supporting people who use drugs & providers: hep c info & care magdalena harris london...
TRANSCRIPT

Supporting people who use drugs & providers: hep C info & care
Magdalena Harris London School of Hygiene and Tropical Medicine
[email protected] LJWG Conference - Hepatitis C in London – practical steps to elimination
17 November 2014, London.
Overview
• State of play in the UK: Prevention, testing & treatment?
– What is the role of hep C literacy?
• Hepatitis C information needs: PWID & providers
– Current resource provision
• Our response: LJWG & LSHTM partnership
Information resource development & production
• The process ….
• The resources
• Next steps
The state of play in the UK …. • Prevalence ~185,000 people living with chronic hep C
• Prevention 90% new cases due to use of unsterile injecting equipment
• TestingOnly ~40% of people diagnosed: ~100,000 undiagnosed 36% of PWID attending drug services have never received a hep C test
• Treatment<3% receive treatment in the UK. Few are current PWID
• Elimination? Requires intensive scale up of prevention initiatives, case finding (often ex-PWID) & treatment provision for current PWID
What is the role of hep C literacy?• For prevention
– Enhance safe practices
• For testing– Reduce rates of undiagnosed
• For treatment– Increase access to & uptake of HCV treatment
• For health – Enable engagement in health care & HCV self management
• For empowerment – Enhance needed advocacy & activism

An information need: PWID• PreventionThrough them years, I have used a spoon that maybe someone else has used, but I’ve never used dirty works. You know, nothing dirty. (Max)
• TestingI’ve had boosters for hep C. I’m not due anymore boosters now. (Colin)
• Treatment With the treatment, you can’t use or drink alcohol or anything on top (Ivana)
• Hep C / cirrhosisI just want to know what’s going on with me, what do the pains mean? Can you tell, what is my [life] expectancy? ... It’s scary because you haven’t got a clue what’s going on. (Frieda)
An information need: providers ….• Missed opportunities for hep C prevention information • Missed opportunities for testing • Missed opportunities for treatment referral & initiation
I was only diagnosed last June, but I had been backwards and forwards to the GP for many years just unwell and they did loads of tests, even gave me a hysterectomy, full hysterectomy, had the lot out ... so I don’t know if that was necessary or not. (Jane)
The [drug services] workforce haven’t got the right information so they don’t feel confident in helping someone to make the decision about treatment. (Focus group)
I think that we lack the tools. Almost all that I do in consultation is verbal, and yet I’m a very visual person. I would much sooner somebody showed me in pictures what cirrhosis was … massively [ helpful] just to have a resource that I can show somebody what cirrhosis looks like. (Hepatologist)
Current resources • Poor range & availability There’s nothing about hep C in the doctor’s surgery, there’s nothing about hep C in the hepatology clinic, you’d think that it’s about liver health, there’s nothing about hep C. (Sally)
• Language employed can be stigmatising, misleading, moralising“What kinds of people get hepatitis C ...”“people around you are only at risk if they come in contact with your bodily fluids”“taking recreational drugs is dangerous and harmful to your health”
• Perceived as out of date / patronising … This is what is still on display in my GPs, this is ’03, they look dated … And the language in some of them, this is what I was given at [hospital] when we talked about treatment … the language used in that, I didn't like it at all, I found it very patronising. (Rita)
Our response ….
• Resource development plan (LJWG & LSHTM)
• Focus groups / workshops assessing need & developing content
– Initial focus: treatment decision making resource
• Gilead support – making project tangible
– Advisory board meeting, additional workshops, writer & designer
• A broader scope
– Two booklets: Hep C info, Hep C care
• An iterative process – bottom up!
– Resource development working group & advisory group
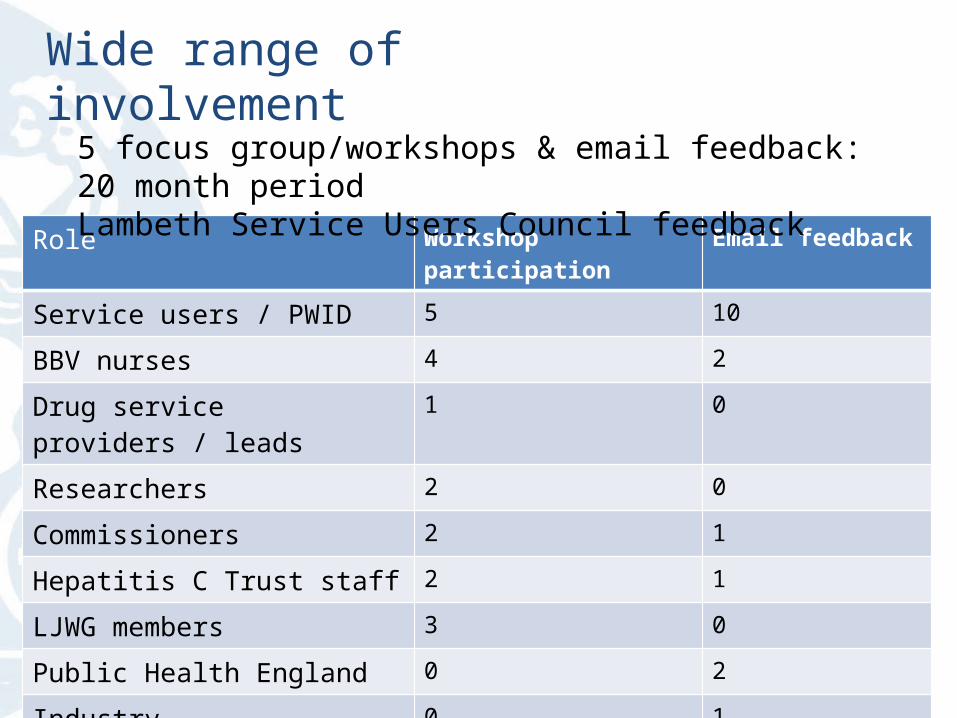
Wide range of involvement
Role Workshop participation Email feedback
Service users / PWID 5 10
BBV nurses 4 2
Drug service providers / leads 1 0
Researchers 2 0
Commissioners 2 1
Hepatitis C Trust staff 2 1
LJWG members 3 0
Public Health England 0 2
Industry 0 1
Total 19 17
5 focus group/workshops & email feedback: 20 month periodLambeth Service Users Council feedback
What was important?
• Clear, non-stigmatising language & visuals
• Rights rather than responsibility emphasis
• Harm reduction info acknowledging structural constraints to best practice
• Non-biased, not pushing treatment
• Drawing on research findings (re barriers & what is important to PWUD)
• Incorporating voices of people living with hepatitis C &/or PWUD
• Signposting links to other support

What was included? Resource 1: Hep C info• Understanding hep C: prevalence, role of liver, natural history, cirrhosis,
symptoms, transmission • Testing: where to go, what it involves, antibody/PCR, testing reasons and
rights, changing GP info, availability of DBS• Disclosure: family/friends, work, finance, medical etc• Staying safe: where to get injecting supplies, how to inject safely,
tattooing / piercing info, transmission around the home /first aidResource 2: Hep C Care• Understanding hep C: genotypes, natural history, cirrhosis• Living well with hep C – symptoms, self management, lifestyle• Treatment: rights, eligibility (OST info, co-infection), testing / liver
monitoring, new & current treatments, side effects, self management, support, appointment & medications, treatment pros & cons
• Support/ resource links (in both booklets)

Some examples• Rights basedAll people with hep C are entitled to assessment and, unless there is a medical reason (contraindication) such as pregnancy, heart disease or severe depression, they are also entitled to treatment
• Real voicesI come back and I told her, she was outside waiting for me, and she took one look at my face and she went, “It is isn’t it?” and I went, “Yeah,” and then I started crying and she went, “It’s alright, don’t worry about it, you know, I’ll do the test now and see if I’ve got it and if we have we’ll both start treatment and we do this together babe,”(Abel)
• Pragmatic harm reduction adviceIf you can’t clean a surface for preparing your hit or if you’re injecting outside, use a layer of tissue, toilet paper, or newspaper to lay your injecting equipment on.
Ongoing / next steps….
• Workshop at 4th National Recovery Conference, Glasgow
• Launch of resources at LJWG conference
• Resource circulation to Addaction South West, Blenheim CDP, Lambeth & Southwark
• Feedback collation, changes to content & redesign
• January 2015: larger print run & distribution
• Paper on process for peer-reviewed journal
• PHE has supported concept of wider roll out.
• Possible evaluation

Current design
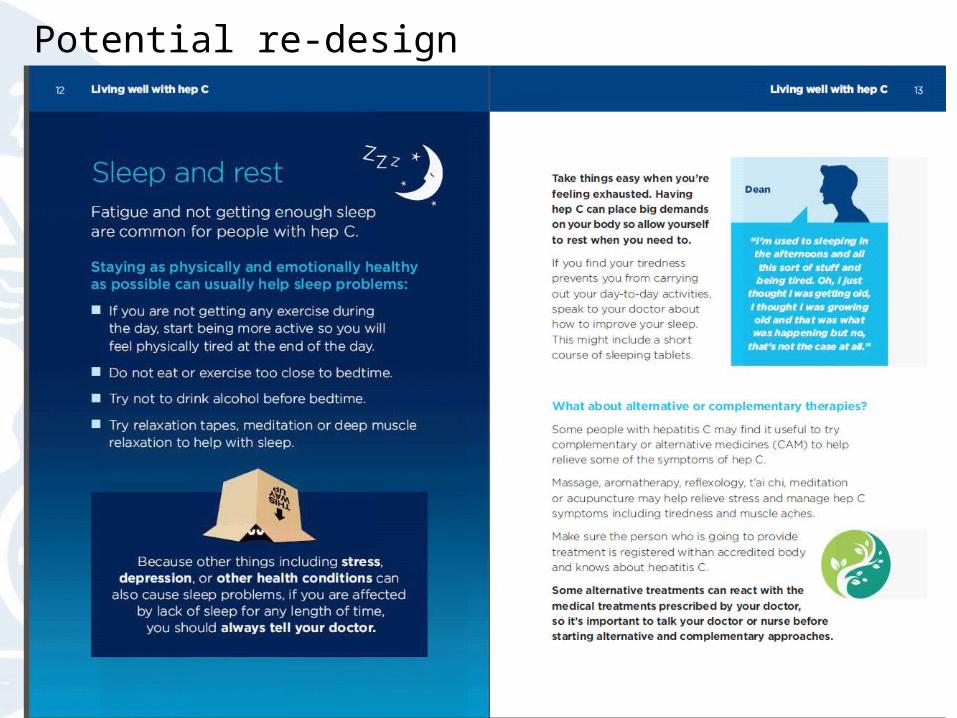
Potential re-design

In summary• Little knowledge among PWID about eligibility for treatment • Little knowledge about new treatments on horizon• Few referrals & treatment assessments despite eligibility • Many missed opportunities for testing and diagnosis
• A desire for relevant hep C information: PWID & providers
• Resources were produced in partnership & through consultation• Vital peers are central to any intervention development • Information → advocacy → action
I don’t think we can underestimate the impact of patient power or lobbying that actually brought about change in terms of accessing those drugs for people living with HIV. (Hepatologist)
Acknowledgements • Everyone who took part in the resource development process!!!
THANK YOU!!!!
• Lambeth Service Users Council
• Danny Morris, Jon Daniel, Dee Cunniffe, Nicola Brett, Claire Munro, David Badcock, Murad Ruf, Ashley Brown, David Nutt
• The Hepatitis C Treatment Journey study participants, partners & study sites.
• National Institute of Health Research, Gilead Sciences, LJWG
• Magdalena Harris is funded by a National Institute of Health Research Postdoctoral fellowship: NIHR-PDF-2011-04-031