Valsalva 1666-1723

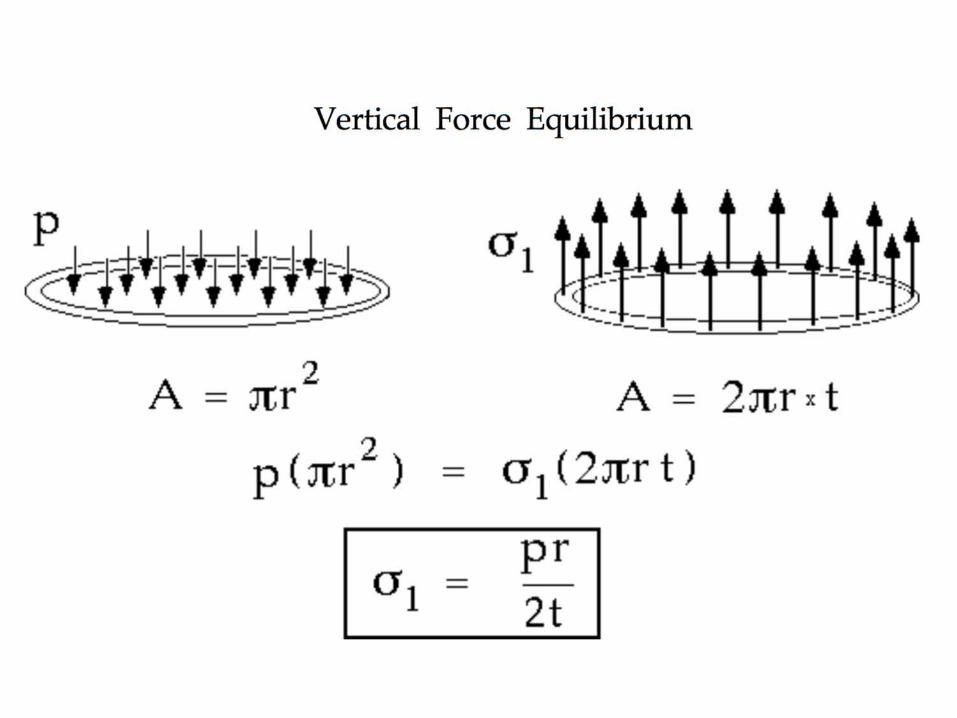
Sinuses of Valsalva: Role?“The aortic sinuses have no effective on valve competence, but are important in reducing mechanical stress on the aortic cusps during the cardiac cycles by creating eddies and currents between the cusps and the sinus walls.”T. David Nat. Rev. Cardiol 2013
Furukawa ATS 1999Bellhouse Nature 1968
De Paulis ATS 2001Aybek JHVD 2005
Flexible Heart Valves Modeled Using FIDAPSchool of Mechanical Engineering, University of Leeds

Sinuses of Valsalva
Sinuses of Valsalva
Force (stress) = Pressure x Area




The Sinuses of ValsalvaCoronary Artery Positions.Distance from nadir (mm)Smallest
Largest
Left coronary sinus
Right coronarysinus

LCA RCAPost-Mortem (n=51)Arq Bras Cardio 2003;81:359
12.6 ± 2.6 mm 13.2 ± 2.6 mm
MSCT (n=169)JACC Img 2008;1:321-330
14.4 ± 2.9 mm 17.2 ± 3.3 mm
Angiography (n=63)Rotterdam experience
13.6 ± 2.2 mm 15.7 ± 2.3 mm25
Aortic Root: Coronary Ostia
Average HeightConsiderable Variation
Nicolo Piazza, MD Anderson MMCTS 2006
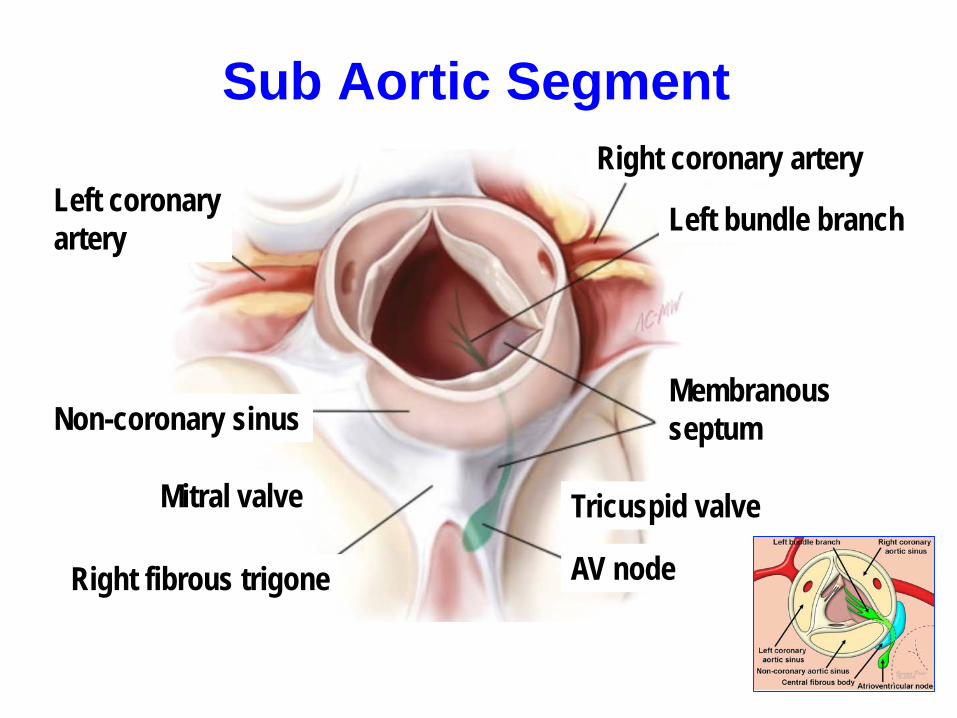
Sub Aortic Segment
Left bundle branch
Right coronary arteryLeft coronaryartery
Tricuspid valve
MembranousseptumNon-coronary sinus
AV node
Mitral valve
Right fibrous trigone

Aortic Leaflets
Coaptingsurfaces
BellyHingeAnnulus
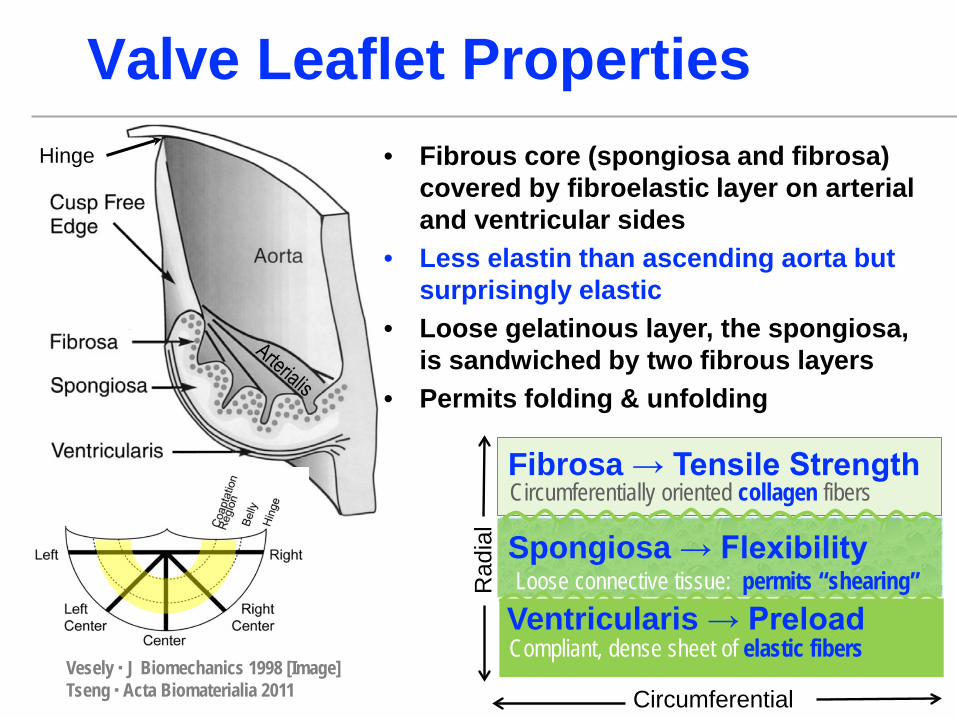
Valve Leaflet Properties• Fibrous core (spongiosa and fibrosa)
covered by fibroelastic layer on arterial and ventricular sides
• Less elastin than ascending aorta but surprisingly elastic
• Loose gelatinous layer, the spongiosa, is sandwiched by two fibrous layers
• Permits folding & unfolding
Ventricularis → Preload
Fibrosa → Tensile StrengthCircumferentially oriented collagen fibers
Compliant, dense sheet of elastic fibers
Spongiosa → FlexibilityLoose connective tissue: permits “shearing”
Vesely ▪ J Biomechanics 1998 [Image]Tseng ▪ Acta Biomaterialia 2011
Rad
ial
Circumferential
Hinge
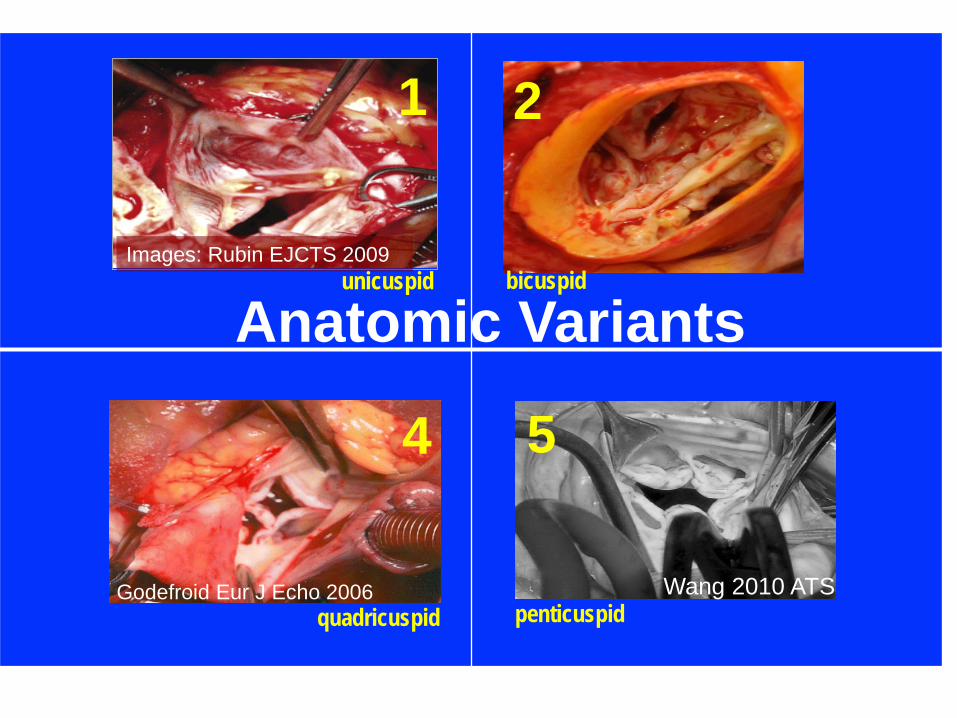
Images: Rubin EJCTS 2009
Godefroid Eur J Echo 2006 Wang 2010 ATS
Anatomic Variants
1
4 5
2
unicuspid bicuspid
penticuspidquadricuspid
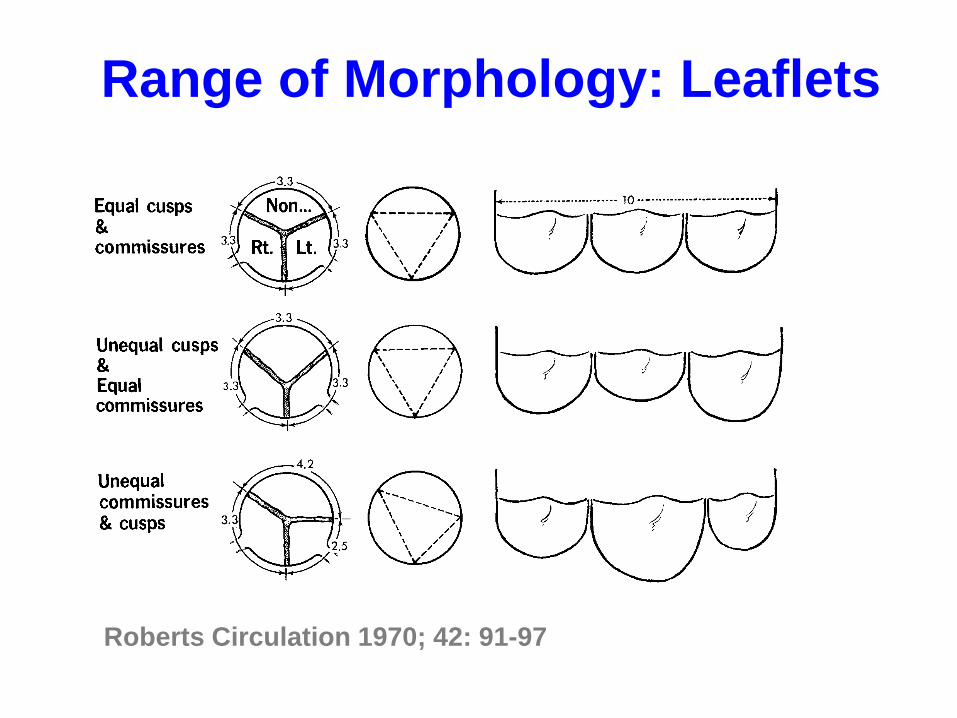
30Roberts Circulation 1970; 42: 91-97
Range of Morphology: Leaflets
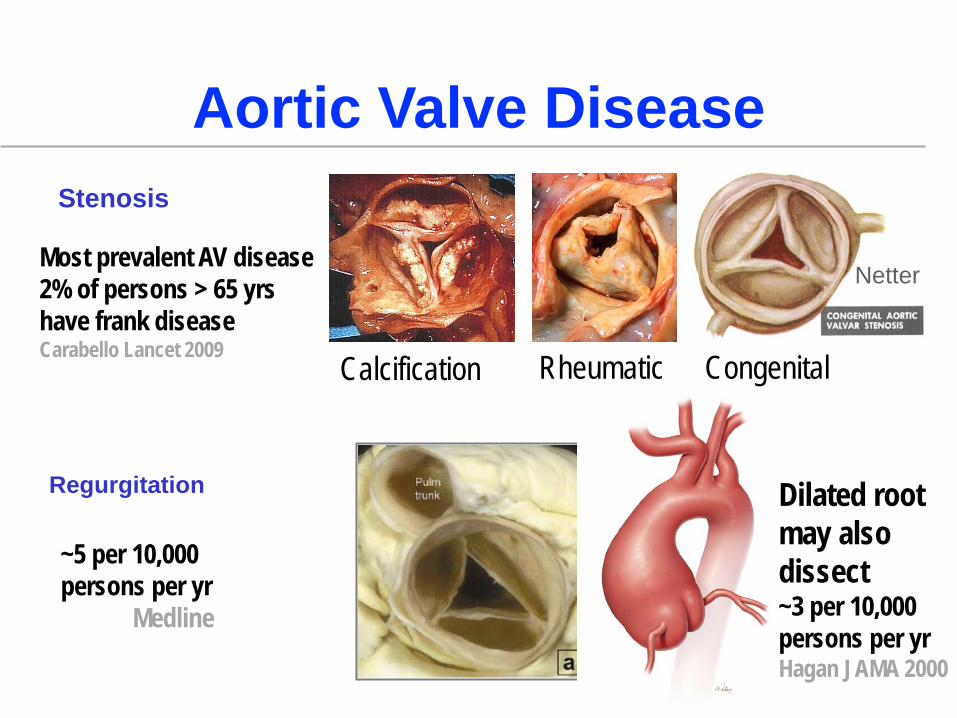
Aortic Valve Disease
Netter
Stenosis
Regurgitation
Calcification Rheumatic Congenital
Dilated root may also dissect~3 per 10,000 persons per yrHagan JAMA 2000
~5 per 10,000 persons per yr
Medline
Most prevalent AV disease2% of persons > 65 yrshave frank diseaseCarabello Lancet 2009
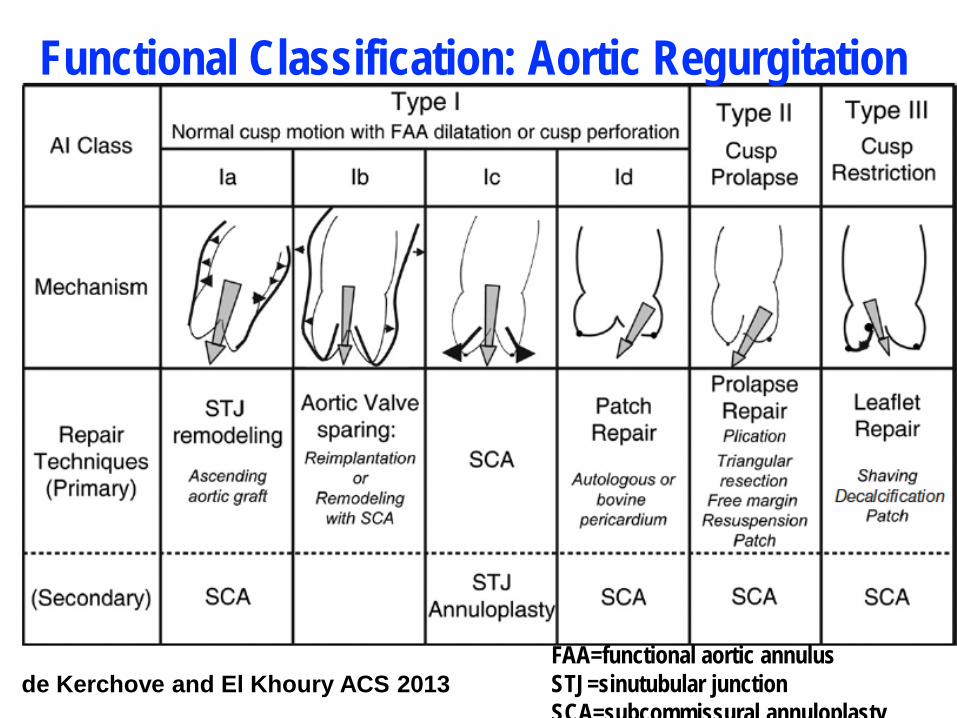
de Kerchove and El Khoury ACS 2013
Functional Classification: Aortic Regurgitation
FAA=functional aortic annulusSTJ=sinutubular junctionSCA=subcommissural annuloplasty
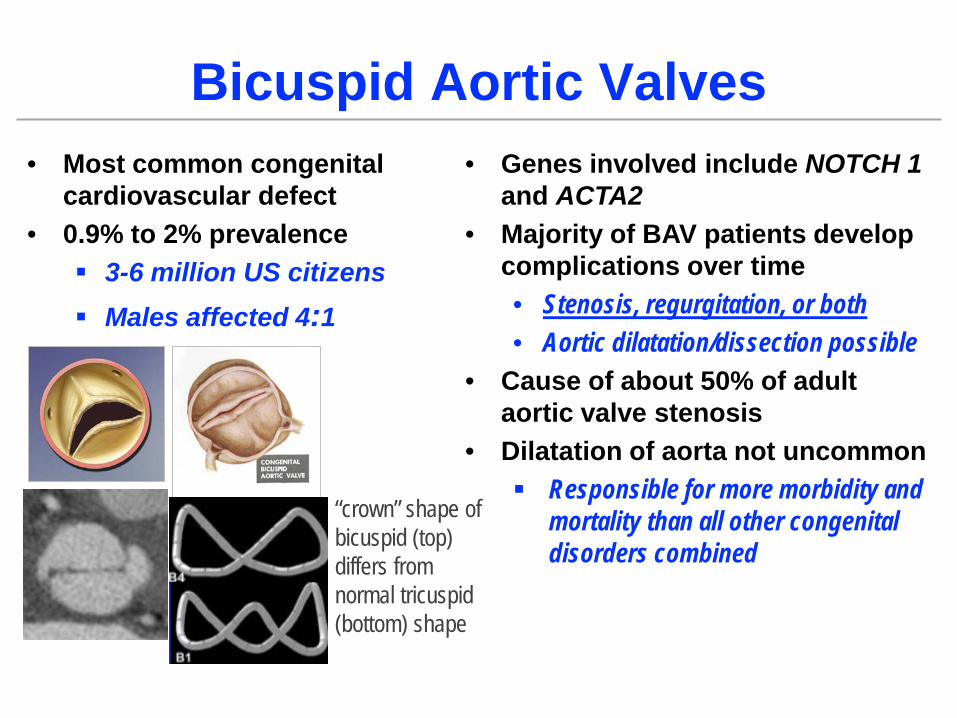
Bicuspid Aortic Valves• Most common congenital
cardiovascular defect• 0.9% to 2% prevalence
3-6 million US citizens Males affected 4:1
• Genes involved include NOTCH 1 and ACTA2
• Majority of BAV patients develop complications over time• Stenosis, regurgitation, or both• Aortic dilatation/dissection possible
• Cause of about 50% of adult aortic valve stenosis
• Dilatation of aorta not uncommon Responsible for more morbidity and
mortality than all other congenital disorders combined
“crown” shape of bicuspid (top) differs from normal tricuspid (bottom) shape
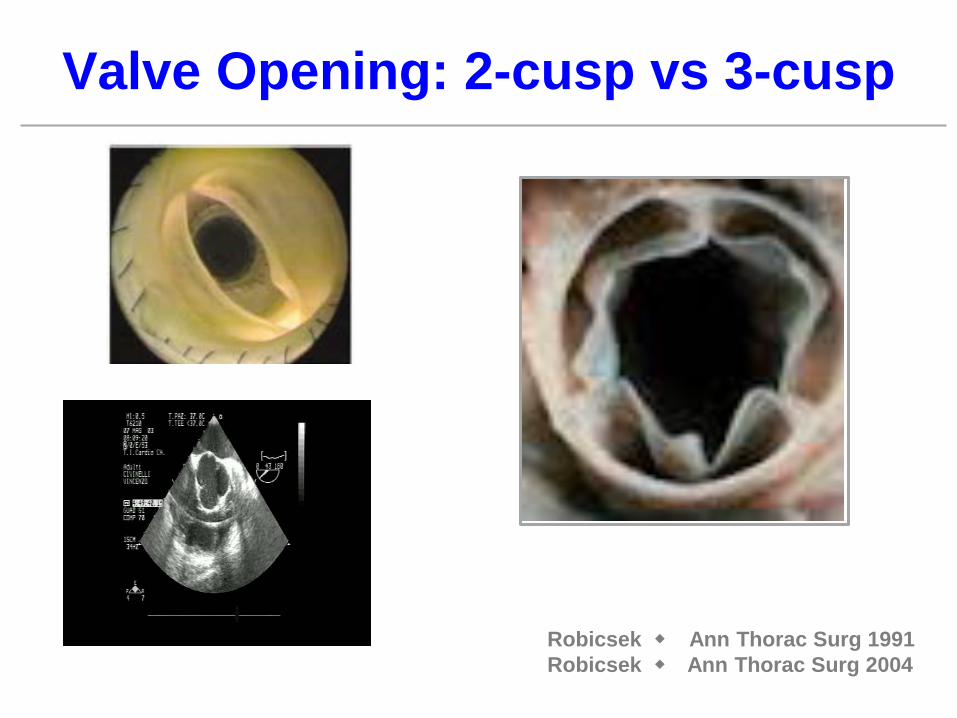
Valve Opening: 2-cusp vs 3-cusp
Robicsek Ann Thorac Surg 1991Robicsek Ann Thorac Surg 2004

Circumference = 2 π r = 6 r
2r
2r
Total ~ 4r
r
Total ~ 6r
rrr
r r
~
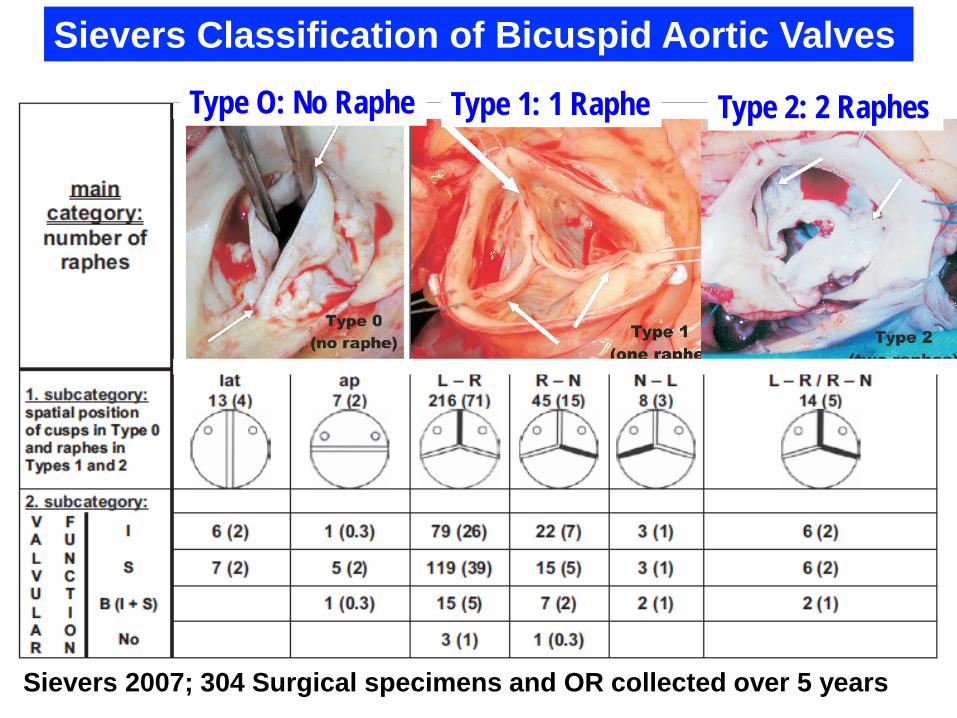
Sievers 2007; 304 Surgical specimens and OR collected over 5 years
Sievers Classification of Bicuspid Aortic ValvesType O: No Raphe Type 1: 1 Raphe Type 2: 2 Raphes

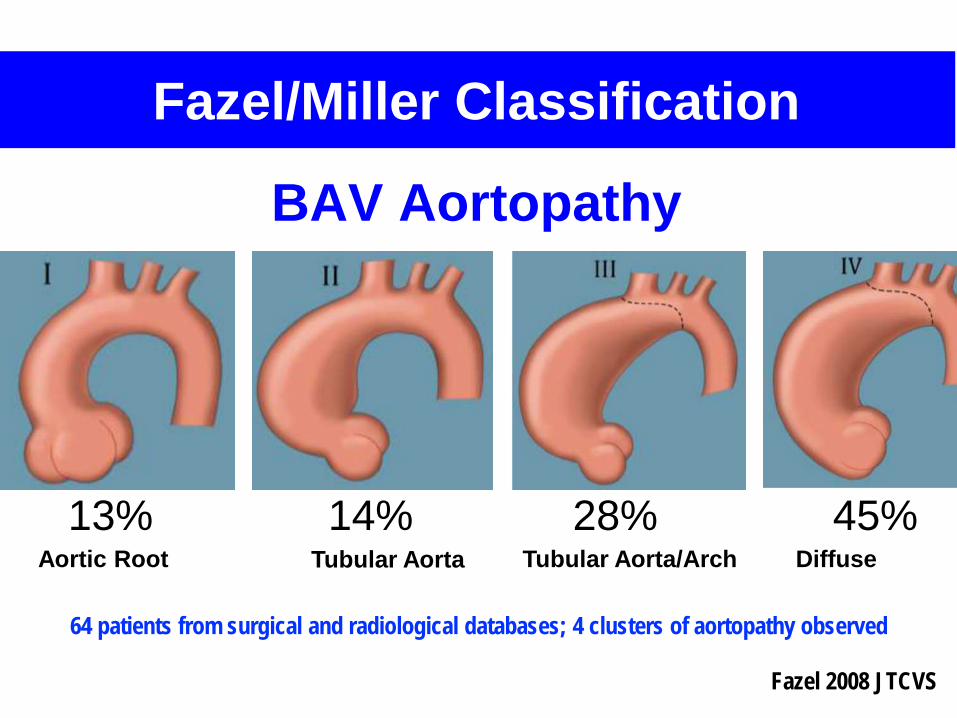
13% 14% 28% 45%
Fazel 2008 JTCVS
Fazel/Miller Classification
64 patients from surgical and radiological databases; 4 clusters of aortopathy observed
Aortic Root Tubular Aorta Tubular Aorta/Arch Diffuse
BAV Aortopathy

Verma 2014 NEJM Review Article
• Most common pattern• Associated with R-L cusp
fusion
R
L
Wall stress differs by fusion patternR-L: Right anterior wall of ascending aorta
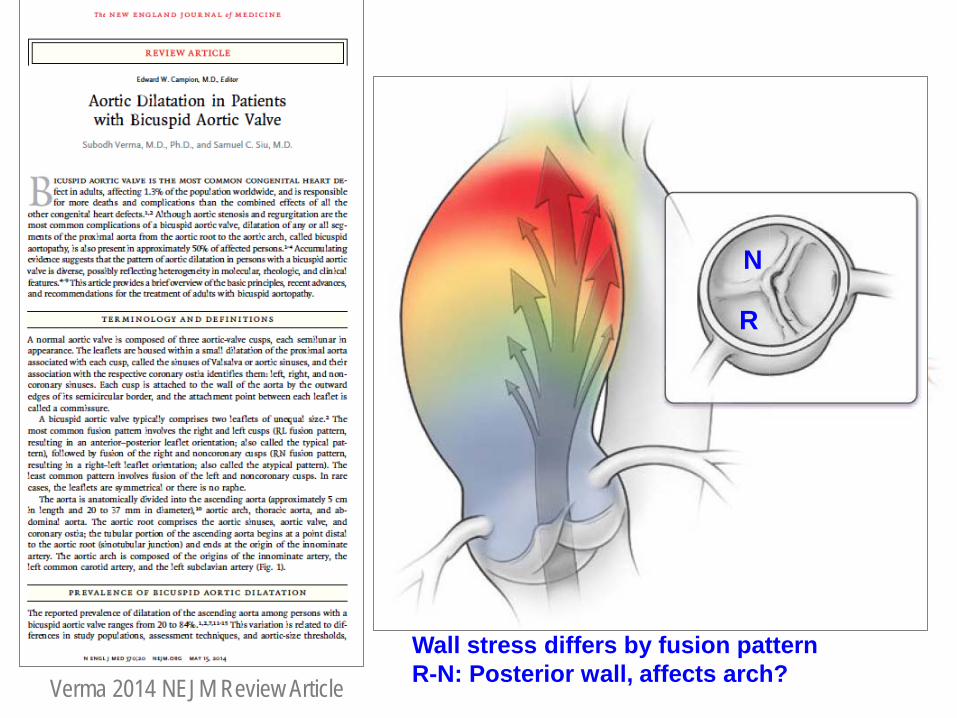
Verma 2014 NEJM Review Article
R
N
Wall stress differs by fusion patternR-N: Posterior wall, affects arch?

There is no substitute for knowing the anatomy and physiologic function

Obrigado!