supplementary appendix - the lancet€¦ · supplementary appendix ... ketonal or fastum gel or...
TRANSCRIPT

Supplementary appendixThis appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors.
Supplement to: da Costa BR, Reichenbach S, Keller N, Nartey L, Wandel S, Jüni P, Trelle S. Effectiveness of non-steroidal anti-inflammatory drugs for the treatment of pain in knee and hip osteoarthritis: a network meta-analysis. Lancet 2016; published online March 17. http://dx.doi.org/10.1016/S0140-6736(16)30002-2.

WEB-APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of
Osteoarthritis Pain: A Network Meta-Analysis
Table of Contents Web-appendix 1. Search Strategy ........................................................................................................... 2
Web-appendix 2. Additional methods ................................................................................................... 10
Main model: Random walk ................................................................................................................. 10
Alternative model 1: Full exchangeability ......................................................................................... 13
Alternative model 2: Unconstrained baseline, random-walk on treatment effect ....................... 15
References ............................................................................................................................................ 18
Web-appendix 3. Definitions used to classify trials according to components of methodological
quality ......................................................................................................................................................... 19
Web-appendix 4. Flow diagram and references of included trials .................................................... 20
Web-appendix 5. Treatment effect according to time point ............................................................... 26
Web-appendix 6. Assessment of Model Fit .......................................................................................... 29
Web-appendix 7. Inconsistency ............................................................................................................. 30
Web-appendix 8. Analyses using alternative models for network meta-analysis .......................... 34
Web-appendix 9. Results of adjusted models ..................................................................................... 36
Web-appendix 10. Comparison adjusted funnel plots ........................................................................ 41

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
2 | 42
Web-appendix 1. Search Strategy MEDLINE and EMBASE were searched through the OVID platform (www.ovid.com). The Cochrane
Central Register of Controlled Trials was searched through the Cochrane library
(http://www.cochranelibrary.com/). The search was last updated on February 24 2015.
Cochrane Central Register of Controlled Trials (CENTRAL)
Step Search Strategy
1 (osteoarthriti* OR osteoarthro* OR gonarthriti* OR gonarthro* OR coxarthriti* OR coxarthro*
OR arthros* OR arthrot*) in Clinical Trials
2 MeSH descriptor Osteoarthritis explode all trees
3 1 OR 2
Ovid (MEDLINE and EMBASE)
Step Search Strategy
1 randomized controlled trial.pt.
2 controlled clinical trial.pt.
3 randomized controlled trial.sh.
4 random allocation.sh.
5 double blind method.sh.
6 single blind method.sh.
7 clinical trial.pt.
8 exp clinical trial/
9 (clin$ adj25 trial$).ti,ab.
10 ((singl$ or doubl$ or trebl$ or tripl$) adj25 (blind$ or mask$)).ti,ab.
11 placebos.sh.
12 placebo$.ti,ab.
13 random$.ti,ab.
14 research design.sh.
15 comparative study.sh.
16 exp evaluation studies/
17 follow up studies.sh.
18 prospective studies.sh.
19 (control$ or prospectiv$ or volunteer$).ti,ab.
20 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19
WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
3 | 42
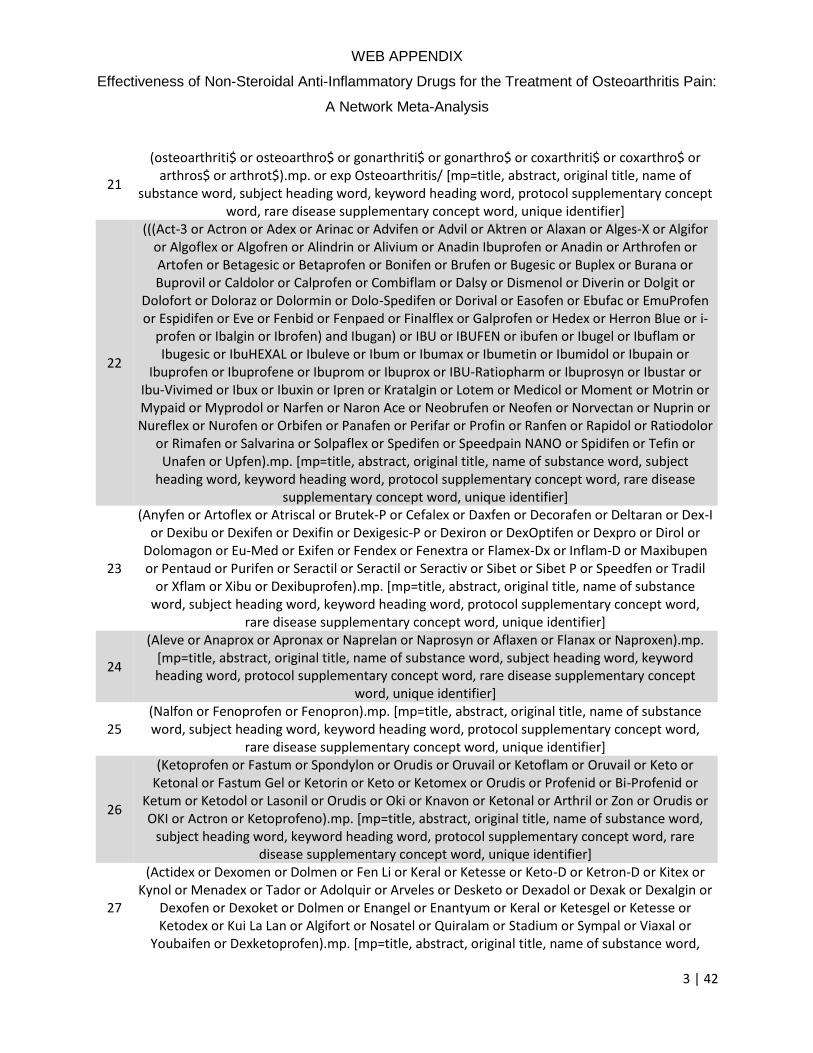
21
(osteoarthriti$ or osteoarthro$ or gonarthriti$ or gonarthro$ or coxarthriti$ or coxarthro$ or arthros$ or arthrot$).mp. or exp Osteoarthritis/ [mp=title, abstract, original title, name of
substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
22
(((Act-3 or Actron or Adex or Arinac or Advifen or Advil or Aktren or Alaxan or Alges-X or Algifor or Algoflex or Algofren or Alindrin or Alivium or Anadin Ibuprofen or Anadin or Arthrofen or Artofen or Betagesic or Betaprofen or Bonifen or Brufen or Bugesic or Buplex or Burana or Buprovil or Caldolor or Calprofen or Combiflam or Dalsy or Dismenol or Diverin or Dolgit or
Dolofort or Doloraz or Dolormin or Dolo-Spedifen or Dorival or Easofen or Ebufac or EmuProfen or Espidifen or Eve or Fenbid or Fenpaed or Finalflex or Galprofen or Hedex or Herron Blue or i-
profen or Ibalgin or Ibrofen) and Ibugan) or IBU or IBUFEN or ibufen or Ibugel or Ibuflam or Ibugesic or IbuHEXAL or Ibuleve or Ibum or Ibumax or Ibumetin or Ibumidol or Ibupain or
Ibuprofen or Ibuprofene or Ibuprom or Ibuprox or IBU-Ratiopharm or Ibuprosyn or Ibustar or Ibu-Vivimed or Ibux or Ibuxin or Ipren or Kratalgin or Lotem or Medicol or Moment or Motrin or Mypaid or Myprodol or Narfen or Naron Ace or Neobrufen or Neofen or Norvectan or Nuprin or Nureflex or Nurofen or Orbifen or Panafen or Perifar or Profin or Ranfen or Rapidol or Ratiodolor
or Rimafen or Salvarina or Solpaflex or Spedifen or Speedpain NANO or Spidifen or Tefin or Unafen or Upfen).mp. [mp=title, abstract, original title, name of substance word, subject
heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
23
(Anyfen or Artoflex or Atriscal or Brutek-P or Cefalex or Daxfen or Decorafen or Deltaran or Dex-I or Dexibu or Dexifen or Dexifin or Dexigesic-P or Dexiron or DexOptifen or Dexpro or Dirol or
Dolomagon or Eu-Med or Exifen or Fendex or Fenextra or Flamex-Dx or Inflam-D or Maxibupen or Pentaud or Purifen or Seractil or Seractil or Seractiv or Sibet or Sibet P or Speedfen or Tradil
or Xflam or Xibu or Dexibuprofen).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word,
rare disease supplementary concept word, unique identifier]
24
(Aleve or Anaprox or Apronax or Naprelan or Naprosyn or Aflaxen or Flanax or Naproxen).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept
word, unique identifier]
25 (Nalfon or Fenoprofen or Fenopron).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word,
rare disease supplementary concept word, unique identifier]
26
(Ketoprofen or Fastum or Spondylon or Orudis or Oruvail or Ketoflam or Oruvail or Keto or Ketonal or Fastum Gel or Ketorin or Keto or Ketomex or Orudis or Profenid or Bi-Profenid or
Ketum or Ketodol or Lasonil or Orudis or Oki or Knavon or Ketonal or Arthril or Zon or Orudis or OKI or Actron or Ketoprofeno).mp. [mp=title, abstract, original title, name of substance word,
subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
27
(Actidex or Dexomen or Dolmen or Fen Li or Keral or Ketesse or Keto-D or Ketron-D or Kitex or Kynol or Menadex or Tador or Adolquir or Arveles or Desketo or Dexadol or Dexak or Dexalgin or
Dexofen or Dexoket or Dolmen or Enangel or Enantyum or Keral or Ketesgel or Ketesse or Ketodex or Kui La Lan or Algifort or Nosatel or Quiralam or Stadium or Sympal or Viaxal or
Youbaifen or Dexketoprofen).mp. [mp=title, abstract, original title, name of substance word,

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
4 | 42
subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
28 (Ansaid or Flurbiprofen).mp. [mp=title, abstract, original title, name of substance word, subject
heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
29 (Daypro or Oxaprozin).mp. [mp=title, abstract, original title, name of substance word, subject
heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
30
(An Pu Luo or Analoxo or Bei Luo or Cobalokinin or Confatanin or Kentan or Letrac or Lexofen or Lobafen or Lobu or Lockpain or Locpren or Loxefin or Loxfen or Loxfenine or Loxipain or
Loxipronal or Loxodfen or Loxofen or Loxomarin or Loxonin Dongwha or Loxonin or Loxot or Loxpain or Luo Lie Tong or Luo Na or Nobfen or Okiminas or Oxeno or Ponapelt or Qing Fu or
Ringereaze or Rokifen or Roseol or Roxonin or RoxsogenRuo Mai or Sai Ke Tong or San Yuan Shu or Xing or Sanloxo or Tsurumerin or Unastin or Weikang Dike or Zhen Tong Yan or Loxoprofen or Loxomac).mp. [mp=title, abstract, original title, name of substance word, subject heading word,
keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
31 (Indocid or Indocin or Tivorbex or Indometacin).mp. [mp=title, abstract, original title, name of
substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
32 (Tolectin or Tolmetin).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease
supplementary concept word, unique identifier]
33 (Clinoril or Sulindac).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease
supplementary concept word, unique identifier]
34
(Etodolac or Lodine or Etova or Dualgan or Etodin or Etofree or Etopan or Flancox or Haipen or Proxym or Etol or Eccoxolac).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare
disease supplementary concept word, unique identifier]
35 (Toradol or Acular or Sprix or Ketorolac).mp. [mp=title, abstract, original title, name of substance
word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
36
(Diclofenac or Aclonac or Cataflam or Voltaren or Cambia or Zipsor or Zorvolex or Lodex or Flector or Pennsaid or Solaraze).mp. [mp=title, abstract, original title, name of substance word,
subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
37 (Aceclofenac or Hifenac or Cincofen or Nacsiv or Acenac).mp. [mp=title, abstract, original title,
name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
38 (Nabumetone or Relafen or Relifex or Gambaran).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept
word, rare disease supplementary concept word, unique identifier]
39 ((Piroxicam or Candyl or Arantil or Brexidol or Brexin or Erazon or Exipan or Faxiden or Felden or Feldene or Feldoral or Flamexin or Hawksone or Hotemin or Lubor or Mobilis or Novo-Pirocam

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
5 | 42
or Pirox von ct or Proponol or Reumador or Remox or Roxam or Sinartrol or Toricam or Tracam or Ugesic or Veral) and Vurdon).mp. [mp=title, abstract, original title, name of substance word,
subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
40 (Meloxicam or Mobic).mp. [mp=title, abstract, original title, name of substance word, subject
heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
41
(Tenoxicam or Admiral or Alganex or Algin-Vek or Amcinafal or Apo-Tenoxicam or Artoxan or Artricom or Artroxicam or Aspagin or Atroxicam or Bart or Biodruff or Dolmen or Hobaticam or Indo-Bros or Inoten or Istotosal or Liaderyl or Memzotil or Mitrotil or Mobiflex or Neo Kalmol or Neo-Antiperstam or Neo-Endusix or Notritis or Octiveran or Oksamen or Oksamen-L or Oxaflam or Oxicam or Oxytel or Palitenox or Pilopil or Ponsolit or Portonal or Pycitil or Redac or Reutenox or Rheuflex or Rucornart or Seftil or Sinoral or Soral or Sutondin or Teconam or Teflan or Tenax
or Tencam or Tenocam or Tenoksan or Tenorix or Tenotec or Tenox or Tenoxicam Generis or Tenoxicam LPH or Tenoxicam Mintlab or Tenoxicam Mylan or Tenoxicam Sanitas or Tenoxicam
or Tenoxil or Tenoxin or Tentepanil or Tenxil or Texicam or Thenil or Tilarco or Tilatil or Tilcitin or Tilcotil or Tilflam or Tilko or Tilnoxcam or Tiloxican or Tobitil or Tonox or Toscacalm or Velasor or
Vienoks or Voir or Xicotil or Zibelant or Zikaral).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept
word, rare disease supplementary concept word, unique identifier]
42 Droxicam.mp. [mp=title, abstract, original title, name of substance word, subject heading word,
keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
43
(Lornoxicam or Acabel or Bosporon or Camri or Coslor-PDa Lu or Hypodol or Lezdes-P or Lolira-P or Lorcam or Lorchek-MR or Lorchek-P or Lornica or Lornofan or Lornoxi or Lornoxi-P or Lorsaid
or Lorter-P or Lorter-P Forte or Lorthox-P or Lorup Plus or Lorwalk or Luloxy-P or Mitilor or Movilor or Neucam or Neucam-P or Noxon or Powernac-L or Qinda or Quando or Renox-A or
Taigalor or Telos or Univer or Xafon or Xefo or Xefocam or Xilor or Zelorn or Zheng Ting or Chlortenoxicam).mp. [mp=title, abstract, original title, name of substance word, subject heading
word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
44 (Isoxicam or Floxicam or Maxicam or Pacyl or Vectren).mp. [mp=title, abstract, original title,
name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
45
(Mefenamic acid or Dolfenal or Beafemic or Mefalth or Mefalth or Mefivan or Ponstel or Ponstan or Ponstal or Parkemed or Revalan or Mafepain or Mefamed or Mephadolor or Meftal
or Dyfenamic or Potalon or Meyerdonal or Alfoxan or Fenagesic or Fenamin or Spiralgin or Almus or Mefacit or Pangesic Forte or Kalmadol or Fespa or Mefcox or Mefanorm or Meftal or
Mefkind or Vidan).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease
supplementary concept word, unique identifier]
46
(Flufenamic acid or Antirheumatic or Flufemin or Kanyen or Mobilat or Suyanlen or Flufen or Opaferumin or Opyrin or Youfenil or Combec or Fenazol).mp. [mp=title, abstract, original title,
name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
6 | 42
47
(Tolfenamic acid or Clotam or Clotan or Dolfenax or Fenamic or Flocur or Gantil or Migea or Purfalox or Te Fen Ta or Tolfedine or Tolfejec or Tolfine or Tolmic or Tufnil or Turbaund).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept
word, unique identifier]
48 (Celecoxib or Celebrex or Celebra).mp. [mp=title, abstract, original title, name of substance
word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
49 (Rofecoxib or Vioxx or Ceoxx or Ceeoxx).mp. [mp=title, abstract, original title, name of substance
word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
50 (Valdecoxib or Bextra).mp. [mp=title, abstract, original title, name of substance word, subject
heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
51
(Parecoxib or Dynastat or Praxis or Rayzon or Valdy-P or Valto-P or Valus-P or Vorth-P or Dynastat or Pro-Bextra or Valdure).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word,
rare disease supplementary concept word, unique identifier]
52 (Lumiracoxib or Prexige).mp. [mp=title, abstract, original title, name of substance word, subject
heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
53
(Etoricoxib or Algirex or Algix or Arcoxia or ARCOXIA or Artorix or Auxib or Coxet or Coxia or Ebov or Eflam or Eoxy-H or Erofica or Eticox or Eto or Etocox or Etodolo or Etody or Etofan or
Etoflam or Etom or Etorica or Etorix or Etoshine or Etoxib or Etro or Etrobax or Exinef or Exxiv or Hicox or Hireto or Ifydrox or Kingcox or Kretos or L-Kon or M-Kon or Nucoxia or Nucoxia-P or
Nucoxia-SP or Oricox or Ranacox or Retoz or Ribox or Rito or Setorib or Tauxib or Tory or Tro or Tro-P or Turox or Xibra or Ezact or Coxyveen or Vargus or Starcox or Exxiv).mp. [mp=title,
abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique
identifier]
54 (Firocoxib or Equioxx or Previcox).mp. [mp=title, abstract, original title, name of substance word,
subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
55
(Nimesulide or Actalide or Actasulid or Actinim or Aglonim or Ainex or Alencast or Algifeno or Algimesil or Algolider or Algosulid or Algover or Allgone or Ameolin or Amocetin or Amsolide or
Anjielishu or Antalor or Aponil or Areuma or Arslide or Artilide or Aulin or Auromedil or Auromelid or Bangni or Biolin or Bioxidol or Blunid or Ceralide-MD or Chemisulide or Cimelide or
Cliovyl or Coxtral or Deflogen or Degorflan or Dimesul or Discorid or Doloc or Dolonime or Dolostop or Domes or Drexel or Edrigyl or Efridol or Elinap or Emdon or Enetra or Erlecit or
Erreflog or Eskaflam or Fansulide or Feverein or Fladalgin or Flamide or Flogostop or Fu Mei Shu or Genlide or Hua Shuang Jie or Huang Xing Yun Shu or Igrexa RD or Igrexa or Isodol or Kartal or Kind-MD or Kitedo-Li or Lalide or Lanimex or Ledoren or Lemesil or Li Nuo Ke or Li Shu Tong or Lizepat or Lovirem or Lupisulide or Magenol or Maoxing or Melicat or Melimont or Mesilex or
Mesulid or Mesupon or Min-a-pon or Minesulin or Mosuolit or Motival or Moxenil or Multiformil or Myxina or Nam or Naofid or Nemil-Os or Neosili or Neosulida or Neptide or

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
7 | 42
Nerelid or New Nicip or Nexen or Niberan or Nibid or Nidol or Nidolon or Nile or Nilide or Nilup or Nimalgex or Nimdal or Nimdus or Nimed or Nimedol or Nimegel or Nimegesic or Nimel or Nimelid or Nimelide or Nimepast or Nimepis or Nimes or Nimesil or Nimesilam or Nimesul or
Nimesulid or Nimesulide or Nimesuvar or Nimesyl or Nimeter or Nimex or Nimfast or Nim-H or Nimica or Nimill or Nimind or Nimiz or Nimlide or Nimm or Nimo or Nimotas or Nimotas-CD or
Nimras-MD or Nims or Nimulex-FD or Nimulid or Nimustar or Nimutab or Nimvar-MD or Nimvista or Nincolide or Nisalgen or Nise or Nisulid or Nisural or Niyan or Nizer or Normosilen or
Novolid or NS100 Nimesulide or Nuleb or Numusyp or Nuo Zheng or Oronime or Orthobid or Orthobid Plus or Orthobid-MR or Pacimol Plus or Pantames or Pentra or Pu Fei Te or Pu Wei or
Pymenimis or Pyranim or Qnim or Quelodin or Reduben or Relisulide or Relmex or Remesulid or Remov or Reumolide or Ristolzit or Ritamine or Rolaket or Romasulid or Rui Li or Rui Pu Le or Rui
Zhi Li or Rui Zhi Qing or Sai Pu Da or Scaflam or Scaflan or Scalid or Seren-N or Serralex-NM or Severin or Severin NF or Shan Yi Ting or Si Rui or Solving or Soonil or Specilid or Suaron or Sulicox or Sulidamor or Sulidene or Sulidex or Sulidin or Sulidor or Sumo or Sumo or Sumo-MR or Sumo-Spas or Surong or Tengke or Tizanim or Tizu or Toro-Sanovel or Tranzicalm or Tredical or Ventor or Virobron or Volonten or Windose or Xianleke or Xilox or Ximede or Yi Mei Li or Yi Ya Xuan or
Zalide or Zimnil or Zitroflam or Zolan or Zolandin-MR or Maxsulid or Nimecox or Nimedex or Penalgin or Sulide or Coxtal or Sintalgin or Octaprin or Nimside or Nilsid or Donulide or Heugan
or Minapon or Nilden or Nimed or Nimedex or Nimesil or Nimulid or Nimutab or Nimdase or Nimopen or Nisulid or Nodard or Nicip or Nimcap or Nic or Nic-Spas or Novolid or Relmex or
Remisid or Scaflam or Scaflan or Sulidin or Xilox or Modact or Sulidene or Zolan or Lusemin or Medicox or Nidol or Nimalox or Nimesil or Nimotas or Nimulid or Nizer or Sorini or Ventor or
Vionim or Neolide or Willgo or Nims).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word,
rare disease supplementary concept word, unique identifier]
56
(Clonixin or Adoplan or Algimate or Blonax or Celex or Clonalgin or Clonix or Clonixil or Clonixinato de lisina Larjan or Clonixinato de lisina Mintlab or Clonixinato de lisina Sanderson or
Clonixinato de lisina or Colmax or Dentagesic or Diclen or Disinal or Dolalgial or Dolamin or Dolex or Donodol or Dorix or Dorixina or Dorixina Forte or Dorixina or Dorixyl or Firac or Fultat or
Laboxina or Lafigesic or Ledosin or Libralgen or Lisina Clonixinato or Lixitin or Nefersil or Sedepron or Valoron).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease
supplementary concept word, unique identifier]
57 (Licofelone or Harpagide).mp. [mp=title, abstract, original title, name of substance word, subject
heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
58
(Pranoprofen or Cesflan or Difen Oculum or Difen or Flanin or Mulchina or Niflan or Oftalar or Pranofen or Pranoflog or Pranoprofen-Hai Shan Pharm or Pranopulin or Pranox or Pransus or
Proranon or Rupock or Valraizer).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare
disease supplementary concept word, unique identifier]
59
(Tiaprofenic acid or Acide Tiaprofenique or Apo-Tiaprofenic or Atrogem or Bi-Tiapram or Flanid or Pain Will Pass or Refen or Sufen or Sulgem or Sulimen or Surgam Leciva or Surgam Retard or
Surgam or Surgamyl or Suroten or Surugafen or Sutain or Synotec or Tecon or Tia Ton or Tiagam or Tiap or Tiaprofenic Acid Zensei Yakuhin or Tifen or Tifenic or Tiogam or Tiprofen or Turganil or

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
8 | 42
Tiaprofen).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary
concept word, unique identifier]
60 (Alminoprofen or Minalfene).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare
disease supplementary concept word, unique identifier]
61
(Zaltoprofen or Borbit or Peleton or Peon or Salafapinon or Soleng or Soleton or Soluirubin or Zaltoprofen Tatsumi Kagaku or Zatferon or Zyrogen).mp. [mp=title, abstract, original title, name
of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
62 (Amfenac or Fenazox).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease
supplementary concept word, unique identifier]
63
(Acemetacin or Acemet or Acemetacin-CT or Aceo or Baydol or Cobametacin or Emflex or Pranex or Pranex LP or Rantudal or Rantudil or Rheutrop or Shun Song or Tilur or Acemetadoc or
Acephlogont or Azeat or Gamespir or Oldan or Reudol or Ost-map).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol
supplementary concept word, rare disease supplementary concept word, unique identifier]
64
(Proglumetacin or Afloxan or Bruxel or Afloxan or Miridacin or Protaxil or Protaxon forte or Proxil or Tolindol).mp. [mp=title, abstract, original title, name of substance word, subject
heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
65 (Mofezolac or Disopain).mp. [mp=title, abstract, original title, name of substance word, subject
heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
66 (Ampiroxicam or Ampiroam or Flucam).mp. [mp=title, abstract, original title, name of substance
word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
67 (Tiaramide or Bemidon or Solantal or Tiamide or Tiaram).mp. [mp=title, abstract, original title,
name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
68 (Epirizole or Karmarte or Mebron or Melon or Meyuan or Miton).mp. [mp=title, abstract,
original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
69 (Emorfazone or Emazon or Pentoil or Therapyace).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept
word, rare disease supplementary concept word, unique identifier]
70 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 or 51 or 52 or 53 or 54 or
55 or 56 or 57 or 58 or 59 or 60 or 61 or 62 or 63 or 64 or 65 or 66 or 67 or 68 or 69
71 exp Anti-Inflammatory Agents, Non-Steroidal/ or ($steroidal and ($inflammatory or
$rheumatic)).mp. or ((Prostaglandin or Cyclooxygenase or Cyclo-Oxygenase or COX$) adj3 (Inhibitor$ or Antagonist$)).mp.
72 (Acetaminophen or Paracetamol or Tylenol or Datril or Panadol or Dafalgan or Panadol or Tipol or Calpol).mp. [mp=title, abstract, original title, name of substance word, subject heading word,

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
9 | 42
keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier]
73 70 or 71 or 72
74 20 and 21 and 73
75 limit 74 to (humans and "all adult (19 plus years)")
76 limit 75 to yr="2009 -Current"

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
10 | 42
Web-appendix 2. Additional methods
Main model: Random walk
The assumption that the standardized effects at each timepoint are fully exchangeable around a
common standardized effect (alternative model 1) may be considered too restrictive, especially
when the course of the disease has a potential temporal pattern. We may weaken this
assumption by using a (first order) random walk. A random walk of first order assumes that any
adjacent standardized effects are more similar to each other than non-adjacent standardized
effects. Therefore, if there is an underlying temporal pattern, a random walk model may capture
this more appropriately than a full exchangeability model.
We use the following notation:
𝑖 denotes the study
𝑘 denotes the study arm
𝑡 denotes the timepoint
𝑡𝑟𝑡(𝑖, 𝑘) denotes the treatment in arm 𝑘 in study 𝑖
𝑏𝑠𝑙(𝑖) denotes the “baseline” treatment in study 𝑖
𝑔 = 1,2, …, are the treatments
𝑥𝑖 is a covariate on the study-level (e.g. adequate blinding)
In mathematical terms, the model is then written as follows:
𝑠𝑒𝑓𝑓𝑖𝑡𝑘| 𝜃𝑖𝑡𝑘, 𝑠𝑒𝑖𝑡𝑘~ 𝒩(𝜃𝑖𝑡𝑘 , 𝑠𝑒𝑖𝑡𝑘2 )
𝑓𝑜𝑟 𝑡 > 1
𝜃𝑖𝑡𝑘| 𝜃𝑖(𝑡−1)𝑘, 𝜏𝑡𝑖𝑚𝑒~ 𝒩(𝜃𝑖(𝑡−1)𝑘, 𝜏𝑡𝑖𝑚𝑒2 )
and
𝜃𝑖1𝑘 = {𝜇𝑖 𝑖𝑓 𝑡𝑟𝑡(𝑖, 𝑘) = 𝑏𝑠𝑙(𝑖)
𝜇𝑖 + δ𝑖𝑘 𝑒𝑙𝑠𝑒
𝛿𝑖𝑘| 𝑑𝑡𝑟𝑡(𝑖,𝑘), 𝑑𝑏𝑠𝑙(𝑖), 𝜏𝑅𝐸~ 𝒩(𝑑𝑡𝑟𝑡(𝑖,𝑘) − 𝑑𝑏𝑠𝑙(𝑖) + 𝛽 ∗ 𝑥𝑖 , 𝜏𝑅𝐸2 )
Furthermore, the following prior distributions were used:
𝜇𝑖~𝑁(0,1000)
𝑑𝑔~𝑁(0,1000)
𝛽~𝑁(0,1000)

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
11 | 42
𝜏𝑡𝑖𝑚𝑒~ 𝒰(0,50)
𝜏𝑅𝐸−2 ~ 𝒢(0.1,0.1)Ι(0,2000)
We note a few points with respect to this model:
𝜃𝑖𝑡𝑘 is the estimated standardized effect of arm 𝑘 in study 𝑖 at timepoint 𝑡
𝜏𝑡𝑖𝑚𝑒2 is the variance determining how close two adjacent 𝜃𝑖𝑡𝑘 are to each other
𝜇𝑖 is the baseline effect at time 1 in study 𝑖
𝛿𝑖𝑘 is the treatment effect at time 1 in study 𝑖
𝑑𝑔 is the overall (treatment) effect at timepoint 1
An adjustment for multi-arm trials based on the approach proposed by Cooper et al1
was done (for simplification, this is omitted in the model formulation above)
One advantage of such (or any similar model) is that it can handle incomplete data structures,
i.e. also in studies for which outcome data was reported only for some of the timepoints of
interest. In a Bayesian framework, such an incomplete data structure does not pose a problem.
For example, studies which only reported outcomes at later timepoints (t > 1) will contribute less
to the estimated treatment effect 𝑑𝑔 since they are naturally down-weighted through the random
walk structure.
One challenge with such a model is that the estimated overall treatment effects corresponds to
timepoint 1. Thus, we performed our main analysis using timepoint 4 as the reference timepoint
and performed a sensitivity analysis with timepoint 1 as the reference (data not shown).
Timepoint 4 was selected because a) it was the timepoint where most trials reported data and b)
it was considered more clinically relevant than timepoint 1.
WinBUGS code used for random walk model (timepoint 4 as reference i.e. main analysis)1: model {
for(i in 1:nobs){
prec.t[i,4] <- pow(set[i,4],-2)
sefft[i,4] ~ dnorm(mean.t[i,4],prec.t[i,4])
mean.t[i,4] <- mu[trial[i]] + delta[trial[i],arm[i]]
rest[i,4] <- (mean.t[i,4] - sefft[i,4])
for(k in 1:3){
prec.t[i,k] <- pow(set[i,k],-2)
sefft[i,k] ~ dnorm(mean.t[i,k],prec.t[i,k])
mean.t[i,k] <- mu[trial[i]] + delta[trial[i],arm[i]]
rest[i,k] <- (mean.t[i,k] - sefft[i,k])
1 The code includes two additional priors for the between-trial heterogeneity that we used to assess sensitivity
of the analysis to the prior distribution. These additional analyses showed similar results.

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
12 | 42
}
for(k in 5:n.times){
prec.t[i,k] <- pow(set[i,k],-2)
sefft[i,k] ~ dnorm(mean.t[i,k],prec.t[i,k])
mean.t[i,k] ~ dnorm(mean.t[i,k-1],prec.RW[k])
rest[i,k] <- (mean.t[i,k] - sefft[i,k])
}
}
for (j in 1:ns){
mu[j] ~ dnorm(0,0.001)
delta[j,1] <- 0
w[j,1] <- 0
for (k in 2:na[j]){
delta[j,k] ~ dnorm(md[j,k],tau[j,k])
md[j,k] <- d[t.s[j,k]] - d[t.s[j,1]] + sw[j,k] + beta*x[j]
tau[j,k] <- 2*tau.re*(k-1)/k
w[j,k] <- delta[j,k] - (d[t.s[j,k]] - d[t.s[j,1]] + beta*x[j])
sw[j,k] <- sum(w[j,1:(k-1)])/(k-1)
}
}
d[1] <- 0
for (k in 2:nt){
d[k] ~ dnorm(0,0.001)
}
beta ~ dnorm(0,0.001)
prec.RW[1] <- 0
indep[1] <- 0
for(i in 2:n.times){
sd.RW[i] <- pow(prec.RW[i], -0.5)
prec.RW[i] <- prec.RW.which[i,indep[i]]
prec.RW.which[i,1] <- prec.RW.common
prec.RW.which[i,2] <- pow(sd.RW.indep[i], -2)
sd.RW.indep[i] ~ dunif(0, 50)
}
prec.RW.common <- pow(sd.RW.common, -2)
sd.RW.common ~ dunif(0,50)
tau.re ~ dgamma(0.1,0.1)I(0,2000)
# Alternative prior: half normal
# tau.re <- pow(sd.re,-0.5)
# sd.re ~ dnorm(0,1)I(0,)
# Alternative prior: Rhodes 20152, drug versus placebo
# tau.re ~ dgamma(0.21,0.0003) #
}

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
13 | 42
In order to model a treatment specific dose-response relationship, for each preparation the
maximum approved dose in Switzerland for the indication “osteoarthritis” was defined as the
reference dose. The treatment effect d is with respect to this reference dose, and for the
remaining doses of the preparation, the respective treatment effect was defined as
𝑑𝑔′ = 𝛾𝑔 ∗ log (
𝑑𝑜𝑠𝑒′
𝑟𝑒𝑓𝑒𝑟𝑒𝑛𝑐𝑒 𝑑𝑜𝑠𝑒)
Non-informative prior distributions (normal with mean 0 and variance 1000) were given for the
parameters 𝛾𝑔 .
Alternative model 1: Full exchangeability
This model has been previously used in a network meta-analysis investigating the effectiveness
of food supplements for the treatment of osteoarthritic pain.3 It makes a relatively strong
assumption on full exchangeability in the sense that any variation between timepoints is thought
to be random around study-arm-specific standardized mean effects in the trial. In other words, it
assumes that observations over time randomly vary around an average study-arm specific
reduction.
In mathematical terms:
𝑠𝑒𝑓𝑓𝑖𝑡𝑘| 𝜃𝑖𝑡𝑘, 𝑠𝑒𝑖𝑡𝑘~ 𝒩(𝜃𝑖𝑡𝑘 , 𝑠𝑒𝑖𝑡𝑘2 )
𝜃𝑖𝑡𝑘|𝜇𝑖, 𝛿𝑖𝑘 , 𝜏𝑣 ~𝒩(𝜇𝑖 + 𝛿𝑖𝑘 , 𝜏𝑣2)
𝛿𝑖𝑘|𝑑𝑡𝑟𝑡(𝑖,𝑘), 𝑑𝑏𝑠𝑙(𝑖), 𝜏𝑅𝐸 {= 0 𝑖𝑓 𝑡𝑟𝑡(𝑖, 𝑘) = 𝑏𝑠𝑙(𝑖)
~𝒩(𝑑𝑡𝑟𝑡(𝑖,𝑘) − 𝑑𝑏𝑠𝑙(𝑖) + 𝛽 ∗ x𝑖, 𝜏𝑅𝐸2 ) 𝑒𝑙𝑠𝑒
Furthermore, the following prior distributions were used:
𝜇𝑖~𝒩(0,1000)
𝑑𝑔~𝑁(0,1000)
𝜏𝜈~ 𝒰(0,50)
𝜏𝑅𝐸−2 ~ 𝒢(0.001,0.001)Ι(0,2000)
We note a few points:
𝜃𝑖𝑡𝑘 is the estimated standardized effect of arm 𝑘 in study 𝑖 at timepoint 𝑡

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
14 | 42
𝜏𝜈 is the variance determining how close the arm-specific standardized effects are
distributed around the overall arm-specific standardized effect
𝜇𝑖 is the average standardized baseline effect in study 𝑖
𝛿𝑖𝑘 is the average treatment effect in study 𝑖
𝑑𝑔 is the overall (treatment) effect
An adjustment for multi-arm trials based on the approach proposed by Cooper et al1
was done (for simplification, this is omitted in the model formulation above)
𝜏𝜈~ 𝒰(0,50)
𝜏𝑅𝐸−2 ~ 𝒢(0.001,0.001)Ι(0,2000)
WinBUGS code used for full exchangeability model: model {
for(i in 1:nobs){
for (k in 1:na[trial[i]]){
prec.y[i,k] <- pow(se[i,k],-2)
seff[i,k] ~ dnorm(mean.y[i,k],prec.y[i,k])
res[i,k] <- (mean.y[i,k] - seff[i,k])
mean.y[i,k] ~ dnorm(nu[i,k],prec.nu[i,k])
prec.nu[i,k] <- pow(sd.nu[i,k],-2)
sd.nu[i,k] <- sd.rm[time[i]]
nu[i,k] <- mu[trial[i]] + delta[trial[i],k]
}
}
for (j in 1:ns){
mu[j] ~ dnorm(0,0.001)
delta[j,1] <- 0
w[j,1] <- 0
for (k in 2:na[j]){
delta[j,k] ~ dnorm(md[j,k],tau[j,k])
md[j,k] <- d[t.s[j,k]] - d[t.s[j,1]] + sw[j,k] + beta*x[j]
tau[j,k] <- 2*tau.re*(k-1)/k
w[j,k] <- delta[j,k] - (d[t.s[j,k]] - d[t.s[j,1]] + beta*x[j])
sw[j,k] <- sum(w[j,1:(k-1)])/(k-1)
}
}
d[1] <- 0
for (k in 2:nt){
d[k] ~ dnorm(0,0.001)
}
beta ~ dnorm(0,0.001)

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
15 | 42
for(m in 1:7){
sd.rm[m] <- pow(prec.RM[m], -0.5)
prec.RM[m] <- prec.RM.which[m,indep[m]]
prec.RM.which[m,1] <- prec.RM.common
prec.RM.which[m,2] <- pow(sd.RM.indep[m],-2)
sd.RM.indep[m] ~ dunif(0,50)
}
prec.RM.common <- pow(sd.RM.common, -2)
sd.RM.common ~ dunif(0,50)
tau.re ~ dgamma(0.001,0.001)I(,2000)
sd.re <- pow(tau.re,-0.5)
}
Alternative model 2: Unconstrained baseline, random-walk on treatment effect
Following Dakin et al it may be desirable to relax assumptions further by using unconstrained baselines.4
At the same time, a random walk on the treatment effect may offer a sensible way to capture potential
temporal patterns. This model may thus be described as follows:
𝑠𝑒𝑓𝑓𝑖𝑡𝑘| 𝜇𝑖𝑡 , 𝛿𝑖𝑡𝑘 , 𝑠𝑒𝑖𝑡𝑘~ 𝒩(𝜇𝑖𝑡 + 𝛿𝑖𝑡𝑘 , 𝑠𝑒𝑖𝑡𝑘2 )
𝑓𝑜𝑟 𝑡 > 1
𝛿𝑖𝑡𝑘|𝛿𝑖(𝑡−1)𝑘, 𝜏𝑡𝑖𝑚𝑒 {= 0 𝑖𝑓 𝑡𝑟𝑡(𝑖, 𝑘) = 𝑏𝑠𝑙(𝑖)
~𝒩(𝛿𝑖(𝑡−1)𝑘, 𝜏𝑡𝑖𝑚𝑒2 ) 𝑒𝑙𝑠𝑒
𝛿𝑖1𝑘|𝑑𝑡𝑟𝑡(𝑖,𝑘), 𝑑𝑏𝑠𝑙(𝑖), 𝜏𝑅𝐸~~𝒩(𝑑𝑡𝑟𝑡(𝑖,𝑘) − 𝑑𝑏𝑠𝑙(𝑖) + 𝛽 ∗ x𝑖, 𝜏𝑅𝐸2 )
Furthermore, the following prior distributions were used:
𝜇𝑖𝑡~𝑁(0,1000)
𝑑𝑔~𝑁(0,1000)
𝛽~𝑁(0,1000)
𝜏𝑡𝑖𝑚𝑒~ 𝒰(0,50)
𝜏𝑅𝐸−2 ~ 𝒢(0.001,0.001)Ι(0,2000)
We note a few points with respect to this model:
𝜏𝑡𝑖𝑚𝑒2 is the variance determining how close two adjacent 𝛿𝑖𝑡𝑘 are to each other
𝜇𝑖𝑡 is the baseline effect at time 𝑡 in study 𝑖

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
16 | 42
𝛿𝑖𝑡𝑘 is the treatment effect at time 𝑡 in study 𝑖
𝑑𝑔 is the overall (treatment) effect at timepoint 1
An adjustment for multi-arm trials based on the approach proposed by Cooper et al1
was done (for simplification, this is omitted in the model formulation above)

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
17 | 42
WinBUGS code used for unconstrained baseline, random walk on treatment effect model:
model {
for(i in 1:nobs){
prec.t[i,1] <- pow(set[i,1],-2)
sefft[i,1] ~ dnorm(mean.t[i,1],prec.t[i,1])
mean.t[i,1] <- mu[trial[i],1] + delta[trial[i],arm[i],1]
rest[i,1] <- (mean.t[i,1] - sefft[i,1])
for(k in 2:n.times){
prec.t[i,k] <- pow(set[i,k],-2)
sefft[i,k] ~ dnorm(mean.t[i,k],prec.t[i,k])
mean.t[i,k] <- mu[trial[i],k] + delta[trial[i],arm[i],k]
rest[i,k] <- (mean.t[i,k] - sefft[i,k])
}
}
for (j in 1:ns){
for(m in 1:n.times){
mu[j,m] ~ dnorm(0,0.0001)
delta[j,1,m] <- 0
}
w[j,1] <- 0
for (k in 2:na[j]){
delta[j,k,1] ~ dnorm(md[j,k],tau[j,k])
md[j,k] <- d[t.s[j,k]] - d[t.s[j,1]] + sw[j,k] + beta*x[j]
tau[j,k] <- 2*tau.re*(k-1)/k
w[j,k] <- delta[j,k,1] - (d[t.s[j,k]] - d[t.s[j,1]] + beta*x[j])
sw[j,k] <- sum(w[j,1:(k-1)])/(k-1)
for(g in 2:n.times){
delta[j,k,g] ~ dnorm(delta[j,k,g-1],prec.RW[g])
}
}
}
d[1] <- 0
for (k in 2:nt){
d[k] ~ dnorm(0,0.001)
}
beta ~ dnorm(0,0.001)
prec.RW[1] <- 0
indep[1] <- 0
for(i in 2:n.times){

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
18 | 42
sd.RW[i] <- pow(prec.RW[i], -0.5)
prec.RW[i] <- prec.RW.which[i,indep[i]]
prec.RW.which[i,1] <- prec.RW.common
prec.RW.which[i,2] <- pow(sd.RW.indep[i], -2)
sd.RW.indep[i] ~ dunif(0, 50)
}
prec.RW.common <- pow(sd.RW.common, -2)
sd.RW.common ~ dunif(0,50)
tau.re ~ dgamma(0.001,0.001)I(,2000)
sd.re <- pow(tau.re,-0.5)
}
References
1. Cooper NJ, Sutton AJ, Lu G, Khunti K. Mixed comparison of stroke prevention treatments in individuals with nonrheumatic atrial fibrillation. Archives of internal medicine. 2006;166(12):1269-1275.
2. Rhodes KM, Turner RM, Higgins JP. Predictive distributions were developed for the extent of heterogeneity in meta-analyses of continuous outcome data. J Clin Epidemiol. 2015;68(1):52-60.
3. Wandel S, Juni P, Tendal B, et al. Effects of glucosamine, chondroitin, or placebo in patients with osteoarthritis of hip or knee: network meta-analysis. BMJ. 2010;341:c4675.
4. Dakin HA, Welton NJ, Ades AE, Collins S, Orme M, Kelly S. Mixed treatment comparison of repeated measurements of a continuous endpoint: an example using topical treatments for primary open-angle glaucoma and ocular hypertension. Stat Med. 2011.

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
19 | 42
Web-appendix 3. Definitions used to classify trials according to
components of methodological quality
Concealment of allocation
We considered allocation concealment adequate if the investigators responsible for
patient selection were unable to suspect before allocation which treatment was next.
Methods considered adequate included central randomization, coded drugs, and
sequentially numbered, sealed, opaque envelopes. Concealment was downgraded to
inadequate, if there was evidence of inadequate sequence generation.
Blinding of patients
We considered blinding of patients adequate if a trial was placebo-controlled, if
interventions were described as indistinguishable, or if double-dummy technique was
used.
Blinding of therapist
We considered blinding of therapists adequate if it was explicitly mentioned in the text
that therapists were blinded.
Completeness of outcome data
We considered statistical analyses to be adequate if all randomised patients were
included in the analysis according to the intention-to-treat principle.

Web-appendix 4. Flow diagram and references of included trials
Web-appendix Figure 1. Flow diagram of systematic review
43 potentially eligible reports retrieved for
more detailed assessment
2863 potentially relevant references
identified from Jan 2009 to Feb 2015
CENTRAL = 511
MEDLINE = 668
EMBASE = 1684
24 reports excluded based on full-text
screening
• No knee or hip OA = 1
• No RCT = 1
• Editorial, comment, review = 0
• Less then 100 Patients per trial arm = 2
• No NSAID = 2
• No Control of interest = 2
• No NSAID included in our Review = 0
• Topical NSAID = 0
• No outcome measure of interest = 7
• Post-operative pain = 1
• Multiple report from included trial = 8
2821 reports excluded from further review
• No knee or hip OA = 650
• No RCT = 358
• Editorial, comment, review = 159
• Less then 100 Patients per trial arm = 21
• No NSAID = 591
• No Control of interest = 84
• No NSAID included in our Review = 7
• Topical NSAID = 66
• Post-operative pain = 69
• Duplicates = 815
19 Trials included
598 potentially eligible reports retrieved for
more detailed assessment
5389 potentially relevant references
identified from inception to December 2010
CENTRAL = 5389
548 reports excluded based on full-text
screening
• No knee or hip OA = 22
• No RCT = 26
• Editorial, comment, review = 47
• Less than 100 patients per trial arm = 203
• No NSAID = 0
• No Control of interest = 1
• No NSAID included in our Review = 0
• Topical NSAID = 0
• No outcome measure of interest = 26
• Post-operative pain = 0
• Multiple report from included trial = 6
• Insufficient data = 5
• Non-English = 171
• Abstract = 40
• Other = 1
4791 reports excluded from further review
• No knee or hip OA = 1274
• No RCT = 275
• Editorial, comment, review = 29
• Less than 100 patients per trial arm = 2175
• No NSAID = 414
• No Control of interest = 109
• No NSAID included in our Review = 11
• Topical NSAID = 7
• Published before 1980 = 328
• Post-operative pain = 101
• Non-English = 56
• Abstract = 12
50 trials included
74 trials included in main analysis
721 potentially relevant trials identified in
internal database
(1275 comparisons)
281 potentially eligible trials retrieved for
more detailed assessment
(542 comparisons)
440 trials excluded from further review
(733 comparisons)
234 trials excluded (418 comparisons)
• No knee or hip OA = 105
• No RCT = 0
• Editorial, comment, review = 0
• No NSAID = 39
• No Control of interest = 0
• No NSAID included in our Review = 39
• Topical NSAID = 13
• No outcome measure of interest = 128
• Post-operative pain = 0
• Less than 100 patients per trial arm = 63
• Multiple report from included trial = 0
• Insufficient data = 24
• Non-English = 0
• Abstract = 24
• Other = 747 eligible trials retrieved for more
detailed assessment
(124 comparisons)
5 unpublished trials included
(5 comparisons)
42 trials excluded (119 comparisons)
• Duplicates = 119

References to included trials
Altman et al (2007)1, Baerwald et al (2010)2, Bensen et al (1999)3, Bin et al (2007)4, Bingham et al (2007)5, Bingham et al (2007a)5, Birbara et al (2006)6, Birbara et al (2006a)6, Bocanegra et al (1998)7, Boureau et al (2004)8, Cannon et al (2000)9, Caruso et al (1987)10, Conaghan et al (2013)11, Dahlberg et al (2009)12, Day et al (2000)13, DeLemos et al (2011)14, Doherty et al (2011)15, Ehrich et al (2001)16, Emery et al (2008)17, Essex et al (2012)18, Essex et al (2012a)19, Essex et al (2014)20, Fleischmann et al (2006)21, GAIT (2006)22-24, Gibofsky et al (2003)25, Gibofsky et al (2014)26, Gottesdiener et al (2002)27, Hawkey et al (2000)28, Herrero-Beaumont et al (2007)29, Hochberg et al (2011)30, Hochberg et al (2011a)30, Karlsson et al (2009)31, Kivitz et al (2001)32, Kivitz et al (2002)33, Kivitz et al (2004)34, Lehmann et al (2005)35, Leung et al (2002)36, Lohmander et al (2005)37, Makarowski et al (2002)38, McKenna et al (2001)39, Miceli-Richard et al (2004)40, Novartis (2005)41, Novartis (2005a)42, Novartis (2006)43, Novartis (2006a)44, Novartis (2007)45, PACES (2004)46, PACESa (2004)46, Prior et al (2014)47, Puopolo et al (2007)48, Reginster et al (2007)49, Rother et al (2007)50, Saag et al (2000)51, Saag et al (2000a)51, Schnitzer et al (2004)52, Schnitzer et al (2005)53, Schnitzer et al (2005a)54, Schnitzer et al (2009)55, Schnitzer et al (2010)56, Schnitzer et al (2011)57, Schnitzer et al (2011a)58, Sheldon et al (2005)59, Smugar et al (2006)60, Smugar et al (2006a)60, Sowers et al (2005)61, Tannenbaum et al (2004)62, Weaver et al (2006)63, Wiesenhutter et al (2005)64, Williams et al (2000)65, Williams et al (2001)66, Wittenberg et al (2006)67, Yoo et al (2014)68, Zacher et al (2003)69, Zhao et al (1999)70.
1. Altman RD, Zinsenheim JR, Temple AR, Schweinle JE. Three-month efficacy and safety of acetaminophen extended-release for osteoarthritis pain of the hip or knee: a randomized, double-blind, placebo-controlled study. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society, 2007. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/291/CN-00586291/frame.html Journal Article; Randomized Controlled Trial . 2. Baerwald C, Verdecchia P, Duquesroix B, Frayssinet H, Ferreira T. Efficacy, safety, and effects on blood pressure of naproxcinod 750 mg twice daily compared with placebo and naproxen 500 mg twice daily in patients with osteoarthritis of the hip: a randomized, double-blind, parallel-group, multicenter study. Arthritis and rheumatism, 2010. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/856/CN-00777856/frame.html . 3. Bensen WG, Fiechtner JJ, McMillen JI, et al. Treatment of osteoarthritis with celecoxib, a cyclooxygenase-2 inhibitor: a randomized controlled trial. Mayo Clinic proceedings Mayo Clinic, 1999. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/056/CN-00264056/frame.html . 4. Bin SI, Wu SS, Zeng X, Moore A, Frank N. Efficacy of lumiracoxib in relieving pain associated with knee osteoarthritis: A 6-week, randomized, double-blind, parallel-group study. APLAR Journal of Rheumatology, 2007. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/938/CN-00641938/frame.html . 5. Bingham CO, Sebba AI, Rubin BR, et al. Efficacy and safety of etoricoxib 30 mg and celecoxib 200 mg in the treatment of osteoarthritis in two identically designed, randomized, placebo-controlled, non-inferiority studies. Rheumatology (Oxford, England), 2007. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/419/CN-00576419/frame.html . 6. Birbara C, Ruoff G, Sheldon E, et al. Efficacy and safety of rofecoxib 12.5 mg and celecoxib 200 mg in two similarly designed osteoarthritis studies. Current medical research and opinion, 2006. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/019/CN-00554019/frame.html . 7. Bocanegra TS, Weaver AL, Tindall EA, et al. Diclofenac/misoprostol compared with diclofenac in the treatment of osteoarthritis of the knee or hip: a randomized, placebo controlled trial. Arthrotec Osteoarthritis Study Group. J Rheumatol 1998; 25(8): 1602-11. 8. Boureau F, Schneid H, Zeghari N, Wall R, Bourgeois P. The IPSO study: ibuprofen, paracetamol study in osteoarthritis. A randomised comparative clinical study comparing the efficacy and safety of ibuprofen and paracetamol analgesic treatment of osteoarthritis of the knee or hip. Annals of the Rheumatic Diseases, 2004. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/958/CN-00480958/frame.html . 9. Cannon GW, Caldwell JR, Holt P, et al. Rofecoxib, a specific inhibitor of cyclooxygenase 2, with clinical efficacy comparable with that of diclofenac sodium: Results of a one-year, randomized, clinical trial in patients with osteoarthritis of the knee and hip. Arthritis & Rheumatism, 2000. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/080/CN-00424080/frame.html .

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
22 | 42
10. Caruso I, Pietrogrande V. Italian double-blind multicenter study comparing S-adenosylmethionine, naproxen, and placebo in the treatment of degenerative joint disease. The American journal of medicine, 1987. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/222/CN-00051222/frame.html . 11. Conaghan PG, Dickson J, Bolten W, Cevc G, Rother M. A multicentre, randomized, placebo- and active-controlled trial comparing the efficacy and safety of topical ketoprofen in Transfersome gel (IDEA-033) with ketoprofen-free vehicle (TDT 064) and oral celecoxib for knee pain associated with osteoarthritis. Rheumatology (Oxford, England), 2013. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/886/CN-00876886/frame.html . 12. Dahlberg LE, Holme I, Høye K, Ringertz B. A randomized, multicentre, double-blind, parallel-group study to assess the adverse event-related discontinuation rate with celecoxib and diclofenac in elderly patients with osteoarthritis. Scandinavian Journal of Rheumatology, 2009. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/518/CN-00682518/frame.html . 13. Day R, Morrison B, Luza A, et al. A randomized trial of the efficacy and tolerability of the COX-2 inhibitor rofecoxib vs ibuprofen in patients with osteoarthritis. Archives of Internal Medicine, 2000. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/169/CN-00424169/frame.html . 14. DeLemos BP, Xiang J, Benson C, et al. Tramadol hydrochloride extended-release once-daily in the treatment of osteoarthritis of the knee and/or hip: a double-blind, randomized, dose-ranging trial. Am J Ther 2011; 18(3): 216-26. 15. Doherty M, Hawkey C, Goulder M, et al. A randomised controlled trial of ibuprofen, paracetamol or a combination tablet of ibuprofen/paracetamol in community-derived people with knee pain. Annals of the rheumatic diseases, 2011. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/579/CN-00798579/frame.html . 16. Ehrich EW, Bolognese JA, Watson DJ, Kong SX. Effect of rofecoxib therapy on measures of health-related quality of life in patients with osteoarthritis. The American journal of managed care, 2001. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/256/CN-00349256/frame.html . 17. Emery P, Koncz T, Pan S, Lowry S. Analgesic effectiveness of celecoxib and diclofenac in patients with osteoarthritis of the hip requiring joint replacement surgery: a 12-week, multicenter, randomized, double-blind, parallel-group, double-dummy, noninferiority study. Clinical Therapeutics, 2008. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/458/CN-00707458/frame.html . 18. Essex MN, Bhadra P, Sands GH. Efficacy and tolerability of celecoxib versus naproxen in patients with osteoarthritis of the knee: a randomized, double-blind, double-dummy trial. Journal of international medical research, 2012. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/943/CN-00878943/frame.html . 19. Essex MN, O'Connell M, Bhadra Brown P. Response to nonsteroidal anti-inflammatory drugs in African Americans with osteoarthritis of the knee. Journal of International Medical Research 2012; 40(6): 2251-66. 20. Essex MN, Behar R, O'Connell MA, Brown PB. Efficacy and tolerability of celecoxib and naproxen versus placebo in Hispanic patients with knee osteoarthritis. International journal of general medicine, 2014. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/846/CN-00992846/frame.html . 21. Fleischmann R, Sheldon E, Maldonado-Cocco J, Dutta D, Yu S, Sloan VS. Lumiracoxib is effective in the treatment of osteoarthritis of the knee: a prospective randomized 13-week study versus placebo and celecoxib. Clinical Rheumatology, 2006. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/046/CN-00552046/frame.html . 22. Clegg DO, Reda DJ, Harris CL, et al. Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis. N Engl J Med 2006; 354(8): 795-808. 23. Sawitzke AD, Shi H, Finco MF, et al. The effect of glucosamine and/or chondroitin sulfate on the progression of knee osteoarthritis: a report from the glucosamine/chondroitin arthritis intervention trial. Arthritis Rheum 2008; 58(10): 3183-91. 24. Sawitzke AD, Shi H, Finco MF, et al. Clinical efficacy and safety of glucosamine, chondroitin sulphate, their combination, celecoxib or placebo taken to treat osteoarthritis of the knee: 2-year results from GAIT. Ann Rheum Dis 2010; 69(8): 1459-64. 25. Gibofsky A, Williams GW, McKenna F, Fort JG. Comparing the efficacy of cyclooxygenase 2-specific inhibitors in treating osteoarthritis: appropriate trial design considerations and results of a

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
23 | 42
randomized, placebo-controlled trial. Arthritis and rheumatism, 2003. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/844/CN-00458844/frame.html . 26. Gibofsky A, Hochberg MC, Jaros MJ, Young CL. Efficacy and safety of low-dose submicron diclofenac for the treatment of osteoarthritis pain: A 12 week, phase 3 study. Current medical research and opinion, 2014. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/072/CN-01002072/frame.html . 27. Gottesdiener K, Schnitzer T, Fisher C, et al. Results of a randomized, dose-ranging trial of etoricoxib in patients with osteoarthritis. Rheumatology (Oxford, England) 2002; 41(9): 1052-61. 28. Hawkey C, Laine L, Simon T, et al. Comparison of the effect of rofecoxib (a cyclooxygenase 2 inhibitor), ibuprofen, and placebo on the gastroduodenal mucosa of patients with osteoarthritis: A randomized, double-blind, placebo-controlled trial. Arthritis & Rheumatism, 2000. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/108/CN-00424108/frame.html . 29. Herrero-Beaumont G, Ivorra JA, Del Carmen Trabado M, et al. Glucosamine sulfate in the treatment of knee osteoarthritis symptoms: a randomized, double-blind, placebo-controlled study using acetaminophen as a side comparator. Arthritis Rheum 2007; 56(2): 555-67. 30. Hochberg MC, Fort JG, Svensson O, Hwang C, Sostek M. Fixed-dose combination of enteric-coated naproxen and immediate-release esomeprazole has comparable efficacy to celecoxib for knee osteoarthritis: two randomized trials. Current medical research and opinion, 2011. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/394/CN-00800394/frame.html . 31. Karlsson J, Pivodic A, Aguirre D, Schnitzer TJ. Efficacy, safety, and tolerability of the cyclooxygenase-inhibiting nitric oxide donator naproxcinod in treating osteoarthritis of the hip or knee; 2009. 32. Kivitz AJ, Moskowitz RW, Woods E, et al. Comparative efficacy and safety of celecoxib and naproxen in the treatment of osteoarthritis of the hip. The Journal of international medical research, 2001. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/263/CN-00377263/frame.html . 33. Kivitz A, Eisen G, Zhao WW, Bevirt T, Recker DP. Randomized placebo-controlled trial comparing efficacy and safety of valdecoxib with naproxen in patients with osteoarthritis. The Journal of family practice, 2002. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/059/CN-00390059/frame.html . 34. Kivitz AJ, Greenwald MW, Cohen SB, et al. Efficacy and safety of rofecoxib 12.5 mg versus nabumetone 1,000 mg in patients with osteoarthritis of the knee: a randomized controlled trial. Journal of the American Geriatrics Society, 2004. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/569/CN-00469569/frame.html . 35. Lehmann R, Brzosko M, Kopsa P, et al. Efficacy and tolerability of lumiracoxib 100 mg once daily in knee osteoarthritis: a 13-week, randomized, double-blind study vs. placebo and celecoxib. Current medical research and opinion, 2005. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/826/CN-00511826/frame.html . 36. Leung AT, Malmstrom K, Gallacher AE, et al. Efficacy and tolerability profile of etoricoxib in patients with osteoarthritis: A randomized, double-blind, placebo and active-comparator controlled 12-week efficacy trial. Current medical research and opinion, 2002. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/667/CN-00408667/frame.html . 37. Lohmander LS, McKeith D, Svensson O, et al. A randomised, placebo controlled, comparative trial of the gastrointestinal safety and efficacy of AZD3582 versus naproxen in osteoarthritis. Annals of the Rheumatic Diseases, 2005. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/674/CN-00501674/frame.html . 38. Makarowski W, Zhao WW, Bevirt T, Recker DP. Efficacy and safety of the COX-2 specific inhibitor valdecoxib in the management of osteoarthritis of the hip: a randomized, double-blind, placebo-controlled comparison with naproxen. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society, 2002. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/495/CN-00379495/frame.html . 39. McKenna F, Borenstein D, Wendt H, Wallemark C, Lefkowith JB, Geis GS. Celecoxib versus diclofenac in the management of osteoarthritis of the knee. Scandinavian Journal of Rheumatology, 2001. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/327/CN-00328327/frame.html .

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
24 | 42
40. Miceli-Richard C, Le Bars M, Schmidely N, Dougados M. Paracetamol in osteoarthritis of the knee. Annals of the Rheumatic Diseases, 2004. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/494/CN-00482494/frame.html . 41. Novartis. CCOX189A2303. https://www.novctrd.com/CtrdWeb/displaypdf.nov?trialresultid=1559 (accessed 17 Jul 2012). 42. Novartis. CCOX189A2360. https://www.novctrd.com/CtrdWeb/displaypdf.nov?trialresultid=1553 (accessed 17 Jul 2012). 43. Novartis. CCOX189A2361. https://www.novctrd.com/CtrdWeb/displaypdf.nov?trialresultid=1552 (accessed 17 Jul 2012). 44. Novartis. CCOX189A2364. https://www.novctrd.com/CtrdWeb/displaypdf.nov?trialresultid=2167 (accessed 17 Jul 2012). 45. Novartis. CCOX189A2367. https://www.novctrd.com/CtrdWeb/displaypdf.nov?trialresultid=2394 (accessed 17 Jul 2012). 46. Pincus T, Koch G, Lei H, et al. Patient Preference for Placebo, Acetaminophen (paracetamol) or Celecoxib Efficacy Studies (PACES): two randomised, double blind, placebo controlled, crossover clinical trials in patients with knee or hip osteoarthritis. Annals of the Rheumatic Diseases, 2004. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/496/CN-00482496/frame.html . 47. Prior MJ, Harrison DD, Frustaci ME. A randomized, double-blind, placebo-controlled 12 week trial of acetaminophen extended release for the treatment of signs and symptoms of osteoarthritis. Current medical research and opinion 2014; 30(11): 2377-87. 48. Puopolo A, Boice JA, Fidelholtz JL, et al. A randomized placebo-controlled trial comparing the efficacy of etoricoxib 30 mg and ibuprofen 2400 mg for the treatment of patients with osteoarthritis. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society, 2007. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/319/CN-00706319/frame.html . 49. Reginster JY, Malmstrom K, Mehta A, et al. Evaluation of the efficacy and safety of etoricoxib compared with naproxen in two, 138-week randomised studies of patients with osteoarthritis. Annals of the Rheumatic Diseases, 2007. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/014/CN-00609014/frame.html . 50. Rother M, Lavins BJ, Kneer W, Lehnhardt K, Seidel EJ, Mazgareanu S. Efficacy and safety of epicutaneous ketoprofen in Transfersome (IDEA-033) versus oral celecoxib and placebo in osteoarthritis of the knee: multicentre randomised controlled trial. Annals of the Rheumatic Diseases, 2007. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/361/CN-00609361/frame.html . 51. Saag K, van der Heijde D, Fisher C, et al. Rofecoxib, a new cyclooxygenase 2 inhibitor, shows sustained efficacy, comparable with other nonsteroidal anti-inflammatory drugs: a 6-week and a 1-year trial in patients with osteoarthritis. Osteoarthritis Studies Group. Archives of family medicine, 2000. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/421/CN-00330421/frame.html . 52. Schnitzer TJ, Burmester GR, Mysler E, et al. Comparison of lumiracoxib with naproxen and ibuprofen in the Therapeutic Arthritis Research and Gastrointestinal Event Trial (TARGET), reduction in ulcer complications: randomised controlled trial. Lancet, 2004. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/441/CN-00481441/frame.html . 53. Schnitzer TJ, Kivitz AJ, Lipetz RS, Sanders N, Hee A. Comparison of the COX-inhibiting nitric oxide donator AZD3582 and rofecoxib in treating the signs and symptoms of Osteoarthritis of the knee. Arthritis and rheumatism, 2005. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/414/CN-00532414/frame.html . 54. Schnitzer TJ, Weaver AL, Polis AB, et al. Efficacy of rofecoxib, celecoxib, and acetaminophen in patients with osteoarthritis of the knee. A combined analysis of the VACT studies. The Journal of rheumatology, 2005. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/354/CN-00522354/frame.html . 55. Schnitzer TJ, Tesser JR, Cooper KM, Altman RD. A 4-week randomized study of acetaminophen extended-release vs rofecoxib in knee osteoarthritis. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society, 2009. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/398/CN-00680398/frame.html .

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
25 | 42
56. Schnitzer TJ, Kivitz A, Frayssinet H, Duquesroix B. Efficacy and safety of naproxcinod in the treatment of patients with osteoarthritis of the knee: a 13-week prospective, randomized, multicenter study. Osteoarthritis and cartilage, 2010. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/153/CN-00752153/frame.html . 57. Schnitzer TJ, Dattani ID, Seriolo B, et al. A 13-week, multicenter, randomized, double-blind study of lumiracoxib in hip osteoarthritis. Clinical rheumatology, 2011. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/831/CN-00882831/frame.html . 58. Schnitzer TJ, Hochberg MC, Marrero CE, Duquesroix B, Frayssinet H, Beekman M. Efficacy and safety of naproxcinod in patients with osteoarthritis of the knee: a 53-week prospective randomized multicenter study. Seminars in arthritis and rheumatism, 2011. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/854/CN-00780854/frame.html . 59. Sheldon E, Beaulieu A, Paster Z, Dutta D, Yu S, Sloan VS. Efficacy and tolerability of lumiracoxib in the treatment of osteoarthritis of the knee: a 13-week, randomized, double-blind comparison with celecoxib and placebo. Clinical Therapeutics, 2005. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/402/CN-00502402/frame.html . 60. Smugar SS, Schnitzer TJ, Weaver AL, Rubin BR, Polis AB, Tershakovec AM. Rofecoxib 12.5 mg, rofecoxib 25 mg, and celecoxib 200 mg in the treatment of symptomatic osteoarthritis: results of two similarly designed studies. Current medical research and opinion, 2006. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/460/CN-00566460/frame.html . 61. Sowers JR, White WB, Pitt B, et al. The Effects of cyclooxygenase-2 inhibitors and nonsteroidal anti-inflammatory therapy on 24-hour blood pressure in patients with hypertension, osteoarthritis, and type 2 diabetes mellitus. Archives of Internal Medicine, 2005. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/965/CN-00502965/frame.html . 62. Tannenbaum H, Berenbaum F, Reginster JY, et al. Lumiracoxib is effective in the treatment of osteoarthritis of the knee: a 13 week, randomised, double blind study versus placebo and celecoxib; 2004. 63. Weaver AL, Messner RP, Storms WW, et al. Treatment of patients with osteoarthritis with rofecoxib compared with nabumetone; 2006. 64. Wiesenhutter CW, Boice JA, Ko A, et al. Evaluation of the comparative efficacy of etoricoxib and ibuprofen for treatment of patients with osteoarthritis: A randomized, double-blind, placebo-controlled trial. Mayo Clinic Proceedings 2005; 80: 470-9. 65. Williams GW, Ettlinger RE, Ruderman EM, et al. Treatment of osteoarthritis with a once-daily dosing regimen of celecoxib: A randomized, controlled trial; 2000. 66. Williams GW, Hubbard RC, Yu SS, Zhao W, Geis GS. Comparison of once-daily and twice-daily administration of celecoxib for the treatment of osteoarthritis of the knee; 2001. 67. Wittenberg RH, Schell E, Krehan G, et al. First-dose analgesic effect of the cyclo-oxygenase-2 selective inhibitor lumiracoxib in osteoarthritis of the knee: a randomized, double-blind, placebo-controlled comparison with celecoxib [NCT00267215]. Arthritis research & therapy, 2006. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/546/CN-00562546/frame.html . 68. Yoo MC, Yoo WH, Kang SB, et al. Etoricoxib in the treatment of Korean patients with osteoarthritis in a double-blind, randomized controlled trial. Current medical research and opinion 2014; 30(12): 2399-408. 69. Zacher J, Feldman D, Gerli R, et al. A comparison of the therapeutic efficacy and tolerability of etoricoxib and diclofenac in patients with osteoarthritis. Current medical research and opinion, 2003. http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/699/CN-00481699/frame.html . 70. Zhao SZ, McMillen JI, Markenson JA, et al. Evaluation of the functional status aspects of health-related quality of life of patients with osteoarthritis treated with celecoxib. Pharmacotherapy 1999; 19(11): 1269-78.

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
26 | 42
Web-appendix 5. Treatment effect according to time point Web-appendix Figure 2. Graphical display of available information according to timepoint. The
size of the circle is proportional to the statistical information available for a specified preparation
at a specified timepoint across trials (precision).

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
27 | 42
Web-appendix Table 1. Treatment effect according to time point. Data displayed are effect
sizes and 95% credibility intervals

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
28 | 42
*Maximum daily dosage. We included in our analysis data at 1, 2, 4, 6, 12, 26 weeks after end of
treatment. There was not sufficient data to perform an analysis for week 52. Please note that the
estimates come from separate network meta-analyses per timepoint and do not take into account the
correlated nature of the data. The credibility intervals may therefore be too narrow. Colors correspond to
the estimated effect size per timepoint with the following color code:
Effect size -0.72 -0.37 0 0.37
Color code

Web-appendix 6. Assessment of Model Fit
Web-appendix Table 2 Assessment of model fit
Outcome Data points DIC Residuals Q-Q plots
Number (%)
within 1·96 SND
All trials
Pain 473 -917.6 469 (99.2%) Adequate
Physical function 303 -559.9 303 (100%) Adequate
DIC: Deviance information criterion; SND: Standard normal distribution

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
30 | 42
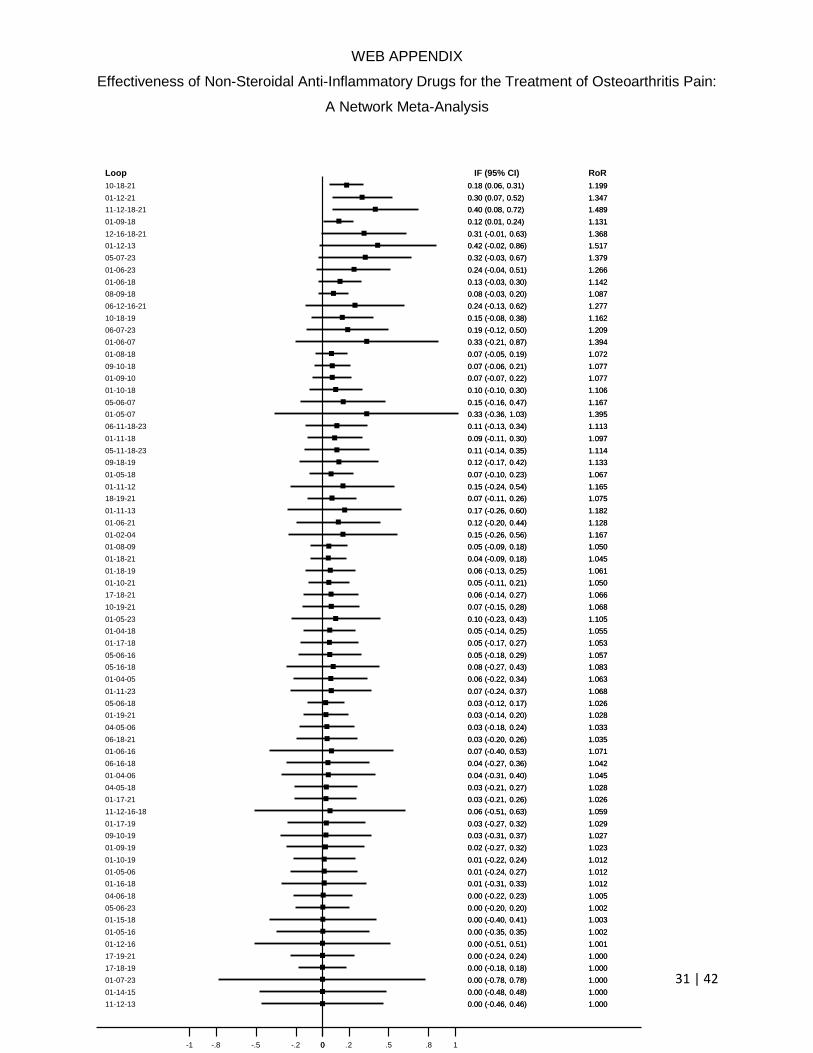
Web-appendix 7. Inconsistency Inconsistency was assessed based on the main model which used timepoint 6 as reference
timepont
Pain outcome
The median inconsistency factor (ICF) for pain was 0.06 and it ranged from 0.00 to 0.42. Four
out of 69 ICFs were statistically significant. None of the ICFs for pain were clinically relevant.
Web-appendix Figure 2. Inconsistency factors for pain outcome analysis. CI: confidence
interval. RoM: Ratio of means. 01 = Placebo; 02 =Paracetamol <2000mg; 03 = Paracetamol
3000mg; 04 = Paracetamol 3900-4000mg; 05 = Rofecoxib 12.5mg; 06 = Rofecoxib 25mg; 07
=Rofecoxib 50mg; 08 = Lumiracoxib 100mg; 09 = Lumiracoxib 200mg; 10 = Lumiracoxib
400mg; 11 = Etoricoxib 30mg; 12 = Etoricoxib 60mg; 13 = Etoricoxib 90mg; 14 = Diclofenac
70mg; 15 = Diclofenac 100mg; 16= Diclofenac 150mg; 17 = Celecoxib 100mg; 18 = Celecoxib
200mg; 19 = Celecoxib 400mg; 20 = Naproxen 750mg; 21 = Naproxen 1000mg; 22 = Ibuprofen
1200mg; 23 = Ibuprofen 2400mg
WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
31 | 42
10-18-21
01-12-21
11-12-18-21
01-09-18
12-16-18-21
01-12-13
05-07-23
01-06-23
01-06-18
08-09-18
06-12-16-21
10-18-19
06-07-23
01-06-07
01-08-18
09-10-18
01-09-10
01-10-18
05-06-07
01-05-07
06-11-18-23
01-11-18
05-11-18-23
09-18-19
01-05-18
01-11-12
18-19-21
01-11-13
01-06-21
01-02-04
01-08-09
01-18-21
01-18-19
01-10-21
17-18-21
10-19-21
01-05-23
01-04-18
01-17-18
05-06-16
05-16-18
01-04-05
01-11-23
05-06-18
01-19-21
04-05-06
06-18-21
01-06-16
06-16-18
01-04-06
04-05-18
01-17-21
11-12-16-18
01-17-19
09-10-19
01-09-19
01-10-19
01-05-06
01-16-18
04-06-18
05-06-23
01-15-18
01-05-16
01-12-16
17-19-21
17-18-19
01-07-23
01-14-15
11-12-13
Loop
0.18 (0.06, 0.31)
0.30 (0.07, 0.52)
0.40 (0.08, 0.72)
0.12 (0.01, 0.24)
0.31 (-0.01, 0.63)
0.42 (-0.02, 0.86)
0.32 (-0.03, 0.67)
0.24 (-0.04, 0.51)
0.13 (-0.03, 0.30)
0.08 (-0.03, 0.20)
0.24 (-0.13, 0.62)
0.15 (-0.08, 0.38)
0.19 (-0.12, 0.50)
0.33 (-0.21, 0.87)
0.07 (-0.05, 0.19)
0.07 (-0.06, 0.21)
0.07 (-0.07, 0.22)
0.10 (-0.10, 0.30)
0.15 (-0.16, 0.47)
0.33 (-0.36, 1.03)
0.11 (-0.13, 0.34)
0.09 (-0.11, 0.30)
0.11 (-0.14, 0.35)
0.12 (-0.17, 0.42)
0.07 (-0.10, 0.23)
0.15 (-0.24, 0.54)
0.07 (-0.11, 0.26)
0.17 (-0.26, 0.60)
0.12 (-0.20, 0.44)
0.15 (-0.26, 0.56)
0.05 (-0.09, 0.18)
0.04 (-0.09, 0.18)
0.06 (-0.13, 0.25)
0.05 (-0.11, 0.21)
0.06 (-0.14, 0.27)
0.07 (-0.15, 0.28)
0.10 (-0.23, 0.43)
0.05 (-0.14, 0.25)
0.05 (-0.17, 0.27)
0.05 (-0.18, 0.29)
0.08 (-0.27, 0.43)
0.06 (-0.22, 0.34)
0.07 (-0.24, 0.37)
0.03 (-0.12, 0.17)
0.03 (-0.14, 0.20)
0.03 (-0.18, 0.24)
0.03 (-0.20, 0.26)
0.07 (-0.40, 0.53)
0.04 (-0.27, 0.36)
0.04 (-0.31, 0.40)
0.03 (-0.21, 0.27)
0.03 (-0.21, 0.26)
0.06 (-0.51, 0.63)
0.03 (-0.27, 0.32)
0.03 (-0.31, 0.37)
0.02 (-0.27, 0.32)
0.01 (-0.22, 0.24)
0.01 (-0.24, 0.27)
0.01 (-0.31, 0.33)
0.00 (-0.22, 0.23)
0.00 (-0.20, 0.20)
0.00 (-0.40, 0.41)
0.00 (-0.35, 0.35)
0.00 (-0.51, 0.51)
0.00 (-0.24, 0.24)
0.00 (-0.18, 0.18)
0.00 (-0.78, 0.78)
0.00 (-0.48, 0.48)
0.00 (-0.46, 0.46)
IF (95% CI)
1.199
1.347
1.489
1.131
1.368
1.517
1.379
1.266
1.142
1.087
1.277
1.162
1.209
1.394
1.072
1.077
1.077
1.106
1.167
1.395
1.113
1.097
1.114
1.133
1.067
1.165
1.075
1.182
1.128
1.167
1.050
1.045
1.061
1.050
1.066
1.068
1.105
1.055
1.053
1.057
1.083
1.063
1.068
1.026
1.028
1.033
1.035
1.071
1.042
1.045
1.028
1.026
1.059
1.029
1.027
1.023
1.012
1.012
1.012
1.005
1.002
1.003
1.002
1.001
1.000
1.000
1.000
1.000
1.000
RoR
0.18 (0.06, 0.31)
0.30 (0.07, 0.52)
0.40 (0.08, 0.72)
0.12 (0.01, 0.24)
0.31 (-0.01, 0.63)
0.42 (-0.02, 0.86)
0.32 (-0.03, 0.67)
0.24 (-0.04, 0.51)
0.13 (-0.03, 0.30)
0.08 (-0.03, 0.20)
0.24 (-0.13, 0.62)
0.15 (-0.08, 0.38)
0.19 (-0.12, 0.50)
0.33 (-0.21, 0.87)
0.07 (-0.05, 0.19)
0.07 (-0.06, 0.21)
0.07 (-0.07, 0.22)
0.10 (-0.10, 0.30)
0.15 (-0.16, 0.47)
0.33 (-0.36, 1.03)
0.11 (-0.13, 0.34)
0.09 (-0.11, 0.30)
0.11 (-0.14, 0.35)
0.12 (-0.17, 0.42)
0.07 (-0.10, 0.23)
0.15 (-0.24, 0.54)
0.07 (-0.11, 0.26)
0.17 (-0.26, 0.60)
0.12 (-0.20, 0.44)
0.15 (-0.26, 0.56)
0.05 (-0.09, 0.18)
0.04 (-0.09, 0.18)
0.06 (-0.13, 0.25)
0.05 (-0.11, 0.21)
0.06 (-0.14, 0.27)
0.07 (-0.15, 0.28)
0.10 (-0.23, 0.43)
0.05 (-0.14, 0.25)
0.05 (-0.17, 0.27)
0.05 (-0.18, 0.29)
0.08 (-0.27, 0.43)
0.06 (-0.22, 0.34)
0.07 (-0.24, 0.37)
0.03 (-0.12, 0.17)
0.03 (-0.14, 0.20)
0.03 (-0.18, 0.24)
0.03 (-0.20, 0.26)
0.07 (-0.40, 0.53)
0.04 (-0.27, 0.36)
0.04 (-0.31, 0.40)
0.03 (-0.21, 0.27)
0.03 (-0.21, 0.26)
0.06 (-0.51, 0.63)
0.03 (-0.27, 0.32)
0.03 (-0.31, 0.37)
0.02 (-0.27, 0.32)
0.01 (-0.22, 0.24)
0.01 (-0.24, 0.27)
0.01 (-0.31, 0.33)
0.00 (-0.22, 0.23)
0.00 (-0.20, 0.20)
0.00 (-0.40, 0.41)
0.00 (-0.35, 0.35)
0.00 (-0.51, 0.51)
0.00 (-0.24, 0.24)
0.00 (-0.18, 0.18)
0.00 (-0.78, 0.78)
0.00 (-0.48, 0.48)
0.00 (-0.46, 0.46)
1.199
1.347
1.489
1.131
1.368
1.517
1.379
1.266
1.142
1.087
1.277
1.162
1.209
1.394
1.072
1.077
1.077
1.106
1.167
1.395
1.113
1.097
1.114
1.133
1.067
1.165
1.075
1.182
1.128
1.167
1.050
1.045
1.061
1.050
1.066
1.068
1.105
1.055
1.053
1.057
1.083
1.063
1.068
1.026
1.028
1.033
1.035
1.071
1.042
1.045
1.028
1.026
1.059
1.029
1.027
1.023
1.012
1.012
1.012
1.005
1.002
1.003
1.002
1.001
1.000
1.000
1.000
1.000
1.000
0-1 -.8 -.5 -.2 0 .2 .5 .8 1

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
32 | 42
Function outcome
The median inconsistency factor (ICF) for function was 0.07 and it ranged from 0.00 to 0.57.
Three out of 57 ICFs were statistically significant. None of ICFs for function were clinically
relevant.
Web-appendix Figure 3. Inconsistency factors for physical function outcome analysis. CI:
confidence interval. RoM: Ratio of means. 01 = Placebo; 02 =Paracetamol <2000mg; 03 =
Paracetamol 3000mg; 04 = Paracetamol 3900-4000mg; 05 = Rofecoxib 12.5mg; 06 = Rofecoxib
25mg; 07 =Rofecoxib 50mg; 08 = Lumiracoxib 100mg; 09 = Lumiracoxib 200mg; 10 =
Lumiracoxib 400mg; 11 = Etoricoxib 30mg; 12 = Etoricoxib 60mg; 13 = Diclofenac 70mg; 14 =
Diclofenac 100mg; 15= Diclofenac 150mg; 16 = Celecoxib 100mg; 17 = Celecoxib 200mg; 18 =
Celecoxib 400mg; 19 = Naproxen 750mg; 20 = Naproxen 1000mg; 21 = Ibuprofen 1200mg; 22
= Ibuprofen 2400mg

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
33 | 42
01-06-07
01-07-22
12-15-17-20
01-06-17
01-16-20
06-12-15-20
10-18-20
01-18-20
01-06-22
01-12-15
01-09-10
01-12-20
01-08-17
01-02-04
10-17-18
01-06-20
04-05-06
01-11-17
06-17-20
05-06-15
01-17-20
09-10-17
01-14-17
10-17-20
01-08-09
01-11-22
01-15-17
17-18-20
01-10-17
01-10-18
04-06-17
01-05-15
01-04-17
06-07-22
16-17-20
06-15-17
01-05-22
05-11-17-22
01-09-17
01-10-20
05-06-17
06-11-17-22
01-05-06
08-09-17
01-16-17
04-05-17
01-06-15
01-16-18
01-05-17
05-06-22
16-17-18
01-04-06
01-17-18
05-15-17
16-18-20
01-04-05
01-13-14
Loop
0.57 (0.19, 0.94)
0.38 (0.07, 0.69)
0.31 (0.01, 0.60)
0.14 (-0.00, 0.29)
0.15 (-0.01, 0.31)
0.28 (-0.02, 0.57)
0.25 (-0.02, 0.53)
0.14 (-0.02, 0.30)
0.23 (-0.04, 0.49)
0.21 (-0.08, 0.49)
0.18 (-0.08, 0.43)
0.16 (-0.08, 0.40)
0.07 (-0.04, 0.18)
0.19 (-0.14, 0.52)
0.16 (-0.13, 0.45)
0.16 (-0.14, 0.46)
0.11 (-0.10, 0.32)
0.10 (-0.10, 0.29)
0.10 (-0.10, 0.30)
0.13 (-0.13, 0.40)
0.05 (-0.07, 0.18)
0.07 (-0.09, 0.22)
0.17 (-0.22, 0.56)
0.06 (-0.08, 0.19)
0.09 (-0.12, 0.29)
0.12 (-0.19, 0.43)
0.12 (-0.19, 0.42)
0.07 (-0.12, 0.25)
0.07 (-0.12, 0.26)
0.10 (-0.19, 0.39)
0.06 (-0.12, 0.24)
0.13 (-0.27, 0.52)
0.05 (-0.11, 0.22)
0.10 (-0.21, 0.41)
0.05 (-0.12, 0.22)
0.07 (-0.18, 0.32)
0.11 (-0.27, 0.48)
0.07 (-0.18, 0.32)
0.03 (-0.09, 0.15)
0.06 (-0.17, 0.28)
0.04 (-0.13, 0.20)
0.04 (-0.19, 0.28)
0.05 (-0.25, 0.36)
0.02 (-0.10, 0.13)
0.02 (-0.14, 0.19)
0.03 (-0.19, 0.25)
0.06 (-0.40, 0.52)
0.03 (-0.23, 0.30)
0.02 (-0.15, 0.19)
0.02 (-0.21, 0.26)
0.01 (-0.16, 0.19)
0.02 (-0.32, 0.36)
0.01 (-0.16, 0.18)
0.01 (-0.26, 0.28)
0.00 (-0.17, 0.18)
0.00 (-0.30, 0.30)
0.00 (-0.48, 0.48)
IF (95% CI)
1.760
1.466
1.361
1.153
1.163
1.319
1.286
1.153
1.253
1.230
1.195
1.170
1.074
1.211
1.177
1.176
1.119
1.104
1.107
1.144
1.056
1.071
1.186
1.058
1.089
1.127
1.123
1.069
1.070
1.101
1.060
1.136
1.055
1.104
1.053
1.074
1.114
1.074
1.031
1.060
1.038
1.045
1.056
1.019
1.025
1.030
1.061
1.035
1.019
1.022
1.012
1.019
1.007
1.009
1.003
1.001
1.000
RoR
0.57 (0.19, 0.94)
0.38 (0.07, 0.69)
0.31 (0.01, 0.60)
0.14 (-0.00, 0.29)
0.15 (-0.01, 0.31)
0.28 (-0.02, 0.57)
0.25 (-0.02, 0.53)
0.14 (-0.02, 0.30)
0.23 (-0.04, 0.49)
0.21 (-0.08, 0.49)
0.18 (-0.08, 0.43)
0.16 (-0.08, 0.40)
0.07 (-0.04, 0.18)
0.19 (-0.14, 0.52)
0.16 (-0.13, 0.45)
0.16 (-0.14, 0.46)
0.11 (-0.10, 0.32)
0.10 (-0.10, 0.29)
0.10 (-0.10, 0.30)
0.13 (-0.13, 0.40)
0.05 (-0.07, 0.18)
0.07 (-0.09, 0.22)
0.17 (-0.22, 0.56)
0.06 (-0.08, 0.19)
0.09 (-0.12, 0.29)
0.12 (-0.19, 0.43)
0.12 (-0.19, 0.42)
0.07 (-0.12, 0.25)
0.07 (-0.12, 0.26)
0.10 (-0.19, 0.39)
0.06 (-0.12, 0.24)
0.13 (-0.27, 0.52)
0.05 (-0.11, 0.22)
0.10 (-0.21, 0.41)
0.05 (-0.12, 0.22)
0.07 (-0.18, 0.32)
0.11 (-0.27, 0.48)
0.07 (-0.18, 0.32)
0.03 (-0.09, 0.15)
0.06 (-0.17, 0.28)
0.04 (-0.13, 0.20)
0.04 (-0.19, 0.28)
0.05 (-0.25, 0.36)
0.02 (-0.10, 0.13)
0.02 (-0.14, 0.19)
0.03 (-0.19, 0.25)
0.06 (-0.40, 0.52)
0.03 (-0.23, 0.30)
0.02 (-0.15, 0.19)
0.02 (-0.21, 0.26)
0.01 (-0.16, 0.19)
0.02 (-0.32, 0.36)
0.01 (-0.16, 0.18)
0.01 (-0.26, 0.28)
0.00 (-0.17, 0.18)
0.00 (-0.30, 0.30)
0.00 (-0.48, 0.48)
1.760
1.466
1.361
1.153
1.163
1.319
1.286
1.153
1.253
1.230
1.195
1.170
1.074
1.211
1.177
1.176
1.119
1.104
1.107
1.144
1.056
1.071
1.186
1.058
1.089
1.127
1.123
1.069
1.070
1.101
1.060
1.136
1.055
1.104
1.053
1.074
1.114
1.074
1.031
1.060
1.038
1.045
1.056
1.019
1.025
1.030
1.061
1.035
1.019
1.022
1.012
1.019
1.007
1.009
1.003
1.001
1.000
0-1 -.8 -.5 -.2 0 .2 .5 .8 1

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
34 | 42
Web-appendix 8. Analyses using alternative models for network meta-
analysis
Web-appendix Figure 4. Analysis of primary outcome pain using the alternative model with full
exchangeability, mean effect.
CrI: Credibility interval; *Maximum daily dosage. Area between dashed lines indicates treatment
effect estimates below the minimal clinically important difference.
Paracetamol <2000mg
Paracetamol 3000mg
*Paracetamol 3900-4000mg
Rofecoxib 12.5mg
*Rofecoxib 25mg
Rofecoxib 50mg
Lumiracoxib 100mg
*Lumiracoxib 200mg
Lumiracoxib 400mg
Etoricoxib 30mg
*Etoricoxib 60mg
Etoricoxib 90mg
Diclofenac 70mg
Diclofenac 100mg
*Diclofenac 150mg
Celecoxib 100mg
Celecoxib 200mg
*Celecoxib 400mg
Naproxen 750mg
*Naproxen 1000mg
Ibuprofen 1200mg
*Ibuprofen 2400mg
-0.08 (-0.31, 0.17)
-0.16 (-0.48, 0.16)
-0.18 (-0.26, -0.10)
-0.42 (-0.48, -0.35)
-0.49 (-0.55, -0.43)
-0.51 (-0.67, -0.34)
-0.33 (-0.40, -0.26)
-0.34 (-0.40, -0.28)
-0.42 (-0.51, -0.32)
-0.49 (-0.58, -0.40)
-0.53 (-0.64, -0.42)
-0.58 (-0.85, -0.32)
-0.22 (-0.51, 0.07)
-0.30 (-0.46, -0.13)
-0.55 (-0.64, -0.46)
-0.16 (-0.27, -0.06)
-0.35 (-0.39, -0.32)
-0.34 (-0.42, -0.25)
-0.04 (-0.26, 0.18)
-0.40 (-0.46, -0.35)
-0.34 (-0.70, 0.02)
-0.42 (-0.50, -0.33)
Active treatment better Placebo better
0-1.25 -1 -.75 -.5 -.25 .25 .5
Intervention Effect size (95% CI)

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
35 | 42
Web-appendix Figure 5. Analysis of primary outcome pain using the alternative random-walk
model with unconstrained baseline estimates.
CrI: Credibility interval; *Maximum daily dosage. Area between dashed lines indicates treatment
effect estimates below the minimal clinically important difference.
Intervention Effect size (95% CI)
Paracetamol <2000mg
Paracetamol 3000mg
*Paracetamol 3900-4000mg
Rofecoxib 12.5mg
*Rofecoxib 25mg
Rofecoxib 50mg
Lumiracoxib 100mg
*Lumiracoxib 200mg
Lumiracoxib 400mg
Etoricoxib 30mg
*Etoricoxib 60mg
Etoricoxib 90mg
Diclofenac 70mg
Diclofenac 100mg
*Diclofenac 150mg
Celecoxib 100mg
Celecoxib 200mg
*Celecoxib 400mg
Naproxen 750mg
*Naproxen 1000mg
Ibuprofen 1200mg
*Ibuprofen 2400mg
-0.08 (-0.33, 0.20)
-0.19 (-0.48, 0.11)
-0.18 (-0.26, -0.09)
-0.41 (-0.48, -0.35)
-0.49 (-0.55, -0.43)
-0.48 (-0.65, -0.31)
-0.33 (-0.40, -0.25)
-0.34 (-0.41, -0.28)
-0.42 (-0.51, -0.33)
-0.48 (-0.57, -0.39)
-0.53 (-0.64, -0.42)
-0.56 (-0.85, -0.30)
-0.14 (-0.45, 0.14)
-0.27 (-0.44, -0.06)
-0.55 (-0.64, -0.46)
-0.17 (-0.27, -0.07)
-0.35 (-0.39, -0.31)
-0.34 (-0.43, -0.25)
-0.05 (-0.27, 0.18)
-0.40 (-0.46, -0.35)
-0.37 (-0.71, -0.02)
-0.41 (-0.50, -0.32)
Active treatment better Placebo better
0-1.25 -1 -.75 -.5 -.25 .25 .5

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
36 | 42
Web-appendix 9. Results of adjusted models
Web-appendix Figure 6. Analysis of primary outcome pain adjusted for concealment of
allocation.
CrI: Credibility interval; *Maximum daily dosage.
Paracetamol <2000mg
Paracetamol 3000mg
*Paracetamol 3900-4000mg
Rofecoxib 12.5mg
*Rofecoxib 25mg
Rofecoxib 50mg
Lumiracoxib 100mg
*Lumiracoxib 200mg
Lumiracoxib 400mg
Etoricoxib 30mg
*Etoricoxib 60mg
Etoricoxib 90mg
Diclofenac 70mg
Diclofenac 100mg
*Diclofenac 150mg
Celecoxib 100mg
Celecoxib 200mg
*Celecoxib 400mg
Naproxen 750mg
*Naproxen 1000mg
Ibuprofen 1200mg
*Ibuprofen 2400mg
-0.10 (-0.45, 0.24)
-0.17 (-0.66, 0.33)
-0.18 (-0.29, -0.07)
-0.46 (-0.55, -0.36)
-0.54 (-0.63, -0.44)
-0.64 (-0.88, -0.41)
-0.37 (-0.48, -0.25)
-0.36 (-0.46, -0.26)
-0.45 (-0.61, -0.30)
-0.51 (-0.64, -0.39)
-0.60 (-0.76, -0.45)
-0.63 (-0.92, -0.34)
-0.26 (-0.65, 0.13)
-0.37 (-0.62, -0.12)
-0.61 (-0.75, -0.47)
-0.19 (-0.34, -0.05)
-0.39 (-0.47, -0.32)
-0.36 (-0.50, -0.23)
-0.08 (-0.46, 0.29)
-0.43 (-0.53, -0.33)
-0.32 (-0.87, 0.23)
-0.45 (-0.58, -0.32)
Active treatment better Placebo better
0-1.25 -1 -.75 -.5 -.25 .25 .5
Intervention Effect size (95% CI)

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
37 | 42
Web-appendix Figure 7. Analysis of primary outcome pain adjusted for blinding of therapist.
CrI: Credibility interval; *Maximum daily dosage.
Paracetamol <2000mg
Paracetamol 3000mg
*Paracetamol 3900-4000mg
Rofecoxib 12.5mg
*Rofecoxib 25mg
Rofecoxib 50mg
Lumiracoxib 100mg
*Lumiracoxib 200mg
Lumiracoxib 400mg
Etoricoxib 30mg
*Etoricoxib 60mg
Etoricoxib 90mg
Diclofenac 70mg
Diclofenac 100mg
*Diclofenac 150mg
Celecoxib 100mg
Celecoxib 200mg
*Celecoxib 400mg
Naproxen 750mg
*Naproxen 1000mg
Ibuprofen 1200mg
*Ibuprofen 2400mg
-0.07 (-0.42, 0.27)
-0.17 (-0.66, 0.33)
-0.16 (-0.28, -0.05)
-0.43 (-0.50, -0.35)
-0.51 (-0.58, -0.43)
-0.61 (-0.84, -0.39)
-0.34 (-0.44, -0.23)
-0.34 (-0.43, -0.25)
-0.43 (-0.58, -0.28)
-0.49 (-0.61, -0.37)
-0.58 (-0.73, -0.43)
-0.62 (-0.91, -0.33)
-0.22 (-0.61, 0.17)
-0.34 (-0.58, -0.10)
-0.57 (-0.70, -0.45)
-0.16 (-0.30, -0.03)
-0.36 (-0.42, -0.31)
-0.33 (-0.46, -0.21)
-0.05 (-0.42, 0.32)
-0.40 (-0.48, -0.31)
-0.29 (-0.84, 0.25)
-0.43 (-0.54, -0.31)
Active treatment better Placebo better
-1.25 -1 -.75 -.5 -.25 0 .25 .5
Intervention Effect size (95% CI)

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
38 | 42
Web-appendix Figure 8. Analysis of primary outcome pain adjusted for completeness of
outcome data.
CrI: Credibility interval; *Maximum daily dosage.
Paracetamol <2000mg
Paracetamol 3000mg
*Paracetamol 3900-4000mg
Rofecoxib 12.5mg
*Rofecoxib 25mg
Rofecoxib 50mg
Lumiracoxib 100mg
*Lumiracoxib 200mg
Lumiracoxib 400mg
Etoricoxib 30mg
*Etoricoxib 60mg
Etoricoxib 90mg
Diclofenac 70mg
Diclofenac 100mg
*Diclofenac 150mg
Celecoxib 100mg
Celecoxib 200mg
*Celecoxib 400mg
Naproxen 750mg
*Naproxen 1000mg
Ibuprofen 1200mg
*Ibuprofen 2400mg
-0.08 (-0.42, 0.26)
-0.19 (-0.69, 0.31)
-0.17 (-0.28, -0.06)
-0.44 (-0.55, -0.33)
-0.52 (-0.63, -0.41)
-0.63 (-0.87, -0.39)
-0.35 (-0.48, -0.23)
-0.35 (-0.46, -0.24)
-0.44 (-0.60, -0.28)
-0.51 (-0.65, -0.37)
-0.59 (-0.75, -0.43)
-0.63 (-0.92, -0.33)
-0.23 (-0.62, 0.16)
-0.34 (-0.58, -0.10)
-0.59 (-0.74, -0.44)
-0.18 (-0.33, -0.03)
-0.38 (-0.47, -0.29)
-0.35 (-0.49, -0.20)
-0.06 (-0.45, 0.31)
-0.41 (-0.52, -0.30)
-0.33 (-0.90, 0.24)
-0.44 (-0.59, -0.30)
Active treatment better Placebo better
0-1.25 -1 -.75 -.5 -.25 .25 .5
Intervention Effect size (95% CI)

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
39 | 42
Web-appendix Figure 9. Analysis of primary outcome pain adjusted for approach used for data
imputation.
CrI: Credibility interval; *Maximum daily dosage.
Paracetamol <2000mg
Paracetamol 3000mg
*Paracetamol 3900-4000mg
Rofecoxib 12.5mg
*Rofecoxib 25mg
Rofecoxib 50mg
Lumiracoxib 100mg
*Lumiracoxib 200mg
Lumiracoxib 400mg
Etoricoxib 30mg
*Etoricoxib 60mg
Etoricoxib 90mg
Diclofenac 70mg
Diclofenac 100mg
*Diclofenac 150mg
Celecoxib 100mg
Celecoxib 200mg
*Celecoxib 400mg
Naproxen 750mg
*Naproxen 1000mg
Ibuprofen 1200mg
*Ibuprofen 2400mg
-0.07 (-0.41, 0.27)
-0.16 (-0.66, 0.33)
-0.16 (-0.27, -0.06)
-0.42 (-0.51, -0.33)
-0.50 (-0.59, -0.41)
-0.61 (-0.85, -0.38)
-0.34 (-0.45, -0.22)
-0.34 (-0.44, -0.24)
-0.43 (-0.58, -0.27)
-0.49 (-0.62, -0.36)
-0.58 (-0.73, -0.43)
-0.61 (-0.90, -0.32)
-0.22 (-0.60, 0.17)
-0.34 (-0.58, -0.10)
-0.57 (-0.70, -0.44)
-0.16 (-0.30, -0.02)
-0.36 (-0.43, -0.29)
-0.33 (-0.46, -0.19)
-0.05 (-0.42, 0.32)
-0.39 (-0.48, -0.30)
-0.29 (-0.85, 0.27)
-0.42 (-0.55, -0.30)
Active treatment better Placebo better
0-1.25 -1 -.75 -.5 -.25 .25 .5
Intervention Effect size (95% CI)

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
40 | 42
Web-appendix Figure 10. Analysis of primary outcome pain adjusted for joint affected by
osteoathritis.
CrI: Credibility interval; *Maximum daily dosage.
Paracetamol <2000mg
Paracetamol 3000mg
*Paracetamol 3900-4000mg
Rofecoxib 12.5mg
*Rofecoxib 25mg
Rofecoxib 50mg
Lumiracoxib 100mg
*Lumiracoxib 200mg
Lumiracoxib 400mg
Etoricoxib 30mg
*Etoricoxib 60mg
Etoricoxib 90mg
Diclofenac 70mg
Diclofenac 100mg
*Diclofenac 150mg
Celecoxib 100mg
Celecoxib 200mg
*Celecoxib 400mg
Naproxen 750mg
*Naproxen 1000mg
Ibuprofen 1200mg
*Ibuprofen 2400mg
-0.07 (-0.41, 0.27)
-0.16 (-0.66, 0.33)
-0.16 (-0.27, -0.06)
-0.42 (-0.51, -0.33)
-0.50 (-0.59, -0.41)
-0.61 (-0.85, -0.38)
-0.34 (-0.45, -0.22)
-0.34 (-0.44, -0.24)
-0.43 (-0.58, -0.27)
-0.49 (-0.62, -0.36)
-0.58 (-0.73, -0.43)
-0.61 (-0.90, -0.32)
-0.22 (-0.60, 0.17)
-0.34 (-0.58, -0.10)
-0.57 (-0.70, -0.44)
-0.16 (-0.30, -0.02)
-0.36 (-0.43, -0.29)
-0.33 (-0.46, -0.19)
-0.05 (-0.42, 0.32)
-0.39 (-0.48, -0.30)
-0.29 (-0.85, 0.27)
-0.42 (-0.55, -0.30)
Active treatment better Placebo better
0-1.25 -1 -.75 -.5 -.25 .25 .5
Intervention Effect size (95% CI)

WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
41 | 42
Web-appendix 10. Comparison adjusted funnel plots
Web-appendix Figure 11. Comparison adjusted funnel plot for the outcome pain.
0.1
.2S
tand
ard
err
or
of
effe
ct
siz
e
-.5 -.25 0 .25 .5Effect size centred at comparison-specific pooled effect (yiXY-µXY)
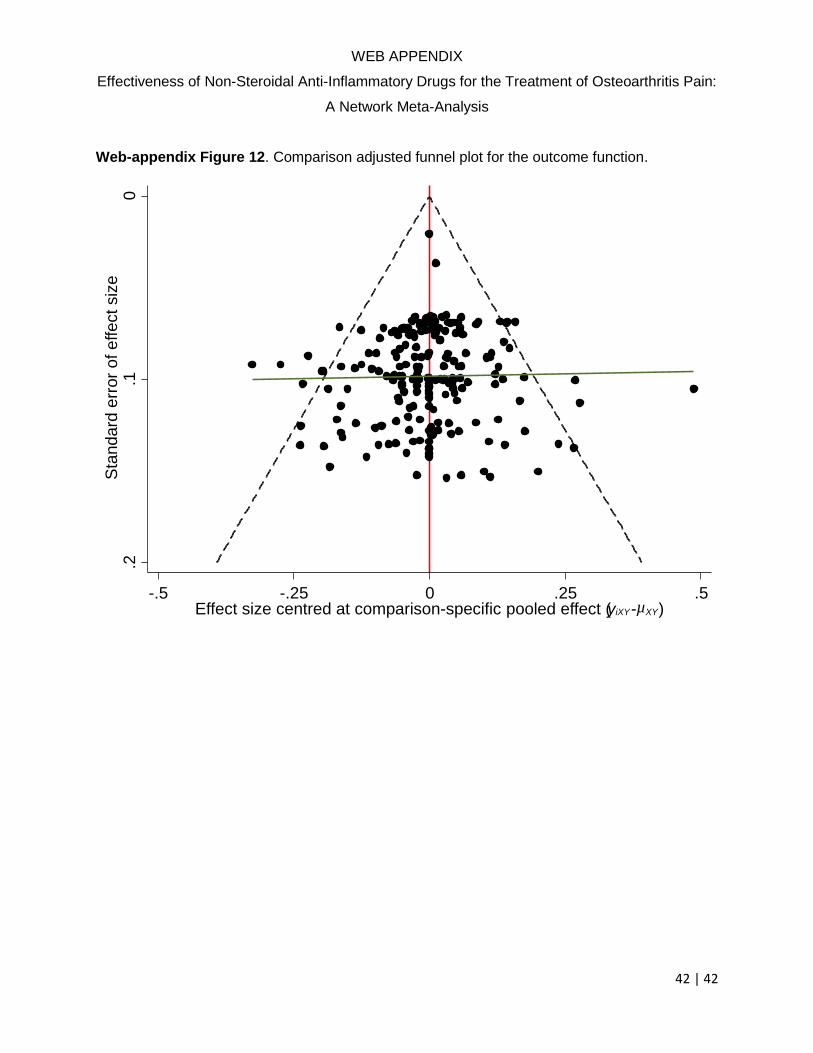
WEB APPENDIX
Effectiveness of Non-Steroidal Anti-Inflammatory Drugs for the Treatment of Osteoarthritis Pain:
A Network Meta-Analysis
42 | 42
Web-appendix Figure 12. Comparison adjusted funnel plot for the outcome function.
0.1
.2S
tandard
err
or
of
effect
siz
e
-.5 -.25 0 .25 .5Effect size centred at comparison-specific pooled effect (yiXY-µXY)

Protocol for a systematic review and network
meta-analysis
Clinical effectiveness of non-steroidal anti-
inflammatory drugs: a comprehensive network
meta-analysis
Authors: Trelle S, Nüesch E, Jüni P
Date: September 25, 2012 (replaces version of December 7th, 2010)
Content
Background ............................................................................................................................ 2 Objectives ............................................................................................................................... 2
Criteria for considering studies for this review ...................................................................... 3 Types of studies .................................................................................................................. 3
Types of participants .......................................................................................................... 3 Types of interventions ........................................................................................................ 3 Types of outcome measures ............................................................................................... 3
Search methods for identification of studies .......................................................................... 3 Electronic searches ............................................................................................................. 3
Searching other ressources ................................................................................................. 4 Data collection and analysis ................................................................................................... 4
Selection of studies ............................................................................................................. 4 Data extraction and management ....................................................................................... 4
Assessment of risk of bias in included studies ................................................................... 5
Measures of treatment effect .............................................................................................. 5
Data synthesis ..................................................................................................................... 6 Role of the funding source ................................................................................................. 7 References .......................................................................................................................... 7
Change history ........................................................................................................................ 9
Protocol for a systematic review and network meta-analysis Clinical effectiveness of non-steroidal anti-inflammatory drugs: a comprehensive network meta-analysis
September 25, 2012 2 | 9
Background
Pain is the most relevant symptom of osteoarthritis from a patient perspective with a major
impact on quality-of-life (1). Management of pain is based on a sequential, hierarchical
approach with non-steroidal anti-inflammatory drugs being among the most often used
interventions (2). Several systematic reviews investigated the effectiveness of these agents (3).
However, previous systematic reviews only considered direct evidence from head-to-head
comparisons and did not aim at synthesizing all available evidence. Moreover, review authors
often refrained from conducting a meta-analyses because of differences in outcome measures
reported in individual trials therefore limiting their use for informing clinical practice.
As noted in the previous section most meta-analyses consider pair-wise, direct comparisons of
interventions. This makes it often difficult to determine the best treatment. Indirect
comparisons are often needed to establish a 'ranking' (sometimes called league table) of
interventions. For example, we indirectly compare naproxen and diclofenac if naproxen is
only tested versus rofecoxib and diclofenac is only tested versus rofecoxib. Usually, these
indirect comparisons are done informally which increases the risk of bias. Suppose that
rofecoxib is better than diclofenac and naproxen is better than rofecoxib. Then it is usually
assumed that naproxen is better than diclofenac. In the field of non-steroidal anti-
inflammatory drugs, however, the situation is actually more complex with several
preparations tested (see figure below). The method of network-meta-analysis allows to
combine the available information in one meta-analysis and to rank interventions accordingly.
This approach provides estimates of treatment differences and assesses the uncertainties in
these estimates by detecting heterogeneity and inconsistencies among the trials. It is
especially useful in situations with many different interventions (4).
Objectives
The overarching aim of the project is to describe the current evidence of pharmacological pain
management for osteoarthritis. The proposed network meta-analysis will enable us:
To summarize and compare the effectiveness of non-steroidal anti-inflammatory drugs
(NSAIDs), including cox-2 selective inhibitors and acetaminophen, in terms of pain
relief, improvement of physical function, and quality of life.
To rank the different preparations according to their effectiveness.
To provide a risk-benefit perspective of the different preparations (taking into
consideration results of other network meta-analysis on cardiovascular and
gastrointestinal safety).

Protocol for a systematic review and network meta-analysis Clinical effectiveness of non-steroidal anti-inflammatory drugs: a comprehensive network meta-analysis
September 25, 2012 3 | 9
Criteria for considering studies for this review
Types of studies
Randomized-controlled trials with at least 100 patients per trial arm. Trials only published as
abstract will be excluded.
Types of participants
Patients with osteoarthritis of the hip or knee (trials with mixed populations must either report
results separately or must have included at least 80% patients in the relevant comparisons in
order to be eligible).
Types of interventions
Comparisons of oral
Placebo,
Paracetamol, or
Non-steroidal anti-inflammatory drug(s) included in our safety analyses (GI and CV).
Consequently, the following comparisons are eligible: placebo vs. paracetamol, placebo vs.
NSAID, paracetamol vs. NSAID, NSAID vs. NSAID.
NSAIDs not licensed in the USA, UK, Germany and Switzerland will be excluded.
Types of outcome measures
Primary outcome
The primary outcome measure will be reduction in pain. Several methods to assess pain are
employed in clinical trials in osteoarthritis. We will use a hierarchy of pain outcomes that is
informed by a PhD project at the Institute of Social and Preventive Medicine Bern and extract
the outcome that is highest in this hierarchy (5).
Secondary outcomes
Function-related and quality-of-life outcomes will be extracted as secondary outcomes
whenever available. As with the pain-related primary outcomes we will employ a hierarchy
informed by the PhD project.
Search methods for identification of studies
Electronic searches
The Cochrane Central Register of Controlled Trials (CENTRAL) will be searched from
inception until December 31th, 2010 using the following search terms:
Text words
osteoarthriti* OR
osteoarthro* OR

Protocol for a systematic review and network meta-analysis Clinical effectiveness of non-steroidal anti-inflammatory drugs: a comprehensive network meta-analysis
September 25, 2012 4 | 9
gonarthriti* OR
gonarthro* OR
coxarthriti* OR
coxarthro* OR
arthros* OR
arthrot*.
MeSH terms
Osteoarthritis (explode all trees)
N.B. this is the search strategy used for the PhD (Bruo da Costa).
Searching other ressources
We will screen reference lists of all obtained articles, including relevant reviews. Finally, we
will search clinical trial registries through the WHO International Clinical Trials Registry
Platform (ICTRP; http://apps.who.int/trialsearch/) .
Data collection and analysis
Selection of studies
Two review authors will independently evaluate all identified potentially eligible titles and
abstracts for eligibility. Disagreements will be resolvedby discussion. No language
restrictions will be applied. If multiple reports describe the same trial, we will consider the
most comprehensive information. In case of discrepencies, information submitted to
regulatory authorities will take precedence over peer-reviewed information and non-peer
reviewed information and more up-to-date information will take precedence over older
information.
Data extraction and management
Two review authors will extract trial information independently using a standardised, piloted
data extraction form accompanied by a codebook. Disagreements will be resolved by
consensus or discussion with a third author. The following information will be extracted:
Trial design (including eligibility criteria of patients)
Publication status
Type and source of financial support
Trial size
Details of intervention including dosage and treatment duration
Patient characteristics (average age, gender, mean duration of symptoms)
Protocol for a systematic review and network meta-analysis Clinical effectiveness of non-steroidal anti-inflammatory drugs: a comprehensive network meta-analysis
September 25, 2012 5 | 9
Type of pain- or function-related outcome
Duration of follow up
Outcome data for each timepoint of interest (see below: ). When necessary, we will
approximate means and measures of dispersion from figures in the reports. For cross-
over trials, we will extract data from the first period only, because of possible carry-
over effects. Whenever possible, we will use results from an intention-to-treat analysis.
If we can not calculate effect sizes, we will contact the authors for additional data.
Assessment of risk of bias in included studies
Two review authors will independently assess randomisation, blinding, and adequacy of
analyses. Disagreements will be resolved by consensus. We will assess two components of
randomisation: generation of allocation sequences and concealment of allocation. We will
consider the generation adequate if it resulted in unpredictable allocation sequences;
mechanisms considered adequate include random-number tables, computer-generated random
numbers, minimisation, coin tossing, shuffling of cards, and drawing of lots. We will consider
allocation concealment adequate if the investigators responsible for patient selection were
unable to deduce before allocation which treatment was next; methods considered adequate
included central randomisation and sequentially numbered, sealed, opaque envelopes. We will
consider blinding of the patients adequate if the interventions were explicitly described as
indistinguishable. We will consider analyses adequate if all randomised patients were
included in the analysis according to the intention-to-treat principle.
Measures of treatment effect
All outcomes will be continuous outcomes expressed as effect sizes over time. Outcome data
will be extracted and analysed for the following timepoints of interest: up to 3 months, 6
months, 9 months, 12 months, 15 months, 18 months, 21 months, 24 months, 27 months, 30
months, 33 months, 36 months (all with in a window of 1.5 months; if a trial reports more
than one measurement per time window the nearest to the timepoint of interest will be used
for the analysis).
Effect sizes will be calculated by dividing the differences in mean values in a time-window
between treatment groups by the median pooled standard deviation observed across all time-
points in a trial (6). If standard deviations are not provided, we will calculate them from
standard errors, confidence intervals, or p-values as described elsewhere (5, 7). To allow
intuitive interpretation of pooled effects, we will back transform effect sizes to differences on
a 10 cm visual analogue scale (VAS) on the basis of a median pooled SD of 2.5 cm found in
large-scale osteoarthritis trials that assessed pain on a 10 cm VAS (8). In addition, we will
compare results with the pre-specified minimal clinically important difference which is based
on the median minimal clinically important difference found in recent studies in patients with
osteoarthritis (9-12) of 0.37 standard deviation units, corresponding to 0.9 cm on a 10 cm
VAS.

Protocol for a systematic review and network meta-analysis Clinical effectiveness of non-steroidal anti-inflammatory drugs: a comprehensive network meta-analysis
September 25, 2012 6 | 9
Data synthesis
We will use a Bayesian random effects model which fully preserves randomized treatment
comparisons within trials and which allows for multiple follow-up times (13). It fully
preserves the within-trial randomized treatment comparison of each trial while combining all
available comparisons between treatments, and accounts for multiple comparisons within a
trial in case of more than two treatment arms (14, 15). For the analysis of effect sizes, the
model include random-effects at the level of trials and time-points. It accounts for the
correlation of outcome data reported at different time-points within a trial and allows the
estimation of the between-trial variance of treatment effects τ2. The between-trial
heterogeneity will be estimated from the median between-trial variance τ² observed in the
posterior distribution (accompanied by the 5th and 95th percentile). To determine whether the
variation of treatment effects over time is over and above of what would be expected by
chance, we will calculate a p-value for heterogeneity across time-points of follow-up (16).
The p-value will be derived from the proportion of observations of the posterior distribution
of the variance observed across time-points within trials smaller than or equal to the within-
trial variance typically found in large osteoarthritis trials (0.01 expressed on an effect size
scale, 0.0625 expressed on a 10 cm VAS). We will use the following prior distributions for
the heterogeneity parameters: a gamma distribution for between-trial heterogeneity (1/τ² ~
gamma(0.001,0.001)I(0,2000)), and a uniform distribution for between-timepoint
heterogeneity (τ ~ unif(0,50)). In a sensitivity analysis we will use the uniform prior also for
the between-trial heterogeneity. The consistency of the network will be determined by use of
inconsistency factors: the estimated difference between the effect size from direct
comparisons within randomized trials and the effect size from indirect comparisons between
randomized trials with one intervention in common (17). Estimates of variation and
consistency will be presented based on back transformations to differences on a 10 cm VAS.
Goodness of fit will be assessed by use of Q-Q-plots.
Analyses will be performed using Markov chain Monte Carlo methods. Convergence of
Markov chains will be deemed to be achieved if plots of the Gelman-Rubin statistics indicate
that widths of pooled runs and individual runs stabilize around the same value and their ratio
around one (18). We will use Stata (StataCorp LP 2005. Stata Statistical Software: Release 11.
College Station, TX) and WinBUGS (MRC Biostatistics Unit 2007. Version 1.4. Cambridge,
UK) for all analyses.
Additional analyses
To explore possible time trends of treatment estimates in the trials we will include a linear
term for time as covariate in the analyses. If data allows non-linear terms for time will be also
explored.
To explore robustness of results, we will include characteristics of the trials as covariates in
the network meta-analysis to estimate effects according to concealment of allocation;
intention-to-treat analysis; high methodological quality defined as adequate concealment of
allocation, adequate blinding of patients and the presence of an intention-to-treat analysis;

Protocol for a systematic review and network meta-analysis Clinical effectiveness of non-steroidal anti-inflammatory drugs: a comprehensive network meta-analysis
September 25, 2012 7 | 9
source of funding (industry independent versus other); minimum joint pain required for entry
into the trial. P-values for interaction between trial characteristics and treatment effect will be
derived from the posterior distribution of covariates and can be interpreted in the same way as
a traditional p-value for interaction (19). Finally, we will perform pair-wise meta-analyses
with random-effects at the level of trials and time-points, as well as a simpler network
approach including only one treatment effect per trial (absolute pain intensity at the longest
follow-up available).
Role of the funding source
ARCO foundation will have no role in study design, data collection, data synthesis, data
interpretation, writing the report, or the decision to submit the manuscript for publication.
None of the authors is affiliated with or funded by any manufacturer of any of the agents
evaluated in this study.
References
1. Rosemann T, Wensing M, Joest K, Backenstrass M, Mahler C, Szecsenyi J. Problems
and needs for improving primary care of osteoarthritis patients: the views of patients, general
practitioners and practice nurses. BMC Musculoskelet Disord. 2006;7:48. [PMID: 16749935]
2. Porcheret M, Jordan K, Jinks C, Croft P. Primary care treatment of knee pain--a survey
in older adults. Rheumatology (Oxford). 2007;46:1694-700. [PMID: 17938135]
3. Chen YF, Jobanputra P, Barton P, Bryan S, Fry-Smith A, Harris G, et al.
Cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs (etodolac, meloxicam,
celecoxib, rofecoxib, etoricoxib, valdecoxib and lumiracoxib) for osteoarthritis and
rheumatoid arthritis: a systematic review and economic evaluation. Health Technol Assess.
2008;12:1-278, iii. [PMID: 18405470]
4. Caldwell DM, Ades AE, Higgins JP. Simultaneous comparison of multiple treatments:
combining direct and indirect evidence. BMJ. 2005;331:897-900. [PMID: 16223826]
5. Reichenbach S, Sterchi R, Scherer M, Trelle S, Burgi E, Burgi U, et al. Meta-analysis:
chondroitin for osteoarthritis of the knee or hip. Ann Intern Med. 2007;146:580-90. [PMID:
17438317]
6. Cohen J. Statistical power analysis for the behavioral sciences. Hillsdale: Lawrence
Erlbaum; 1988.
7. Follmann D, Elliott P, Suh I, Cutler J. Variance imputation for overviews of clinical
trials with continuous response. J Clin Epidemiol. 1992;45:769-73. [PMID: 1619456]
8. Nüesch E, Trelle S, Reichenbach S, Rutjes AW, Bürgi E, Scherer M, et al. The effects
of the exclusion of patients from the analysis in randomised controlled trials: meta-
epidemiological study. BMJ. 2009;339:b3244.
9. Eberle E, Ottillinger B. Clinically relevant change and clinically relevant difference in
knee osteoarthritis. Osteoarthritis Cartilage. 1999;7:502-3. [PMID: 10489324]
10. Angst F, Aeschlimann A, Stucki G. Smallest detectable and minimal clinically important
differences of rehabilitation intervention with their implications for required sample sizes
using WOMAC and SF-36 quality of life measurement instruments in patients with
osteoarthritis of the lower extremities. Arthritis Rheum. 2001;45:384-91. [PMID: 11501727]
11. Angst F, Aeschlimann A, Michel BA, Stucki G. Minimal clinically important
rehabilitation effects in patients with osteoarthritis of the lower extremities. J Rheumatol.
2002;29:131-8. [PMID: 11824949]

Protocol for a systematic review and network meta-analysis Clinical effectiveness of non-steroidal anti-inflammatory drugs: a comprehensive network meta-analysis
September 25, 2012 8 | 9
12. Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi W. Minimal clinically important
changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur J
Pain. 2004;8:283-91. [PMID: 15207508]
13. Wandel S, Reichenbach S, Tendal B, Nüesch E, Juni P, Trelle S. Effectiveness of
chondroitin, glucosamine, or the combination of both in the treatment of osteoarthritis: a
network meta-analysis. 2009:Submitted.
14. Cooper NJ, Sutton AJ, Lu G, Khunti K. Mixed comparison of stroke prevention
treatments in individuals with nonrheumatic atrial fibrillation. Arch Intern Med.
2006;166:1269-75. [PMID: 16801509]
15. Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment
comparisons. Stat Med. 2004;23:3105-24. [PMID: 15449338]
16. Stettler C, Allemann S, Wandel S, Kastrati A, Morice MC, Schomig A, et al. Drug
eluting and bare metal stents in people with and without diabetes: collaborative network meta-
analysis. BMJ. 2008;337:a1331. [PMID: 18757996]
17. Lu G, Ades AE. Assessing evidence inconsistency in mixed treatment comparisons. J.
Am. Stat. Assoc. . 2006;101:447–59.
18. Brooks S, Gelman A. Alternative methods for monitoring convergence of iterative
simulations. Journal of Computational and Graphical Statistics. 1998;7:434-55.
19. Altman DG, Bland JM. Interaction revisited: the difference between two estimates. BMJ.
2003;326:219. [PMID: 12543843]

Protocol for a systematic review and network meta-analysis Clinical effectiveness of non-steroidal anti-inflammatory drugs: a comprehensive network meta-analysis
September 25, 2012 9 | 9
Change history
Changes from version December 7th, 2010 to version September 25, 2012
1. Clarification that only NSAIDs included in our safety analyses (CV and GI) are
eligible for this analysis.