surgery in bleeding diathesis
TRANSCRIPT

SURGERY IN BLEEDING DIATHESIS
Dr.B.Selvaraj MS;Mch;FICS;Professor of Surgery
Melaka Manipal Medical CollegeMelaka 75150 Malaysia

SURGERY IN BLEEDING DIATHESIS
Introduction Physiology Of Hemostasis Pre-op Evaluation Cases Managed Common Bleeding Disorders Surgery In Hemophiliacs Clinical vignettes
PLAN

SURGERY IN BLEEDING DIATHESIS
A challenging & fascinating problem Pre-existing hemostatic defects can be
detected with proper H&P and screening lab tests
Occasionally the first sign of the defect would be excessive intra-op bleeding
Nightmare to any surgeon

SURGERY IN BLEEDING DIATHESIS

PHYSIOLOGY OF HEMOSTASIS
FOUR COMPONENTS:
VESSEL WALL RESPONSE PLATELET ACTIVITIES COAGULATION CASCADE FIBRINOLYTIC SYSTEM

PHYSIOLOGY OF HEMOSTASIS
VESSEL WALL RESPONSE - Intact endothelium maintain fluidity of blood - Endothelial disruption initiates hemostasis PLATELET ACTIVITIES - Adhesion to denuded endothelium by VWBF - Aggregation into an unstable mass by fibrinogen&Thromboxane A2

PHYSIOLOGY OF HEMOSTASIS
PLATELETACTIVITIES

COAGULATION FACTORS
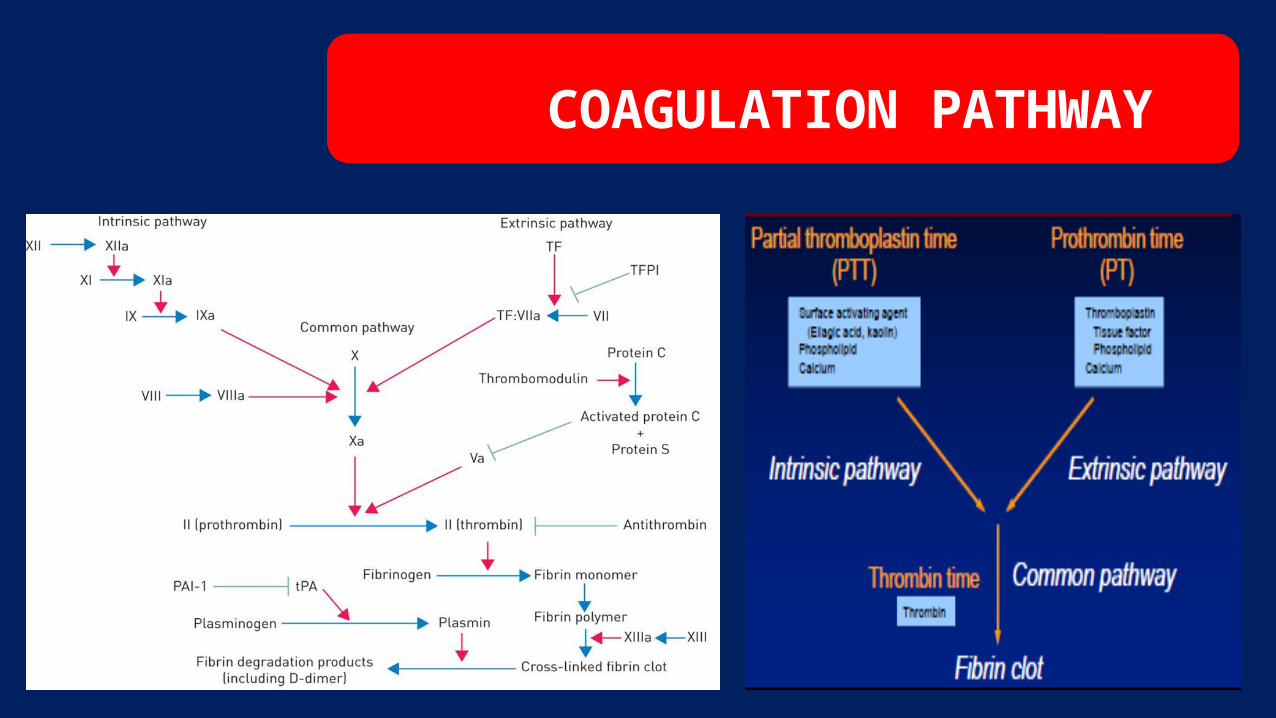
COAGULATION PATHWAY
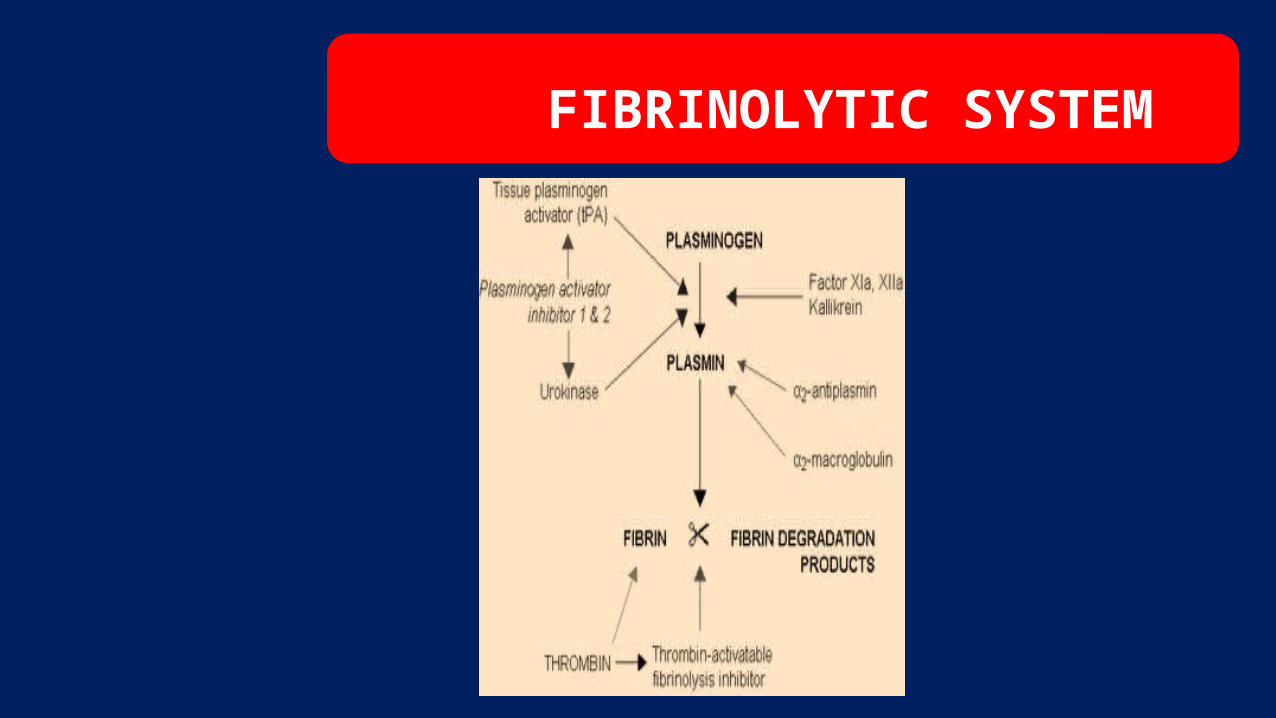
FIBRINOLYTIC SYSTEM

PRE-OPERATIVE EVALUATION
Thorough personal medical history, family history& drug ingestion history
Physical Exam: Skin: Petechiae Thrombocytopenia Ecchymosis & Hematomas Platelet dysfunction Joints: Hemarthrosis severe coagulation defect Organomegaly: Hepatomegaly Coagulopathy of Cirrhosis Spleenomegaly Possible thrombocytopenia

PRE-OPERATIVE EVALUATION

LAB SCREENING TESTS


CASE NO: 1
2 Yrs old 1st born male child was brought with obstructed RIH H/O Epistaxis & easy bruisability Ear boring ceremony resulted in prolonged bleeding Emergency, so extensive workup was not done Emergency herniotomy was done

CASE NO: 1
Basic screening tests for bleeding diathesis:
Hb 11Gms Bleeding time >15mts Prothrombin time 12 sec Partial thromboplastin time 39 sec Blood group B +ve

CASE NO: 1
Only B.T. was prolonged Provisional Diagnosis: Functional Platelet problem -
Thrombocytopathy Emergency Herniotomy with 200 ml of fresh whole blood Readmitted after 10 days for prolonged bleeding from a small cut to
upper lip Managed by multiple WB transfusions

CASE NO: 1
Hematological workup:
Hb 11.5 GMs PCV 36% TC 12000/Cmm DC P33,L43,E18, M4 Platlets200,000/ Bleeding time > 15 mts
•
Clotting time13 mts Clot retraction Nil Clot lysis Nil PT 12 sec PTT 40 sec Plasma fibrinogen 280
mgms Factor xiii activity normal

CASE NO: 1
PLATELET FUNCTION TESTS: -Invivo Platelet Adhesion10.8% -ADP Aggregation Absent Aggregometer Studies -ADP No Aggregation -Collagen No Aggregation Thrombin Time 8sec Blood group B+ve

CASE NO: 1
Normal Platelet count&morphology
Normal Clotting tests
Prolonged Bleeding Time
Absent Platelet Aggregation with ADP and Collagen
Absent Clot Retraction
GLANZMAN`S THROMBASTHENIA

CASE NO: 2 11 yrs old boy with no known H/O any bleeding diathesis
underwent emergency appendicectomyHe started oozing from the operated site in immediate post-
operative period In subsequent interrogation parents came out with the H/O
ingestion of aspirin tablet by the boyLabs: BT- prolonged; PT, PTT- Normal; Platelet count- NormalSince this is a functional disorder of
Platelets(Thrombocytopathy) the boy was treated with Platelet concentrate

CASE NO: 3
4 yrs old boy was brought with pain abdomen and fever for 1 day
O/E: Abdomen- diffuse tenderness with rigidityAXR- erect revealed free gas under diaphragmBoy is a known HemophiliacLaparotomy and ileal perforation closure was done with Anti
hemophilic factorOn 2nd POD boy was oozing from the surgical site. So factor8
assay was done in hematology lab and dose of AHF was adjusted.

CASE NO: 4 5 yrs old boy with a H/O fall over cycle bar presented with
retention of urineO/E: Drop of blood at uretheral meatus, perineal hematoma
and extravasation of urine were presentEmergency SPC was done after confirming rupture urethra
with Retrograde urethrogramThe next day the boy started bleeding from SPC siteOn subsequent interrogation parents told the boy is a known
HemophiliacHe was managed with AHF
Hematological Disorders Commonly Encounter by surgeons Thrombocytopenia Thrombocytopathy Hemophilia- A Hemophilia- B- Christmas disease Von Willebrand Disease Disseminated Intravascular
Coagulation Liver Disease– Factor vii & x deficiency

THROMBOCYTOPENIA
Low Platelet CountAcquired or InheritedPurpura & Ecchymosis superficial bleedingLabs: BT- prolonged, PC- decreased, PT, PTT-
NormalTreatment: Platelet concentrates
THROMBOCYTOPATHY Functional Platelet Abnormality
Acquired due to drugs like Aspirin and Uremia Inherited Defective Platelet adhesion Bernard
Soulier Syndrome Defective Platelet aggregation Glanzman’s Thrombasthenia Labs: BT- Prolonged; PC,PT,PTT Normal Ecchymosis & Epistaxis Superficial hemorrhage Treatment: Platelet concentrates

HEMOPHILIA- A
Factor viii procoagulant deficiencySex linked recessive inheritanceDeep tissue bleed & hemarthrosisLABS: PTT- Prolonged; PC,PT,BT- Normal Individual factor assay Treatment: AHF- 1U/Kg raises the level by 2% For 5 Kg baby 250U for 100% raise Cryoprecipitate & FFP

HEMOPHILIA- B
Factor ix deficiency Christmas diseaseSex linked recessive inheritanceDeep tissue bleed&HemarthrosisLABS: PTT- Prolonged; BT,PC,PT- Normal Individual factor assay Treatment: Factor 9 concentrates or FFP

VON WILLEBRAND’S DISEASE
Factor viii vwf deficiencyAutosomal Dominant InheritanceEpistaxis, easy bruising and prolonged bleeding
from dental extractionLABS: BT & PTT- Prolonged; PC,PT- Normal Individual factor assayTreatment: Cryoprecipitate or FFP or DDAVP

Disseminated Intravascular Coagulation
Thrombohemorrhagic disorderAcquired: Abruptio placenta, septic abortion,
toxemia, Gram-ve sepsis, massive tissue injury, snake bite Etc
Activation of coagulation cascade Microthrombi throughout the micro circulation
Consumption of coagulation factors, platelets and fibrin
Activation of fibrinolytic system

Disseminated Intravascular Coagulation
Mucosal bleeding, oozing from wound sites and
ecchymosisLABS: BT,PC,PT,PTT,TT- all prolonged; FDP-
increasedTreat the underlying causesFFP & Platelete concentrates

Advanced Liver Disease Acquired
Factor vii & x deficiencyEpistaxis, Menorrhagia and HemarthrosisLABS: BT,PC- normal; Factor x PT,PTT both elevated Factor vii PT- Prolonged; PTT- Normal; Specific factor assays Treatment: FFP & Vitk

Treatment Algorithm

Give Factor viii, dose calculated to bring patient’s plasma level to 100% 1 hour prior to surgery(50 units/kg q12h); Assay daily prior to dose
For Minor Surgery: Maintain plasma level > 60% for 1st 4days Maintain plasma level > 20% for next 4days For Major Surgery: Maintain plasma level > 60% for 1st 4days Maintain plasma level > 40% for next 4 days For Orthopedic Surgery: Maintain plasma level > 80% for 1st 4days Maintain plasma level > 40% for next 4 days

40yrs old man c/o bleeding PR Colonoscopy revealed single polyp in descending colon Colonoscopic snare polypectomy was done Postop profuse bleeding+ Labs: only B.T is prolonged; PC,PT,PTT- Normal Diagnosis& Treatment ?
Answer: Diagnosis Thrombocytopathy due to aspirin ingestion
Treatment Platelet concentrates

3 months old congenital Biliary Atresia baby Was brought with purpuric skin lesions&oozing from gums Labs: PT&PTT- prolonged; BT,PC- Normal Diagnosis & Treatment ?
Answer: Diagnosis Advanced liver disease Treatment FFP & individual factors x & vii

3 days old baby was brought with H/O Hemetemesis & Melena
O/E Well baby Labs: Hb –N; B.T,P.C,PT,PTT -Normal Diagnosis ?
Answer: Normal baby- No pathology Baby swallowed maternal blood during labour
and subsequently vomiting the same. No need for any treatment

60 yrs old man a case of ESRD on chronic hemodialysis Called to see him for profuse oozing from puncture site @ AV
fistula LABS: BT,PC,PT- normal; PTT, TT- prolonged Diagnosis and Treatment?
Answer: Diagnosis: Heparin overdosage Treatment: Protamine 1mgm counter 1 unit of heparin

12 yrs old girl on chronic hemodialysis for ESRD Uremia developed because of temporary interruption of
dialysis Developed brisk epistaxis Labs:BUN-164 mgms, BT>20mts Diagnosis & Treatment?
Answer: Diagnosis: Thrombocytopathy due to uremia Treatment: Platelet concentrates

50 yrs old lady with severe burns injury became febrile & toxic Epistaxis, Hemetemesis & melena Wound Swab Gram –ve sepsis Labs: BT,PC,PT&PTT,TT- all are prolonged Diagnosis & Treatment?
Answer: Diagnosis: DIC Treatment: FFP

THANK YOU
Subscribe to get notified regarding my
latest uploads