surgical anatomy of breast and approach to breast carcinoma
TRANSCRIPT
Surgical Anatomy of Breast and History Taking (Breast Carcinoma)
By; Arravindh Vivekananthan
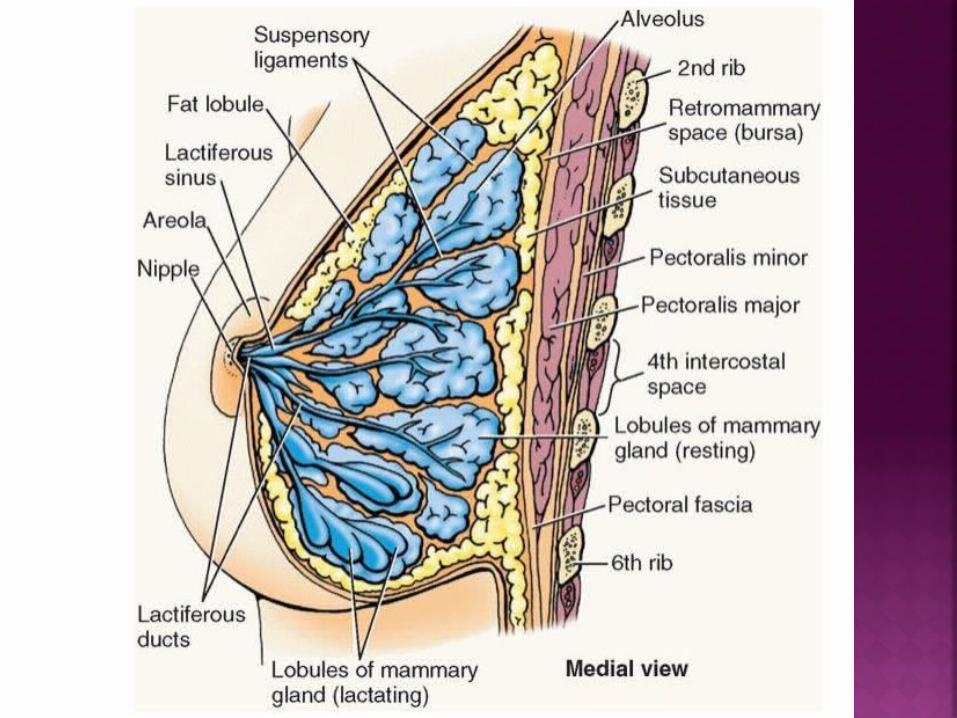
The breast is a modified sweat gland
1
2
3
(of Spence) 1
2
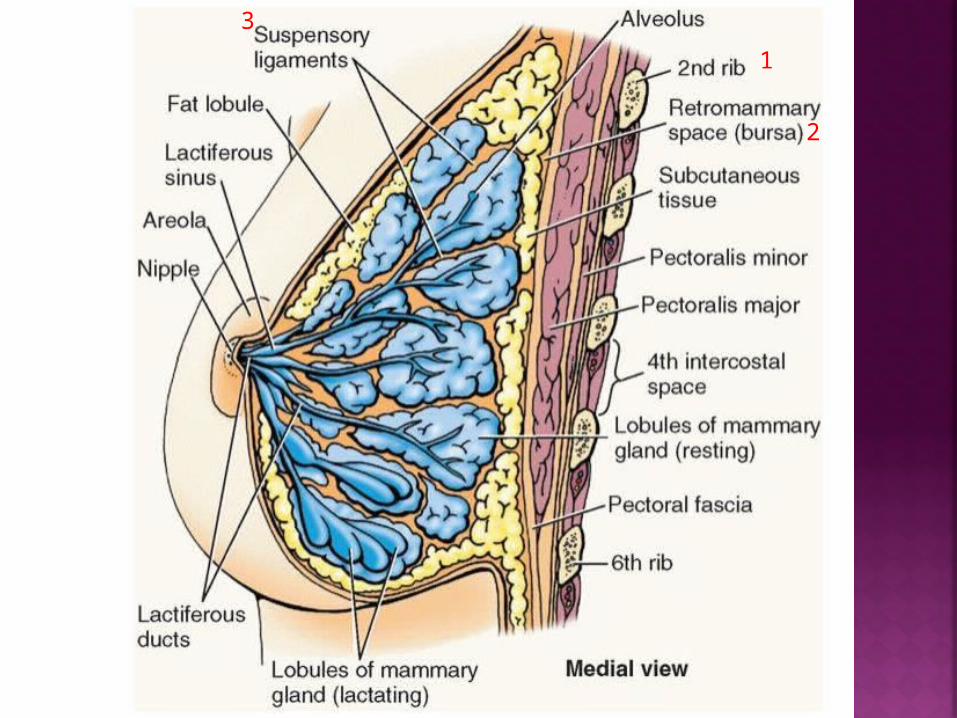
Lobules are the chief functional and structural unit of the breast.
Many lobules join to make a lobe.
There are 15–20 lobules of glandular tissue embedded in fat, and
Each lobe is drained by a lactiferous duct (2-4 mm)
Fat accounts for its smooth contour and most of its bulk. These lobules are separated by fibrous septa running from
the subcutaneous tissues to the fascia of the chest wall
(the ligaments of Cooper/ Astley Cooper fibers/ suspensory ligaments)
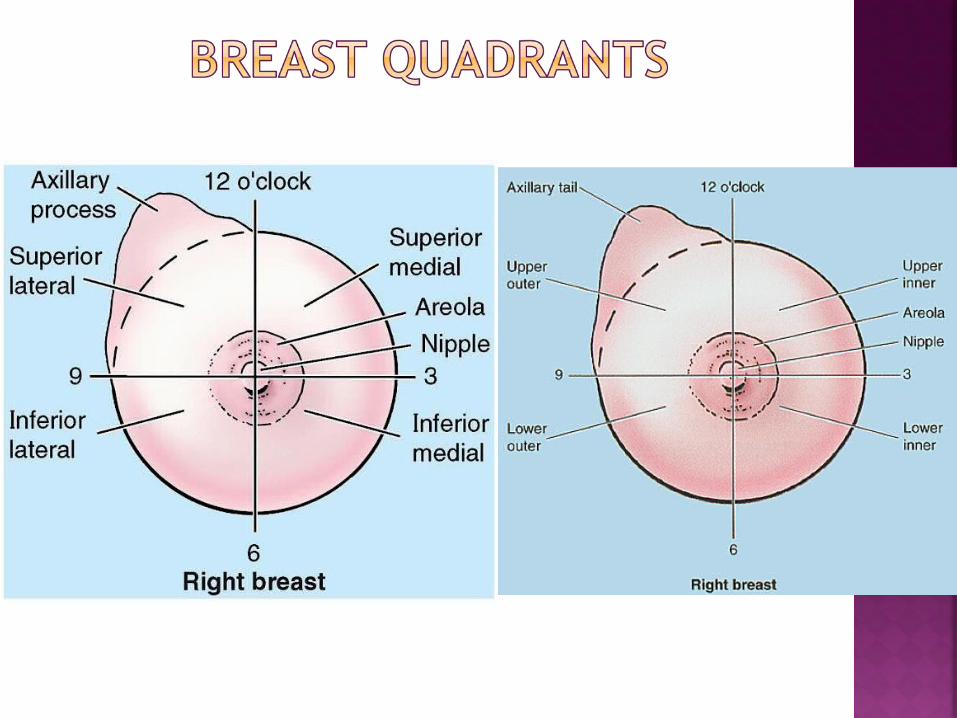
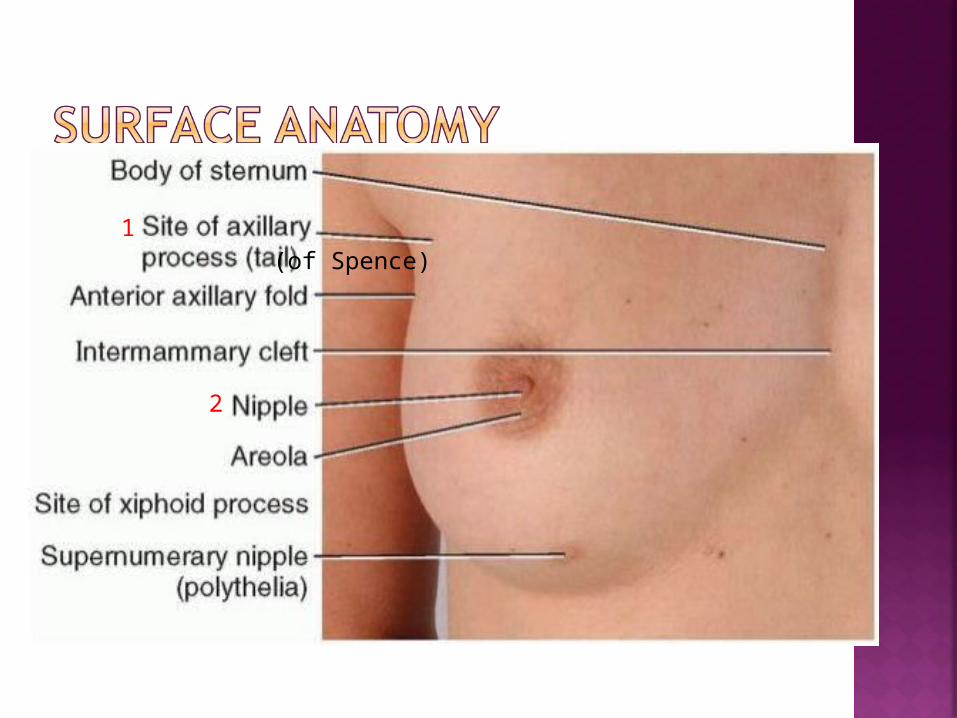
• Majority of cancers develop in upper outer quadrant; large amount of glandular tissues present.• An axillary tail of breast tissue often extends into axilla
In advanced breast cancer • Tumors may grow through retromammary space• Subsequently invade deep fascia & pec. major m.• Leads to fixation of malignant breast lesion to chest wall • Shortens suspensory (Cooper’s) ligs.• Leads to irregular dimpling of skin or retraction of nipple
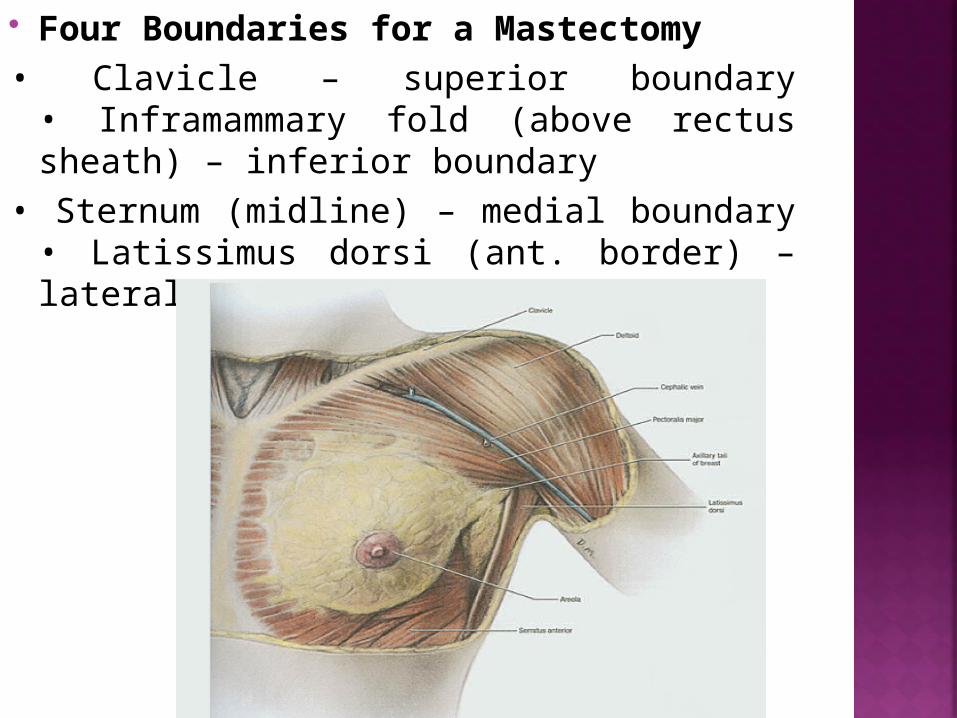
Four Boundaries for a Mastectomy • Clavicle – superior boundary
• Inframammary fold (above rectus sheath) – inferior boundary
• Sternum (midline) – medial boundary• Latissimus dorsi (ant. border) – lateral boundary
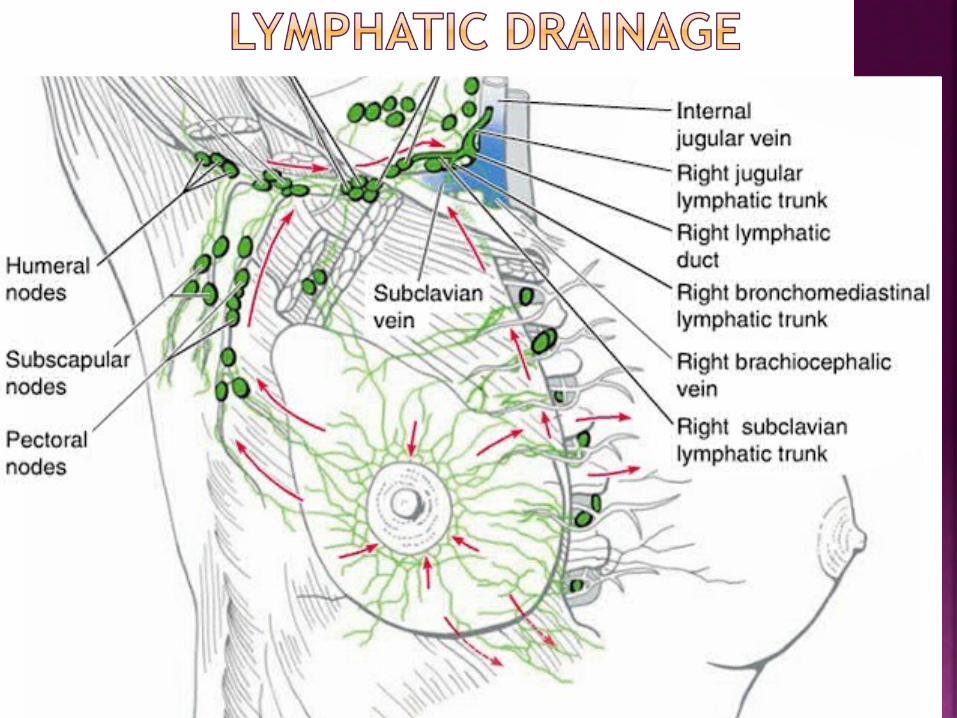
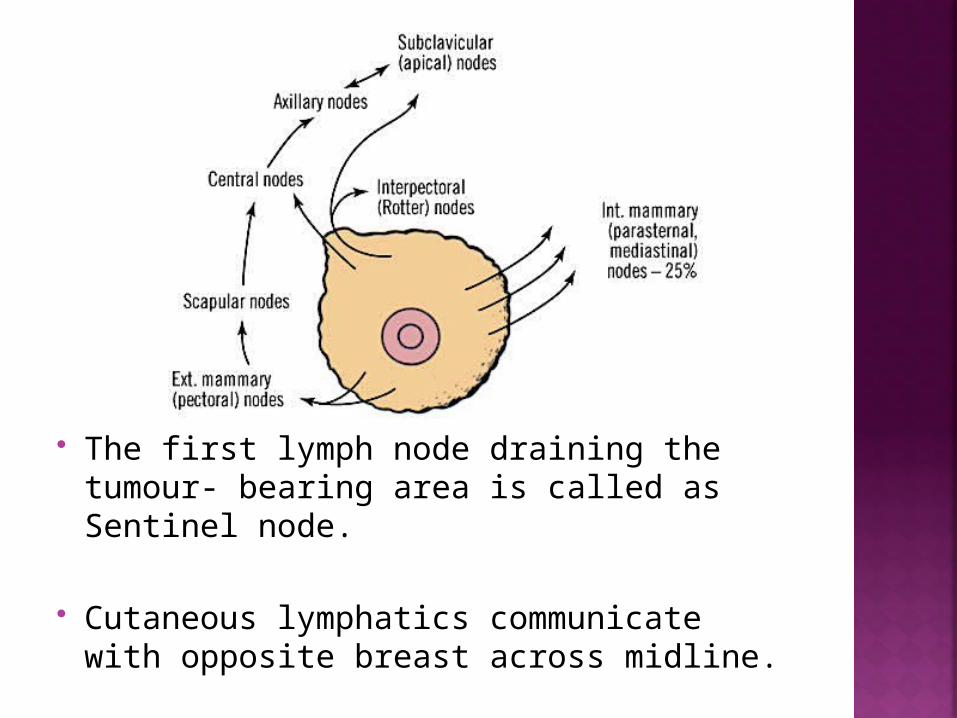
The first lymph node draining the tumour- bearing area is called as Sentinel node.
Cutaneous lymphatics communicate with opposite breast across midline.
• Cutaneous innervation (T1-T6)• Medial pectoral n.• Lateral pectoral n.• Long thoracic n. Supplies serratus anterior superficially
1. Pain/discomfort
Onset, duration, intermittent?Association with menses : timing, severityCharacter of painAssociated symptoms : Lump, dischargeContributing factors: trauma, strenuous activity
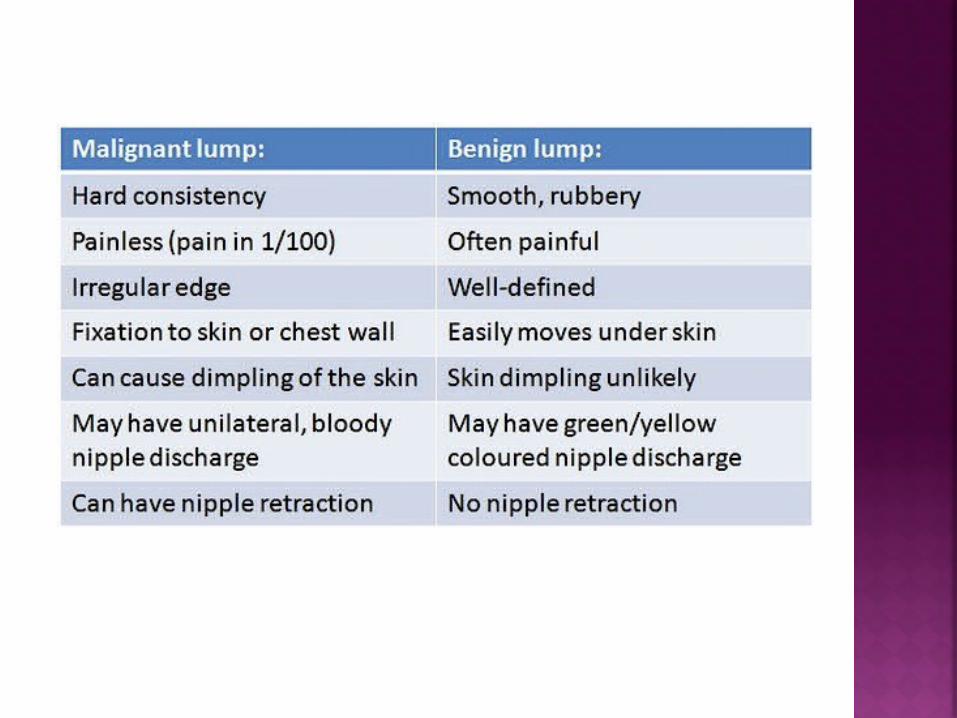
2. Lump
Duration since lump first noted Consistency of lump presenceChange in sizeLocationShapeConsistency of lump, mobility
Assoc. with menses, tenderness, dimpling, discharge, nipple retraction, tender lymph nodes
3. Nipple discharge
Yellowish (pus) Breast abscess
Serous, greenish FC, duct ectasia
Bloody discharge Duct papilloma, ca.
Milky Galactocoele
Loss of weight, lost of appetite
Bone pain, dyspnea, jaundice, abdominal pain/distension.
Fever, breasts trauma, breastfeeding history
Female Age >40 y.o Early menarche Use of OCPs Late age of 1st child >30 y.o Breastfeeding Nulliparous Late menopause Prolonged HRT>5 years
Radiation (Hodgkin’s Lymphoma) Positive family history of malignancy,
previous lump Alcohol, smoking history.
In a patient above the age of 40, with recently detected lump in the breast, it
should be considered to be carcinoma of breast until proven otherwise.