surgery class #3 part 2
TRANSCRIPT

SURGERY CLASS #3 Part 2
16 Januari 2021
Curriculum Vitae
Nama : Dr. Dion Faisal, Sp.B FICS
TTL : Balikpapan, 31 Mei 1985
Istri & anak :
Dr. Dian Manggiasih
Muhammad Nabil
Muhammad Dhafin
Pendidikan :
S1 Kedokteran Umum FK Unmul 2009
Spesialis Bedah Umum FK Unair 2018
Fellow International College of Surgeon 2020
Pekerjaan :
Kepala SMF Bedah, Subkomite Mutu
RSUD Tarakan
Webinar lecturer in General Surgery

THE PERFECT INTERN •
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
ADVANCED SURGICAL RECALL 4th ed

WHAT THE PERFECT SURGICAL STUDENT CARRIES IN HER LAB COAT
• Stethoscope
• Penlight
• Scissors
• Minibook on medications (e.g., trade names, doses)
• Tape/4 4s
• Sutures to practice tying
• Pen/notepad/small notebook to write down pearls
• Notebook or clipboard with patient’s data (always write down chores with a box next to them so you can check off the box when the chore is completed)
• Small calculator
• List of commonly used telephone numbers (e.g., radiology)
ADVANCED SURGICAL RECALL 6th ed


BUKU BEDAH GRATIS???
https://t.me/joinchat/H98ar0DCkng16V57nkxD-w
PEMBAHASAN

Berikut ini pernyataan yang tepat mengenai terapi radiasi pada keganasan
payudara, kecuali
a. Tidak digunakan pada semua tahap kanker payudara
b. Dapat dilakukan pre operasi
c. Pada perempuan yang menjalani mastectomy dengan kanker pada batas
pembedahan perlu radiasi post op
d. Pada stage III A radiasi diberikan untuk menurunkan rekurensi
e. Pada stage III A radiasi diberikan post op

RADIOTERAPI CA MAMMA
Indikasi :
1. Setelah BCS
2. Tepi sayatan dekat atau tidak bebas tumor
3. Tumor letak sentral atau medial
4. Tumor > 5cm ( T3 )
5. KGB (+) dengan ekstensi ekstra kapsuler
6. Kontrol lokal untuk perdarahan, fraktur
• Bahan isotop Co60 atau dengan sinar X
Volume target :
1. Mama
2. Axilla
• RT axilla setelah diseksi axilla radikal meningkatkan resiko limfedema
3. Supraclavicula
• Tidak dilakukan pada T2N0 atau stadium lebih rendah
4. Mamaria interna
• Pada lokasi tumor di sentral & medial
Komplikasi :
1. Nekrosis soft tissue, edem payudara, fraktur iga ( 1-3% )
2. Kelemahan gerak bahu ( 12-15% )
3. Brachial plexopathy
4. Limfedema
5. Sekunder malignansi : angiosarkoma, ca paru
6. Pneumonitis

Kemoterapi ajduvant pada keganasan payudara diberikan pada pasien berikut ini,
kecuali
a. Pasien usia di bawah < 70 tahun dengan kanker payudara stage I
b. Pasien usia di bawah < 70 tahun dengan kanker payudara stage IIA
c. Pasien usia di bawah < 60 tahun dengan kanker payudara stage IIB
d. Pasien usia di bawah < 70 tahun dengan kanker payudara stage IIB
e. Pasien usia di bawah < 70 tahun dengan kanker payudara stage III A

Immunohisto chemistry (IHC) • Jenis: ER/PR, Her2 Neu, Ki67
• Dari pemeriksaan IHC dapat ditentukan subtipe intrinsik biologi sel kanker berdasarkan kriteria St Gallen 2013
Subtipe intrinsik Definisi kliniko-patologi Rekomendasi terapi sistemik
Luminal A ER, PgR (+), Her2 (-)
Ki67 rendah (<14%)
Hormonal terapi
Luminal B Her2 (-)
ER (+), Her2 (-)
Salah satu dari :
- Ki67 tinggi ( > 14%)
- PgR (-) atau rendah
Hormonal + Kemoterapi
Her2 (+) /
Triple
positif
ER (+), Her2 (+)
Ki67 berapapun nilainya
PgR berapapun nilainya
Hormonal + Kemo + Targeted terapi
Erb-B2 overexpression
(Her2 type)
Her2 (+), ER dan PgR (-) Kemo + Targeted terapi
Triple negatif ( TNBC ) ER, PgR (-), Her2 (-) Kemoterapi
KEMOTERAPI CA MAMMA
1. Adjuvant diberikan setelah terapi utama
2. Neoadjuvant/induksi/preoperatif diberikan sebelum
terapi utama
3. Primer/terapeutik/paliatif diberikan pada kanker
stadium IV

ADJUVANT NEOADJUVANT Waktu Setelah terapi utama Sebelum terapi utama Ca mama EBC IIIA LABC Indikasi 1.KGB axilla (+)
2.KGB axilla (-) namun high risk
- usia < 40 th
- high grade
- ER/PR (-)
- Her 2 (+)
- Invasi limfatik atau vaskuler
- High tymidin index
3.Ukuran tumor > 2cm (dipertimbangkan jika ER +, Her 2 -)
1.LABC
2.High grade
3.(unicentris)
4.(ER/PR(-))
Evaluasi DFI, OS, efek samping Response rate, efek samping Keuntungan -Burden tumor minimal -Kontrol mikrometastasis
-Vaskularisasi masih baik
-Dapat menilai respon kemoterapi prognostic factor
-Downsizing
-Memungkinkan operasi yang lebih sederhana
Kerugian -Penilaian respon susah -Untuk grup yang tidak respon, penanganan lokoregional menjadi terlambat
-Burden tumor masih besar
-Peningkatan resiko operasi / radiasi

Rekomendasi Kemoterapi Adjuvant ( Devita, Principle & Practise of Oncology )
St Gallen Consensus
Conference
2005 – 2007
National Comprehensive
Cancer Network 2007
Her-2
(+)
Tidak tergantung ukuran T > 0,5 cm dan/atau N (+)
Her-2
(-) ER
(-)
Tidak tergantung ukuran T > 1 cm dan/atau N (+)
Dipertimbangkan untuk T
0,5-1 cm jika faktor
prognostik jelek
Her-2
(-)
ER (+)
N > 4 (+)
Dipertimbangkan jika
- T > 2 cm
- Grade 2-3
- Usia < 35 th
- Invasi lymphovakuler (+)
N (+)
Dipertimbangkan jika :
- T > 1 cm
- T 0,6-1 cm, invasi
lymphovaskuler (+)
- Grade 2-3
Kelompok wanita berikut ini yang tidak direkomendasikan mendapat tamoxifen
sebagai terapi kanker payudara adalah
a. Keganasan dengan reseptor esterogen +
b. Keganasan stage I
c. Menjalani mastektomi ipsilateral
d. Keganasan stage II
e. Menjalani mastektomi bilateral

HORMONAL TERAPI Indikasi :
1. ER/PR (+) > 10 mol/mg
2. Tanpa pemeriksaan reseptor ( ablasi )
• ER/PR (-) 16 % ada respon karena :
- Bisa terjadi mutasi sehingga menjadi ER/PR (+)
- Sifat heterogenitas, di satu sisi ER/PR (-), di lain tempat ER/PR (+)
Mekanisme kerja :
1. Additif pemberian estrogen, progesteron, kortikosteroid
2. Ablatif menghilangkan sumber estrogen dari ovarium dengan BSO atau radiokastrasi, adrenalektomi, hipofisektomi
3. Kompetitif blokade reseptor estrogen dengan Selective Estrogen Receptor Modulator (SERM) Tamoxifen
4. Supresi supresi sintesis estrogen langsung pada kelenjar adrenal dengan Aromatase Inhibitor atau pada hipofise dengan analog LHRH / GnRH

Pemilihan terapi hormonal
Disesuaikan dengan status menopause pasien. Untuk premenopause diberikan
Tamoxifen atau GnRH agonis, sedangkan untuk postmenopause diberikan
Aromatase Inhibitor diikuti Tamoxifen. Terapi hormonal diberikan selama 5 tahun
Menopause ( ACOG )
• 1. Usia > 55 th
• 2. Usia < 55 th, amenorhe > 12 bulan tanpa KB
• 3. Post BSO
• 4. Post radiokastrasi, amenorhe > 3 bulan
• 5. HRT, usia > 55 th

Tamoxifen
• Indikasi : hormonal terapi premenopause
• Cara kerja : blokade reseptor estrogen dengan Selective Estrogen Receptor Modulator
(SERM)
• Dosis : 20 mg/hr (selama 5 tahun, penelitian terbaru ada yang menyebutkan selama
10 tahun)
• Efek samping :
- Kanker endometrium: Tamoxifen bekerja pada reseptor α mamae secara antagonis
sedangkan pada reseptor β endometrium, prostat & liver bekerja secara agonis
terjadi kanker. Gejala : vaginal discharge
- Perimenopausal symptoms : hot flushes & mood changes Tx : selective serotonin
uptake inhibitor
- Katarak
Tn. J baru saja mengalami kecelakaan lalu lintas sejak 2 jam yang lalu. Warga
melihat leher pasien tertabrak mobil, dan segera dilarikan ke RS. Resusitasi dan
terapi awal sudah diberikan, saat ini keadaan pasien stabil. Jika dokter mencurigai
adanya fraktur C1, maka pemeriksaan penunjang paling baik yang perlu dilakukan
adalah
a. X ray Spine lateral
b. X ray spine posterior
c. X ray spine lateroposterior
d. CT scan
e. X ray spine lateroanterior

Fraktur yang terjadi pada C2 juga sering disebut sebagai
a. Jefferson Fracture
b. Odontoid Fracture
c. Kawasaki Fracture
d. Cowboy fracture
e. Horse rider fracture


Tatalaksana pada Hangman’s Fracture dari C 2 yang tidak didapatkan pergeseran
adalah dengan
a. Imobilisasi dengan halo vest
b. Imobilisasi dengan crtuches
c. Imobilisasi dengan spalk
d. ORIF
e. OREF


Fraktur kompresi yang terjadi pada C3, diterapi dengan menggunakan
a. Cervical brace dan analgesic
b. Cervical brace dan steroid
c. Halo vest dengan steroid
d. Steroid topical
e. OREF

CERVICAL FRACTURE BY MECHANISM
• compression fracture • compressive failure of
anterior vertebral body without disruption of posterior body cortex and without retropulsion into canal
• often associated with posterior ligamentous injury

• burst fracture
• characterized by • fracture extension through posterior
cortex with retropulsion into the spinal canal
• often associated with posterior ligamentous injury
• prognosis • often associated with complete and
incompete spinal cord injury
• treatment • unstable and usually requires
surgery

• flexion teardrop fracture
• characterized byanterior column failure in flexion/compression
• posterior portion of vertebra retropulsed posteriorly
• posterior column failure in tension
• larger anterior lip fragments may be called 'quadrangular fractures’
• prognosis • associated with SCI
• treatment • unstable and usually requires
surgery

• extension teardrop avulsion fracture
• characterized by • small fleck of bone is avulsed of
anterior endplate • usually occur at C2 • must differentiate from a true
teardrop fracture
• mechanism • extension
• prognosis • stable injury pattern and not
associated with SCI
• treatment • cervical collar

TREATMENT • Nonoperative
• collar immobilization for 6 to 12 weeks
• indications
• stable mild compression fractures (intact posterior ligaments & no significant kyphosis)
• anterior teardrop avulsion fracture
• external halo immobilization
• indications
• only if stable fracture pattern (intact posterior ligaments & no significant kyphosis)
• Operative
• anterior decompression, corpectomy, strut graft, & fusion with instrumentation
• indications
• compression fracture with 11 degrees of angulation or 25% loss of vertebral body height
• unstable burst fracture with cord compression
• unstable tear-drop fracture with cord compression
• minimal injury to posterior elements
• early decompression (< 24 hours) has been shown to improve neurologic outcomes compared with delayed (>/ 24 hours) decompression
• posterior decompression, & fusion with instrumentation
• indications
• significant injury to posterior elements
• anterior decompression not required


Mekanisme yang dapat menyebabkan trauma pada saraf perifer adalah, kecuali
a. Laserasi
b. Stretched
c. Compressed
d. Contusio
e. Reductio



Tn. D 50 tahun, dicurigai menderita trauma saraf perifer setelah tangannya terkena
pisau saat mempertahankan diri dari perampok. Saat ini pasien kehilangan fungsi
pada nervus ulnaris pada tangan kirinya. Tatalaksana berupa pembedahan
eksplorasi diindikasikan pada
a. Saat ini juga
b. Tidak perlu karena nervus sudah rusak
c. Observasi 3 bulan, jika tidak ada perbaikan maka lakukan pembedahan
eksplorasi
d. Jika tidak membaik dalam 3 hari
e. Tidak perlu karena cukup dengan terapi neurotropika



Grinsell, D & Keating, C. (2014). Peripheral Nerve Reconstruction after Injury: A Review of Clinical and Experimental Therapies. BioMed research international. 2014. 698256.
10.1155/2014/698256.

Tn. J datang ke dokter dengan keluhan nyeri perut kiri bawah. Nyeri perut terjadi
terus menerus dan semakin berat. Pada pemeriksaan fisik ditemukan nyeri perut
kiri bawah dan demam, pemeriksaan lain dalam batas normal. Pada pemeriksaan
CT Scan nampak pericolic soft tissue stranding, penebalan dinding kolon, dan
flegmon. Diagnosis pasien ini yang paling mendekati adalah
a. Apendisitis
b. Ca colon
c. Diverticulitis
d. Cholelitihiasis
e. Pendarahan kolon

DIVERTIKEL KOLON
• Protrusi dinding kolon berbentuk kantong dengan leher sempit, berukuran beberapa milimeter sampai dua sentimeter.
• Divertikel sejati (true diverticle): kantong terdiri dari seluruh lapisan dinding kolon
• Divertikel palsu (false diverticle): kantong hanya terdiri dari lapisan mukosa dan submukosa
• Sering ditemukan di kolon, terutama sigmoid
• Penyebab
• Tekanan intra luminal yang tinggi
• Defek dinding kolon pada tempat keluarnya arteri ke appendiks epiploika
• Tekanan intra lumen tergantung kepadatan feses


Gambaran Klinik
• 80 % tanpa gejala
• Keluhan : • Nyeri • Obstipasi • Diare • Gangguan motilitas usus
• Gejala jelas bila ada komplikasi
• Pemeriksaan foto barium dapat membantu diagnosa
• Pemeriksaan endoskopi untuk diagnosa

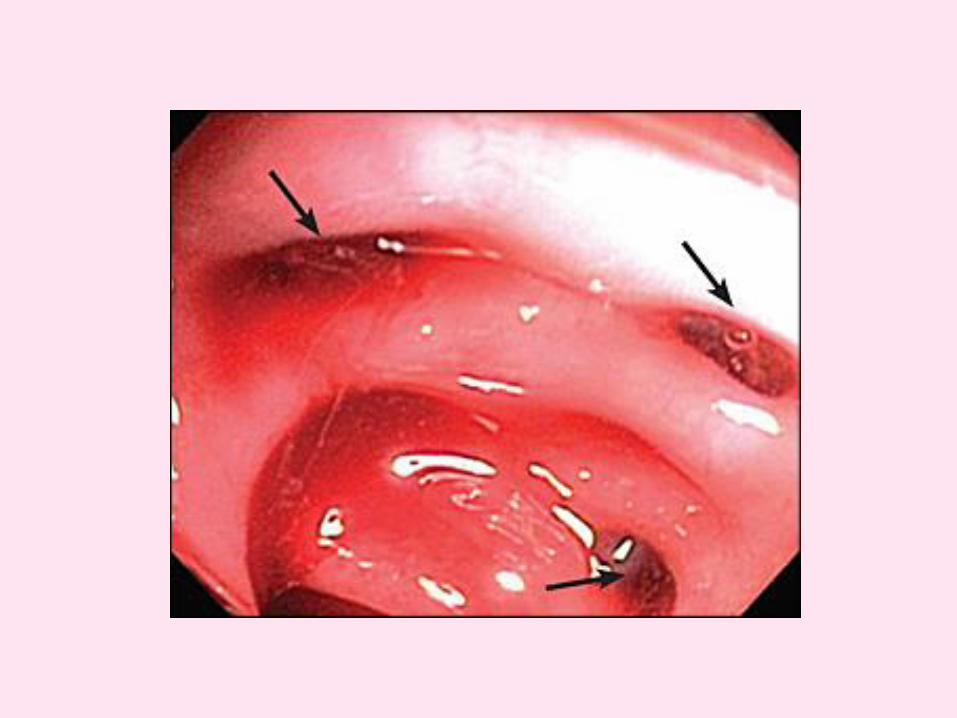
Divertikulitis
Peridivertikulitis
Abses
Perforasi
Peritonitis
Fistula entero-kolo -vesikal
Perdarahan
Obstruksi karena fibrosis pasca radang
Komplikasi Divertikel Kolon
Divertikulitis
• Radang akut dari divertikel
• Disebabkan retensi feses
• Gejala klinik : • Nyeri lokal
• Serangan akut
• Konstipasi
• Diare
• Pemeriksaan foto barium dan endoskopi dilakukan setelah proses akut reda

Terapi
1. Tanpa keluhan tidak perlu terapi 2. Fase akut
–Puasa –Cairan parenteral –Pemasangan pipa lambung –Antibiotika sistemik –Analgetika
3. Fase tenang –Reseksi kolon –Reseksi sigmoid metode Hartmann
4. Terapi bedah diperlukan bila timbul komplikasi : • Perforasi • Perdarahan hebat • Fistula • Obstruksi

Pendarahaan pada diverticulum colon terjadi akibat
a. Pecahnya anastomosis
b. Pecahnya polip colon
c. Erosi ariteriol peridiverticular
d. Erosi kolon primer
e. Pecahnya abses kolon

Berikut ini pernyataan yang tepat mengenai diverticula kolon sisi kanan
a. Paling sering terjadi pada ras afrika
b. Terjadi paling banyak pada lansia
c. Umumnya tidak menunjukkan gejala
d. Jarang terjadi
e. Sering salah diagnosis sebagai keganasan

Tn. J, 50 tahun, baru saja mengalami kecelakaan lalu lintas dengan kepala bagian
depan terbentur aspal. Pada pemeriksaan fisik ditemukan luka terbuka pada regio
frontal. Pada pemeriksaan radiologis ditemukan fraktur orbita. Sebelum melakukan
tatalaksana pembedahan pada fraktur orbita, hal apa yg perlu dilakukan
a. Memeriksa apa ada riwayat katarak
b. Memeriksa apakah ada riwayat laserasi kornea
c. Mengeksklusi globe rupture
d. Memeriksaa apakah ada kerusakan pada nervus olfaktori
e. Memeriksa kerusakan nervus optikus

GLOBE RUPTURE
• Occurs when the integrity of the outer membranes of the eye is disrupted by blunt or penetrating trauma.
• Any full-thickness injury to the cornea, sclera, or both is considered an open globe injury and is approached in the same manner in the acute setting.
• Globe rupture is an ophthalmologic emergency and requires definitive management by an ophthalmologist.
• Damage to the posterior segment of the eye is associated with a very high frequency of permanent visual loss.
• Prompt recognition and ophthalmologic intervention are essential to maximizing functional outcome.

Operating microscope view of a globe rupture secondary to blunt trauma by a fist. Notice the dark arc in the bottom of the photo representing the ciliary body visible through the
scleral breach. Subconjunctival hemorrhage of this severity should raise suspicion of occult globe rupture. Photo courtesy of Brian C Mulrooney, MD.

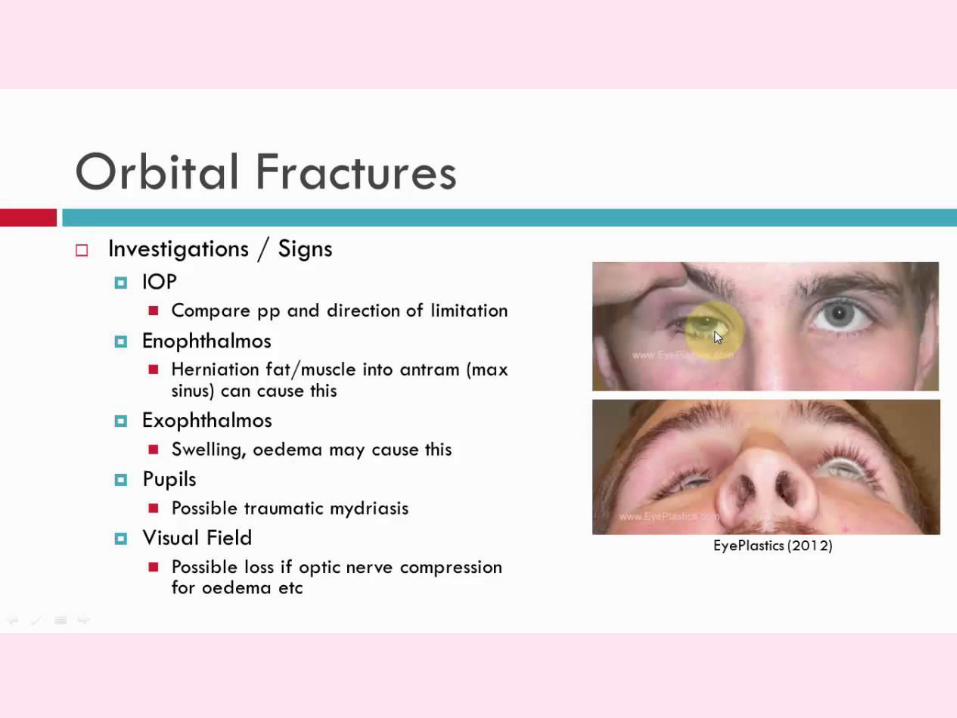
Selain sindroma apeks orbita, komplikasi lain yang dapat muncul dari fraktur orbita
adalah
a. Orbital fissure syndrome
b. Ortholi syndrome
c. Jackson syndrome
d. Horner syndrome
e. Open floor globe fracture

Superior orbital fissure syndrome (SOFS)
• Known as Rochen-Duvigneaud syndrome is a collection of symptoms caused by
compression of structures just anterior to the orbital apex
• The complex and crowded anatomy of the superior orbital fissure produces a
characteristic pattern of cranial nerve, pupillary and extraocular findings.
• The most frequent cause is now known to be trauma (0.3-0.8%). Common
associations are motorcycle accidents, zygomatic fractures and orbital fractures.
• Other causes include neoplasms (particularly lymphoma and
rhabdomyosarcoma), infections (such as meningitis), syphilis, sinusitis, herpes
zoster, inflammation (such as SLE, sarcoidosis, Tolosa-Hunt syndrome) and
vascular phenomena (such as carotid-cavernous fistulas, retro-orbital haematoma
and carotid aneurysms), or idiopathic.
• The syndrome is characterized by ophthalmoplegia, ptosis, proptosis of eye,
dilation and fixation of the pupil, and anesthesia of the upper eyelid and
forehead.

ANATOMY
Frontal view of right internal orbit indicated
optic foramen (arrow), superior orbital fissure
(arrowhead), and inferior orbital fissure (line).
Contents of right superior orbital
fissure.

• Ptosis lost tension and function of the levator palpebrae superior muscle involving the superior branch of the oculomotor nerve, and loss of tone in Muller's muscle involving the sympathetic fiber arising from the cavernous sinus.
• Proptosis decreased tension of the extraocular muscles, which normally are
globe retractors, thereby allowing forward movement of the globe.
• The fixed dilated pupil with loss of accommodation disruption of the parasympathetic fibers coursing with the oculomotor nerve.
• Compromise of the lacrimal and frontal nerves of the ophthalmic branches of the trigeminal nerve anesthesia of the forehead and upper eyelid, lacrimal hyposecretion, and possibly in retro-orbital pain and neuralgia along the path of the nerve.
• Because of the disruption of the sensory nasociliary nerve anesthesia of the cornea and the bridge of the nose with loss of the corneal reflex.
• If the optic nerve is also involved including the above-mentioned symptoms, it is known as the orbital apex syndrome, a term coined by Kjaer.

Fractures of right temporal, sphenoid, and zygomatic bone are observed on the
computed tomographic (CT) scan. The superior orbital fissure (arrow) becomes
narrow and compressed by the sphenoid fracture. (A) Submental view on three-
dimensional CT (3D-CT). (B) Coronal plane. (C) Horizontal plane.
Chen CT, Chen YR. Traumatic superior orbital fissure syndrome: current
management. Craniomaxillofac Trauma Reconstr. 2010;3(1):9-16. doi:10.1055/s-
0030-1249369

Bagian yang paling rentan terjadi fraktur pada orbita adalah
a. Apeks
b. Dinding anterior
c. Dinding medial
d. Dinding lateral
e. Dasar orbita


Berikut ini merupakan batas-batas tulang zygoma, kecuali
a. Tulang sphenoid di medial
b. Maksila di medial
c. Maksila di inferior
d. Frontal di superior
e. Temporal di lateral


Berikut ini adalah etiologic yang dapat menyebabkan striktur uretra kecuali
a. Trauma
b. Iatrogenik
c. Inflamasi
d. Idiopathic
e. Autoimun

Anatomi uretra
• Dibagi 2 : A. Anterior : pars bulbosa pars pendulosa fossa naviculare B. Posterior : pars prostatica pars membranacea
• Epitel pelapis uretra anterior : epitel skuamous uretra posterior : epitel transisional
A. Melalui uretra pars bulbosa
B. Melalui uretra pars pendulosa
C. Melalui uretra pada bagian koronal penis
D. Melalui fossa navicularis

Batasan
• Penyempitan atau penyumbatan dari lumen uretra
sebagai akibat dari pembentukan jaringan fibrotik
(jaringan parut) pada uretra dan/ atau pada daerah
peri uretra
• Penyebab:
• Infeksi: uretritis GO, infeksi ikutan akibat kateter
indwelling
• Trauma:
iatrogenik : kateterisasi, kaliberasi, reseksi transuretra,
tindakan endourogi lain
eksterna : patah tulang panggul, straddle injury

Patah tulang panggul

Straddle injury

Patogenesis
Infeksi
Trauma
Lesi epitel uretra putusnya kontinuitas uretra
Proses keradangan Reaksi Fibrosis / kolagen
Jaringan fibrotik
Penyempitan lumen uretra
Penyumbatan lumen uretra
Bila terjadi kebocoran urine
(ekstravasasi urin)
Keradangan periuretra
Terjadi abses
Fistel uretrokutan

Jenis Striktur Uretra
A. Lipatan mukosa / mucosal fold
B. Kontriksi iris / iris constriktion
C. Fibrosis minimal
D. Spongiofibrosis
E. Inflamasi dan fibrosis sampai jaringan corpus spongiosum
F. Striktur dengan komplikasi fistel. Dapat terbentuk abses,
fistel kearah kulit dan rektum

Gejala klinis
• Kesukaran kencing
• Harus mengejan
• Pancaran mengecil
• Pancaran bercabang
• Menetes sampai retensi urine
• Pembengkakan / nanah di perineum
• Kadang bercak darah di celana dalam
• Bila sistemik : febris, warna urine keruh

Tatalaksana striktur uretra terbagi menjadi dua yaitu endoskopi dan rekonstruksi.
Tatalaksana rekonstruksi dilakukan melalui
a. Balantomi
b. Uretrotomi
c. Uretroplasti
d. Uretrogram
e. Uretroinsisial

Penatalaksanaan
• Tergantung : lokalisasi panjang / pendeknya striktur keadaan darurat : retensio urine
• Dilatasi uretra (periodik) harus dengan halus dan hati-hati kontraindikasi : anak kecil striktur cenderung timbul kembali
• Uretrotomi interna : visual (sachse) blind (Otis)

Penatalaksanaan
• Selalu dilakukan uretrotomi lebih dahulu kecuali terdapat fistel uretrokutan atau abses periuretra
• Follow up : dilatasi uretra hidrolik self catheterization
• Penyulit follow up : perdarahan false passage infeksi restriktur

Penatalaksanaan
• Bila dilatasi atau uretrotomi gagal, atau terdapat fistel atau abses periuretra : plastik uretra satu tahap bila tak ada infeksi plastik uretra 2 tahap bila inf + 1. eksisi jar. Abses/fistel 2. rekonstruksi uretra bila striktur o.k. trauma di uretra post : operasi melalui perineum transpubik dg pubektomi pada kasus yg tak mungkin rekonst: uretroperiostomi permanen sistostomi permanen urine diversion

Catatan untuk dokter umum
• Diagnosa ditegakkan dengan : anamnesa, pemeriksaan fisik, colok dubur, coba kateterisasi
• Retensi urine: sistostomi , kemudian rujuk
• Infiltrat urine: sistostomi, insisi multipel, kemudian rujuk bila proses infeksi sudah tenang

Standar baku emas pemeriksaan penunjang untuk mendiagnosis trauma ginjal
adalah
a. CT Urogram
b. Biopsi ginjal
c. UGFR serial
d. Urin tampung 24 jam
e. Urin serial setiap 3 jam
Trauma GINJAL
• klinis: • anamnesa: mode of injury • pem. fisik : jejas • urinalisis: hematuria
• mekanisme trauma: tr.tajam, tr.tumpul
• klasifikasi (Moore dkk 1989)
• 1. Trauma ginjal minor (85% kasus) • grade I & II
• 2. Trauma ginjal mayor (15% kasus) • grade III, IV, & V
• 3. Trauma vaskular

DIAGNOSIS
• evaluasi • anamnesa
• jejas
• urin keluar? Warna?
• hati2 trauma organ lain: costae, abdomen
• CT Abdomen kontras
• IVP (harus dilakukan, terutama untuk melihat ginjal kontralateral)
• USG, arteriografi (angiography) bila perlu
DIAGNOSIS
• evaluasi dan diagnosa
Riwayat trauma +
atau Hematuria
Ax: trauma lumbal
deselerasi mendadak + / -
Fx: hematoma lumbal
luka penetrasi

TERAPI
• Terapi konservatif • observasi:
• tanda2 vital: T/N/t • masa lumbal • warna urine serial • tanda anemis / Hb serial
• Indikasi bedah:
• perdarahan tak dapat diatasi • injury renovascular • parenkhim tidak viable • ektravasasi urin luas • pembedahan: laparotomi eksplorasi, repair, k/p nefrektomi

AAST Grading
Renal injury scale of The American Association for The Surgery of trauma
Grade Description
I Contusion Micros/gross hematuria, urologic studies normal
II Hematoma Subcapsular, non expanding without parenchymal laceration
Non expanding perirenal hematoma confined to renal peritoneum
III Laceration <1 cm parenchymal depth of renal cortex w/o urinary extravasation
IV Laceration >1 cm parenchymal depth of renal cortex w/o collecting system rupture or urinary extravasation
Laceration parencymal laceration extending through the renal cortex, medulla, & collecting system
V Vascular main renal artery or vein injury with contained hemorrhage
Laceration completely shattered kidney
Vascular Avulsion of renal hilum, which devascularizes kidney

Tn. J, 55 tahun, datang dengan keluhan nyeri perut kolik hilang timbul, demam,
tidak mau makan, dan muntah, serta obstipasi. Pada pemeriksaan fisik nampak
perut yang distended dengan peningkatan bising usus. Pada pemeriksaan
penunjang ditemukan leukositosis ringan dan abnormalitas dari serum elektrolit.
Diagnosis yang paling mendekati adalah
a. Gastritis
b. Barett’s eosphagus
c. Obstruksi usus halus
d. Polip colon
e. Ileus paralitik

BOWEL OBSTRUCTION TERMINOLOGY
• “Simple” obstruction: the bowel is blocked, compressed, or kinked, but its vascular supply is not threatened.
• Strangulation-obstruction: the vascular supply to the segment of obstructed bowel is compromised.
• Closed-loop obstruction: a segment of bowel is obstructed at a proximal and distal point. Commonly, the involved bowel is strangulated.
Plain abdominal X-ray
• Partial obstruction: there is gas seen in the colon in addition to the small bowel distension with fluid levels.
• Complete obstruction: no gas is seen in the colon. Moshe Schein, Paul N. Rogers, Ahmad Assalia. Schein’s Common Sense Emergency
Abdominal Surgery An unconventional book for trainees and thinking surgeons. Third Edition

Peritoneal adhesions
• “peritoneal adhesions” or simply “adhesions” is defined as fibrous tissue that connects surfaces or organs within the peritoneal cavity that are normally separated.
• The results of a pathological healing response of the peritoneum upon injury, as opposed to the normal “ad integrum” repair.
• Typical adhesions form after peritoneal injury from abdominal surgery.
• Other conditions include radiotherapy, endometriosis, inflammation, and local response to tumors.

SMALL BOWEL OBSTRUCTION
• a surgical emergency in which the obstruction of the small intestine hinders passage of intestinal contents.
• Characterized by abdominal pain, vomiting, distention, and constipation.
• Adhesions are the single most common cause for small bowel obstruction.
• Nonadhesive etiologies of bowel obstruction include incarcerated hernias, obstructive lesions (malignant and benign), bezoars, inflammatory bowel disease, and volvulus.
• Definitive confirmation of the adhesive etiology of bowel obstruction is made during operative treatment.
• Methods to confirm the adhesive etiology of bowel obstruction non-invasively include a history of previous episodes of bowel obstruction by adhesions or exclusion of other causes of bowel obstruction by imaging (often CT scan).

Pemeriksaan penunjang obstruksi usus halus yang paling tepat pada setting gawat
darurat adalah
a. CT Scan abdomen dengan kontras oral
b. CT Scan abdomen tanpa kontras
c. BOF LLD
d. MRI Abdomen tanpa kontras
e. MRI abdomen dengan kotnras

Imaging studies
• Plain X-rays: In high-grade obstruction, a triad of multiple air-fluid levels, distention of small bowel loops, and absence of gas in the colon are pathognomonic for small bowel obstruction, overall sensitivity and specificity are low (sensitivity approximately 70%)
• Water-soluble contrast studies: If the contrast has not reached the colon on an abdominal X-ray taken 24 h following administration of the contrast, this is highly indicative of failure of non-operative management.

• CT scans: not only have good test characteristics for diagnosing small bowel obstruction but also have approximately 90% accuracy in predicting strangulation and the need for urgent surgery. Diagnostic value of CT scan can be enhanced with the use of water-soluble contract.
• Ultrasound: operator dependent but in experienced hands can provide more information than plain X-rays, and is also available in most low income settings. Apart from distension of bowel loops, ultrasound enables detection of free fluid (that might indicate the need for urgent surgery) and assessment of the degree of shock in dehydrated patients.

Tatalaksana obstruksi usus halus parsial adalah sebagai berikut, kecuali
a. Laparatomi eksplorasi
b. Analgesik
c. Resusitasi cairan
d. Pemasangan NGT
e. Monitor keluaran urin

Adhesive small bowel obstruction (ASBO)
• Common surgical emergency, causing high morbidity and even some mortality.
• The adhesions causing such bowel obstructions are typically the footprints of previous abdominal surgical procedures.
ten Broek, R.P.G., Krielen, P., Di Saverio, S. et
al. Bologna guidelines for diagnosis and
management of adhesive small bowel obstruction
(ASBO): 2017 update of the evidence-based
guidelines from the world society of emergency
surgery ASBO working group. World J Emerg
Surg 13, 24 (2018). https://doi.org/10.1186/s13017-018-0185-2

Bowel obstruction ec. adhesi
Small bowel obstruction

Adhesi intestinal grade 3

RECOMENDATIONS
• Adhesion formation might be reduced by minimally invasive surgical techniques and the use of adhesion barriers.
• Non-operative treatment is effective in most patients with ASBO.
• Contraindications for non-operative treatment include peritonitis, strangulation, and ischemia.
• When the adhesive etiology of obstruction is unsure, or when contraindications for non-operative management might be present, CT is the diagnostic technique of choice.
• The principles of non-operative treatment are nil per os, naso-gastric, or long-tube decompression, and intravenous supplementation with fluids and electrolytes.
• When operative treatment is required, a laparoscopic approach may be beneficial for selected cases of simple ASBO.

Berikut ini langkah-langkah yang dapat mencegah adhesive small bowel
obstruction kecuali
a. Teknik bedah yg baik
b. Handle jaringan yang hati-hati
c. Paparan yang lebih dari instrument pada peritoneum
d. Bedah laparoskopi
e. Pemberian agen hyaluronan
ASBO PREVENTION
• Surgical technique
• Adhesion barriers: solid membranes, gels, and liquids hyaluronate carboxymethylcellulose
• Secondary prevention
ten Broek, R.P.G., Krielen, P., Di Saverio, S. et al. Bologna guidelines for diagnosis and
management of adhesive small bowel obstruction (ASBO): 2017 update of the evidence-
based guidelines from the world society of emergency surgery ASBO working
group. World J Emerg Surg 13, 24 (2018). https://doi.org/10.1186/s13017-018-0185-2

Berikut ini merupakan factor risiko untuk necrotizing enterocolitis, kecuali
a. Bayi post date
b. Inisasi makan enteral
c. Asfiksia
d. Kanulasi arteri umbilical
e. PDA

NEC RISK FACTORS
Preterm:
• Birth weight < 1000 g
• Highest risk with lowest GA
• Feeding: Unstandardized approach to feeding and management of feeding intolerance, Formula feeding, Breast milk fortifier
• H2 blockers
• Chorioamnionitis
• Sepsis
• Number of infections
• Prolonged (≥5 d) first course of antibiotics
• Patent ductus arteriosus
• Indomethacin treatment
• Glucocorticoids and Indomethacin in first week of life
• Absence of umbilical arterial catheter
• Mechanical ventilation
• Transfusions
• HIV-positive mother
• Antenatal cocaine use
• Perinatal asphyxia
• Apgar score < 7 at 5 min
• Black race
• Antenatal glucocorticoids
• Morphine infusion
• Vaginal delivery
Gephart SM, McGrath JM, Effken JA, Halpern MD. Necrotizing enterocolitis risk: state of the science. Adv Neonatal Care. 2012;12(2):77-89. doi:10.1097/ANC.0b013e31824cee94

NEC RISK FACTORS
Late Preterm and Full-Term Infants:
• Cyanotic congenital heart disease
• Polycythemia
• Intrauterine growth restriction
• Formula feeding
• Maternal hypertensive disease
• HIV-positive mother
• Umbilical catheters
• Exchange transfusion
• Perinatal asphyxia
• Mechanical ventilation
• Sepsis
• Maternal illicit drug use
• Respiratory distress syndrome
• Apgar score < 7 at 5 min




Tanda patognonomonik untuk necrotizing enterocolitis dari pemeriksaan radiologis
adalah
a. Double bubble
b. Single bubble
c. Olive sign
d. Pneumatosis intestinalis
e. Pneumatosis kredens

Pneumatosis intestinalis in a patient of NEC. White arrow showed portal venous gas. Black arrow linear or string sign. Hollow white arrow
showed soap bubble sign.

Pneumoperitoneum. Big white arrows showed air under diaphragm leading to its elevation. Small white arrows
delineate pushed down liver border. Empty arrows show Rigler's sign.

CT Pneumatosis intestinalis in a patient of NEC

@dionfaisal31
Life only has one rule:
Never quit. – Unknown
Surgery Class
SEMOGA BERMANFAAT